elevated plasma marinobufagenin, an endogenous cardiotonic...
TRANSCRIPT

Elevated Plasma Marinobufagenin, An Endogenous Cardiotonic Steroid, Is
Associated with Right Ventricular Dysfunction and Nitrative Stress in Heart Failure
Kennedy et al: Marinobufagenin in Heart Failure
David J. Kennedy, PhD1,3; Kevin Shrestha, MD1; Brendan Sheehey, BS1; Xinmin S. Li, PhD1;
Anuradha Guggilam, DVM, PhD1; Yuping Wu, PhD1; Michael Finucan, BS1; Alaa Gabi, MD1;
Charles M. Medert, BS1; Kristen Westfall, MBA1; Allen Borowski, RDCS1;
Olga Fedorova, PhD5; Alexei Y. Bagrov, MD, PhD5; W.H. Wilson Tang, MD1, 2, 4
1Department of Cellular and Molecular Medicine, 2Center for Cardiovascular Diagnostics and
Prevention, Lerner Research Institute 3Department of Nephrology and Hypertension, Glickman
Urological and Kidney Institute 4Department of Cardiovascular Medicine, Heart and Vascular
Institute, Cleveland Clinic, Cleveland, OH; 5Laboratory of Cardiovascular Science, National
Institute on Aging, National Institutes of Health, Baltimore, MD
Correspondence to W.H. Wilson Tang, MD 9500 Euclid Ave, Desk J3-4 Cleveland, OH 44195 Phone: 216.444.2121 Fax: 216.445.6165 E-mail: [email protected] DOI: 10.1161/CIRCHEARTFAILURE.114.001976 Journal Subject Codes: [110] Congestive heart failure, [115] Remodeling, [33] Other diagnostic testing, [100] Health policy and outcome research, [130] Animal models of human disease, [91] Oxidant stress
Prevention, Lerner Research Institute 3Department of Nephrology and Hyperteennnsioioion,n,n, GGGlililickckckmamaman
Urollogogogicicicalalal aaandnn KKKidii ney Institute 4Department oooff f CaCC rdiovascular Mediiicicicinenn , Heart and Vascula
nnnstttiti ute, Cleveveelalalannnd CCClililinininic,c,c, CCClelelevevevelalalandndnd, OHOHH; 5Laabobboraatototorryry ooof ff CaCaCardddioioiovavavasccculu ararar SSScicicienenencecece, NaNaNatititiononona
nnnstss itititutu e on AAAgigg ngngng, Naaatiooonal IIInsnsnstit tutttesese ooof ff Heaaalttth, BBBalltimmmooore,,, MMMD
CoCoCorrrrrresesespopopondndndenenencecece tttooo W H Wil T MD
by guest on May 19, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
by guest on M
ay 19, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
by guest on May 19, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
by guest on M
ay 19, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
by guest on May 19, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
by guest on M
ay 19, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
by guest on May 19, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
by guest on M
ay 19, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
by guest on May 19, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
by guest on M
ay 19, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

Abstract
Background—Plasma levels of cardiotonic steroids (CTS) are elevated in volume-expanded
states such as chronic kidney disease, but the role of these natriuretic hormones in subjects with
heart failure (HF) is unclear. We sought to determine the prognostic role of the CTS
marinobufagenin (MBG) in HF, particularly in relation to long-term outcomes.
Methods and Results—We first measured plasma MBG levels and performed comprehensive
clinical, laboratory, and echocardiographic assessment in 245 HF patients. All-cause mortality,
cardiac transplantation, and HF hospitalization were tracked for 5 years. In our study cohort,
median [interquartile range] MBG was 583 [383-812] pM. Higher MBG was associated with
higher myeloperoxidase (MPO, r=0.42, p<0.0001), BNP (r=0.25, p=0.001), and asymmetric
dimethylarginine (ADMA, r=0.32, p<0.001). Elevated levels of MBG were associated with
measures of worse right ventricular function (RV s’: r= -0.39, p<0.0001) and predicted increased
risk of adverse clinical outcomes (MBG 574 pM: HR 1.58 [1.10-2.31], p=0.014) even after
adjustment for age, gender, diabetes mellitus, and ischemic etiology. In mice, a left anterior
descending coronary artery ligation model of heart failure lead to increases in MBG, while
infusion of MBG into mice for 4 weeks lead to significant increases in MPO, ADMA, and
cardiac fibrosis.
Conclusions—In the setting of heart failure, elevated plasma levels of MBG are associated with
right ventricular dysfunction and predict worse long-term clinical outcomes in multivariable
models adjusting for established clinical and biochemical risk factors. Infusion of MBG appears
to directly contribute to increased nitrative stress and cardiac fibrosis.
Key Words: heart failure, cardiotonic steroids, outcome, nitrative stress, cardiac fibrosis
higher myeloperoxidase (MPO, r=0.42, p<0.0001), BNP (r=0.25, p=0.001), andndnd aaasysysymmmmmmetric
dimethhylyly arargigig nin neee (ADMA, r=0.32, p<0.001). Elevevated levels of MBGBGBG were associated with
mmmeaaasures of wowoworsrsrsee e riighghght t t veveventnn riiicucuculalalarrr fufuuncncnctit ononon (((RRRV s’: r== --0.0.0.393939, p<p<p<0...000000010101))) ana d prprpredededicicicteted d d ininincrcrcreaeaeaseses dRR
iiisksksk of adverse cllliniccalal outtcococomemm s (M(M(MBGBGBG 575774 pMppM: HRHRHR 111.5558 [[1.10-2.3111], p=0== .011414))) eeeveeen aaafttte
adjustment for age, gender, diabbbetetetesee mellitutuus, aaandnn iiiscscscheh mic etiology. In mice, a left anterio
dedescscenendidingngg ccororononarary y y ararteteryryy lligiggatatioion n momodedel l ofof hheaeartrt ffaiailulurere lleaead d toto iincncrereasaseses iin n MBMBG,G,, wwhihilele
by guest on May 19, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

