edwin cox, m.d. olli fall 2017
TRANSCRIPT

What to Eat – and Why ?
Edwin Cox, M.D.
OLLI Fall 2017

The goal: a long and healthy life
What can we can do in our daily life and behavior (diet, exercise)...• to live as long as possible, and• to stay as well as possible?
I wanted to know for myself what I should be eating!

Why ask Why?Know the rationale for eating specific foods and avoiding others, empowering you to...• Think for yourself• Make informed choices• Develop willingness to try new foods that are good for you• Resist being swept along with each new fad• Gain skills to critically evaluate new recommendations• Reduce enticing foods that are detrimental• Satisfy curiosity

The Diet Gurus don’t agreeNutrition advisors say...• Atkins Diet: Carbohydrate is the culprit; restrict carbohydrates,
consume mainly protein and fat; animal sourced foods are fine• Campbell Diet: Animal proteins are toxic; plant-based, whole-food
diet avoids harm• USDA: Fats, especially saturated fat, cause heart attacks and
strokes; eat low-fat diet with as much carbohydrate as you want
They reach opposite conclusions - they can't all be right!
All have an element of truth, but all miss the mark, due to “cherry-picking” data!

Que sera, sera?We’ve been conditioned to think, “what will be, will be”
Just accept that nobody really knows what to do to stay alive and well
We might as well eat, drink and be merry
When disease strikes, look to doctors to push back, i.e., pills, surgery, chemotherapy
But, doing that just makes us a pawn of powerful commercial forces – the “manufactured food” industry• They wants us to buy prepared foods that yield them big profits but
expose us to disease and premature death

My approach:Let the evidence speak!
Do what I did as a physician when faced with patients
Consult original sources in the medical literature for the best current treatment results
Accept nothing pre-processed through someone else’s filter
Use my background in statistics and epidemiology to rigorously evaluate data
Over 500 publications reviewed

Timing... is everything!
My research started in 2013• Numerous large, high-quality studies were just bearing fruit
Published results dealt with individual questions• How does total mortality relate to dairy consumption?• What is the incidence of diabetes relative to nut consumption?• Does eating more fiber prevent colon cancer?
No single researcher had compiled an complete overview that synthesized the results into a comprehensive plan• My goal was a holistic approach to lifestyle, weighing the pros and cons of
all elements to arrive at a balanced approach

Mission Accomplished!
A wide array of conclusions and recommendations were gleaned
I compiled my findings into this course
I’ve continued to research and update knowledge base
The course is now in its seventh iteration, with several useful new findings from 2017 research reports

Where danger lurks...
We freak out over the pesticides on our fruits and veggies, antibiotics and hormones in our meat, mercury in our light bulbs
We’re oblivious to the fact that the greatest threats to our well-being are when we sit down to the dinner table – what we eat – and sit in front of the TV – instead of exercising

An Ounce of Prevention...
We can prevent disease
It’s in our power, and it’s not that hard
It’s never too late to make a difference
More can be done to prevent and delay illness and death by good eating habits and exercising than by any doctor’s prescription
“The fork is mightier than the pen”

The 80/20 Rule
We don’t have to change everything we eat
80% of the effects come from 20% of the causes• 80% of a company’s sales come from 20% of the
customers• 80% of the profit comes from 20% of the sales
Be strategic and change the things that will produce the greatest results
Is Longevity a Matter of Choice?Dr. Fraser is professor of medicine and public health at Loma Linda U. in California, where he directs the famous Adventist Health Study focusing on vegetarian eating patterns
Article is from Archives of Internal Medicine, 2001

Seventh-day AdventistsProtestant Christian denomination
Adventists emphasize diet and healthy habits• Avoidance of meat• Vegetarian diet common• Abstinence from alcohol and tobacco
Notable members included John Harvey Kellogg• Development of breakfast cereals as a health food • Brother William founded Kellogg’s
Enclave of Adventists in California (Loma Linda)

Adventists live longer!
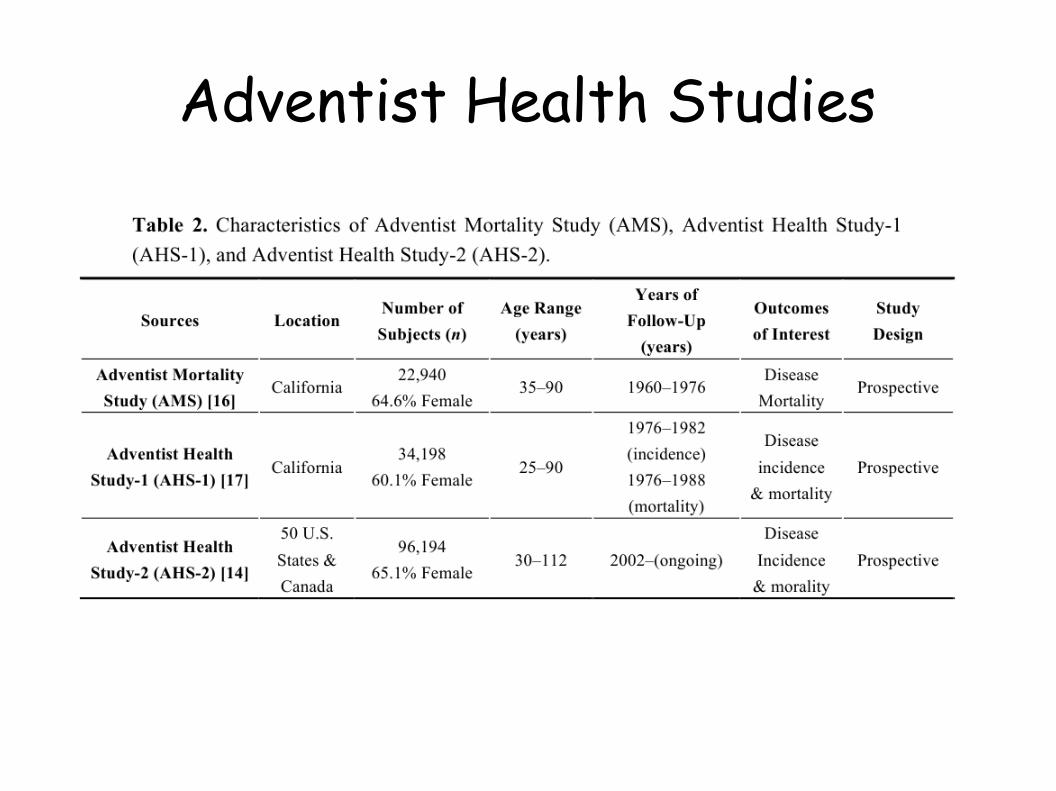
Adventist Health Studies

