effect of a closed foldable equator ring on capsular bag shrinkage in cataract surgery
TRANSCRIPT

J CATARACT REFRACT SURG - VOL 32, OCTOBER 2006
Effect of a closed foldable equator ring
on capsular bag shrinkage in cataract surgery
Sabine Kurz, MD, Frank Krummenauer, DSc, Carolin Dumbach, Norbert Pfeiffer, MD, H. Burkhard Dick, MD
PURPOSE: To evaluate the effect of a closed foldable equator ring (CFER) versus a conventional cap-sular tension ring (CTR) on capsular bag shrinkage.
SETTING: Department of Ophthalmology, Johannes Gutenberg-University, Mainz, Germany.
METHODS: In this prospective study, 70 eyes of 70 patients were randomized to 2 groups using a 1:1block scheme. After uneventful cataract surgery, a capsular measuring ring was implanted in all eyes tomeasure the capsular bag diameter in vivo. In Group 1, a CTR was implanted in the capsular bag. InGroup 2, a CFER was inserted. Biometric characteristics such as axial length and the horizontal and ver-tical corneal radii were measured preoperatively. The capsular bag diameter and capsulorhexis diam-eter were measured intraoperatively and 2 or 3 days as well as 1 and 3 months postoperatively.
RESULTS: There were no statistically significant or clinically relevant between-group differences in co-variants such as axial length, vertical and horizontal corneal radii, and capsulorhexis diameter. Eyeswith the CTR had slight but statistically significant capsular bag shrinkage from a median of 10.4 toa median of 10.2 mm after 3 months (P<.001). Eyes with the CFER also had slight but statistically sig-nificant capsular bag shrinkage from a median of 10.3 to a median of 10.2 mm 3 months postopera-tively (P Z .021). At baseline, the CTR group had a larger capsular bag diameter, but there were nostatistically significant differences between the groups at the 3-month follow-up (P Z .669).
CONCLUSIONS: No clinically relevant capsular bag shrinkage was observed after implantation ofa CFER or a CTR. The expected capsular bag shrinkage was the same in both groups.
J Cataract Refract Surg 2006; 32:1615–1620 Q 2006 ASCRS and ESCRS
Over the past 14 years, capsular tension rings (CTRs) have
become indispensable in cataract surgery. The rings are de-
signed to maintain the configuration and stability of the
capsule equator by improving zonular integrity and dimin-
ishing traction on the zonules.1–3 Intraoperative complica-tions such as preexisting zonular dehiscence and zonular
weakness can be managed easier with a CTR.4,5 Some
CTR designs have been developed for specific indica-
tions.6–9 Most commercially available CTRs are open and
Accepted for publication May 17, 2006.
From the Department of Ophthalmology (Kurz, Dumbach,Pfeiffer, Dick), Johannes Gutenberg-University, Mainz, and theDepartment of Clinical Epidemiology and Health Economy(Krummenauer), Technical University of Dresden, Dresden,Germany.
No author has a financial or proprietary interest in any material ormethod mentioned.
Corresponding author: Dr. Sabine Kurz, Department of Ophthal-mology, Johannes Gutenberg-University, Langenbeckstrasse 1,55101 Mainz, Germany. E-mail: [email protected].
Q 2006 ASCRS and ESCRS
Published by Elsevier Inc.
consist of single-piece, rigid poly(methyl methacrylate)
(PMMA).3,10
Shrinkage of the capsular bag, which can start im-
mediately after cataract surgery, usually stops 3 months
postoperatively.11 It can lead to intraocular lens (IOL)decentration, deformation, or tilting.12 Implanting a CTR
reduces capsular bag shrinkage.13
The goal of this randomized prospective study was to
compare the effect of a foldable closed equator ring (CFER)
and with that of an open CTR on capsular bag shrinkage.
PATIENTS AND METHODS
This study comprised 70 eyes of 70 patients having cataractsurgery by the same surgeon (H.B.D.). All patients gave written in-formed consent before surgery in accordance with the Declarationof Helsinki. The study was approved by the local ethics committeein May 2003.
