effects of an individualized caregiver training intervention on self-efficacy of cancer caregivers
TRANSCRIPT
http://wjn.sagepub.com/Research
Western Journal of Nursing
http://wjn.sagepub.com/content/35/5/590The online version of this article can be found at:
DOI: 10.1177/0193945911420742
2013 35: 590 originally published online 26 September 2011West J Nurs ResCristina C. Hendrix, Richard Landerman and Amy P. Abernethy
Self-Efficacy of Cancer CaregiversEffects of an Individualized Caregiver Training Intervention on
Published by:
http://www.sagepublications.com
On behalf of:
Midwest Nursing Research Society
at: can be foundWestern Journal of Nursing ResearchAdditional services and information for
http://wjn.sagepub.com/cgi/alertsEmail Alerts:
http://wjn.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- Sep 26, 2011 OnlineFirst Version of Record
- Mar 31, 2013Version of Record >>
at Bartin Universitesi on November 14, 2014wjn.sagepub.comDownloaded from at Bartin Universitesi on November 14, 2014wjn.sagepub.comDownloaded from

Western Journal of Nursing Research35(5) 590 –610
© The Author(s) 2011Reprints and permissions:
sagepub.com/journalsPermissions.navDOI: 10.1177/0193945911420742
wjn.sagepub.com
1Duke University School of Nursing, Durham, NC, USA2Durham Veterans Affairs Medical Center, NC, USA3Duke Center for Aging, Durham, NC4Duke Comprehensive Cancer Center, Durham, NC5Duke University School of Medicine, Durham, NC
Corresponding Author:Cristina C. Hendrix, Duke University School of Nursing, DUMC 3322, Durham, NC 27710, USA. Email: [email protected]
Effects of an Individualized Caregiver Training Intervention on Self-Efficacy of Cancer Caregivers
Cristina C. Hendrix1,2, Richard Landerman3, and Amy P. Abernethy4,5
Abstract
Caring for older cancer patients after hospital discharge is challenging and many of their caregivers lack confidence to do so. This study investigated the effects of an individualized caregiver training program on self-efficacy in home care and symptom management. A total of 120 patient–caregiver dyads were randomly assigned to either the treatment (n = 60) or control group (n = 60). The training focused on prevention of infection, pain control, maintenance of nutrition and adequate elimination, and specific care issues identified by the caregiver. Control group received information about community-based resources. Results revealed a significant increase in self-efficacy after the training in the treatment group but not in the control group. No intervention effect was seen on caregiver’s psychological well-being (depression, anxiety, and quality of life) and patient’s physical symptoms.
Article
at Bartin Universitesi on November 14, 2014wjn.sagepub.comDownloaded from
Hendrix et al. 591
Keywords
family caregivers, symptom management, caregiver training, cancer
In 2010, more than 1.5 million new cases of cancer were projected to occur in the United States (Jemal, Siegel, Xu, & Ward, 2010), adding to the already 12 million Americans who have cancer (American Cancer Society, 2011). The majority of cancer care is delivered in outpatient settings, with only the sickest patients admitted to hospitals and then discharged as quickly as pos-sible. Many patients return home while still convalescing from the effects of treatment creating heightened caregiving responsibilities during the first few days of hospital discharge. Lack of confidence and preparedness to provide the necessary complex care at home may intensify caregiver distress that may be already prominent because of the concern of life-limiting illness afflicting a loved one (Given & Sherwood, 2006; Papastavrou, Charalambous, & Tsangari, 2009).
Shorter hospital stays and expansion of home care technology have trans-ferred the responsibility for the care of cancer patients to their informal care-givers (Schumacher et al., 2002; Sutton, Demark-Wahnefried, & Clipp, 2003). These responsibilities are especially heightened during the hospital-to-home transition period (Coleman, 2003). With little or no preparation, training, or support, informal caregivers assume health management roles and carry out medical tasks traditionally performed by professional health care providers (Donelan et al., 2002). Understandably, acquisition of knowl-edge and skills in symptom management has been identified as a major unmet need of many informal cancer caregivers (Oldham & Kristjanson, 2004; Schumacher et al., 2002).
As a consequence of the physical and emotional toll associated with care-giving, evidence suggests that caregiving is associated with depression (Braun, Mikulincer, Rydall, Walsh, & Rodin, 2007; Carter & Chang, 2000) and anxi-ety (Aranda & Hayman-White, 2001), worsening as patient’s cancer advances. Inability to alleviate symptoms remains a constant source of anxiety for care-givers and does not improve over time (Aranda & Hayman-White, 2001). Being a caregiver is associated with higher burden (Garlo, O’Leary, Van Ness, & Fried, 2010) and distress (Cameron, Franche, Cheung, & Stewart, 2002) as well as decreased marital satisfaction (Fang, Manne, & Pape, 2001) and physical well-being (Carter & Chang, 2000). The period after hospitaliza-tion is particularly stressful as there is often a lack of continuity in clinical care and providers (Coleman, 2003).
at Bartin Universitesi on November 14, 2014wjn.sagepub.comDownloaded from
592 Western Journal of Nursing Research 35(5)
Self-efficacy is a prerequisite to the actual performance of tasks and strat-egies by an individual (Bandura, 1986, 1997). Even if individuals believe that particular actions will produce certain results, they will not act on that belief if they question whether they have the ability to engage in the necessary actions or behaviors. According to Bandura, self-efficacy is the confidence or belief in one’s capabilities to organize and execute the courses of action required to produce given outcomes (Bandura, 1997). In the context of cancer caregiving in symptom management, self-efficacy includes the caregivers’ confidence that they can help alleviate their loved ones’ symptoms.
To date, few studies have examined caregivers’ self-efficacy in symptom management within the context of cancer. In a study of caregiver assistance with pain management at the end of life, when caregivers reported high self-efficacy, patients had more energy, felt less ill, and spent less time in bed (Keefe et al., 2003). In another study, caregivers with greater confidence in their caregiving skills experienced less depression (Nijboer, Tempelaar, Triemstra, van den Bos, & Sanderman, 2001). Meanwhile, when caregivers reported lower levels of self-efficacy for helping their partners manage pain and other symptoms, these caregivers had higher levels of anxiety and depres-sion (Porter, Keefe, Garst, McBride, & Baucom, 2008).
In the authors’ previous pilot studies, individualized training in symptom management before hospital discharge was feasible and associated with an immediate improvement in informal cancer caregivers’ self-efficacy in symp-tom management (Hendrix, Abernethy, Sloane, Misuraca, & Moore, 2009; Hendrix & Ray, 2006). This training combined didactic teaching and actual performance of the necessary skills to carry out cancer symptom interven-tions, under the tutelage of a health care professional (expert). One-on-one training allowed caregivers to ask questions and ensured that information pre-sented to caregivers was tailored and personally relevant. This was consistent with other studies demonstrating that information matched to patient’s condi-tion and caregiver needs improved self-efficacy for cancer symptom manage-ment (Iconomou, Vagenakis, & Kalofonos, 2001; Schmall, 1995). The training was provided to caregivers when the hospital discharge of patients was immi-nent as home care issues are particularly anxiety provoking for informal care-givers as hospital discharge nears (Coleman, 2003). The caregiver training was administered at the hospital bedside to encourage patient participation and to recreate the milieu of home-based caregiving.