Cardiotonic steroids (CTS) are a class of endogenous volume-sensitive hormones that bind to the
Na/K-ATPase, and include cardenolides (such as digoxin and ouabain) as well as aglycone
bufadienolides (such as telocinobufagin and marinobufagenin [MBG])1, 2. Increased circulating
levels of CTS have been proposed as a compensatory mechanism for natriuresis and vascular
tone in volume-expanded conditions including salt-sensitive hypertension, chronic kidney
disease, and preeclampsia3-5. In these settings, CTS contribute to enhanced natriuresis by
inducing endocytosis of proximal tubule cell Na/K-ATPase. This serves to remove the Na/K-
ATPase from the basolateral membrane and thus reduces the transport of sodium from the
tubular lumen to the blood compartment, thereby increasing sodium excretion6, 7. However, CTS
may exert “off-target” signal transduction effects beyond their direct effects on the sodium
pump2, 8. Hence, chronic stimulation of Na/K-ATPase signaling by CTS has important
implications for not only for the natriuretic response to increased salt load9 but also has been
implicated in pathological adaptation to volume expansion including hypertension, hypertrophy,
and fibrosis10, 11. Accumulation of MBG and other CTS has been documented in a variety of
cardiovascular disease states beyond conditions marked by plasma volume expansion and fluid
retention4, 12-15. Furthermore, myocardial hypertrophy and growth effects of CTS have been
proposed in the setting of hypertension and renal dysfunction16, and supported by both
experimental and clinical data demonstrating the association between an endogenous “digoxin-
like substance" and the development and severity of heart failure (HF)17, 18. Clinical and
experimental evidence from our group and others has also demonstrated the pro-oxidant and pro-
fibrotic effects of these steroid hormones in both cardiac and renal tissue19-23. As the relationship
among MBG and myocardial structure and performance in the contemporary HF population has
not been examined, we hypothesized that an increase in circulating MBG levels may track with
may exert “off-target” signal transduction effects beyond their direct effectsss ononon tthehehe sssododo iui m
pumpp2, 8.. HeHencce,e,e chronic stimulation of Na/KK-ATPase signaling bybyby CTS has importan
mmmplplplications fororor nnnott ooonlnln y y y fofof r thththe e e nanan trtrtriuiuiurerr tititic c c rerr sponoonse tttoo o ininincrcc eaaasssed d d sasasaltltlt llloao dd9 bbbututut aaalssooo hahahasss bebebeene
mmmplpllicated in papaathththologggicccal aadddapapaptationonon ttto voluuummme eeexppannnsisisioon innncluuudiiing hyyyppepertrttennnsion,,, hhyhyppperrrtrophphphy
and fibrosis10, 11. Accumulationnn ooof f f MBG ananand ototothehh r r r CTCTC S has been documented in a variety od
cacardrdioiovavascsculularar ddisiseaeasese sstatatetes s bebeyoyoy ndnd cconondidititionons s mamarkrkeded bby y y plplp asasmama vvololumume e exexpapap nsnsioion n anand d flfluiuidd
by guest on May 19, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

disease severity and provide important prognostic information in the setting of HF. Further, as
MBG in increased in volume overloaded states and associated with diastolic dysfunction in
animal models, we hypothesized that circulating levels would be increased in HF patients with
preserved ejection fraction and associate with echocardiographic indices of diastolic dysfunction.
Herein, we examined the relationship among circulating levels of MBG with echocardiographic
parameters, as well as long-term adverse clinical outcomes in patients with HF. We also used an
animal infusion model to demonstrate the contribution of MBG to the clinical phenotype
observed in our human study.
Methods
Study Design and Population. We prospectively enrolled 245 HF patients ( 18 years) seen at the
Cleveland Clinic with a clinical diagnosis of HF and New York Heart Association (NYHA)
functional class I-IV symptoms, who were free of significant renal, hepatic, and valvular
diseases. Study participants were excluded if they experienced any of the following: (1) major
cardiovascular event (myocardial infarction, unstable angina, stroke, transient ischemic attack,
pulmonary embolism) within the preceding 30 days; (2) significant lung diseases, including
chronic obstructive pulmonary disease, pulmonary fibrosis, pulmonary arterial hypertension, and
asthma; or (3) major surgery or use of inotropic agents within the past month. We prospectively
followed a composite endpoint including adverse clinical events (all-cause mortality, cardiac
transplantation and HF hospitalization) and all-cause mortality through a process confirmed by
chart review and the Social Security Death Index. Thirteen sex-matched apparently healthy
volunteer participants without a history of heart failure served as non-heart failure controls.
They were prospectively recruited outside of any healthcare institution setting, and did not report
Methods
Study y DeDesis gngng andndd PPopulation. We prospectivelyy eenrnrolled 245 HF patientntntss ( 18 years) seen at the
CCClevvveland ClClClinnnicicic wititthhh a a a clclclini icicicalalal dddiaiaiagngngnosoo isisis ooof f HFFF anddd NNNewewew YoYoYorkrkk HHHeaeaeartrtr AAssssssococociaiaiatitit ononn (((NYNYNYHAHAH
fufuunccctit onal claass III-IVV sssymppptooomsm , whww ooo werrre freeee offf sssiigignnniffficaanntnt renaaal, heheheppapatic, aaandndnd vvvalvvvullla
diseases. Study participants wereree eeexcxx luded ififif thhheyeyey expxpxperee ienced any of the following: (1) majo
cacardrdioiovavascsculularar eeveventnt (((mymyyococarardidialal ininfafarcrctitionon,,, ununststabablele aangngginina,a,, sstrtrookeke, , , trtranansisienent t isischchememicic aattttacackk
by guest on May 19, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

any active medical conditions at the time of blood draw. The study protocol was approved by the
Cleveland Clinic Institutional Review Board and written informed consent was obtained from
each of the study participants prior to their participation in the study.
Biochemical Assays. Blood samples were collected in ethylenediaminetetraacetic acid (EDTA)-
plasma vacutainers at the time of clinical and echocardiographic and hemodynamic evaluation,
were immediately aliquotted and stored at 80°C until analysis. Plasma samples were extracted
for MBG measurements using C18 SepPak cartridges (Waters Inc., Cambridge, MA) and MBG
levels were measured using a competitive fluoroimmunoassay [dissociation enhanced
fluoroimmunoassay (DELFIA)] as previously described22, 24. The MBG DELFIA uses a murine
monoclonal antibody (anti-MBG 4G4) and employs competition between immobilized antigen
(MBG-glycoside-thyroglobulin) and MBG, other cross-reactants, or endogenous cardiotonic
steroids within the sample for a limited number of binding sites on the 4G4 anti-MBG
monoclonal antibodies. Secondary (goat anti-mouse) europium labeled antibody was obtained
from Perkin-Elmer (Waltham, MA). Data on cross reactivity of the MBG antibody have been
reported previously3, 23. For analysis of MBG tissue levels, adrenal glands were homogenized
(TissueLyserII, Quiagen, 5 mm stainless steel beads) and homogenate was extracted with 10 fold
excess of methyl tert-butyl ether before drying under nitrogen gas and resuspension in assay
buffer (50 mM Tris-hydrochloride, 154 mM sodium chloride, 7.7 mM sodium azide, pH 7.8).
Plasma myeloperoxidase (MPO) levels were determined by an enzyme-linked immunosorbent
assay (CardioMPO II test, Cleveland Heart Labs, Cleveland OH). Arginine metabolomic profiles
were quantified by liquid chromatography-electrospray ionization tandem mass spectrometry
(LC-ESI-MS/MS) as previously described25, 26. All other assays including BNP, basic metabolic
fluoroimmunoassay (DELFIA)] as previously described22, 24. The MBG DELFIAIAIA uuuseseess s aa a mumum rine
monoclclononala aantibibbodo y (anti-MBG 4G4) and empplooysyy competition betweweweene immobilized antigen
MMMBBBG-glycoosssidedede-t-t-thyyyrororoglglglobobobuluu ininn) ) ) ananand d MBMM G,G,G, ootheeer crosososs-s-s-rerereacaa taaannnts,s,s, oorrr eeendn ogogogenenenououous ss cacacardrdrdioioiotototoninn crrr
ttteree ooioids within thhhe sssammmpleee ffforo a llimmmiiited nnnumbebber ofofof biinindddinggg sites ooon n thhhe 4GGG44 4 aaanttti-MMMBBBG
monoclonal antibodies. Secondaaryryry ((gogg at antntti-ii mmmououousee))) eueue ropipp um labeled antibody was obtained
frfromom PPererkikin-n ElElmemer r (W(W( alalththamam, , , MAMA).).) DDatata a onon ccrorossss rreaeactctivivitity y y ofof tthehe MMBGBG aantntibibodody y y hahaveve bbeeeenn
by guest on May 19, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
profile and lipid profile were measured on the Architect platform (Abbott Laboratories, Abbott
Park IL). The 4-variable Modification of Diet in Renal Disease (MDRD) equation was used to
calculate estimated glomerular filtration rate (eGFR)27.
Transthoracic Echocardiography. Comprehensive 2-dimensional echocardiography was
performed in standard parasternal and apical views on all participants by an American Society of
Echocardiography registered research sonographer using a Vivid 7 echocardiography machines
(GE Healthcare, Waukesha WI) equipped with a phased-array transducer and following the
American Society of Echocardiography recommendations28, 29. Further detail on
echocardiographic analysis is described in the Supplemental Material.
Animal study. In order to assess MBG levels in a mouse model of post-myocardial infarction
heart failure, left anterior descending (LAD) artery ligation was performed in C57BL6J mice and
plasma MBG was assayed after 4 weeks. Briefly, mice were intubated and ventilated with 60%
oxygen at 120 breaths per minute with an inspiratory pressure of 16 to 18 cm H2O using a rodent
ventilator (Harvard Apparatus). After sternotomy was performed, the left atrium was retracted
for visualization of the proximal LAD using a surgical microscope (Leica M500) and the LAD
was ligated with 10-0 prolene suture. Blanching and dysfunction of the anterior wall verified
LAD ligation. To directly test for a potential contribution of MBG to promotion of cardiac
dysfunction and nitrative stress, osmotic minipumps (Alzet® model 1004) were placed
intraperitoneally in order to deliver MBG (0.1 ug/g/day) or vehicle to mice for 4 weeks similar to
what we have reported in the rat22. Quantitative real-time PCR was used to measure gene
expression with 18S rRNA used as the internal control (TaqMan®, Life Technologies). These
echocardiographic analysis is described in the Supplemental Material.
AAnAnimmmal studyyy. InInIn ordrdrdererer tttooo asa sesesessssss MMMBGBGBG levevevelelels innn aa mmououousesese mmmodddelel ooof ff popopoststs -mmyoyoyocacacardrdrdiaialll inininfafafarcrcrctititiono
hehehearrrt tt failure,, leffttt aaanterrriooor deesssceene dingngng (LALALAD)) aarrteryyy lligagaatititioon wwwas ppeperrformmmeddd ininn CCC57BLBLBL66J6J mmmice annnd
plasma MBG was assayed after 444 wwweeks. Brrrieiei flflly,y,y, micicice e e were intubated and ventilated with 60%
oxoxygygygenen aat t 121200 brbreaeaththss pepep r r miminunutete wwitith h anan iinnspsppiriratatorory y y prprp esessusurere ofof 116 6 toto 1188 cmcm HH222O O ususining g g a a rorodedenn
by guest on May 19, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

