e:kims new ackup 6janclinical meetings 201501.08.2015 · pdf file ·...
TRANSCRIPT

Case Presentation
SIGMOID VOLVULUSBy,Dr. ANSARI SANA AFREEN1 yr PGDept. of General Surgery KIMS Narketpally

Sathish a 18yr old male presented to the EMD on 10-06-2015
COMPLAINTS AND DURATION:
• Pain in Abdomen since 3 days• Not passing stools since 3 days• 4 episodes of vomiting since 1 day

HISTORY OF PRESENT ILLNESS:• Patient was apparently asymptomatic 3 days back then he
developed Pain Abdomen sudden in onset, diffuse and colicky in nature associated with gradually increasing Abdominal distension. No aggravating /relieving factors
• H/o Obstipation since 3 days.• H/o Nausea and vomiting 4 episodes since 1 day non projectile
non bilious.• There was no associated history of trauma/bleeding per rectum/
mucous discharge per rectum/ fever/ burning micturition• No history of significant weight loss/ anorexia.

PAST HISTORY: • No similar complaints in the Past.• No history of Diabetes, Hypertension, TB, CAD, CVA, Bronchial
Asthma, Epilepsy • No history of previous abdominal surgeries.
PERSONAL HISTORY:
• Appetite is Normal• Consumes Mixed Diet• Normal Bowel and Bladder habits• No known Allergies• No Addictions

FAMILY HISTORY:• No h/o Diabetes, Hypertension, Heart Disease, Stroke,
Cancers, tuberculosis or Asthma in Family.• No other Hereditary Disease.
DRUG HISTORY: • Nil significant.

PHYSICAL EXAMINATION:
GENERAL:-Patient is conscious, coherent, cooperativeNo signs of Pallor / Icterus / Cyanosis / Clubbing / Lymphadenopathy / Oedema of
feet
Patient is dehydrated. • Temperature : 98.6F• Pulse Rate : 100/ min• BP : 110/80 mm of Hg• Respiratory Rate : 20/ min

SYSTEMIC EXAMINATION:-
• CVS- S1 S2 heard No Murmurs
• RESPIRATORY SYSTEM- BAE + NVBS No Adventitious sounds
• CNS- No focal neurological deficit

ABDOMEN: INSPECTION:• Abdomen is Distended• No visible Peristalsis• No visible mass • No scars or sinuses• Hernial orifices are normal
PALPATION: Tense Generalized Tenderness is present no guarding no rigidity no organomegaly no signs of free fluid in the peritoneal cavity. PERCUSSION : tympanic note found all over abdomen.AUSCULTATION: Bowel sounds – absent

X-RAY ERECT ABDOMEN –• Evidence of large dilated bowel loop showing
Coffee-Bean Appearance is seen in left side of Abdomen extending into right side inferiorly
• No evidence of Air under Diaphragm.• Few Air-fluid levels noted.• Visualized bone and soft tissues appear normal
Impression: D/D 1. sigmoid volvulus
2. caecal volvulus
INVESTIGATIONS:

INVESTIGATIONS:
USG ABDOMEN –
Impression: free fluid noted in Peri-hepatic ,RIF and Inter-Bowel spaces no evidence of internal echoes correlate with erect X-ray Abdomen.

BLOOD GROUP: AB positive
CBP:Hb : 13gm%TLC : 8,600/cu . mmPlatelets : 2.4 lakh/ cu .mmSmear : Normocytic Normochromic
Bleeding Time : 2minClotting time : 3min 30sec
RBS : 92 mg/dl
ECG : normal findingsChest X-RAY : normal findings
PROVISIONAL DIAGNOSIS : SIGMOID VOLVULUS
Initial treatment :• NBM• Ryles tube aspiration • foleys catherisation • IV fluids • Inj cefotaxim 1gm iv • Inj metronidazole 100ml iv • Inj pantoprazole 40mg iv • Inj tramadol 50mg slow iv

