effects of venous leg ulceration on patients’ quality of lifevenous leg ulcer, either alone or in...
TRANSCRIPT

42 may 23 :: vol 26 no 38 :: 2012 © NURSING STANDARD / RCN PUBLISHING
Art & science literature review
AbstractThis article reviews the literature on quality of life of people with venous leg ulcers. Research indicates that, in most people, chronic ulceration is a continuous cycle of skin breakdown over a period of decades and is associated with impaired quality of life. Management of leg ulceration represents a major component of the community nursing workload, with community nurses spending approximately half of their time treating patients with leg ulcers. However, the complex psychological and social effects of ulceration on the patient are often overlooked as the nurse’s main focus is on clinical aspects of wound care. This article identifies the importance of adopting a holistic approach to the care of patients with venous leg ulcers to improve outcomes and quality of life.
AuthorDebbie MaddoxCommunity staff nurse, Shelton Primary Care Centre, Stoke-on-Trent.Correspondence to: [email protected]
KeywordsChronic wound, literature review, quality of life, venous leg ulcer
ReviewAll articles are subject to external double-blind peer review and checked for plagiarism using automated software.
OnlineGuidelines on writing for publication are available atwww.nursing-standard.co.uk. For related articles visit the archive and search using the keywords above.
Effects of venous leg ulceration on patients’ quality of lifeMaddox D (2012) Effects of venous leg ulceration on patients’ quality of life. Nursing Standard. 26, 38, 42-49. Date of acceptance: February 14 2012.
There are beTween 70,000 and 190,000 individuals with an open ulcer at any one time in the UK, and annual costs to the nhS, mainly in primary care services, are estimated to be £200 million (Posnett and Franks 2007). Chronic venous leg ulceration is a serious condition, usually attributed to venous insufficiency, and recurrence is common (Morris and Sander 2007) (Figure 1). research indicates that the prevalence of chronic venous leg ulcers increases with age, therefore the number of people with leg ulcers is likely to increase as life expectancy in the UK continues to rise (Posnett and Franks 2007).
The psychological and social effects of leg ulceration on the patient are often overlooked because nursing staff focus mainly on the clinical aspects of wound care (husband 2001, rich and McLachlan 2003). evidence indicates that community nurses spend a significant proportion of their time treating patients with leg ulcers (Morris and Sander 2007), therefore they need to adopt a holistic approach to patient care and demonstrate an understanding of the complex effects of chronic leg ulcers on patients’ quality of life.
Individuals with chronic leg ulcers experience multiple problems, including pain, leakage of exudate and associated odour, altered body image, reduced mobility, and discomfort associated with wearing bulky bandages. These physical problems can lead to social isolation and psychological dysfunction (ebbeskog and ekman 2001, rich and McLachlan 2003, hopkins 2004, ebbeskog and emami 2005, Jones et al 2006, edwards et al 2009). This literature review explores the patient’s experience of living with a chronic venous leg ulcer and effects on quality of life.
Literature searcha systematic search strategy was used to identify articles relevant to the chosen subject. The databases searched were CInahL (Cumulative Index to nursing and allied health Literature), eMbaSe, MeDLIne, PsychInFO, british nursing Index, Cochrane library, wiley Online library, Internurse and Google Scholar. Key terms
p42-49w38.indd 42 21/05/2012 10:44

© NURSING STANDARD / RCN PUBLISHING may 23 :: vol 26 no 38 :: 2012 43
used included chronic wound, quality of life, and venous leg ulcer, either alone or in combination. reference searching and searching done by hand to identify additional bibliographic material was undertaken in the local university library.
Inclusion criteria were a publication date of 1990 onwards, participants aged 19 or over, any type of venous leg ulceration and articles in english only. articles focusing on arterial wounds were excluded. articles identified from the search included six qualitative studies, three quantitative studies and two that used mixed methods. Thematic analysis of the literature identified four key aspects relating to quality of life and venous leg ulceration, including physical symptoms, social functioning, psychological effects and the nurse-patient relationship. evidence from the literature review is used to support clinical practice recommendations outlined in this article. The themes identified are interrelated because similarities were revealed when exploring each theme. a summary of the studies identified in the literature search is provided in Table 1.
