effect of concomitant ingestion of alcohol on the in vivo pharmacokinetics of kadian (morphine...
TRANSCRIPT
EPE
FA
AiDathD
R2SAp01©d
The Journal of Pain, Vol 9, No 4 (April), 2008: pp 330-336Available online at www.sciencedirect.com
3
ffect of Concomitant Ingestion of Alcohol on the In Vivoharmacokinetics of KADIAN (Morphine Sulfatextended-Release) Capsules
ranklin Johnson, George Wagner, Stephen Sun, and Joseph Staufferlpharma Pharmaceuticals LLC, Piscataway, New Jersey.
Abstract: The recent withdrawal of hydromorphone hydrochloride extended-release capsules (Pal-ladone; Purdue Pharma L.P., Stamford, CT) from the market after pharmacokinetic data revealed a riskof alcohol-induced dose-dumping prompted a re-examination of the risk-benefit profiles of extended-release drugs. Although warnings on concomitant alcohol use are included on opioid product labels,further investigations of extended-release formulations to determine the risk of dose-dumping wererecommended by the US Food and Drug Administration. The present study was undertaken to assessthe single-dose relative bioavailability of polymer-coated, extended-release morphine sulfate cap-sules (KADIAN, 100 mg; Alpharma Pharmaceuticals LLC, Piscataway, NJ). This open-label, randomized,3-way crossover study with an additional index arm, conducted among 32 healthy male volunteers,found no significant evidence of a formulation interaction between KADIAN and alcohol, in vivo. Thepharmacokinetics of serum morphine did not differ significantly among subjects taking KADIAN withwater (fasted) or with 240 mL 40% alcohol under fasted or fed conditions. Analysis of variance ratiosof least-squares means for ln-transformed AUC� and Cmax satisfied the criteria (90% confidenceintervals within 80%–125%) to declare no drug formulation interaction among the KADIAN regimensdosed with alcohol compared with KADIAN taken with water. There were no serious adverse eventsor deaths reported during the study.Perspective: Because of the high rate of alcohol use in the United States, the potential for drug-alcohol interactions is an important clinical concern. Although it is recommended that alcohol not beused while the patient is taking opioids, results of this in vivo study indicate that the risk of alcohol-induced dose-dumping in connection with the use of KADIAN is negligible.
© 2008 by the American Pain Society
Key words: KADIAN, opioid, morphine sulfate extended-release, alcohol, naltrexone, pharmacokinetics.cwdbtget
t1ecptg
lcohol enhances the effects of opioids on the cen-tral nervous system (CNS), and even moderatedrinking may pose a risk of potential drug-drug
nteraction.20 Results of the 2005 National Survey onrug Use and Health indicate a high rate of alcohol usemong Americans. Sixty-seven percent of those aged 21o 25 years, and nearly half of those aged 60 to 64 years,ad consumed alcohol in the previous month.13 Therug Abuse Warning Network (DAWN) reported that
eceived June 6, 2007; Revised November 1, 2007; Accepted November 9,007.upported by Alpharma Pharmaceuticals LLC, Piscataway, New Jersey.ddress reprint requests to Franklin Johnson, Clinical Pharmacology, Al-harma Pharmaceuticals LLC, 1 New England Avenue, Piscataway, NJ8854. E-mail: [email protected]/$34.002008 by the American Pain Society
toi:10.1016/j.jpain.2007.11.009
30
oncomitant use of alcohol and pharmaceuticals, with orithout other illicit drugs, accounted for 13.5% of totalrug-related emergency room visits in 2005.12 The possi-ility of concomitant use of alcohol with pain medica-ion, including opioids, is a reasonable concern. The dan-ers of concomitant consumption of alcohol andxtended-release opioids have recently attracted atten-ion in the scientific and regulatory arenas.Extended-release formulations contain enough opioid
o provide analgesia over the dosing interval, generally2 to 24 hours. There are several strategies used in creatingxtended-release tablets and capsules. Tablet formulationsontain opioid enmeshed within a matrix consisting ofolymers that are hydrophobic, hydrophilic, or combina-ions of more than 1 type of polymer.7-11 On tablet in-estion, the hydrophilic polymer swells in the gastroin-
estinal (GI) fluid. Drug release can be controlled by the
rotfmbas
cidrmIl
tarfrt4pwpp4vhhm
trtctorPaewtSfEobu
dccaw
M
O
dds
P
v2wsoosw(adalopdsnswre
S
P4Kipcf
opobdro2m
R
f
331ORIGINAL REPORT/Johnson et al
ates of diffusion of liquid into the tablet and diffusionf drug into the system, or by the partition coefficients ofhe drug between the 2 polymer types.7,9,11 Some tabletormulations may use 2 types of hydrophobic polymeratrices, which enable dual control: One component cane released immediately upon contact with GI fluids, and
sustained-release component can be released bylower diffusion through the matrix pores.10,11
Capsule formulations adsorb morphine onto an inertore bead, which is then enclosed within a polymer coat-ng. The chemistry of the polymer (hydrophobicity, pHependence) surrounding each bead controls the rate ofelease of active drug.1,3,4,19 One formulation uses fu-aric acid as an osmotic agent and local pH modifier.
