effect of central venous catheter type on infections: a prospective clinical trial
TRANSCRIPT

Effect of central venous catheter type oninfections: a prospective clinical trialq
B. Richardsa, W. Chaboyerb,*, T. Bladena, P.J. Schluterc
aIntensive Care Unit, Gold Coast Hospital, Southport, Qld, AustraliabFaculty of Nursing and Health, Griffith University, Gold Coast Centre, PMB 50 Gold Coast Mail Centre,Bundall, Qld 9726, AustraliacSchool of Population Health, University of Queensland, Brisbane, Qld, Australia
Received 2 October 2001; accepted 14 January 2003
KEYWORDSCatheterization;
Catheter-related
infection; Central venous
catheter; Bacteraemia;
Nosocomial infection
Summary This study reports on a block clinical trial of two types of central venouscatheters (CVCs): antiseptic-impregnated catheters (AIC) and non-impregnatedcatheters (non-AIC), on catheter tip colonization and bacteraemia. In total, 500catheters were inserted in 390 patients over the 18 month study period, 260 (52.0%)AIC and 240 (48.0%) non-AIC. Of these, 460 (92.0%) tips (237 AIC and 223 non-AIC) werecollected. While significantly fewer AIC, 14 (5.9%), than non-AIC, 30 (13.5%), catheterswere colonized ðP , 0:01Þ; there was no difference in the rates of bacteraemias in thetwo groups (0.8% vs. 2.7%, respectively, P ¼ 0:16). There were 6.87 (95% CI 3.38–14.26) and 16.92 (95% CI 10.61–27.12) colonized AIC and non-AIC catheters,respectively, per 1000 catheter days, a difference that was significant ðP , 0:01Þ:However, no difference emerged between bacteraemias in AIC and non-AIC cathetersper 1000 catheter days measured at 0.98 (95% CI 0.24–5.54) and 3.38 (95% CI 1.29–9.34), respectively (P ¼ 0:10). Of the 444 CVCs that were sited in the subclavian orjugular veins and had tips collected, significantly more catheters were colonized in thejugular group, 19 (20%), compared with the subclavian group, 24 (6.9%; P # 0:01).Overall, the low rates of colonization and bacteraemia may be explained by thepopulation studied, the policies used and the employment of a clinical nurse dedicatedto CVC management.Q 2003 The Hospital Infection Society. Published by Elsevier Science Ltd. All rightsreserved.
Introduction
Central venous catheter (CVC)-related bacteraemiais a common problem in hospitals, with catheter-related sepsis causing excess morbidity,1,2 mortal-
ity3–7 and increasing hospital costs.6,7 Numerousresearchers have attempted to identify practicesthat limit these negative outcomes. Considerationof insertion techniques and personnel,8 –11 main-tenance protocols3,10,12 and catheter type3,13 –16
have been examined. This study reports on aprospective block clinical trial of two types ofCVCs, antiseptic-impregnated catheters (AIC) andnon-impregnated catheters (non-AIC), on cathetertip colonization and bacteraemia. Originally part of
Journal of Hospital Infection (2003) 54, 10–17
www.elsevierhealth.com/journals/jhin
0195-6701/03/$ - see front matter Q 2003 The Hospital Infection Society. Published by Elsevier Science Ltd. All rights reserved.doi:10.1016/S0195-6701(03)00071-9
q This research was conducted at the Gold Coast Hospital,Southport, Queensland, Australia by the authors.
*Corresponding author. Fax: þ61-755-528-526.E-mail address: [email protected]
a larger multi-site study that was never completedandafterdiscussingownershipofdataand recheckingall data, this paper reports on the results from theGold Coast Hospital (GCH), Queensland, Australia,over an 18 month period from 1995 to 1997.
Several studies have demonstrated that AICcatheters result in less bacterial colonization thannon-AIC,13 –21 however, only a few have showncatheter-related bloodstream infection (CR-BSI) tobe diminished.3 Veenstra et al.22 published theresults of their meta-analysis of the efficacy ofantiseptic-impregnated CVC in preventing cathetercolonization and CR-BSI. Pooled results demon-strated significant reductions in catheter coloniza-tion and CR-BSI with the antiseptic-impregnatedgroup. Colonization rates ranged from 1.7 to 39.7%in the treatment catheters and from 13.7 to 71.4%in the control catheters. CR-BSI ranged from 0 to10.5% in the treatment catheters and from 2.1 to11.7% in the control catheters. After pooling thestudies, the odds ratio for colonization was 0.44(95% CI 0.36–0.54) and for CR-BSI was 0.56 (95% OR0.37–0.84). They were not able to identify anytrend towards increasing colonization or CR-BSIwith increasing duration of dwell time. A retro-spective review conducted by Hanley et al.23
identified an association between AIC and reductionin CR-BSI and more recently the Centres for DiseaseControl and Prevention24 recommended that anti-septic or antibiotic impregnated CVCs be used wheninfection rates were high despite implementingother strategies.