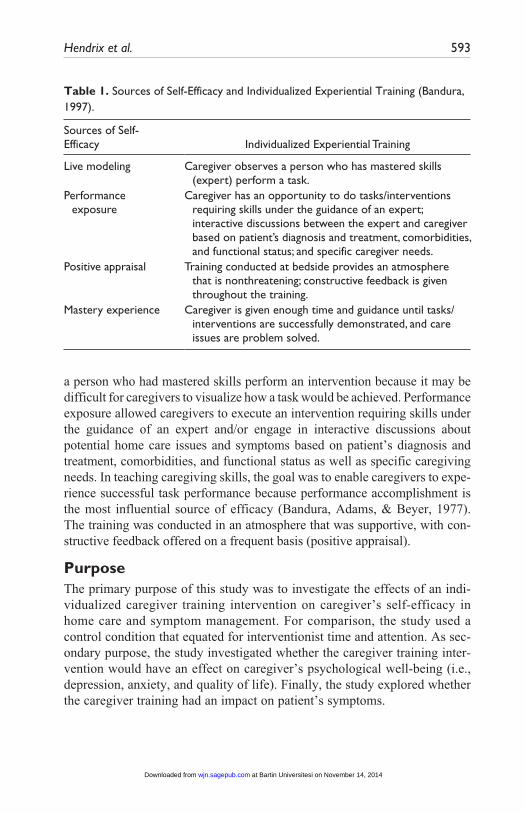
The individualized training contained the different sources of self-efficacy: live modeling, performance exposure, positive appraisal, and mastery experi-ence (Bandura, 1997; Table 1). Live modeling allowed caregivers to observe
at Bartin Universitesi on November 14, 2014wjn.sagepub.comDownloaded from
Hendrix et al. 593
Table 1. Sources of Self-Efficacy and Individualized Experiential Training (Bandura, 1997).
Sources of Self-Efficacy Individualized Experiential Training
Live modeling Caregiver observes a person who has mastered skills (expert) perform a task.
Performance exposure
Caregiver has an opportunity to do tasks/interventions requiring skills under the guidance of an expert; interactive discussions between the expert and caregiver based on patient’s diagnosis and treatment, comorbidities, and functional status; and specific caregiver needs.
Positive appraisal Training conducted at bedside provides an atmosphere that is nonthreatening; constructive feedback is given throughout the training.
Mastery experience Caregiver is given enough time and guidance until tasks/interventions are successfully demonstrated, and care issues are problem solved.
a person who had mastered skills perform an intervention because it may be difficult for caregivers to visualize how a task would be achieved. Performance exposure allowed caregivers to execute an intervention requiring skills under the guidance of an expert and/or engage in interactive discussions about potential home care issues and symptoms based on patient’s diagnosis and treatment, comorbidities, and functional status as well as specific caregiving needs. In teaching caregiving skills, the goal was to enable caregivers to expe-rience successful task performance because performance accomplishment is the most influential source of efficacy (Bandura, Adams, & Beyer, 1977). The training was conducted in an atmosphere that was supportive, with con-structive feedback offered on a frequent basis (positive appraisal).
PurposeThe primary purpose of this study was to investigate the effects of an indi-vidualized caregiver training intervention on caregiver’s self-efficacy in home care and symptom management. For comparison, the study used a control condition that equated for interventionist time and attention. As sec-ondary purpose, the study investigated whether the caregiver training inter-vention would have an effect on caregiver’s psychological well-being (i.e., depression, anxiety, and quality of life). Finally, the study explored whether the caregiver training had an impact on patient’s symptoms.
at Bartin Universitesi on November 14, 2014wjn.sagepub.comDownloaded from
594 Western Journal of Nursing Research 35(5)
Hypotheses. The following hypotheses were tested in this study:
Hypothesis 1: Informal caregivers who received the individualized caregiving intervention will have increased levels of self-efficacy in home care and symptom management after hospital discharge of their loved ones.
Hypothesis 2: Informal caregivers who received the individualized caregiving intervention will have improved psychological well-being (depression, anxiety, and quality of life).
In addition, patients whose caregivers received the caregiver training inter-vention will experience less physical symptoms at home after their hospital discharge.
MethodStudy design. The study design was an experimental, two-group design,
with data collection before (T1) and after training (T2) and at 1 week (T3), 2 weeks (T4), and 4 weeks (T5) after the patient’s hospital discharge. The early time points at 1 and 2 weeks after discharge were intended to inform the impact of the intervention on caregiver self-efficacy during the most trying time in symptom management following hospital discharge. The later time point at 4 weeks provided information on the sustainability of the impact of intervention, if there was any.
Sample and setting. The study was conducted in a 31-bed cancer unit at Duke University Hospital in Durham, North Carolina. Study participants consisted of caregiver–patient dyads. Cancer patients were eligible to partici-pate if they were aged 50 or above; oriented to place, person, and time; and were anticipated to be discharged home from the hospital. To control for wide variations in symptomatology associated with different types of can-cers, only patients with a confirmed diagnosis of a hematological malignancy and admitted for treatment of cancer or for treatment-related or cancer-related complications were targeted for the study. Caregiver participants were English-speaking adults who lived in the same household as eligible cancer patients, were anticipated to provide most of the “hands-on” care after dis-charge, and willing to spend at least 2 to 3 hr at the bedside for intervention training.
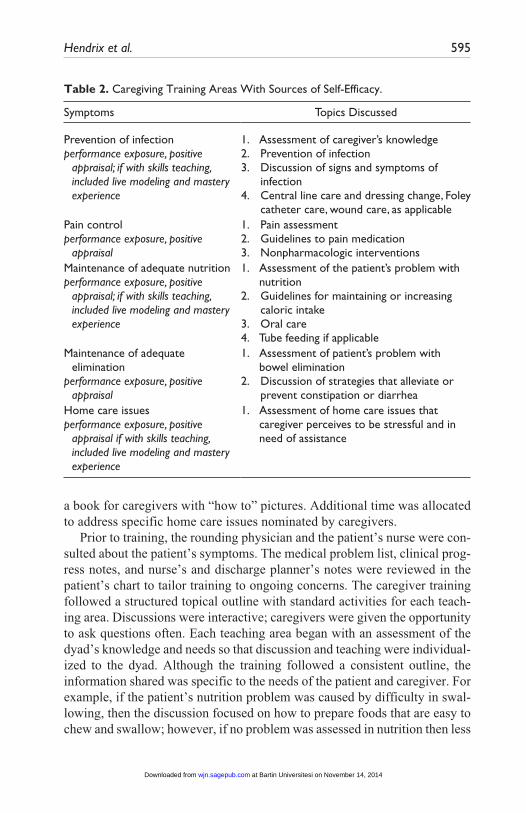
Caregiver training intervention. The intervention provided caregivers train-ing on strategies for managing patients’ cancer symptoms, with four major components: prevention of infection, pain control, maintenance of nutrition, and adequate elimination (Table 2). The program was manualized, including
at Bartin Universitesi on November 14, 2014wjn.sagepub.comDownloaded from
Hendrix et al. 595
a book for caregivers with “how to” pictures. Additional time was allocated to address specific home care issues nominated by caregivers.