Additional Life Expectancy (Adventist Men)
Higher nut consumption +2.7 yrs
Higher physical activity +2.7 yrs
Vegetarian +1.5 yrs
Lower body mass index +1.4 yrs
Never smoker +1.3 yrs
All factors favorable +9.7 yrs

The Evidence: Types of studies
The purpose of studies is to infer causes• For example, meat causes disease coronary
heart disease or sugar shortens life span
Basic research
Randomized controlled trials
Cohort (observational) studies
Basic research
Genomics• Look for genes that are associated with diseases and
susceptibility to exposures
Environmental factors• Exposures correlated with disease causation and
progression
Mechanisms of benefit or harm• How do walnuts lower LDL-cholesterol?
Randomized controlled trialsSubjects allocated to different treatment arms by randomization
Outcomes of treatment arms evaluated by statistical tests
Statistically significant results allow us to infer causality
Drawbacks• Long, expensive, intrusive• Short-term studies inconclusive• Rarely done in nutritional research• False positives and false negatives

Randomized Clinical TrialsLyon Diet Heart Study (France) • 300 subjects • Followup: 5 yrs
PREDIMED (Spain) • 8000 subjects • Followup: 5 yrs
Both studied Mediterranean Diet
Both showed significant benefit in reducing coronary heart disease compared to control diet

Observational studies
Obtain a large sample of individuals with some well defined common attributes (nationality, occupation, age, etc)
Record age, weight, height, blood pressure, educational level, exercise level, blood tests
Obtain dietary history by food frequency questionnaire (FFQ), food diary, or 24 hr recall
Follow up to determine end points: death, cause of death, and/or onset of specific diseases
Observational study analysisEvaluate outcomes with respect to the “risk factors” (demographic, personal and diet data) with statistical tests• Example: Heart attack rate is higher in people eating more
processed meat
Statistical significance indicates association between risk factors and outcome
Association does not prove causation• Achilles’ heel of observational studies• Replication in different settings, plausible biological
mechanisms can validate

Major observational studiesNurses Health Study (NHS) 100K 30yrs
Health Professional Followup Study (HPFS) 50K 25yrs
Physicians' Health Study (PHS) 50K 25yrs
NIH-AARP Diet and Health Study (AARP) 500K 10yrs
European Prospective Investigation into Cancer and Nutrition (EPIC) 500K 18yrs
Adventist Health Study (AHS)
Health Survey for England (HSE)

Diseases to focus on: Sutton’s lawWhen famed serial bank robber Willie Sutton was asked, “Why do you rob banks?”, he replied, “That's where they keep the money!”
Let’s focus on common impactful diseases highly influenced by lifestyle
Diseases where diet, exercise and/or smoking make a difference

Diseases to focus on
Common impactful diseases highly influenced by lifestyle• Coronary heart disease (“heart attacks”)• Cerebrovascular disease (“strokes”)• Type 2 diabetes mellitus & metabolic syndrome• Obesity and its complications• Lung cancer• Colon cancer

Mortality ratesSample: 20,000 men age 55 during one year of follow-up
Subjects:• 10,000 never-smokers (NS)• 10,000 current smokers (CS)
Deaths:• 40 NS• 120 CS
Mortality rate:• 4/1000/yr NS• 12/1000/yr CS
Mortality ratio
Mortality rate:• 4/1000/yr NS• 12/1000/yr CS
Mortality ratio:• CS vs. NS• 12 ÷ 4 = 3

Mortality ratioConclusion:• Current smokers had a mortality ratio of 3 compared to age-matched
never-smokers• Current smokers are three times more likely to die compared to
never-smokers the same age
Mortality ratio synonyms: • Risk ratio• Relative risk • Hazard ratio• Relative hazard

Mortality ratios
Study of milk product consumption and mortality in men: Netherlands
50,000 men, divided into 5 quintiles by amount of total dairy consumed
10,000 deaths over 10 years
1,980 deaths in 5th quintile (560 g/d avg.)
2,020 deaths in 1st quintile (80 g/d avg.)