The lack of primary evidence at the time ofstarting the present study regarding the effective-ness of AIC versus non-AIC in preventing CR-SBImotivated this study. Thus, clinicians insertingCVCs were making the choice of CVC type basedon an incomplete knowledge of the relative benefitsand risks of each. The apparent advantage ofreduced colonization of AICs needs to be set againstpotential risks. Indeed, some researchers havereported anaphylactic shock as a risk in the use ofAICs.25 –27 Others have reported mechanical failureof the catheters in prolonged use.28 Our hypothesiswas that AIC would have lower rates of tipcolonization and bacteraemia than non-AIC.
Methods
This research was conducted at the GCH, which is a540 bed tertiary referral hospital accommodatingall major specialties except cardiothoracic surgeryand paediatric intensive care. At the time of thestudy, the hospital served a community of approxi-
mately 300 000. Ethical approval was obtained fromthe hospital ethics committee, in compliance withNational Health Medical Research Council guide-lines for research. During the study, writtenconsent by patients was not required because theprocedure was considered standard practice, withdoctors normally choosing the type of catheter tobe inserted. All triple lumen CVCs inserted at thehospital for both ward and intensive care patientsover an 18 month period were included in the trial.A process of block assignment was used, namely allpatients in the first two-month period requiring atriple lumen polyurethane CVC were allocated toreceive an AIC (7 F Arrowgard Blue, impregnatedwith chlorhexidine and silver–sulfadiazine, ArrowInternational Inc., Pennsylvania, USA), and in thenext two months all received a non-AIC (7 Fstandard Arrow International Inc., Pennsylvania,USA). This process continued for the duration of thestudy, which resulted in nine two-month blocks ofeach catheter type. No other CVCs, such ashaemodialysis, single lumen or silicone catheterswere studied. At the end of each two-month block,all remaining stock was removed from the shelvesand replaced with the alternate catheter.
Definitions
Catheter tip colonization was defined as 15 or morecolony forming units identified using the Maki semi-quantitative method for culturing the tip.15 Cath-eter-related bacteraemia was defined as clinicalsuspicion of infection (temperature greater than38.5 8C or signs of localized infection includingredness or pus at the site), and the same organismidentified with same antibiogram grown in bloodculture and catheter tip, with no other sites forsepsis identified by microbiology. This definition forbacteraemia was based on that of Collignon et al.29
and is similar to the more recent definitions byPolderman and Girbes30 and Eggiman and Pittet.31
Procedure
All CVC insertions were completed or supervised byexperienced medical staff according to hospitalpolicy. All CVCs were inserted percutaneously usingthe Seldinger technique. Full barrier precautionswere observed during insertion, including use ofsterile gowns, sterile gloves, masks and largedrapes. Insertion sites were cleansed with singlebottle alcoholic 30% povidine–iodine 10% (Viodine).Adhesive gauze dressings (Primaporee) were usedat all times and changed every 48 h in the IntensiveCare Unit (ICU) and every 72 h in the general wardareas. CVC dressings and line changes were to be
Infections in central venous catheters 11

performed together as a single procedure. If thedressing became wet, loose or soiled, the CVCdressing was changed. Aseptic technique andstandard precautions were maintained during theprocedure. If the CVC was required for more than 10days, a new catheter was inserted at a new site inthe procedure room dedicated for CVC insertions.Rewiring the same site (by placing a new CVC in thesame site by means of a gauze wire) only took placeif no other access was available and because oftheir small numbers ðN ¼ 14; 2:8%Þ; were insufficientto examine their influence on study outcomes. Thenew catheter was of whichever type was used in thecurrent block of the experiment and not necessarilyidentical to the previous catheter used. Thus, asingle patient may have received more than onetype of catheter.