studies were approved by the Cleveland Clinic Institutional Animal Care and Use Committee
and the procedures followed were in accordance with institutional guidelines.
Quantitative Histologic Techniques. Mason’s trichome and picosirius red staining was
performed on deparafinized 5 μm serial heart sections. The sections were mounted under a Leica
DM 2500 microscope and digitized with a QImaging MicroPublisher 5.0 RTV camera. Further
detail on quantitative morphometric analysis is described in the Supplemental Material.
Statistical Analysis. Normally distributed continuous variables were summarized as mean ±
standard deviation if normally distributed, or median (interquartile range [IQR]) if non-normally
distributed. If more than two groups were compared, one-way analysis of variance (ANOVA)
was performed prior to comparison of individual groups with the unpaired Student’s t-test with
Bonferroni’s correction for multiple comparisons. If only two groups of normal data were
compared, the Student’s t-test was used without correction. P values for non-parametric
comparisons or those based on small sample size were performed using the Mann-Whitney test.
Associations between changes in MBG and clinical, biochemical, and echocardiographic
measures were performed using the Spearman's rank correlation method. Clinical risk and time
to clinical adverse events associated with increased MBG levels were assessed by Cox
proportional hazard analysis and the units for hazard ratios represent the dichotomized values of
MBG 574 pM and <574 pM. The optimal sensitivity and specificity cutoff of MBG ( 574 pM)
levels in our cohort was determined using receiver operator characteristic (ROC) curve analyses
in the context of the time to event and the Hazard Ratios reported represent the risk associated
with MBG levels 574 pM. This value was chosen as the optimal ROC cut-point that
tandard deviation if normally distributed, or median (interquartile range [IQR]))) if f f nooon-n-n-nononormrmrmally
distribubuteted.d IIf f momomorer than two groups were compparared, one-way analyssisisis of variance (ANOVA
wwwass s performemeed d prprprioii r r tototo cccomomompapapariririsssononon ooof f f ininindididivivividudd al groupupups s s wiwiwithtt ttthhhe unununpapapairirirede SSStututudededentntnt’ss ttt-t-t-tesesesttt wiwiw th
BBoBonfnfnferroni’s coorreeectiooonn n for r mmmultippplelel cooomppparrrisonnns. IfIfIf ooonlnlly twwoo groupspsps ooof non rmmmalall dddattta wewewere
compared, the Student’s t-test wwwasaa used wiwiw ttthohohout cccoroo rection. P values for non-parametric
cocompmppararisisonons s oror tthohosese bbasaseded oon n smsmalall l sasampmpplele ssizizee wewerere pppererfoformrmeded uusisingngg tthehe MManann-n WhWhititneney y y tetestst
by guest on May 19, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

