effect of myofascial trigger point - lib.pt.cu.edu.eg fayek hammam mansour 4493-4494.pdf · pre and...
TRANSCRIPT

EFFECT OF MYOFASCIAL TRIGGER POINT
PRESSURE RELEASE ON HEADACHE IN
CHRONIC MECHANICAL NECK PAIN
By
Radwa Fayek Hammam Mansour
First of all I would like to kneel thanking to ALLAH that
enable me to conduct this work.
I would like to thank Prof. Dr. Ragia Mohamed Kamel,
Professor of Physical Therapy, Basic Science Department, Faculty
of Physical Therapy, Cairo University for her great support and
advice to start and complete this study as the best as I could do.
My gratitude appreciation wishes Dr. Amro Saber El Sayed,
Lecturer of orthopedic surgery department, faculty of medicine,
Menofia University, for his great support.
My deepest thanks to Dr. Salah El Din Bassit Ahmed,
Lecturer of Physical Therapy Basic Science Department,
Faculty of Physical Therapy, Cairo University, for her
kind help, valuable advices, constant encouragement to
complete this study.
I would like to thank My Parents for great support
and constant encouragement to complete this study.
Headache is a common experience in adults.
Recurring headaches negatively impact family life,
social activity, and work capacity. For many people,
headache starts as pain or tension at the top of the
neck. As the pain worsens, it may spread to the back
of the head, the temples, the forehead, or behind the
eyes. Moving the neck or bending forward for a long
time tends to make it worse. A disorder of the upper
neck joints or muscles can cause referred pain to the
head.
Cervicogenic headache (CH) is a secondary
headache, which means head pain with a cervical
source. It is characterized by unilateral headache
with symptoms and signs of neck involvement, for
example, pain by movement, external pressure over
the upper cervical, and/or sustained awkward head
positions.
It has been hypothesized that muscle TrPs can
play a relevant role in the genesis of headache. A TrP
is usually defined as a hyperirritable spot within a
taut band of a skeletal muscle that elicits a referred
pain upon examination
However, data related to TrPs in CH are scarce.
Therefore the aim of the present study was to
investigate the efficacy of myofasial trigger point
release for upper cervical muscles on CH in patients
with chronic mechanical neck pain.
Could myofascial trigger point pressure
release for active trigger points (ATrPs) in upper
cervical muscles reduce pain and improve
functional ability in patients with CH ?

Conservative therapies are recommended as the first
treatment of choice. Few studies have been directed towards
evaluating the efficacy of treatment methods for CH.
There are other physical therapeutic modalities that can
only add to the beneficial short term effects of myofascial
trigger point pressure release or exercises. These modalities are
such as ultrasonic, acupuncture , and such modalities cause an
improvement in the signs and symptoms, and are not treatment
for the pathological changes. That is because the short
sarcomeres forming the taut bands are not stretched, and the
release of the trigger points themselves does not occur , so they
have only a temporary effect, without treatment of the
pathology itself as do our treatment (myofascial trigger point
pressure release).
The purpose of the study was to determine the effect of
myofascial trigger point pressure release for upper cervical
muscles on pain and functional ability on patients with CH.
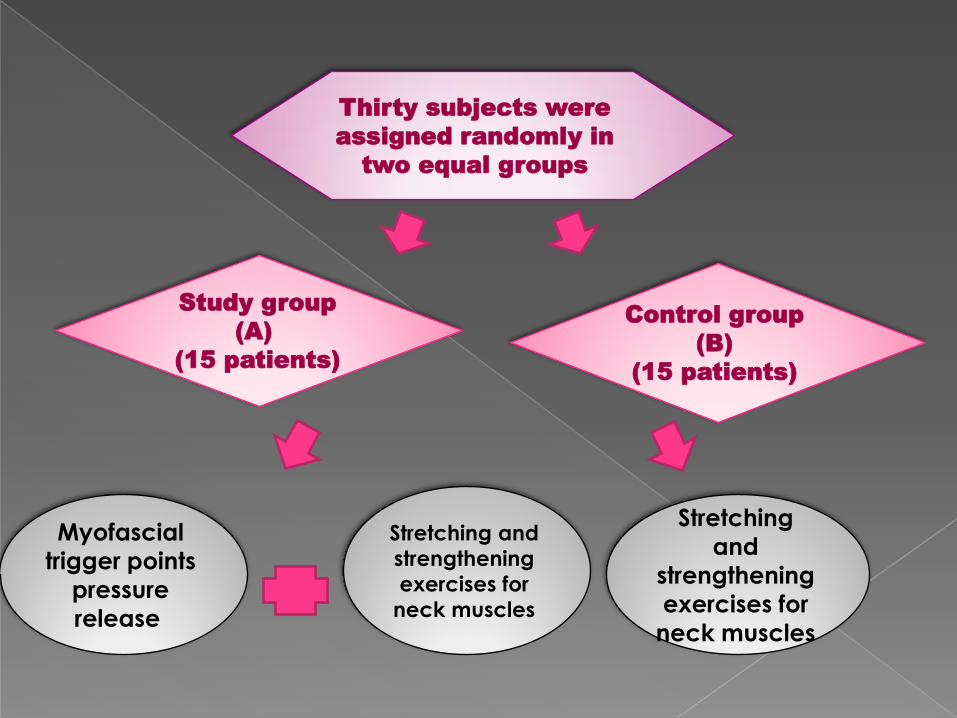
Control group
(B)
(15 patients)
Study group
(A)
(15 patients)
Stretching
and
strengthening
exercises for
neck muscles
Myofascial
trigger points
pressure
release
Stretching and
strengthening
exercises for
neck muscles
Thirty subjects were
assigned randomly in
two equal groups
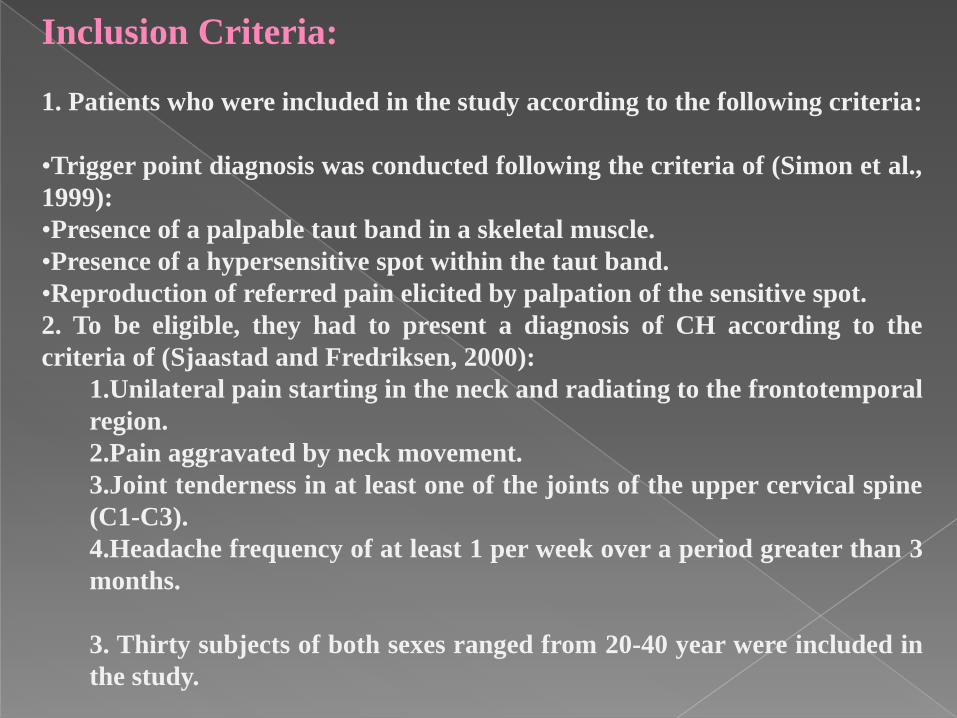
Inclusion Criteria:
1. Patients who were included in the study according to the following criteria:
•Trigger point diagnosis was conducted following the criteria of (Simon et al.,
1999):
•Presence of a palpable taut band in a skeletal muscle.