All lines were reviewed three times per week bythe total parenteral nutrition (TPN) clinical nurse toensure compliance with hospital guidelines. Ifparticipants’ temperature rose to 38.58C bloodcultures were collected. If there were signs oflocalized infection (redness or pus) a swab wascollected from the catheter exit site. If thetemperature remained elevated, the CVC wasremoved. Before CVC removal the skin site wascleaned with alcoholic povidine–iodine 10%, andallowed to dry. Using standard precautions and anaseptic procedure the catheter was removed takingcare not to contaminate the tip by contacting withthe skin. While there was no way to eliminate therisk of micro-organisms on the skin contaminatingthe catheter at the time of its removal,32 allindividuals removing catheters were trained andinitially supervised in the activity. After removalsterile adhesive gauze dressing was applied to theexit site and reviewed 24 h later. Approximately5 cm of the distal catheter segment including thetip was cut with sterile scissors or blade, placed in asterile jar for culture, transported to the laboratoryand cultured within 2 h on a non-selective all-purpose medium (sheep blood agar). The standardMaki roll-plate method33 was used and all micro-biology results were checked independently by tworesearch team members. Biochemical testing wasundertaken in the GCH microbiology departmentusing standard culture and identificationtechniques.
Statistical methods
Data were entered into a database designed for thetrial. This was exported to Excel for additional datacleaning to determine out of range and miscodedvalues. The data were then analysed using SPSSWindows version 10.0 (SPSS Inc., Chicago, IL, USA).
Fisher’s exact test and Student’s t-test were usedto compare categorical and continuous groups ofdata, respectively. Poisson regression was used tocalculate the 95% confidence intervals (95% CI) forthe colonization and bacteraemia rates per 1000catheter days. For all statistical comparisons, thesignificance level was taken as a ¼ 0:05:
Results
In total, 500 catheters were inserted in 390 patientsduring the study period, 260 (52.0%) AIC and 240(48.0%) non-AIC. Of these, 460 (92.0%) tips (237 AICand 223 non-AIC) were collected and 40 (8.0%) (23AIC and 17 non-AIC) were missed, respectively. Tipswere lost because of accidental removal and deathwith catheter in situ, however, we were unable todetermine why some other catheter tips were notcollected. Table I summarizes catheter character-istics. There was no significant difference betweenAIC and non-AIC groups for any variable exceptcatheter dwell time, where the AIC group mean of8.4 days was significantly longer than for the non-AIC group mean of 7.8 days ðP ¼ 0:03Þ: In total, thecatheter dwell time was 2188 days in the AIC groupand 1866 days in the non-AIC group. The majority ofthe catheters were placed in the subclavian veinwith very few complications. Approximately one-third of both groups received antibiotics during thestudy.
Table II lists the research outcomes. There wasno difference in the catheter tips used for eachgroup ðP ¼ 0:51Þ: Significantly fewer AIC group tipswere colonized, 14 (5.9%), than non-AIC group tips,30 (13.5%) P , 0:01: After adjusting for the missingtips, the colonization rate per 1000 catheter dayswas 6.87 (95% CI 3.38–14.26) in the AIC groups and16.92 (95% CI 10.61–27.12) in the non-AIC groupðP , 0:01Þ: No such difference emerged betweenthe bacteraemia rates per 1000 days for the AICgroup, 0.98 (95% CI 0.24–5.54), and the non-AICgroup, 3.38 (95% CI 1.29–9.34), P ¼ 0:10: Overall,the rates of colonization and bacteraemia per 1000catheter days were low in both groups.
Further analysis of colonization and bacteraemiawas undertaken to determine whether patientswith multiple catheter insertions or different in situdwell time of catheters had different positiveinfection rates. Table III reveals no statisticalassociation between catheter insertion frequencyand colonization or bacteraemia. This table alsodemonstrates that all instances of bacteraemia andall but one of colonization occurred in cathetersthat had a dwell time of three days or greater.
B. Richards et al.12

Table IV shows the organisms that were identi-fied in the tip and blood cultures. Because some tipsand cultures grew more than one organism, thenumbers represented in the table exceed the totalnumbers of colonizations and bacteraemias.