maximized sensitivity plus specificity in ROC curve analysis of the nominal logistic regression
fit between MBG modeled as a continuous variable and adverse clinical outcomes modeled as a
nominal dichotomous variable. Survival curves (all-cause mortality, cardiac transplantation or
HF hospitalization) were generated from Kaplan-Meier survival analysis. Continuous net
reclassification improvement (NRI) was used as test of association and integrated discrimination
improvement (IDI) was to measure improvement in model performance. The p values compare
models with and without MBG. The model was adjusted for traditional risk factors, including
age, sex, diabetes mellitus and ischemic etiology. Statistical analysis was performed using
GraphPad Prism®, JMP 10.0 (SAS Institute, Cary, NC), and R 3.1.2 (Vienna, Austria). P values
<0.05 were considered statistically significant.
Results
Subject Characteristics. Baseline characteristics of our study cohort are presented in the Table.
Median MBG level was 583 [IQR 383-812] pM in patients with HF compared to 241 [IQR 212,
281] pM in non-HF controls (n=13, mean age 43 12 years, 64% male, body mass index 27 3,
15% African American). Patients with HF have higher MBG levels when compared to that of
non-HF controls, regardless of whether they have reduced or preserved LVEF (Figure 1).
Furthermore, higher MBG was associated with higher indices of inflammation/oxidative stress
(MPO: r=0.42, p<0.0001), myocardial stress (BNP: r=0.25, p=0.001), and nitrative stress
[asymmetric dimethylarginine (ADMA): r=0.32, p<0.001; symmetric dimethylarginine (SDMA):
r=0.34, p<0.001; and mono methyl arginine (MMA): r=0.40, p<0.0001]. In our study cohort,
there was no significant association between MBG and cystatin C (p=0.485) and estimated GFR
(p=0.345).
<0.05 were considered statistically significant.
ReRR suultss
SuSuSubjbjjece t Characttterrristicccs.. Baaaseseselill ne cchahh rrracccteriiistttics off oururur sstuuudyyy cohohohoort arrre prprrf esessenee teddd ininn tttheee Taaabllle
Median MBG level was 583 [IQR R R 38383 3-812]] pppM M M ininin ppatatatieieients with HF compared to 241 [IQR 212
2828281]1]1] pppMMM ininin nnnononon-HHHFFF cococontntntrororolslsls (((n=nn 131313,,, mememeananan aaagegege 444333 121212 yyyeaeaearsrsrs,,, 646464%%% mamamalelele,,, bobobodydydy mmmasasassss ininindededexxx 272727 333
by guest on May 19, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
MBG Levels and Myocardial Structure and Performance. Supplemental Table 1 presents the
relationships between MBG levels and echocardiographic parameters of cardiac structure and
performance. In univariate analysis, higher MBG was associated with indices of LV diastolic
function (Mitral deceleration time: r= -0.24, p=0.007) and RV diastolic function (Tricuspid E/e’:
r=0.22, p=0.027; Tricuspid deceleration time: r= -0.38, p=0.002), as well as larger RV size (RV
end-diastolic area: r=0.21, p=0.023). Elevated levels of MBG were associated with measures of
worse RV systolic function (RV s’: r= -0.39, p<0.0001), but not left-sided systolic function
(Supplemental Table 1).
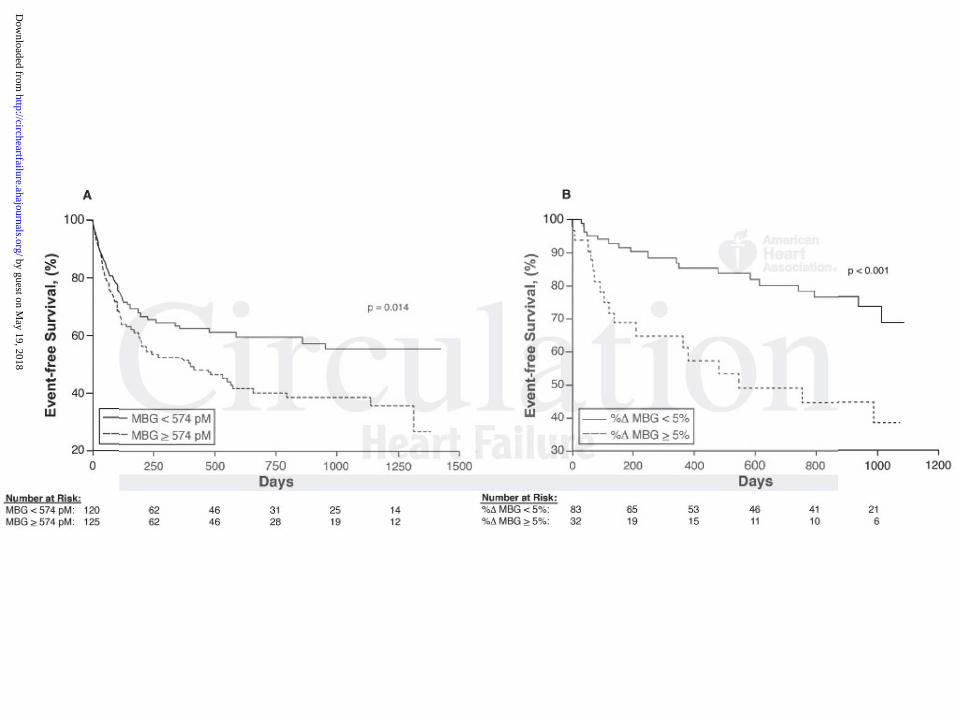
MBG Levels and Prognosis. In our study cohort, 118 patients experienced an adverse event of
death, cardiac transplantation, or HF hospitalization over the 5 year follow-up. When divided as
dichotomous variable according to optimal cut-point (574 pM), elevated MBG was a predictor of
increased risk of 5-year adverse outcomes, with higher MBG predicting increased risk of adverse
clinical events (Hazard ratio 1.58 [95% confidence interval 1.10-2.31], p=0.014, Figure 2A). The
predictive value of MBG remained statistically significant after adjustment for age, gender,
diabetes mellitus, and ischemic etiology, but not eGFR (Supplemental Table 2). Moreover, the
addition of MBG to traditional risk factors such as age, gender, ischemic etiology, and diabetes
resulted in an 33.6% event-specific net reclassification (95% confidence interval 9.3%-57.8%,
p=0.007) and a 3% integrated discrimination improvement (Supplemental Table 3). When
defined by quartiles, this trend was confirmed using Cochran-Amitage test for the trend over
quartiles (p=0.0297), although the trend was not monotonic (Supplemental Table 4). MBG did
not predict events when modeled as a continuous variable (Hazard ratio 1.14 [0.95 – 1.37],
MBG LeLevevels anddd PPrognosis. In our study cohort,,, 1118 patients experiennncec d an adverse event o
dededeattth,h cardiacacc tttrararansnn plplplananantatatatititionoo , , , ororor HHHF FF hohohospss itittalalalizizizationoon oveveer r r thththeee 5 yyeyeararar fffololllololoww-w upupp. WWWheheh n n dididivivividedededd d a
dididichchhoto omous varrriaaable accccordddingngng to opopoptiiimmmal cccuttt-po niint (5(55747474 pppMMM), eeeleeevateddd MMMBGBGBG was a pprreedddictooor o
ncreased risk of 5-year adverse oooutututcocc mes,, wwwititi h hhhigigigheeer r r MBMM G prpp edicting increased risk of adverse
clclininicicalal eeveventnts s (H(H( azazarard d raratitio o 1.1.5858 [[[9595%% coconfnfididenencece iintnterervaval l 1.1.1010-22.3.31]1]], , , p=pp 0.0.01014,4,, FFigiggurure e 2A2A).).) TThehe
by guest on May 19, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
p=0.15, per 1 standard deviation increment 0.62 with MBG modeled as a natural log transformed
continuous variable).
We next selected a subgroup of the HF patients that had serial blood draws available at the time
of their initial presentation in the hospital and 48-72 hours after admission (n=115 and included
35 events) and measured MBG. Rising MGB levels over the course of admission predicted
increased risk of adverse outcomes [% MBG modeled as a continuous variable per standard
deviation increments where 1 standard deviation = 0.91%, Hazard ratio 1.30 (95% confidence
interval 1.04-1.56), p=0.025, per 1 standard deviation increment, Figure 2B].
MBG Promotes Cardiac Fibrosis and Nitrative Stress in Animal Models. In order to assess
MBG levels in a mouse model of post-myocardial infarction heart failure, left anterior
descending artery ligation (LADx) was performed in C57BL6J mice. After 4 weeks of LADx we
observed a significant decrease in left ventricular ejection fraction and increases left ventricular
size (Figure 3A and B). We also observed changes in left ventricular homogenate of molecular
markers of cardiac calcium handling [sarcoplasmic reticulum calcium ATPase 2a (SERCA2a)
and sodium calcium exchanger (NCX-1)] and cardiac hypertrophy [beta myosin heavy chain
( MHC) and atrial natriuretic peptide (ANP)] consistent with a heart failure phenotype in this
model (Figure 3C-F). Further, we noted increases in MBG levels in the post-MI heart failure
mice (Figure 3G), with MBG levels observed within the range of values detected among HF
subjects studied (50th percentile 585 pM). We also performed the LAD ligation procedure on a
separate group of mice (n=5) and, after 1 week, isolated and extracted the adrenal glands and
MBG PrPromo ototes CCCardiac Fibrosis and Nitrative SSStrt ess in NN Animal Mododdele s. In order to asses
MBMBMBGGG levelsss iiinnn a a momomousususeee momomodededelll ofofof pppososst-t-t-mymm occcaardialalal iiinfnfnfarctctctiiion n n heheeararart t faaailililururure,e,e, lefefefttt anananteteterirrio
dededescccene ding arterrry ligaaatiooon (LALALADxD ) waww sss ppperfooormmmeddd inn CCC575757BLBLL666J mmmiccce. Afffteeer 444 wwweeksss ooof f LALALADxxx wwwe
observed a significant decrease ininn llleeeft ventricicicullararar ejejejectctctioioi n fraction and increases left ventricula
iizeze (((FiFigugug rere 33A A anand d B)B)).. WeWe aalslso o obobseservrveded cchahangnggeses iin n leleftft vvenentrtriicuculalar r hohomomogegeg nanatete oof f momolelecuculala
by guest on May 19, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