Physical symptomsThe physical effects of leg ulceration are multiple and include pain, leakage of exudate and odour, altered body image and impaired mobility.
PainPain is one of the main symptoms referred to in quality of life studies exploring individuals’ experiences of living with a venous leg ulcer. The literature indicates that management of pain by nurses and doctors is not always addressed alongside the clinical aspects of wound care (Douglas 2001, husband 2001, hareendran et al 2005, Morgan and Moffatt 2008). The world health Organization (2010) postulated that unresolved pain can have a negative effect on wound healing, which in turn has a negative effect on quality of life. To support clinical practice, the Essence of Care (Department of health (Dh) 2010) benchmark defines pain management as any intervention to prevent or alleviate pain and the effect of pain so that quality of life and functional ability are optimised.
Grounded theory uses a systematic qualitative approach to generate theory from various data sources and allows the researcher to modify and extend different theories (Gerrish and Lacey 2010). husband (2001) conducted a qualitative study using grounded theory to explore the personal experiences of 39 patients with venous leg ulcers and their perception of management by nurses and doctors in two health districts in
england. The main symptom that led patients to consult with practitioners was pain. Pain increased to intolerable levels at night and was associated with increased temperature as a result of bed clothes and difficulty finding a comfortable position for the ulcerated limb. Patients’ descriptions of pain did not result in management of this symptom by doctors and nurses. The study identified pain as a central recurring physical symptom of venous leg ulcers, both in the acute and chronic stages of ulceration.
ebbeskog and ekman (2001) interviewed 15 older people (74-89 years) to determine their experiences of living with a venous leg ulcer. Interviews lasted between 45 minutes and two hours, which may have limited the findings. Participants reported that they lived a restricted life, were unable to take daily walks and that their sleep was interrupted by pain. Participants described pain as being ‘so awful’ that the leg ulcer controlled their lives. when severity of pain increased, patients reported consuming ‘several packages of painkillers’. This, in combination with disruption to daily life, significantly reduced participants’ quality of life.
rich and McLachlan (2003) also identified pain as a major issue for people with venous leg ulcers, even though pain was not one of the aspects that individuals were asked about during the interview. Participants described days spent in pain as ‘horrible’ and that their daily living was restricted. Systematic use of pain assessment tools combined with a holistic initial assessment of pain and continuous evaluation thereafter may help to alleviate some of these problems.
Various pain assessment tools to suit individual needs are available. however, standardising pain
FIGURE 1 Venous leg ulcer
AlA
My
p42-49w38.indd 43 21/05/2012 10:44
Art & science literature review
44 may 23 :: vol 26 no 38 :: 2012 © NURSING STANDARD / RCN PUBLISHING
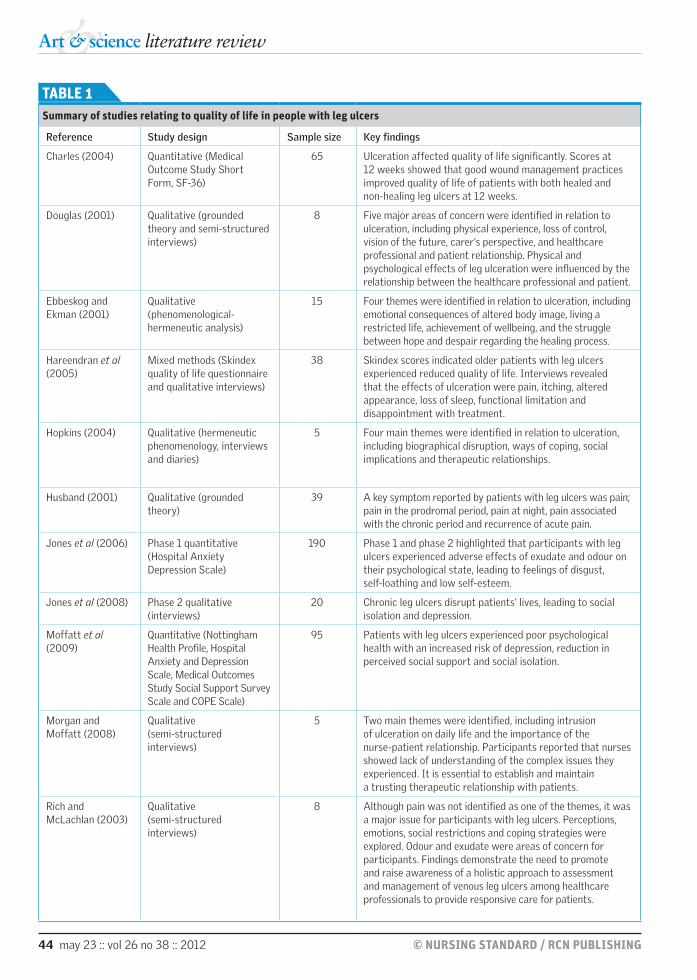
TABLE 1 Summary of studies relating to quality of life in people with leg ulcers
Reference Study design Sample size Key findings
Charles (2004) Quantitative (Medical Outcome Study Short Form, SF-36)
65 Ulceration affected quality of life significantly. Scores at 12 weeks showed that good wound management practices improved quality of life of patients with both healed and non-healing leg ulcers at 12 weeks.