Inclusion criteria were senile cataract, axial length between21.5 mm and 26.0 mm, and intact zonules and capsular bag. Pa-tients with intraoperative complications such as capsule tears orzonulysis were excluded. Other exclusion criteria were lenticularpseudoexfoliation, proliferative diabetic retinopathy, uveitis,
0886-3350/06/$-see front matterdoi:10.1016/j.jcrs.2006.05.012
1615
FOLDABLE EQUATOR RING AND CAPSULAR BAG SHRINKAGE
intraocular surgery, corneal diseases, ocular trauma, and pupilssmaller than 8.0 mm after medical dilation.
Preoperatively, slitlamp examination of the anterior and pos-terior segments was performed under mydriasis with tropicamideand phenylephrine hydrochloride (Neo-Synephrine). Axial lengthand anterior chamber depth were measured with the IOLMaster(Carl Zeiss).14–16
Study Design
Immediately preoperatively, the eyes were randomized into 2groups using a 1:1 block randomization scheme; the random listwas generated by an independent medical biometrician (F.K.) us-ing unit SPSS statistical software. Group 1 received a CTR, andGroup 2 received a CFER. Patients were masked to which ringthey received.
The sample size was based on the findings of a previous inde-pendent randomized trial13 that indicated an expected capsularbag shrinkage of 0.15 mm after CTR implantation and 0.38 mmafter implantation of a capsular measuring ring (CMR). This dif-ference led to the following assumptions about whether a clinicallyrelevant difference in capsular bag shrinkage inhibition betweenthe CTR and CFER supplementation could be established: Supe-riority of the CFER over the CTR would be established if theCTR led to a median shrinkage of 0.20 mm and the CFER led toa median shrinkage of 0.10 mm or less in the new trial. A samplesize of 70 eyes was derived to enable the trial to detect this differ-ence at a 5% significance level based on a statistical power of 90%.A 10% dropout rate was introduced into this setting.