•Presence of a hypersensitive spot within the taut band.
•Reproduction of referred pain elicited by palpation of the sensitive spot.
2. To be eligible, they had to present a diagnosis of CH according to the
criteria of (Sjaastad and Fredriksen, 2000):
1.Unilateral pain starting in the neck and radiating to the frontotemporal
region.
2.Pain aggravated by neck movement.
3.Joint tenderness in at least one of the joints of the upper cervical spine
(C1-C3).
4.Headache frequency of at least 1 per week over a period greater than 3
months.
3. Thirty subjects of both sexes ranged from 20-40 year were included in
the study.
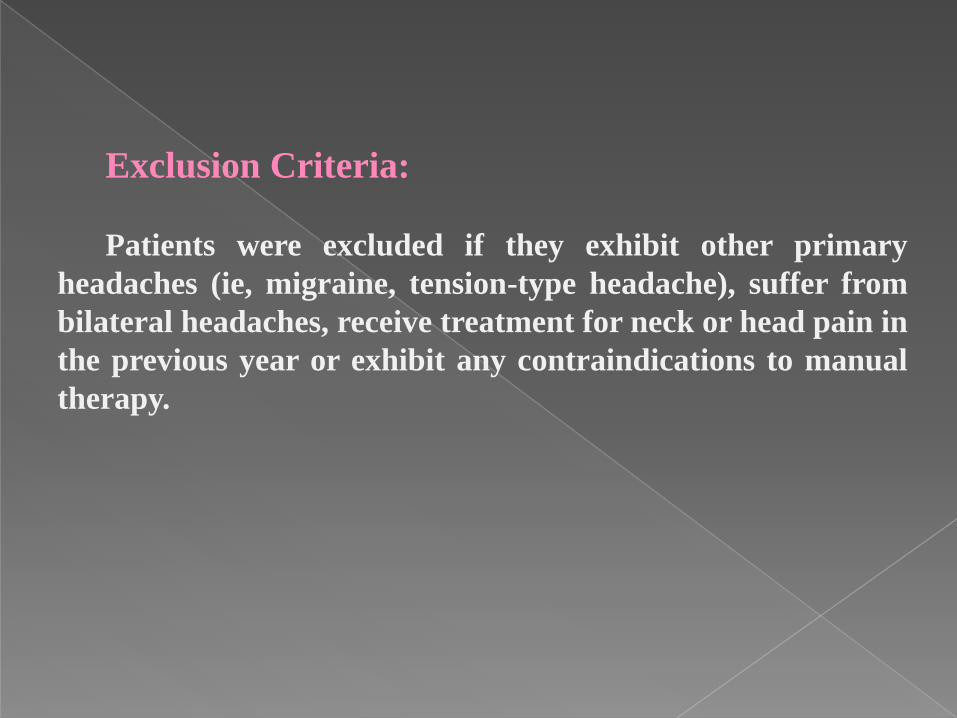
Exclusion Criteria:
Patients were excluded if they exhibit other primary
headaches (ie, migraine, tension-type headache), suffer from
bilateral headaches, receive treatment for neck or head pain in
the previous year or exhibit any contraindications to manual
therapy.
Instrumentations:
(a) Visual analogue scale.
(b) Neck disability index (NDI): (Vernon and Mior, 1991).
(c) Smart phone inclinometer was used to measure active
cervical range of motion.
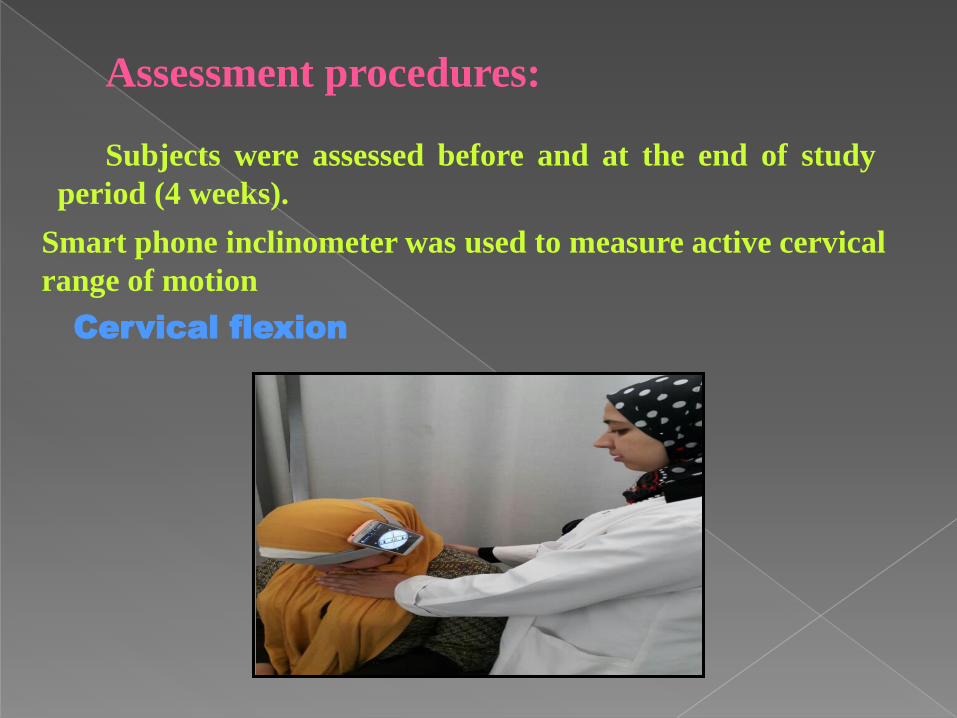
Assessment procedures:
Subjects were assessed before and at the end of study
period (4 weeks).
