effect of preexisting bundle branch block on the electrocardiographic diagnosis of ventricular...
TRANSCRIPT
Effect of Preexisting Bundle Branch Block on the Electrocardiographic Diagnosis
of Ventricular Tachycardia Mark S. Kremers, MD, William H. Black, MD, Peter J. Wells, MD, and Martha Solodyna, RN
The electrocardiograms (ECGs) of 80 ventricular tachycardias (VTs) occurring in 52 patients with a normal baseline QRS duration (group 1) were com- pared with 26 VTs in 18 patients with preexisting bundle branch block (group 2). The effects of bun- dle branch block on the sensitivity of previously de- fined electrocardiographic criteria for differentiat- ing VT from supraventricular tachycardia with ab- erration were under investigation. Specificity was examined by comparing VT to the baseline ECG in group 2 patients. The VTs in groups 1 and 2 were comparable with respect to rate, bundle branch pattern, R-wave pattern in VI with right bundle, frequency of an R/S ratio <l in Vs with right bun- dle, Q-wave frequency in Vs with left bundle and quadrant of the frontal plane axis. Precordial QRS concordance was more frequent (35 vs 15%, p = 0.045) and a >30 ms R wave in VI or Vp with left bundle pattern was less frequent (18 vs 63%, p = 0.015) in group 2 vs group 1 arrhythmias. Right bundle pattern VT usually had a monophasic R wave in VI (69%), whereas preexisting right bun- dle usually had a biphasic R wave in VI (82%, p = 0.001). The quadrant of the frontal plane axis was significantly different between the VT ECGs and the ECGs with preexisting bundle branch block (p = 0.029) with a right superior quadrant axis only seen in VT (19%). A >30 ms R wave in VI or VZ with left bundle was also only seen in VT (52 vs 0%, p = 0.052). These data suggest that the sensi- tivity for VT of a >30 ms R wave in VI or VZ with left bundle pattern is diminished by preexisting bundle branch block but the sensitivity of other ECG markers of VT are not affected. Precordial QRS concordance, a monophasic R wave in VI, a right superior axis and a >30 ms R wave in VI or V2 with left bundle are infrequently seen with pre- existing bundle branch block and therefore should suggest a diagnosis of VT even if a baseline ECG is unavailable.
(Am J Cardiol 1988;62:1208-1212)
From the Department of Internal Medicine, Cardiology Division, the University of Texas Southwestern Medical Center at Dallas, and the Electrophysiology Laboratory, Parkland Memorial Hospital, Dallas, Texas. Manuscript received June 21,1988; revised manuscript received August 4, 1988, and accepted August 7.
Address for reprints: Mark S. Kremers, MD, Cardiology Division, University of Texas Southwestern Medical Center, 5323 Harry Hines Boulevard, Dallas, Texas 75235-9034.
1208 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 62
T he differentiation of supraventricular tachycardia with a wide QRS from ventricular tachycardia (VT) is a difficult diagnostic problem upon
which important therapeutic decisions are based.‘e3 Multiple electrocardiographic criteria have been pro- posed to assist in this differentiation including ,certain QRS morphologic patterns.4-9 The best known QRS patterns were described by Wellens et al* and were de- rived from patients with normal baseline electrocardio- grams (ECGs). However, their value when the baseline ECG is abnormal or unavailable is incompletely de- fined.
We examined the effect of preexisting bundle branch block on several electrocardiographic markers of VT by comparing the ECGs of sustained VT in patients with normal baseline QRS complex duration to those of patients with preexisting bundle branch block. In this manner, we sought to determine if the sensitivity of pro- posed QRS criteria for diagnosing VT are affected by an abnormal baseline tracing. We also compared the baseline ECGs with preexisting bundle branch block to those of VT to determine the specificity of the QRS morphologic patterns.
METHODS The 12-lead ECGs during sinus rhythm and VT of
all patients who had sustained uniform VT (2 15 beats) induced and confirmed at electrophysiologic study at Parkland Memorial Hospital or the Veterans Adminis- tration Hospital in Dallas, Texas, from February 1984 to December 1987 were evaluated in this study. Electro- physiologic study was performed in a standard fashion after discontinuing all antiarrhythmic drugs for >5 half-lives. VT was confirmed by the inability to record a His potential, the presence of atrioventricular dissocia- tion, or both. ECGs were recorded with a Nihon-Koden or Marquette Electronics machine at a paper speed of 25 mm/s and 1 mV/cm amplification. All ECGs were independently graded by 3 of us for cycle length, mean frontal plane QRS axis and QRS pattern. Disagree- ments were resolved by discussion and mutual consent. The baseline QRS was considered of normal duration if it was <120 ms. Bundle branch block was diagnosed when the baseline QRS width was 2 120 ms.
