edward sloan, md, mph traumatic brain injury: specific management items of note for the emergency...
TRANSCRIPT
Edward Sloan, MD, MPH
Traumatic Brain Injury:Specific Management Items
of Note for theEmergency Physician
Edward Sloan, MD, MPH
Edward P. Sloan, MD, MPH
Associate ProfessorDept of Emergency Medicine
University of Illinois College of Medicine
Chicago, IL
Edward Sloan, MD, MPH
Attending Physician Emergency Medicine
University of Illinois Hospital
Our Lady of the Resurrection
Medical Center
Chicago, IL
Edward Sloan, MD, MPH
OverviewGlobal Objectives
• Understand disease state (TBI)
• Utilize best management strategies
• Have many options available
• Optimize patient outcome
• Maximize resource use
• Make our practice enjoyable
Edward Sloan, MD, MPH
OverviewSession Specifics
• Review Italian guidelines• Discuss the EM Reports• Examine the ACR head trauma criteria • Summarize minor TBI practice parameters• Detail trephination and antibiotic use• Look at some head CTs• Journal club articles
Edward Sloan, MD, MPH
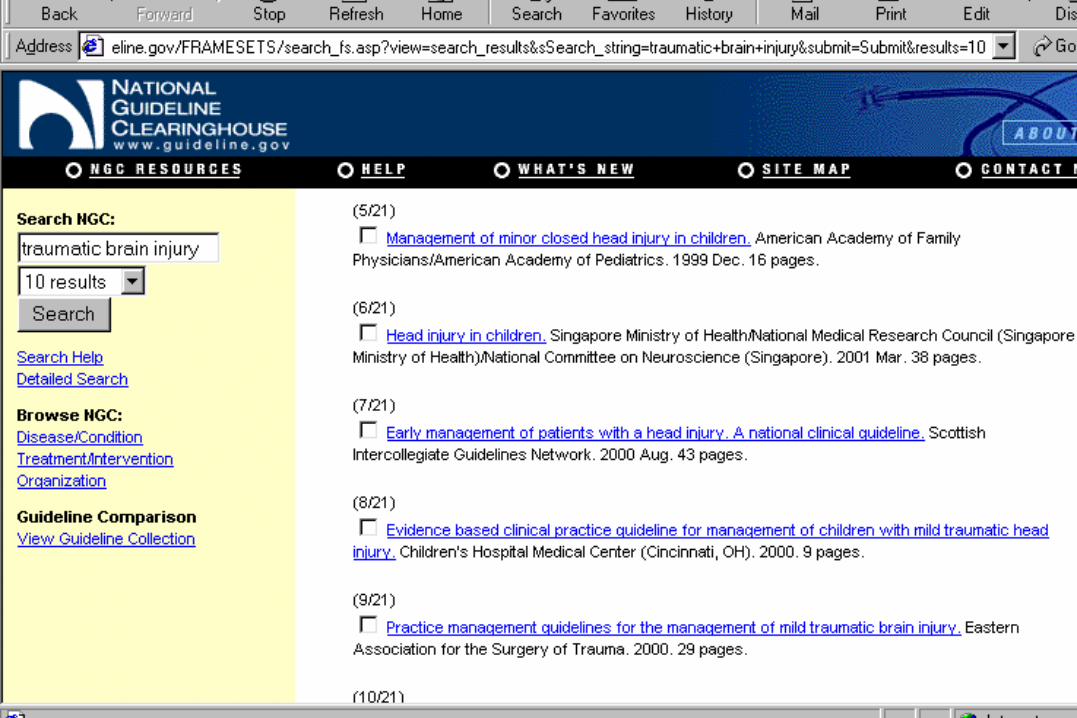
Methodology Literature Search
• www.guidelines.gov
• Traumatic Brain Injury
• 21 guidelines provided
• Relevant US guides used
Edward Sloan, MD, MPH
Methodology Internet Sources• www.guideline.gov/
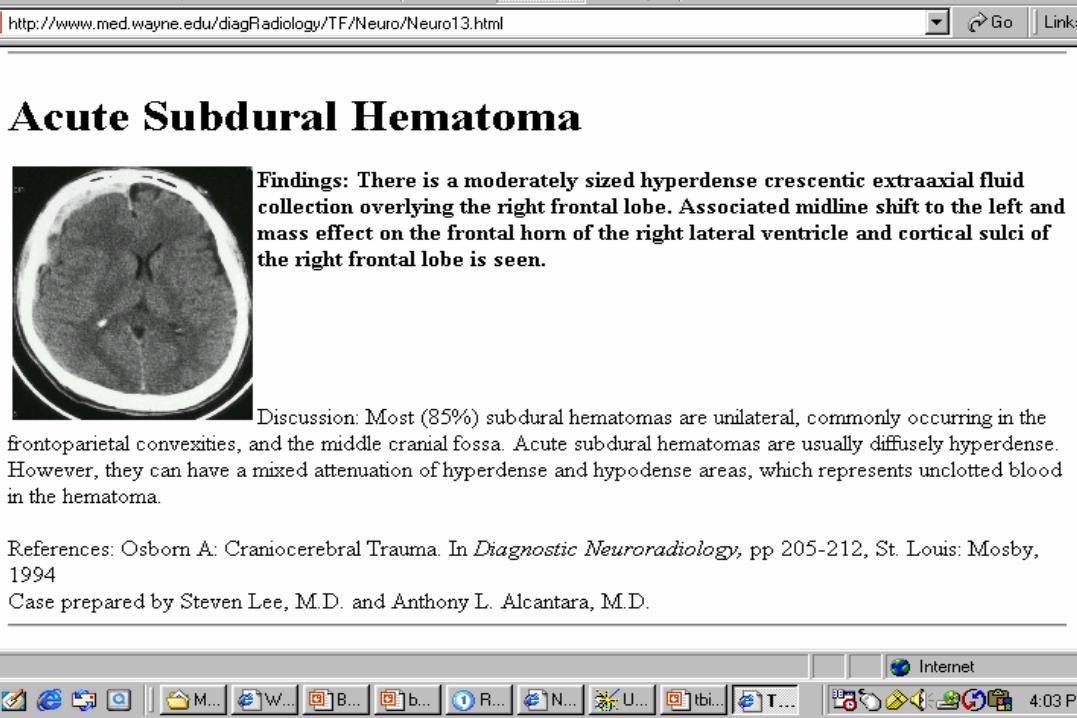
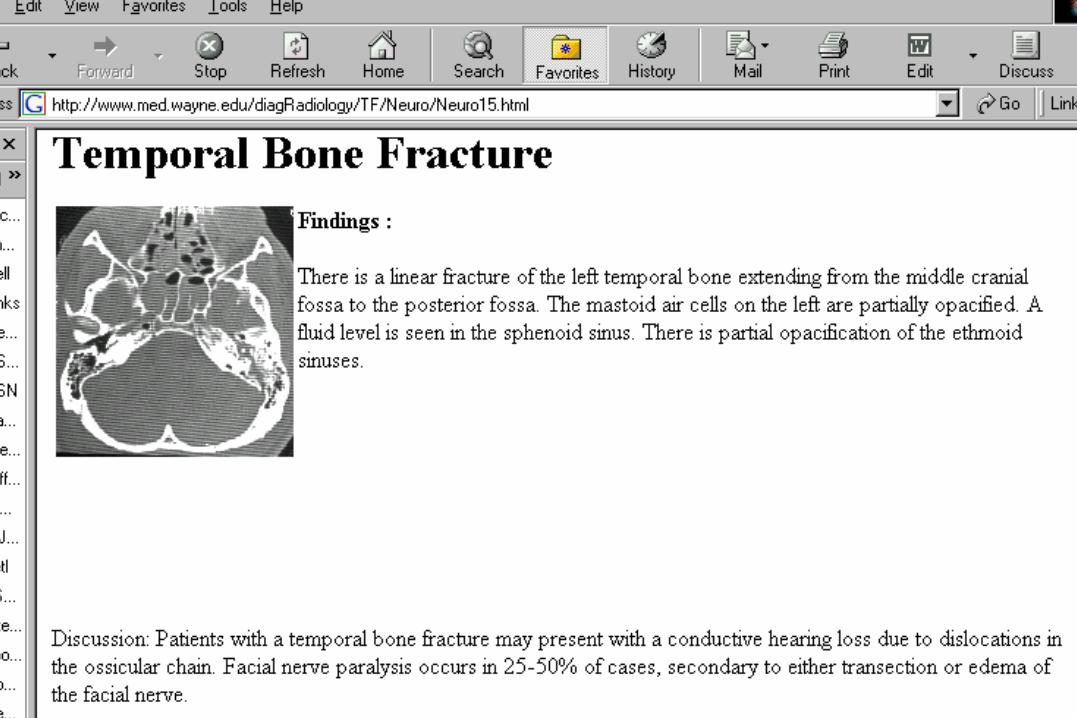
• www.med.wayne.edu/diagRadiology/TF/
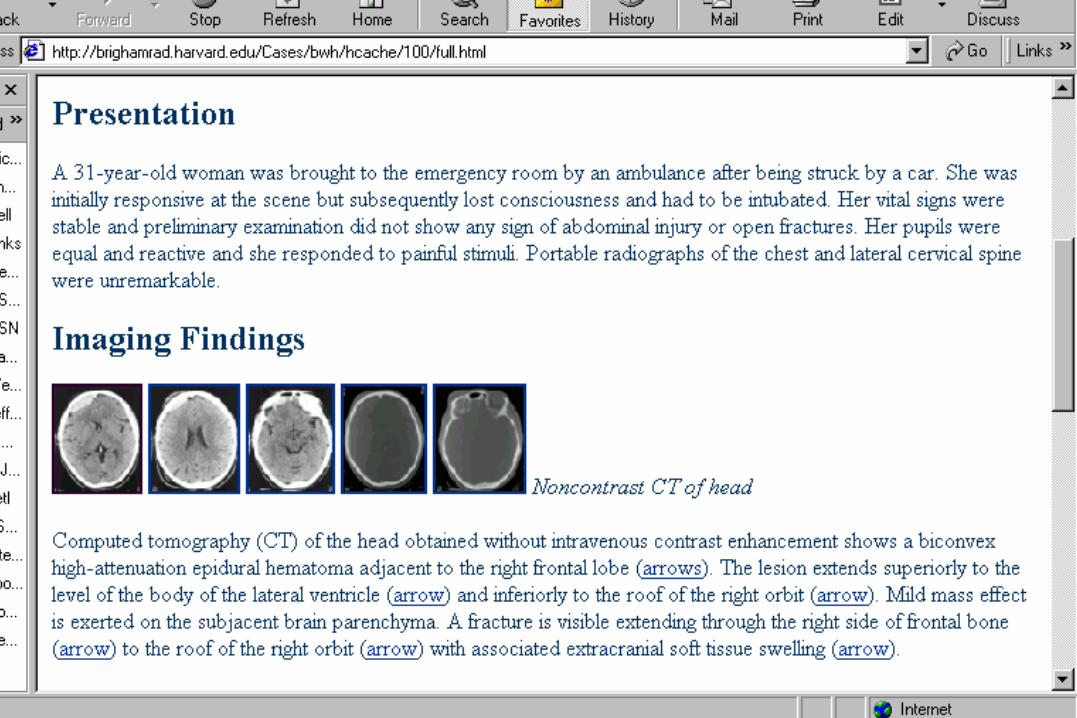
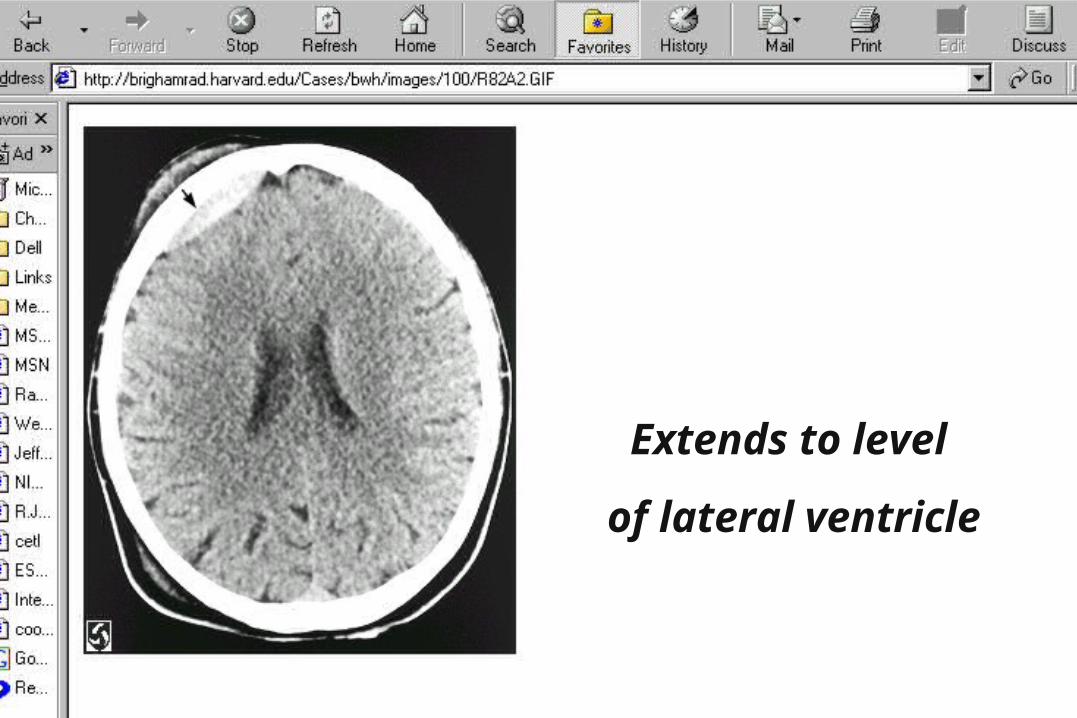
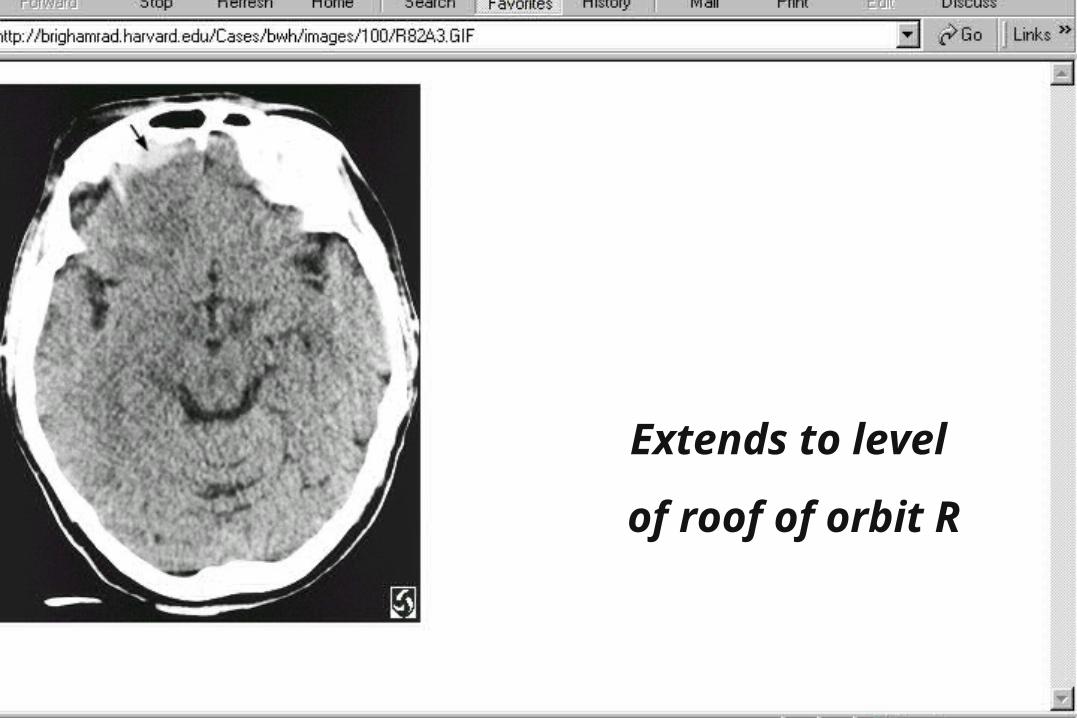
• www.brighamrad.harvard.edu/cases/
• www.ferne.org/
• www.google.com/
Edward Sloan, MD, MPH
Methodology Source Documents• Guidelines for Rx of Adults with TBI–J of Neurosurgical Sciences
–Vol 44:1 March 2000
–Three articles
– Initial assessment, medical, surgical Rx
• Emergency Medicine Reports–December 3, and December 17, 2001
Edward Sloan, MD, MPH
Methodology Source Documents• Roberts, Hedges: Clinical Procedures
in Emergency Medicine, 2nd Edition
• EM journal club articles–make a point–describe a clinical entity–have medicolegal import
Edward Sloan, MD, MPH
GuidelinesItalian Recommendations
• I: Initial Assessment
• RSI: Thiopental (ketamine or midazolam) Sux or vecuronium
• GCS: In comatose pts (eye=1, verbal=1,2)Motor component very important.Use best response from either
side.