Smart phone inclinometer was used to measure active cervical
range of motion
Cervical flexion
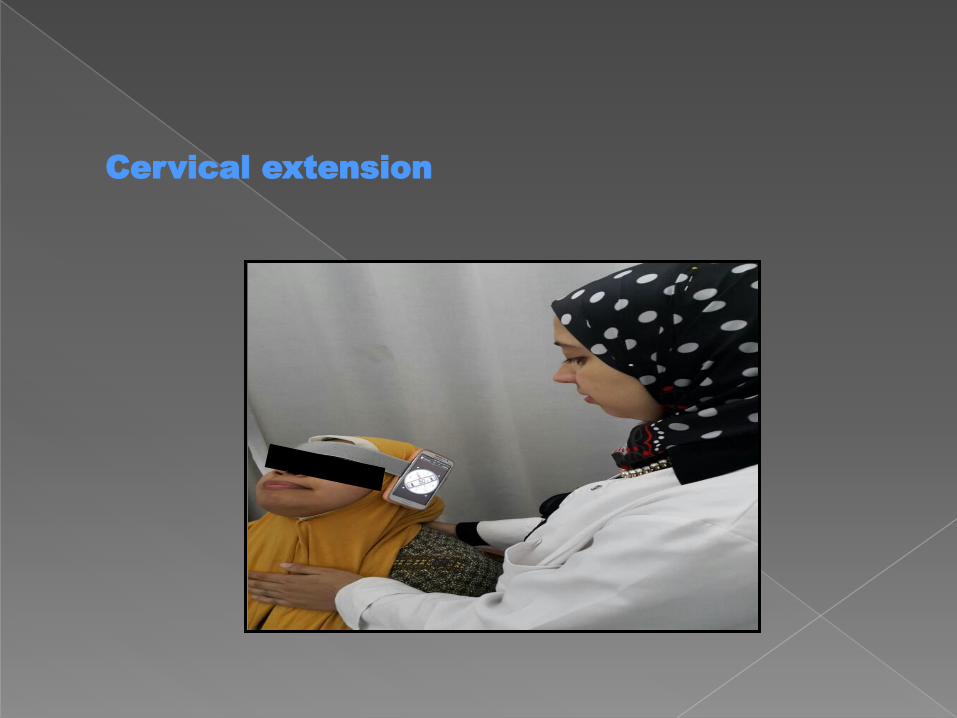
Cervical extension
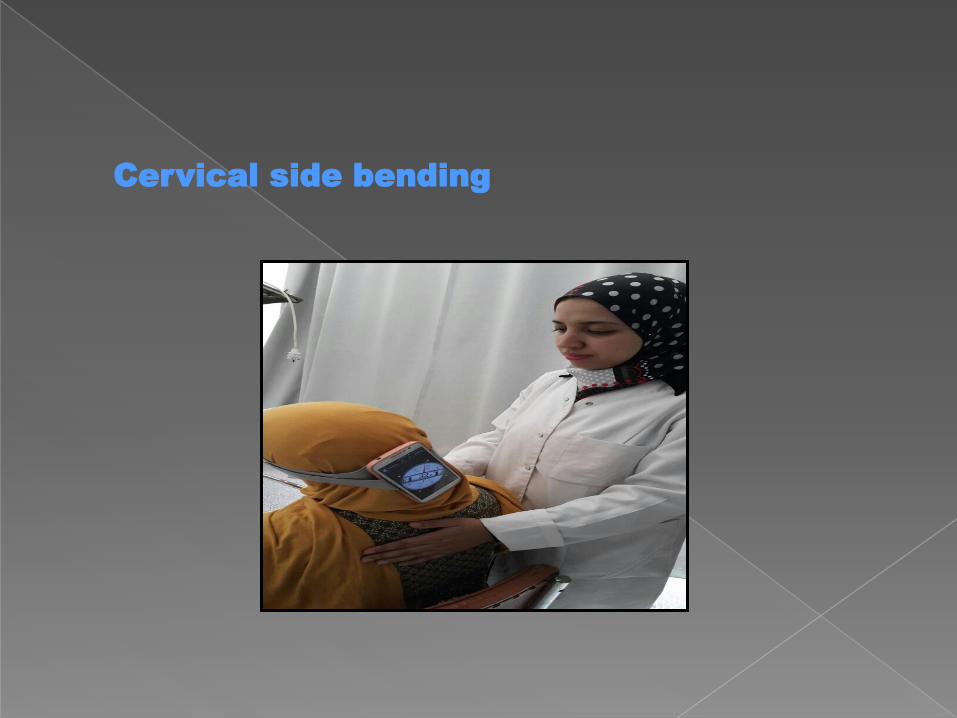
Cervical side bending
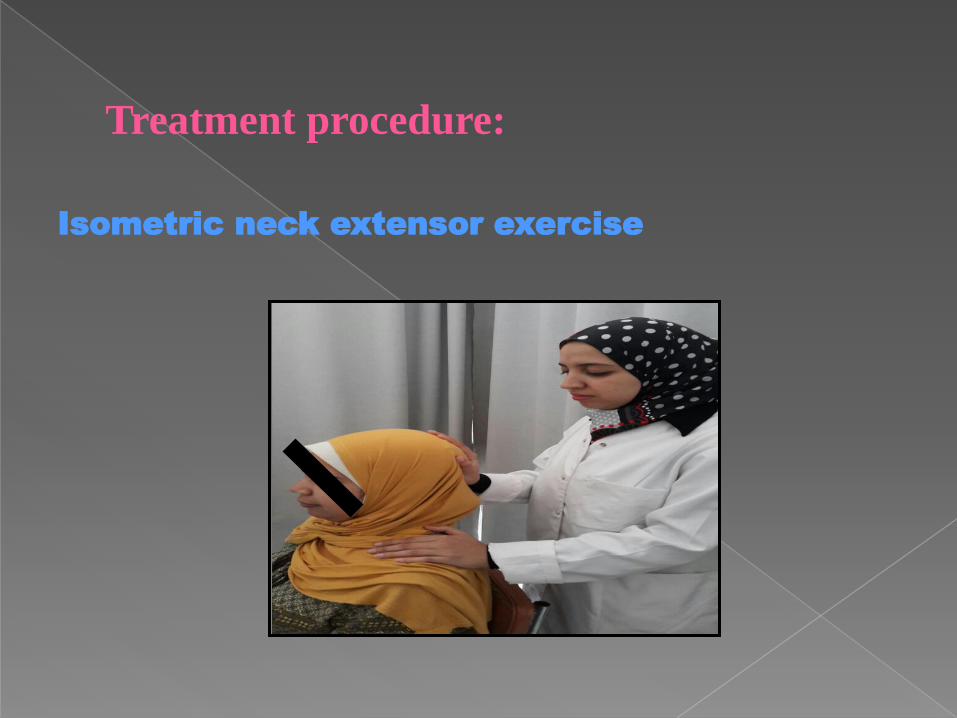
Treatment procedure:
Isometric neck extensor exercise