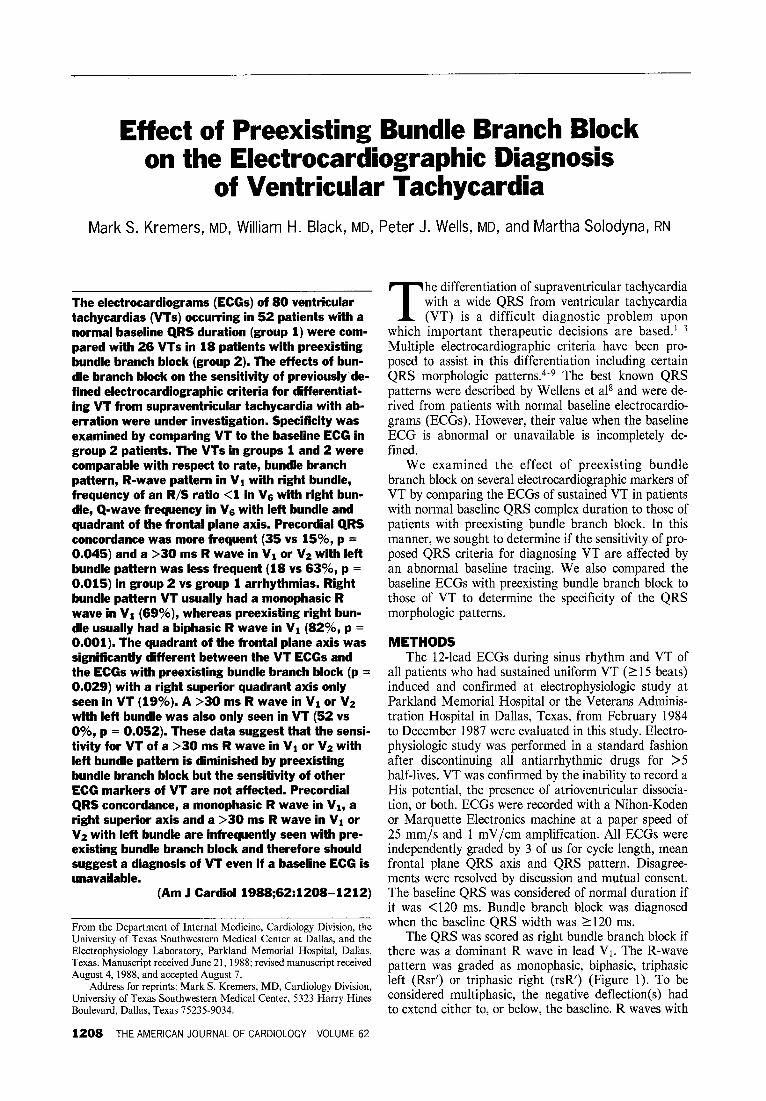
The QRS was scored as right bundle branch block if there was a dominant R wave in lead Vl. The R-wave pattern was graded as monophasic, biphasic, triphasic left (Rsr’) or triphasic right (rsR’) (Figure 1). To be considered multiphasic, the negative deflection(s) had to extend either to, or below, the baseline. R waves with
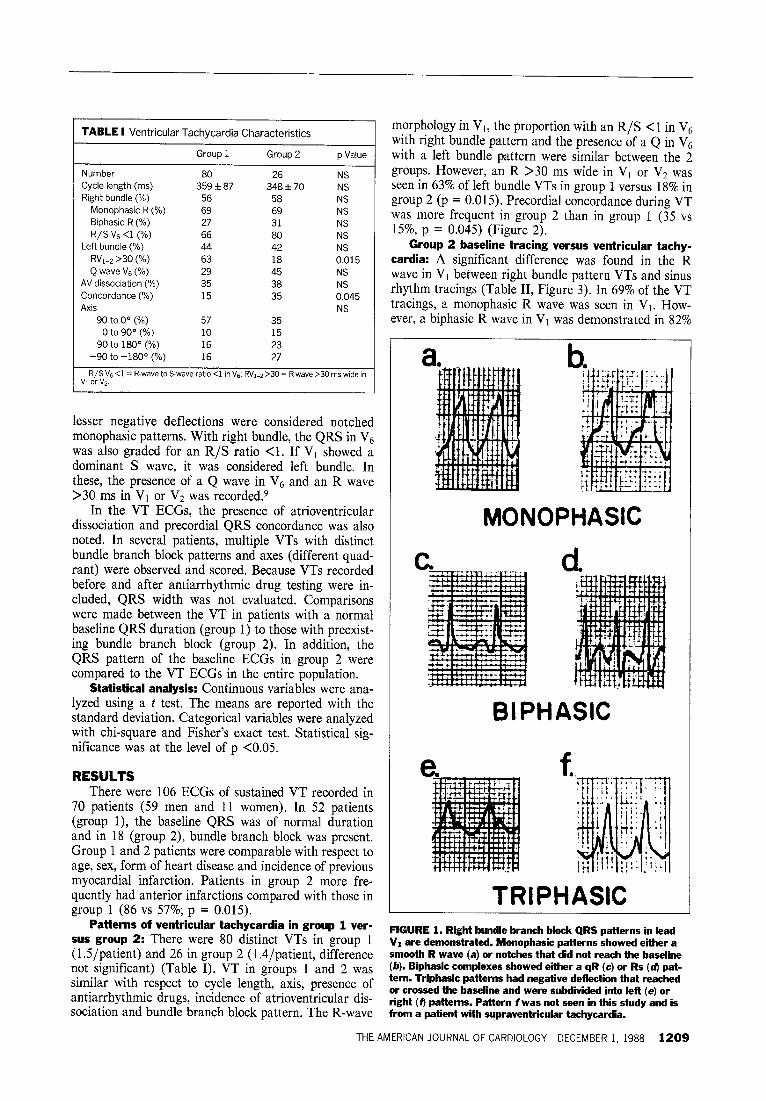
TABLE I Ventricular Tachycardia Characteristics
Group 1 Group 2 p Value
Number 80 26 NS Cycle length (ms) 359 f 87 348 f 70 NS Right bundle (%) 56 58 NS
Monophasic R (%) 69 69 NS
Biphasic R (%) 27 31 NS R/S V,j <l (%) 66 80 NS
Left bundle (%) 44 42 NS RVI-z >30 (%) 63 18 0.015 Q wave V6 (%) 29 45 NS
AV dissociation (%) 35 38 NS
Concordance (%) 15 35 0.045 Axis NS
-90 to 00 (%) 57 35 0 to 900 (%) 10 15
90 to 180° (%) 16 23 -90 to -180° (%) 16 27
R/S Vs <l = R-wave to S-wave ratio 4 in VS; RVI-2 >30 = R wave >30 rns wide in v, or VP.
lesser negative deflections were considered notched monophasic patterns. With right bundle, the QRS in V6 was also graded for an R/S ratio <l. If Vi showed a dominant S wave, it was considered left bundle. In these, the presence of a Q wave in V6 and an R wave >30 ms in Vi or VZ was recorded.9
In the VT ECGs, the presence of atrioventricular dissociation and precordial QRS concordance was also noted. In several patients, multiple VTs with distinct bundle branch block patterns and axes (different quad- rant) were observed and scored. Because VTs recorded before and after antiarrhythmic drug testing were in- cluded, QRS width was not evaluated. Comparisons were made between the VT in patients with a normal baseline QRS duration (group 1) to those with preexist- ing bundle branch block (group 2). In addition, the QRS pattern of the baseline ECGs in group 2 were compared to the VT ECGs in the entire population.
Statistical analysis: Continuous variables were ana- lyzed using a t test. The means are reported with the standard deviation. Categorical variables were analyzed with chi-square and Fisher’s exact test. Statistical sig- nificance was at the level of p <0.0.5.
