elbow tendinopathy
TRANSCRIPT

Elbow tendinopathy update
Adam C Watts
Consultant Elbow Surgeon, Wrightington Hospital Visiting Professor, University of Manchester
1

www.wrightington.com
Why is the elbow prone to tendinopathy?
2

www.wrightington.com
Tendinopathies around the elbow
Lateral epicondylosis (Tennis elbow)
Medial epicondylosis (Golfer’s elbow)
Distal biceps tendinopathy
Distal triceps tendinopathy
3
decr
easi
ng in
cide
nce

www.wrightington.com4

www.wrightington.com5

www.wrightington.com6

www.wrightington.com7

www.wrightington.com8
Pronator teres tendon origin

www.wrightington.com
Presentation
Insidious onset
Change in activity/technique
9
Weekend warrior >>> club athlete > elite

www.wrightington.com
Clinical Diagnosis
10

www.wrightington.com
O’Driscoll hook test for distal biceps
11

www.wrightington.com 12
Assess whole kinetic chain
90% of tennis players have scapula dyskinesia
84% have GIRD
Lopez Vidriero, ESSKA 2016

www.wrightington.com
Assess whole patient! - Psychological factors
Association between catastrophisation and tennis elbow
Moderate association with distress
No relationship to kinesiophobia
13

www.wrightington.com
When to get plain radiographs
Younger and older patients
Past history elbow trauma
Mechanical symptoms
Positive grip and grind
14
important to exclude OCD in the young

www.wrightington.com
Is there a role for MRI?
15

www.wrightington.com16
NormalTendinopathic

www.wrightington.com
What is a tendinopathy?
Chronic degenerative condition
Angiofibroblastic tendinosis
Myofibroblast proliferation
17
Still none the wiser!

www.wrightington.com
Normal Tendon
18

www.wrightington.com19

www.wrightington.com20

www.wrightington.com
Tendon Biology
Slow metabolism
Poor vascular supply
Neural elements
Tenocytes and mast cells
21

www.wrightington.com
Neurocellular Model Tendon Homeostasis
22
Proteases
Chemotactic factors

www.wrightington.com23
Nerve - Mast Cell Units
‘Normal’ physiological
loads
Tissue Homeostasis
Exercise - modest overload
Functional Adaptation
Overload - acute
or chronic
Neurocellular degeneration