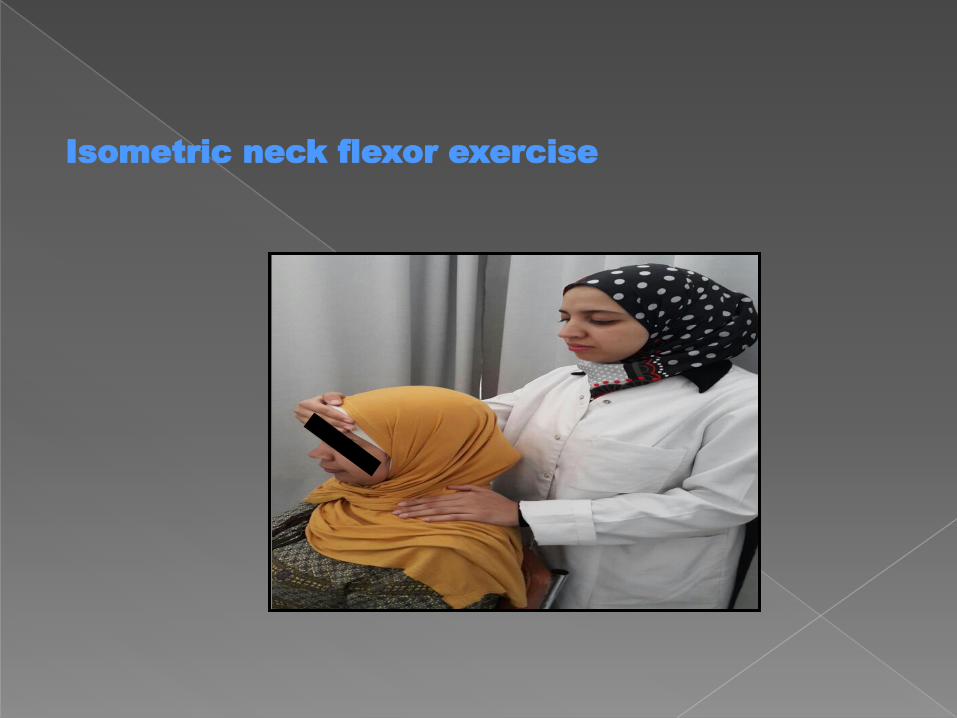
Isometric neck flexor exercise
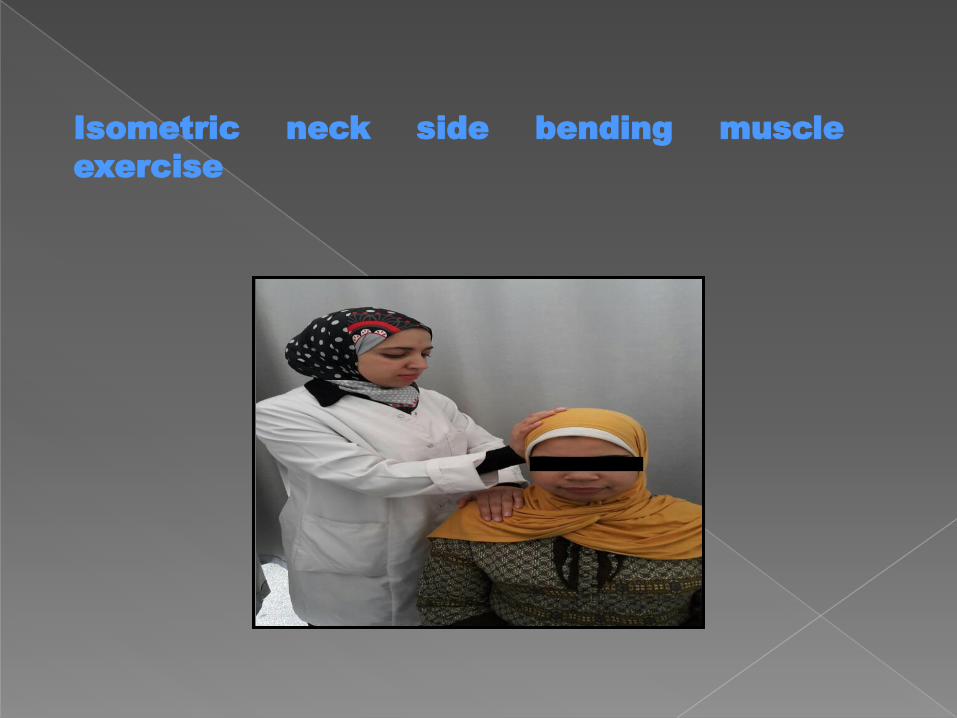
Isometric neck side bending muscle
exercise
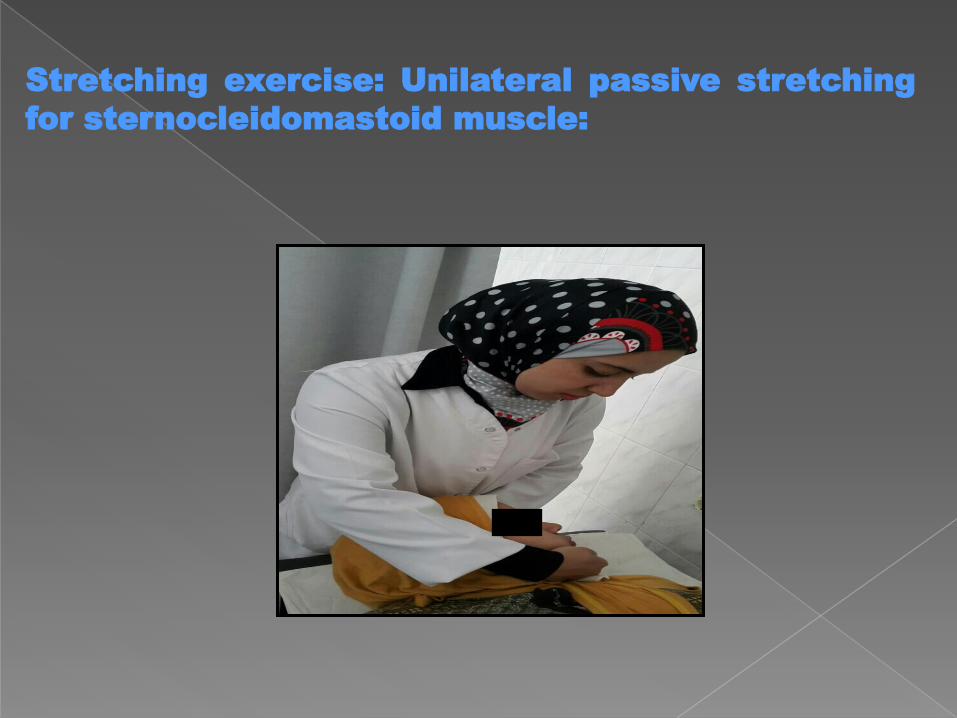
Stretching exercise: Unilateral passive stretching
for sternocleidomastoid muscle:
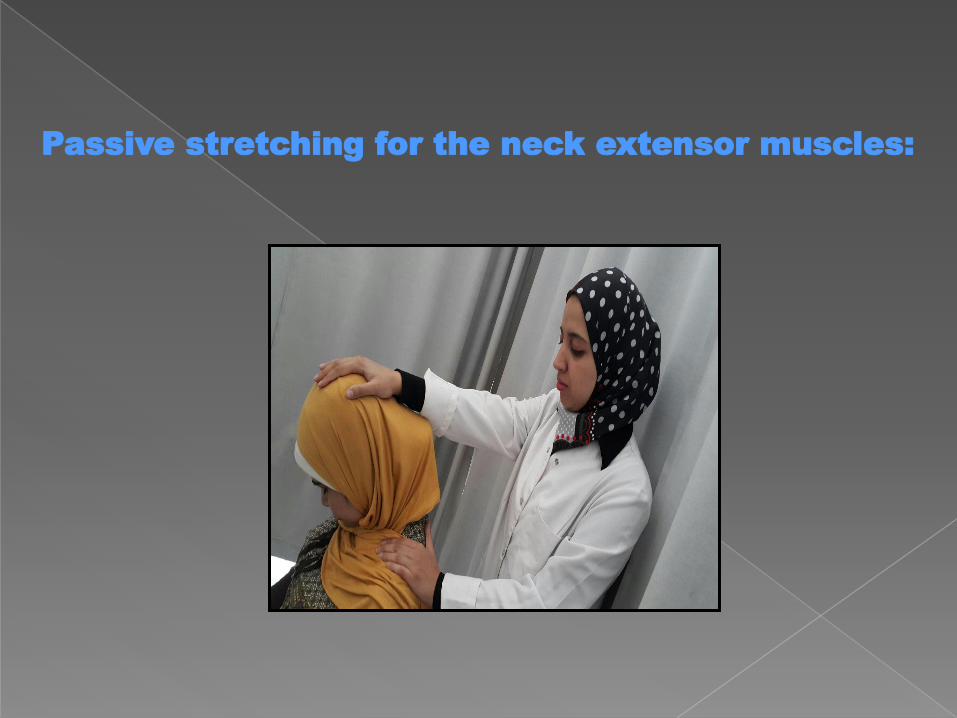