Prior to training, the rounding physician and the patient’s nurse were con-sulted about the patient’s symptoms. The medical problem list, clinical prog-ress notes, and nurse’s and discharge planner’s notes were reviewed in the patient’s chart to tailor training to ongoing concerns. The caregiver training followed a structured topical outline with standard activities for each teach-ing area. Discussions were interactive; caregivers were given the opportunity to ask questions often. Each teaching area began with an assessment of the dyad’s knowledge and needs so that discussion and teaching were individual-ized to the dyad. Although the training followed a consistent outline, the information shared was specific to the needs of the patient and caregiver. For example, if the patient’s nutrition problem was caused by difficulty in swal-lowing, then the discussion focused on how to prepare foods that are easy to chew and swallow; however, if no problem was assessed in nutrition then less
Table 2. Caregiving Training Areas With Sources of Self-Efficacy.
Symptoms Topics Discussed
Prevention of infectionperformance exposure, positive
appraisal; if with skills teaching, included live modeling and mastery experience
1. Assessment of caregiver’s knowledge2. Prevention of infection3. Discussion of signs and symptoms of
infection4. Central line care and dressing change, Foley
catheter care, wound care, as applicablePain controlperformance exposure, positive
appraisal
1. Pain assessment2. Guidelines to pain medication3. Nonpharmacologic interventions
Maintenance of adequate nutritionperformance exposure, positive
appraisal; if with skills teaching, included live modeling and mastery experience
1. Assessment of the patient’s problem with nutrition
2. Guidelines for maintaining or increasing caloric intake
3. Oral care4. Tube feeding if applicable
Maintenance of adequate elimination
performance exposure, positive appraisal
1. Assessment of patient’s problem with bowel elimination
2. Discussion of strategies that alleviate or prevent constipation or diarrhea
Home care issuesperformance exposure, positive
appraisal if with skills teaching, included live modeling and mastery experience
1. Assessment of home care issues that caregiver perceives to be stressful and in need of assistance
at Bartin Universitesi on November 14, 2014wjn.sagepub.comDownloaded from
596 Western Journal of Nursing Research 35(5)
time was devoted to the topic allowing more time for other symptom areas. If there were no active problems in a symptom area, the discussion was about symptom prevention; for example, if the patient had neither constipation nor diarrhea, training was on preventive measures.
For home care issues areas that required skills (e.g., care of a central cath-eter), the caregiver was initially shown how to perform the intervention, then the caregiver was given an opportunity to demonstrate back the intervention, and additional time was given, if necessary, to ensure successful performance of skills. Training lasted 2 to 3 hr and was delivered in one to two sessions, depending on caregiver preference.
Control intervention. Similar to the treatment group, caregivers in the con-trol group received standardized, manualized training. However, the infor-mation was about community resources for caregiving, including, but not limited to, home health agencies, respite care, and caregiver support services. General health education focused on maintaining healthy lifestyle habits such as exercise, sleep habits, and smoking cessation (if applicable). The training was interactive and tailored to specific caregiver’s needs. For example, if a caregiver requested more information about community support groups, then more time was allocated to this discussion. However, there were no discus-sions on symptom management strategies and no skills for home care were discussed nor taught. The session lasted 2 to 3 hr and could be delivered in one to two sessions as requested by caregivers.
Nurse interventionists and fidelity to protocol. Different nurses delivered the treatment and control interventions, according to procedures as set out in study manuals approved by the Institutional Review Board (IRB). To prepare for the delivery of the intervention, role-plays and feedback were conducted weekly to practice and improve intervention delivery. Supplemental discus-sions centered on assessing and responding to undue stress and anxiety among caregivers as well as the importance of maintaining fidelity to the approved protocol.
During the first 3 months of the study, weekly debriefing sessions for the nurse interventionists provided a forum to discuss experiences and ensure fidelity to study protocols. Thereafter, meetings were monthly. Both inter-ventionists kept a log of particular issues and study-related questions dis-cussed during monthly meetings.
Study procedures. The study was approved by the Duke University Health System IRB. Review of the list of patients on the hospital ward was con-ducted at least weekly. For potentially eligible patients, the attending phy-sician was notified and was asked to voice any concerns about study participation of patients. When no concerns were received, the patient was approached and asked for the presence of a caregiver. If the patient had a
at Bartin Universitesi on November 14, 2014wjn.sagepub.comDownloaded from
Hendrix et al. 597
caregiver, the study was explained and the patient was invited to participate in the study. If both patient and caregiver agreed to participate, consent forms were signed.
Dyads completed baseline data (T1): patients completed questionnaires on demographics, functional status, comorbidity, and symptoms, whereas care-givers completed questionnaires on demographics, self-efficacy, depression, anxiety, and quality of life. After completing baseline questionnaires, dyads were randomly assigned to either the treatment or control group. Randomization sequence was generated by using a computer a priori.
Training was offered when discharge was imminent. Immediately after the caregiver training, caregivers completed questionnaires on self-efficacy (T2). Caregivers and patients were then given follow-up questionnaires with prestamped envelopes. Follow-up questionnaires were on self-efficacy, anxi-ety, depression, and quality of life for caregivers and physical symptoms for patients for completion at 1 week (T3), 2 weeks (T4), and 4 weeks (T5) after hospital discharge of patients. A total of 3 days before follow-up data were due, a reminder phone call was conducted. After the dyads completed the 4th-week follow-up questionnaires, a thank you card with a US$20.00 gift card was sent to the caregiver.
MeasuresSelf-efficacy. Lorig’s self-efficacy scale (Lorig, Chastain, Ung, Shoor, &
Holman, 1989) was modified to include items directly relevant to the train-ing. The self-efficacy scale has 23 items and uses ratings on a scale of 10 (not confident) to 100 (very confident). The items are phrased in terms of can rather than will because can is a judgment of capability, whereas will is a statement of intention. For example, for central catheter care, caregivers were asked, “How confident are you that you can clean and dress the central cath-eter using the proper technique?” For nausea, caregivers were asked, “If your loved one is nauseated, how confident are you that you can help in decreasing his or her nausea?” Higher score indicates greater perceived self-efficacy in home care and symptom management. Internal consistency reliability, α = .94, was reported in a sample of cancer caregivers, and there was evidence of validity based on significant correlation in change of self-efficacy total score with change in the Archbold, Stewart, Greenlick, and Harvath (1990) Care-giving Preparedness Scale (Hendrix et al., 2009).
Caregiver well-being. Caregiver psychological well-being (depression, anxiety, and quality of life) were measured using the Hospital Anxiety and Depression Scale (HADS; Zigmond & Snaith, 1983) and the Caregiver Qual-ity of Life–Cancer Scale (CQOLC; Weitzner, Jacobsen, Wagner, Friedland, & Cox, 1999). The HADS consists of 14 items (7 items on depression and
at Bartin Universitesi on November 14, 2014wjn.sagepub.comDownloaded from
598 Western Journal of Nursing Research 35(5)
7 items on anxiety) scored on 4-point Likert-type scale; scores between 11 and 21 are classified as “cases,” between 8 and 10 as “borderline cases,” and between 0 and 7 as “noncases.” The HADS has been used in a number of recent caregiving studies to assess for anxiety and depression among caregiv-ers (e.g., Burridge, Barnett, & Clavarino, 2009; Jenewein et al., 2008; Spittle et al., 2010). The HADS has also been found to be a suitable tool to screen for depression and anxiety among family caregivers (Gough & Hudson, 2009). The CQOLC consists of 35 items scored on 5-point Likert-type scales and divided into four subscales as follows: Burden, Disruptiveness, Positive Adaptation, and Financial Concerns. The total possible score is 140 and higher scores indicate better quality of life. Using 263 family caregivers of patients with lung, breast, or prostate cancers, test–retest reliability of the CQOLC was 0.95, and internal consistency was 0.91 (Weitzner et al., 1999).
