effective use of educational technology in medical education · pdf fileeffective use of...
TRANSCRIPT

Effective Use of EducationalTechnology in Medical EducationColloquium on Educational Technology:Recommendations and Guidelines forMedical Educators
AAMC Institute for Improving Medical Education
March 2007

To request additional copies of this publication, please contact:
Chris Candler, M.D.Director of Educational Technology, Medical EducationAAMC2450 N Street, N.W.Washington, D.C. 20037T 202-828-0253 F [email protected]
©2007 by the Association of American Medical Colleges. All rights reserved.
Case Study 1
A biochemistry course director receives a grant to develop a Web site for teaching first-year medicalstudents in metabolic pathways. To better understand typical student perception and performance, heholds a student feedback session and analyzes pre-test scores. Before selecting a technical approach, heconsults other basic scientists and clinicians to ensure that the educational objectives are relevant,well-organized, and integral to other elements of the curriculum. A professional educator with technologyexpertise is consulted to carefully analyze the objectives and suggest an appropriate instructional strategy.The decision is made that use of the Web site will be mandatory for all students enrolled in the course.
The instructor apportions content into topic-based chapters organized around patient cases, which aredesigned to focus learner attention and integrate various concepts. Each chapter begins with a descriptionof the learning objectives and a brief tutorial to stimulate recall of relevant prerequisite information. Thematerial is presented through interactive animation using Mayer’s ten principles of effective multimedia.Learners are occasionally given advice and tips for learning particularly difficult concepts. Each chapterends with a succinct summary and practice problems. The last section of the Web site offers a sampleexam with multiple-choice questions derived from each of the learning objectives. Learners are providedindividualized feedback based on their performance.
The instructor provides appropriate basic science and clinical faculty with links to the Web site and helpsthem understand how they can use relevant content. The instructor uses student feedback to furtherrefine the site.

Executive Summary
Medical educators increasingly use technology tosupplement the delivery of learning resources.The advent of multimedia technology, the WorldWide Web and the ubiquitous nature of networkedcomputers, have transformed educational technologiesfrom esoteric legacy applications used by a fewpioneering faculty to mainstream applicationsintegral to the medical school educationalenterprise. This increased use is reflected in thegrowing number of publications and conferencepresentations related to educational technology.
There is no doubt that educational technologieshave enhanced teaching and learning in medicaleducation. There is also no doubt that technologieswill continue to evolve and become furtherintegrated into all facets of our professional andpersonal settings. The medical educationcommunity must be able to assure itself that theinformation presented to medical students and thevenues through which it is presented are compatibleand optimize learning and justify the substantialinvestment of resources (people, facilities, money)that these resources require. For medical schools to“make the case” for such investments it is imperativethat use of technology be linked to what we knowabout learning. Often there is a “cultural lag” inappropriately pairing novel technology witheffective use, making it essential that medicaleducators be confident that educational theoryguides and supports their use of technology.
AAMC’s Institute for Improving Medical Educationconvened an invited colloquium of national expertsto consider the state of research and documentedefficacy of educational technologies in the medicalschool curriculum. Indeed these participantsconfirmed that more evidence is needed to determineprecisely when to employ technology during themedical education process and how best to use itwhen it is employed. This summary report offers theconsensus of the IIME expert panel around theseissues, suggests recommendations on how best toutilize available technologies in the medicaleducation setting, and proposes research questionsto further guide our understanding and advancethe established literature.
Carol A. Aschenbrener, M.D.Executive Vice President
Effective Use of EducationalTechnology in Medical Education
Association of American Medical Colleges, 20073

Background
Educational technology tools offer compellinginstructional capabilities and provide faculty andstudents with new educational possibilities. Theseresources can portray anatomical and physiologicalprocesses with remarkable clarity, tailor instructionto learner needs, allow learners to practice skills ina safe environment, standardize instruction andassessment activities, and be offered anywhere andanytime. Furthermore, today’s learners areaccustomed to technology-enhanced learningenvironments.
Educational technologies are used extensively at allpoints on the medical education continuum and varywidely in complexity, degree of realism, and cost.Such resources include relatively straightforwardonline multimedia tutorials; high-fidelity virtualpatient applications that ask learners to diagnoseand manage simulated patients; and immersive,team-based simulations designed around lifelikemannequins. Many institutions have purchasedcommercial products developed for the medicaleducation market, while others have created in-house development teams of educators, illustrators,Web designers, programmers, and other multimediaspecialists, who create excellent products for theirown use.
The widespread adoption of information technologieshas led to a corresponding growth in the develop-ment of sophisticated, realistic teaching resources.However, our understanding of how these resourcesmight best be incorporated into the curriculum isinadequate, as advances in what could be createdoften outpace our ability to understand how theyshould be developed or used. While a variety ofcompelling studies in the medical educationliterature have described new applications andoccasionally compared their effectiveness withtraditional instructional approaches such as lectures,they generally do not examine which technologyapproaches are best suited for a given educationalgoal. Fortunately, several studies in the educationaland cognitive sciences offer evidence-based principlesthat might be used to guide the effective use oftechnology in medical education.