Passive stretching for the neck extensor muscles:
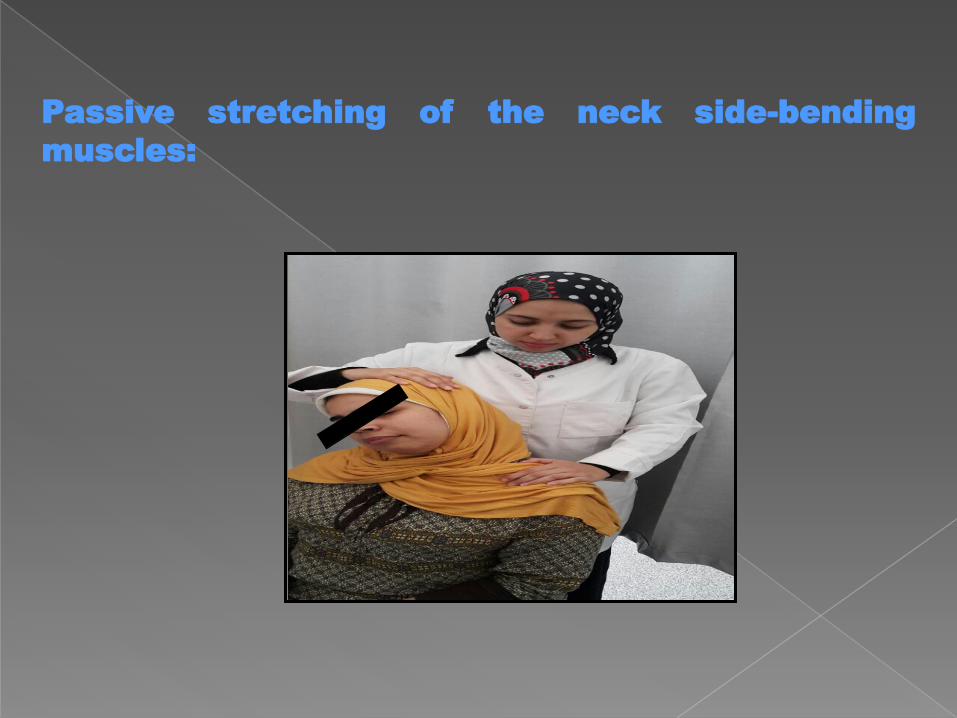
Passive stretching of the neck side-bending
muscles:
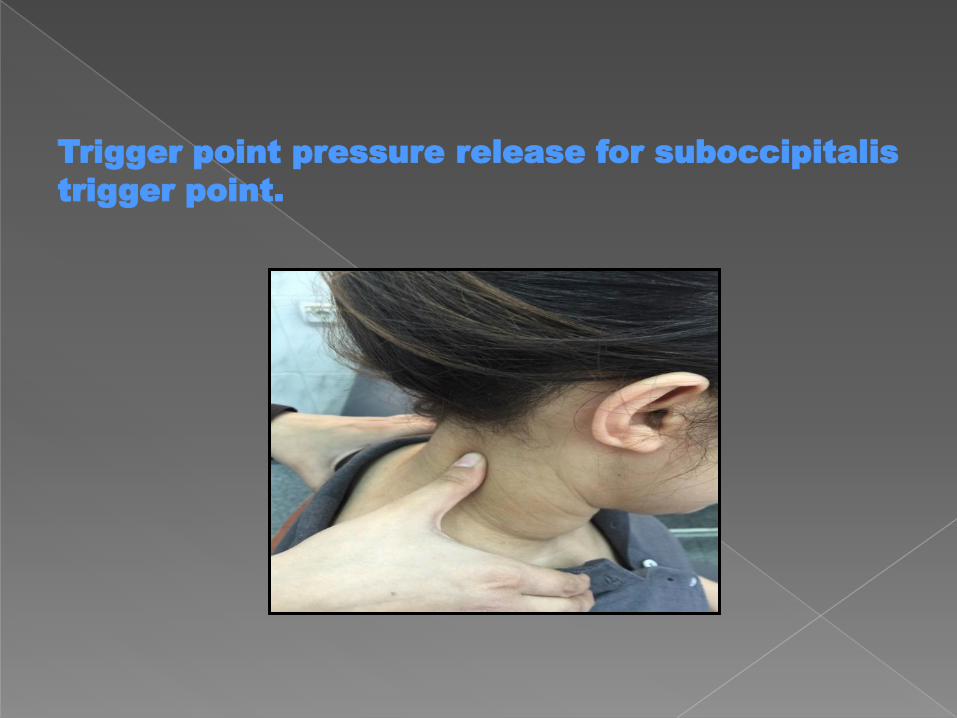
Trigger point pressure release for suboccipitalis
trigger point.
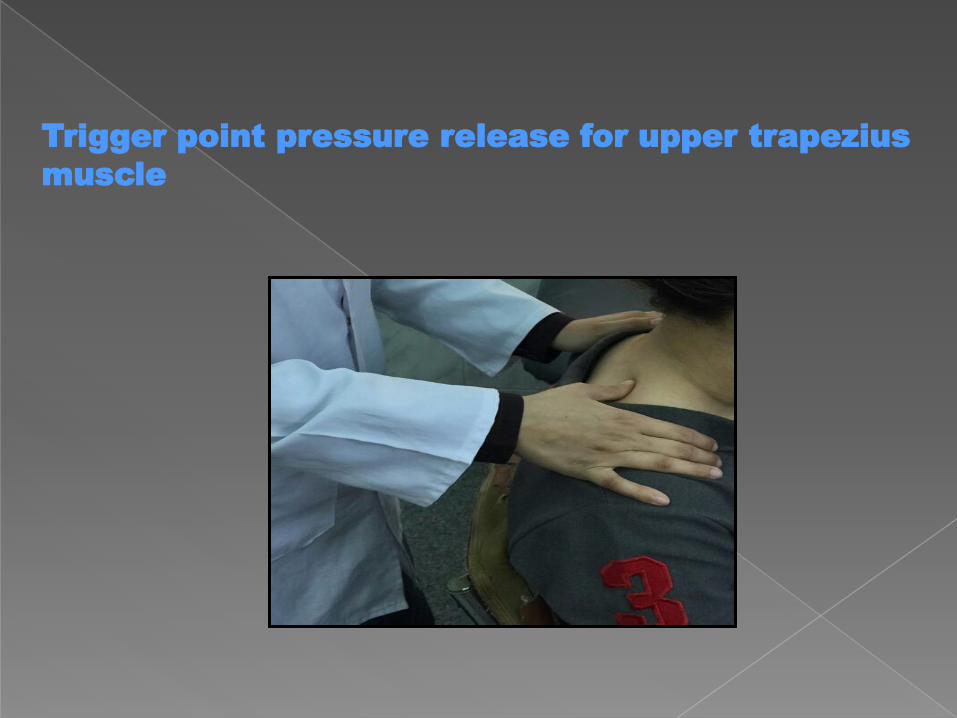