Functional status of patients. The Instrumental and Physical subscales of the Older Americans Resources and Services (OARS) Multidimensional Func-tional Assessment Questionnaire were used to measure patient functional status (Fillenbaum, 1988). Physical activities of daily living pertain to the everyday function of a person such as walking, bathing, and grooming. Pos-sible answers are needing no help, needing some help, and unable to do. The lower the total score, the higher the level of independence. Instrumental activities are related to independent living and include preparing meals, man-aging money, shopping for groceries or personal items, performing light or heavy housework, and using a telephone. The answers to each question are similar to those for the physical activities of daily living.
Comorbidity. Patient’s comorbid conditions were assessed using the modi-fied OARS comorbid scales (Fillenbaum, 1988). In this scale, patients were asked to indicate the presence (yes) or absence (no) of 25 medical conditions common in older population.
Symptoms. Patient symptoms were measured by the Memorial Symptom Assessment Scale (MSAS; Portenoy et al., 1994). The MSAS provides mul-tidimensional information of common physical and psychological symptoms. Using the scale, patients are asked whether they have had any symptoms dur-ing the previous week; if they respond “yes” to a symptom, then they are further asked on (a) how often did they have it (frequency), (b) how severe was it usually (characteristics or intensity), and (c) how much did it distress or bother them (distress). Patients rate these questions on a scale of 1 to 4 for prevalence and characteristics, and 0 to 4 for distress, with lower scores indi-cating less prevalent, intensity, and distress. For this study, scores on the Physical Symptom subscale were used, which was the average of the fre-quency, severity, and distress associated with 12 prevalent physical symp-toms: lack of appetite, lack of energy, pain, feeling drowsy, constipation, dry
at Bartin Universitesi on November 14, 2014wjn.sagepub.comDownloaded from

Hendrix et al. 599
mouth, nausea, vomiting, change in taste, weight loss, feeling bloated, and dizziness. Recent empirical studies on cancer symptoms have favored the use of the MSAS over other symptom measures (Sun et al., 2005; Turner, Kelly, Swanson, Allison, & Wetzig, 2005).
Data analysis. Mixed models were used to test the effects of the interven-tion over time, using SAS PROC MIXED (SAS Version 9.2). With this approach, each participant’s repeated measures on a dependent variable were first parameterized as an individual growth trajectory plus an error term. In a second stage, the estimated trajectories were modeled as a function of differ-ences between individuals on independent variables of interest. To test whether the intervention affected the trajectory of change on a dependent variable, two mixed models were estimated: an initial model where a depen-dent variable was regressed on intervention, time (three dummy variables), and intervention by time product terms, and a second model with the inter-vention by time product terms deleted. Baseline comorbidity, instrumental activities of daily living (IADL), the memorial physical symptom assessment scale, caregiver employment status, and (for caregiver self-efficacy) depres-sion were related to treatment group at baseline and/or subsequent dropout, and were included as covariates in both models. A likelihood ratio–based chi-square test was used for the difference in fit between Models 1 and 2 to determine whether the intervention had a statistically significant effect on the trajectory of change.
Statistical power. Our target sample size was 120 cancer caregiver–patient dyads to accommodate an estimated attrition rate of 10%. Using our baseline sample of 120 and the actual attrition rate of 17.5%, power was estimated using specialized software for power analysis with repeated measures data (Rochon, 1999). With alpha set to .05 (two-tailed), standardized differences of .40 with power equal to .80 were detected. These differences were consid-ered “medium-sized” in the statistical literature (Cohen, 1987). The data- analytic models provided unbiased parameter estimates as long as attrition-related missing are missing at random (MAR)—MAR conditional on the predictors included in the data-analytic model (Schafer & Graham, 2002). To maximize the plausibility of the MAR assumption, we tested whether each of our independent variables was related to dropout and included patient comor-bidities, IADL score, and memorial physical symptom score as covariates in our regression models.
ResultsIn 30 months of participant recruitment, 763 patients were screened for the study where 498 (65%) met the study eligibility criteria. Of these, 318 were approached. A total of 120 dyads (38%) agreed to participate and the rest either
at Bartin Universitesi on November 14, 2014wjn.sagepub.comDownloaded from

600 Western Journal of Nursing Research 35(5)
