effective electronic medical records: moving beyond · pdf fileeffective electronic medical...
TRANSCRIPT

Global PHAT 2010 – Panel II Session Summary
- 1 -
Panel Session II
EFFECTIVE ELECTRONIC MEDICAL RECORDS: MOVING BEYOND THE TECHNOLOGY www.globalphat.com/panel2.html Saturday, May 1, 2:00pm – 3:15pm Nye, Taubman Building
SUMMARY Electronic medical records (EMR) are growing in prevalence and beginning to change the way medicine is practiced in the developing world, but positive impact on outcomes has been minimal. This panel will discuss technical and ideological differences between the 3 EMRs represented, practical implementation strategies, return on investment, and critical non-technological factors that ultimately determine the success or failure of an implementation. Insights gathered during this session will serve as a starting point for developing framework to guide implementers in the field.
MODERATOR
Jonathan Payne is a graduate student at the Harvard School of Public Health, Department of Health Policy & Management. Jon's academic focus is the utilization of health information systems to improve population health outcomes and promote economic development. Jon recently worked in Honduras designing the technical specifications for a nationwide orphan case file management system.
PANELISTS
Hamish Fraser, MBChB, MRCP, MSc is an Assistant Professor at Harvard Medical School (HMS) and Associate Physician at Brigham and Women's Hospital. As the Director of Informatics and Telemedicine at Partners In Health he leads the development of web-based medical record systems and data analysis tools to support the treatment of drug-resistant tuberculosis and HIV. Dr Fraser is also co-founder of the OpenMRS collaborative.
Bobby Jefferson is Senior Health Informatics Advisor at Futures Group in Washington, DC. He provides information communication technology (ICT) technical leadership providing innovative solutions to support resource limited, rural hospitals treating those most affected by diseases. He provides technical expertise in developing electronic data collection and reporting solutions using cost effective, freely available software tools, as part of the technical solution.
Mike McKay aspires to be a social justice hacker (think MLK + MacGyver). He lived in Malawi from 2005 until 2009, where he was the Country Director for Baobab Health. With one million people living with HIV and fewer than 300 doctors, Malawi needed a new approach to fighting the epidemic. Mike led a team that created an open source, touch screen-based, HIV treatment system to guide minimally trained healthcare workers through the complicated process of treating HIV. This point of care system now provides more than 42,000 Malawians with their HIV treatment.