Edward Sloan, MD, MPH
GuidelinesItalian Recommendations
• I: CT Indications
• Loss of two points on GCS
• Rise in ICP above 25 mm Hg
• Decrease in CPP below 70 mm Hg > 15 min
• Decrease in O2 sat below 50% > 15 min
Edward Sloan, MD, MPH
GuidelinesItalian Recommendations
• II: Medical Therapy
• Inotropes once blood volume restored
• To maintain MAP above 90 mm Hg
• To achieve CPP > 70 mm Hg if ICP high
• Not in lieu of ICP management
Edward Sloan, MD, MPH
GuidelinesItalian Recommendations
• III: Surgical Therapy • Absolute: –Focal lesion, midline shift > 5 mm–Space occupying lesion > 25 cc
• Relative:– ICP > 20 mm Hg or CPP < 70 mm Hg–Optimal medical ICP management
• Case-specific criteria also
Edward Sloan, MD, MPH
LiteratureEM Reports: TBI, Subdural
• I: Emergency Rx, Imaging • Pathophysiology• Neurologic exam • CT indications• MRI: DAI, subcortical injury, brainstem• Angiography: Penetrating TBI, vascular
occlusion, dissection, aneurysm

Edward Sloan, MD, MPH
LiteratureEM Reports: TBI, Subdural
• II: Emergency Rx of Severe TBI • Severe TBI Rx, including ICP Rx• Cranial decompression indications • Monitoring indications
• Moderate TBI Rx, outcome• Minor TBI, and post-concussion syndrome
Edward Sloan, MD, MPH
ACR GuidelinesAppropriateness Criteria
• Imaging in head trauma• Classified by clinical condition• Provides summary by imaging modality• CT: screening tool in mild TBI to determine