The AAMC Educational Technology ColloquiumThe Association of American Medical Colleges(AAMC) has a longstanding interest in the use ofeducational technology by its institutional members.To facilitate the use of effective educationaltechnologies in medical education, the AAMC’sInstitute for Improving Medical Education chargeda panel of experts to consider the current use ofcertain educational applications at medical schools,and to examine the relevant literature in order todevelop recommendations that could be used tohelp medical schools select, develop, and useappropriate technologies.
In April 2006, the institute convened recognizedexperts in educational technology to participate ina one-day colloquium, charged with three specificgoal;
1. Identify the advantages that educationaltechnologies provide over traditional approaches
2. Recommend the educational theories, principles,and features that should be considered whendeveloping or purchasing educational technologies
3. Suggest directions for future research
Because the overall technology topic is so broad,colloquium participants were charged to focusconsideration on interactive instructional andassessment applications: namely, those that teach orassess understanding of biomedical concepts,patient diagnosis and management, and proceduralskill training. Resources with little interactivity—such as those that only enable basic learnernavigation of text and images—were consideredless relevant to the colloquium’s scope. Likewise,the group did not discuss delivery systems such asteaching management systems (e.g., BlackBoard),pod-casting, computer-based testing, digitizedlecture dissemination, and distance learning.
With a few notable exceptions, the bulk ofeducational technology research in the medicaleducation literature has been criticized as deficientin either methodological approach, conceptualframework, or both. However, scores of rigorousstudies have been published in the fields of
Effective Use of EducationalTechnology in Medical Education
Association of American Medical Colleges, 20075

educational psychology, cognitive science, informationscience, military and aviation training, andeducational technology. The colloquium participantsagreed to consider the seminal literature from eachof these fields and suggest principles that may bereasonably inferred from them.
This report summarizes the findings of the April2006 Colloquium on Educational Technology heldin Washington, D.C. The report does not prescribea single educational technology approach that canbe adopted in all learning environments, nor is it aformal analysis of the literature. Instead, it offersprinciples and recommendations derived frommultiple disciplines and perspectives. Notably, thisreport highlights the essential role of instructionaldesign principles to promote the effective use ofeducational technology.
The primary audience for this report is medicalschool teaching faculty members who develop,purchase, or use educational technology to enhancelearning. A secondary audience is staff memberswho support the development, procurement, andimplementation of these applications.
Advantages of Educational TechnologiesEducational technologies provide instructors withnumerous advantages in the areas of contextuallearning, active and individualized learning, andautomation.
Technology can reproduce an object or concept in aform that may be manipulated by the designer and,ideally, the user for educational purposes. Theseadvantages are particularly clear in simulationtechnologies and can also exist with computer-based models of real-life processes. Exploration in arealistic environment provides multiple benefits tolearners: opportunities to practice rare and criticalevents, safe and controlled environments thateliminate risk to patients, enhanced visualization,and authentic contexts for both learning andassessment. In these environments, assessment oflearner behavior and outcomes can be documented.
Modern educational technologies can processlearner decisions and present realistic responses toprovide an individualized learning experience.Educational technologies attuned to the characteristicsof adult learners promote active, student-centeredlearning. Instruction can also be tailored to individualneeds by empowering learners to control theireducational experience, including opportunities forrepetition and deliberate practice with structuredguidance. These principles apply to both group andindividual instructional settings.
Because of their automated nature, educationaltechnologies provide perpetual resources thatuncouple instruction from physical space constraintsor instructor availability. These tools can facilitatestandardized instruction and assessment and offernew economies of scale, despite the higher initialinvestment likely to be required.
Effective Use of EducationalTechnology in Medical Education
Association of American Medical Colleges, 20076
Educational technologies are advantageous in providing:
• safe, controlled environments that eliminate risk to patients• enhanced, realistic visualization• authentic contexts for learning and assessment• documentation of learner behavior and outcomes• instruction tailored to individual or group needs• learner control of the educational experience• repetition and deliberate practice• uncoupling of instruction from place and time• standardization of instruction and assessment• perpetual resources and new economies of scale

Common Technologies in Medical EducationThere are numerous frameworks that may be usedto characterize and classify educational technologyapplications. Colloquium participants consideredthree broad categories based on the predominantusage in medical education. While these applicationsoverlap in terms of technology components andinstructional possibilities, they are sufficientlydistinctive to consider independently:
1. Computer-aided Instruction (CAI)—Instructionin which computers play a central role as themeans of information delivery and directinteraction with learners (in contrast to applicationssuch as PowerPoint); to some extent humaninstructors are replaced. These programs maymake use of Internet technologies (Web-basedlearning), and include a wide variety ofstandalone applications or online materials.
2. Virtual Patients (VP)—A specific type of com-puter-based program that simulates real-life clinicalscenarios; learners emulate the roles of healthcare providers to obtain a history, conduct aphysical exam, and make diagnostic andtherapeutic decisions.