www.wrightington.com24

www.wrightington.com
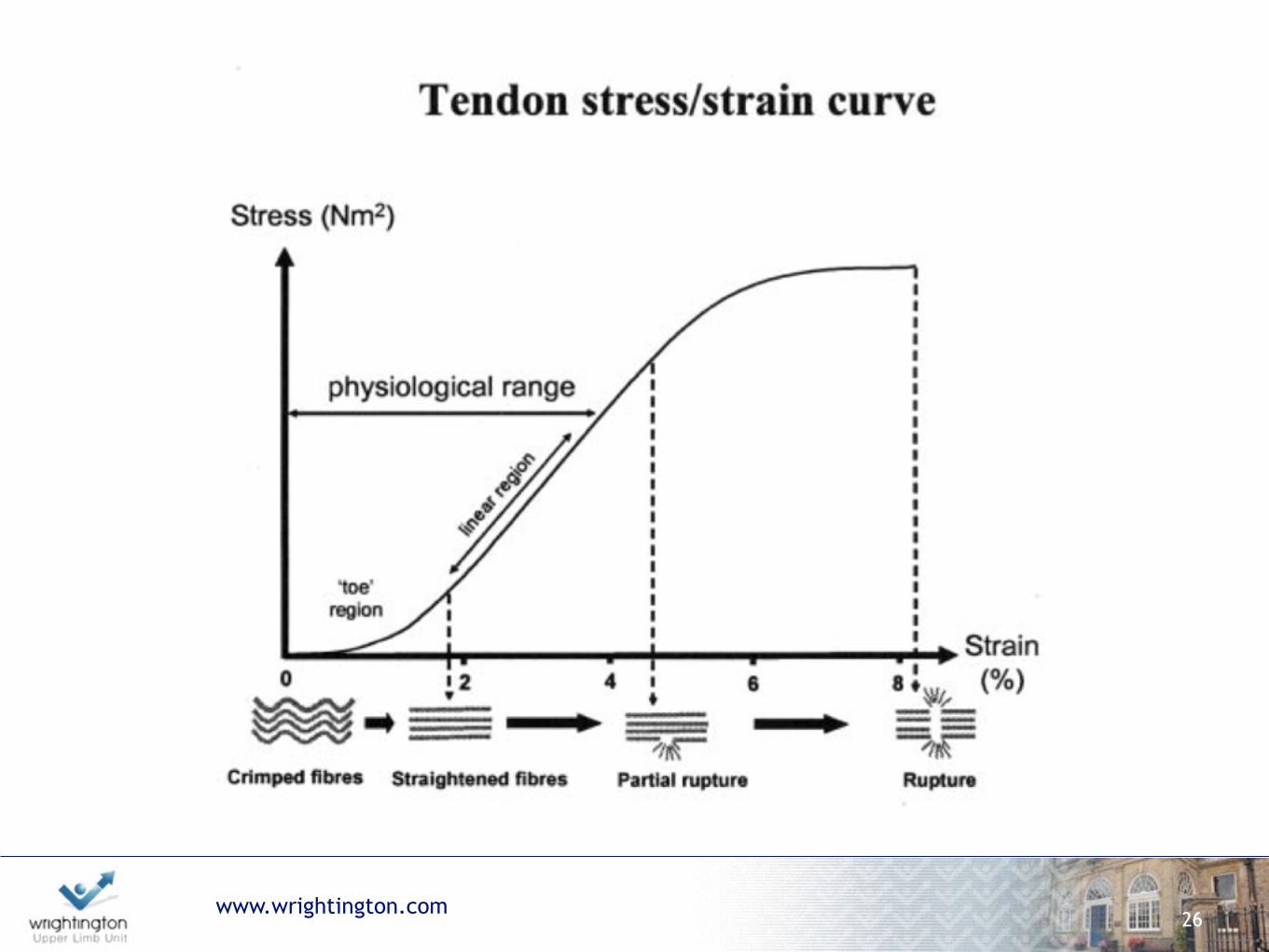
Why does risk increase with age?
Crimping lost during adulthood
25
www.wrightington.com26

www.wrightington.com27
Ageing
Uncrimped fibres more sensitive to changes in load?

www.wrightington.com
4 stages of tendinopathy
28

www.wrightington.com29

www.wrightington.com
Suggested Algorithm
30

www.wrightington.com
Eccentric loading for tendon dysrepair
Significant improvement in DASH score and VAS pains score when compared to standard treatment
31

www.wrightington.com
Eccentric Loading Distal Biceps
Biceps predominantly a supinator of forearm
32

www.wrightington.com33
physiotherapy did not optimise long-term outcome
short-term benefit in the absence of corticosteroid injection

www.wrightington.com34
Steroid Injection
Physiotherapy

www.wrightington.com
Is there any place for corticosteroids?
35
www.wrightington.com
Corticosteroids
Inhibit tenocyte proliferation
Inhibit tenocyte activity
Inhibit collagen synthesis
Increase tenocyte necrosis
36