refused or were undecided about study participation. No dyad was lost before randomization. Postrandomization, the following attrition occurred in data col-lection: immediate posttraining = 0; 1 week after hospital discharge = 7; 2 weeks after hospital discharge= 8; and 4 weeks after hospital discharge = 6, for a total of 21 dyads (17.5% attrition rate). Participant dropout was not sig-nificantly related to group assignment: 12 were observed in the control group, whereas 9 dropouts were in the treatment group. Mean self-efficacy of caregiv-ers who dropped out was 140 and was 151 for nondropouts; this difference was not statistically significant. Reasons for not completing the study were because patients died or were referred to hospice (n = 12) or lost to follow-up (n = 9).
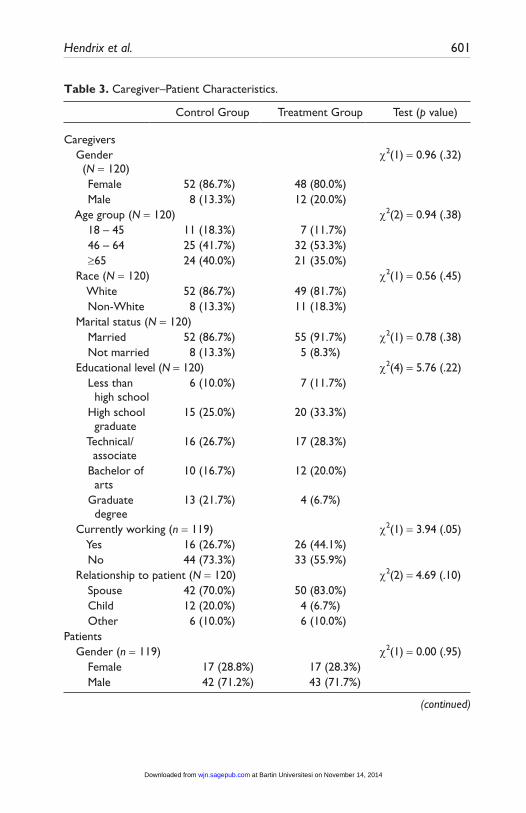
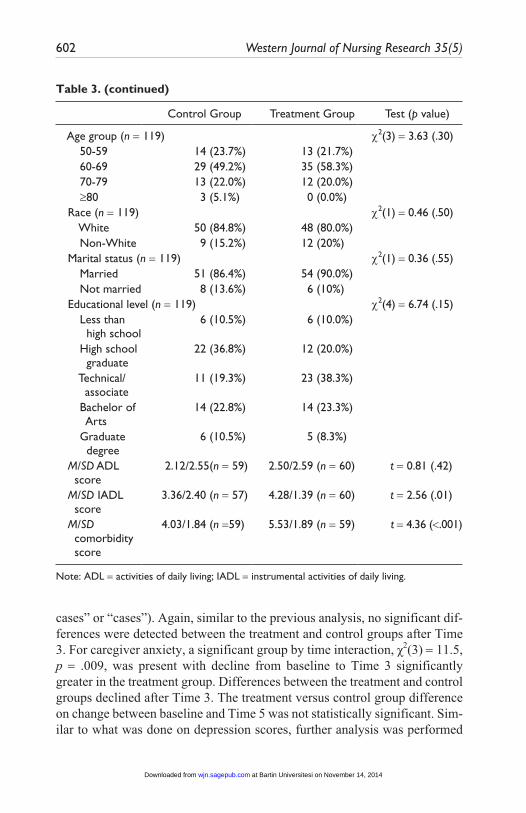
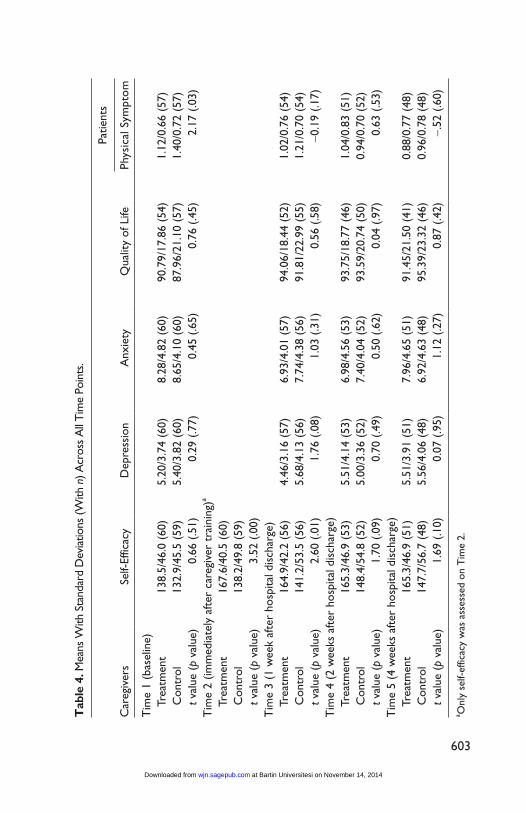
Characteristics of study participants are summarized in Table 3. Most of the caregiver participants were female above the age of 45 years, White, spouses of patients, married, and had at least a high school degree (see Table 3). Characteristics of caregivers in both groups were similar except that there were more caregivers in the treatment group who were currently employed. Similar to caregiver participants, patients in the study were mostly White, married, and had at least a high school degree. A vast majority of the patients were husbands of the caregivers in the study. Patients in the treatment group appeared to have more comorbidities and lower capacity for independent activities of daily liv-ing. As indicated above, these variables were included as covariates in the sta-tistical analysis. Although patients in both treatment and control group reported low levels of physical symptoms as indicated by their baseline mean scores of 1.12 versus 1.40, respectively (Table 4), the difference in their scores were statistically significant (t test = 2.7, p = .03). Therefore, Physical Symptom subscale was also included as a covariate in subsequent analyses.
In initial tests, all dependent variables were normally distributed. Table 4 presents means and standard deviations of primary and secondary outcomes across all time points.
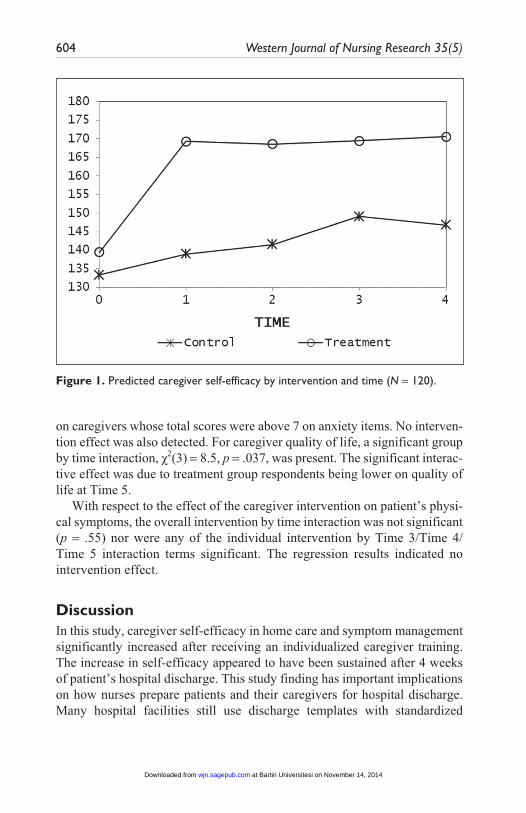
Results of Hypothesis 1. The mean regression-predicted scores in Figure 1 show an immediate increase in self-efficacy subsequent to the intervention (between Time 1 and Time 2) and a higher self-efficacy in the treatment group through Time 5. The overall group by time interaction was highly sig-nificant, χ2(4) =21.2, p < .001, indicating that increases in efficacy from base-line to each time point were significantly greater in the treatment group.
Results of Hypothesis 2. A significant group by time interaction, χ2(3) = 11.9, p = .008, was present with decline in caregiver depression from baseline to Time 3 significantly greater in the treatment group. Significant differences between the treatment and control groups were not present after Time 3. Fur-ther analysis was done on caregivers whose total scores were above 7 on depression items (i.e., caregivers whose scores indicated either “borderline
at Bartin Universitesi on November 14, 2014wjn.sagepub.comDownloaded from
Hendrix et al. 601
Table 3. Caregiver–Patient Characteristics.
Control Group Treatment Group Test (p value)
Caregivers Gender
(N = 120)χ2(1) = 0.96 (.32)
Female 52 (86.7%) 48 (80.0%) Male 8 (13.3%) 12 (20.0%) Age group (N = 120) χ2(2) = 0.94 (.38) 18 – 45 11 (18.3%) 7 (11.7%) 46 – 64 25 (41.7%) 32 (53.3%) ≥65 24 (40.0%) 21 (35.0%) Race (N = 120) χ2(1) = 0.56 (.45) White 52 (86.7%) 49 (81.7%) Non-White 8 (13.3%) 11 (18.3%) Marital status (N = 120) Married 52 (86.7%) 55 (91.7%) χ2(1) = 0.78 (.38) Not married 8 (13.3%) 5 (8.3%) Educational level (N = 120) χ2(4) = 5.76 (.22) Less than
high school6 (10.0%) 7 (11.7%)
High school graduate
15 (25.0%) 20 (33.3%)
Technical/ associate
16 (26.7%) 17 (28.3%)
Bachelor of arts
10 (16.7%) 12 (20.0%)
Graduate degree
13 (21.7%) 4 (6.7%)
Currently working (n = 119) χ2(1) = 3.94 (.05) Yes 16 (26.7%) 26 (44.1%) No 44 (73.3%) 33 (55.9%) Relationship to patient (N = 120) χ2(2) = 4.69 (.10) Spouse 42 (70.0%) 50 (83.0%) Child 12 (20.0%) 4 (6.7%) Other 6 (10.0%) 6 (10.0%) Patients Gender (n = 119) χ2(1) = 0.00 (.95) Female 17 (28.8%) 17 (28.3%) Male 42 (71.2%) 43 (71.7%)
(continued)
at Bartin Universitesi on November 14, 2014wjn.sagepub.comDownloaded from
602 Western Journal of Nursing Research 35(5)
Control Group Treatment Group Test (p value)
Age group (n = 119) χ2(3) = 3.63 (.30) 50-59 14 (23.7%) 13 (21.7%) 60-69 29 (49.2%) 35 (58.3%) 70-79 13 (22.0%) 12 (20.0%) ≥80 3 (5.1%) 0 (0.0%) Race (n = 119) χ2(1) = 0.46 (.50) White 50 (84.8%) 48 (80.0%) Non-White 9 (15.2%) 12 (20%) Marital status (n = 119) χ2(1) = 0.36 (.55) Married 51 (86.4%) 54 (90.0%) Not married 8 (13.6%) 6 (10%) Educational level (n = 119) χ2(4) = 6.74 (.15) Less than
high school6 (10.5%) 6 (10.0%)
High school graduate
22 (36.8%) 12 (20.0%)
Technical/ associate
11 (19.3%) 23 (38.3%)
Bachelor of Arts
14 (22.8%) 14 (23.3%)
Graduate degree
6 (10.5%) 5 (8.3%)
M/SD ADL score
2.12/2.55(n = 59) 2.50/2.59 (n = 60) t = 0.81 (.42)
M/SD IADL score
3.36/2.40 (n = 57) 4.28/1.39 (n = 60) t = 2.56 (.01)
M/SD comorbidity score
4.03/1.84 (n =59) 5.53/1.89 (n = 59) t = 4.36 (<.001)
Note: ADL = activities of daily living; IADL = instrumental activities of daily living.