RESULTS There were 106 ECGs of sustained VT recorded in
70 patients (59 men and 11 women). In 52 patients (group l), the baseline QRS was of normal duration and in 18 (group 2), bundle branch block was present. Group 1 and 2 patients were comparable with respect to age, sex, form of heart disease and incidence of previous myocardial infarction. Patients in group 2 more fre- quently had anterior infarctions compared with those in group 1 (86 vs 57%; p = 0.015).
morphology in Vi, the proportion with an R/S <l in V6 with right bundle pattern and the presence of a Q in V6 with a left bundle pattern were similar between the 2 groups. However, an R >30 ms wide in Vt or VZ was seen in 63% of left bundle VTs in group 1 versus 18% in group 2 (p = 0.015). Precordial concordance during VT was more frequent in group 2 than in group 1 (35 vs 15%, p = 0.045) (Figure 2).
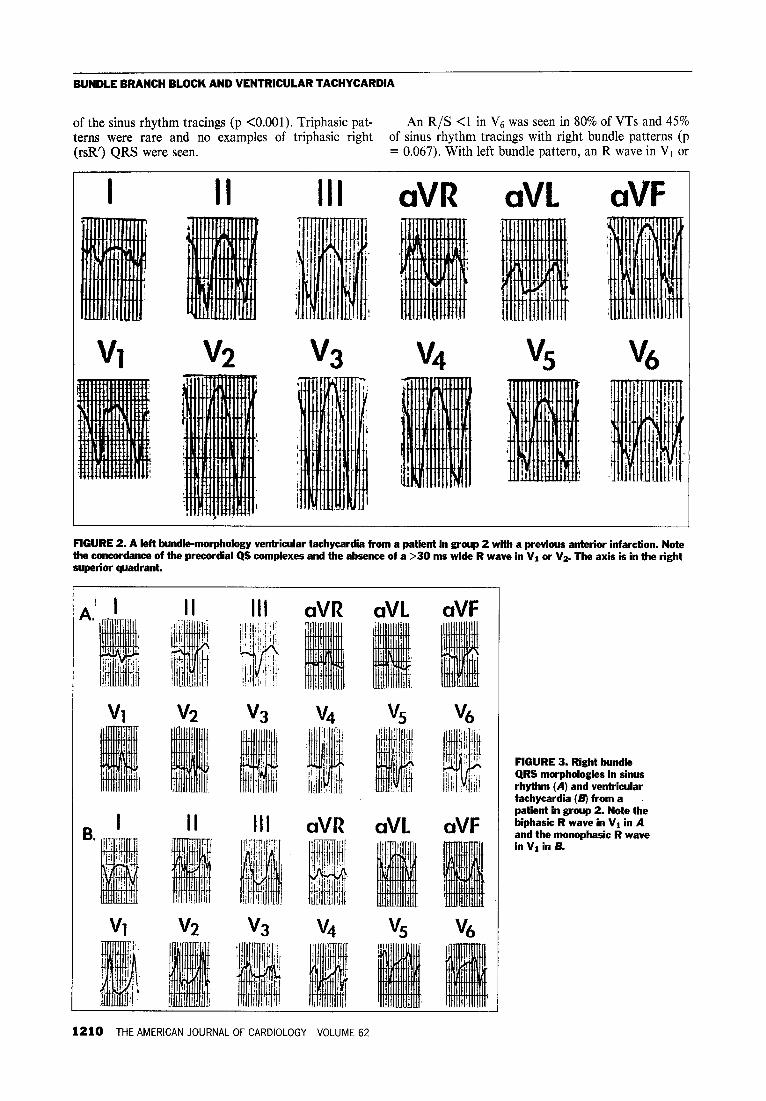
Group 2 baseline tracing versus ventricular tachy- cardia: A significant difference was found in the R wave in VI between right bundle pattern VTs and sinus rhythm tracings (Table II, Figure 3). In 69% of the VT tracings, a monophasic R wave was seen in VI. How- ever, a biphasic R wave in Vi was demonstrated in 82%
a.
MONOPHASIC
d
BIPHASIC
TRIPHASIC Patterns of ventricular tachycardia in group 1 ver-
sus group 2: There were 80 distinct VTs in group 1 FIGURE 1. Right bundle branch block QRS patterns in lead
(1.5/patient) and 26 in group 2 (1,4/patient, difference VI are demonstrated. Monophasic patterns showed either a smooth R wave (a) or notches that did not reach the baseline
not significant) (Table I). VT in groups 1 and 2 was (/J). Riphasic complexes showed either a qR (c) or Rs (d) pat-
similar with respect to cycle length, axis, presence of tern. Triphasic patterns had negative deflection that reached
antiarrhythmic drugs, incidence of atrioventricular dis- or crossed the baseline and were subdivided into left (e) or
sociation and bundle branch block pattern. The R-wave right (Q patterns. Pattern f was not seen in this study and is from a patient with supraventricular tachycardia.