www.wrightington.com37
Steroid Injection
Physiotherapy
Natural History
www.wrightington.com38
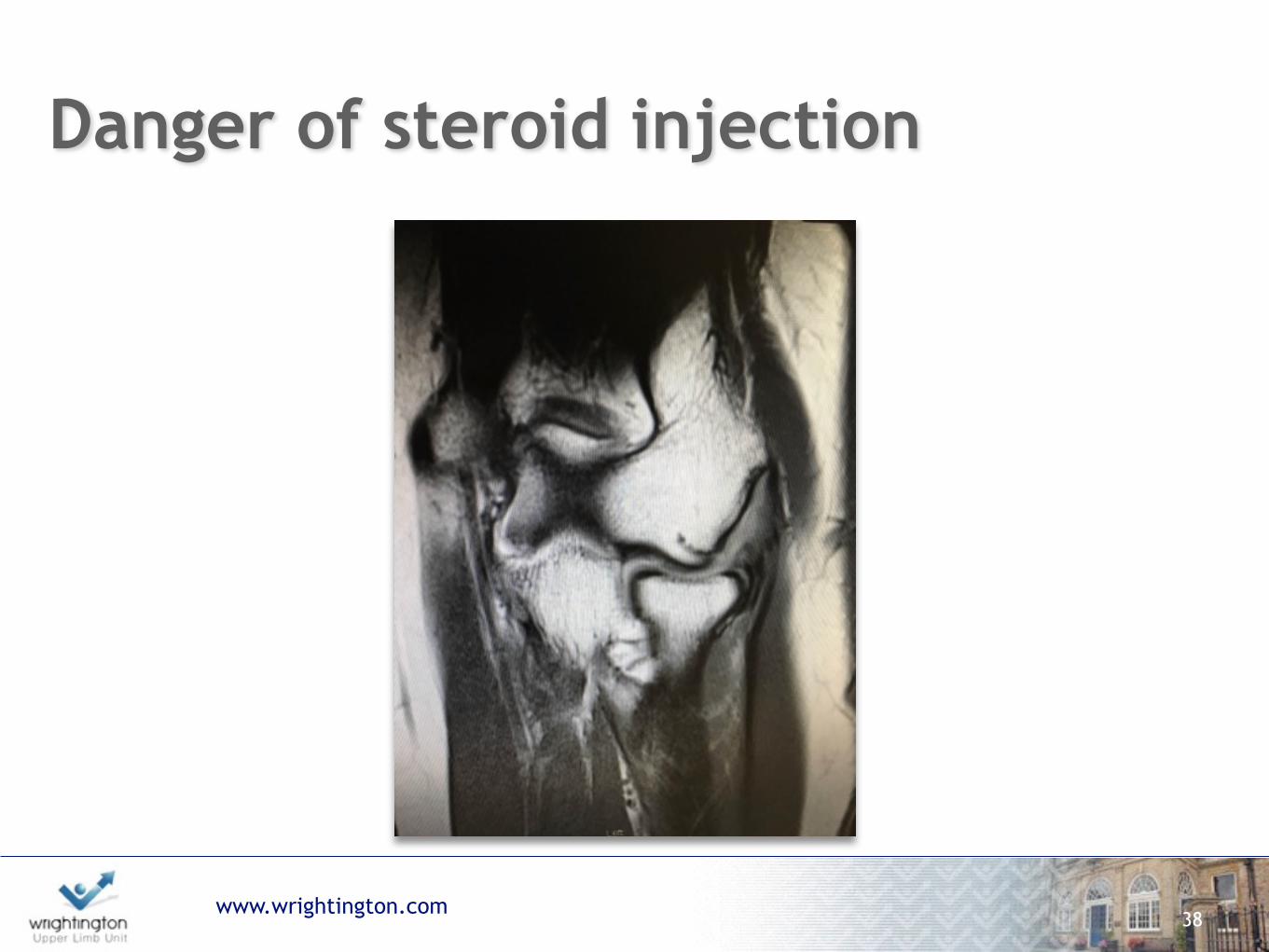
Danger of steroid injection

www.wrightington.com
Danger of steroid injection - lateral ligament rupture (PLRI)
39

www.wrightington.com
Dose dependent tenocyte death
40

Autologous blood source
Concentrated platelet solution (2 to 8x normal)
PDGF, TGF, VEGF, FGF
www.wrightington.com41
Platelet Rich Plasma