nclusion of beads that are not enclosed within a rate-imiting polymer produces immediate-release beads.2
After a pharmacokinetic (PK) study in healthy volun-eers indicated a potentially fatal interaction betweenlcohol and hydromorphone hydrochloride extended-elease capsules (Palladone; Purdue Pharma L.P., Stam-ord, CT), the US Food and Drug Administration (FDA)equested the removal of this opioid from the market. Inhe study, co-ingestion of Palladone with 240 mL (8 oz) of0% (80 proof) alcohol raised peak plasma hydromor-hone concentrations approximately 6-fold, comparedith ingestion with water. One subject in this study ex-erienced a 16-fold increase in peak plasma hydromor-hone concentrations after ingesting Palladone with0% alcohol compared with water.19 Of interest, the inivo PK study showed that lower concentrations of alco-ol, eg, a mixed drink (20% alcohol) or beer (4% alco-ol), also led to potentially serious increases in hydro-orphone concentrations.14
After the withdrawal of Palladone from the market,he FDA recommended that makers of other extended-elease formulations conduct investigations to determinehe risk of alcohol-induced dose-dumping, whereby al-ohol interacts with the extended-release characteristicso yield unintended, rapid drug release in a short periodf time.6,14 In vitro studies conducted with an extended-elease formulation of morphine sulfate (AVINZA; Kingharmaceuticals, Inc., Bristol, TN) demonstrated acceler-ted release of morphine in buffer solutions containingthanol. As a result, the AVINZA label was revised toarn against consumption of alcohol and use of medica-
ions containing alcohol while taking the product.2,5
imilar information was placed as a Black Box Warningor extended-release oxymorphone hydrochloride (OPANAR; Endo Pharmaceuticals, Chadds Ford, PA) due to resultsf an in vivo study examining the effect of alcohol on theioavailability of a single 40-mg dose in healthy fasted vol-nteers.8
The current study was conducted to assess the single-ose bioavailability of morphine sulfate extended-releaseapsules (KADIAN; Alpharma Pharmaceuticals LLC, Pis-ataway, NJ) when dosed with alcohol in the fastednd fed conditions relative to KADIAN administered
ith water.aterials and Methods
bjectiveThe objective of this study was to compare the single-ose relative bioavailability of KADIAN (100 mg) whenosed with alcohol under fasted and fed conditions ver-us water.
articipantsParticipants were opioid-naive, healthy, adult male
olunteers (N � 32) with a mean age of 24 years (range,1–37 years). To be eligible for participation, subjectsere required to have a history of moderate alcohol con-
umption, operationally defined as at least 7 to 21 unitsf alcohol per week, with 1 alcohol unit equivalent to 12z of beer or 1.5 oz of 80-proof (40% alcohol) distilledpirits. The inclusion criteria also specified that subjectsere nonsmokers for at least 3 months or light smokers
�10 pack-years), were within 20% of their ideal weight,nd had no clinically significant laboratory abnormalitiesuring screening. Exclusion criteria included history oflcoholism or drug abuse; history of no alcohol intake;ess than moderate, or excessive alcohol intake; historyr presence of significant cardiovascular, pulmonary, he-atic, renal, hematologic, GI, endocrine, immunologic,ermatologic, neurologic, or psychiatric disease; hyper-ensitivity to morphine, other opioids, or opioid antago-ists; and other physical or laboratory abnormalities con-idered clinically significant. The protocol for this studyas approved by the MDS Pharma Services institutional
eview board, and informed consent was obtained fromach participant.
tudy DesignThis was an open-label, single-dose, 3-way crossover
K drug interaction study between 100 mg KADIAN and0% alcohol in the fasted and fed conditions and 100 mgADIAN with water administered in a randomized fash-
on. Pharmacokinetics of an immediate-release mor-hine oral solution (20 mg) without alcohol in the fastedondition, as an index arm, were explored during theourth period.Typically, subjects enrolled in PK studies are healthy,pioid-naive, adult volunteers. As such, it is commonractice to provide 1 or more oral administrations of thepioid receptor antagonist, naltrexone hydrochloride,efore dosing with an opioid to attenuate opioid-in-uced adverse events (AEs), in particular, vomiting andespiratory depression. Therefore, in this study, naltrex-ne hydrochloride (50 mg tablet) was administered with40 mL of water at 12 hours and 2 hours before treat-ent.
