ectopic pancreas and the islet cell dysmaturational … · exclude other causes of hypoglycemia ......
TRANSCRIPT

ANNALS O F CLINICAL AND LABORATORY SCIEN CE, Vol. 21, No. 1Copyright © 1991, Institute for Clinical Science, Inc.
Ectopic Pancreas and the Islet Cell Dysmaturational Syndrome*
STEPHEN QUALMAN, M .D .f, DONNA CANIANO, M.D.rj:,
DENIS KING, M .D 4 and WILLIAM ZIPF, M .D.§
Divisions o f Pediatric Pathology f , Pediatric Surgeryt, and Pediatric Endocrinology§,
Departments o f Pathology, Surgery, and Pediatrics, Ohio State University and Childrens Hospital,
Columbus, OH 43205
ABSTRACT
Two cases of ectopic pancreas are described in the setting of the islet cell dysmaturational syndrome. Microscopic and immunostaining studies revealed both lesions to be composed of primarily (80 percent to 90 percent) is let tissue with nuclear hyperchromasia and probable depletion of immunoreactive insulin in one case. Persistent hyperinsulinemic hypoglycemia required a second laparotomy with resection of ectopic pancreas in one case. Awareness of the phenom enon led to successful identification and resection of ectopic islet tissue on first surgery in a subsequent case. Ectopic pancreas is a relatively common developmental pancreatic anomaly, and knowledge of its potential contribution to life-threatening hypoglycemia may obviate the need for multiple surgeries in some cases of islet cell dysmaturational syndrome.
Introduction th e pancreas p ro p er. Two cases arereported of ectopic pancreas in infants
Islet cell dysmaturational syndrome is w ith h yperin su linem ic hypoglycem iaa general designation for the spectrum of and associated intrapancreatic islet cellhistopathologic changes in the pancreas .lesion's. T he o rig in of th ese ec top icthat are associated with hyperinsulin- lesions and th e ir possib le functionalemic hypoglycemia and its presentation ac tiv ity have im p o rta n t th e ra p e u ticduring infancy .2 The usual pathologic implications',finding in this se tting 11 has been the presence of islet cell lesions lim ited to
M aterials and M ethods
* Send rep rin t requests to: S tephen J. Qualman, M .D ., Chief, D epartm en t o f Laboratory M edicine, C h i ld r e n ’s H o s p ita l , 700 C h i ld r e n ’s D r iv e , Colum bus, O H 43205.
This pap er was p re sen te d at th e Association of C lin ica l S c ien tis ts M ee tin g , C in c in n a ti , O h io , N ovem ber 10, 1990.
P a t ie n t s
Case 1: This w hite female infant was the 36-week gestational age, 3.82 kilogram product of a 28-year- old Gravida 1, Para 1 O-positive m other whose pregnancy was uncom plicated, with vaginal delivery. In itial dextrose stick at 30 m inutes of life was less than
190091-7370/91/0100-0019 $01.20 © Institute for Clinical Science, Inc.

20 QUALMAN, CANIANO, KING, AN D ZIPF
25 m g per dL. D esp ite oral and intravenous boluses of glucose, th e infant rem ained persistently hypoglycemic. An initial insulin level was m easured a t 142.8 U p e r ml w ith a glucose level of 13.
Serum glucose control was difficult, necessitating frequen t increases in dextrose load. Diazoxide was utilized w ithout any effect. A persisten t hypoglycem ia rem ained in the face of hypertonic glucose infusions and elevated insulin levels. On th e 18th day of life, a subtotal (90 to 95 percent) pancreatectom y was perform ed.
A fter surgery, p e rs is ten t hypoglycem ia necessita ted in stitu tio n of to ta l p a ren tera l n u tritio n and p lacem en t on a som atostatin protocol to increase serum glucose. Because of unstable glucose levels, the pa tien t was re tu rn ed to the operating room th ree m onths later for exploratory laparotom y and a total pancreatectomy.
T he p a tie n t has done w ell postoperatively w ith gradual weaning from total parentera l nutrition and institution of oral feedings which she has to lerated w ell. T h ree y ears a fte r su rg e ries , sh e has b een trea te d w ith pancreatic exocrine enzym e rep lacem en t, n o c tu rn a l feed in g s th ro u g h a gastrostom y tube, and in te rm itten t cornstarch feedings. Fasting glucoses are in the range of 40 to 80 mg per dL, and no insulin replacem ent has b een needed.