performed MBG measurement. Here we found that adrenal MBG levels were elevated vs control
mice, but this did not reach statistical significance (Mann-Whitney p value = 0.056, Figure 3H).
To directly test for a potential contribution of MBG to promotion of cardiac dysfunction and
nitrative stress, mice were infused intraperitoneally with MBG (0.1 ug/g/day) which results in
comparable levels to the post-MI heart failure mice (Figure 4A). MBG infusion did not result in
decreased ejection fraction, but was accompanied by a significant increase in left ventricular size
(Figure 3A and B). Importantly, mice infused with MBG demonstrated corresponding increases
in MPO (Figure 4B) as well as increases in several methylated arginine markers of nitrative
stress including ADMA, SDMA, and MMA (Figure 4 C-E). Furthermore, while MBG infused
mice experienced significant left ventricular cardiac fibrosis vs vehicle treated controls, right
ventricular cardiac fibrosis appeared to be increased vs vehicle treated controls but this did not
reach statistical significance (Mann-Whitney p value = 0.219, Figure 5).
Discussion
While elevated CTS have been associated with cardiac hypertrophy and dysfunction in subjects
with hypertension30, 31, hypertrophic cardiomyopathy32, decompensated HF33, 34, and
cardiomyopathy in chronic kidney disease15, 23, this is the first study to our knowledge that
examines the relationship between plasma MBG and cardiac parameters as well as adverse
clinical events in a broad and contemporary cohort of patients with HF. The relationships
between elevated MBG and indices of inflammation/oxidative stress, myocardial stress, and
nitrative stress and the predominantly diastolic dysfunction is consistent with the physiologic
effects of MBG on the myocardium in volume-expanded states. These findings support future
tress including ADMA, SDMA, and MMA (Figure 4 C-E). Furthermore, whiiilele MMMBGBGBG iiinfnfnfused
mice eexpxppere ieencn ededed significant left ventricular carddiai c fibrosis vs vehiclclclee treated controls, righ
veveventnttricular cacaardrddiaiaiac cc fifiibrbrbrosososisisis appppppeaeaearrrededed tttooo bebebe iiincncncreaseed vvsss vevevehihihicle e e trtreaeaeatetedd d cococ ntrororolslsls bbbututu tthihihisss didididdd nonnt
eeeacacch hh statistical sssigggniffiiicaaancee (MMMann-W-WWhhhitttneyyy ppp vallluee === 000 22.219,,, Figugugurre 5)..
DiDiscscusussisionon
by guest on May 19, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

investigations on the potential role of modulation of MBG levels or activity as a novel targeted
therapy in the population of HF patients burdened with significant cardiovascular disease and
death.
Contribution of CTS in Heart Failure. While previous human studies have demonstrated
the detection of elevated CTS in the setting of acute myocardial infarction13, 35, 36 and HF37, the
novel findings in the current study was the relationship between elevated MBG and worsened
right ventricular function (a condition often associated with venous congestion) as assessed by
standard echocardiographic indices as well as adverse clinical outcomes and nitrative stress.
Further, the data from the subgroup of patients who had serial MBG measurements suggests that
MBG levels are dynamic and supports the view that rising levels of MGB during admission
predict worse long-term clinical outcomes.
The relationship between cardiac structure, hemodynamics and CTS has also been
observed in several other cohort studies. Endogenous plasma ouabain levels are elevated in
patients with severely impaired left ventricular function (EF< 30%)34 and demonstrated
significant positive correlation with hemodynamics such as blood pressure as well as cardiac
indices such as left ventricular mass index, left ventricular end diastolic volume, as well as
eccentric remodeling in hypertensive patients30, 31. Both circulating and myocardial tissue CTS
immunoreactivity was positively correlated with left ventricular end-diastolic pressures and
inversely correlated with cardiac index in patients with hypertrophic cardiomyopathy32. The
shift from compensated left ventricular hypertrophy to CHF is not only marked by a three-fold
increase in endogenous plasma ouabain levels in decompensated CHF, but also an increase in the
sensitivity of cardiac Na/K-ATPase to ouabain33, 34. Levels of circulating endogenous ouabain
also predicted HF progression in idiopathic dilated cardiomyopathy patients38 and left ventricular
MBG levels are dynamic and supports the view that rising levels of MGB dududuririringngng aaadmdmdmisisissisis ono
predicicicttt wowoworsrsrseee loongngng-term clinical outcomes.m
The relalalatioononshshshippp bbbeetetweweweenenn cccarrrdididiac sstrrructuuurre, hhhemememodododynnamamamiicics ananand d CTCTCTSSS hahahas s aaalsososo bbbeeeeen
obbbseseservrvrved in n n sess vvverrral ooothhher cococohohohortrt ssstuttudddieees. EnEnEndogggennooususus ppplalalasssma oououababaiiin leeevevevelsll arerere ellevvvateddd in
patients with severely impairedd d leleleftftft vvvenenentrtrtricici ulululararar fffunununctctctioioion n n (E(( F< 30%)34 and demonstrated
iiigngnifififiicicananttt popo isisitititiveve ccororrerellalatititionon wititithhh hhehemomoddydynana imimicscs susu hchch aass blblblooooddd prpresessusurere aass wewellllll aass caca drdrdiiaiacc
by guest on May 19, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