To avoid bias, all postoperative measurements were done bythe same investigator (C.D.) and all intraoperative measurementsby the same surgeon.
Ring Designs
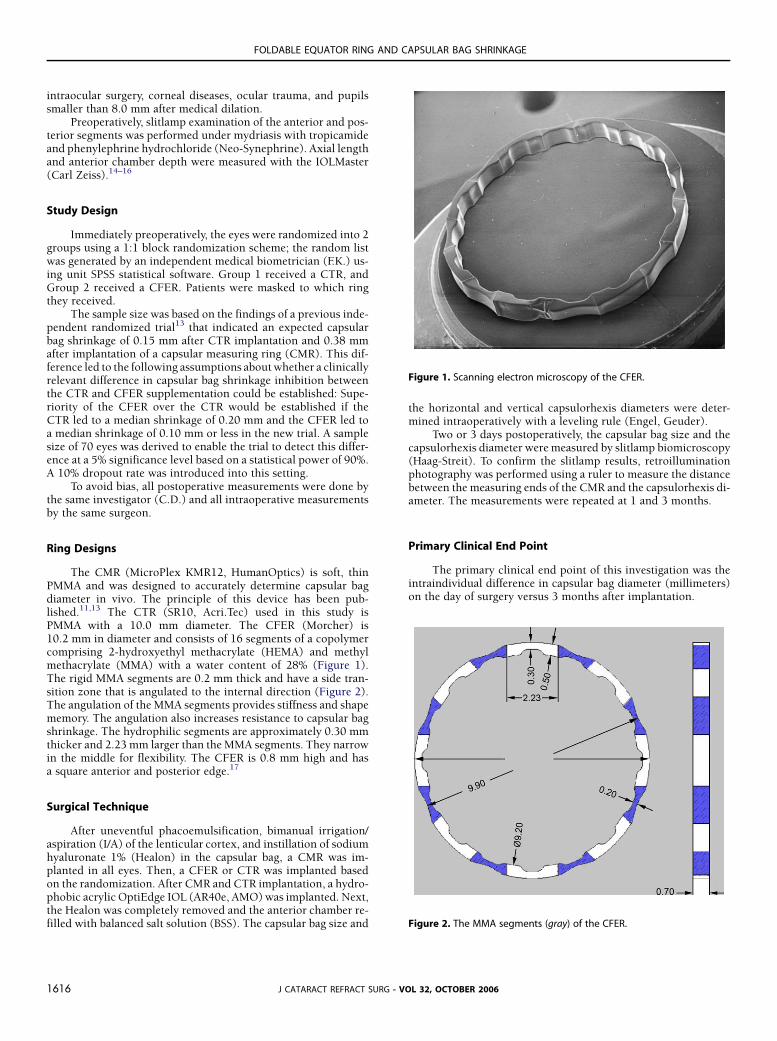
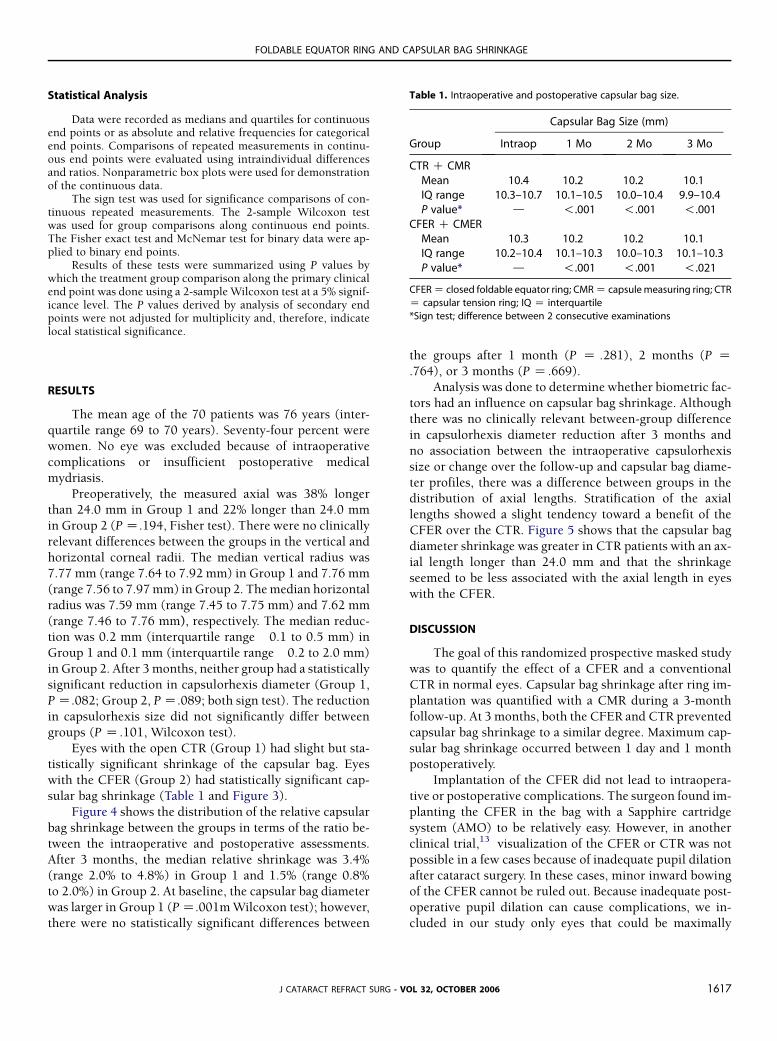
The CMR (MicroPlex KMR12, HumanOptics) is soft, thinPMMA and was designed to accurately determine capsular bagdiameter in vivo. The principle of this device has been pub-lished.11,13 The CTR (SR10, Acri.Tec) used in this study isPMMA with a 10.0 mm diameter. The CFER (Morcher) is10.2 mm in diameter and consists of 16 segments of a copolymercomprising 2-hydroxyethyl methacrylate (HEMA) and methylmethacrylate (MMA) with a water content of 28% (Figure 1).The rigid MMA segments are 0.2 mm thick and have a side tran-sition zone that is angulated to the internal direction (Figure 2).The angulation of the MMA segments provides stiffness and shapememory. The angulation also increases resistance to capsular bagshrinkage. The hydrophilic segments are approximately 0.30 mmthicker and 2.23 mm larger than the MMA segments. They narrowin the middle for flexibility. The CFER is 0.8 mm high and hasa square anterior and posterior edge.17
Surgical Technique
After uneventful phacoemulsification, bimanual irrigation/aspiration (I/A) of the lenticular cortex, and instillation of sodiumhyaluronate 1% (Healon) in the capsular bag, a CMR was im-planted in all eyes. Then, a CFER or CTR was implanted basedon the randomization. After CMR and CTR implantation, a hydro-phobic acrylic OptiEdge IOL (AR40e, AMO) was implanted. Next,the Healon was completely removed and the anterior chamber re-filled with balanced salt solution (BSS). The capsular bag size and
J CATARACT REFRACT SURG1616
the horizontal and vertical capsulorhexis diameters were deter-mined intraoperatively with a leveling rule (Engel, Geuder).