Global PHAT 2010 – Panel II Session Summary
- 2 -
Session Summary
Panel II – Effective EMR: Moving Beyond the Technology Contributors: Prerna Srivastava, Jonathan Payne, Sugam Bhatnagar
We heard from three different panelists: Mike McKay, former Country Director, Baobab Health; Hamish Fraser, Director of
Informatics and Telemedicine, Partners in Health; and Bobby Jefferson, Senior Health Informatics Advisor, Futures Group.
This session explores design differences between the three EMR systems, and the attendant impact on quality of care and
availability / usability of information, as well as factors related to financial viability. The video and presentations are
available at www.globalphat.com/panel2.html.
The three EMR platforms presented – Baobab Health, OpenMRS, and IQCare – have marked design differences, both on the
front-end and the back-end. As described by Mike McKay, Baobab’s vision is to put a touch screen-based clinical care
workstation at every point of care. Through this system, critical data (ie. WHO protocols) is entered real-time, enabling both
real-time decision support and data quality checks. The number of data elements recorded is relatively small. Currently,
approximately 25% of the population on an ARV drug regimen receives care through the Baobab system, and over a million
patients have been registered using the Baobab system over the past 10 years.
Compared to the Baobab system, OpenMRS operates on a larger scale – in 34 countries – and is customizable based on user
specifications – for example, additional forms and modules can be added to the platform in order to meet country-level data
requirements. Clinical data is typically recorded on paper forms and entered into OpenMRS retrospectively by data entry
clerks. Forms often range from 1 to 5 pages, depending on the type of visit and setting. OpenMRS is used primarily for ART
and TB care, but several sites are either piloting or already using it for primary care.
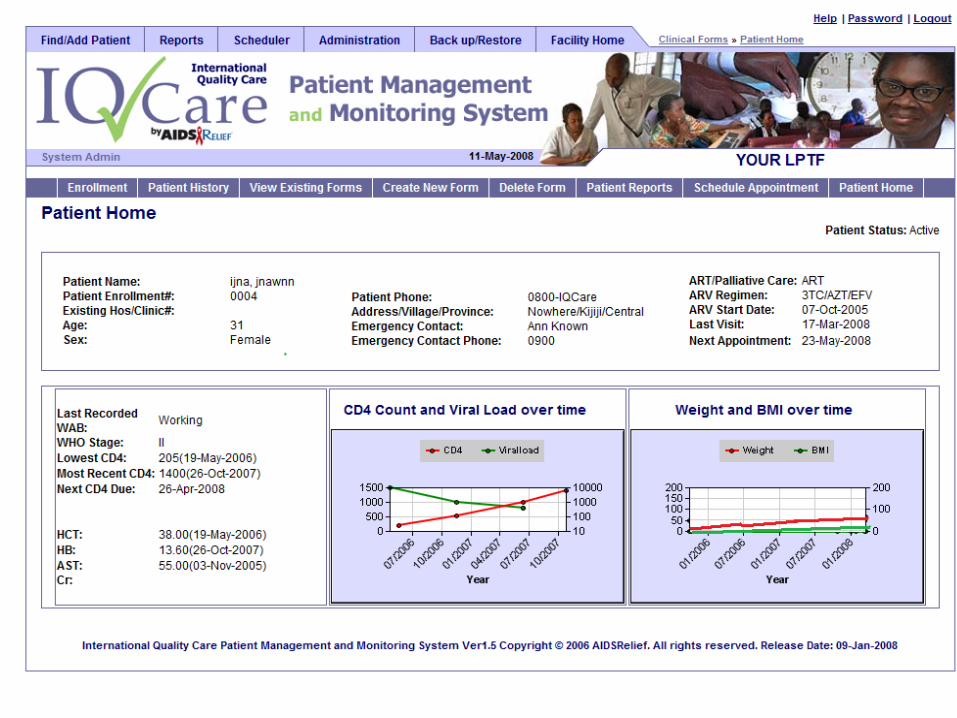
Finally, IQ Care is a patient management and monitoring system that informs decision-making at the clinician and program
manager level. For example, based on patient data, IQ Care can perform a workload analysis, and provide data that can then
inform decisions regarding how best to allocate human resources to various tasks. IQ Care utilizes GoogleMaps in order to
track geographical drug adherence patterns, and provides decision support regarding which geographic regions to target for
future drug adherence related interventions. IQCare is used in 10 countries at 244 sites and hospitals.
A comparison of these 3 platforms raises further questions regarding the strengths and drawbacks of data entry at the point of
care vs. retrospective data entry, out-of-box solutions vs. modular platforms that enable significant customization and
adaptability. What settings are most suited for Baobab as opposed to OpenMRS or IQCare and how does an implementer
make this choice?
The second issue that was raised during the panel was related to financial viability - for example, how is the break-even point
defined in the context of the above three systems? Is there a financial reason for implementing EMR, in terms of cost-
savings, and at what point in terms of patient-load / staff ratio? In response to these questions, Mike McKay provided
concrete figures – for example, it costs $4 / patient / year in order to implement the Baobab system, and the government of
Malawi has $300 / ARV patient / year through the Global Fund for HIV care. The Global Fund dictates that 10% of this
funding, or $30 / patient, should go towards M&E. Dr. Fraser did not provide the panel with concrete figures, but he raised
some interesting points regarding costs – for example, data entry costs represent the bulk of overall costs for implementation,
as well as redundancies related to multiple entries of the same information. Dr. Fraser also differed on the point of when
clinics start to struggle with the scalability of a paper-based system in terms of report generation, patient data tracking, and
drug report generation. He claimed the breakeven point for implementing EMR is closer 500 patients, as opposed to McKay’s
number, which was 2000 patients.
Additional Questions for further discussion:
How do country-level or donor-specific data requirements dictate the type of electronic medical record (EMR) system that is
implemented on a national level? How does EMR fit into the monitoring and evaluation (M&E) framework? What are the
implications of real-time data entry v. back-end data entry, or a standardized EMR platform v. an adaptable, customizable
EMR platform? How do we determine the break-even point for EMR systems in terms of financial viability? How is M&E
defined in the context of EMR? How can cost savings realized as a result of EMR be quantified, both in the short-term and
the long-term? What are the major cost drivers, and how can these be addressed?