Mortality ratioMortality rate, exposed• 1,980/10,000 = 19.8%
Mortality rate, not exposed• 2,200/10,000 = 20.2%
Mortality ratio• 19.8/20.2 = 0.98, or 98%
Lower means better, but how much better?• 1.0, or 100%, is the ratio of “no difference”• 98% -100% = -2%, a 2% reduction
Mortality ratio with confidence interval
Statistical theory gives us a “95% confidence interval”• 0.92 to 1.04 (-8% to +4%)• With 95% confidence, the “true value” of the mortality ratio lies within that
interval
A mortality ratio of 1.0 is the ratio of “no effect”• Exposed and unexposed subjects have the same mortality rate• If 1.0 falls within the 95% confidence interval, we are unable to declare a
significant difference between the exposed and unexposed subjects in the outcome
“Men consuming the highest amount of milk products had a mortality rate no different than those consuming the lowest amount”

Mortality ratio with confidence interval
Confidence interval depends on number of subjects• The larger the number of subjects, the smaller
the confidence interval, and the more precise the estimate of the true effect of the exposure
More subjects are required when we are trying to detect small effects

Dose-response curve
Plotting mortality ratio vs. magnitude of the exposure

Dose-response curveRising D-R higher risk of death; harmful→
Falling D-R lower risk of death; beneficial→
U-shaped D-R beneficial at low dose, but harm with increasing dose→
Food and health:The good, the bad, and the so-soCertain foods are very good for us ****• Lower your risk of diseases and death• Chow down on those
Other foods are very bad for us • Raise your risk of diseases and deaths• Best to reduce your consumption of those
Yet others are not especially good or bad ±• Replace the “bads” with these• But don’t overdo it: replace these with “goods” when possible
**** The “Goods” ****Foods we should consume, without fail, in sufficient quantities• Exception: Allergies (e.g., nuts) or intolerance (e.g., celiac disease
from gluten)
In general, the more, the better
With fruit & vegetables, the sky is the limit, practically speaking• Caution – vegetables: undesirable excess of certain nutrients, e.g.,
carotene• Caution – fruit: undesirable excess of high sugar fruits

**** The “Goods” ****
By nutrient• Fiber• Essential fatty acids• Protein• Vitamins• Anti-oxidants• Phyto-compounds
By food• Nuts• Whole grains• Fruits• Vegetables• Fish*• Alcohol*
* At low dose

± Moderation ±
Foods that may be consumed in moderation as part of a balanced diet
No demonstrated relationship between higher intake and worse, or better, outcome
May displace foods that are harmful (e.g., red meat) but should not displace foods that are beneficial (e.g., nuts)

± Moderation ±Dairy• Milk, cheese, butter, sour cream, cream cheese, ice cream,
yogurt
Eggs
Poultry• Chicken, turkey
Saturated fats

Restraint
Foods for which there is no known requirement
Foods that have identified risks associated with regular consumption
Foods with substitutes that are more beneficial
Foods that are often consumed mindlessly due to convenience, taste, rebound effects, food addiction

Restraint Processed meats• Lunch meat, sausage, bacon
Red meat• Beef• Pork• Mutton
Alcohol in excess
Fish in excess (?)
Trans fats
Refined grains (pure starch)• Refined wheat as breads, pasta,
desserts• White rice
White potatoes (pure starch)• Chips• French fries
Sugar• Beverages, including fruit juices• Desserts• Snacks• High-fructose corn syrup

**** Fiber ****
Indigestible carbohydrate compounds from plant-based foods• Inulin, pectin, raffinose, xylose, cellulose, hemi-cellulose
Soluble fiber feeds the intestinal microbiome• Byproducts of bacterial fermentation – short-chain
fatty acids, immune system stimulants, neuro-active compounds – are exceedingly valuable
• Some now call it “the gut microbial endocrine organ”

**** Fiber ****
Sources of fiber include nearly all plant-based foods• Grains (wheat, rice, corn, oats, barley, quinoa)
It’s the bran and germ that contain the goodness• Vegetables• Fruits• Tubers• Nuts• Legumes

**** Fiber ****Observational trials show strong beneficial relationship between total amount of dietary fiber and health outcomes, including all-cause mortality
Fiber from grains is especially beneficial

**** Fiber ****Total daily fiber target: 25+ g women, 30+ g men• Average American gets only half that amount; only 10% reach the target
Total daily carbs: 250 g woman, 300 g men
Rule of 1 in 10• Read Nutrition Facts label• Choose products with 1 or more g fiber for every 10 g total carbs• Whole grain pasta has 5 g fiber for 40 g total carbs GOOD!→
• White pasta has 2 g fiber for 40 g total carbs less desirable→
• Saltines have 0 g fiber for 20 g total carbs YUCK!→
Use whole grains for essentially all of your grain consumption, falling back on refined grains only when absolutely necessary (e.g., desserts)
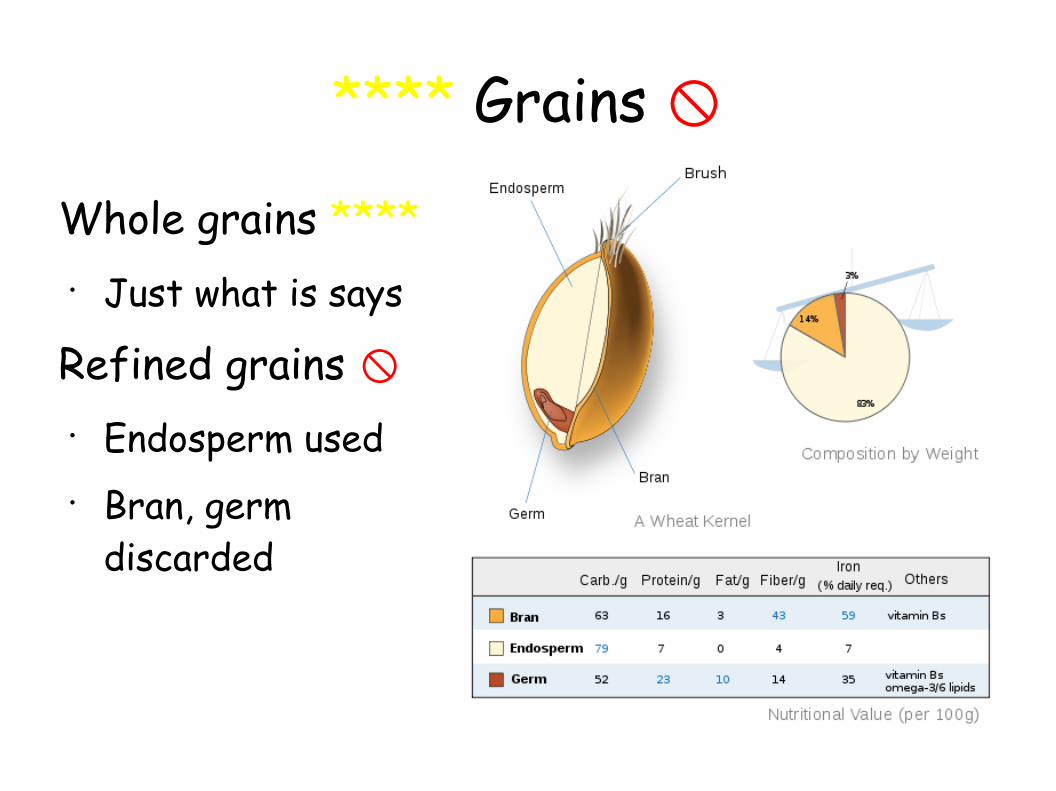
**** Grains
Whole grains ****• Just what is says
Refined grains • Endosperm used• Bran, germ
discarded