Douglas (2001) Qualitative (grounded theory and semi-structured interviews)
8 Five major areas of concern were identified in relation to ulceration, including physical experience, loss of control, vision of the future, carer’s perspective, and healthcare professional and patient relationship. Physical and psychological effects of leg ulceration were influenced by the relationship between the healthcare professional and patient.
Ebbeskog and Ekman (2001)
Qualitative (phenomenological-hermeneutic analysis)
15 Four themes were identified in relation to ulceration, including emotional consequences of altered body image, living a restricted life, achievement of wellbeing, and the struggle between hope and despair regarding the healing process.
Hareendran et al (2005)
Mixed methods (Skindex quality of life questionnaire and qualitative interviews)
38 Skindex scores indicated older patients with leg ulcers experienced reduced quality of life. Interviews revealed that the effects of ulceration were pain, itching, altered appearance, loss of sleep, functional limitation and disappointment with treatment.
Hopkins (2004) Qualitative (hermeneutic phenomenology, interviews and diaries)
5 Four main themes were identified in relation to ulceration, including biographical disruption, ways of coping, social implications and therapeutic relationships.
Husband (2001) Qualitative (grounded theory)
39 A key symptom reported by patients with leg ulcers was pain; pain in the prodromal period, pain at night, pain associated with the chronic period and recurrence of acute pain.
Jones et al (2006) Phase 1 quantitative (Hospital Anxiety Depression Scale)
190 Phase 1 and phase 2 highlighted that participants with leg ulcers experienced adverse effects of exudate and odour on their psychological state, leading to feelings of disgust, self-loathing and low self-esteem.
Jones et al (2008) Phase 2 qualitative (interviews)
20 Chronic leg ulcers disrupt patients’ lives, leading to social isolation and depression.
Moffatt et al (2009)
Quantitative (Nottingham Health Profile, Hospital Anxiety and Depression Scale, Medical Outcomes Study Social Support Survey Scale and COPE Scale)
95 Patients with leg ulcers experienced poor psychological health with an increased risk of depression, reduction in perceived social support and social isolation.
Morgan and Moffatt (2008)
Qualitative (semi-structured interviews)
5 Two main themes were identified, including intrusion of ulceration on daily life and the importance of the nurse-patient relationship. Participants reported that nurses showed lack of understanding of the complex issues they experienced. It is essential to establish and maintain a trusting therapeutic relationship with patients.
Rich and Mclachlan (2003)
Qualitative (semi-structured interviews)
8 Although pain was not identified as one of the themes, it was a major issue for participants with leg ulcers. Perceptions, emotions, social restrictions and coping strategies were explored. Odour and exudate were areas of concern for participants. Findings demonstrate the need to promote and raise awareness of a holistic approach to assessment and management of venous leg ulcers among healthcare professionals to provide responsive care for patients.
p42-49w38.indd 44 21/05/2012 10:44

© NURSING STANDARD / RCN PUBLISHING may 23 :: vol 26 no 38 :: 2012 45
assessment in the community setting may alleviate inconsistencies in pain assessment and management. Guidelines on the management of leg ulcers have been published by the royal College of nursing (rCn) (2006) and the Scottish Intercollegiate Guidelines network (SIGn) (2010). They state that healthcare professionals should be sensitive to the needs of the patient during assessment, and that they should highlight the importance of joint decision making, patient involvement and patient understanding in leg ulcer management. Previous research suggests that district nurses do not assess pain consistently (roe et al 1993). There is also lack of research on the preferred method of pain assessment for individuals with venous leg ulcers (rCn 2006). however, Stevens (2006) concluded that thorough and regular pain assessment has a positive effect on patients’ quality of life.