egimensSubjects were randomly assigned to begin with 1 of the
ollowing regimens:● Regimen A: KADIAN 100 mg � 240 mL 40% alcohol
(four 60-mL shots of 40% [80-proof] alcohol [101 mL

t
f
P
tubhcitawc
sCimmr
afa9s1as
P
m
idtlutrelomfifve
S
tecdewevmptrAcTt8
S
Apa
R
uy
332 Effect of Alcohol on Pharmacokinetics of KADIAN
190-proof Everclear (Luxco, St. Louis, MO), 139 mLwater]) under fasted conditions
● Regimen B: KADIAN 100 mg � 240 mL 40% alcohol(four 60-mL shots of 40% [80-proof] alcohol) imme-diately after ingestion of a standard FDA high-fatmeal
● Regimen C: KADIAN 100 mg � 240 mL water underfasted conditions
Subjects were required to consume all alcohol (or wa-er) within 20 minutes of dosing.All subjects who completed the study then received the
ollowing regimen during period 4:● Regimen D: Concentrated oral morphine solution
(20 mg/5 mL) 5 mL � 235 mL water under fastedconditions
roceduresSubjects assigned to regimens A, B, or C were housed at
he study center from at least 15 hours before dosingntil 36 hours after dosing. They returned for a 48-hourlood sample. Subjects assigned to regimen D wereoused until completion of the 24-hour blood sample. Atheck-in, each subject was screened for alcohol and var-ous controlled substances. In addition, serum aspartateransaminase, serum alanine transaminase, and serummylase assessments were repeated at each check-in,hereas hemoglobin and hematocrit were assessed at
heck-in for subjects in regimens C and D.All subjects were fed according to a standardized meal
chedule. For those undergoing the fasted regimens (A,, and D), food was restricted from 10 hours before dos-
ng until 4 hours after dosing. Subjects assigned to regi-en B consumed a standard high-fat breakfast within 30inutes before dosing. A 7-day washout period sepa-
ated each regimen.Pharmacokinetic blood sampling (ie, serum morphine
nd metabolites) took place before dosing and at theollowing time intervals after dosing for regimens A, B,nd C: 0.33, 0.67, 1.0, 1.5, 2.0, 2.5, 3.0, 4.0, 6.0, 7.0, 8.0,.0, 10, 12, 18, 24, 36, and 48 hours. For regimen D, bloodamples were collected before dosing and at 0.33, 0.67,.0, 1.5, 2.0, 2.5, 3.0, 4.0, 6.0, 8.0, 10, 12, and 24 hoursfter dosing. An overview of the study design is pre-ented in Fig 1.
harmacokinetic AnalysesPharmacokinetic measurements for serum morphine,orphine-3-glucuronide, and morphine-6-glucuronide
Figure 1. Stud
ncluded the following parameters: AUC0-t, the area un-er the serum concentration versus time curve, fromime 0 to the last measurable concentration, as calcu-ated by the linear trapezoidal method; AUC�, the areander the serum concentration versus time curve fromime 0 to infinity, calculated as the sum of AUC0-t plus theatio of the last measurable serum concentration to thelimination rate constant; percentage of AUC extrapo-ated; Cmax, the maximum measured serum concentrationver the time span specified; Tmax, the time of the maxi-um measured serum concentration; kel, the apparentrst-order terminal elimination rate constant calculated
rom a semilogarithmic plot of the serum concentrationersus time curve; and t½, the apparent first-order terminallimination half-life calculated as 0.693/kel.
tatistical AnalysesAnalyses of variance (ANOVA) were performed on
he ln-transformed AUC0-t, AUC�, and Cmax PK param-ters for regimens A, B, and C. Each ANOVA includedalculation of ratios of least-squares means (LSMs), theifferences between regimen LSMs, and the standardrror associated with these differences. LSMs ratiosere expressed as a percentage relative to the refer-nce regimen (C). The comparisons of interest were Aersus C and B versus C. In addition, A versus D (the oralorphine solution) was compared for investigational
urposes. Ninety percent confidence intervals (CIs) forhe ratios of the LSMs of regimens A and B, relative toegimen C, were calculated from the ln-transformedUC� and Cmax data. Calculation of these 90% CIs was
onsistent with the statistical test for bioequivalence.raditional criteria for bioequivalence recommendhat ratios for AUC� and Cmax fall within the limits of0% to 125%.16-18
afety AssessmentsSafety and tolerability were assessed by monitoringEs, clinical laboratory results, vital signs, ECGs, andhysical examinations. In addition, alcohol blood testsnd alcohol breath tests were performed.
esultsThe study population consisted of 32 adult male vol-nteers, with a mean age of 24 years (range, 21–37ears), mean height of 182 cm (range, 168 –193 cm),
y design.