Case 2: This 6-week-old w hite male infant was initially evaluated for hard stools and rectal bleeding; the la tter was subsequently found to be due to a rectal fissure. In th e hospital, blood glucoses w ere found to range b etw een 19 and 40 m g per dL. Insulin levels ranged from 13.4 to 18.9 U per ml w ith fasting blood sugars of 25 to 27 m g p e r dL. The hypoglycemia was refractory to m edical therapies, including in travenous glucose and som atostatin analogue (octreotide acetate). T he pa tien t was subsequently taken to surgery for 95 p e rce n t pancreatectom y 35 days after admission.
The patien t has done well postoperatively. W ith th ree m onths o f follow-up, the pa tien t s fasting blood sugars are in th e 200 range with no insulin replacem ent currently required .
T i s s u e S t u d i e s
Pancreatic and extrapancreatic tissues were formalin-fixed and paraffin-embedded for histologic examination in both cases. They w ere totally subm itted for hematoxylin-eosin staining in both cases at initial surgery. In case 1, subsequent resection specimens were also subm itted in their entirety for histologic examination.
Representative paraffin tissue sections w ere processed for im m unoperoxidase staining using the avidin-biotin-peroxi- d a se te c h n iq u e .5 P r im a ry a n tis e ra
included rabbit antihum an neuron-specific eno lase , in su lin , g lucagon and som atostatin.* Results w ere evaluated qualitatively by thé absence or presence and localization of the staining to specific cell types.
Results
Case 1: Subtotal pancreatectom y (90 p e r c e n t to 95 p e r c e n t e s t im a te d ) included a portion of uncinate process (8 mm X 4 mm X 4 mm) and pancreatic body and tail (4 cm X 8 mm X 8 mm). The total weight of subm itted tissues was1.8 gms.
Histologic and immunostaining studies of subm itted tissues revealed segmental adenomatosis of islet cell tissue involving the proximal half of the body of th e p a n c re a s . A d en o m ato s is3,4 was defined as nodular hyperplasia of islet cell tissue occupying g rea ter than 40 percent of the cross-sectional area of the pancreas in any given tissue section and displacing exocrine elem ents. In areas of the body of the pancreas, these islet cell nodules occupied up to 75 percent of the tissue cross-sectional areas. Im m unostaining confirmed the presence of a normal spatial rela tionship4 of endocrine cells w ith periphera l alpha and delta cells and cen tra l b e ta cells. M inim al nuclear hyperchromasia was present.
Subsequen t to tal (com pletion) pan createctom y perform ed th ree m onths later included a rem nant of pancreatic head measuring 3 cm X 2 cm X 1 cm. A separate nodular portion of tissue was identified adjacent to the portal vein and common bile duct m easuring 1.5 cm X 5 mm X 5 mm, and thought to represent fleshy portal lymph nodes (figures 1A and B).
Exam ination of the pancreatic rem nant microscopically revealed residual
* DAKO Corporation, C arpinteria, CA.

ECTOPIC PANCREAS AND ISLET CELL DYSMATURATIONAL SYNDROME 2 1
FIGURE 1A. Ectopic pancreas (EP) with admixed portal lymph nodes (LN) in Case 1. (H&E stain, 15 X magnification). B. The ectopic pancreas seen above is composed prim arily of islet tissue w ith a few associated ducts. (H& E stain, 350 x magnification).
adenom atosis (at least four separate foci), again occupying up to 75 p ercen t of the cross-sectional area of the pancreatic sections.
T he portal vein nodule was com posed of 50 p ercen t benign lym ph nodes and
50 p ercen t ectopic pancreatic tissue (figu re 1A). T he la tter tissue was com posed of 80 p ercen t islet tissue (figure IB) w ith exocrine tissue seen only focally.
Im m unostain ing of the portal nodular islet lesion revealed the norm al spatial

22 QUALMAN, CANIANO, KING, A ND ZIPF
relationship of central beta cell mass and peripheral alpha and delta cells.