hypertrophy in the setting of end-stage renal disease39. Increased plasma MBG levels parallel the
progression of HF37 and are associated with a “uremic cardiomyopathy” in chronic kidney
disease15, 22, 23. Experimentally, Dahl salt-sensitive rats fed a high-salt diet demonstrated
compensated left ventricular hypertrophy progressing to dilated cardiomyopathy in parallel with
increasing plasma MBG level as well as increased expression and sensitivity of the Na/K-
ATPase -1 to MBG33. Interestingly, in our study, MBG was not significantly associated with
cystatin C or estimated GFR, suggesting factors beyond renal insufficiency that influence MBG
production. As we have previously demonstrated that MBG is synthetized by adrenocortical cells
and that Angiotensin II can be its secretagogue 40, 41 we isolated and extracted the adrenal glands
and performed MBG measurement in a group of mice one week after LADx and noted it was
significantly elevated. This supports the adrenal tissue as a significant contributor to the pool of
circulating MBG in a post-MI heart failure model. Taken together with our findings, these
observations suggest that the elevated CTS levels which accompany edematous states like HF
may promote downstream adverse cardiovascular consequences.
Mechanisms Linking CTS to Cardiovascular Pathology in Heart Failure. In addition to
their well known effects on the ion transporting functions of the Na/K-ATPase, CTS also bind to
and initiated signaling through a non-pumping pool of the Na/K-ATPase which reside in
caveolae6. CTS confer a conformational change to the Na/K-ATPase that releases the Src kinase
domain, thus activating Src kinase and multiple downstream targets2, 8, 11. This novel Na/K-
ATPase-mediated signaling is responsible for a variety of key cellular roles involving cell
growth/hypertrophy, reactive oxygen species production, and collagen synthesis6.
In the present study we demonstrate for the first time that increased circulating levels of
MBG in human heart failure associate with elevations in markers of inflammation and nitrative
and performed MBG measurement in a group of mice one week after LADx aaanddd nnnotototededed iiittt wa
ignifificicicananantltlt y yy elee evevvataa ed. This supports the adrenal ttisisissuerr as a significant ccconoo tributor to the pool o
cicicircccuulating MBMBMBGG G innn aaa pppososost-t MIMIMI hhheeeararart tt fafafaillururure mooodeel. TTTakakakenenen togogogetetethhhererr wwwiti h ououourrr fififindndn ininingsgsgs, , , thththesee e
obobbseeervr ations sssuggggggest ttthhaat thhhe e elee evatatatededd CCCTSS leeevellls whwhhicicichh aacaccompmpmpany eededememmatttouo s ssstaatatess llikee HHHF
may promote downstream adverssee cccarara did ovovasascucuculaaar r r cococ nsnsnseqeqequeuencceses. .
MeMeMechchchanananisisismsmsms LLLinininkikikingngng CCCTSTSTS tttooo CaCaCardrdrdioioiovavavascscsculululararar PPPatatathohohololologygygy iiinnn HeHeHearararttt FaFaFailililururureee. IIInnn adadaddididitititiononon tttooo
by guest on May 19, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

stress including MPO and the methylated arginine metabolites ADMA, SDMA, and MMA.
Using an animal model of post-MI heart failure, we also demonstrate a significant increase in
plasma MBG 4 weeks after ligation of the left anterior descending artery in mice. Further,
infusion of mice with MBG, which results in similar circulating levels as those seen in both
human and experimental heart failure, recapitulated the increases in MPO as well as ADMA,
SDMA, and MMA seen in our human heart failure study.
The mechanism whereby MBG may increase methylated arginine metabolites is unclear.
We and others have shown that cardiotonic steroids such as MBG and ouabain increase ROS and
inflammatory cytokines in cardiac42 and renal43 cell types, and also decrease NO bioavailability
without changes in eNOS expression44. Inflammation and increased oxidant stress can
significantly impact methyltransferases necessary for arginine methylation, the proteases
involved in release of free methylargnine metabolites, and the catabolic dimethylarginine
dimethylaminohydrolases responsible for metabolism of ADMA45. Thus, it is possible that some
of the observed associations between methylated arginine metabolites and MBG may occur in
part via ROS mediated perturbations in these enzymatic pathways.
The association of CTS with markers of inflammation and nitrative stress is not however
without precedent. We have previously reported in the rat that treatment of both cardiac
myocytes and isolated perfused hearts with the CTS ouabain yielded increased nitrative
modification and decreased activity of cardiac calcium handling proteins as well as diastolic
dysfunction46. We have also shown that ouabain induces increases in inflammatory cytokine
expression from both macrophage and renal proximal tubular cell types43. Our findings are also
in parallel with animal models such as partial (5/6th) nephrectomy showing elevations in
circulating MBG levels that stimulate systemic oxidant stress, oxidative modification and
without changes in eNOS expression44. Inflammation and increased oxiidadadantnn ssstrtrtresesesss s cacan
ignififficicicananantltltly y y immmpapapact methyltransferases necessasasaryryry for arginine metetethyhh lation, the protease
nnnvooolved in reeeleleleaaase e ofofof fffreeee mememethththylylylarara gggnininne ee metttabbboliliitetetesss, aaanddd thehehe cccatatatababa olicicic dddimimimetete hyhyhylalalargrgrgininininini ea
didiimememethylaminnnohohhydydydrolaaaseees reeespopoponsibibblel fooor mmmetttabolissm m m ofofof ADMDMD AAA4555. Thuuus,, it iiis popp ssibibibllle ttthhhat sooommme
of the observed associations betweweweenenen mememethththylylylatata ededed aaargrgrginininininineee mememetatat bolites and MBG may occur in
papapartrtrt vvviaiaia RRROSOSOS mmmededediaiaiateteteddd pepepertrtrturururbababatititionononsss ininin ttthehehesesese eeenznznzymymymatataticicic pppatatathwhwhwayayaysss.
by guest on May 19, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

fibrosis of cardiac tissue and cardiac dysfunction in the rat19, 22, 47. This cardiac phenotype can
also be recapitulated by infusion of MBG. In contrast, both active and passive immunization
against MBG as well as lowering circulating MBG levels via adrenalectomy significantly reduce
the oxidant stress and cardiac dysfunction independent of changes in blood pressure.
In our study, mice infused with MBG also demonstrated significant increases in cardiac
fibrosis. MBG and ouabain have both been shown to increase [3H]proline incorporation in
addition to collagen expression (both mRNA and protein) in cardiac and renal fibroblast cell
types20 and these effects were blocked by pharmacological antagonism of the TGF beta
pathway19. We have also noted that decreases in Fli-1 (a negative regulator of collagen synthesis)
expression appear to be necessary for MBG to induce increases in collagen in several types of
fibroblasts (cardiac, renal, and dermal). Additionally, MBG induces translocation of PKCdelta
from the cytosol to the nucleus in a PLC dependent manner, and this translocation of PKCdelta
causes the phosphorylation and subsequent degradation of Fli-120. In several fibroblast cell types,
CTS also stimulate Na/K-ATPase and oxidant signaling which induce collagen production19, 22,
43,. These signaling pathways are not only significantly attenuated by oxidant scavenging and
inhibition of Src kinase, but also through competitive inhibitory mechanisms induced by
spironolactone and canrenone binding to the Na/K-ATPase19, 22, 48, 49. Thus, the pro-inflammatory
and pro-fibrotic CTS-Na/K-ATPase signaling axis may provide a novel therapeutic target in
settings such as HF where elevated CTS induce inflammation and cardiac fibrosis.
Study limitations. Despite being the largest study to our knowledge of reporting the
relationship between clinical outcomes and MBG in HF, the current study is still limited in the
relatively small number of patients as well as the selection bias that potentially confounds
interpretation of such cohort studies. We did not have sufficient data to analyze central venous
expression appear to be necessary for MBG to induce increases in collagen in sseveve eeeralalal tttypypypesese o
fibrobbblalalastststss s (c(c(cardididiacaa , renal, and dermal). Additionananallll y, MBG induces trararannnslocation of PKCdelta
frfrfrommm the cytosololol ttto thththee e nununuclcc euuus s s ininin aaa PPPLCLCLC dddepepe eeendeeennnt mmmananannenener,r,r, andndnd ttthihihis trtrtranannslocococatatatioioion n n offf PPPKCKCKCdededeltl a
caaausususesee the phohohosppphhooryllaattion aaandndnd subssseqeqe ueueuent dddegeggraddadatttionnn ooof FFFliii-12000. IIIn sevvverralll fibibibrobbllalasstst cccellll tyyypeees
CTS also stimulate Na/K-ATPasesee aaandndnd oooxixixidadadantnn sssigigignanan lililingngng wwwhihihichchch induce collagen production19, 22
3,. ThThTheseseseee sisisigngngnalalalinininggg papapathththwawawaysysys aaarerere nnnototot ooonlnlnlyyy sisisigngngnififificicicananantltltlyyy atatattetetenununuatatatededed bbbyyy oxoxoxiiiffffff dadadantntnt ssscacacavevevengngnginininggg anananddd
by guest on May 19, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