an understanding of pain control theories and the development of tolerance to pain relief needs to be taken into account, and alternative pain relief options considered. Pain is a complex and subjective experience (Dh 2010). The skills and expert knowledge of the nurse are essential in supporting the desired outcome for individual pain relief. Planning acceptable interventions and regular evaluation of their effectiveness are fundamental. effective communication with patients and patient education regarding pain mechanisms may improve patients’ experiences and clinical outcomes. If unsure of how to manage pain caused by leg ulceration, healthcare professionals should seek advice and support from pain specialist nurses, who are recognised for their expert knowledge in this field.
Further recommendations include planning a convenient time to visit the patient. This will allow the patient to take the required amount of analgesia to relieve painful symptoms experienced when changing or removing dressings, for example. Choice of dressing may also minimise pain and discomfort (rCn 2006, SIGn 2010). wound dressing packs often contain the Faces Pain rating Scale (wong and baker 1988), which may prompt the healthcare professional to assess pain during wound dressing. however, this pain scale is not available in all dressing packs. Standardisation of documentation for pain assessment and wound care products may help to alleviate pain and support continuity of care in this patient group.
Further research is needed on the advantages and disadvantages of the various pain assessment tools to improve assessment and management of pain in patients with leg ulcers in the community setting. healthcare professionals have an important role
in assessing the extent of disruption that pain causes to the patient’s life (husband 2001).
Leakage of exudate and odour although moisture is a necessary and normal part of the wound healing process, excessive moisture may damage the wound bed and surrounding skin, causing maceration, excoriation and odour (Cutting and white 2002, world Union of wound healing Societies (wUwhS) 2007). Odour is particularly distressing for patients and can lead to social isolation as a result of embarrassment (rich and McLachlan 2003, Jones et al 2006, 2008, Moffatt et al 2009). evidence suggests that leakage of exudate adversely affects individuals’ psychological health, which in turn affects quality of life. In addition, odour and leakage of exudate may go unrecognised in clinical practice (rich and McLachlan 2003, Jones et al 2006, 2008, Morgan and Moffatt 2008).
Jones et al (2006, 2008) conducted a mixed methods study to investigate the link between venous leg ulceration, depression, odour and exudate. Participants reported adverse effects of odour and excessive exudate on their psychological wellbeing, leading to feelings of disgust, self-loathing and low self-esteem. Key themes relating to odour were emotional response to odour; limitation of social activities as a result of the fear that odour might be present; and the ways in which odour, or fears about the presence of odour, were managed by nurses. rich and McLachlan (2003) reported that participants viewed odour and exudate as ‘unbearable’ and were concerned about exudate coming into contact with their clothes and household furnishings. Similar findings have been reported elsewhere (Douglas 2001, Morgan and Moffatt 2008).
The rCn (2006) recommends that the assessment of odour should be documented when the patient first presents with a leg ulcer and should form part of routine patient monitoring. education regarding leg ulcer assessment and management is vital and is advocated in wound management guidelines (european wound Management association 1991, 2010, SIGn 2010). Improved understanding of dressing regimens may help to alleviate the problems of leakage of exudate and odour. Dressing products that are effective in the management of exudate and odour are available. Tissue viability nurses and wound care specialists are ideally placed to give healthcare professionals advice on dressings as they have knowledge of the most up-to-date evidence-based guidance. Community nurse champions may also have a role
p42-49w38.indd 45 21/05/2012 10:44

Art & science literature review
46 may 23 :: vol 26 no 38 :: 2012 © NURSING STANDARD / RCN PUBLISHING
to play in supporting staff. Link nurses with a special interest in venous leg ulceration may be able to use their knowledge and skills to disseminate the most up-to-date information to colleagues.