atpnpsfitdgas
P
aTo(rthodr
iditc
yavrtwdciw
dp
cesis
KdBfdKi
sPashBari
AfrwfpstCnsn1ivj
Fe
Ff
333ORIGINAL REPORT/Johnson et al
nd mean weight of 81.0 kg (range, 70.8 –99.8 kg). Ofhe 32 subjects enrolled in the study, PK analyses wereerformed on data from 27 subjects, as 5 subjects didot complete at least 2 study periods enabling a com-arison either of regimens A versus C or B versus C. Oneubject was included in the PK analysis but excludedrom the ANOVA because of a protocol deviation (reg-men C was not administered). Seven subjects discon-inued the study, 5 due to AEs (3 due to vomiting, 1ue to chest pain, and 1 due to streptococcal pharyn-itis), 1 due to a positive urine drug screen for amphet-mines, and 1 who withdrew from the study beforetarting regimen D.
harmacokinetic ResultsMean serum morphine concentration-time profiles for
ll subjects with evaluable data are illustrated in Fig 2.he serum morphine profile after coadministrationf regimens A (KADIAN � 40% alcohol fasted) or BKADIAN � 40% alcohol fed) was comparable to the se-um morphine profile after regimen C (KADIAN � wa-er). Peak absorption was reached at a median Tmax of 8ours after dosing for all 3 regimens. The serum profilef regimen D (oral morphine solution, 20 mg) is alsoisplayed in Fig 2 for visual comparison with the extended-elease morphine time-release profiles.The FDA Guidance for Industry regarding bioavailabil-
ty and bioequivalence studies for orally administeredrugs recommends that data from subjects taking mod-
fied-release products who experience vomiting at anyime during the dosing interval (12 hours for KADIAN)an be excluded from statistical analyses.17
Eleven subjects who were included in the overall anal-sis vomited at times ranging from 0.17 to 11.85 hoursfter administration of regimen A. Five of them alsoomited after administration of regimen B, at timesanging from 0.08 to 7.85 hours. No subject vomited af-er taking regimen C, with the exception of 1 subjectho vomited but also had strep throat and was with-rawn from the study. The mean serum morphine con-entration-time profile for the group of subjects exclud-ng those who had vomited within 12 hours of dosing
igure 2. Mean serum morphine concentration-time profilesor all subjects with evaluable data.
as similar to the group that included all subjects. Fig 3 v
isplays the mean serum morphine concentration-timerofiles for these subjects.Both profiles demonstrate that the extended-release
haracteristics of KADIAN were maintained in the pres-nce of alcohol. A summary of the PK parameters for allubjects with evaluable data, as well as the group exclud-ng patients who had vomited within 12 hours, is pre-ented in Table 1.Overall mean exposure (AUC) was similar between theADIAN regimens (A, B, and C), and to regimen D whenose-normalized to 100 mg. Mean Cmax for regimens A,, and C were similar and were approximately one-ourth of the dose-normalized Cmax for regimen D. Me-ian Tmax was 8.0 hours (range, 2.5 to 18 hours) for all 3ADIAN regimens. The mean t½ for KADIAN was approx-
mately 11 hours.The ANOVA ratios of LSMs for AUC and Cmax are pre-
ented in Table 2. This table includes all subjects who hadK data for a comparison of interest, either regimens A/Cnd/or regimens B/C (n � 26 for all subjects; n � 21 for allubjects excluding those who vomited within the 12-our dosing interval). Comparisons of regimens A/C and/C 90% CIs for the ratio of geometric means for AUC�
nd Cmax were within the 80% to 125% acceptanceange for CI boundaries to declare no drug formulationnteraction.
In addition, individual subject Cmax ratios of regimens/C versus B/C were calculated. The ratios were similar
or most subjects. This trend is depicted in Fig 4. Cmax
atios ranged from 0.43 to 1.89 (overall median, 1.00),ith the exception of 1 subject whose Cmax ratio was 4.54
or regimen A versus C. For this subject, the serum mor-hine concentration-time profile after regimen A stillhowed a time-release pattern consistent with an ex-ended-release formulation. The Tmax was 6 hours, and
max was approximately 42% lower than the dose-ormalized mean Cmax for regimen D (oral morphineolution), which suggests the extended-release mecha-ism of KADIAN was not affected. The data also includesubject who did not consume the fourth shot of alcohol
n regimen A due to an AE (vomiting), but whose PKalues fell within the range for those of the other sub-ects.
igure 3. Mean serum morphine concentration-time profilesxcluding subjects with emesis within the 12-hour dosing inter-
al.
rrtrsctoeimt
aaf8tc
S
po1t(r(amev
T
A
E
Oa
* ects.