Trigger point pressure release for upper trapezius
muscle
Trigger point pressure release for trigger point
at the root of the neck
0
1
2
3
4
Study group Control group
2
3
VA
S
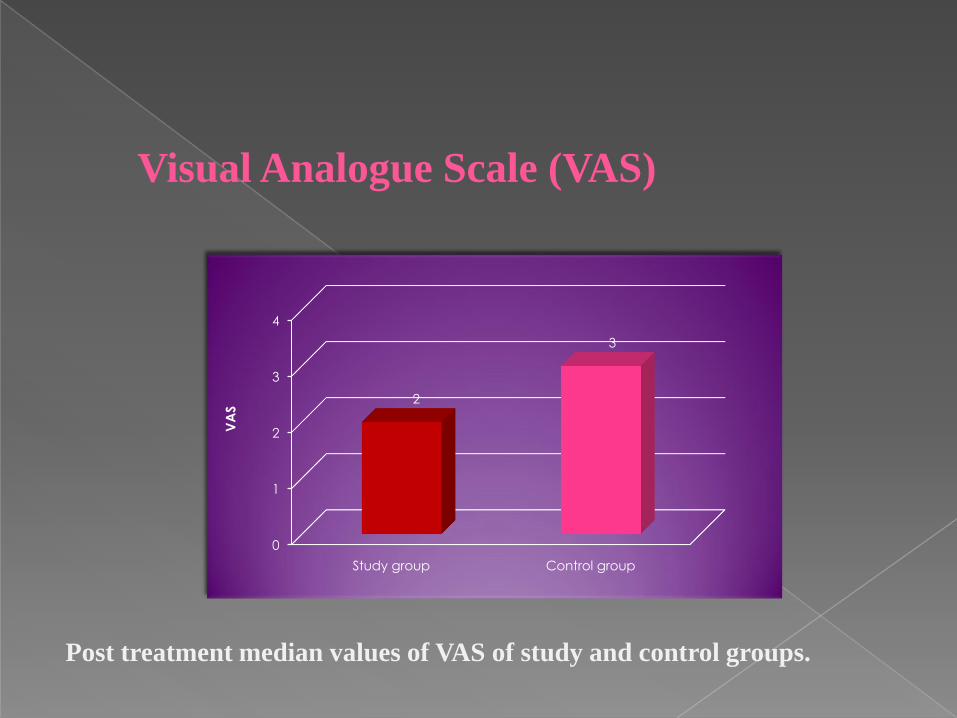
Visual Analogue Scale (VAS)
Post treatment median values of VAS of study and control groups.