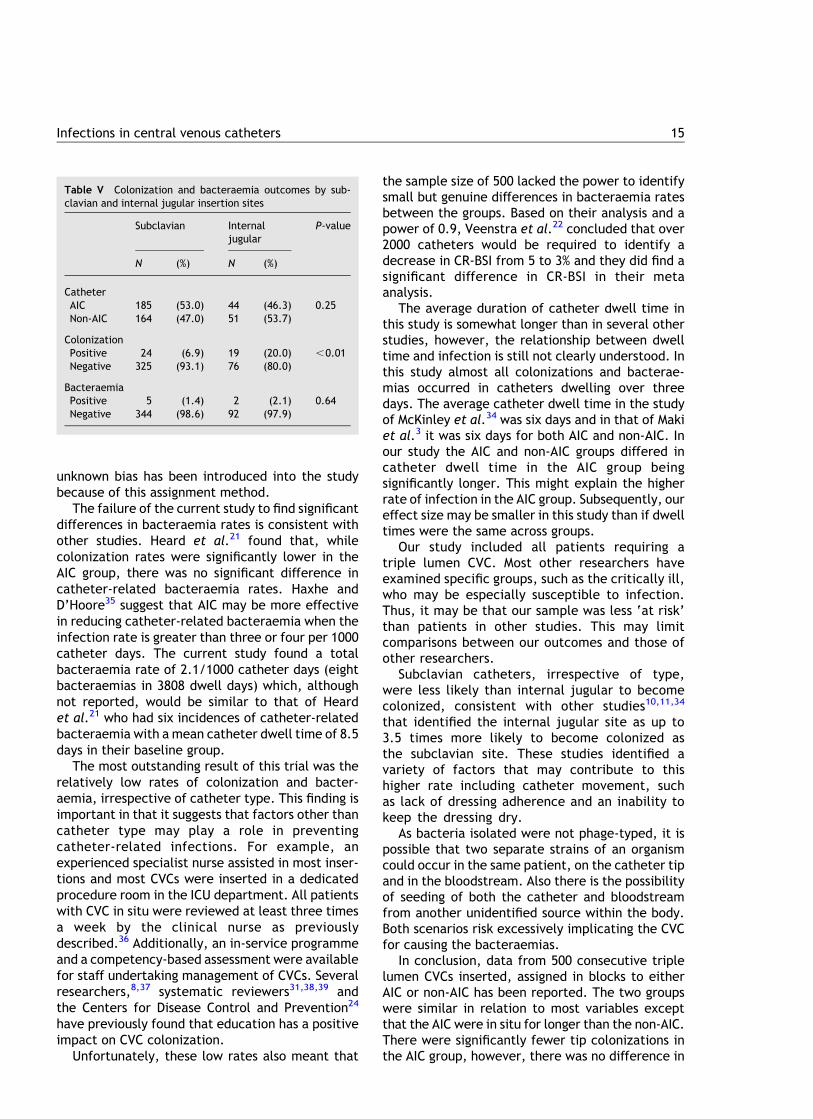
As seen in Table I, most catheters were placed ineither the subclavian, 379 (75.8%), or the jugular,105 (21.0%), vein. Table V compares outcomes forthese two sites. There was no significant differencein the type of catheter used in these two groupsðP ¼ 0:25Þ: Significantly fewer positive catheter tipswere identified in catheters placed in the subcla-vian, 24 (6.9%), than in the internal jugular vein, 19(20.0%), P , 0:01; but there was no difference inbacteraemia-positive results between sites ðP ¼
0:64Þ: After adjusting for missing observations, the
Table I Patient socio-demographic and hospital characteristics overall and compared between antiseptic-impregnated catheters(AIC) and non-impregnated catheters (non-AIC) treatment groups
Total AIC Non-AIC P-value
N x̄ (SD) N x̄ (SD) N x̄ (SD)
Age (years) 486 57.3 (19.5) 254 58.3 (18.7) 232 56.2 (20.3) 0.23APACHE II score on admission 499 14.4 (7.2) 259 14.4 (7.2) 240 14.3 (7.3) 0.81Catheter days 498 8.1 (3.4) 259 8.4 (3.5) 239 7.8 (3.2) 0.03Hospital length of stay (days) 498 27.0 (26.3) 260 28.2 (25.2) 238 25.6 (27.4) 0.25
N (%) N (%) N (%)
SexFemale 198 (39.6) 113 (43.5) 85 (35.4) 0.07Male 302 (60.4) 147 (56.5) 155 (64.6)
Injection siteSubclavian 379 (75.8) 204 (78.5) 175 (72.9) 0.21Internal jugular 105 (21.0) 48 (18.5) 57 (23.8)Femoral 7 (1.4) 2 (0.8) 5 (2.1)Other 9 (1.8) 6 (2.3) 3 (1.3)
Complications during insertionYes 9 (1.8) 4 (1.5) 5 (2.1) 0.74No 491 (98.2) 256 (98.5) 235 (97.9)
Antibiotics used during studyYes 182 (36.4) 96 (36.9) 86 (35.8) 0.85No 318 (63.6) 164 (63.1) 154 (64.2)
Number of catheter insertions1 390 (78.0) 197 (75.8) 193 (80.4) 0.24$ 2 110 (22.0) 63 (24.2) 47 (19.6)
Number of catheters rewiredp at the same site0 486 (97.2) 250 (96.2) 236 (98.3) 0.18$ 1 14 (2.8) 10 (3.8) 4 (1.7)
Highest temperature (8C), 38.5 463 (92.6) 239 (91.9) 224 (93.3) 0.61$ 38.5 37 (7.4) 21 (8.1) 16 (6.7)
Highest rise in white blood cells, 5000 492 (98.6) 258 (99.2) 234 (97.9) 0.27$ 5000 7 (1.4) 2 (0.8) 5 (2.1)
p Rewired ¼ placing a new catheter in the same site by means of a gauze wire.