pressure or other indices of right ventricular function, thus the measurements indicating
worsened RV function are based solely on echocardiographic indices. Our Cox proportional
hazard analyses with multiple covariables was limited by lack of power due to missing data.
Similarly, when defined by quartiles, while the trend between MBG and worse clinical outcomes
was similar to that obtained by the optimal cutpoint analysis, it was not statistically significant.
Nevertheless, our study examines for the first time the contribution of MBG to incident
cardiovascular outcomes in a cohort of patients with HF and demonstrates a novel association
between CTS and markers of inflammation and nitrative stress. We would emphasize that the
purpose of this study was to demonstrate underlying physiology rather than to propose MBG as a
biomarker as it tracks with worsening renal function. The increased inflammation, nitrative stress
and cardiac fibrosis seen with elevations in MBG may be an important mechanism of
cardiovascular dysfunction in patients with heart failure and requires further investigation.
Conclusion
Elevated levels of MBG are associated with indices of worse cardiac dysfunction as well as
increased risk for development of adverse clinical outcomes in patients with HF even after
multivariable models adjustment for established clinical risk factors. Similarly, changes in MBG
levels over time appear to be of prognostic benefit in HF patients, and infusion of MBG in an
animal model appears to directly contribute to increased nitrative stress, cardiac fibrosis and
dysfunction. Thus, MBG may serve as an important therapeutic target in patients with heart
failure.
biomarker as it tracks with worsening renal function. The increased inflammationnn, nninitrtrtratatativiviveee stss res
and cardiac fibrbrrosis seen with elevations in MMBG may be an impmm ortant mechanism o
caaardddiovascularaa dddysysysfuuncncnctitit ononon in papapatititienenentsss wwwitii h hh hhheaeaart fffaiilureee aaandndnd rrreqqquiuiuireeesss fuuurtrtrthehh r innnvevevestststigigigattioioion.nn
Conclusion
ElElevevatateded llevevelels s ofof MMBGBG aarere aassssocociaiateted d wiwithth inindidiceces s ofof wwororsese ccarardidiacac ddysysy fufuncnctitionon aas s wewellll aass
by guest on May 19, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

Sources of Funding
This research was supported by grants from the National Institutes of Health (NIH,
R01HL103931) and the NIH/Office of Dietary Supplements (P20HL113452), and the Cleveland
Clinic Clinical Research Unit of the Case Western Reserve University CTSA (UL1TR 000439).
Dr. Kennedy was supported by an American Heart Association Scientist Development Grant
14SDG18650010. Drs. Fedorova and Bagrov are supported by Intramural Research Program,
National Institute on Aging, National Institutes of Health. Mass spectrometry studies were
performed on instruments housed in a facility supported in part by a Center of Innovations
Award by AB SCIEX.
Disclosures
None.
References
1. Bagrov AY and Shapiro JI. Endogenous digitalis: pathophysiologic roles and therapeutic applications. Nat Clin Pract Nephrol. 2008;4:378-92.
2. Bagrov AY, Shapiro JI and Fedorova OV. Endogenous cardiotonic steroids: physiology, pharmacology, and novel therapeutic targets. Pharmacol Rev. 2009;61:9-38.
3. Fedorova OV, Simbirtsev AS, Kolodkin NI, Kotov AY, Agalakova NI, Kashkin VA, Tapilskaya NI, Bzhelyansky A, Reznik VA, Frolova EV, Nikitina ER, Budny GV, Longo DL, Lakatta EG and Bagrov AY. Monoclonal antibody to an endogenous bufadienolide, marinobufagenin, reverses preeclampsia-induced Na/K-ATPase inhibition and lowers blood pressure in NaCl-sensitive hypertension. J Hypertens. 2008;26:2414-25.
4. Komiyama Y, Dong XH, Nishimura N, Masaki H, Yoshika M, Masuda M and Takahashi H. A novel endogenous digitalis, telocinobufagin, exhibits elevated plasma levels in patients with terminal renal failure. Clinical Biochemistry. 2005;38:36-45.
5. Lopatin DA, Ailamazian EK, Dmitrieva RI, Shpen VM, Fedorova OV, Doris PA and Bagrov AY. Circulating bufodienolide and cardenolide sodium pump inhibitors in preeclampsia. JHypertens. 1999;17:1179-87.
6. Liu J and Xie ZJ. The sodium pump and cardiotonic steroids-induced signal transduction protein kinases and calcium-signaling microdomain in regulation of transporter trafficking. Biochim Biophys Acta. 2010;1802:1237-45.
Disclosuurer s
NNNonnne.
Reeefeferererencnn eseses
1.1. BBagaggrorov v AYAY aandnd SShahapipip roro JJI.I. EEndndogoggenenououss didigigig tatalilis:s: pppatathohophphp ysysy ioiolologigig cc roroleless anand d ththererapappeueutitic c applications Nat Clin Pract Nephrol 2008;4:378-92
by guest on May 19, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