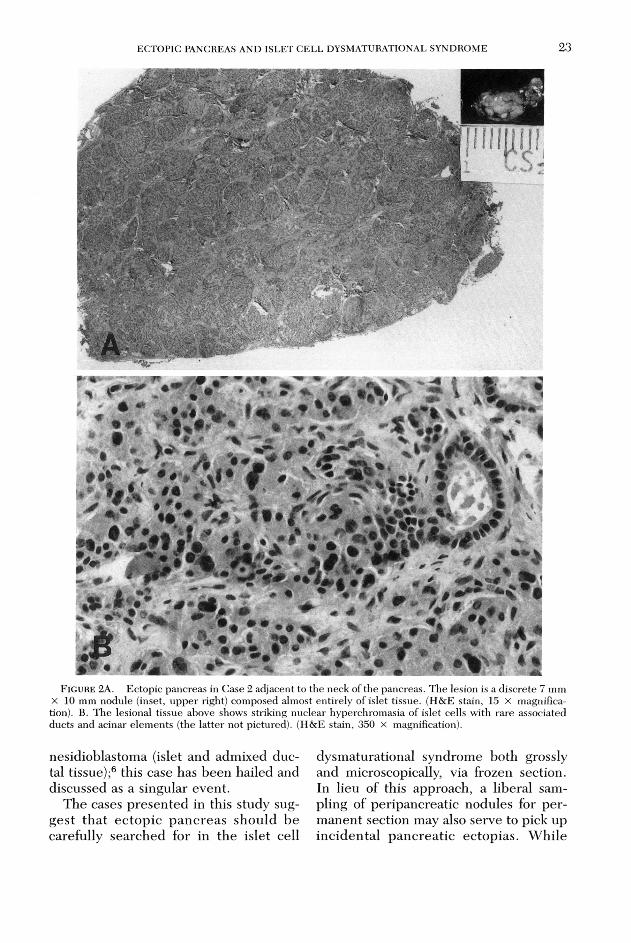
Case 2: Given the experiences with Case 1, the surgeon in this case made a thorough search for ectopic pancreatic tissue during a 95 percent pancreatectom y. A fo u r m m n o d u le re m o v e d around the gallbladder and common bile duct was identified microscopically as a group of benign lymph nodes on frozen section. Another 7 mm X 10 mm nodule (figure 2A) was identified adjacent and superior to the neck of the pancreas with a separate blood supply from the superio r m esen teric a rte ry and vein , and lying anterior to the portal vein. This lesion was thought to be distinctly differen t in appearance from lymph nodes or pancreas, and frozen section was again obtained.
Frozen section and subsequent p e rm anent section of the 7 mm X 10 mm nodule revealed prim arily (90 percent) is le t t is su e w ith e x te n s iv e n u c le a r hyperchrom asia (figure 2B) and a few associated ductal/acinar e lem ents (10 percent).
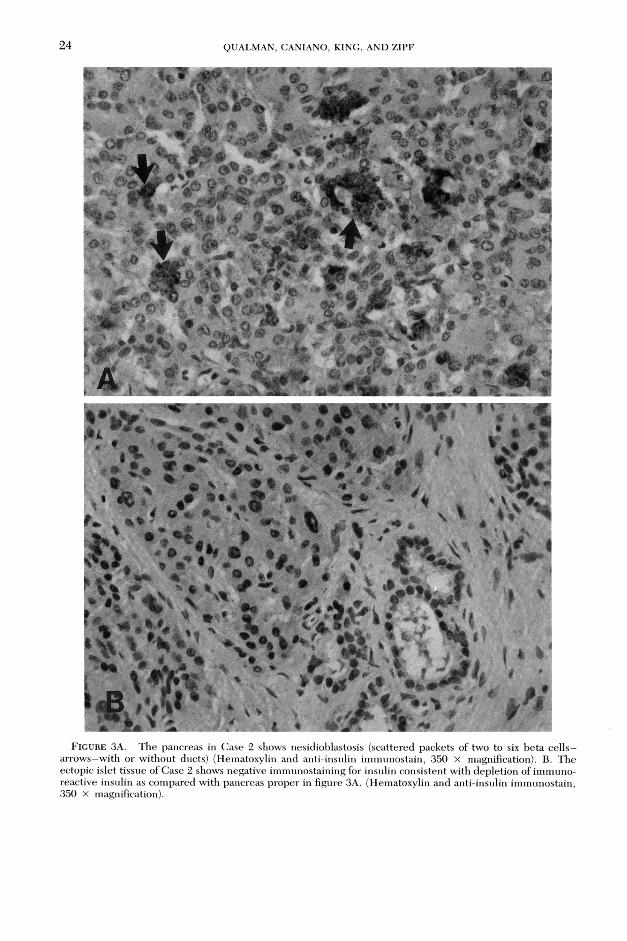
The 95 percent pancreatectomy itself (9.5 cm X 9 mm X 7 mm) showed only so-called nesidioblastosis1 with scattered small packets of two to six b e ta cells (insulin positive) scattered around small ducts or acini w ithout m ore confluent lesions identified (figure 3A). No nuclear hyperchromasia was identified.
Immunostaining did confirm the normal spatial relationship of central beta cell mass and peripheral alpha and delta cells in islets of the pancreas proper. However, the extrinsic pancreatic nodu le fo u n d at th e neck o f th e g land show ed dep letion of im m unoreactive insulin (figure 3B) with intact staining of alpha and delta cells.