THE AMERICAN JOURNAL OF CARDIOLOGY DECEMBER 1, 1988 1209
BUNDLE BRANCH BLOCK AND VENTRICULAR TACHYCARDIA
of the sinus rhythm tracings (p <O.OOl). Triphasic pat- An R/S <l in V6 was seen in 80% of VTs and 45% terns were rare and no examples of triphasic right of sinus rhythm tracings with right bundle patterns (p (rsR’) QRS were seen. = 0.067). With left bundle pattern, an R wave in VI or
aVR aVL aVF
FIGURE 2. A left bundle-morphology ventricular tachycardia from a patient in group 2 with a previous anterior infarction. Note the concordance of the precordial QS complexes and the absence of a >30 ms wide R wave in VI or Vs. The axis is in the right
Ill aVR aVL aVF
FIGURE 3. Right bundle QRS morphologies in sinus rhythm (A) and ventricular tachycardia (B) from a patient in group 2. Note the biphasic R wave in Vi in A and the monophasic R wave in VI in B.
1210 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 62
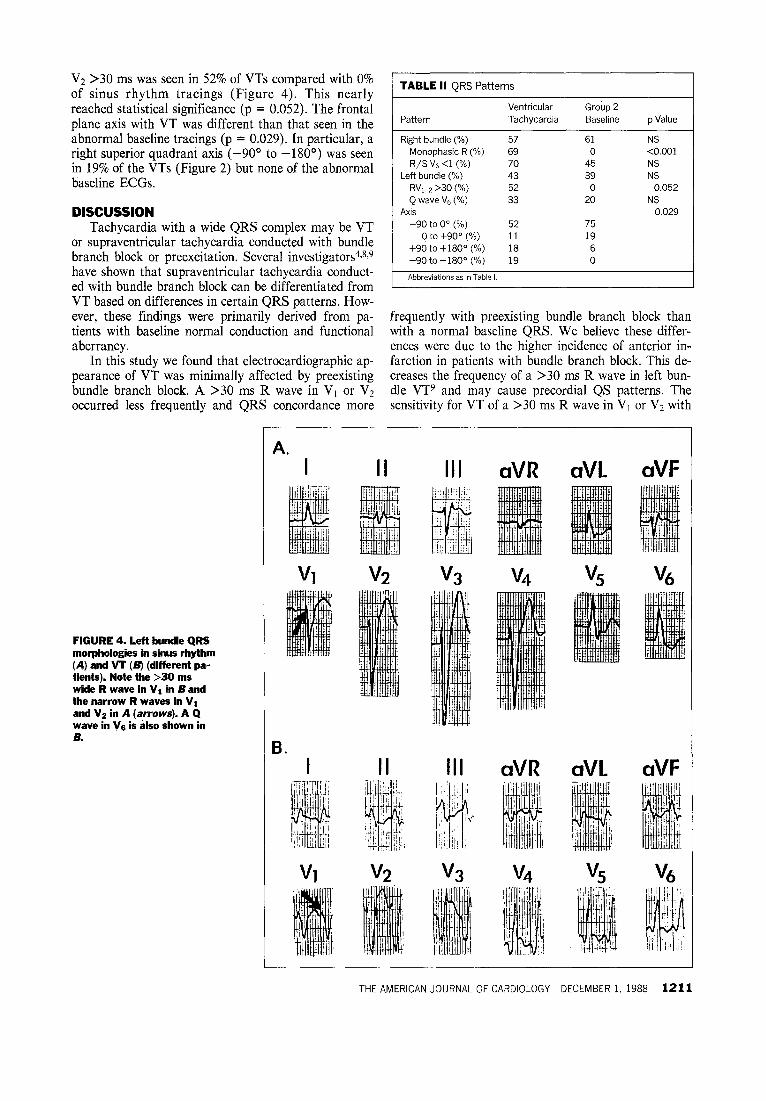
V2 >30 ms was seen in 52% of VTs compared with 0% of sinus rhythm tracings (Figure 4). This nearly
TABLE II QRS Patterns
reached statistical significance (p = 0.052). The frontal Ventricular Group 2
plane axis with VT was different than that seen in the Pattern Tachycardia Baseline p Value
abnormal baseline tracings (p = 0.029). In particular, a Right bundle (%) 57 61 NS
right superior quadrant axis (-90’ to -180’) was seen Monophasic R (%) 69 0 <O.OOl
in 19% of the VTs (Figure 2) but none of the abnormal R/S V6 <l (%) 70 45 NS
baseline ECGs. Left bundle (%) 43 39 NS RV,-7 >30 (%) 52 0 0.052
DISCUSSION Tachycardia with a wide QRS complex may be VT
or supraventricular tachycardia conducted with bundle branch block or preexcitation. Several investigators4J,9 have shown that supraventricular tachycardia conduct- ed with bundle branch block can be differentiated from VT based on differences in certain QRS patterns. How-
Q wave V6 (%%j 33 20 NS Axis 0.029
-90 to 00 (%) 52 75 0 to +900 (%) 11 19
+90 to +180” (%) 18 6 -90 to -180° (“/a) 19 0
Abbreviations as in Table I.