who may benefit from observation• Skull xrays: calvarial fractures, penetrating
injuries, and foreign bodies
Edward Sloan, MD, MPH
EAST GuidelinesMild TBI Management
• Transient neuro deficit, no acute pathology
• CT is gold standard
• Normal CT: 0-3% deterioration (GCS 13-14)
• Neuropsychological testing at 1-2 months
• Most pts recover within one month
• Limited data on those who do not recover
Edward Sloan, MD, MPH
Neurology GuidelinesConcussion in Sports
• Grade 1: Transient sx for < 15 minutes–May return if sx resolve within 15 minutes
• Grade 2: Transient sx for > 15 minutes–No return to contest–CT if sx persist
• Grade 3: Any LOC noted–ED eval if sx persist or more than brief LOC
Edward Sloan, MD, MPH
Emergent Cranial DecompressionIndications• Hippocrates utilized trephination• To evacuate extradural hematomas• To reverse signs of tentorial herniation• Rapid, progressive neurologic deterioration• Coma, fixed, dilated pupil, hemiplegia and
presumed skull fx on side of pupil• Likely intracranial hematoma on same side
Edward Sloan, MD, MPH
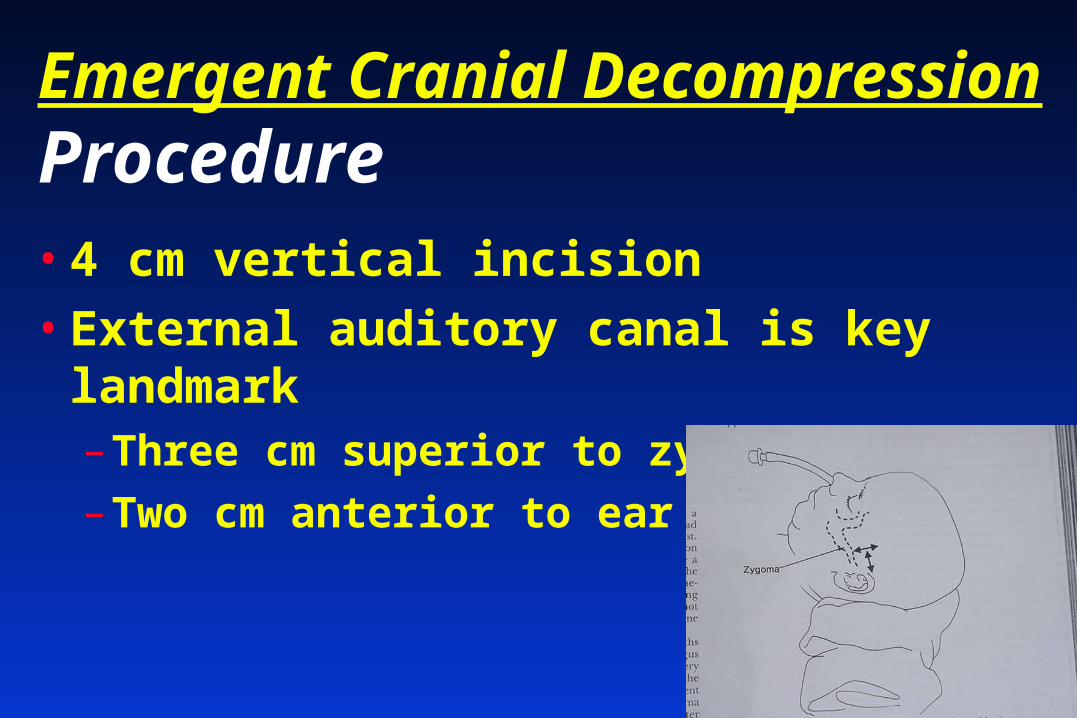
Emergent Cranial DecompressionProcedure• 4 cm vertical incision
• External auditory canal is key landmark–Three cm superior to zygoma
–Two cm anterior to ear
Edward Sloan, MD, MPH
Emergent Cranial DecompressionProcedure• Drill a hole, enlarge with a Burr
• Careful as the inner table is perforated