TM
S
S
F
334 Effect of Alcohol on Pharmacokinetics of KADIAN
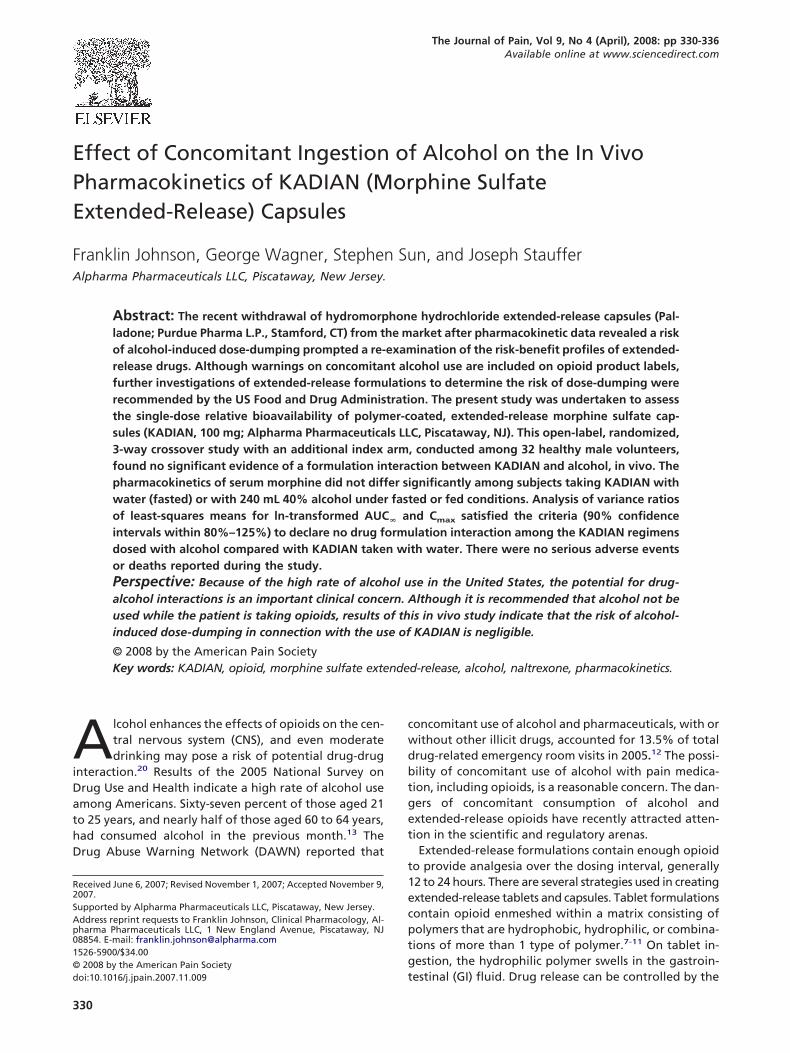
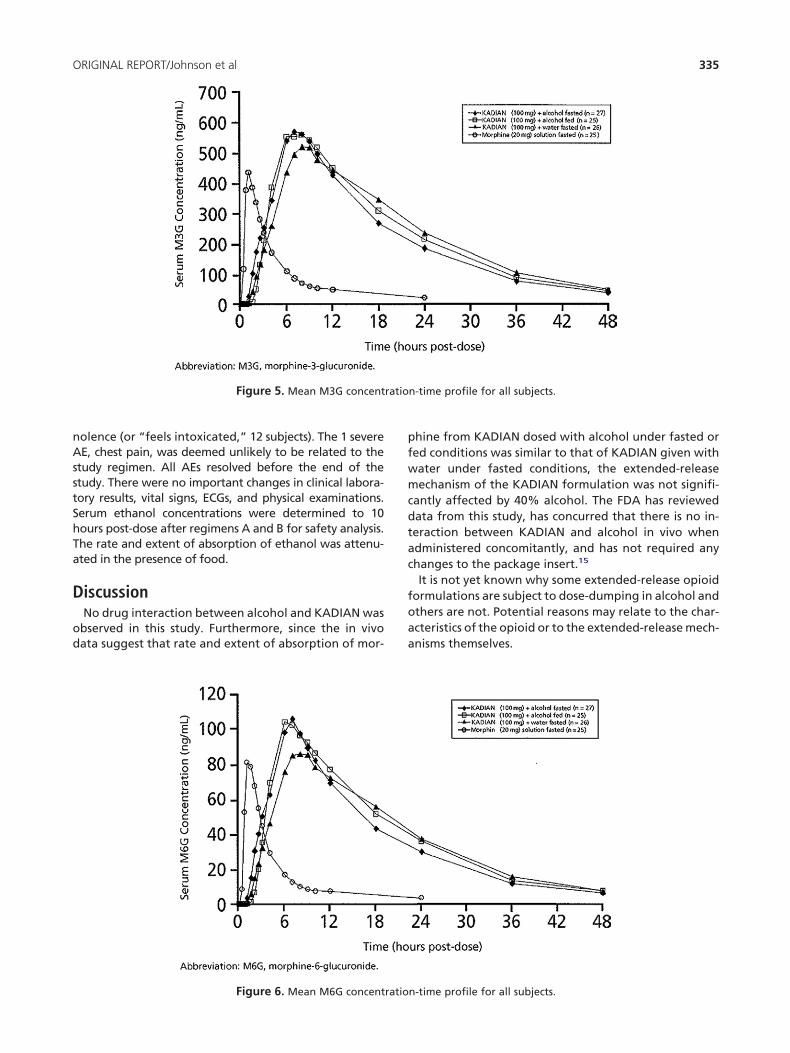
The morphine-3-glucuronides and morphine-6-glucu-onides were also measured during the study. Mean se-um morphine-3- and morphine-6-glucuronide concen-ration-time profiles are presented in Figs 5 and 6,espectively. Visual inspection of the mean profileshows that although the mean peak concentrations withoncomitant alcohol administration were slightly greaterhan the reference treatment, concentrations at the endf terminal elimination phase were similar to the refer-nce treatment. The mean profiles suggest that concom-tant alcohol administration did not adversely affect
orphine metabolism, nor was there any evidence in theerminal phase to suggest the likelihood of metabolite
able 1. Summary of Serum Morphine Pharmac
PARAMETER
REGIMEN A RE
KADIAN � ALCOHOL
FASTED
KADIAN
ll subjects with evaluablepharmacokinetic data
AUC0-ta (ng · h/mL) 271.80 (35.5) (n � 27) 279.33 (2
AUC�a* (ng · h/mL) 300.68 (39.2) (n � 26) 301.6 (3
Cmaxa (ng/mL) 16.95 (42.1) (n � 27) 15.71 (3
Tmaxb (h) 8.0 (4–24) (n � 27) 8.0 (2
t1/2c* (h) 11.8 (4.89) (n � 26) 10.8 (3