ever, these findings were primarily derived from pa- frequently with preexisting bundle branch block than tients with baseline normal conduction and functional with a normal baseline QRS. We believe these differ- aberrancy. ences were due to the higher incidence of anterior in-
In this study we found that electrocardiographic ap- farction in patients with bundle branch block. This de- pearance of VT was minimally affected by preexisting creases the frequency of a >30 ms R wave in left bun- bundle branch block. A >30 ms R wave in V1 or V2 dle VT9 and may cause precordial QS patterns. The occurred less frequently and QRS concordance more sensitivity for VT of a >30 ms R wave in VI or VZ with
FIGURE 4. Left bundle QRS morphologies in sinus rhythm (A) and VT (B) (different pa- tients). Note the >30 ms wide R wave in VI in B and the narrow R waves in VI and Vz in A (arrows). A Q wave in Vs is also shown in B.
A. I aVR aVL
aVR aVL
aVF
aVF
THE AMERICAN JOURNAL OF CARDIOLOGY DECEMBER 1, 1988 1211

BUNDLE BRANCH BLOCK AND VENTRICULAR TACHYCARDIA
left bundle is therefore diminished by preexisting bundle branch block. However, its absence in preexisting left bundle suggests its specificity is not altered. Similarly, precordial concordance was not evident in any sinus ECG and should therefore be a relatively specific clue to the diagnosis of VT.
In patients with normal baseline QRS patterns and wide QRS tachycardias, Wellens et al8 found that monophasic, biphasic or triphasic left (Rsr’) R-wave patterns in Vt, an R/S <l in V6 with right bundle pat- tern and a Q in V6 with left bundle pattern favored VT. Our study suggests the sensitivity of these criteria are not diminished by preexisting bundle branch block. However, except for a monophasic R wave in VI, these same patterns were commonly seen with preexisting bundle branch block. They therefore cannot be relied upon for diagnosis if the baseline ECG is unavailable for comparison. This is supported by results of a pro- spective study of these criteria by Wellens et allo in which 4 of the 5 misdiagnoses occurred in patients with preexisting bundle branch block. However, a monopha- sic R wave in Vt appears to be a useful clue to the diagnosis of VT even in the absence of knowledge about the baseline QRS pattern.
The value of QRS axis in arrhythmia diagnosis is unclear. Our results suggest that an axis in the right superior quadrant favors VT. No sinus ECG with pre- existing bundle branch block had this axis compared with 19% of VT ECGs.
Several limitations of this study must be mentioned. We analyzed only sinus rhythm ECGs with bundle branch block from patients with sustained VT. By ex- cluding patients without tachycardia, we feel our results are relevant to the clinical problem. In addition, we be- lieve this approach minimized differences that might have been seen if patients with isolated bundle branch block and no arrhythmias had been included. Our tind- ings, therefore, should be relatively specific.
Our grading system may have differed from Wellens et al.* Some QRS complexes graded as monophasic in this study (Figure 1B) may have been classified as tri- phasic by Wellens et al (pattern 5). This probably ac- counts for our low frequency of triphasic patterns and the different proportions of QRS patterns in the 2 stud- ies. However, we do not believe this significantly affects the usefulness of our results since both studies clearly identify those complexes that favor functional aberra- tion (Figure lF, pattern 3 + 4).
Our results were derived from a small, select popula- tion with a high frequency of previous myocardial in- farction. We did not examine arrhythmias due to the Wolff-Parkinson-White syndrome. Therefore, extrapo- lation of our results to different patient populations may be limited.
