eating disorders in teens: anorexia/bulimia michelle stauffer, spt amber stanback, rn alison...
TRANSCRIPT

Eating Disorders in Teens:
Anorexia/BulimiaMichelle Stauffer, SPTAmber Stanback, RNAlison Baumann, RN

Eating Disorders: Anorexia Nervosa
• Potentially life threatening eating disorder characterized by self-starvation and excessive weight loss
• 90-95% with this disorder are women
• Highest death rates of any mental health condition
• Typically appears in early to mid-adolescence
• Affects many minorities but exact stats are not available
Photo: http://www.clinicaladvisor.com/anorexia-and-bulimia-warning-signs/slideshow/705/#3

Warning Signs: Anorexia Nervosa
Photo: http://www.methodsofhealing.com/five-anorexia-myths/
• Warning Signs:
o Dramatic weight loss
o Preoccupation with weight, food, calories, fat grams, and dieting
o Refusal to eat certain foods to even cutting out entire food groups
o Comments/anxiety of being overweight
o Denial of hunger
o Development of food rituals
o Consistent excuses to avoid mealtime
o Excessive, rigid exercise program despite the weather, fatigue, illness, or injury
o Withdrawal from usual activities and friends

Health Consequences/Physical Findings:
Anorexia Nervosa• The body is denied of essential
nutrients that it needs to function normally and it is forced to slow down and conserve energy
• Abnormally slow heart rate and low blood pressure results which increases the risk for heart failure
• Reduction in bone density leads to brittle bones
• Muscle loss and weakness
• Severe dehydration which can lead to kidney failure
• Fainting and fatigue are common
• Dry skin and hair along with hair loss
• Growth of lanugo all over body in attempts to keep body in body heat
Photo: http://www.clinicaladvisor.com/anorexia-and-bulimia-warning-signs/slideshow/705/#2

Eating Disorders: Bulimia
• Psychological and life threatening eating disorder characterized by ingestion of an abnormally large amount of food, followed by purging of food so weight isn’t gained. o Purging is to prevent weight gain, establish a sense of
control, or to cope with difficult circumstances
• Causes are unknown but may be attributed to genetics, environmental, physiological, and cultural influences.
• 80% of patients are female; affects 1-2% of adolescent-young women
• Frequently associated with depression and changes in social adjustment
• Most appear of average body weight and recognize their behaviors as abnormal
• May not appear as struggling because eating disorder behaviors are hidden
Warning Signs: Bulimia
• Warning Signs
o Disappearance of large amounts of food in short periods of time
o Finding wrappers and containers indicating consumption of large amounts of food
o Followed by frequent trips to the bathroom, signs or smells of vomiting, presence of laxatives or diuretics
o Excessive, rigid exercise
o Unusual swelling of cheeks or jaws
o Discoloration of teeth
o Withdrawal from friends and usual activities
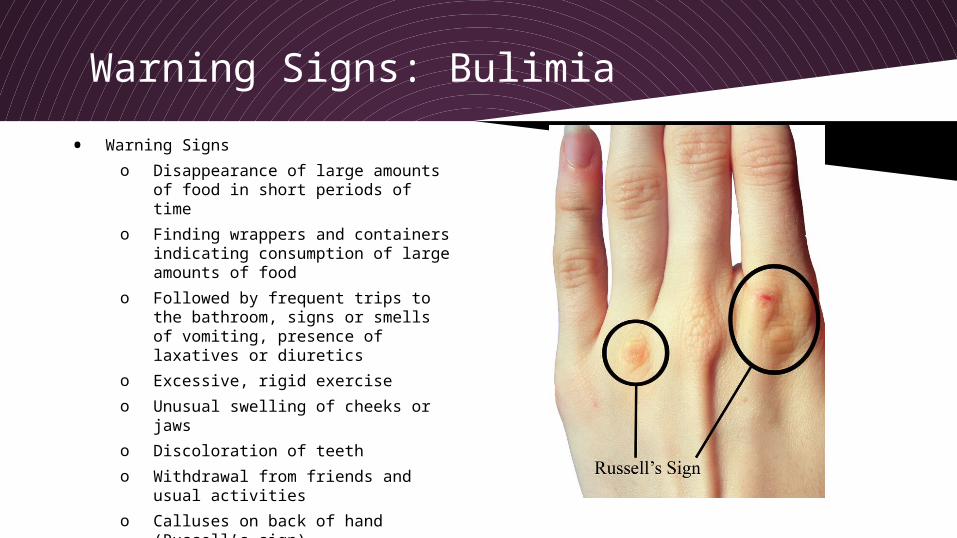
o Calluses on back of hand (Russell’s sign)
Photo: http://commons.wikimedia.org/wiki/File%3ARussell's_Sign.png (Public Domain image)