OPERATIVE PROCEDURE: Detorsion of volvulus and procedure
Surgery Starting time: 10.15pm Ending Time: 11.30pm• Under GA abdomen was prepared with Betadine and Spirit and draped.• Abdomen opened with Left Para Median Incision.• Sigmoid Colon deflated and detorsion done.• Resection of Volvulus Segment done sigmoid colectomy.• End to end anastomosis of descending colon to rectum done .• Rent in sigmoid mesocolon is closed.• Hemostasis is secured.• Flatus tube passed beyond anastomosis.• Wound closed in layers with Abdominal drain in pelvis.
Final DIAGNOSIS: SIGMOID VOLVULUS

Sigmoid volvulus
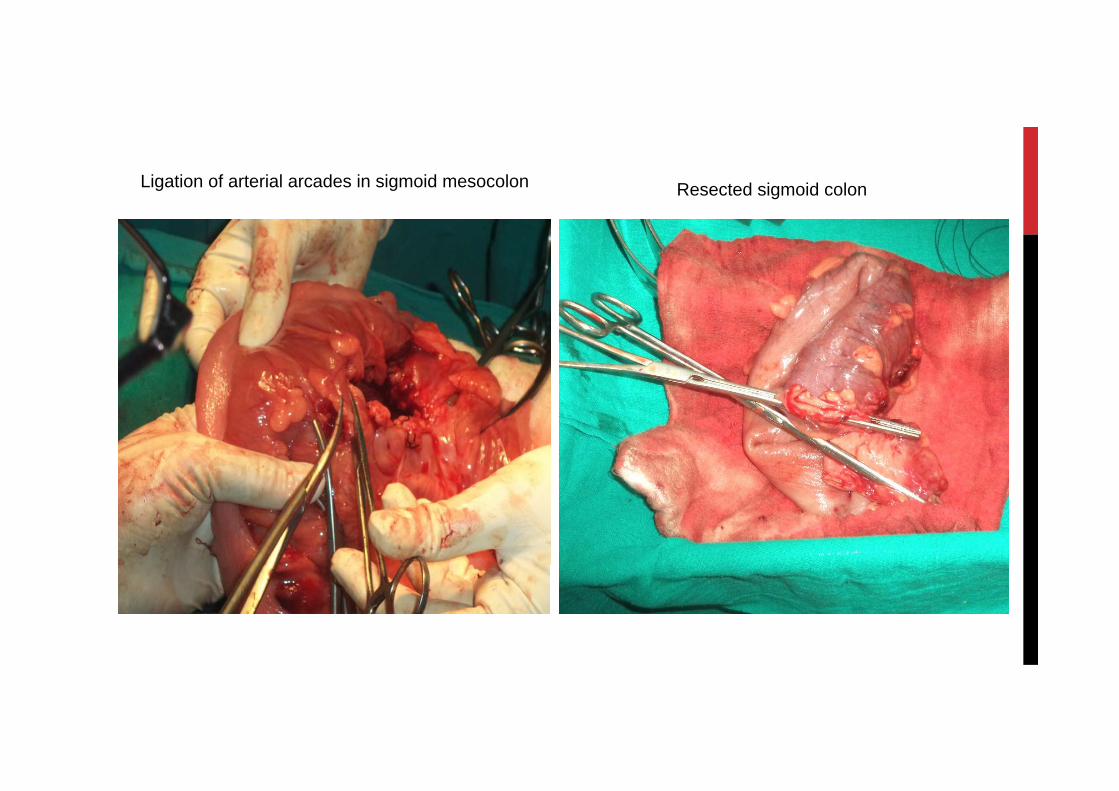
Ligation of arterial arcades in sigmoid mesocolon Resected sigmoid colon

Anastomosis of bowel

Post Operative Management:
POD-1 NBM for 48 hrs with RTA 2nd hrly IV fluids, Antibiotic, Analgesic Flatus tube continued I/O charting
Care of catheters Drain-20ml
POD-2 Patients General condition is stable continued IV fluids , Antibiotics, and other treatment as on 1st POD
Drain-150ml
POD-3 Bowel sounds present Ryles tube removed IV fluids discontinued
liquid diet started, Drain-100ml

POD-4 Flatus tube removed, Drain-minimal
POD-5 Soft diet started , Oral antibiotics instituted, passed stools, Abdominal Drain removed.
POD-8 Suture removal done , wound healthy.
POD-12 Post-operative period is uneventfull. Patient is Discharged

THANK YOU