Table II Outcomes for catheters with collected tips com-pared between AIC and non-AIC treatment groups
Total AIC Non-AIC P-value
N (%) N (%) N (%)
Catheters tips available for collectionYes 460 (92.0) 237 (91.2) 223 (92.9) 0.51No 40 (8.0) 23 (8.8) 17 (7.1)
Catheter tip colonizationPositive 44 (9.6) 14 (5.9) 30 (13.5) ,0.01Negative 416 (90.4) 223 (94.1) 193 (86.5)
BacteraemiaPositive 8 (1.7) 2 (0.8) 6 (2.7) 0.16Negative 452 (98.3) 235 (99.2) 217 (97.3)
Infections in central venous catheters 13

colonization rate per 1000 catheter days was 8.13(95% CI 4.21–15.94) in the subclavian site and 25.71(95% CI 17.56–37.74) in the internal jugular vein, adifference that was statistically significant ðP ,
0:01Þ: No such difference emerged between thebacteraemia rates per 1000 days for the subclavian,1.69 (95% CI 0.49–6.74), and internal jugulargroupings, 2.71 (95% CI 0.94–8.32), P ¼ 0:59:
Patients with a definite CVC-related bacteraemiarequired a total of 26 and 68 days of antibiotictherapy in the AIC and non-AIC groups, respectively.No patient required a second course of therapy.
Discussion
In this study of 500 CVCs, complete data wereavailable for 460 catheters, 237 AIC and 223 non-AIC. Forty (8%) were missed for a number of reasonsand this compares favourably to other publishedstudies.3,34 While this loss of tips for follow-up is alimitation, excluding those when patients had died,it is possible that there may have been a bias
towards collecting tips from patients with possibleinfections. The majority (33 out of 40) of thesemissed tips occurred in the first 200 cathetersinserted, thus it may be that it took staff a while toadhere to the study protocol. Further, 10 missedtips occurred in patients who had died. How thesemissing data may have affected the results of thisstudy is not known. Assuming all lost tips wouldhave cultured positively, the addition of 23 AIC tipsand 17 non-AIC tips would bring the AIC colonizationrate to 14.2% (37/260) and non-AIC rate to 19.6%(47/240).
All hospital patients requiring triple lumen CVCsduring the 18 months of the study were included inthe research. Catheters in place for more than aweek on average indicating that these catheterswere not simply used emergency treatments orperioperative therapies. A limitation of this studywas that catheters were assigned in blocks becauseof practicality. A central randomization service wasnot available and other methods of randomizationwere not feasible due to number of doctors involvedin inserting the lines. However, it may be that some
Table III Relationship between catheter colonization and bacteraemia and the number of insertions and the length of time in situ
Catheter insertions Time catheter in situ
1 $2 P-value ,3 days $3 days P-value
N (%) N (%) N (%) N (%)
ColonizationPositive 33 (9.2) 11 (10.9) 0.57 1 (5.9) 43 (9.7) 1.00Negative 326 (90.8) 90 (89.1) 16 (94.1) 399 (90.3)
BacteraemiaPositive 7 (1.9) 1 (1.0) 1.00 0 (0.0) 8 (1.8) 1.00Negative 352 (98.1) 100 (99.0) 17 (100.0) 434 (98.2)
Table IV Organisms identified in tip and blood culture
Organism Tip culturep Blood culturep
AIC Non-AIC AIC Non-AIC
Staphylococcus epidermidis 10 18 1 1Staphylococcus aureus (MSSA) 1 5 4Methicillin-resistant Staphylococcus aureus (MRSA) 6 1Rifampin-resistant Staphylococcus aureus (RRSA) 3 1Staphylococcus haemolyticus 1 5Candida species 2 1Enterococcus faecalis 2 1Pseudomonas aeruginosa 2 1Staphylococcus capitis 1 1Staphylococcus hominis 1 1Enterobacter cloacae 1Klebsiella species 1
p Some cultures grew more than one organism.