Bobby Jefferson
Senior Health
Informatics
Advisor
Public Health and
Consortium
Nigeria, Kenya, Uganda, Tanzania, Rwanda, Zambia, South Africa, Haiti
Guyana, Ethiopia 244 ART sites 112 Satellites 400 PMTCT sites
Rural, remote, faith based mission hospitals “serving poorest of poor”
No power, intermittent power, No IT staff, No internet, Sparse mobile coverage
Nurses, Clinicians, Adherence Counselors, need health data, M&E program
data in knowledge repository
Lack of referrals or linkage to existing technology systems
Cost effectiveness and sustainability -- no funds for proprietary licenses, or
yearly maintenance fees


Futures GroupeHealth mHealth approach
creative common approach Use of freely available, reusable, tools
Offline Solutions, Disconnected model
Reusable software and technology across countries and programs
Programmers and IT staff in country
Low costs, Inexpensive $200-$300 NetbooksSolar mobile phones, SMS,


Workload Analysis : Over worked Uganda Example
237 237
445496
652
811887 898 903
965
1,185
1,359
1,472
1,5891,651
1,718
1,816
1,019
0
200
400
600
800
1,000
1,200
1,400
1,600
1,800
2,000
# o
f fo
rm
s co
mp
ute
ris
ed
/
M&
E O
ffic
er / m
on
th
LPTF
Data management workload at LPTFs 3 month average (Jan- March 2009)
per M&E Officer
Should consider hiring additional M&E Officer soon. Congratulations
to the current M&E Officers for successfully coping with the high
Note: A competent M&E Officer should easily manage at least 1260 forms / month (~60
forms/day)
LPTFs have made great efforts to clear their backlog and maintain real
timely data entry. Well done
LPTFs urgently needs an aditional
M&E Officers, It is fond of backlogs
MTCT+ & Private Clinic Enter other programs
Competent M&E Team, Congratulations and keep up
LPTF Should start entering all HIV Care and urgently needs an additioal full time M&E Officer
Data Clerk Surge Team