Mini GPS III Biomet
www.wrightington.com
Many systems - many differences
42
RegenLab
Selphyl
Arthrex ACP

www.wrightington.com
How does PRP work?
Stimulates an inflammatory process
Inflammation leads to healing
Is it organised healing?
43

www.wrightington.com44
Platelet Rich Plasma - does it work?
100 Consecutive Patients
All had symptoms for > 6/12
No treatment for tennis elbow for 6/12
Randomised to PRP or 40mg Kenacort Injection

www.wrightington.com45
Platelet Rich Plasma - does it work?
Steroid
PRP
Pain Score
PRP 73% Success
Steroid 51% Success
Follow Up (Weeks)

www.wrightington.com46
Pain
Sco
res
Platelet Rich Plasma - better than steroid

www.wrightington.com47
Pain
Sco
res
Platelet Rich Plasma - may not be better than saline and needling

www.wrightington.com
PRP v Dry Needling
PRP superior to dry needling
At 6 months 84% success with PRP 68% with needling (p=0.012)
48
Am J Sports Med. 2013 Jul 3. [Epub ahead of print] Platelet-Rich Plasma Significantly Improves Clinical Outcomes in Patients With Chronic Tennis Elbow: A Double-Blind, Prospective, Multicenter, Controlled Trial of 230 Patients. Mishra AK, Skrepnik NV, Edwards SG, Jones GL, Sampson S, Vermillion DA, Ramsey ML, Karli DC, Rettig AC.

www.wrightington.com
Autologous Whole Blood v PRP
Several RCTs
No convincing evidence of difference
49

www.wrightington.com
Efficacy v Effectiveness often efficacy seen in RCT is not reproduced in clinical practice so it is important to study ‘real life’ effectiveness
50
Single shot ultrasound guided PRP (1ml, Biomet Recover Miniplatelet) under LA
Personal series 59 patients with recalcitrant tennis elbow with minimum 6 month follow up
Mean age 52 (range 19 to 79 years)
Further intervention 3 repeat injections 9 operative intervention
“Success” rate of PRP injection 85%

www.wrightington.com
PRP and Distal Biceps
Case series
Improvement in pain scores and function
51

www.wrightington.com
How does PRP compare to surgery?
Prospective single blind RCT single shot PRP v open surgery
100 patient recruited (17 withdrawn)
83 patients randomised (2 lost to follow up)
Analysis of 81 patients
52
Morgan B, Trail IA, Watts AC, Birch A, Nuttal D Wrightington Upper Limb Unit