3. Human Patient Simulation (HPS)—The use ofmannequins or models to simulate patient careenvironments for instructional or assessmentpurposes. Tools in this category include task-basedtrainers that simulate specific procedural tasks(e.g., virtual reality colonoscopy trainers).
Each of these approaches has advantages anddisadvantages (see Table 1) based on its inherenttechnical capabilities.
Effective Use of EducationalTechnology in Medical Education
Association of American Medical Colleges, 20077
Type of Instruction
Computer-aidedInstruction
Virtual Patients
Human PatientSimulation
Advantages
• Useful for visualizing complex processes• Independent exploration of complex phenomena• Easy access• Relatively low-cost of production
• Encompasses multiple aspects of clinical encounter• Longitudinal and multidisciplinary care lessons• Easy access• Readily customized
• Immersive, active experience• Engages emotional and sensory learning• Fosters critical thought and communication• Animates basic science in clinical context
Disadvantages
• Limited physical interactivity• Limited fidelity
• Limited physical interactivity• Limited fidelity• High production costs
• Cost and space requirements• Limited to simulator and staff availability• Engineering limitations
Table 1. Advantages and disadvantages of various educational technologies.
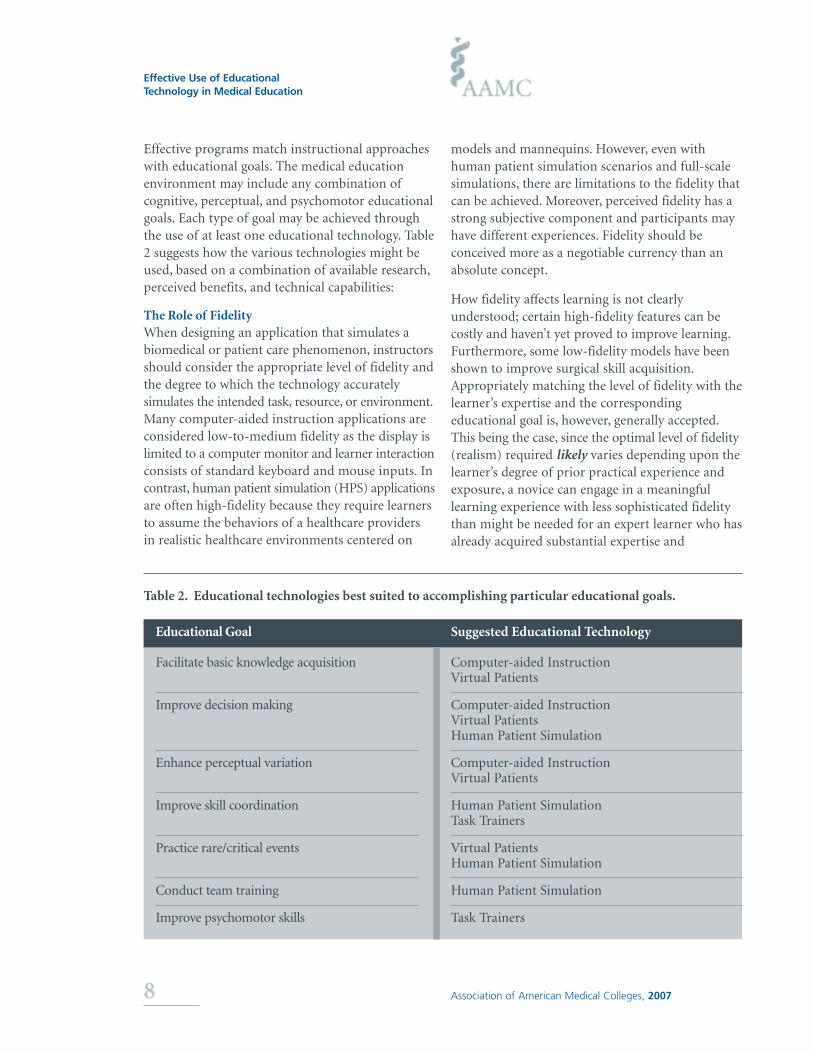
Effective programs match instructional approacheswith educational goals. The medical educationenvironment may include any combination ofcognitive, perceptual, and psychomotor educationalgoals. Each type of goal may be achieved throughthe use of at least one educational technology. Table2 suggests how the various technologies might beused, based on a combination of available research,perceived benefits, and technical capabilities:
The Role of FidelityWhen designing an application that simulates abiomedical or patient care phenomenon, instructorsshould consider the appropriate level of fidelity andthe degree to which the technology accuratelysimulates the intended task, resource, or environment.Many computer-aided instruction applications areconsidered low-to-medium fidelity as the display islimited to a computer monitor and learner interactionconsists of standard keyboard and mouse inputs. Incontrast, human patient simulation (HPS) applicationsare often high-fidelity because they require learnersto assume the behaviors of a healthcare providersin realistic healthcare environments centered on
models and mannequins. However, even withhuman patient simulation scenarios and full-scalesimulations, there are limitations to the fidelity thatcan be achieved. Moreover, perceived fidelity has astrong subjective component and participants mayhave different experiences. Fidelity should beconceived more as a negotiable currency than anabsolute concept.