Health Consequences/Physical Findings: Bulimia• Binge-and-purge can damage the
entire digestive system
• Purging can lead to electrolyte and chemical imbalances in the body that can affect the heart and other major organ functionso Irregular heartbeats, heart
failure, and even death
• Tooth decay and staining from stomach acids being released when vomiting
• Chronic irregular bowel movements and constipation as a result of laxative abuse
Photo: http://commons.wikimedia.org/wiki/File:Oral_manifestation_of_Bulimia..jpg

Tests for Anorexia and Bulimia
• The Practice Guideline for the Treatment of Patients With Eating Disorders, Third Edition, does not recommend specific test for diagnosis. Laboratory blood tests will likely be abnormal, but will normalize as the patient condition begins to improve.3
• The following are recommended for overall health screening:
o Blood chemistry studies (including electrolytes, BUN, creatinine, TSH)
o CBC with differential
o Erythrocyte sedimentation rate
o UA
• For severely malnourished or symptomatic patients:
o Blood chemistry (Ca, Mg, Phos, ferritin)
o ECG
o 24-hour urine for creatinine clearance
• For amenorrheic for >6 months
o Dual-energy x-ray absorptiometry
o Serum estradiol in female patients
o Serum testosterone in male patients

DSM-IV Diagnostic Criteria for Anorexia Nervosa and Bulimia Nervosa6
BULIMIA NERVOSA (307.51)
1. Recurrent episodes of binge eating. An episode of binge eating is characterized by both of the following:( A) eating, in a discrete period of time (e.g., within any two-hour period), an amount of food that is definitely larger than most people would eat during a similar period of time and under similar circumstances;and (B) a sense of lack of control over eating during the episode (e.g., a feeling that one cannot stop eating or control what or how much one is eating).
2. Recurrent inappropriate compensatory behavior in order to prevent weight gain, such as self-induced vomiting; misuse of laxatives, diuretics, or other medications; fasting; or excessive exercise.
3. The binge eating and inappropriate compensatory behaviors both occur, on average, at least twice a week for three months.
4. Self-evaluation is unduly influenced by body shape and weight. 5. The disturbance does not occur during episodes of anorexia nervosa.
Specific Type:
Purging Type: During The current episode of bulimia nervosa, the person has regularly engaged in self-induced vomiting or the misuse of laxatives, diuretics, or enemas.
Non Purging Type: During The current episode of bulimia nervosa, the person has used other compensatory behaviors, such as fasting or excessive exercise, but has not engaged in self-induced vomiting or the misuse of laxatives,diuretics,or enemas.
ANOREXIA NERVOSA (307.1)
1. Refusal to maintain body weight at or above a minimally normal weight for age and height (e.g., weight loss leading to maintenance of body weight less than 85% of that expected; or failure to make expected weight gain during period of growth, leading to body weight less than 85% of that expected).
2. Intense fear of gaining weight or becoming fat, even though underweight.
3. Disturbance in the way in which one's body weight or shape is experienced, undue influence of body weight or shape on self-evaluation, or denial of the seriousness of the current low body weight.
4. In postmenarcheal females, amenorrhea (i.e., the absence of at least three consecutive menstrual cycles).
Specific Type:
Restricting Type: During the current episode of anorexia nervosa,the person has not regularly engaged in binge-eating or purging behavior (i.e., self-induced vomiting or the misuse of laxatives,diuretics, or enemas).
Binge-Eating/Purging Type: During The current episode of anorexia nervosa, the person has regularly engaged in binge-eating or purging behavior (i.e., self-induced vomiting or the misuse of laxatives, diuretics, or enemas)
(Massey-Stokes, 2000)
Treatment
• Bulimia: o Therapy needs to be integrated
because these individual have a negative body image and poor self esteem
o Addressing the underlying issues related to bulimia along with psychotherapy methods can dramatically improve recovery
o Need to break the binge-purge cycle and restore normal eating
o Change irrational beliefs about weight, body shape, and dieting
o Need to heal from emotional issues that may have caused the eating disorder
o Dental treatment to repair/restore damage
o Physical therapy to improve de-conditioned state
• Anorexia: o Underlying psychological,
interpersonal, and cultural forces that are contributing need to be addressed
o Psychologist, psychiatrist, social worker, nutritionist, and medical doctor all need to work together in providing care.
o Physical therapy to improve de-conditioned state
Photo: www.shutterstock.com