**** Whole grains ****
Whole grains are a major source of fiber in the diet
There are WG versions of most common grain foods, including cereals, bread, pasta, and rice
Dose-response curves for WG are very similar to those for fiber• Most of benefit for WG appears to come from fiber
content

**** Whole grains ****
Whole grain breakfast cereals are an especially beneficial addition to the diet and an easy way to add fiber
What about reconstituted whole grain products, especially those in which a single source of fiber is added back (e.g., inulin)?• We don’t know yet

Finding Whole Grain Foods

**** Nuts ****
Nuts, the Superfood
1+ serving/d• One serving is 1 oz, or 28 g, of nuts, or 1 tbsp of peanut
butter
Nuts are an excellent source of protein, fiber and good fats
Nuts travel well, don’t require refrigeration or special storage, make great snacks
**** Vegetables ****4+ servings/day• One serving is ½ cup of vegetables or 1 cup of green leafy
vegetables• 1 cup = 247 g
Vegetables as used here are “plants not included in other categories” (fruits, grains, nuts, seeds, legumes, white potatoes)
Valuable mostly for their micronutrients • Generally provide few calories, so not adequate as a “sole food”
**** Fruits ****3+ servings/day fresh or dried fruit• One serving is ½ cup of berries or 1 medium piece of fruit• 1 cup = 247 g
Only whole fruit considered• Fruit juice is a sugar drink, on par with soda
Some canned and frozen fruits carry risk rather than benefit, likely due to the high sugar content
Fruit contribution to nutrition is mainly micronutrients and fiber• Calories contribute to overall energy need but run the risk over displacing
other valuable foods

**** Legumes ****
Beans are an excellent source of multiple nutrients, especially protein and fiber
Out of favor with general U.S. public, ? because of perception of bloating and flatulence
Hummus (from garbanzo beans) is a good appetizer or snack

**** Polyunsaturated fats ****Essential fatty acids are those that are necessary and cannot be made in the body from other compounds• EPA & DHA – marine Ω-3 PUFA – 250 mg/d (see Fish slide)• Alpha-linolenic acid (ALA) – plant Ω-3 PUFA – 2-3 g/d• Linoleic acid (LA) – Ω-6 PUFA – 3-10 g/d
ALA and LA are abundant, in varying amounts, in vegetable oils, nuts, seeds

**** Fish
Marine omega-3 fatty acids 250 mg/d (EPA + DHA)• Two servings of suitable fish (cold-water fatty
ocean fish) per week supply an average of 250 mg/d, the threshold for full benefit
Fish oil capsules and other omega-3 supplements do not provide the same benefit as obtaining them from food sources (i.e., fish)

**** Fish Swedish Mammography Cohort (SMC) of 34,000 women
Consumption of fatty fish had a U-shaped association with all-cause mortality• Non-consumers had 25% higher
mortality than moderate consumers• High consumers had 68% higher
mortality than moderate consumers
Similar but less dramatic results for parallel group of men
**** Fish Swedish (SMC) study:
Cardiovascular disease risk lower for moderate consumption vs. none• Omega-3?
Cardiovascular disease risk higher for high consumption vs. moderate• PCBs, TMAO, methyl mercury?
Cancer had no association with fish consumption

**** Polyunsaturated fats ****
The minimums reflects the finding that there is a threshold below which a person is deficient in essential PUFA and may have symptoms
The upper limit of linoleic acid (n-6 PUFA) is controversial at this time, because some evidence points to negative effects in CVD, cancer, and other diseases with increasing amounts in the diet• Some authorities recommend no more than about 8 g/d

**** Polyunsaturated fats ****
Use vegetable oils with relatively high amounts of polyunsaturated fats for cooking and spreads instead of saturated fats (butter)
If consuming processed foods, look for those with more polyunsaturated fats and less saturated fats

**** Monounsaturated fats ****
MUFA supply an affordable fuel and substrate for lipid metabolism without adding risk
Oleic acid (Ω-9 MUFA) from olive oil is a poster child of “good fat”• Prominent part of the Mediterranean diet
± Dairy ±There is no established nutritional requirement for dairy products
Dairy is a potentially valuable addition to the diet for providing Vitamin D, calcium and high-quality protein
Saturated fat content of certain milk products, especially butter, cheese, and sour cream, was thought to carry a potential risk for atherosclerotic heart disease and obesity• Full-fat dairy was discouraged by health authorities for decades• Low-fat dairy was strongly promoted