The wUwhS (2007) advocates assessment of exudate by healthcare professionals and offers support and guidance from evidence-based practice. This international consensus document for the management of wound exudate and the role of dressings is a useful resource for all healthcare professionals. Copies of these documents should be readily available in the community and are also easily accessible on the internet. Specialist leg ulcer clinics for treatment of venous leg ulcers in the community are beneficial (edwards et al 2009) and provide peer support (Lindsay 2001). all practitioners should endeavour to optimise their skills in the area of leg ulcer management regardless of the clinical setting (SIGn 2010).
Functional limitationsThe mainstay of treatment for venous leg ulcers is compression therapy (rCn 2006, SIGn 2010). however, several factors influence the effectiveness of this approach, including the practitioner’s knowledge and skill, shape of the limb and patient compliance (rCn 2006). Lay-Flurrie (2005) noted that, even with the correct dressing regimen, patient outcome will be poor if patient assessment is inadequate or bandaging is sub-optimal, resulting in bandage slipping, distortion, pressure damage and infection, all of which may lead to functional limitations and reduced quality of life.
hareendran et al (2005) used a mixed methodology approach to explore quality of life issues in patients with venous leg ulcers with the aim of generating items for a treatment outcome measure. Patients were interviewed following completion of the adapted Skindex questionnaire – a quality of life measure for patients with skin disease (Chren et al 1996). effects of ulceration included altered appearance of the limb, with participants reporting that they felt self-conscious and unattractive and were unable to wear their usual clothes because of the ulcer and associated bandages. a total of 97.2% of patients reported some restriction of function, for example difficulties in bathing (50%) and inability to pursue enjoyable activities (47.2%). Disappointment with treatment (50%) was a common factor, with patients feeling that little was done to speed up the healing process or reduce symptoms. In contrast, participants also reported that many limitations were self-imposed as they often adopted unnecessary avoidance tactics to minimise the risk
of aggravating the ulcer. These findings correlate with previous studies regarding body image and mobility issues experienced by individuals with chronic leg ulcers (Douglas 2001, ebbeskog and ekman 2001, Morgan and Moffatt 2008).
Pain, exudate and extensive bandaging associated with ulceration limits mobilisation and may, in turn, contribute to reduced motivation and poor compliance with treatment. Those who care for patients with venous leg ulcers need to be proactive and responsive to individuals’ needs, and reflect on the outcomes of wound care treatments in relation to quality of life and in particular, altered body image.
Social functioninghopkins (2004) explored the experiences of five people with non-healing venous leg ulcers. Findings revealed four main themes: biographical disruption (such as hopes for the future, general wellbeing and unpredictable nature of the ulcer), ways of coping, social implications and therapeutic relationships. In addition, the findings acknowledged the effects of ulceration on participants’ social life. Participants described previous physical or social activity in which they were no longer able to engage as a result of their leg ulcers. Social exclusion, wasted days and loss of privacy were described by participants as changes that they ‘learned to live with’. Disruption to social networks was related to physical symptoms such as odour and exudate; participants were reluctant to go out in public because of the embarrassment and offence that their malodorous wounds may cause to others. These findings are similar to those of Jones et al (2008) and ebbeskog and ekman (2001), who identified disruption to and restrictions on daily life as a result of venous leg ulcers.
In contrast to husband’s (2001) findings, participants in hopkins’ (2004) study reported that their relationships with healthcare professionals were positive, and they had confidence in the nurses caring for them. Participants’ experiences highlighted how the role of the district nurse was significant in developing participants’ ability to cope with ulceration.
Moffatt et al (2009) reported a reduction in perceived social support leading to feelings of social isolation in participants with chronic leg ulcers. Care provision should include support groups and/or networks for patients. The leg club model of leg ulcer management (Lindsay 2001) aims to address the psychosocial aspects of living with a chronic venous leg ulcer. however, although this innovative model is
p42-49w38.indd 46 21/05/2012 10:44

© NURSING STANDARD / RCN PUBLISHING may 23 :: vol 26 no 38 :: 2012 47
gaining in popularity in australia, it has not been adopted widely in the UK (brown 2010). efficacy studies of the leg club model have demonstrated significantly improved outcomes in quality of life scores, self-esteem, morale, functional ability and improved pain relief for patients (edwards et al 2009). although leg clubs are also cost effective (edwards et al 2009), further research is needed to support dissemination of this model.