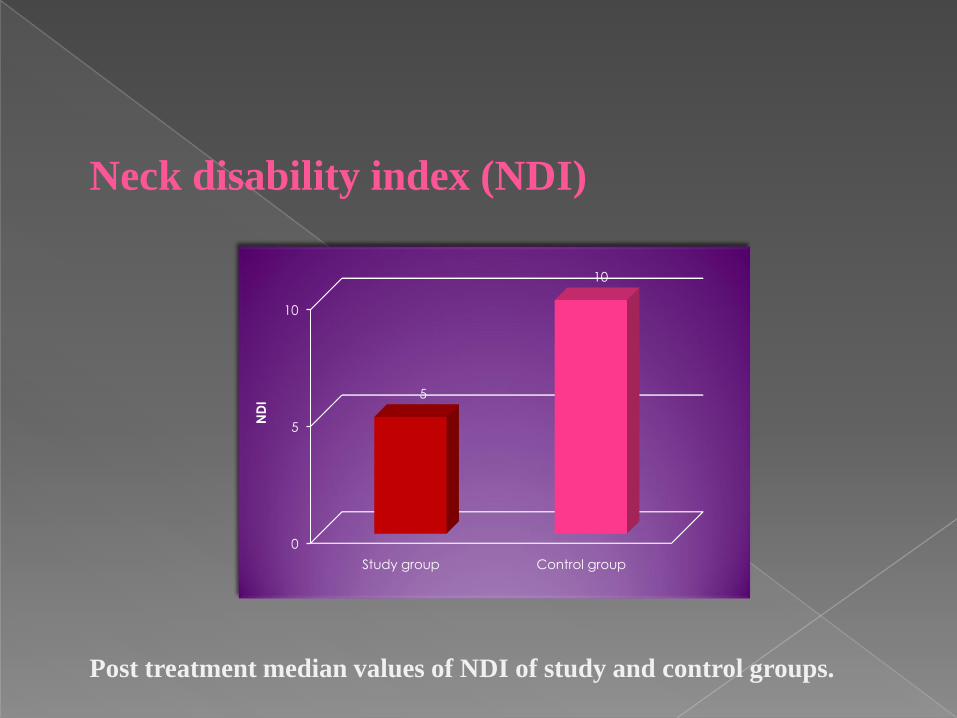
Neck disability index (NDI)
0
5
10
Study group Control group
5
10
ND
I
Post treatment median values of NDI of study and control groups.
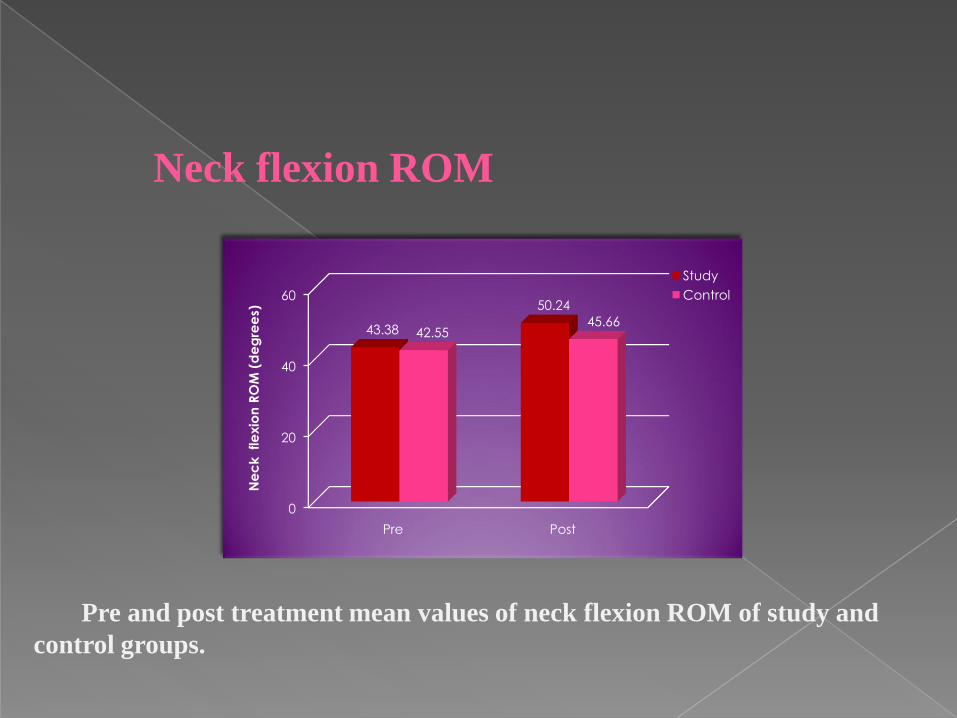
Neck flexion ROM
0
20
40
60
Pre Post
43.38
50.24
42.5545.66
Ne
ck
fle
xio
n R
OM
(d
eg
ree
s)
Study
Control
Pre and post treatment mean values of neck flexion ROM of study and
control groups.
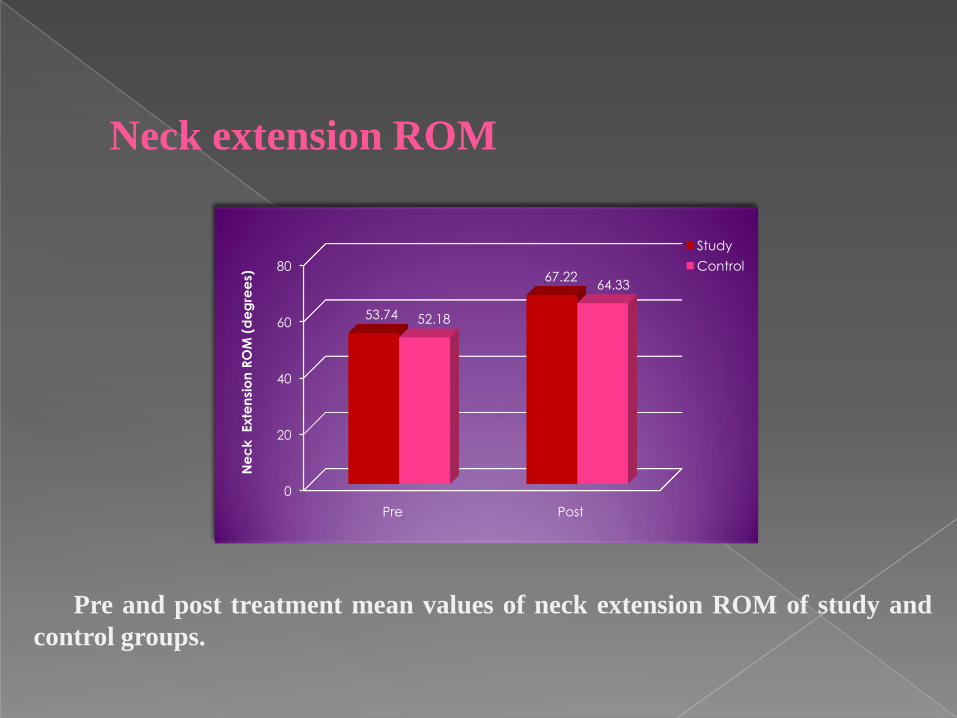
Neck extension ROM
0
20
40
60
80
Pre Post
53.74
67.22
52.18
64.33
Ne
ck
Exte
nsi
on
RO
M (
de
gre
es)
Study
Control
Pre and post treatment mean values of neck extension ROM of study and
control groups.