Table 3. (continued)
cases” or “cases”). Again, similar to the previous analysis, no significant dif-ferences were detected between the treatment and control groups after Time 3. For caregiver anxiety, a significant group by time interaction, χ2(3) = 11.5, p = .009, was present with decline from baseline to Time 3 significantly greater in the treatment group. Differences between the treatment and control groups declined after Time 3. The treatment versus control group difference on change between baseline and Time 5 was not statistically significant. Sim-ilar to what was done on depression scores, further analysis was performed
at Bartin Universitesi on November 14, 2014wjn.sagepub.comDownloaded from
Tab
le 4
. Mea
ns W
ith S
tand
ard
Dev
iatio
ns (W
ith n
) Acr
oss
All
Tim
e Po
ints
.
Patie
nts
Car
egiv
ers
Self-
Effic
acy
Dep
ress
ion
Anx
iety
Qua
lity
of L
ifePh
ysic
al S
ympt
om
Tim
e 1
(bas
elin
e)
Trea
tmen
t 13
8.5/
46.0
(60
)5.
20/3
.74
(60)
8.28
/4.8
2 (6
0)90
.79/
17.8
6 (5
4)1.
12/0
.66
(57)
C
ontr
ol13
2.9/
45.5
(59
)5.
40/3
.82
(60)
8.65
/4.1
0 (6
0)87
.96/
21.1
0 (5
7)1.
40/0
.72
(57)
t v
alue
(p
valu
e)0.
66 (
.51)
0.29
(.7
7)0.
45 (
.65)
0.76
(.4
5)2.
17 (
.03)
Tim
e 2
(imm
edia
tely
aft
er c
areg
iver
tra
inin
g)a
Tr
eatm
ent
167.
6/40
.5 (
60)
Con
trol
138.
2/49
.8 (
59)
t val
ue (
p va
lue)
3.52
(.0
0)
Tim
e 3
(1 w
eek
afte
r ho
spita
l dis
char
ge)
Tr
eatm
ent
164.
9/42
.2 (
56)
4.46
/3.1
6 (5
7)6.
93/4
.01
(57)
94.0
6/18
.44
(52)
1.02
/0.7
6 (5
4)
Con
trol
141.
2/53
.5 (
56)
5.68
/4.1
3 (5
6)7.
74/4
.38
(56)
91.8
1/22
.99
(55)
1.21
/0.7
0 (5
4)
t val
ue (
p va
lue)
2.60
(.0
1)1.
76 (
.08)
1.03
(.3
1)0.
56 (
.58)
−0.1
9 (.1
7)T
ime
4 (2
wee
ks a
fter
hos
pita
l dis
char
ge)
Tr
eatm
ent
165.
3/46
.9 (
53)
5.51
/4.1
4 (5
3)6.
98/4
.56
(53)
93.7
5/18
.77
(46)
1.04
/0.8
3 (5
1)
Con
trol
148.
4/54
.8 (
52)
5.00
/3.3
6 (5
2)7.
40/4
.04
(52)
93.5
9/20
.74
(50)
0.94
/0.7
0 (5
2)
t val
ue (
p va
lue)
1.70
(.0
9)0.
70 (
.49)
0.50
(.6
2)0.
04 (
.97)
0.63
(.5
3)T
ime
5 (4
wee
ks a
fter
hos
pita
l dis
char
ge)
Tr
eatm
ent
165.
3/46
.9 (
51)
5.51
/3.9
1 (5
1)7.
96/4
.65
(51)
91.4
5/21
.50
(41)
0.88
/0.7
7 (4
8)
Con
trol
147.
7/56
.7 (
48)
5.56
/4.0
6 (4
8)6.
92/4
.63
(48)
95.3
9/23
.32
(46)
0.96
/0.7
8 (4
8)
t val
ue (
p va
lue)
1.69
(.1
0)0.
07 (
.95)
1.12
(.2
7)0.
87 (
.42)
−.52
(.6
0)
a Onl
y se
lf-ef
ficac
y w
as a
sses
sed
on T
ime
2.
603
at Bartin Universitesi on November 14, 2014wjn.sagepub.comDownloaded from
604 Western Journal of Nursing Research 35(5)
Figure 1. Predicted caregiver self-efficacy by intervention and time (N = 120).
on caregivers whose total scores were above 7 on anxiety items. No interven-tion effect was also detected. For caregiver quality of life, a significant group by time interaction, χ2(3) = 8.5, p = .037, was present. The significant interac-tive effect was due to treatment group respondents being lower on quality of life at Time 5.
With respect to the effect of the caregiver intervention on patient’s physi-cal symptoms, the overall intervention by time interaction was not significant (p = .55) nor were any of the individual intervention by Time 3/Time 4/ Time 5 interaction terms significant. The regression results indicated no intervention effect.
DiscussionIn this study, caregiver self-efficacy in home care and symptom management significantly increased after receiving an individualized caregiver training. The increase in self-efficacy appeared to have been sustained after 4 weeks of patient’s hospital discharge. This study finding has important implications on how nurses prepare patients and their caregivers for hospital discharge. Many hospital facilities still use discharge templates with standardized
at Bartin Universitesi on November 14, 2014wjn.sagepub.comDownloaded from
Hendrix et al. 605
domains and preset teachings under each domain. Although the domains or areas of needs can be predicted, the exact nature of the problems encountered requires unique problem solving for each caregiver and patient scenario. It is important, therefore, that in order for the teaching to be effective and person-ally relevant, it should be tailored to specific patient’s condition and care-giver informational needs (Iconomou et al., 2001; Schmall, 1995). The approach of a tailored intervention grounded in the predefined areas of teach-ing provides requisite balance between reproducibility and patient/caregiver centeredness.
Caregivers in the study affirmed the added value of individualized atten-tion to discharge teaching and the opportunity to be involved in discussing patient’s home care in a meaningful way (Oldham & Kristjanson, 2004; Schumacher et al., 2002). Frequently, however, discharge teaching is often left to bedside nurses whose attention is focused on caring for those who are still acutely ill. As a consequence, discharge preparation is rushed and inad-equate. Having a dedicated nurse in a hospital who will provide discharge teaching and training may provide additional support to patients and their caregivers during the hospital-to-home transition, an event that is replete with challenges in home care (Coleman, 2003).