Psychological effectsholistic care for people with venous leg ulcers is vital, but current healthcare culture, political initiatives and nursing shortages can limit psychological support for these patients (anderson 2000, hollingworth and hawkins 2002).
In a mixed methods case-controlled study, Moffatt et al (2009) identified deficits in psychological health in a group of 95 patients with venous leg ulcers compared with a control group. Patients had significantly poorer health-related quality of life in all domains of the nottingham health Profile (hunt et al 1986) compared with controls (P=<0.001), and depression was more prevalent in patients with leg ulcers (P=<0.001). Interestingly, there was no significant difference in anxiety scores between the patient and control groups (P=0.59).
The Medical Outcomes Study Social Support Survey (Sherbourne and Stewart 1991) revealed fewer social networks and a reduction in perceived support among patients with leg ulcers compared with controls (P=<0.008). Patients used fewer problem-focused and emotion-focused coping strategies than the control group (P=0.001), as assessed by the COPe scale (Carver et al 1989).
evidence suggests that there is no difference in anxiety between patients with venous leg ulcers and the general population, although those with leg ulcers tend to have higher levels of clinical depression. These findings are supported by Jones et al (2006), who reported that 27% of participants with leg ulcers experienced depression. The two main symptoms associated with anxiety and depression were pain (P=<0.001) and odour (P=<0.001); however, there was no association found between living alone, mobility and exudate (Jones 2006). nonetheless, these studies indicate that patients with venous leg ulcers are at risk of anxiety and depression triggered by the physical symptoms of ulceration.
research has identified the psychological effects of venous leg ulcers and influence of locus of control on patients’ experiences. according
to rotter’s (1966) social learning theory, people have an internal or external locus of control. Charles (1995) reported that participants with an internal locus of control assumed an active approach to ulcer management and were in control of events, whereas participants with an external locus of control believed that others were in control. healthcare professionals have a key role in enabling patients to feel in control of their condition. Morris and white (2007) suggested that communication between the nurse and patient as part of a therapeutic relationship promotes a sense of control and self-efficacy.
Nurse-patient relationshipSeveral factors that influenced the relationship between the nurse and patient with venous leg ulceration are highlighted in the literature.
Morgan and Moffatt (2008) explored the relationship between patients with non-healing leg ulcers and the nurses caring for them in the community. The two main themes identified were intrusion of ulceration on daily life and the importance of the nurse-patient relationship in developing effective strategies for daily living. Patients felt that nurses showed a lack of understanding of the complex issues they experienced. Patients’ perception of nurses’ knowledge, understanding of leg ulcers and commitment to their care was a significant influence on nurse-patient relationships. Use of coping strategies to maintain a balance between managing the physical effects of the ulcer and ensuring the care received met patients’ needs was central. a gap was identified between the goals of the patient to achieve comfort and the goals of the nurse to achieve healing.
Douglas (2001) conducted semi-structured interviews with eight patients who had venous leg ulcers to ascertain their experiences of and feelings about their relationships with healthcare professionals. results showed that physical and psychological effects of leg ulceration were influenced by the nurse-patient relationship. Patients felt that the physical aspects of leg ulceration, for example pain, were not addressed adequately during assessment. recurrent problems included nurses experimenting with various dressings and patients receiving conflicting advice about management of their leg ulcer.
In contrast, Charles’ (2004) quantitative study evaluated the effect of venous leg ulceration and treatment on patients’ quality of life. Data were collected from a small patient sample (n=65) using the Medical Outcome Study 36-Item Short Form
p42-49w38.indd 47 21/05/2012 10:44

Art & science literature review
48 may 23 :: vol 26 no 38 :: 2012 © NURSING STANDARD / RCN PUBLISHING
health Survey (SF-36) (ware and Sherbourne 1992), which measures health across a number of domains. although data were collected over a short period (12 weeks) and the SF-36 is designed to identify differences at 12 months, results showed that good wound management practices improved patients’ quality of life (Charles 2004).
It may be useful for patients to keep a diary of home visits to record any problems encountered in the period between visits by the nurse so that any concerns that arise can be discussed. as the nurse will generally be the patient’s first point of contact and will monitor the patient’s progress, he or she will most likely have a good insight into the patient’s thoughts, feelings and concerns. The rCn (2006) advocates the importance of joint decision making between healthcare professionals and patients, and patient involvement in leg ulcer management.