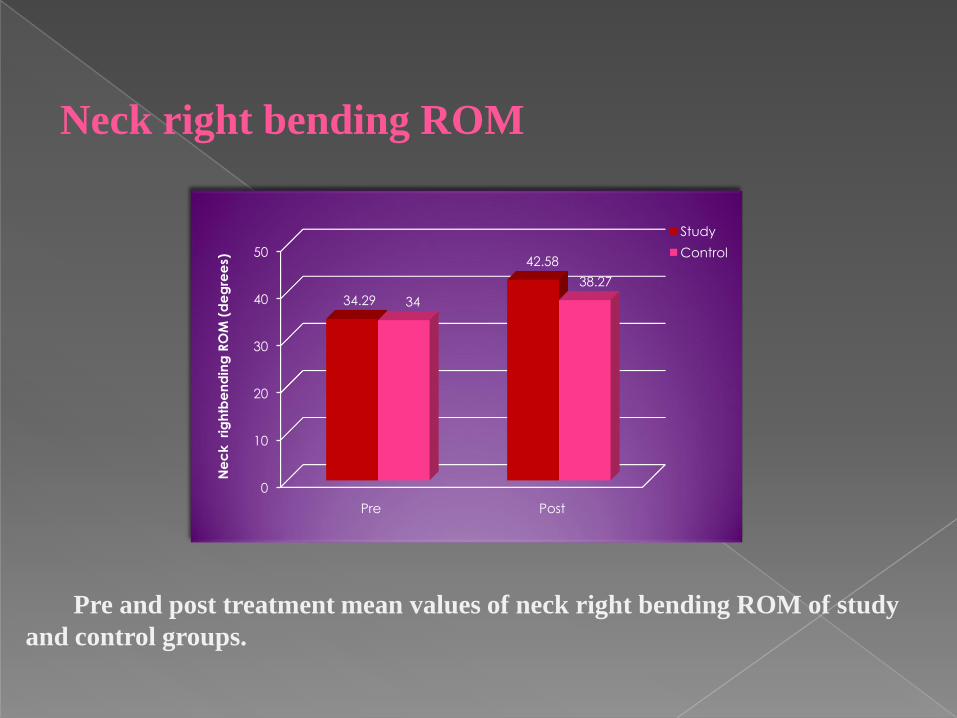
Neck right bending ROM
0
10
20
30
40
50
Pre Post
34.29
42.58
34
38.27
Ne
ck
ri
gh
tbe
nd
ing
RO
M (
de
gre
es)
Study
Control
Pre and post treatment mean values of neck right bending ROM of study
and control groups.
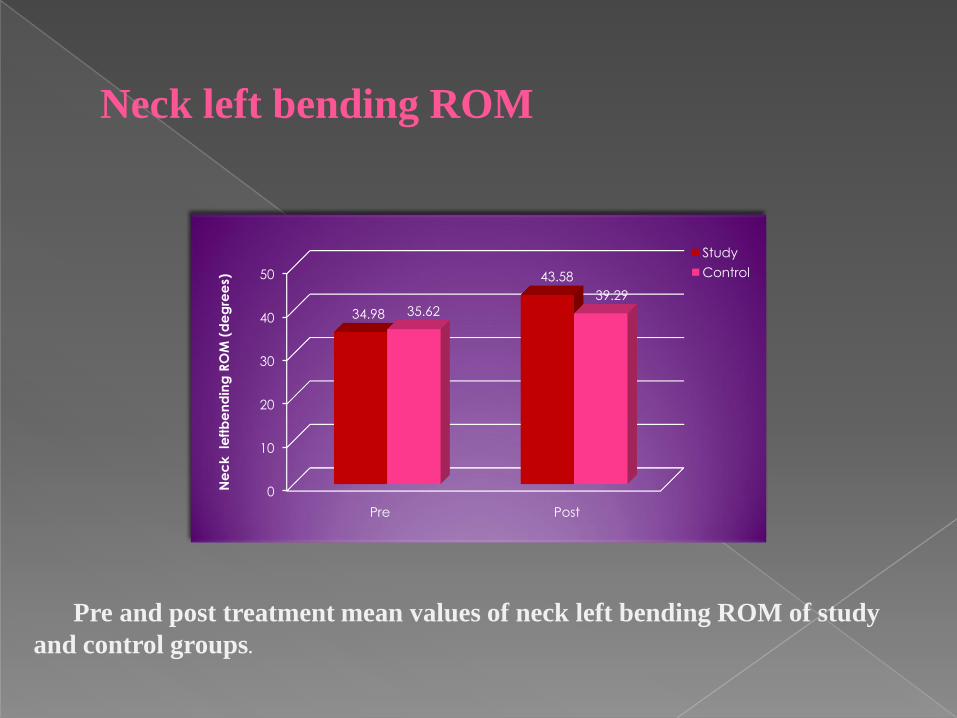
Neck left bending ROM
0
10
20
30
40
50
Pre Post
34.98
43.58
35.62
39.29
Ne
ck
le
ftb
en
din
g R
OM
(d
eg
ree
s)
Study
Control
Pre and post treatment mean values of neck left bending ROM of study
and control groups.
Based on the scope and
findings of this study, It can be
concluded that Myofascial
Trigger Point Pressure Release
Technique is a safe and effective
modality, and resulted in great
improvements in pain
intensity, and functional ability
in patients with cervicogenic
headache.