xcluding subjects withemesis within 12-hourdosing interval
AUC0-ta (ng · h/mL) 283.22 (32.2) (n � 16) 290.37 (2
AUC�a* (ng · h/mL) 305.74 (32.3) (n � 15) 311.36 (2
Cmaxa (ng/mL) 16.96 (35.4) (n � 16) 16.03 (2
Tmaxb (h) 6.0 (4–24) (n � 16) 8.0 (4
t1/2c* (h) 9.96 (3.11) (n � 15) 10.5 (2
S � oral morphine solution.
Geometric mean (CV%); bMedian (range); cArithmetic mean (SD).
Extrapolated parameters AUC� and t1/2 could not be estimated for some subj
able 2. ANOVA Ratios of Least-Squareseans
REGIMEN
RATIO OF
LSMS, %90% CI
(LOWER; UPPER)
ubjects with at least 1comparison of interest(n � 26)
AUC�(ng · h/mL)A/C 89.1 80.3; 98.9B/C 89.7 80.7; 99.6
Cmax (ng/mL)A/C 102.3 89.5; 116.8B/C 98.0 85.5; 112.3
ubjects with at least 1comparison of interestexcluding those withemesis within 12-hourdosing period (n � 21)
AUC�(ng · h/mL)A/C 96.3 89.4; 103.8B/C 94.6 88.7; 100.9
Cmax (ng/mL)A/C 107.6 93.5; 123.8
B/C 100.9 89.1; 114.3w
ccumulation from multiple dosing with KADIAN andlcohol. Furthermore, ANOVA results for the ln-trans-ormed mean AUC ratios of LSMs provided CIs within0% to 125% for both metabolites, confirming that theotal exposures of both metabolites were not signifi-antly affected by alcohol coadministration.