Example: Impact of Staff Attrition at LPTF A
During the past 18 months Site A has lost several staff:
o 2 doctors (1 doubled as the Project Coordinator )
o2 Clinical Officers
o1 adherence nurse
o2 M&E officers
o1 counselor
Many of these have just been replaced and receiving orientation & training
As a result of the attrition one Area affected by the departure of long serving, trained staff - adult enrolment has gone down tremendously as seen on graph to the right.
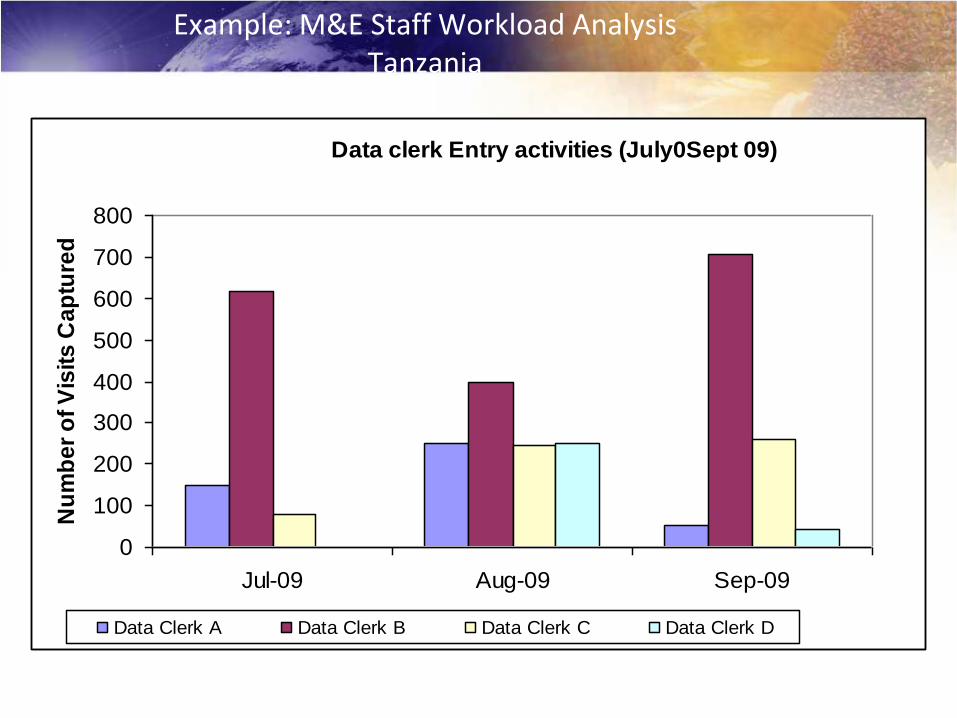
Example: M&E Staff Workload Analysis Tanzania
Muheza DDH Data clerk Entry activities (July0Sept 09)
0
100
200
300
400
500
600
700
800
Jul-09 Aug-09 Sep-09
Nu
mb
er
of
Vis
its
Ca
ptu
red
Data Clerk A Data Clerk B Data Clerk C Data Clerk D
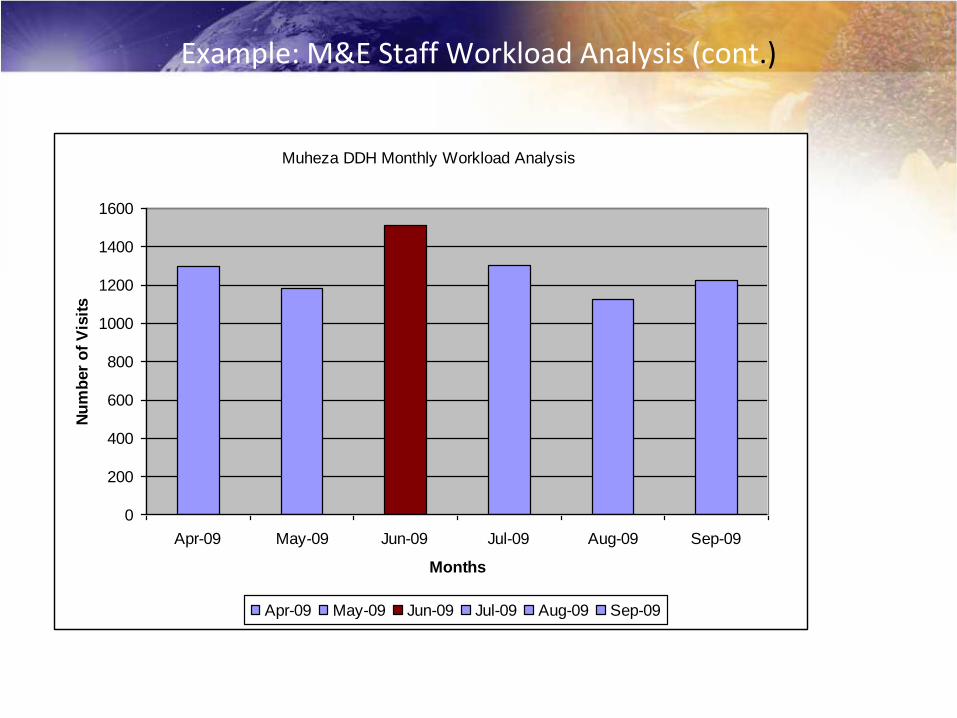
Example: M&E Staff Workload Analysis (cont.)
Muheza DDH Monthly Workload Analysis
0
200
400
600
800
1000
1200
1400
1600
Apr-09 May-09 Jun-09 Jul-09 Aug-09 Sep-09
Months
Nu
mb
er
of
Vis
its
Apr-09 May-09 Jun-09 Jul-09 Aug-09 Sep-09