www.wrightington.com
Baseline data
53

www.wrightington.com54
Pre 1.5 3 6 12Time
Qui
ckD
ASH
PRP
Surgery
www.wrightington.com
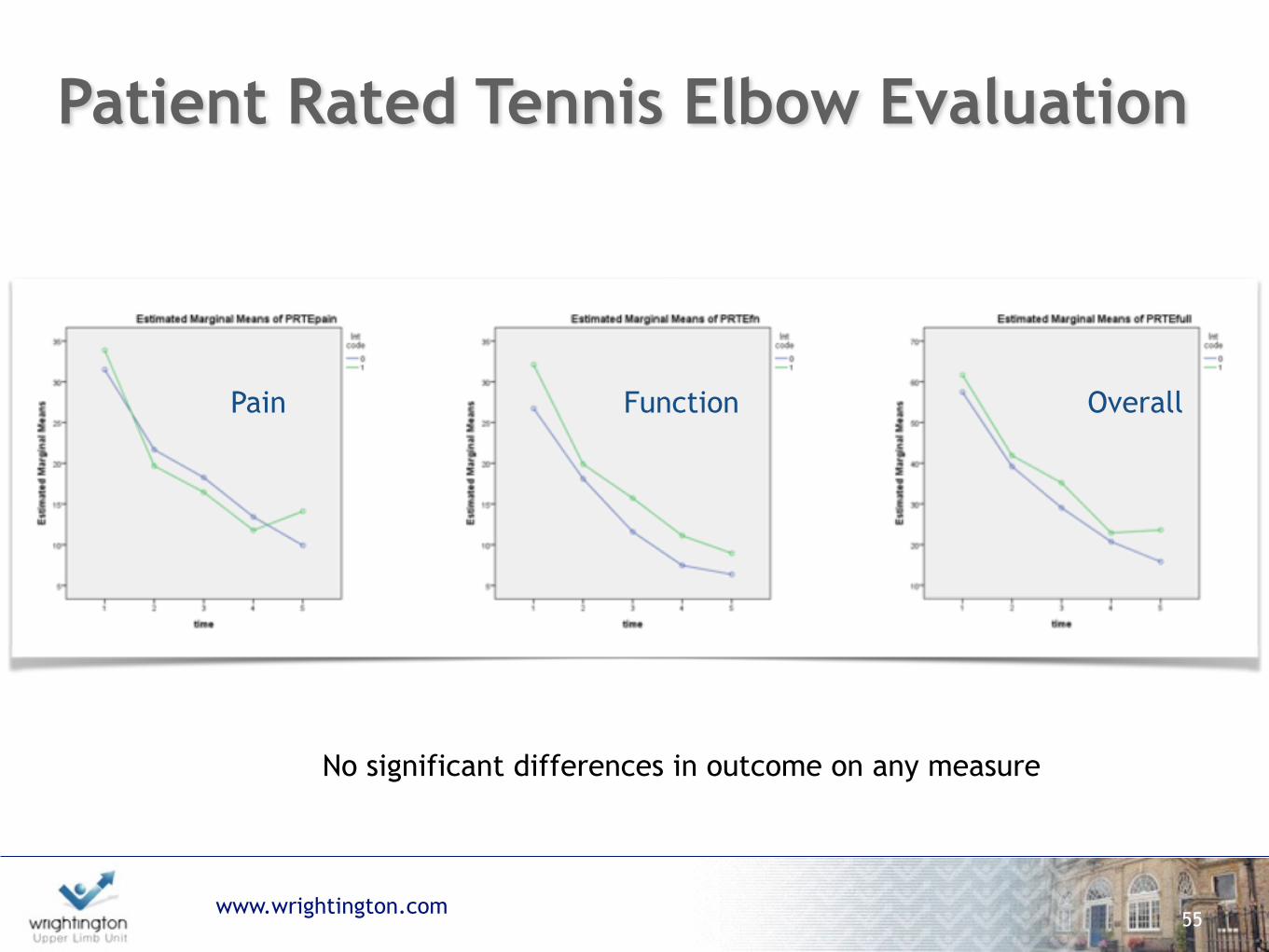
Patient Rated Tennis Elbow Evaluation
55
Pain Function Overall
No significant differences in outcome on any measure

www.wrightington.com
but…additional interventions
1 Surgical patient(3%) had a subsequent PRP injection
13 PRP patients (31%) had surgery within 12 months
“Success” rate 95% for surgery v 69% for PRP
56
p=0.001

www.wrightington.com
Conclusion
No evidence yet that PRP is better than placebo
In practice at least 70% of patients treated with
PRP will avoid surgery
Useful second line treatment if no response to
physio?
57

www.wrightington.com58

www.wrightington.com
Autologous cell implantation
Injection of functioning cells capable of regenerating extracellular matrix Autologous differentiated fibroblasts or tenocytes or skin derived tenocyte like fibroblasts Promising animal models Early clinical trials promising No good RCT
59

www.wrightington.com
Ultrasound driven percutaneous tenotomy
60

www.wrightington.com61

www.wrightington.com62

www.wrightington.com63
Advantages of Arthroscopic Tennis Elbow Release
Better access to ECRB
Smaller Incisions = less post-operative pain
Treatment of associated intra-articular pathology
Earlier return to sports and work

www.wrightington.com
Superior DASH scores in arthroscopic group at average 4 years follow-up
Excellent outcome Open group 67% Arthroscopic group 78%
64

www.wrightington.com65
Wrong Diagnosis
Radiocapitellar plica
Posterolateral rotatory instability
Radial tunnel syndrome
Radiculopathy

www.wrightington.com66
Remove trigger
NSAIDS?
Isometric exercises
Eccentric exercises
Injection
Surgery

www.wrightington.com
Where are we now?
67
Imaging
Insidious onset No history trauma
Adult
History trauma
Adolescent
Elderly
Tendinopathy +/- delamination
Analgesia
Activity modification
Physiotherapy - eccentric loading
Tendinopathy + macrotear/avulsion
SurgeryPRP injection and physio
Initial Presentation

www.wrightington.com
Future research
Double blind randomised controlled trial PRP v HA v sham injection 150 patients
Recruiting soon!
68