Systematic assessment tools for leg ulceration may improve patient outcomes, be cost-effective and allow timely intervention by the nurse. Quality improvement measures such as clinical audits aimed at improving quality of life for patients may also support proactive interventions and benefit future practice within the community setting. Further research is necessary to advance future practice in relation to leg ulcer assessment and management.
however, from the evidence available, the following recommendations can be made for clinical practice:��Pain assessment tools should be used systematically by all members of staff, and knowledge and understating of pain management should be continuously evaluated. Community nurses should use the resources
ReferencesAnderson I (2000) Quality of life and leg ulcers: will NHS reform address patient need? British Journal of Nursing. 9, 13, 830-840.
Brown A (2010) Chronic leg ulceration in the community: changing the focus. British Journal of Community Nursing. 15, 9, S6-S16.
Carver CS, Scheier MF, Weintrauh JK (1989) Assessing coping strategies: a theoretically based approach. Journal of Personality and Social Psychology. 56, 2, 267-283.
Charles H (1995) The impact of leg ulcers on patients’ quality of life. Professional Nurse. 10, 9, 571-574.
Charles H (2004) Does leg ulcer treatment improve patients’ quality of life? Journal of Wound Care. 13, 6, 209-213.
Chren MM, lasek RJ, Quinn lM, Mostow EN, Zyzanski SJ (1996)
Skindex, a quality of life measure for patients with skin disease: reliability, validity and responsiveness. Journal of Investigative Dermatology. 107, 5, 707-713.
Cutting KF, White RJ (2002) Avoidance and management of peri-wound maceration of the skin. Professional Nurse. 18, 1, 33-36.
Department of Health (2010) Essence of Care. Benchmarks for the Prevention and Management of Pain. The Stationery Office, london.
Douglas V (2001) living with a chronic leg ulcer: an insight into patients’ experiences and feelings. Journal of Wound Care. 10, 9, 355-360.
Ebbeskog B, Ekman Sl (2001) Elderly persons’ experiences of living with venous leg ulcer: living in a dialectal relationship between freedom and imprisonment. Scandinavian
Journal of Caring Sciences. 15, 3, 235-243.
Ebbeskog B, Emami A (2005) Older patients’ experience of dressing changes on venous leg ulcers: more than just a docile patient. Journal of Clinical Nursing. 14, 10, 1223-1231.
Edwards H, Courtney M, Finlayson K, Shuter P, lindsey E (2009) A randomised control trial of community intervention: improved quality of life and healing for clients with chronic leg ulcers. Journal of Clinical Nursing. 18, 11, 1541-1549.
European Wound Management Association (1991) History in Brief. http://ewma.org/english/about-ewma.html (last accessed: May 8 2012.)
European Wound Management Association (2010) Outcomes in controlled and comparative studies on non-healing wounds: recommendations to improve
the quality of evidence in wound management. Journal of Wound Care. 19, 6, 239-268.
Gerrish K, lacey A (2010) The Research Process in Nursing. Sixth edition. Blackwell Publishing, Oxford.
Hareendran A, Bradbury A, Budd J et al (2005) Measuring the impact of venous leg ulcers on quality of life. Journal of Wound Care. 14, 2, 53-57.
Hollinworth H, Hawkins J (2002) Teaching nurses psychological support of patients with wounds. British Journal of Nursing. 11, Suppl 20, S8-S18.
Hopkins A (2004) Disrupted lives: investigating coping strategies for non-healing leg ulcers. British Journal of Nursing. 13, 9, 556-563.
Hunt SM, McEwan J, McKenna SP (1986) Measuring Health Status. Croom Helm, Beckenham.
p42-49w38.indd 48 21/05/2012 10:44

© NURSING STANDARD / RCN PUBLISHING may 23 :: vol 26 no 38 :: 2012 49
and knowledge of pain specialist nurses. Patient diaries should be used to recall and prompt pain assessment during visits by the nurse.��effective therapeutic nurse-patient relationships should be established to enhance the patient experience during home visits. Patients should keep a diary of problems encountered in the period between visits by the nurse so that any issues that arise during this time can be discussed at the next visit. a collaborative approach to decision making and management of the ulcer is advocated.��Staff should be educated in assessment and management of venous leg ulcers (rCn 2006, SIGn 2010). They should also have up-to-date knowledge on dressing techniques to minimise odour and exudate. Tissue viability nurses may be approached for advice about dressing
regimens, and link nurses and community nurse champions can provide support to staff.��Specific quality of life instruments should be incorporated in wound care pathways, and should take into account holistic assessment of patients with venous leg ulcers.