Rwanda Team

6.4%
3.0%
1.3%
0.4% 0.4% 0.2% 0.3% 0.2% 0.1% 0.0% 0.1%0.5%
0.1% 0.2% 0.2%
0%
1%
2%
3%
4%
5%
6%
7%
Aug-08 Oct-08 Dec-08 Feb-09 Apr-09 Jun-09 Aug-09 Oct-09
N = 3,721 as of October 09
Missed ARV pickup >20 Days

ARV pick-up analysis: Reduction in number of missed appointments (Uganda)
868
654
296 296
483
221
377
285
169 155 150120
100 101
June 08 July 08 Aug 08 Sept 08 Oct 08 Nov 08 Dec 08 Jan 09 Feb 09 Mar 09 Apr 09 May 09 June 09 July 09
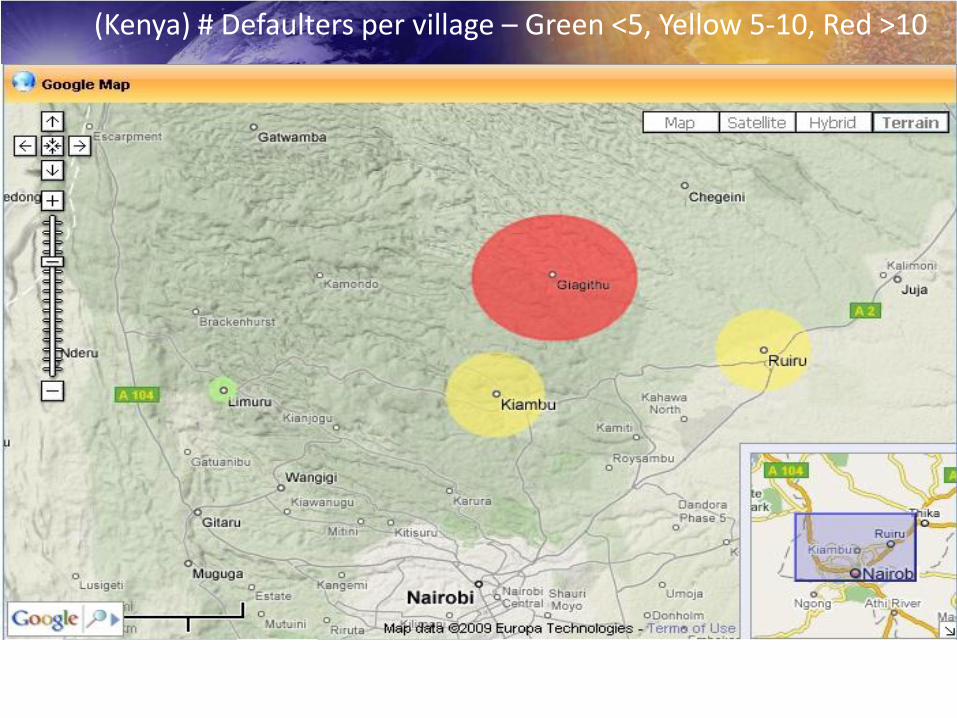
(Kenya) # Defaulters per village – Green <5, Yellow 5-10, Red >10
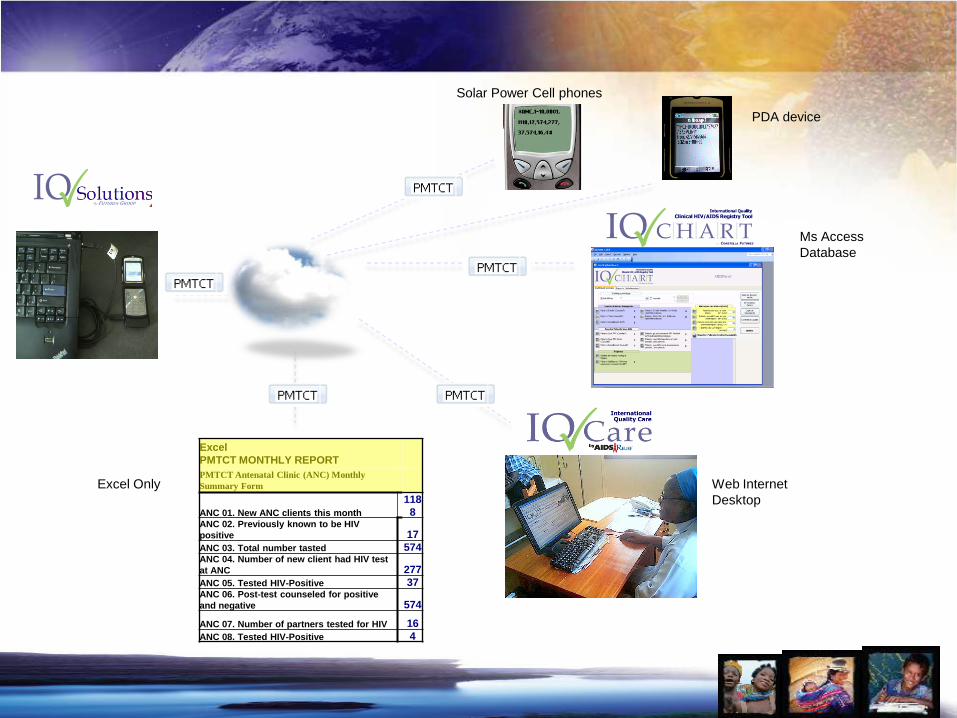
Excel