± Dairy ±
Recent studies indicate that the risks of saturated fat consumption were exaggerated
Dose-response studies show no validated relationship between amount of dairy products consumed and mortality or specific disease rates• Full-fat and low-fat are equivalent
± Eggs ±
There is no established nutritional requirement for eggs
Eggs are a good source of high-quality protein
BUT...
Yolks contain large amounts of cholesterol and choline, of theoretical concern for risk in regard to ASCVD

± Eggs ±Study at UNC showed substantial increase in blood TMAO level in subjects fed 2 or more egg yolks
Choline in egg yolks is transformed to TMA by gut bacteria, and TMA is converted to TMAO by a liver enzyme FMO3

± Eggs ±Study at Cleveland Clinic showed increasing blood TMAO levels are associated with increasing coronary heart disease
TMAO levels attained with 2 or more egg yolk consumption was in the danger range for some of the subjects

± Eggs ±Dose-response studies show no validated relationship between amount of eggs consumed and mortality or specific disease rates• Exception: 42% higher diabetes rates with consumption of
1 or more eggs daily, compared to rare egg consumption• Exception: 69% higher cardiovascular disease rates with
consumption of 1 or more eggs daily in diabetics• Exception: 80% higher presence of coronary artery
calcifications with consumption of 1 or more eggs daily
± Eggs ±Dose-response studies show no validated relationship between amount of eggs consumed and mortality or specific disease rates• Exception: 42% higher diabetes rates with consumption of
1 or more eggs daily, compared to rare egg consumption• Exception: 69% higher cardiovascular disease rates with
consumption of 1 or more eggs daily in diabetics• Exception: 80% higher presence of coronary artery
calcifications with consumption of 1 or more eggs daily

± Eggs ±
Until we know more, it’s probably wisest to limit egg consumption to a few per week

± Poultry ±
There is no established nutritional requirement for white meat in the diet
Poultry is a good source of high-quality protein
Dose-response studies show no validated relationship between amount of poultry consumed and mortality or specific disease rates

Sugar beverages
Sodas and flavored sugar or HFCS beverages are empty calories
Fruit juices may provide vitamins, but their benefit is compromised by contribution of the high sugar content to overload of refined carbohydrates
Dose-response studies show positive relationship between amount of sugar beverages consumed and mortality, as well as heart disease and diabetes
Red / processed meat
Red meat is meat from cows, pigs and sheep
There is no known requirement for this food group
Quality protein, vitamins and energy are supplied by red meat
However, these are readily obtainable from other sources with less risk

Red / processed meat All-cause mortality risk increases 19% for each serving (3 oz unprocessed / 1.5 oz processed), up to 2x for 4 servings a day
Repeatedly associated with substantial risk of coronary heart disease and diabetes, as well as mortality

Red / processed meat
Why is red meat so lethal?• We were told it was the saturated fat; simply trim the fat,
eat low-fat cuts, and all is OK• WRONG!• Remember eggs and choline?• For red meat, it’s a relative of choline, carnitine, that is
converted into TMAO• Red meat, especially beef, has the highest amounts of
carnitine of any food

Red / processed meat
Probably wisest to limit red meat consumption to a couple of servings a week, including processed meats (bacon, sandwich meats, sausages, hot dogs)

Refined grains, starches
Refined grains includes white bread, white pasta, white rice, cakes, cookies, donuts
Starches includes white potatoes, especially chips and fries
These are digested rapidly, beginning in the mouth with salivary amylase, into glucose• Results in rapid blood glucose rise and insulin response

trans fat Trans fats are artificial fats that are solid at room temperature, made by hydrogenating vegetable oils
They were widely used in snack foods and to replace saturated fats in deep-frying
They were discovered to be strongly associated with increased risk for cardiovascular disease
As a result, trans fats are being phased out of the food supply, but perhaps still used in some processed foods

**** Alcoholic beverages
1 drink = 12 oz beer, 4 oz wine, 1.5 oz liquor
There is no established nutritional requirement for alcohol
Alcohol abuse (excessive consumption, addiction) is a major source of disease, distress and disruption in th U.S.
Alcoholic liver disease and other complications are prominent causes of death

**** Alcoholic beverages 1 drink = 12 g alcohol
Numerous studies have shown a similar pattern of substantially lower rates of mortality and heart disease in those consuming small amounts (1-2 drinks) daily
Favorable changes in risk factors (e.g., cholesterol)

**** Alcoholic beverages
If you already enjoy drinking, can do so in a restrained manner, and have no medical contraindications, there is no medically defined reason to discontinue drinking
Otherwise, it is best to discontinue or not begin drinking

**** Effects of Exercise ****All the following are effects of physical activity supported by statistically significant research results; with regular exercise you can:
Control your weight
Reduce your risk of cardiovascular disease
Reduce your risk for type 2 diabetes and metabolic syndrome
Reduce your risk of some cancers
Strengthen your bones and muscles
Improve your mental health and mood
Improve your ability to do daily activities and prevent falls, if you're an older adult
Increase your chances of living longer
http://www.cdc.gov/physicalactivity/basics/pa-health/index.htm
Activity in METsThe intensity of an activity is the total energy expenditure during that activity measured in METs• 1-1.5: sedentary; 1.6-2.9: light; 3-6: moderate; >6: vigorous
Cumulative activity measured in MET-h/wk• Example: Walking 3 mph (3.3 MET) 20 minutes a day• 7.7 MET-h/wk = 3.3 MET x 1/3 h/day x 7 day/wk• 7.5 is the recommended minimum (2008 Physical Activity
Guidelines for Americans)
Physical Activity & Mortality
National Cancer Institute Cohort Consortium
Subjects: 661,137 (44% men) in 6 cohorts
Follow-up: 14.2 yrs
Events: 116,686 deaths
Age: 62 (median)
Physical activity: 8 MET-h/wk (median)