afety ResultsThere were no reported incidents of respiratory de-ression during the study, nor were there any serious AEsr deaths. Overall, 27 subjects (84%) experienced at leastAE that was possibly or probably related to the adminis-
ration of multiple drugs: 21 subjects (66%) with regimen AKADIAN 100 mg � alcohol [fasted]), 19 subjects (59%) withegimen B (KADIAN 100 mg � alcohol [fed]), 7 subjects22%) with regimen C (KADIAN 100 mg � water [fasted]),nd 3 subjects (9%) with regimen D (morphine sulfate 20g oral solution [fasted]). Most AEs were mild to mod-
rate, the most frequent being nausea (15 subjects),omiting (15 subjects), headache (14 subjects), and som-
etic ParametersB REGIMEN C REGIMEN DLCOHOL KADIAN � WATER
FASTED
DOSE-NORMALIZED OS �WATER FASTED
n � 25) 307.2 (32.2) (n � 26) 231.8 (31.6) (n � 25)n � 25) 337.28 (33.3) (n � 26) 347.8 (27.2) (n � 18)n � 25) 16.46 (32.9) (n � 26) 68.4 (39.0) (n � 25)) (n � 25) 8.0 (6–18) (n � 26) 0.67 (0.33–1.5) (n � 25)n � 25) 11.6 (4.46) (n � 26) 14.3 (8.40) (n � 18)
n � 22) 307.2 (32.2) (n � 26) 231.8 (31.6) (n � 25)n � 22) 337.28 (33.3) (n � 26) 347.8 (27.2) (n � 18)n � 22) 16.46 (32.9) (n � 26) 68.4 (39.0) (n � 25)(n � 22) 8.0 (6–18) (n � 26) 0.67 (0.33–1.5) (n � 25)n � 22) 11.6 (4.46) (n � 26) 14.3 (8.40) (n � 18)
igure 4. C ratio of KADIAN � alcohol versus KADIAN �
okinGIMEN
� AFED
9.3) (3.7) (0.3) (.5–18.20) (
1.2) (3.0) (9.1) (–18).56) (
maxater for each subject.
nAsstShTa
D
od
pfwmcdtac
foaa
ratio
335ORIGINAL REPORT/Johnson et al
olence (or “feels intoxicated,” 12 subjects). The 1 severeE, chest pain, was deemed unlikely to be related to the
tudy regimen. All AEs resolved before the end of thetudy. There were no important changes in clinical labora-ory results, vital signs, ECGs, and physical examinations.erum ethanol concentrations were determined to 10ours post-dose after regimens A and B for safety analysis.he rate and extent of absorption of ethanol was attenu-ted in the presence of food.
iscussionNo drug interaction between alcohol and KADIAN wasbserved in this study. Furthermore, since the in vivoata suggest that rate and extent of absorption of mor-
Figure 5. Mean M3G concent
Figure 6. Mean M6G concentratio
hine from KADIAN dosed with alcohol under fasted ored conditions was similar to that of KADIAN given withater under fasted conditions, the extended-releaseechanism of the KADIAN formulation was not signifi-
antly affected by 40% alcohol. The FDA has reviewedata from this study, has concurred that there is no in-eraction between KADIAN and alcohol in vivo whendministered concomitantly, and has not required anyhanges to the package insert.15
It is not yet known why some extended-release opioidormulations are subject to dose-dumping in alcohol andthers are not. Potential reasons may relate to the char-cteristics of the opioid or to the extended-release mech-nisms themselves.
n-time profile for all subjects.
n-time profile for all subjects.

pmtdnplahgmt
awtiatC
dFmhossmt
mb
A
As
R
1NP
2c
3k3
4h
5s
6Rts
7P
8P
9a
1[c
1c
1twDD
336 Effect of Alcohol on Pharmacokinetics of KADIAN
The KADIAN shell is composed of a combination ofH-independent and pH-dependent water-soluble poly-ers interspersed within a water-insoluble polymer ma-
rix. This unique combination results in pH-dependentrug release from KADIAN. Although the exact mecha-ism is not well understood, the poor solubility of theH-dependent polymer, methacrylic acid copolymer, at
ow pH, may offer sufficient protection from coingestedlcohol while the capsule is in the stomach, where alco-ol would be quickly absorbed. The copolymer thenradually dissolves with increasing pH as the capsuleoves from the stomach through the GI tract to release
he morphine sulfate.While KADIAN maintained its extended-release profile
fter co-ingestion with alcohol, consumption of alcoholith any morphine product, whether immediate- or ex-
ended-release, is not recommended. All opioids, includ-ng KADIAN, may be expected to have additive effectsnd potentially serious outcomes when used in conjunc-ion with alcohol, other opioids, or illicit drugs that cause
NS depression.4 MHHS Publication No. (SMA) 07-4256
1sfiHmA
1mQt
1PR
1EDDil
1uaPA
1uBFa
1PH7
2t
In calling for careful evaluation of the potential forose-dumping with extended-release dosage forms, theDA acknowledged that product labeling and othereans of informing patients about potential drug-alco-
ol interactions may not always be effective. The devel-pment of extended-release formulations that are notensitive to alcohol is a goal.6 Further investigations ofocial drinking and prolonged moderate alcohol intakeay clarify the potential for drug interactions when ex-
ended-release formulations are ingested with alcohol.KADIAN is a registered trademark. KADIAN is a trade-ark owned by Alpharma Pharmaceuticals LLC. All other
rand names are the property of their respective owners.