Referral & Follow up
• For eating disorders patient should be referred to psychotherapy or psychological counseling, coupled with careful attention to medical and nutrition needs as soon as possible for best outcomes.
• Dental referral is indicated for bulimia patients.
• Physical therapy for deconditioned patients
• Patient must be continually monitored by family and health care professional throughout treatment for relapse or issues that would hinder further progression.
• Other resources that may be beneficial for patients with eating disorders are group therapy sessions along with antidepressants.

Who is Affect by Eating Disorders?
There is NO Discrimination:
Eating Disorders affect every• Age
o Anorexia average age of onset: 19 years5
No statistically significant lifetime rates for all age groups
o Bulimia average age of onset: 20 years5
Age 20-59 have higher rates of bulimia than those >60
• Race
o Rates are similar across all racial groups
• Gender
o An estimated 10-15% of people with anorexia or bulimia are male5
• Socio-economic Status
o It has been found that more accultured women have higher eating disorder patternsPhoto: www.examiner.com
Why Teenagers and Young Adults?
According to the Healthy People 2020 adolescents are in a “developmental transition”.
● Adolescents are very sensitive to environmental influences○ Family○ Peer group○ School○ Neighborhood○ Societal cues
“Adolescence is a critical transitional period that includes the biological changes of puberty and the need to negotiate key developmental tasks, such as increasing independence and normative experimentation” (Healthy People 2020)

Physical Cues Health Professionals should be aware of in patients with
eating disordersDuring an assessment potential Warning Signs are:
• Malnutrition
• Interference with pubertal development
• Fatigue and dizziness
• Inability to concentrate
• Unhealthy hair, skin, nails
• Less of tooth enamel
• Stomach problems
• Lowered metabolic rate
• Amenorrhea
• Undeveloped bones and bone loss
• Damage to the esophagus, heart, kidneys, digestive system, colon, and reproductive system
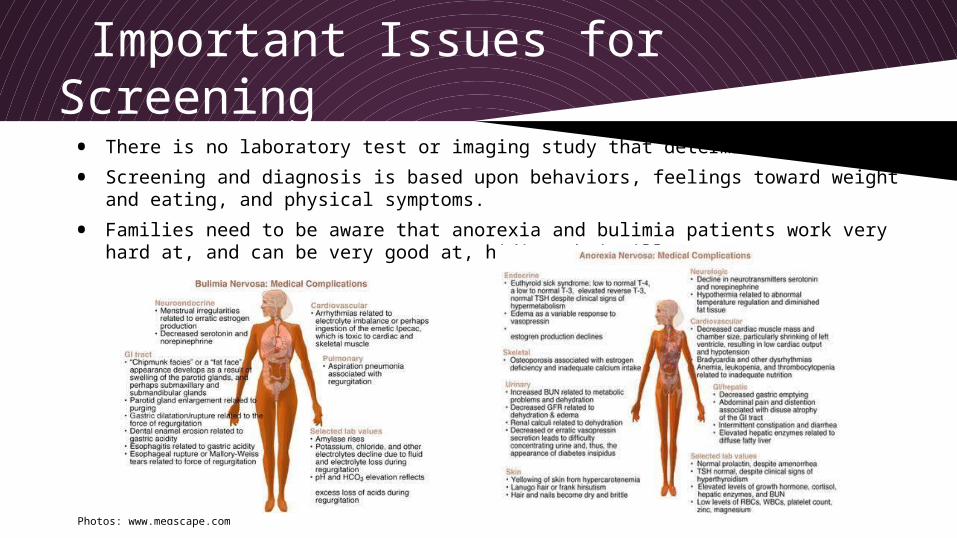
Important Issues for Screening
• There is no laboratory test or imaging study that determines diagnosis.
• Screening and diagnosis is based upon behaviors, feelings toward weight and eating, and physical symptoms.
• Families need to be aware that anorexia and bulimia patients work very hard at, and can be very good at, hiding their illness.
Photos: www.medscape.com
Photos: www.medscape.com