How fidelity affects learning is not clearlyunderstood; certain high-fidelity features can becostly and haven’t yet proved to improve learning.Furthermore, some low-fidelity models have beenshown to improve surgical skill acquisition.Appropriately matching the level of fidelity with thelearner’s expertise and the correspondingeducational goal is, however, generally accepted.This being the case, since the optimal level of fidelity(realism) required likely varies depending upon thelearner’s degree of prior practical experience andexposure, a novice can engage in a meaningfullearning experience with less sophisticated fidelitythan might be needed for an expert learner who hasalready acquired substantial expertise and
Effective Use of EducationalTechnology in Medical Education
Association of American Medical Colleges, 20078
Educational Goal
Facilitate basic knowledge acquisition
Improve decision making
Enhance perceptual variation
Improve skill coordination
Practice rare/critical events
Conduct team training
Improve psychomotor skills
Suggested Educational Technology
Computer-aided InstructionVirtual Patients
Computer-aided InstructionVirtual PatientsHuman Patient Simulation
Computer-aided InstructionVirtual Patients
Human Patient SimulationTask Trainers
Virtual PatientsHuman Patient Simulation
Human Patient Simulation
Task Trainers
Table 2. Educational technologies best suited to accomplishing particular educational goals.

experience. While not definitively substantiated,Figure 1 illustrates the conventionally positedrelationship of optimal level of fidelity along thenovice, experienced, and expert learner continuum.
Evidence-Based Features and Practices that PromoteEffective Learning
Multimedia(computer-aided instruction, virtual patients)
When designing or purchasing an educationaltechnology resource that contains multimediacomponents, particular attention should be paid tothe selection, sequencing, and presentation ofinformation. Certain elements can induce cognitiveoverload and detract from learning, such as thepresentation style of information and the appropri-ateness of the learning material. Thus, one challengeof effective instructional design is creating applicationsthat include only those features that promote learningwhile avoiding gratuitous elements that may distract.Richard Mayer’s widely accepted ten instructionalmultimedia principles can offer medical educatorsguidance on the application of multimedia
components in educational interventions in order tomaximize the positive effects for optimum studentlearning. With these principles in mind, instructionalmultimedia should conform to the following:
1. Coherence Principle—Exclude extraneous words,pictures and sounds.
2. Pre-Training Principle—Ensure students possessprior knowledge about names and characteristicsof the main concepts.
3. Spatial Contiguity Principle—Presentcorresponding words and pictures in closeproximity to one another.
4. Temporal Contiguity Principle—Presentcorresponding words and pictures simultaneouslyrather than successively.
5. Signaling Principle—Highlight important words.
6. Redundancy Principle—Pair animation andnarration together without on-screen text.
7. Voice Principle—Use non-accented humanspoken voice for narration over a machinesimulated or foreign-accented human voice.
8. Personalization Principle—Employ conversationalstyle, instead of formal, to present words.
9. Segmenting Principle—Offer narrated animationin learner-paced segments rather than acontinuous unit.
10. Modality Principle—Pair animation andnarration together instead of pairing animationand on-screen text.
Simulation(virtual patients, human patient simulation)
An increasing number of specialized programs inmedical education employ high-fidelity simulations.They vary in how technology is utilized, howinstructors are engaged, and the extent to which thesimulation activity is incorporated into thecurriculum. Because they can be costly, investmentsin high-fidelity simulations usually demand evidenceof positive results. A recently published qualitative,
Effective Use of EducationalTechnology in Medical Education
Association of American Medical Colleges, 20079
Expert
Experienced
Most cost-effectiveBest learning
Novice
Low Fidelity (realism) High
Hig
hN
oneIn
itia
lLe
arn
ing
Figure 1. The hypothesized relationship betweenlevel of learner and degree of fidelity. Thisdiagram suggests that the optimal level offidelity may change with the learner’s level ofexperience. Diagram adapted from Alessi S.Fidelity in the Design of InstructionalSimulations. Journal of Computer-BasedInstruction. 1988; 15: 40-47.
systematic review—spanning 34 years and 670peer-reviewed journal articles—identified 10characteristics of effective high-fidelity medicalsimulations in a range of specialties, includinganesthesiology, cardiology, and surgery. Manycharacteristics are consonant with Ericsson’s modelof deliberate practice for mastering professionalperformance. Although this list was derived fromresearch on high-fidelity simulation, many principlesmay well apply to virtual patients.
1. Feedback—Formative and constructive feedbackof performance is the single most importantfeature of simulation-based medical education. Itis the most important factor in ensuring skillstransfer to patient settings and helps slow thedeterioration of skill over time.