Physical Activity & Mortality

Physical Activity & MortalityAny physical activity up to recommended minimum (7.5 MET-h/wk) is associated with 20% reduction in all-cause mortality, compared to no activity
Further increased PA is associated with additional reduction, up to maximum 39% reduction at 22.5-40 MET-h/wk
Highest level of activity (>75 MET-h/wk) had slightly less apparent benefit
These results were all after adjustment for other factors, including good risk factors such as lower age, smoking, and BMI

Recommendations
Regular physical activity
Base diet around nuts, whole grains, vegetables, fruits, beans, fish, poultry, olive oil, vegetable oils
Modest amounts of dairy, eggs
Sparing amounts of red meat, processed meats, sugary beverages, white potatoes, refined grains (white bread, rice, cereal, desserts)
Harvard Healthy Eating Pyramid

More information
Web site for my OLLI at Duke class:
http://olli-what-to-eat-and-why.weebly.com
Web site for OLLI courses:
http://learnmore.duke.edu/OLLI

Medicine’s best kept secret:meat and heart disease
The gut microbiome – the resident bacteria of our intestinal tract – plays a major role in health and disease
The link between meat consumption and heart disease has been found – and it involves our gut microbiome!
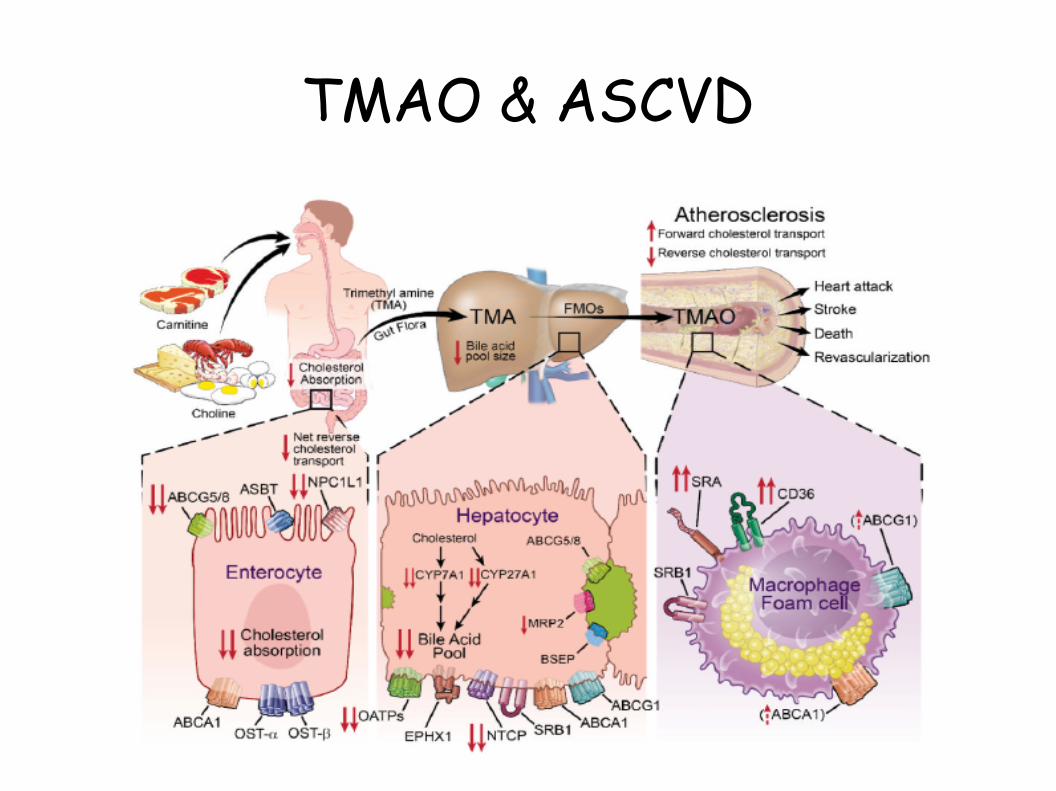
TMAO & ASCVD

Discoverer of the TMAO-ASCVD link
Cleveland Clinic is a major heart disease referral center• Project GeneBank started around 2000,
aiming to advance knowledge of the causes, prevention and treatment of cardiovascular disease
• Goal of enrolling 10,000 subjects• Blood samples obtained for studies
Stanley Hazen, M.D., Ph.D.• Used advanced technology (LC/MS) to
look for molecules in blood associated with ASCVD
• TMAO was that molecule