PMTCT MONTHLY REPORT
PMTCT Antenatal Clinic (ANC) Monthly
Summary Form
ANC 01. New ANC clients this month
118
8ANC 02. Previously known to be HIV
positive 17
ANC 03. Total number tasted 574ANC 04. Number of new client had HIV test
at ANC 277
ANC 05. Tested HIV-Positive 37ANC 06. Post-test counseled for positive
and negative 574
ANC 07. Number of partners tested for HIV 16
ANC 08. Tested HIV-Positive 4
Solar Power Cell phones
Ms Access
Database
PDA device
Web Internet
Desktop
Excel Only
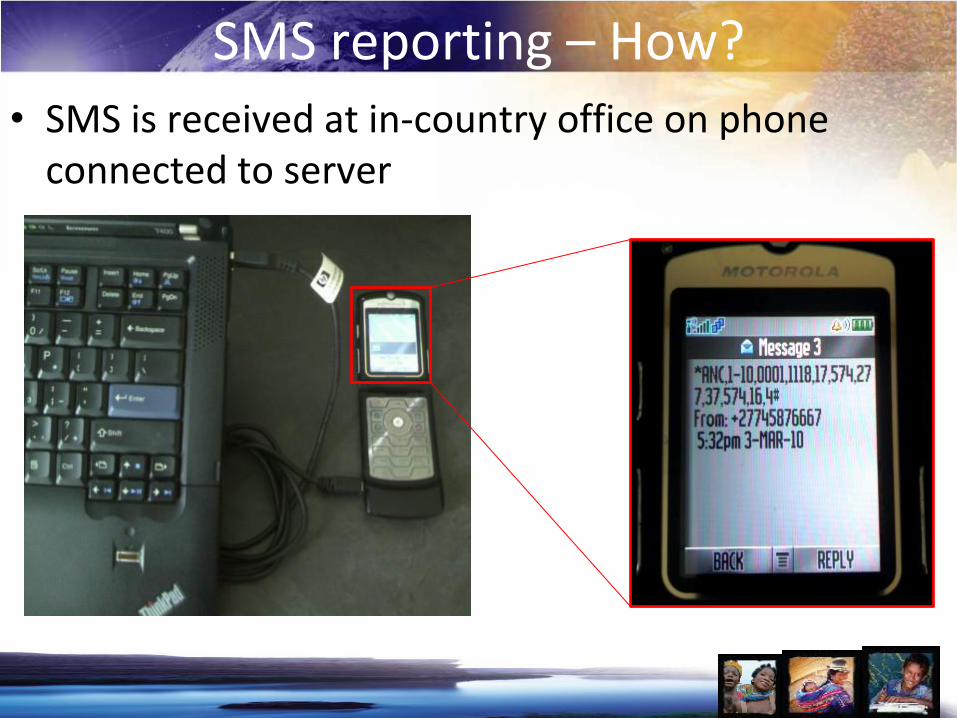
SMS reporting – How?• SMS is received at in-country office on phone
connected to server