B. Richards et al.14
unknown bias has been introduced into the studybecause of this assignment method.
The failure of the current study to find significantdifferences in bacteraemia rates is consistent withother studies. Heard et al.21 found that, whilecolonization rates were significantly lower in theAIC group, there was no significant difference incatheter-related bacteraemia rates. Haxhe andD’Hoore35 suggest that AIC may be more effectivein reducing catheter-related bacteraemia when theinfection rate is greater than three or four per 1000catheter days. The current study found a totalbacteraemia rate of 2.1/1000 catheter days (eightbacteraemias in 3808 dwell days) which, althoughnot reported, would be similar to that of Heardet al.21 who had six incidences of catheter-relatedbacteraemia with a mean catheter dwell time of 8.5days in their baseline group.
The most outstanding result of this trial was therelatively low rates of colonization and bacter-aemia, irrespective of catheter type. This finding isimportant in that it suggests that factors other thancatheter type may play a role in preventingcatheter-related infections. For example, anexperienced specialist nurse assisted in most inser-tions and most CVCs were inserted in a dedicatedprocedure room in the ICU department. All patientswith CVC in situ were reviewed at least three timesa week by the clinical nurse as previouslydescribed.36 Additionally, an in-service programmeand a competency-based assessment were availablefor staff undertaking management of CVCs. Severalresearchers,8,37 systematic reviewers31,38,39 andthe Centers for Disease Control and Prevention24
have previously found that education has a positiveimpact on CVC colonization.
Unfortunately, these low rates also meant that
the sample size of 500 lacked the power to identifysmall but genuine differences in bacteraemia ratesbetween the groups. Based on their analysis and apower of 0.9, Veenstra et al.22 concluded that over2000 catheters would be required to identify adecrease in CR-BSI from 5 to 3% and they did find asignificant difference in CR-BSI in their metaanalysis.
The average duration of catheter dwell time inthis study is somewhat longer than in several otherstudies, however, the relationship between dwelltime and infection is still not clearly understood. Inthis study almost all colonizations and bacterae-mias occurred in catheters dwelling over threedays. The average catheter dwell time in the studyof McKinley et al.34 was six days and in that of Makiet al.3 it was six days for both AIC and non-AIC. Inour study the AIC and non-AIC groups differed incatheter dwell time in the AIC group beingsignificantly longer. This might explain the higherrate of infection in the AIC group. Subsequently, oureffect size may be smaller in this study than if dwelltimes were the same across groups.
Our study included all patients requiring atriple lumen CVC. Most other researchers haveexamined specific groups, such as the critically ill,who may be especially susceptible to infection.Thus, it may be that our sample was less ‘at risk’than patients in other studies. This may limitcomparisons between our outcomes and those ofother researchers.
Subclavian catheters, irrespective of type,were less likely than internal jugular to becomecolonized, consistent with other studies10,11,34
that identified the internal jugular site as up to3.5 times more likely to become colonized asthe subclavian site. These studies identified avariety of factors that may contribute to thishigher rate including catheter movement, suchas lack of dressing adherence and an inability tokeep the dressing dry.
As bacteria isolated were not phage-typed, it ispossible that two separate strains of an organismcould occur in the same patient, on the catheter tipand in the bloodstream. Also there is the possibilityof seeding of both the catheter and bloodstreamfrom another unidentified source within the body.Both scenarios risk excessively implicating the CVCfor causing the bacteraemias.