Discussion
Islet cell dysmaturational syndrome2 is a term designated to include the spec
trum of histopathologic lesions seen with life-threatening hyperinsulinemic hypoglycemia in infancy. The sine qua non of diagnosis in this idiopathic syndrome is not the underlying pathologic substrate, b u t ra th e r in a p p ro p ria te ly e lev a ted plasma insulins (usually > 10 U per ml) in the presence of sim ultaneously low b lo o d g lu co se le v e ls (=£50 m g p e r dL )2,10,11 refractory to medical therapies. The diagnostic a lgorithm follow ed to exclude o th er causes of hypoglycem ia in arriving at this diagnosis is well-estab- lished .11 Both of the cases presented in this study m eet the criteria for the islet cell dysmaturational syndrome.
The recom m ended th erap y for the islet cell dysmaturational syndrome is a near total (90 to 95 percent) pancreatectomy in most case series2,6,8,9,10 unless a discrete adenoma can be identified and resected. The pancreas may show a variety of other pathologic lesions in this setting which are not grossly discernible including nesidioblastosis or isle t cell adenomatosis as seen in our two cases. A plethora of o ther synonyms7 for intra- pancreatic islet cell proliferations in this setting is confusing and does not offer further insight into the m anagement of the lesions. W hatever the term inology used, the irregular distribution of the islet lesions in the pancreas microscopically obviates the use of frozen section2,11 as a guide to resection.
Unfortunately, even w ith 95 percent pancreatectomy, a few patients continue to have life-threatening hypoglycemia.6 In some cases this may be ascribed to residual adenomatous tissue left in the head of the pancreatic rem nant.11 However, at least one case has b een d iscussed anecdotally in the literature of ectopic pancreatic tissue grossly thought to be lymph node from the aortic side of the pancreas, which was associated with erratic blood glucoses on m anipulation .6 Frozen section revealed ectopic pancreas with the microscopic appearance of
ECTOPIC PANCREAS A ND ISLET CELL DYSMATURATIONAL SYNDROME 23
F ig u r e 2A . Ectopic pancreas in Case 2 adjacent to the neck of the pancreas. The lesion is a d iscrete 7 mm X 10 mm nodule (inset, up p er right) com posed almost entirely of islet tissue. (H&E stain, 15 X magnification). B. The lesional tissue above shows striking nuclear hyperchrom asia o f islet cells with ra re associated ducts and acinar e lem ents (the la tter no t pictured). (H&E stain, 350 x magnification).
nesidioblastom a (islet and adm ixed ductal tissue);6 this case has been hailed and discussed as a singular event.
T he cases p resen ted in this study sugg es t th a t e c to p ic p an c re a s sh o u ld b e carefully searched for in th e islet cell
dysm aturational syndrom e both grossly and microscopically, via frozen section. In lieu of this approach, a liberal sam pling of peripancreatic nodules for p e rm anen t section may also serve to pick up in c id en ta l p an c rea tic ec top ias. W hile
24 QUALMAN, CANIANO, KING, AND ZIPF
4 0* ' r h * w c-; ' ®m. ■ • . ̂ ■WL
*<*► % *■ % 1fe A fefc-' . M-' Q «
*'•*•• • % s L ä t’*F ■*<» :
__
" Of
■
* 4 ^ - 0m f * ' £ ’ J“ ¿ { * * * » » w *•• i ?
© 0'f_________ _ ä % V» - — <w~_ y n **, . ' a __ A ^ R ik a L » . » < a K '* g V
• . f fr t ìKW - •
' - I ; . ' - • ' • * $ ?jn ^ r t f« W *• s .s:.1®' i■M ÌH ÌBÌIH mI
#
O c. # ^ 1 ,«, ■
•CiSfcfc
. « " “J r *0 '
(Q o F J C» > 1
%$*• 5# ̂ *
Ä ' ' f i ' * '» >*' ' • A-
: ?» at
*V*vC
i | ’ g f ' i M N*** * i g i r » . «
! " W
Q .
‘^ X •& * j w t*
I
f * v « -« % • v ■
r * * % 4* ® *• ^ '
' W . . >
-A .f t ' * V ry 'X '& *' B i ‘# * t ' i • * • : 'Ì T k ' i ’ / I . * ' ; / ’ ' ' l
F ig u r e 3A. The pancreas in Case 2 shows nesidioblastosis (scattered packets of two to six be ta c e lls - a rrow s-w ith or w ithout ducts) (Hematoxylin and anti-insulin im m unostain, 350 X magnification). B. The ectopic islet tissue of Case 2 shows negative im m unostaining for insulin consistent with depletion of imrnuno- reactive insulin as com pared with pancreas proper in figure 3A. (Hematoxylin and anti-insulin im m unostain, 350 X magnification).