2. Repetitive practice—Opportunities for learnersto engage in focused, repetitive practice with theintent of skill improvement, not idle play, is anessential learning feature. This factor is alsoessential to ensuring skills transfer to actualpatients; the practice “dose” should be determinedby learners’ needs, not instructors’ demands.
3. Curriculum integration—Simulation-basededucation should not be an extraordinary activity,but built into learners’ routines and requiredtraining schedules, and grounded in the wayslearner performance is evaluated. Simulationshould also be fully adopted within the broadermedical school educational program and notdependent on a single “champion,” who often hascompeting research or patient care responsibilities.
4. Range of difficulty level—Learning is enhancedwhen learners have opportunities to engage inmedical skills practice across a wide range ofdifficulty levels. Helping learners master skills atincreasingly difficult levels slows their deteriorationof skills over time.
5. Multiple learning strategies—Ideally,simulations should offer a variety of educationalstrategies including large groups (e.g., lectures),facilitated small groups (e.g., tutorials), andboth individual and small-group learningwithout an instructor. The strategies adoptedshould be determined by the desired outcomes,the available resources, and the institution’seducational culture.
6. Capture clinical variation—High-fidelity medicalsimulations that capture or represent a widevariety of patient problems or conditions aremore effective than simulations having a narrowpatient range. This provides more “contextualexperiences” that are critical for obtainingproblem-solving skills.
7. Controlled environment—In a controlled clinicalenvironment, learners can detect and correctpatient care errors without adverse consequences,while instructors can focus on learners ratherthan patients.
8. Individualized learning—Learners’ opportunitiesfor reproducible, standardized educationalexperiences in which they are active participants,not passive bystanders, is an important feature.
9. Defined outcomes or benchmarks—Learners aremore likely to master key skills if outcomes aredefined and appropriate for their training levelprior to the simulator exercise.
10. Simulator validity—A high degree of realism orfidelity provides an approximation of complexclinical situations, principles, and tasks and isessential to help learners increase their perceptualskills and to sharpen their responses to criticalincidents. Although it is important to note thatthe desired outcome should be matched with theappropriate degree of fidelity. Many competenciescan be learned and mastered with relativelylow-fidelity simulators.
Effective Use of EducationalTechnology in Medical Education
Association of American Medical Colleges, 200710

Faculty Development and TrainingThe effective use of technology in medical educationis in large part dependent on faculty readiness. Thisis especially true for sophisticated mannequin-baseddevices and virtual reality environments that mayinvolve physiological responses to drug administrationand drug interaction, interpretation of three-dimensional visual displays, and interpersonal conflictwithin medical teams. Medical faculty should beprepared in at least two ways to insure optimal useof these educational technologies: they must beskilled in the technical operation of simulators andother devices, and know how to employ thetechnologies to facilitate learning and assessment.
Expertise in clinical teaching is necessary within asimulated clinical environment but is not sufficient,as there are important differences in the twosettings. Faculty training in the specific demands ofsimulation-based teaching is key, especially withhigh-fidelity settings utilizing human patientsimulation technology.
These demands go beyond an understanding ofsimulator technology. In clinical teaching, patients’needs always take priority. In simulation-basedteaching, learners’ needs become central, dramaticallyaltering the emphasis of the encounter. This shiftmay have a significant impact on teaching style andshould be explicitly addressed.
Moreover, approaches to debriefings, feedback, andlearner support within a simulation may differfrom those employed by teachers in clinical practice.Considerable support may be needed to helpclinicians function effectively in simulated settings.
Faculty use of educational technology to maximumadvantage will not occur by chance or seniority.The academic medical community should developcompetency-based faculty training and certificationprograms in the use of advanced educationaltechnologies. The programs should teach thetheoretical underpinnings of educational technology,coupled with practical expertise in specificapproaches. Just as the weight of evidence showsthat clinical experience alone does not determine thequality of an individual’s delivery of health care,
medical faculty competence in educationaltechnologies should be assured, not assumed. Inmany cases, specialists with formal training ininstructional design can serve as useful advisors tofaculty content experts.
In addition, certified training expertise should beavailable to various health professionals, as physiciansare not the sole source of medical education.Clinicians in physical therapy, respiratory therapy,specialized nursing, and surgical support, amongothers, should be eligible for training and certification,especially for simulator operation.
Putting it All TogetherThere is clearly no single theory or set of principlesto guide the practical use of technology in medicaleducation. Researchers have proposed dozens offrameworks and models. Ideally, the effective use ofeducational technology should begin with theclassic instructional design approach, a systematicmethod of analyzing learner needs and developingappropriate instructional activities. The ‘ADDIE’framework is commonly used to help organize aneducational technology project. The acronymrepresents the following steps:
Analyze Analyze relevant learner characteristicsand tasks to be learned
Design Define objectives and outcomes; selectan instructional approach
Develop Create the instructional materials
Implement Deliver the instructional materials
Evaluate Ensure that the instruction achievedthe desired goals
Effective Use of EducationalTechnology in Medical Education
Association of American Medical Colleges, 200711
The design, development, and implementationphases of this process have been further extendedby educational psychology researchers. RobertGagné’s Nine Events of Instruction constitutes oneinstructional design framework:
1. Gain attention—Capture learners’ attention bypresenting a problem, a case, a compellingquestion, or an interesting statistic. Focus learners’attention so they will be engaged by the material.