ASCVD events and TMAO

Atherosclerosis Formation

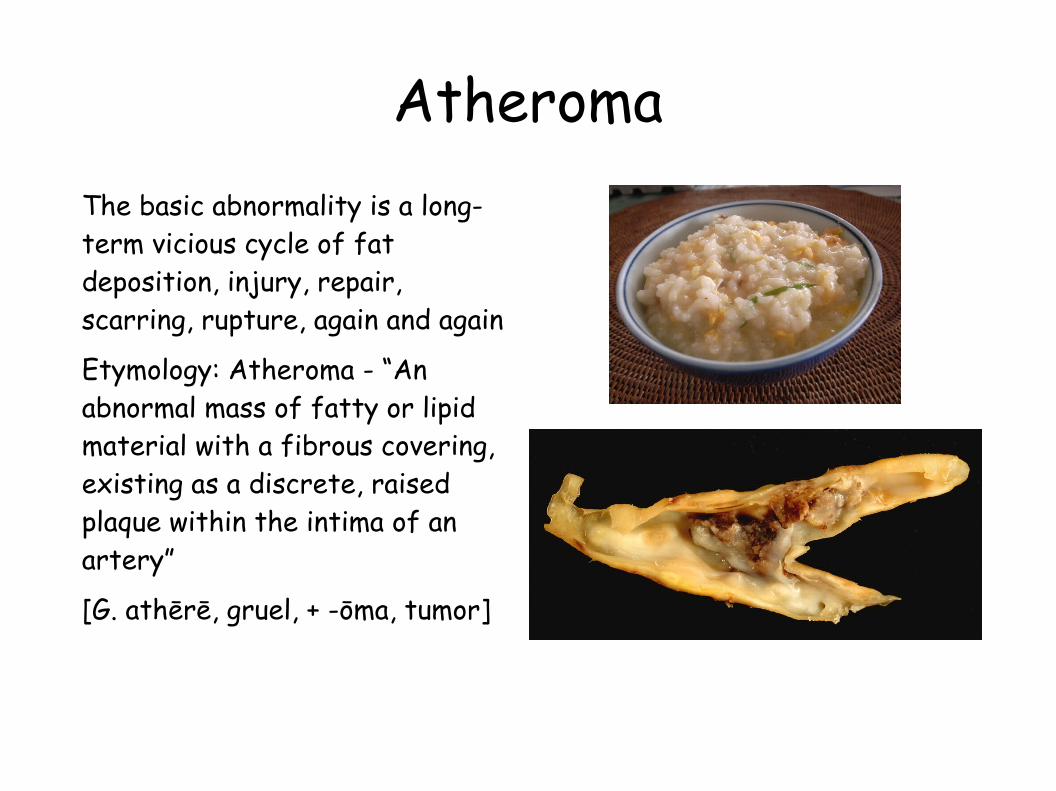
AtheromaThe basic abnormality is a long-term vicious cycle of fat deposition, injury, repair, scarring, rupture, again and again
Etymology: Atheroma - “An abnormal mass of fatty or lipid material with a fibrous covering, existing as a discrete, raised plaque within the intima of an artery”
[G. athērē, gruel, + -ōma, tumor]
Atherosclerosis (AS)The disease process which affects the walls of arteries, eventually leading to blockage
Consequences of AS are effects on specific organs • Myocardial infarction, or heart attack (heart) – ASHD, CHD• Cerebrovascular accidents, or strokes (brain) - CVD• Infarction, or tissue death (extremities, organs) - ASPVD• Known collectively as atherosclerotic cardiovascular disease
(ASCVD, ASVD)

Atherosclerosis (AS)
ASCVDs are the leading preventable causes of death and disability in the U.S. and other developed nations• Most cases can be avoided by appropriate diet,
but we’re just now learning what that is• A small minority are genetically driven by errors
in metabolic pathways (familial hyperlipidemias) or anatomic defects (aneurysms)

ASCVD conundrumRisk factors identified• Lipoprotein (“cholesterol”) metabolism – higher LDL and triglycerides, lower HDL• Hypertension• Obesity• Cigarette smoking• Metabolic syndrome diabetes→
Yet, in statistical analysis of populations, much of the disease risk remained unaccounted for by these factors• Non-smokers with normal blood pressure who are not diabetic or obese and have
“favorable” cholesterol profiles can have MI, CVA• ASCVD becomes nearly universal in upper decades of life
Red meat & ASCVD:Focus on Fat
Association of meat & ASCVD recognized from 1940s
Ancel Keys – Seven Countries Study: Blood cholesterol associated with ASHD• Blood cholesterol highly correlated with saturated fat consumption
McGovern Committee (1970s) focused on saturated fat, leading to USDA emphasis
A generation of nutrition advice based on concept that dietary saturated fat ASCVD→
Saturated fat comes largely from meat and dairy

Red meat & ASCVD: The Conspiracy
Political aspect: Industry associations lobbied tirelessly against placing blame on beef, pork, dairy; pointed the finger at fat
Industry groups promoted low-fat cuts of meat, low-fat dairy as the answer
Food manufacturers promoted low-fat products • Fat had no trade association or lobbyists
USDA promoted substitution of grains and other carbs for fat in the diet • Food Pyramid called for 6-11 daily servings of starchy foods as the
foundation of the diet

ASCVD & diet
• Cohort observational studies pointed to diet as an independent factor
^ red meat consumption associated with higher ASCVD ^ nuts, dietary fiber associated with lower ASCVD
• Randomized clinical trials demonstrate that Mediterranean diet is an independent favorable factor
• What’s responsible?

21st century findingsRed meat – and especially processed meat – is highly associated with ASHD and mortality• 25% increased mortality for each additional serving per day
But, saturated fat turns out not to be the culprit; SF is not correlated with ASHD
21st century findings
Red meat – and especially processed meat – is highly associated with ASHD and mortality
If not the fat, what is the lethal nutrient?• CARNITINE (and its cousins, choline & phosphatidyl
choline)• Red meat has abundant carnitine• Consumed carnitine is transformed into a toxic
molecule, TMAO

Typical Calorie DistributionFuel to run the body’s “engine”
All macronutrients can be used for energy, but generally it’s much more expensive to use proteins for energy
Carbohydrate 50%
Fats 35%
Protein 15%
Sodium
Sodium is an essential mineral in the diet, but sodium deficiency is rare in the modern era
Excessive dietary sodium is of concern to those with heart failure, hypertension and kidney disease
There is still considerable uncertainty about the optimal range for sodium intake in healthy individuals