Two or 3 days postoperatively, the capsular bag size and thecapsulorhexis diameter were measured by slitlamp biomicroscopy(Haag-Streit). To confirm the slitlamp results, retroilluminationphotography was performed using a ruler to measure the distancebetween the measuring ends of the CMR and the capsulorhexis di-ameter. The measurements were repeated at 1 and 3 months.
Primary Clinical End Point
The primary clinical end point of this investigation was theintraindividual difference in capsular bag diameter (millimeters)on the day of surgery versus 3 months after implantation.
Figure 1. Scanning electron microscopy of the CFER.
Figure 2. The MMA segments (gray) of the CFER.
- VOL 32, OCTOBER 2006
FOLDABLE EQUATOR RING AND CAPSULAR BAG SHRINKAGE
Statistical Analysis
Data were recorded as medians and quartiles for continuousend points or as absolute and relative frequencies for categoricalend points. Comparisons of repeated measurements in continu-ous end points were evaluated using intraindividual differencesand ratios. Nonparametric box plots were used for demonstrationof the continuous data.
The sign test was used for significance comparisons of con-tinuous repeated measurements. The 2-sample Wilcoxon testwas used for group comparisons along continuous end points.The Fisher exact test and McNemar test for binary data were ap-plied to binary end points.
Results of these tests were summarized using P values bywhich the treatment group comparison along the primary clinicalend point was done using a 2-sample Wilcoxon test at a 5% signif-icance level. The P values derived by analysis of secondary endpoints were not adjusted for multiplicity and, therefore, indicatelocal statistical significance.
RESULTS
The mean age of the 70 patients was 76 years (inter-
quartile range 69 to 70 years). Seventy-four percent were
women. No eye was excluded because of intraoperative
complications or insufficient postoperative medical
mydriasis.
Preoperatively, the measured axial was 38% longerthan 24.0 mm in Group 1 and 22% longer than 24.0 mm
in Group 2 (P Z.194, Fisher test). There were no clinically
relevant differences between the groups in the vertical and
horizontal corneal radii. The median vertical radius was
7.77 mm (range 7.64 to 7.92 mm) in Group 1 and 7.76 mm
(range 7.56 to 7.97 mm) in Group 2. The median horizontal
radius was 7.59 mm (range 7.45 to 7.75 mm) and 7.62 mm
(range 7.46 to 7.76 mm), respectively. The median reduc-tion was 0.2 mm (interquartile range �0.1 to 0.5 mm) in
Group 1 and 0.1 mm (interquartile range �0.2 to 2.0 mm)
in Group 2. After 3 months, neither group had a statistically
significant reduction in capsulorhexis diameter (Group 1,
P Z.082; Group 2, P Z.089; both sign test). The reduction
in capsulorhexis size did not significantly differ between
groups (P Z .101, Wilcoxon test).
Eyes with the open CTR (Group 1) had slight but sta-tistically significant shrinkage of the capsular bag. Eyes
with the CFER (Group 2) had statistically significant cap-
sular bag shrinkage (Table 1 and Figure 3).
Figure 4 shows the distribution of the relative capsular
bag shrinkage between the groups in terms of the ratio be-
tween the intraoperative and postoperative assessments.