Although significant and sustained improvement in self-efficacy in home care and symptom management was noted after receiving the caregiver train-ing, the training did not offer the same result on caregiver’s psychological well-being as evidenced by scores on Depression, Anxiety, and Quality of Life scales. Even though caregiving is associated with psychological dys-function (Braun et al., 2007), the caregiver participants in both groups had low baseline scores on HADS, especially on depression items, thus making it difficult to improve their scores. In addition, the caregiver training in this study focused on symptom management strategies and caregiving at home. Although, theoretically, improving caregiver’s self-efficacy in symptom management and home care may also lead to better psychological well-being (Bandura, 1997), this reasoning oversimplifies the nature of anxiety and depression, especially among caregivers of people with a life-limiting ill-ness. Nonetheless, there were some improvements noted on caregivers’ level of depression and anxiety at 1 week of hospital discharge in the treat-ment group, but these improvements were not sustained at 2 and 4 weeks of hospital discharge. This may imply that a one-time training before hospital discharge may not be enough to promote sustained effects on psychological well-being of caregivers and that home follow-up interventions may be needed to address the actual demands of caregiving at home. In addition, designing a caregiver training program that incorporates stress management
at Bartin Universitesi on November 14, 2014wjn.sagepub.comDownloaded from
606 Western Journal of Nursing Research 35(5)
strategies for caregivers may be one way to enhance the training to promote sustained effects on caregiver’s psychological well-being. These queries are all fertile areas for future investigations.
Similarly, there was no treatment effect observed in quality of life among caregivers, indicating that a single training may also not be sufficient to improve caregivers’ overall quality of life. However, interestingly, caregiv-ers in the control group were observed to have a steady improvement in quality of life scores, albeit small, from baseline to 4 weeks after hospital discharge. This trend was not observed in the treatment group. A possible explanation may be the suitability of the CQOLC for this particular caregiv-ing study. The CQOLC was selected to assess caregiver quality of life because of its observed psychometric properties in caregiving trials (Weitzner et al., 1999; Weitzner & McMillan, 1999). However, beyond reli-ability and validity, the CQOLC covers different domains (burden, disrup-tiveness, positive adaptation, and financial concerns) that may not be sensitive to the caregiver training intervention offered in this study. Therefore, for future investigations, thoughtful consideration should be used in selecting intervention outcomes including measures to assess changes in quality of life associated with a caregiver training program.
There was no intervention effect observed on patient’s physical symp-toms. However, baseline means of physical symptom scores for both groups indicated low prevalence of physical symptoms. For future trials, it will be important to include caregivers of patients with high symptomatology to determine whether the caregiver training program will have an effect on the physical well-being of symptomatic patients. To promote program sustain-ability, it will also be important to determine the cost-effectiveness of such approach to caregiver training, taking into account reductions in unplanned rehospitalization and emergency department visits, if any, that are associated with the training.
The study has strengths and limitations. Majority of caregivers who par-ticipated were female and married, the same characteristics as caregivers in the United States (National Alliance for Caregiving & American Association for Retired Persons [AARP], 2004). Caregivers in the treatment and control group were similar in most ways and significant differences were treated as covariates in the analytic models. The study has several limitations. Two nurses delivered the treatment and control intervention, thus, neither nurses was blind to group assignment. In addition, the actual performance of home care and symptom management interventions by caregivers was not assessed. Although the caregiver’s level of self-efficacy remained high even after 4 weeks of hospital discharge, this does not imply actual provision of care. This
at Bartin Universitesi on November 14, 2014wjn.sagepub.comDownloaded from

Hendrix et al. 607
may potentially explain why there was no reduction in patient’s symptoms associated with improved caregiver self-efficacy in home care and symptom management. In addition, no data were collected on whether patients received professional home care services after hospital discharge. However, because of the randomization used in group assignment, this probably did not play a factor in determining study outcomes.
In summary, as family caregivers play a major role in determining the success of hospital-to-home transitions, nurses must continually find ways to improve how caregivers are prepared for home care. Nurses have a critical role to play because hospital discharge preparation is generally the responsi-bility of nurses and because patients and informal caregivers view nurses as sources of information and support. This study has shown that an individual-ized approach to caregiver training is effective in promoting self-efficacy in home care and symptom management among informal caregivers of cancer patients. It is the hope that by assisting informal caregivers in their home caregiving role, favorable patient outcomes may soon follow.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Institute of Nursing Research Grant R15 NR009489.
References
American Cancer Society. (2011). Number of US cancer survivors growing. Retrieved from http://www.cancer.org/Cancer/news/News/numberofuscancersurvivorsgrowing
Aranda, S. K., & Hayman-White, K. (2001). Home caregivers of the person with advanced cancer: An Australian perspective. Cancer Nursing, 24, 300-307. doi:10.1097/00002820-200108000-00011
Archbold, P. G., Stewart, B. J., Greenlick, M. R., & Harvath, T. (1990). Mutuality and preparedness as predictors of caregiver role strain. Research in Nursing & Health, 13, 375-384. doi:10.1002/nur.4770130605
Bandura, A. (1986). Social foundations of thought and action: A social cognitive theory. Englewood Cliffs, NJ: Prentice Hall.
Bandura, A. (1997). Self-efficacy: The exercise of control. New York, NY: Freeman.Bandura, A., Adams, N. E., & Beyer, J. (1977). Cognitive processes mediating
behavioral change. Journal of Personality and Social Psychology, 35, 125-139. doi:10.1037/0022-3514.35.3.125
at Bartin Universitesi on November 14, 2014wjn.sagepub.comDownloaded from
608 Western Journal of Nursing Research 35(5)
Braun, M., Mikulincer, M., Rydall, A., Walsh, A., & Rodin, G. (2007). Hidden mor-bidity in cancer: Spouse caregivers. Journal of Clinical Oncology, 25, 4829-4834. doi:10.1200/JCO.2006.10.0909
Burridge, L. H., Barnett, A. G., & Clavarino, A. M. (2009). The impact of perceived stage of cancer on carers’ anxiety and depression during the patients’ final year of life. Psycho-Oncology, 18, 615-623. doi:10.1002/pon.1435
Cameron, J. I., Franche, R. L., Cheung, A. M., & Stewart, D. E. (2002). Lifestyle interference and emotional distress in family caregivers of advanced cancer patients. Cancer, 94, 521-527. doi:10.1002/cncr.10212
Carter, P. A., & Chang, B. L. (2000). Sleep and depression in cancer caregivers. Cancer Nursing, 23, 410-415. doi:10.1097/00002820-200012000-00002
Cohen, J. (1987). Statistical power analysis for the behavioral sciences (Rev. ed.). Hillsdale, NJ: Lawrence Erlbaum.
Coleman, E. A. (2003). Falling through the cracks: Challenges and opportunities for improving transitional care for persons with continuous complex care needs. Journal of the American Geriatrics Society, 51, 549-555. doi:10.1046/j.1532-5415.2003.51185.x
Donelan, K., Hill, C. A., Hoffman, C., Scoles, K., Feldman, P. H., Levine, C., & Gould, D. (2002). Challenged to care: Informal caregivers in a changing health system. Health Affairs, 21, 222-231. doi:10.1377/hlthaff.21.4.222
Fang, C. Y., Manne, S. L., & Pape, S. J. (2001). Functional impairment, marital quality, and patient psychological distress as predictors of psychological distress among cancer patients’ spouses. Health Psychology, 20, 452-457. doi:10.1037/0278-6133.20.6.452
Fillenbaum, G. G. (1988). Multidimensional functional assessment of older adults: The Duke older Americans resources and services procedures. Hillsdale, NJ: Erlbaum.