2. Inform learners of educational objectives—Convey expectations to learners by introducingthe educational objectives. Consider describingthem in terms of specific knowledge, skills, orbehaviors that learners are expected to acquire.
3. Stimulate recall of prior knowledge—Helplearners build on what they already know byreminding them of prior knowledge (previousmaterial, personal experience, etc.) that isrelevant to the current material.
4. Present the material—Present logicallyorganized information (or practice) to avoidcognitive overload. Consider incorporatingMayer’s principles for the effective use ofmultimedia. Organize material in order ofincreasing difficulty. Periodically revisit conceptsto facilitate recall.
5. Provide guidance for learning—Offer learnersspecific guidance on how to best understandconcepts or acquire skills. Use a different mediaor format to avoid confusion with theinstructional material.
6. Elicit performance—Present learners withnumerous opportunities to use newly acquiredknowledge, skills, or behavior. Repeated practiceallows learners to confirm their understanding.
7. Provide feedback—Provide learners withspecific, constructive, and immediate feedbackregarding their performance.
8. Assess performance—Assess learners againstthe aforementioned learning objectives todetermine if the knowledge, skills, or behaviorhave been appropriately acquired.
9. Enhance retention and transfer—Review thematerial. Inform learners of opportunities toapply the new knowledge, skills, or behavior.Offer opportunities for additional practice.
Gagné’s method is intuitive to many instructors andcan readily be used within educational technologyenvironments. While the relative merit has not beenproven for each recommendation, they continue toserve as ‘good practices’ employed by researchers.Table 3 suggests how the principles might beeffectively used with the three common educationaltechnologies. While, medical educators may not beaccustomed to such a formal approach in developingan educational activity, instructional design may beeven more important when using educationaltechnologies than in face-to-face teaching, becausethe learning activities must be explicitly planned inadvance. A systematic approach to instructionaldesign is essential to the effective use of educationaltechnology, and indeed, educators unfamiliar withsuch approaches may benefit from engaging expertsin instructional design when newly developinglearning materials.
Effective Use of EducationalTechnology in Medical Education
Association of American Medical Colleges, 200712

Table 3. Technical approaches to help realize each phase of instructional design.
Effective Use of EducationalTechnology in Medical Education
Association of American Medical Colleges, 200713
Gain attention
Inform learners ofeducational objectives
Stimulate recall ofprior knowledge
Present the material
Provide guidance forlearning
Elicit performance
Provide feedback
Assess performance
Enhance retention andtransfer
Computer-aided Instruction
Present a short patient scenario, aninteractive model, or a compellingvideo clip.
Clearly state desired learningobjectives/outcomes.
Analyze material presented in“gain attention” phase or offer anadvance organizer to help bridgeprior and new knowledge.
Use text or multimedia to presentbasic concepts (see Mayer’sprinciples) through combinationsof lecture, narratives, cases,interactive multimedia, and drilland practice problems.
Guide understanding by analyzingproblems, summarizing, oralternate explanation of concepts.
Assign practice problems or cases.
Deliver specific feedback regardingpractice problem performance.
Deliver a post-exercise examaligned with the learningobjectives.
Consider revisiting materialthrough periodic email updates,reminders, or practice cases.
Virtual Patients
Display an opening video (e.g., adramatic patient presentation).
Clearly state desired learningobjectives/ outcomes.
Present a series of multiple choicequestions related to the “gainattention” phase and consideroffering succinct feedback.
At the end of a single virtualencounter, direct learners to aWeb-based, menu-driven tutorialthat addresses core topics of thecase.
Use a virtual preceptor to providedecision guidance when too muchtime has elapsed.
After they view a tutorial ondiagnostic imaging, ask learners tointerpret a series of radiographs.
When learners ask virtual patientsinterview questions, the virtualpreceptor comments on theirrelevance to the chief complaint.
At program’s end, learners receivescores summarizing theirperformance on multiple-choicequestions.
After using the virtual patient,learners write a narrative reflectionon how it reminded them of areal-life patient experience.
Human Patient Simulation
Put learners in urgent patientscenarios (e.g., cardiac arrest) withworsening condition until appropriateaction taken.
Clearly state desired learningobjectives/ outcomes.
In “gain attention” phase, elicit properactions to manage cardiac arrest—e.g., implement proper protocol forpulseless ventricular tachycardia.
Provide clinical experiences incontrolled settings applicable to realclinical situations. Learnerexperiences should evoke feelingsassociated with similar clinicalsituations.
With clear goals allow learners tomake mistakes while guiding themon technique or course of action.
Offer opportunities for all learners tobe actively engaged and evaluated insimulation experience regardless ofrole.
Focused formative feedback duringsimulation or teachable moment.Review video recordings duringformal debriefing with faculty andpeers.