In conclusion, data from 500 consecutive triplelumen CVCs inserted, assigned in blocks to eitherAIC or non-AIC has been reported. The two groupswere similar in relation to most variables exceptthat the AIC were in situ for longer than the non-AIC.There were significantly fewer tip colonizations inthe AIC group, however, there was no difference in
Table V Colonization and bacteraemia outcomes by sub-clavian and internal jugular insertion sites
Subclavian Internaljugular
P-value
N (%) N (%)
CatheterAIC 185 (53.0) 44 (46.3) 0.25Non-AIC 164 (47.0) 51 (53.7)
ColonizationPositive 24 (6.9) 19 (20.0) ,0.01Negative 325 (93.1) 76 (80.0)
BacteraemiaPositive 5 (1.4) 2 (2.1) 0.64Negative 344 (98.6) 92 (97.9)
Infections in central venous catheters 15

the proportion of each group who developed localsepsis or bacteraemia. Given this finding, thedecision to utilize AICs must be balanced againstthe potential risks associated with their use.
Acknowledgements
We gratefully acknowledge the work of Dr Colligonin planning the multi-site study and in the adviceprovided during the course of data collection. Weare grateful for the advice of Dr Renu Vohra of theMicrobiology Department, GCH. We acknowledgethe support of three Research Assistants, MandyTallot, Trish Richards and Julia McCann.
References
1. Pinilla JC, Ross DF, Martin T, Crump H. Study of the incidenceof intravascular catheter infection and associated septi-cemia in critically ill patients. Crit Care Med 1983;11:21—25.
2. Collignon PJ. Intravascular catheter associated sepsis: acommon problem. Med J Aust 1994;161:374—378.
3. Maki DG, Stolz SM, Wheeler S, Mermel LA. Prevention ofcentral venous catheter-related bloodstream infection byuse of an antiseptic-impregnated catheter a randomizedcontrolled trial. Ann Intern Med 1997;127:257—266.
4. Pearson ML. Guidelines for prevention of intravasculardevice-related infections. Am J Infect Control 1996;24:262—293.
5. Pittet D, Tarara D, Wenzel RP. Nosocomial bloodstreaminfections in critically ill patients. JAMA 1994;271:1598—1601.
6. Wenzel RP. Perspective: attributable morality—the promiseof better antimicrobial therapy. J Infect Dis 1998;178:917—919.
7. Farr BM. Understaffing: a risk factor for infection in the eraof downsizing? Infect Control Hosp Epidemiol 1996;17:147—149.
8. Parras F, Ena J, Bouza E, et al. Impact of an educationalprogram for the prevention of colonization of intravascularcatheters. Infect Control Hosp Epidemiol 1994;15:239—242.
9. Ena J, Cercenado E, Martinez D, Bouza E. Cross-sectionalepidemiology of phlebitis and catheter-related infections.Infect Control Hosp Epidemiol 1992;13:15—20.
10. Ricket H, Hubert B, Nitemberg G, et al. Prospective multi-center study of vascular-catheter-related complications andrisk factors for positive central-catheter cultures in inten-sive care unit patients. J Clin Microbiol 1990;28:2520—2525.
11. Moro ML, Vigano EF, Cozzi Lepri A. Risk factors for centralvenous catheter-related infections in surgical and intensivecare units. The Central Venous Catheter-Related InfectionStudy Group. Infect Control Hosp Epidemiol 1994;15:253—264.
12. Hoffman KK, Weber DJ, Samsa GP, Rutala WA. Transparentpolyurethane film as an intravenous catheter dressing. Ameta-analysis of the infection risks. JAMA 1992;267:2072—2076.
13. Hannan M, Juste RN, Umasanker S. Antiseptic-bonded
central venous catheters and bacterial colonisation. Anaes-thesia 1999;54:868—872.
14. Loo S, van Heerden PV, Golleege CV, Roberts BL, Power BM.Infection in central lines: antiseptic-impregnated vs. stan-dard non-impregnated catheters. Anaesth Intens Care 1997;25:637—639.
15. Sheng WH, Ko WJ, Wang JT, Chang SC, Hsueh PR, Luh KT.Evaluation of antiseptic-impregnated central venous cath-eters for prevention of catheter-related infection in inten-sive care unit patients. Diagn Microbiol Infect Dis 2000;38:1—5.
16. Logghe C, Van-Ossel C, D’Hoore W, Ezzedine H, Wauters G,Haxhe JJ. Evaluation of chlorhexidine and silver-sulfadiazineimpregnated central venous catheters for prevention ofbloodstream infection in leukaemic patients: a randomizedcontrolled trial. J Hosp Infect 1997;37:145—156.