cknowledgmentsTechnical expertise was provided by Alfred Liang,lpharma Pharmaceuticals LLC. Writing and editorial
upport for this manuscript was provided by Innovex
edical Communications, Parsippany, NJ.eferences
. American Pharmacists Association. Palladone Capsulesew Product Bulletin. 2004. Washington, DC, Americanharmacists Association
. AVINZA [package insert]. 2006. Bristol, TN, King Pharma-euticals, Inc
. Gourlay GK: Sustained relief of chronic pain: Pharmaco-inetics of sustained release morphine. Clin Pharmacokinet5:173-190, 1998
. KADIAN [package insert]. 2007, Piscataway, NJ, Alp-arma Pharmaceuticals LLC
. Ligand Pharmaceuticals Inc. Dear Health Care Profes-ional Letter. 2005. Ligand Pharmaceuticals Inc
. Meyer RJ, Hussain AS: Awareness Topic: Mitigating theisks of Ethanol Induced Dose Dumping from Oral Sus-ained/Controlled Release Dosage Forms. 2005. FDA Advi-ory Committee for Pharmaceutical Services Meeting
. MS Contin [package insert]. 2005. Stamford, CT, Purdueharma LP
. OPANA ER [package insert]. 2007. Chadds Ford, PA, Endoharmaceuticals Inc
. Oramorph SR [package insert]. 2005. Wilmington, NC,aiPharma Inc
0. Oxycodone hydrochloride extended-release tabletspackage insert]. 2004. Chadds Ford, PA, Endo Pharmaceuti-als Inc
1. Reder RF: Opioid formulations: Tailoring to the needs inhronic pain. Eur J Pain 5(Suppl A):109-111, 2001
2. Substance Abuse and Mental Health Services Adminis-ration, Office of Applied Studies. Drug Abuse Warning Net-ork, 2005: National Estimates of Drug-Related Emergencyepartment Visits. 2007. Rockville, MD. DAWN Series D-29,
3. US Department of Health and Human Services, Sub-tance Abuse and Mental Health Services Administration Of-ce of Applied Studies. National Survey on Drug Use andealth (NSDUH). 2005, US Department of Health and Hu-an Services. Substance Abuse and Mental Health Servicesdministration Office of Applied Studies
4. US Food and Drug Administration. Palladone (Hydro-orphone Hydrochloride Extended-Release) Capsules:uestions and Answers. 2005. US Food and Drug Adminis-
ration
5. US Food and Drug Administration. Letter to Alpharmaharmaceuticals NDA 20-616/S-017 and S-021. 2-27-2007.ockville, MD, US Food and Drug Administration
6. US Food and Drug Administration, Center for Biologicsvaluation and Research. Guidance for Industry: In Vivorug Metabolism/Drug Interaction Studies-Study Design,ata Analysis, and Recommendations for Dosing and Label-
ng. 1999. US Food and Drug Administration, Center for Bio-ogics Evaluation and Research
7. US Food and Drug Administration, Center for Drug Eval-ation and Research. Guidance for Industry: Bioavailabilitynd Bioequivalence Studies for Orally Administered Drugroducts–General Considerations. 2007. US Food and Drugdministration, Center for Drug Evaluation and Research
8. US Food and Drug Administration, Center for Drug Eval-ation and Research. Guidance for Industry: Food-Effectioavailability and Fed Bioequivalence Studies. 2002, USood and Drug Administration, Center for Drug Evaluationnd Research
9. US Food and Drug Administration. FDA Alert: Alcohol-alladone Interaction. Alert for Healthcare Professionals:ydromorphone hydrochloride extended-release capsules.-13-2005. US Food and Drug Administration. 2-23-2007
0. Weathermon R, Crabb DW: Alcohol and medication in-
eractions. Alcohol Res Health 23:40-54, 1999