ECTOPIC PANCREAS A N D ISLET CELL DYSMATURATIONAL SYNDROM E 25thorough gross evaluation for pancreatic ectopias is advocated9 prior to subtotal pancreatectom y, large review s10 of the literature (71 total cases) have shown no identification of ectopic pancreas using this approach. How ever, ectopic pan creas is the most common form of pancreatic maldevelopment (2); it affects one percent to two percent of the population with over 50 percent of cases identified in the region of the stomach or duodenum (often the second part), and 60 to 70 percent of cases containing islet tissue. In our cases, knowledge of this phenom enon discerned from the second laparotom y in the first p a tie n t, allow ed for effective frozen section identification of ectopic pancreas on first surgery in the subsequent case.
The functional significance of these pancreatic ectopias found with the islet cell dysmaturational syndrome could be questioned; however, the high percentage of islet tissue in our cases (80 to 90 percent), the presence of nuclear pleo- morphism, and the depletion of immu- noreactive insulin are all supportive correlates with hypoglycemia.3,5
The present study does not offer new insights into the relationship of intrinsic pancreatic pathology to the islet cell dysm aturational syndrom e. It does, however, emphasize the need for a careful search for ectopic pancreas by intraoperative gross and subsequent microscopic inspection of tissues to help obviate the need for recurrent surgery. By this prosp e c tiv e a p p ro a c h , one m ay b e t te r define the contribution of ectopic pancreas to the islet cell dysm aturational syndrome.
Acknow ledgm ents
Thanks are ex tended to Karen Jones for th e typing of th e m anuscript.
References
1. D a h m s , B. B ., L a n d i n g , B . H ., B l a s k o v ic s , M ., and R oe, T. F. : Nesidioblastosis and o ther is le t cell a b n o rm a litie s in h y p e rin su lin e m ic hypoglycem ia o f childhood. H um . Pathol. 11: 641-649 , 1980.
2. D e h n e r , L. P. : Pancreas, congenital and develop m en ta l anom alies. In : P ediatric Surg ica l Pathology , 2nd ed. B altim ore, W illiam s and W ilkins, 1987, pp. 543—550.
3. Ja f f e , R., H a s h id a , Y., and Yu n i s , E. J.: Pancreatic pathology in hyperinsulinem ic hypoglycem ia of infancy. Lab. Invest. 42:356-365, 1980.
4 . Ja f f e , R ., H a s h id a , Y , and Yu n is , E . J.: The endocrine pancreas o f the neonate and infant. Perspect. Pediatr. Pathol. 7:137-165, 1983.
5. H ò f l e r , H . , D e L e l l i s , R. A ., an d W o l f e ,H . J.: In situ hybridization and im m unohisto- chemistry. In: D eLellis, R. A., ed. A dvances in Im m unohistochem istry. New York, Raven Press,1988, pp. 4 7 -6 6 .
6. L a n c e r , J. C ., F il l e r , R. M ., W e s s o n , D . E ., S h e r w o o d , G., and C u t z , E.: Surgical m anagem ent of p e rsisten t neonatal hypoglycem ia d ue to islet cell dysplasia. J. Pediatr. Surg. 19:786— 792, 1984.
7. L l o y d , R. V., C a c e r e s , V ., W a r n e r , T., and G il b e r t , E. F. : Isle t cell adenom atosis. Arch. Pathol. Lab. M ed. 105:198-202, 1981.
8. S h e r m e t a , D . W. a n d M e n d e l s o h n , G..- H y p e rin su lin hyp o g ly cem ia in th e n eo n a te : therapeu tic choices. J. Pediatr. Surg. 15:3 9 8 - 399, 1980.
9. S pitz , L ., B u ic k , R. G ., G r a n t , D. B ., L e o n a r d , J. V., a n d P in c o t t , J. R.: S u rg ica l tr e a tm e n t o f n e s id io b la s t o s is . P e d ia tr . S u rg . In t . 1:26—29, 1986.
10. T e l a n d e r , R. L ., W o l f , S . A., S im m o n s , P. S ., Z im m e r m a n , D . , and H a y m o n d , M. W .: E ndocrine disorders o f the pancreas and adrenal cortex in p e d ia tr ic p a tie n ts . M ayo C lin . Proc. 61:459-466 , 1986.
11. T h o m a s , C . G ., Jr. , U n d e r w o o d , L . E ., C a r ney , C . N., D o l c o u r t , J. L ., and W h it t , J. J.: N eo n ata l an d in fan tile hypog lycem ia d u e to insulin excess. Ann. Surg. 185:505—516, 1977.