• Epidural: clotted, unless bleeding persists
• Middle meningeal artery is deep to clot
• Be prepared to replace blood loss
• Bilateral fixed pupils, or no clot, repeat on contra-lateral side
Edward Sloan, MD, MPH
Prophylactic AntibioticsSkull Fx, Penetrating TBI
• Sanford, ePocrates: no recommendations• EM study guide: ask neurosurgeon• Prophylaxis controversial• Skull fracture and fever:–Pneumococcus within 72 hours–Staph aureus and gram negs after 72 hours–Vancomycin, 3rd gen ceph (ceftazadime)
Edward Sloan, MD, MPH
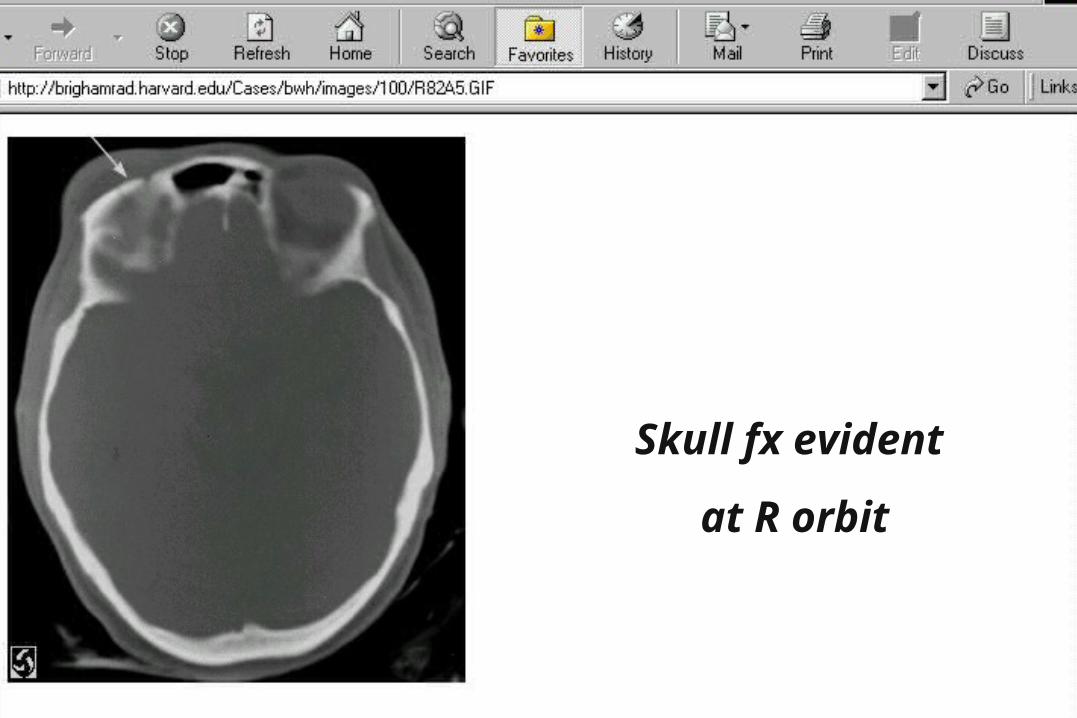
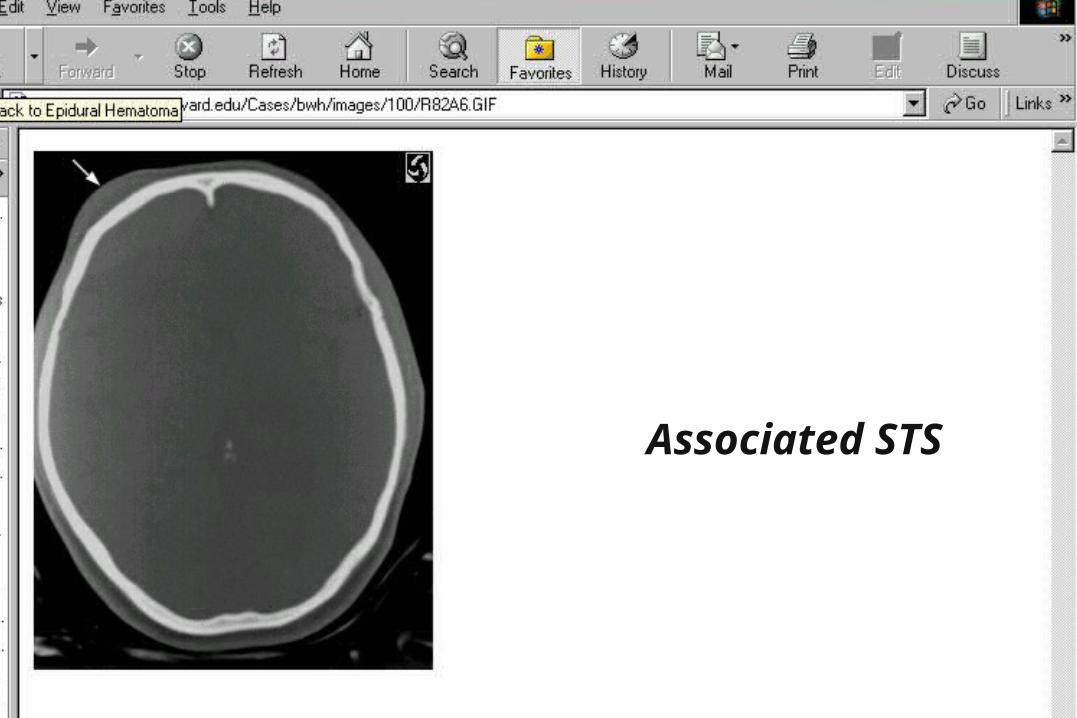
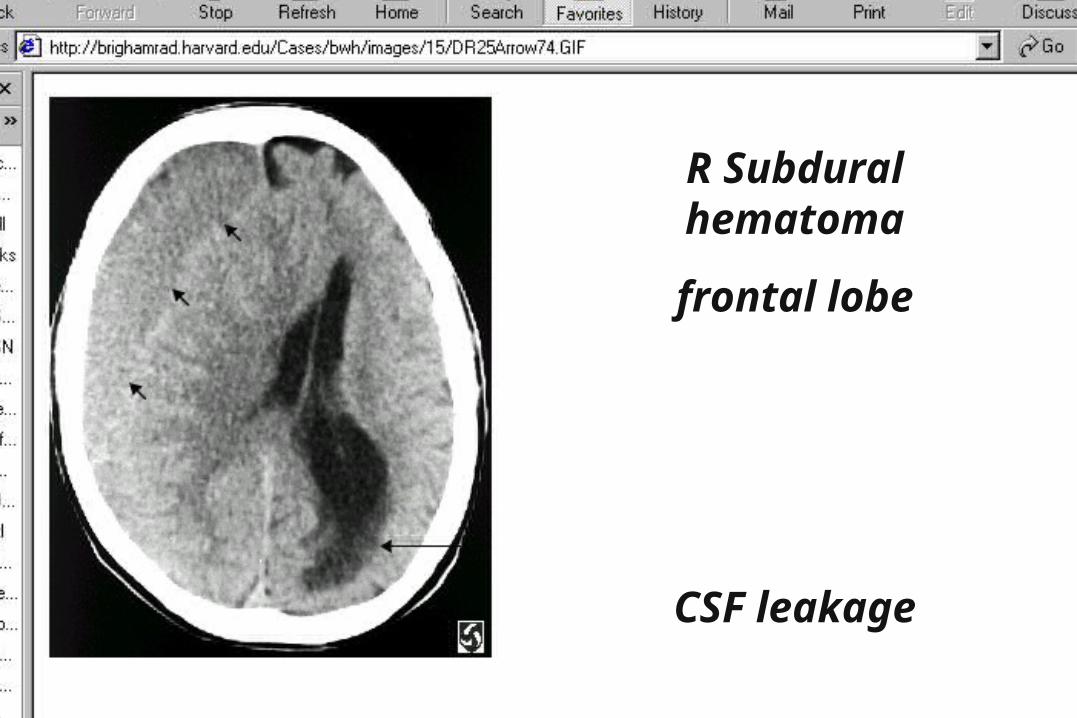
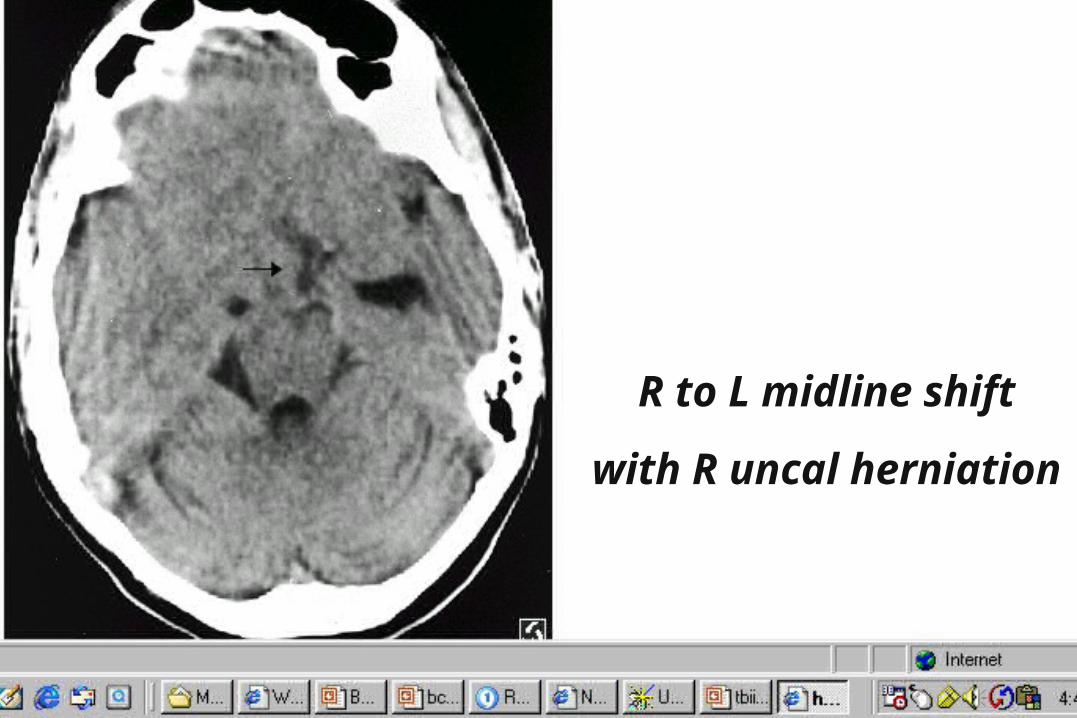
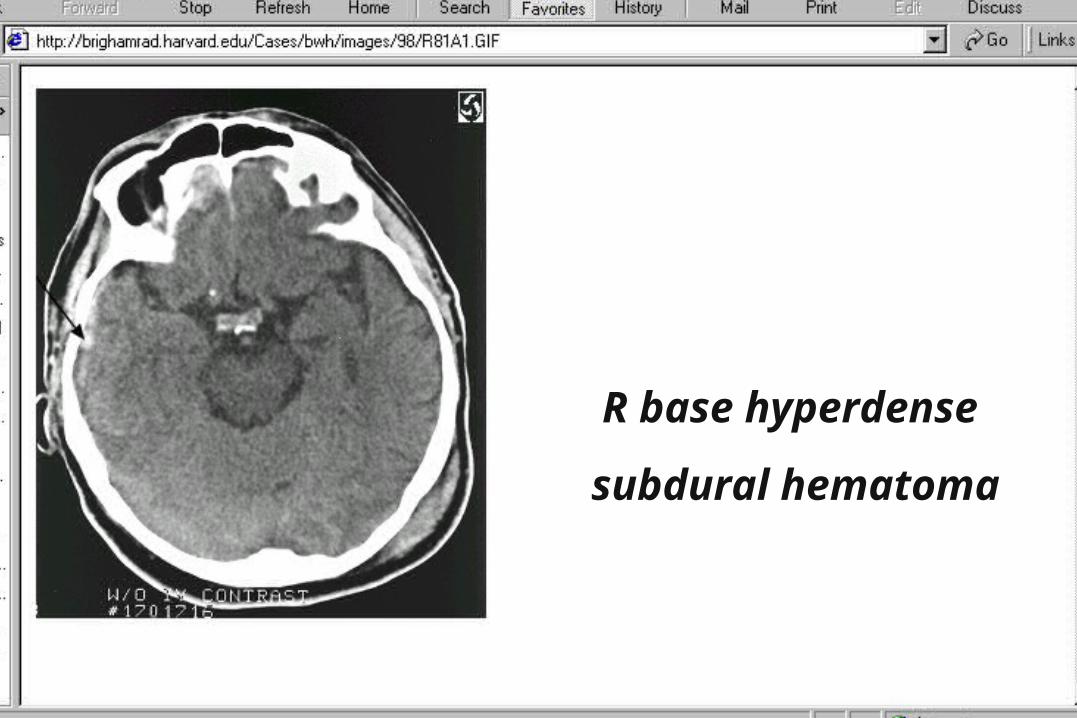
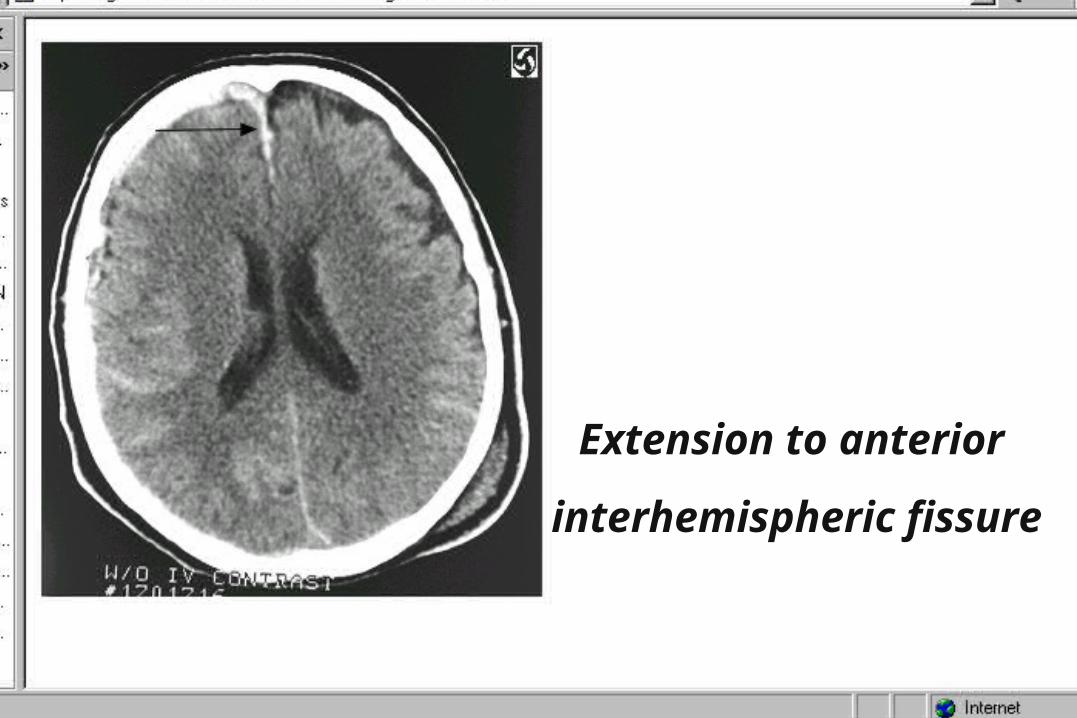
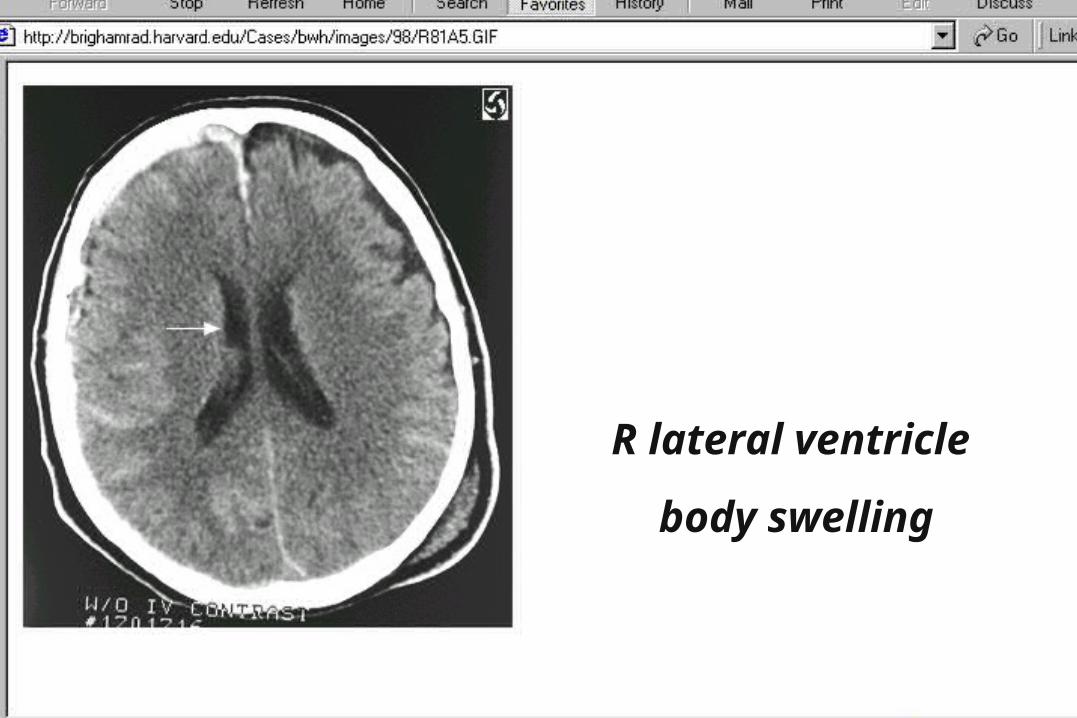
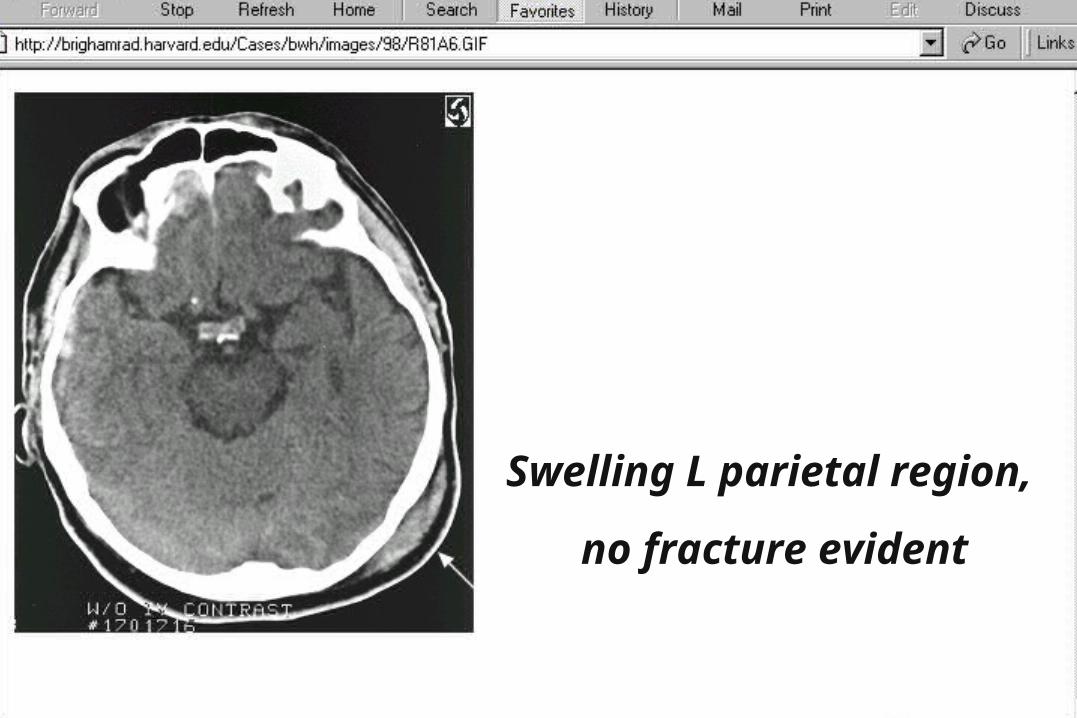
Radiology CasesSearching for Teaching Files
• Google: Radiology Teaching Files
• Many universities post files
• Two examples of content
• Easy to use in the E.D.
• Radiology of Emergency Medicine




Edward Sloan, MD, MPH
Radiology CasesHow to Obtain Images
• Get the image on the screen
• Hit the print screen button
• Go to PowerPoint
• Edit: Office Clipboard
• Double click on R to paste
• Resize to fit, add text box as needed
Edward Sloan, MD, MPH
Journal Club ArticlesBTF Guidelines • Basis for lecture on TBI Rx• Explains guideline development• Guides acute ED therapies