Align objectives and learningopportunities with performanceevaluations. Use checklists and ratingscales to evaluate processes oroutcomes.
Integrate learning strategies andevaluation tools from simulation intoclinical practice. Implement mandatoryremediation training for skills mostprone to deterioration.

A Research Agenda
Colloquium participants agreed that the currentevidence base for educational technology in medicineis anemic. Although numerous publications havedocumented the feasibility of technology toenhance learning in various settings, little isestablished about precisely when to employtechnology during medical education (versus themany other methods and media available), andhow best to use it when it is employed. Althoughmuch can be learned from research in non-medicaleducation fields, future research on educationaltechnology in medical training will require asignificant change in focus. Simple answers areunlikely. Rather, solutions will be contingent uponmultiple factors including learner attributes,desired learning outcomes, institutionalcharacteristics, and other factors in the learningenvironment. Future research will have toaccommodate these complexities as well.
Colloquium participants called for fewer studiesthat simply compare instructional approaches(e.g., computer-aided instruction versus lectures)and instead set out the challenge that subsequentresearch should clarify the uses of technology tofacilitate learning—for example, the effectiveness ofspecific technological features or instructionalmethods—and when and how to integrateeducational technology into the medical trainingcontinuum.
Proposed Research QuestionsAddressing the following research questions willserve to clarify the appropriate use of educationtechnologies in medical education:
HOW• How can instructional methods and designs be
tailored to individual learner’s needs?
• How does the use of educational technologydiffer for groups compared with individuals?
• How does fidelity impact learning outcomes,educational contexts, and learner characteristics?
• Which technology approaches are appropriate forparticular learning outcomes?
• How can we best integrate educational technologyinto existing curricula?
• What is the most appropriate use of specificsimulation technologies?
• What infrastructure (human and technical) isneeded to effectively support educationaltechnology in the curriculum?
WHEN• What are the barriers to successful integration of
educational technology into the curriculum?
• What are the characteristics of individuals andinstitutions that have successfully integratededucational technology into the curriculum?
• How can educational technology be integrated inexisting educational settings?
• What is the cost-benefit ratio of varioustechnologies?
• What outcome measures are reliable, valid, andfeasible?
• What training opportunities will help ensure thateducators possess the necessary competencieslisted above?
Effective Use of EducationalTechnology in Medical Education
Association of American Medical Colleges, 200714
Effective Use of EducationalTechnology in Medical Education
Association of American Medical Colleges, 200715
Case Study 2
A surgery residency program director would like to improve her junior residents’ ability towork as a cooperative team during patient crises in the Surgical Intensive Care Unit (SICU).She asks a professional educator to help plan and design the instructional activity. Theeducator suggests conducting the communication training with a new human patientsimulator capable of portraying crisis scenarios. Before designing a simulation scenario, theyagree to conduct a literature search and consult other faculty to develop the relevantknowledge, skills, and behaviors; they then develop specific learning objectives and desiredoutcomes.
They choose a high level of fidelity, designing an environment that includes the humanpatient simulation device, a nurse, and recognizable features of the SICU. They willvideotape group performance to facilitate feedback sessions; some scenarios vary in level ofdifficulty. Each scenario requires active participation from all residents.
The session is offered at the start of the PGY-1 year and again at the end of PGY-2. Theinstructor begins the session by sharing an incident from her own experience and asksparticipants to articulate what they know about teamwork. Educational goals are sharedwith the team before the scenario begins. After each scenario the instructor plays the videoand offers specific feedback. Participants are encouraged to exchange roles duringsubsequent practice scenarios. The instructor revisits key concepts through an existingweekly seminar series.