Most important, we compared QRS patterns during VT to those during sinus rhythm. Unfortunately, we study few patients with supraventricular tachycardia and preexisting bundle branch block, and atria1 pacing at rates comparable to tachycardia was not routinely performed. Since supraventricular tachycardia and VT
1212 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 62
may have virtually identical QRS appearances in the same patient,’ 1 we included only ECGs whose mecha- nism was confirmed at electrical study. However, the QRS pattern during supraventricular tachycardia in pa- tients with preexisting bundle branch block is similar to that observed during sinus rhythmI and supports this approach. Nonetheless, we cannot rule out minor changes in configuration that might occur with tachy- cardia that could affect these results. Drug therapy in some patients may have also altered the QRS pattern. However, patients frequently present with arrhythmias while taking medication and therefore this should not affect the clinical value of our findings.
This study, therefore, does not directly address the electrocardiographic differentiation of VT from supra- ventricular tachycardia with a wide QRS. Nonetheless, our data provide insight into the potential value and limitations of the QRS criteria-derived from studies of VT and supraventricular tachycardia with functional bundle branch block-to arrhythmia diagnosis when no baseline tracing is available, or when the baseline trac- ing shows fixed bundle branch block. In addition to be- ing infrequent in patients with functional aberration, a monophasic R wave in VI, QRS concordance, a right superior axis and a >30 ms R wave in Vi or V2 with left bundle pattern are infrequent in patients with preexist- ing bundle branch block and therefore may be relatively specific for VT. However, these were only seen in 38, 21, 19 and 2376, respectively, of VT ECGs and there- fore show poor sensitivity.
REFERENCES 1. Stewart RB, Bardy GH, Greene HL. Wide complex tachycardia: misdiagnosis and outcome after emergent therapy. Ann Intern Med 1986;104:766-771. 2. Dancy M, Camm AJ, Ward D. Misdiagnosis of chronic recurrent ventricular tachycardia. Lmcet 1985;2:320-323, 3. Morady F, Baerman JM, DiCarlo LA Jr, DeBuitleir M, Krol RB, Wahr DW. A prevalent misconception regarding wide-complex tachycardias. JAMA 1985; 254:2790-2792. 4. Sandier IA, Marriott H. The differential morphology of anomalous ventricular complexes of RBBB-type in lead Vi. Ventricular ectopy versus aberration. Circu- lation 1965;31:551-563. 5. Kistin AD. Problems in the differentiation of ventricular arrhythmias from supraventriculararrhythmia with abnormal QRS. Prog Cardiouasc Dis 1966:9;1- 17. 6. Marriott HJL, Sandier JA. Criteria, old and new, for differentiating between ectopic ventricular beats and aberrant ventricular conduction in the presence of atrial fibrillation. Prog Cardiomsc Dis 1966;9:18-28. 7. Kuchar DL, Thorburn CW, Sammel NL, Garan H, Ruskin JN. Surface electrocardiographic manifestations of tachyarrhythmias: Clues to diagnosis and mechanism. PACE 1988;11:61-82. 6. Wellens HJJ, Blr FW, Lie KI. The value of the electrocardiogram in the differential diagnosis of a tachycardia with a widened QRS complex. Am J Med 1978;64:27-33. 9. Kindwall KE, Brown J, Josephson ME. Electrocardiographic criteria for ven- tricular tachycardia in wide complex left bundle branch morphology tachycardias. Am J Cardiol 1988;61:1279-1283. 10. Wellens HJJ, B%r FW, Vanagt EJ, Brugada P, Farre J. The differentiation between ventricular tachycardia and supraventricular tachycardia with aberrant conduction: the value of the 124ead electrocardiogram. In: Wellens HJJ, Kulber- tus HE, eds. What’s New in Electrocardiography. The Hague: Martinus Nijhoff; 1981:184-199. 11. Ross DL, Vohra JK, Sloman JG. Similar QRS morphology in sinus rhythm and ventricular tachycardia. PACE 1979;2:486-489. 12. Dongas J, Lehmann MH, Muhmud R, Denker S, Soni J, Akhtar M. Value of preexisting bundle branch block in the electrocardiographic differentiation of supraventricular from ventricular origin of wide QRS tachycardia. Am J Cardiol 198X55:71 7-721.