• Brain Trauma Foundation: J Neurotrauma, 1996; 13: 643-645• Brain Trauma Foundation : J Neurotrauma, 1996; 13: 653-659
Edward Sloan, MD, MPH
Journal Club ArticlesSkull X-ray Indications • Multi-disciplinary study• Provided key recommendations• Changed clinical practice• Skull xrays: occult penetrating trauma
• Masters SJ: N Engl J Med, 1987; 316: 84-91 • The Selection of Patients for X-Ray Examinations: Skull
X-Ray Examination for Trauma
Edward Sloan, MD, MPH
Journal Club ArticlesHypertonic Saline in TBI
• J Trauma literature review
• Proven mechanism for benefit
• Conflicting clinical data
• Restores MAP without edema, inc ICP
• Doyle JA: J Trauma, 2001; 50: 367-383
Edward Sloan, MD, MPH
Journal Club ArticlesPEG-SOD in TBI
• JAMA article
• SOD: oxygen radical scavenger
• EM physicians involved
• No benefit, control group did well
• Young B: JAMA, 1996; 276(7): 538-543

Edward Sloan, MD, MPH
Journal Club ArticlesCT in Mild TBI
• J Trauma article
• Is CT of all mild TBI pts cost-effective?
• CT is cost effective, no need to admit
• Normal CT and neuro exam: home
• Shackford SR: J Trauma, 1992; 33(3): 385-394
Edward Sloan, MD, MPH
Journal Club ArticlesCT in TBI & Hypotension
• Annals EM article
• CT prior to laparotomy?
• If stable after initial resus, OK to CT
• Average delay of 68 minutes
• Winchell RJ: Ann Emerg Med, 1995; 25(6): 737-742
Edward Sloan, MD, MPH