After 3 months, the median relative shrinkage was 3.4%
(range 2.0% to 4.8%) in Group 1 and 1.5% (range 0.8%to 2.0%) in Group 2. At baseline, the capsular bag diameter
was larger in Group 1 (P Z.001m Wilcoxon test); however,
there were no statistically significant differences between
J CATARACT REFRACT SURG
the groups after 1 month (P Z .281), 2 months (P Z.764), or 3 months (P Z .669).
Analysis was done to determine whether biometric fac-
tors had an influence on capsular bag shrinkage. Although
there was no clinically relevant between-group difference
in capsulorhexis diameter reduction after 3 months and
no association between the intraoperative capsulorhexis
size or change over the follow-up and capsular bag diame-
ter profiles, there was a difference between groups in thedistribution of axial lengths. Stratification of the axial
lengths showed a slight tendency toward a benefit of the
CFER over the CTR. Figure 5 shows that the capsular bag
diameter shrinkage was greater in CTR patients with an ax-
ial length longer than 24.0 mm and that the shrinkage
seemed to be less associated with the axial length in eyes
with the CFER.
DISCUSSION
The goal of this randomized prospective masked study
was to quantify the effect of a CFER and a conventional
CTR in normal eyes. Capsular bag shrinkage after ring im-
plantation was quantified with a CMR during a 3-month
follow-up. At 3 months, both the CFER and CTR prevented
capsular bag shrinkage to a similar degree. Maximum cap-
sular bag shrinkage occurred between 1 day and 1 monthpostoperatively.
Implantation of the CFER did not lead to intraopera-
tive or postoperative complications. The surgeon found im-
planting the CFER in the bag with a Sapphire cartridge
system (AMO) to be relatively easy. However, in another
clinical trial,13 visualization of the CFER or CTR was not
possible in a few cases because of inadequate pupil dilation
after cataract surgery. In these cases, minor inward bowingof the CFER cannot be ruled out. Because inadequate post-
operative pupil dilation can cause complications, we in-
cluded in our study only eyes that could be maximally
Table 1. Intraoperative and postoperative capsular bag size.
Capsular Bag Size (mm)
Group Intraop 1 Mo 2 Mo 3 Mo
CTR C CMRMean 10.4 10.2 10.2 10.1IQ range 10.3–10.7 10.1–10.5 10.0–10.4 9.9–10.4P value* d !.001 !.001 !.001
CFER C CMERMean 10.3 10.2 10.2 10.1IQ range 10.2–10.4 10.1–10.3 10.0–10.3 10.1–10.3P value* d !.001 !.001 !.021
CFER Z closed foldable equator ring; CMR Z capsule measuring ring; CTR
Z capsular tension ring; IQ Z interquartile
*Sign test; difference between 2 consecutive examinations
- VOL 32, OCTOBER 2006 1617

FOLDABLE EQUATOR RING AND CAPSULAR BAG SHRINKAGE
Figure 3. Nonparametric box plots of capsular bag
shrinkage (mm) distribution after 2 to 3 days as well
as 1 and 3 months after surgery (pre – post) (horizontal
lines indicate median and quartiles, minimum and
maximum values, which do not exceed a deviation
from the quartiles or more than 1.5 times the inter-
quartile ranges; o Z statistical outliers with deviation
from the quartiles of more than 1.5 times the inter-
quartile range; * Z statistical extreme values with de-
viation from the quartile of more than 3 times the
interquartile range).
dilated preoperatively. Even in cases of inadequate dilationresulting from the cataract surgery, the measuring exten-
sions of the CMR could be visualized at the slitlamp post-
operatively in all eyes.
Hara et al.18,19 first described a ring that was inserted in
the capsular bag equator to support the zonular apparatus
J CATARACT REFRACT SURG -1618
and to maintain the complete circular contour of the capsu-lar bag equator after cataract extraction. The closed, flexible
circular ring was silicone. It had a diameter of 10.0 mm, an
inner ring surface groove, and a square cross-section. Their
goal was to prevent capsular bag deformation and posterior
capsule opacification (PCO) after cataract extraction.
Figure 4. Nonparametric box plots of the relative
shrinkage (post/pre) of the capsular bag diameter
(horizontals Z medians and quartiles, minimum and
maximum values, which do not exceed a deviation
from the quartiles or more than 1.5 times the inter-
quartile ranges; o Z statistical outliers with deviation
from the quartiles of more than 1.5 times the inter-
quartile range; * Z statistical extreme values with de-
viation from the quartile of more than 3 times the
interquartile range).