17. Tacconelle E, Tumbarello M, Cauda R. Central venouscatheters and bloodstream infection. JAMA 2000;283:478—479.
18. Tennenberg S, Lieser M, McCurdy B, et al. A prospectiverandomized trial of an antibiotic- and antiseptic-coatedcentral venous catheter in the prevention of catheter-related infections. Arch Surg 1997;132:1348—1351.
19. Collin GR. Decreasing catheter colonization through the useof antiseptic-impregnated catheter: a continuous qualityimprovement project. Chest 1999;115:1632—1640.
20. George SJ, Vuddamalay P, Boscoe MJ. Antiseptic-impreg-nated central venous catheters reduce the incidence ofbacterial colonization and associated infection in immuno-compromised transplant patients. Eur J Anaesthesiol 1997;14:428—431.
21. Heard SO, Wagle M, Vijayakumar E, et al. Influence of triplelumen central venous catheters coated with chlorhexidineand silver sulfadiazine on the incidence of catheter-relatedbacteraemia. Arch Int Med 1998;158:81—87.
22. Veenstra DL, Saint S, Saha S, et al. Efficacy of antiseptic-impregnated central venous catheters in preventingcatheter-related bloodstream infection a meta-analysis.JAMA 1999;28:261—267.
23. Hanley EM, Veeder A, Smith T, et al. Evaluation of anantiseptic triple-lumen catheter in an intensive care unit.Crit Care Med 2000;28:366—370.
24. O’Grady NP, Alexander M, Dellinger EP, et al. Guidelines forthe prevention of intravascular catheter-related infections.Centers for Disease Control and Prevention. MMWR RecommRep 2000;9(5RR-10):1—29.
25. Oda T, Hamasaki J, Kanda N, Mikami K. Anaphylactic shockinduced by an antiseptic-coated central venous catheter.Anaesthesiology 1997;87:1242—1244.
26. Terazawa E, Shimonaka H, Nagase K, Masue T, Dohi S. Severeanaphylactic reaction due to a chlorhexidine-impregnatedcentral venous catheter. Anaesthesiology 1998;89:1296—1298.
27. Stephens R, Mythen M, Kallis P, et al. Two episodes of life-threatening anaphylaxis in the same patient to a chlor-hexidine-sulfadiazine-coated central venous catheter. Br JAnaesth 2001;87:306—308.
28. Ellis ME, Rhydderch D, Zwaan F, Guy ML, Baillie F. Highincidence of line-related infection and mechanical failure ofan antiseptic-impregnated central venous catheter in highlyimmunocompromised patients. Scand J Infect Dis 1996;28:91—93.
29. Collignon PJ, Munro R, Sorrell TC. Systematic sepsis andintravenous devices. A prospective survey. Med J Aust 1984;141:345—348.
30. Polderman KH, Girbes ARJ. Central venous catheter use Part
B. Richards et al.16

2: infectious complications. Intens Care Med 2002;28:18—28.
31. Eggimann P, Pittet D. Overview of catheter-related infec-tions with special emphasis on prevention based oneducational programs. Clin Microbiol Infect 2002;8:295—309.
32. Egebo K, Toft P, Jakobsen CJ. Contamination of centralvenous catheters. The skin insertion wound is a major sourceof contamination. J Hosp Infect 1996;32:99—104.
33. Maki DG, Weise CE, Sarafin IIW. A semiquantitative culturemethod for identifying intravenous-catheter-related infec-tion. N Engl J Med 1977;296:1305—1309.
34. McKinley S, Mackenzie A, Finfer S, et al. Incidence andpredictors of central venous catheter-related infection inintensive care patients. Anaesth Intens Care 1999;27:164—169.
35. Haxhe JJ, D’Hoore W. A meta-analysis dealing with theeffectiveness of chlorhexidine and silver-sulfadiazine-impregnated central venous catheters. J Hosp Infect 1998;40:166—168.
36. Jansen D. The impact of a clinical nurses’ role on CVCinfections and bacteremia a two year comparative, retro-spective study. Aus Nurs J 1994;1:22—25.
37. Coopersmith CM, Rebmann TL, Zack JE, et al. Effect of aneducation program on decreasing catheter-related blood-stream infections in the surgical intensive care unit. CritCare Med 2002;30:59—64.
38. O’Grady NP. Applying the science to the prevention ofcatheter-related infections. J Crit Care 2002;17:114—121.
39. Frankel DJ, Rickard C, Lipman J. Can we achieve consensuson central venous catheter-related infections? AnaesthIntens Care 2000;28:475—490.
Infections in central venous catheters 17