Journal Club ArticlesEtOH and Minor TBI
• Acad EM article
• CT in intoxicated minor TBI pts?
• 8% Positive CT, 2% craniotomy rate
• May need to CT with mild TBI and EtOH
• Cook LS: Acad Emerg Med, 1994; 1(3): 227-234
Edward Sloan, MD, MPH
Journal Club ArticlesPts Who Talk & Deteriorate • Annals EM article• Can speak and then coma within 48 hrs• 75% intracranial hematoma rate• Deterioration: bad prognosis• Need to achieve early decompression
• Rockswold GL: Ann Emerg Med, 1993; 22(6):1004-100
Edward Sloan, MD, MPH
ConclusionsTBI Rx in the ED• GCS motor key in coma
• RSI with Thiopental/sux
• Clear CT, surgery indications
• Inotrope, PRN if volume OK
• MRI, angio less needed
Edward Sloan, MD, MPH
ConclusionsTBI Rx in the ED• CT is best screening tool
• Mild TBI: 1 month recovery
• Concussion: LOC is key
• Trephination: epidural Rx
• Drill on side of blown pupil
• Anbx: prophylaxis unclear
Edward Sloan, MD, MPH
ConclusionsTBI Journal Club• BTF guidelines key
• Skull xray: penetrating trauma
• HTN saline unclear
• CT even if hypotension prior
• EtOH: CT liberally
• Talk & deteriorate: evacuate
Edward Sloan, MD, MPH
ConclusionsInternet Medical Information• Guidelines.gov
• Google: radiology teaching file
• PrintScreen, paste to PowerPoint
• FERNE.org

Edward Sloan, MD, MPH
RecommendationsTBI Rx in the ED• Liberal CT use• Follow guidelines• Surf the web• Maximize patient outcome
[email protected](312) 413-7490