Garlo, K., O’Leary, J. R., Van Ness, P. H., & Fried, T. R. (2010). Burden in caregivers of older adults with advanced illness. Journal of the American Geriatrics Society, 58, 2315-2322.
Given, B., & Sherwood, P. R. (2006). Family care for the older person with cancer. Seminars in Oncology Nursing, 22, 43-50. doi:10.1016/j.soncn.2005.10.006
Gough, K., & Hudson, P. (2009). Psychometric properties of the Hospital Anxiety and Depression Scale in family caregivers of palliative care patients. Journal of Pain and Symptom Management, 37, 797-806. doi:10.1016/j.jpainsymman.2008.04.012
Hendrix, C. C., Abernethy, A., Sloane, R., Misuraca, J., & Moore, J. (2009). A pilot study on the influence of an individualized and experiential training on cancer caregiver’s self-efficacy in home care and symptom management. Home Health-care Nurse, 27, 271-278. doi:10.1097/01.NHH.0000356777.70503.62
Hendrix, C. C., & Ray, C. (2006). Informal caregiver training on home care and can-cer symptom management prior to hospital discharge: A feasibility study. Oncol-ogy Nursing Forum, 33, 793-798. doi:10.1188/06.ONF.793-798
at Bartin Universitesi on November 14, 2014wjn.sagepub.comDownloaded from

Hendrix et al. 609
Iconomou, G., Vagenakis, A. G., & Kalofonos, H. P. (2001). The informational needs, satisfaction with communication, and psychological status of primary caregivers of cancer patients receiving chemotherapy. Supportive Care in Cancer, 9, 591-596. doi:10.1007/s005200100259
Jemal, A., Siegel, R., Xu, J., & Ward, E. (2010). Cancer statistics, 2010. CA: A Cancer Journal for Clinicians, 60, 277-300. doi:10.3322/caac.20073
Jenewein, J., Zwahlen, R. A., Zwahlen, D., Drabe, N., Moergeli, H., & Buchi, S. (2008). Quality of life and dyadic adjustment in oral cancer patients and their female partners. European Journal of Cancer Care, 17, 127-135. doi:10.1111/j.1365-2354.2007.00817.x
Keefe, F. J., Ahles, T. A., Porter, L. S., Sutton, L. M., McBride, C. M., Pope, M. S., . . . Baucom, D. H. (2003). The self-efficacy of family caregivers for helping can-cer patients manage pain at end-of-life. Pain, 103, 157-162. doi:10.1016/S0304-3959(02)00448-7
Lorig, K., Chastain, R. L., Ung, E., Shoor, S., & Holman, H. R. (1989). Development and evaluation of a scale to measure perceived self-efficacy in people with arthri-tis. Arthritis & Rheumatism, 32, 37-44. doi:10.1002/anr.1780320107
National Alliance for Caregiving and AARP. (2004). Caregiving in the US. Retrieved from http://www.caregiving.org/data/04finalreport.pdf
Nijboer, C., Tempelaar, R., Triemstra, M., van den Bos, G. A., & Sanderman, R. (2001). The role of social and psychologic resources in caregiving of cancer patients. Cancer, 91, 1029-1039. doi:10.1002/1097-0142(20010301)91:5<1029::AID-CNCR1094>3.0.CO;2-1
Oldham, L., & Kristjanson, L. J. (2004). Development of a pain management pro-gramme for family carers of advanced cancer patients. International Journal of Palliative Nursing, 10, 91-99.
Papastavrou, E., Charalambous, A., & Tsangari, H. (2009). Exploring the other side of cancer care: The informal caregiver. European Journal of Oncology Nursing, 13, 128-136. doi:10.1016/j.ejon.2009.02.003
Portenoy, R. K., Thaler, H. T., Kornblith, A. B., Lepore, J. M., Friedlander-Klar, H., Kiyasu, E., . . . Scher, H. (1994). The Memorial Symptom Assessment Scale: An instrument for the evaluation of symptom prevalence, characteristics and distress. European Journal of Cancer, 30, 1326-1336. doi:10.1016/0959-8049(94)90182-1
Porter, L. S., Keefe, F. J., Garst, J., McBride, C. M., & Baucom, D. (2008). Self-efficacy for managing pain, symptoms, and function in patients with lung cancer and their informal caregivers: Associations with symptoms and distress. Pain, 137, 306-315. doi:10.1016/j.pain.2007.09.010
Rochon, J. (1999). Design and analysis of repeated measures studies using GEE procedures, Version 3.2. Washington, DC: The Biostatistics Center, George Washington University.
at Bartin Universitesi on November 14, 2014wjn.sagepub.comDownloaded from

610 Western Journal of Nursing Research 35(5)
Schafer, J. L., & Graham, J. W. (2002). Missing data: Our view of the state of the art. Psychological Methods, 7, 147-177. doi:10.1037/1082-989X.7.2.147
Schmall, V. L. (1995). Family caregiver education and training: Enhancing self-efficacy. Journal of Case Management, 4, 156-162.
Schumacher, K. L., Koresawa, S., West, C., Hawkins, C., Johnson, C., Wais, E., . . . Miaskowski, C. (2002). Putting cancer pain management regimens into practice at home. Journal of Pain and Symptom Management, 23, 369-382. doi:10.1016/S0885-3924(02)00385-8
Spittle, A. J., Anderson, P. J., Lee, K. J., Ferretti, C., Eeles, A., Orton, J., . . . Doyle, L. W. (2010). Preventive care at home for very preterm infants improves infant and caregiver outcomes at 2 years. Pediatrics, 126, e171-e178. doi:10.1542/peds.2009-3137
Sun, C. C., Bodurka, D. C., Weaver, C. B., Rasu, R., Wolf, J. K., Bevers, M. W., . . . Rubenstein, E. B. (2005). Rankings and symptom assessments of side effects from chemotherapy: Insights from experienced patients with ovarian cancer. Supportive Care in Cancer, 13, 219-227. doi:10.1007/s00520-004-0710-6
Sutton, L. M., Demark-Wahnefried, W., & Clipp, E. C. (2003). Management of termi-nal cancer in elderly patients. Lancet Oncology, 4, 149-157. doi:10.1016/S1470-2045(03)01019-2
Turner, J., Kelly, B., Swanson, C., Allison, R., & Wetzig, N. (2005). Psychosocial impact of newly diagnosed advanced breast cancer. Psycho-Oncology, 14, 396-407. doi:10.1002/pon.856
Weitzner, M. A., Jacobsen, P. B., Wagner, H., Jr., Friedland, J., & Cox, C. (1999). The Caregiver Quality of Life Index-Cancer (CQOLC) Scale: Development and validation of an instrument to measure quality of life of the family caregiver of patients with cancer. Quality of Life Research, 8, 55-63. doi:10.1023/A:1026407010614
Weitzner, M. A., & McMillan, S. C. (1999). The Caregiver Quality of Life Index-Cancer (CQOLC) Scale: Revalidation in a home hospice setting. Journal of Pal-liative Care, 15(2), 13-20.
Zigmond, A. S., & Snaith, R. P. (1983). The hospital anxiety and depression scale. Acta Psychiatrica Scandinavica, 67, 361-370. doi:10.1111/j.1600-0447.1983.tb09716.x
at Bartin Universitesi on November 14, 2014wjn.sagepub.comDownloaded from