VOL 32, OCTOBER 2006

FOLDABLE EQUATOR RING AND CAPSULAR BAG SHRINKAGE
Figure 5. Nonparametric box plots of the relative
shrinkage (3 months after surgery/intraoperatively)
of the capsular bag diameter separated by axial length
(horizontals Z medians and quartiles, minimum and
maximum values, which do not exceed a deviation
from the quartiles or more than 1.5 times the inter-
quartile ranges; o Z statistical outliers with deviation
from the quartiles of more than 1.5 times the inter-
quartile range; * Z statistical extreme values with de-
viation from the quartile of more than 3 times the
interquartile range).
Because the ring did not adapt to various capsule sizes, it
was never implanted in human eyes.
Nishi et al.20 report inhibition of epithelial cell migra-
tion at the capsular equator with an open, rigid bending
ring; the inhibition was the result of the ring’s square-edged
design. They found statistically reduced PCO 2 years afterIOL and capsular bending ring implantation.9 Because of
the lateral height (0.7 mm) of the capsular bending ring,
adhesion between the anterior and posterior lens capsules
can be reduced. Such adhesion can lead to lens epithelium
transformation on the back of the anterior capsule. There-
fore, anterior capsule fibrosis and shrinkage as well as PCO
can be reduced. The ring’s sharp, square-edged design can
inhibit epithelial cell migration from the periphery to thecenter of the capsular bag. However, lens epithelial cell
migration between the 2 ends of a capsular bending ring
is still possible9 because the ends do not always overlap.
In contrast, the ends of CTRs can push on each other
when capsular bag shrinkage occurs. Therefore, to our
understanding, a closed circular capsular ring with a large
lateral height and a sharp-edged design could achieve
360-degree reduction of PCO. This would keep the capsu-lar bag open, reduce anterior capsule opacification for good
visualization of the peripheral retina, and provide even ex-
tension of the capsular bag. The most commonly used
CTRs today are open and made of rigid single-piece
PMMA. Because of the characteristics of PMMA, a closed
capsular ring is almost impossible to implant safely in the
capsular bag. The composition of the CFER allows implan-
tation of a closed and foldable system.
J CATARACT REFRACT SURG
One limitation of this study is the method to determine
the capsular bag size with the CMR. Although the CMR is
very soft acrylic, one cannot predict the fraction of capsular
bag shrinkage prevented by the CMR itself. At present, the
CMR is used only for clinical research purposes and no un-
biased methods to precisely assess capsular bag diameterexist.
Furthermore, although the 2 patient groups were
strictly randomized to receive a CFER or a CTR, the eyes
with the CTR were statistically significant higher axial
length than those with the CFER. Therefore, the difference
in shrinkage from 10.4 to 10.2 mm with the CFER and 10.3
to 10.2 mm with the CTR after 3 months appears to be clin-
ically irrelevant.Another limitation of this study was the short follow-up
of 3 months. This study would be stronger if the patients had
been evaluated for 6 months or longer. However, Tehrani
et al.11 found no significant capsular bag shrinkage in nor-
mal eyes between 3 months and 6 months after CMR im-
plantation. Therefore, we selected a follow-up of 3 months.
CONCLUSION
No clinically relevant capsular bag shrinkage was ob-
served with a CFER or a CTR, and capsular bag shrinkage
was the same between the two designs. However, these con-
clusions are applicable only to the equator and tension ringsand the hydrophobic acrylic IOL used in our study. Further
examinations are necessary to evaluate the effect of the
CFER or other rings in eyes with severe capsular bag
- VOL 32, OCTOBER 2006 1619

FOLDABLE EQUATOR RING AND CAPSULAR BAG SHRINKAGE
shrinkage (eg, eyes with pseudoexfoliation). Unfortunately,
in these cases, the CMR method cannot be used because of
inadequate pupil dilation. Alternative assessment methods
should be considered to enable further investigations and
improvements to capsular rings because their ability to re-
duce capsular bag shrinkage could prevent IOL dislocationand, therefore, improve postoperative outcomes.