Dietary ProteinDaily protein requirement for a moderately active adult is 0.8 mg/kg• Average 70 kg adult needs 56 g/d, equivalent to 224 Cal, or ~10% of daily calorie
requirement
Recommendation of 15% calories from protein gives a 50% “cushion”
Protein is so plentiful in any reasonable Western diet that only those on very poor diets are likely to fall short
Excessive protein in the diet has no proven adverse effects, but is a waste of money, since protein is generally much more expensive, calorie for calorie
Those on strict vegetarian diets must pay careful attention to getting complete protein, that is, adequate amounts of all essential amino acids, because (unlike animal-sourced foods) plants have restricted amino acid distributions
Diet definitionsOmnivore• All food types – animal- and plant-sourced
Vegan or Strict Vegetarian• Only plant-sourced foods
Lacto-ovo-vegetarian• Plant-sourced foods plus eggs & dairy
Pescotarian• Plant-sourced foods plus seafood, eggs & dairy
Semi-vegetarian• Plant-sources foods plus animal-source foods less than once per week
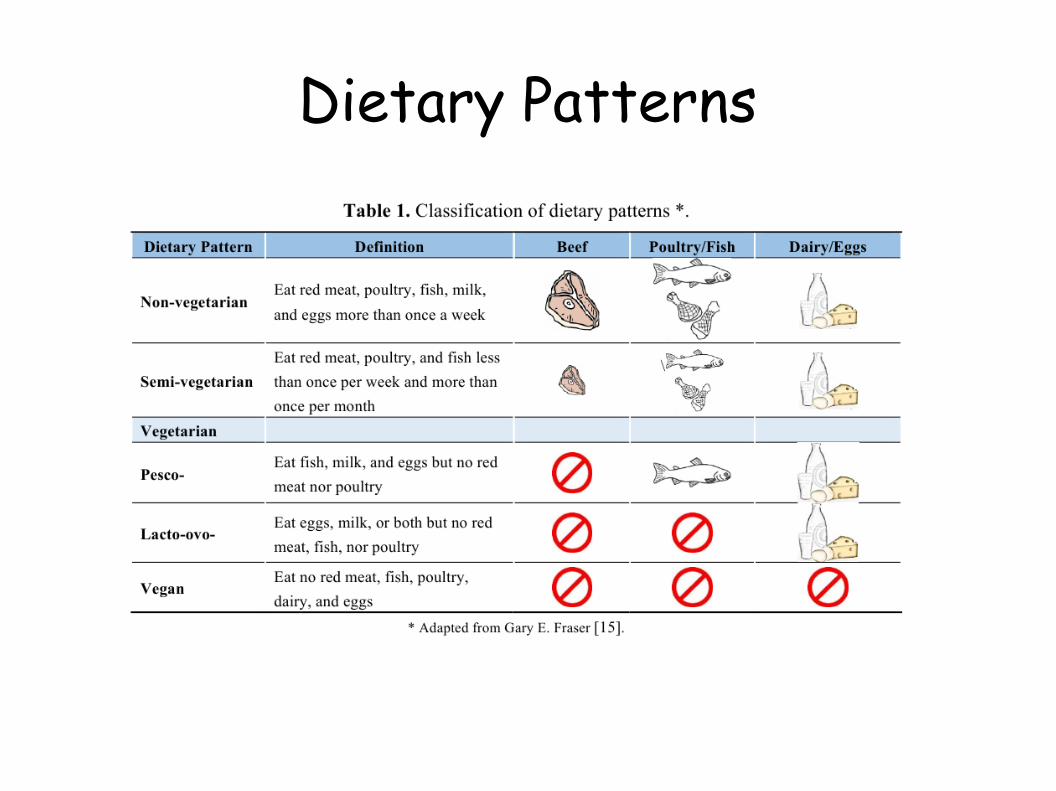
Dietary Patterns

Vegetarian advantage?Adventist Health Studies• Observational studies on Seventh Day Adventists• Adventists follow healthy lifestyles: few smoke or drink, and
many eat vegetarian diets• Within their cohort, all vegetarian subgroups have superior
survival to non-vegetarians• Pescoterians have the greatest reduction in mortality compared
to non-vegetarians• Vegan advantage is possibly explained by their dramatically
higher fiber intake (46g/d) vs. non-vegetarians (30g/d)

Vegetarian advantage?EPIC-Oxford study was unable to detect a survival advantage for vegetarians compared to non-vegetarians
My current conclusion is that the benefit from a vegetarian diet can be explained by the high amount of fiber and avoidance of red meat• The addition of fish could be beneficial to get marine omega-3• Vegans must be careful to get supplemental vitamin B-12 and to have
balanced protein sources to get all essential amino acids• Unlikely to appeal to large segment of the population, so not a
general solution for the nutritional deficiencies of the American diet

Mediterranean Diet

Mediterranean Diet TrialsRandomized controlled trials in patients with established coronary disease or diabetes (secondary prevention)
Lyon Diet Heart Study (France) • 420 patients, followup 4yrs• 70% reduction in heart attacks, cardiac deaths
PREDIMED (Spain) • 8000 patients, followup 5yrs• 30% reduction in heart attack, strokes, cardiac deaths
Can these results be generalized to primary prevention, other populations?
Would results hold up under longer followup?

Mediterranean Diet - ConclusionsPeople who have had their first MI, or who have not had CVD but have strong risk factors, may reduce their risk of having an MI or death from CHD by following a Mediterranean diet by comparison to following a low-fat diet
These conclusions were demonstrated in RCT; therefore, one may draw valid conclusions about causality
However, follow-ups are short in both Lyon Diet Heart Study and PREDIMED study; stay tuned to this channel for future developments
Significance of our microbiomeWe are all gardeners
Our “inner garden”, is the community of micro-organisms that live in our colon
These bacteria consume undigested residue, mainly fiber, from our diet
They provide us a broad array of metabolic, immune, anti-inflammatory, and hormonal functions
The more diverse and prolific our garden, the more it benefits us

Weight ControlObesity: a national – and now worldwide – epidemic
Fat tissue is “greedy”, never satisfied• Sends metabolic signals saying “more, more”• Like a one-way turnstile• Difficult to overcome
Good new book by Dr. David Ludwig• “Always Hungry”
Ketogenic diets• An encouraging method for durable fat redemption• Separate slide set on web site