ConclusionQuality of life may be significantly affected by venous leg ulcers. It is imperative that distressing symptoms, such as pain, leakage of exudate and odour, and the effects of leg ulcers on psychological wellbeing and social interaction, are acknowledged and assessed. Therefore, a holistic approach to care and management of patients with venous leg ulcers is essential to improve patient outcomes and ultimately quality of life NS
Husband ll (2001) Venous ulceration: the pattern of pain and the paradox. Clinical Effectiveness in Nursing. 5, 1, 35-40.
Jones J, Barr W, Robinson J, Carlisle C (2006) Depression in patients with chronic venous ulceration. British Journal of Nursing. 15, 11, 17-23.
Jones JE, Robinson J, Barr W, Carlisle C (2008) Impact of exudate and odour from chronic venous leg ulceration. Nursing Standard. 22, 45, 53-61.
lay-Flurrie K (2005) Assessment and good technique are key to effective compression therapy. Professional Nurse. 20, 7, 31-34.
lindsay E (2001) Compliance with science: benefits of developing community leg clubs. British Journal of Nursing. 10, 22, S66-S74.
Moffatt CJ, Franks PJ, Doherty DC, Smithdale R, Steptoe A (2009)
Psychological factors in leg ulceration: a case-control study. British Journal of Dermatology. 161, 4, 750-756.
Morgan PA, Moffatt CJ (2008) Non-healing leg ulcers and the nurse-patient relationship. Part 1: the patient’s perspective. International Wound Journal. 5, 2, 340-348.
Morris P, Sander R (2007) leg ulcers. Nursing Older People. 19, 5, 33-37.
Morris T, White G (2007) Motivational interviewing with clients with chronic leg ulceration. British Journal of Community Nursing. 12, 3, S26-S30.
Posnett J, Franks P (2007) The costs of skin breakdown and ulceration in the UK. In Skin Breakdown: The Silent Epidemic. The Smith & Nephew Foundation, UK. 6-12.
Rich A, Mclachlan l (2003) How living with a leg ulcer affects
people’s daily life: a nurse-led study. Journal of Wound Care. 12, 2, 51-54.
Roe BH, luker KA, Cullum NA, Griffiths JM, Kenrick M (1993) Assessment, prevention and monitoring of chronic leg ulcers in the community: report of a survey. Journal of Clinical Nursing. 2, 5, 299-306.
Rotter JB (1966) Generalized expectancies for internal versus external control of reinforcement. Psychology Monographs. 80, 1, 1-28.
Royal College of Nursing (2006) Clinical Practice Guidelines: The Nursing Management of Patients with Venous Leg Ulcers. RCN, london.
Scottish Intercollegiate Guidelines Network (2010) Management of Chronic Venous Leg Ulcers: A National Clinical Guideline. Guideline No. 120. SIGN, Edinburgh.
Sherbourne CD, Stewart Al (1991) The MOS Social Support Survey.
Social Science and Medicine. 32, 6, 705-714.
Stevens H (2006) The impact of venous ulcer pain: what can the patient teach us? Wound Care. 11, Suppl 12, 27-30.
Ware JE, Sherbourne CD (1992) The MOS 36-item Short-Form Health Survey (SF-36): 1. Conceptual framework and item selection. Medical Care. 30, 6, 473-483.
Wong Dl, Baker CM (1988) Pain in children: comparison of assessment scales. Paediatric Nursing. 14, 1, 9-17.
World Health Organization (2010) Wound and Lymphoedema Management. World Health Organization, Geneva.
World Union of Wound Healing Societies (2007) Wound Exudate and the Role of Dressings: A Consensus Document. Medical Education Partnership, london.
p42-49w38.indd 49 21/05/2012 10:44