REFERENCES
1. Strenn K, Menapace R, Vass C. Capsular bag shrinkage after implanta-
tion of an open-loop silicone lens and a poly(methyl methacrylate)
capsule tension ring. J Cataract Refract Surg 1997; 23:1543–1547
2. Nagamoto T, Eguchi G. Effect of intraocular lens design on migration
of lens epithelial cells onto the posterior capsule. J Cataract Refract
Surg 1997; 23:866–872
3. Gimbel HV, Sun R. Clinical applications of capsular tension rings in cat-
aract surgery. Ophthalmic Surg Lasers 2002; 33:44–53
4. Gimbel HV, Sun R, Heston JP. Management of zonular dialysis in pha-
coemulsification and IOL implantation using the capsular tension ring.
Ophthalmic Surg Lasers 1997; 28:273–281
5. Sun R, Gimbel HV. In vitro evaluation of the efficacy of the capsular
tension ring for managing zonular dialysis in cataract surgery. Oph-
thalmic Surg Lasers 1998; 29:502–505
6. Menapace R, Findl O, Georgopoulos M, et al. The capsular tension ring:
designs, applications, and techniques. J Cataract Refract Surg 2000;
26:898–912
7. Cionni RJ, Osher RH. Endocapsular ring approach to the subluxed cat-
aractous lens. J Cataract Refract Surg 1995; 21:245–249
8. Cionni RJ, Osher RH. Management of profound zonular dialysis or
weakness with a new endocapsular ring designed for scleral fixation.
J Cataract Refract Surg 1998; 24:1299–1306
J CATARACT REFRACT SURG -1620
9. Nishi O, Nishi K, Menapace R, Akura J. Capsular bending ring to pre-
vent posterior capsule opacification: 2 year follow-up. J Cataract Re-
fract Surg 2001; 27:1359–1365
10. Kurz S, Dick HB. Spring constants of capsular tension rings. J Cataract
Refract Surg 2004; 30:1993–1997
11. Tehrani M, Dick HB, Krummenauer F, et al. Capsule measuring ring to
predict capsular bag diameter and follow its course after foldable
intraocular lens implantation. J Cataract Refract Surg 2003; 29:
2127–2134
12. Apple DJ, Solomon KD, Tetz MR, et al. Posterior capsule opacification.
Surv Ophthalmol 1992; 37:73–116
13. Kurz S, Krummenauer F, Hacker P, et al. Capsular bag shrinkage after
implantation of a capsular bending or capsular tension ring. J Cataract
Refract Surg 2005; 31:1915–1920
14. Tehrani M, Krummenauer F, Blom E, Dick HB. Evaluation of the practi-
cality of optical biometry and applanation of ultrasound in 253 eyes.
J Cataract Refract Surg 2003; 29:741–746
15. Tehrani M, Krummenauer F, Kumar R, Dick HB. Comparison of bio-
metric measurements using partial coherence interferometry and
applanation ultrasound. J Cataract Refract Surg 2003; 29:747–752
16. Vogel A, Dick HB, Krummenauer F. Reproducibility of optical biometry
using partial coherence interferometry; intraobserver and interob-
server reliability. J Cataract Refract Surg 2001; 27:1961–1968
17. Dick HB. Closed foldable capsular rings. J Cataract Refract Surg 2005;
31:467–471
18. Hara T, Hara T, Yamada Y. ‘‘Equator ring’’ for maintenance of the com-
pletely circular contour of the capsular bag equator after cataract re-
moval. Ophthalmic Surg 1991; 22:358–359
19. Hara T, Hara T, Sakanishi K, Yamada Y. Efficacy of equator rings in an
experimental rabbit study. Arch Ophthalmol 1995; 113:1060–1065
20. Nishi O, Nishi K, Mano C, et al. The inhibition of lens epithelial cell mi-
gration by a discontinuous capsular bend created by a band-shaped
circular loop or a capsule-bending ring. Ophthalmic Surg Lasers 1998;
29:119–125
VOL 32, OCTOBER 2006