ParticipantsDavid A. Cook, M.D., M.H.P.E.Associate Professor of MedicineChair, Medical Education Research GroupMayo Clinic College of Medicine
Charles P. Friedman, Ph.D.Associate Director for Research Informatics andInformation TechnologyNational Heart, Lung, and Blood InstituteNational Institutes of Health
Peter S. Greene, M.D.Executive DirectorMedBiquitous ConsortiumAssociate Dean for Emerging TechnologiesJohns Hopkins Medicine
Tiffany Grunwald, M.D., M.S.Ed.Surgical FellowDivision of Plastic andReconstructive SurgeryKeck School of MedicineUniversity of Southern California
Grace C. Huang, M.D.Director, Office of Educational TechnologyCarl J. Shapiro Institute forEducation and ResearchBeth Israel Deaconess Medical CenterHarvard Medical School
S. Barry Issenberg, M.D.Associate Professor of MedicineAssistant Dean, Research in Medical EducationDirector, Division of Research and TechnologyUniversity of Miami Miller School of Medicine
Carol S. Kamin, M.S., Ed.D.Associate Professor, PediatricsDirector, Project L.I.V.EUniversity of Colorado School of Medicine
Roger Kneebone, M.D., Ph.D.Senior Lecturer in Surgical EducationDepartment of Biosurgery and TechnologyDivision of Surgery, Oncology, Reproduction andAnaestheticsFaculty of MedicineImperial College London
William C. McGaghie, Ph.D.Professor of Medical EducationProfessor of Preventive MedicineOffice of Medical Education andFaculty DevelopmentNorthwestern UniversityFeinberg School of Medicine
Geoff Norman, Ph.D.Assistant Dean, Programme for EducationalResearch and DevelopmentProfessor, Department of Clinical Epidemiologyand BiostatisticsMcMaster University
Eduardo Salas, Ph.D.Trustee Chair and Professor of PsychologyProgram Director, Human Systems IntegrationResearch DepartmentInstitute for Simulation and TrainingUniversity of Central Florida
Effective Use of EducationalTechnology in Medical Education
Association of American Medical Colleges, 200716
Effective Use of EducationalTechnology in Medical Education
Association of American Medical Colleges, 200717
AAMC StaffChris Candler, M.D.Director of Educational TechnologyCo-Director and Editor, MedEdPORTAL
M. Brownell Anderson, M.S.Senior Associate Vice PresidentDivision of Medical Education
Carol Aschenbrener, M.D.Executive Vice PresidentDirector, Institute for Improving Medical Education
Robby Reynolds, M.P.A.Director, Educational ResourcesCo-Director, MedEdPORTAL
Alexis L. Ruffin, M.S.Deputy Director, Institute for Improving Medical Education
Michael E. Whitcomb, M.DEditor, Academic Medicine

Bibliography
American College of Surgeons Division of Education: Accredited Education Institutes. Available at:www.facs.org/education/accreditationprogram/. Accessed on August 30, 2006.
The American Society of Anesthesiologists. “3-16-06 - White Paper: ASA Approval of AnesthesiologySimulation Programs.” Available at: www.asahq.org/. Accessed on August 30, 2006.
Alessi S. Fidelity in the Design of Instructional Simulations. Journal of Computer-Based Instruction. 1988; 15: 40-47.
Choudhry NK, Fletcher RM, Soumerai SB. Systematic review: the relationship between clinical experience andquality of health care. Ann Intern Med. 2005; 142: 260-273.
Cook D. The Research We Still Are Not Doing: An Agenda for the Study of Computer-Based Learning.Academic Medicine. 2005; 80: 541-548.
Downing SM. Reliability: on the reproducibility of assessment data. Medical Education 2004; 38: 1006-1012.
Downing SM. Validity: on the meaningful interpretation of assessment data. Medical Education 2003; 37: 830-837.
Ericsson KA. Deliberate practice and the acquisition and maintenance of expert performance in medicine andrelated domains. Academic Medicine 2004; 79 (10, Suppl.): S70-S81.
Fleming VM, Schindler N, Martin GJ, DaRosa DA. Separate and equitable promotion tracks for clinician-educators. JAMA 2005; 294(9): 1101-1104.
Friedman, CP. The Marvelous Medical Education Machine or How Medical Education Can Be Unstuck inTime. Academic Medicine. 2000; 75(10): S137-S142.
Friedman CP. Anatomy of the Clinical Simulation. Academic Medicine. 1995; 70: 205-09.
Fowlkes J, Dwyer D. Osler R, Salas E. Event-based approach to training. International Journal of AviationPsychology.1998; 8:209-22.
Grunwald T. Guidelines for Cognitively Efficient Multimedia Learning Tools: Educational Strategies, CognitiveLoad, and Interface Design. Academic Medicine. 2006; 81: 213-223.
Issenberg SB, McGaghie WC, Petrusa ER, Lee Gordon D, Scalese RJ. Features and uses of high-fidelity medicalsimulations that lead to effective learning: a BEME systematic review. 2005. Medical Teacher. 2005; 271:10-28.
Kamin C, Souza K, Heestand D, Moses A, O'Sullivan P. Educational Technology Infrastructure and Services inNorth American Medical Schools. Academic Medicine. 2006; 81:632-637.
Keane D, Norman G, Vickers J. The Inadequacy of Recent Research on Computer-Assisted Instruction.Academic Medicine. 1991;66: 444-448.
Kneebone R. Evaluating Clinical Simulations for Learning Procedural Skills: A Theory-Based Approach.Academic Medicine. 2005; 80: 549-553.
Effective Use of EducationalTechnology in Medical Education
Association of American Medical Colleges, 200718

Main RG. Integrating Motivation into the Design Process. Educational Technology. 1993; 33(12): 37-41.
Strauss, S. Learning theories of Gagné and Piaget: Implications for curriculum development. TeachersCollege Record. 1972; 74(1): 81-102.
Strickland AW. ADDIE. Idaho State University College of Education Science, Math & TechnologyEducation. Retrieved June 29, 2006, from http://ed.isu.edu/addie/index.html
Veronikas S. An Interview with Richard Mayer. Educational Psychology Review. 2005; 17: 179 - 189.
Effective Use of EducationalTechnology in Medical Education
Association of American Medical Colleges, 200719