RebeccaOlivia


“AIDSRelief has given me the drugs to stay healthy, and it’s helped my family and many
other children too.” Rebecca Ushindi

Futures Group
“After successful assessment, the IQ Care system developed and supported by the Futures
Group and Catholic Relief Services came up top in terms of overall features (technical and non
technical) and also in terms of largest number of installations “
WHO sponsored EMR Assessment Report ,
Kenya May 2009
Rwanda
ICAP Columbia University 44 sites
Intra Health International 17 sites
Elizabeth Glaser EGPAF 16 sites
Family Health Inter FHI 45 sites
Catholic Relief Services 13 sites
Kenya
Catholic Relief Services 28 sites
Pathfinder International
Gertrude Children Hospital
Catholic Relief Services 20
John Snow International
Rakai Health Services Vaccine Research
Uganda
Intra Health International Southern Sudan
Mennonite Christian Charities
Catholic Relief Services 27 sites
Nigeria

Futures GroupThank You
Bobby Jefferson bjefferson @ futuresgroup
Lanette Burrows lburrows @ futuresgroup
Futures SI Advisor in-country
www.futuregroup.com
www.iqstrategy.net

Effective EMRs: Moving Beyond
the Technology
Dr Hamish SF FraserPartners In Health
Division of Global Health Equity, BWH
Harvard Medical School

Physician looking up ARV patient

Evaluation of access to CD4 counts
• The proportion of CD4 counts conducted
within the past 60 days but unknown to the
clinician at the time of consultation was:
• 24.7% in the pre-intervention period
• 16.7% in the post intervention period
• This is a 32.4% reduction in CD4 loss
(p=.002)
• We will evaluate the effect of direct
clinician access to the EMR next
Amoroso C, et al: Medinfo2010 in press

Detecting kids with HIV
• On a weekly basis, an automated report is produced that
lists all children of HIV positive parents enrolled in the
program who have not been tested for HIV as reported
by their parent.
• In six months 178 children found and tested, 122 testing
HIV negative and 15 found to be HIV positive, (41
currently awaiting results).
• All positive children started on ARV treatment
Systematic review of
evaluation studies
Health Affairs 2010, 29;2: 244-251

Developer training, Rwanda
• Training program in Kigali for computer science graduates
• One year, mentored training course
– Web development
– Java programming
– OpenMRS programming
– Medical informatics
• Ten students graduated last fall
• Now supporting OpenMRS rollout
as well as building software development capacity in
Rwanda
International Development Research Center