Education is the KeyEducation is considered one of the primary
vehicles for prevention 6

ResourcesBooks:Agras WS, Apple RF: Overcoming Eating Disorders: A Cognitive-
Behavioral Treatment for Bulimia Nervosa and Binge-Eating Disorder. New York, Oxford University Press, 1997
Cash TF: The Body Image Workbook: An 8-Step Program for Learning to Like Your Looks. Oakland, CA, New Harbinger, 1997
Goodman LJ, Villapiano M: Eating Disorders: The Journey to Recovery Workbook.New York, Brunner-Routledge, 2001 (client workbook)
Goodman LJ, Villapiano M: Eating Disorders: Time for Change. Plans, Strategies, and Worksheets. New York, Brunner-Routledge, 2001 (therapist workbook)
Bulik CM, Taylor N: Runaway Eating: The 8-Point Plan to Conquer Adult Food and Weight Obsessions. New York, Rodale Books, 2005
Goodman LJ, Villapiano M: Eating Disorders: The Journey to Recovery Workbook.New York, Brunner-Routledge, 2001 (client workbook)
Lock J, le Grange D: Help Your Teenager Beat an Eating Disorder. New York, Guilford, 2005
Walsh BT, Cameron VL: If Your Child Has an Eating Disorder: An Essential Resource for Parents. New York, Guilford, 2005
Internet resources for healthcare professionals:
Academy for Eating Disorders (http://www.aedweb.org)
Internet resources for patients, families, and professionals:
National Eating Disorders Association (http://www.nationaleatingdisorders.org)
National Association of Anorexia Nervosa and Associated Disorders (http://www.anad.org/site/anadweb/)
Eating Disorder Referral and Information Center (
http://www.edreferral.com)
Something Fishy (http://www.something-fishy.org; a well-
monitored advocacy site)
References1. Jacquelyn Ekern, MS, LPC. Bulimia nervosa: causes, symptoms, signs, and treatment. Eating Disorder Education and
Awareness. 2014. Available at: http://www.eatingdisorderhope.com/information/bulimia. Accessed February 2014.
2. National Eating Disorder Association.Anorexia nervosa. Information on Eating Disorders. 2011. Available at: http://www.nationaleatingdisorders.org/anorexia-nervosa. Accessed February 2014.
3. Yager, Joel, Michael Devlin, Katherine Halmi, David Herzog, James Mitchell, Pauline Powers, Kathryn Zerbe. “Practice Guidelines for the Treatment of Eating Disorders, Third Edition”. 2013 Available at: http://psychiatryonline.org/content.aspx?bookid=28§ionid=1671334. Accessed February 2014
4. Herpertz S, Hagenah U, Vocks S, von Wietersheim, Cuntz U, Zeeck A. The Diagnosis and Treatment of Eating Disorders. Deutsches Aerzteblatt International [serial online]. October 6, 2011;108(40):678-685. Available from: CINAHL Plus with Full Text, Ipswich, MA. Accessed February 14, 2014.
5. National Institutes of Mental Health. Eating Disorders. 2007. Available at: http://www.nimh.nih.gov/health/publications/eating-disorders/index.shtml. Accessed February 2014
6. Massey-Stokes, M. S. (2000, Jul.-Aug.). Prevention of Disordered Eating among Adolescents. TheClearingHouse,73(6),335-340.
I pledge to support the Honor System of Old Dominion University. I will refrain from any form of academic dishonesty or deception, such as cheating or plagiarism. I am aware that as a mamber of the academic community it is my responsibility to turn in all suspected violators of the Honor Code. I will report to a hearing if summond.Alison BaumannMichelle StaufferAmber StanbackFebruary 15, 2014