7. Liu J, Kennedy DJ, Yan Y and Shapiro JI. Reactive Oxygen Species Modulation of Na/K-ATPase Regulates Fibrosis and Renal Proximal Tubular Sodium Handling. International Journal of Nephrology. 2012;2012:1-14.
8. Xie JX, Shapiro AP and Shapiro JI. The Trade-Off between Dietary Salt and Cardiovascular Disease; A Role for Na/K-ATPase Signaling? Front Endocrinol (Lausanne). 2014;5:97.
9. Loreaux EL, Kaul B, Lorenz JN and Lingrel JB. Ouabain-Sensitive alpha1 Na,K-ATPase enhances natriuretic response to saline load. J Am Soc Nephrol. 2008;19:1947-54.
10. Blaustein MP, Zhang J, Chen L, Song H, Raina H, Kinsey SP, Izuka M, Iwamoto T, Kotlikoff MI, Lingrel JB, Philipson KD, Wier WG and Hamlyn JM. The pump, the exchanger, and endogenous ouabain: signaling mechanisms that link salt retention to hypertension. Hypertension. 2009;53:291-8.
11. Lingrel JB. The physiological significance of the cardiotonic steroid/ouabain-binding site of the Na,K-ATPase. Annu Rev Physiol. 2010;72:395-412.
12. Bagrov AY, Fedorova OV, Austin-Lane JL, Dmitrieva RI and Anderson DE. Endogenous marinobufagenin-like immunoreactive factor and Na+, K+ ATPase inhibition during voluntary hypoventilation. Hypertension. 1995;26:781-8.
13. Bagrov AY, Fedorova OV, Dmitrieva RI, Howald WN, Hunter AP, Kuznetsova EA and Shpen VM. Characterization of a urinary bufodienolide Na+,K+-ATPase inhibitor in patients after acute myocardial infarction. Hypertension. 1998;31:1097-103.
14. Fedorova OV, Doris PA and Bagrov AY. Endogenous marinobufagenin-like factor in acute plasma volume expansion. Clin Exp Hypertens. 1998;20:581-91.
15. Gonick HC, Ding Y, Vaziri ND, Bagrov AY and Fedorova OV. Simultaneous measurement of marinobufagenin, ouabain, and hypertension-associated protein in various disease states. Clin Exp Hypertens. 1998;20:617-27.
16. Schreiber V, Kolbel F, Stepan J, Gregorova I and Pribyl T. Digoxin-like immunoreactivity in the serum of rats with cardiac overload. J Mol Cell Cardiol. 1981;13:107-10.
17. Liu ZQ, Ma AQ, Zhang L and Yang DY. Intra-cellular electrolyte changes and levels of endogenous digoxin-like substance within the plasma in patients with congestive heart failure. Int J Cardiol. 1990;27:47-53.
18. Morise T, Okamoto S, Takasaki H, Ikeda M, Takeda R, Kiuti F and Tuda Y. Biological activity of partially purified digitalis-like substance and Na-K-ATPase inhibitor in rats. JpnCirc J. 1988;52:1309-16.
19. Elkareh J, Kennedy DJ, Yashaswi B, Vetteth S, Shidyak A, Kim EG, Smaili S, Periyasamy SM, Hariri IM, Fedorova L, Liu J, Wu L, Kahaleh MB, Xie Z, Malhotra D, Fedorova OV, Kashkin VA, Bagrov AY and Shapiro JI. Marinobufagenin stimulates fibroblast collagen production and causes fibrosis in experimental uremic cardiomyopathy. Hypertension. 2007;49:215-24.
20. Elkareh J, Periyasamy SM, Shidyak A, Vetteth S, Schroeder J, Raju V, Hariri IM, El-Okdi N, Gupta S, Fedorova L, Liu J, Fedorova OV, Kahaleh MB, Xie Z, Malhotra D, Watson DK, Bagrov AY and Shapiro JI. Marinobufagenin induces increases in procollagen expression in a process involving protein kinase C and Fli-1: implications for uremic cardiomyopathy. AmJ Physiol Renal Physiol. 2009;296:F1219-26.
21. Fedorova LV, Raju V, El-Okdi N, Shidyak A, Kennedy DJ, Vetteth S, Giovannucci DR, Bagrov AY, Fedorova OV, Shapiro JI and Malhotra D. The cardiotonic steroid hormone marinobufagenin induces renal fibrosis: implication of epithelial-to-mesenchymal transition. Am J Physiol Renal Physiol. 2009;296:F922-34.
Shpen VM. Characterization of a urinary bufodienolide Na+,K+-ATPase inhibiiitototor ininin pppatata ieientn safter acute myocardial infarction. Hypertension. 1998;31:1097-103.
14. Fedorova OV, Doris PA and Bagrov AY. Endogenous marinobufagenin-like fffacacacttotor rr ininin aaacucucutetete plp asasmama vvolo ummme e expansion. Clin Exp Hypertenss.. 1998;20:581-91.
155. GoGoGoninickckck HHHC,C, DDDing Y, Vaziri ND, Bagrov AY Y aaandd Fedorova OV.V.V Simmmululultaneous measurement oof marinobobo ufufufagagagennnininin,, , ouououabaa aiaiain,n,n, aaandndnd hyhyhypepepertrtrtenenensionnn-assococociaiaiateteted d prprprototeieiein nn ininin vvvarioooususus dddisisiseaeasesese ssstatatatetetes.s.s. ClC in Exp Hypppeeertennns.. 19998988;2;2;20:616161777-2227.
16166. SScS hreiber V,V, KKKolbbeel F, SSteteteppap n J,,, GGrrregggorooovva I aaandd PrPrPribibibylyll TTT. DDigggoxin---likkeke immmmunnnorrreaeaactttivi ityyy iiinthththe ee seseserururummm ofofof ratatatsss wwwiththth carrdididiacc ooovvverllloaoaoad.d.d. JJ J MoMoMolll CeCeCellllll CCCararardddiololol. 191919818181;1;1;13:3:3:1010107-7-101010.
17. Liu ZQ, Ma AQ, Zhang L anddd YYYana g gg DY. InII trtrtra-a-a-cellllllululular electrolyte changes and levels of endogenous digoxin-like subssstataancncnce e e wiwiwithththininin thehehe ppplllasasasmamama iiin nn papapatititients with congestive heart fafaililurure.e. InInt t J J CaCardrdioioll.. 19199090;2;2; 7:7:4747-553.3.
18 Morise T Okamoto S Takasaki H Ikeda M Takeda R Kiuti F and Tuda Y Biological
by guest on May 19, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

22. Kennedy DJ, Vetteth S, Periyasamy SM, Kanj M, Fedorova L, Khouri S, Kahaleh MB, Xie Z, Malhotra D, Kolodkin NI, Lakatta EG, Fedorova OV, Bagrov AY and Shapiro JI. Central role for the cardiotonic steroid marinobufagenin in the pathogenesis of experimental uremic cardiomyopathy. Hypertension. 2006;47:488-95.
23. Kolmakova EV, Haller ST, Kennedy DJ, Isachkina AN, Budny GV, Frolova EV, Piecha G, Nikitina ER, Malhotra D, Fedorova OV, Shapiro JI and Bagrov AY. Endogenous cardiotonic steroids in chronic renal failure. Nephrol Dial Transplant. 2011;26:2912-9.
24. Fedorova OV, Talan MI, Agalakova NI, Lakatta EG and Bagrov AY. Endogenous ligand of alpha(1) sodium pump, marinobufagenin, is a novel mediator of sodium chloride--dependent hypertension. Circulation. 2002;105:1122-7.
25. Shao Z, Wang Z, Shrestha K, Thakur A, Borowski AG, Sweet W, Thomas JD, Moravec CS, Hazen SL and Tang WH. Pulmonary hypertension associated with advanced systolic heart failure: dysregulated arginine metabolism and importance of compensatory dimethylarginine dimethylaminohydrolase-1. J Am Coll Cardiol. 2012;59:1150-8.
26. Wilson Tang WH, Tong W, Shrestha K, Wang Z, Levison BS, Delfraino B, Hu B, Troughton RW, Klein AL and Hazen SL. Differential effects of arginine methylation on diastolic dysfunction and disease progression in patients with chronic systolic heart failure. Eur Heart J. 2008;29:2506-13.
27. Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF, 3rd, Feldman HI, Kusek JW, Eggers P, Van Lente F, Greene T, Coresh J and Ckd EPI. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150:604-12.
28. Nagueh SF, Appleton CP, Gillebert TC, Marino PN, Oh JK, Smiseth OA, Waggoner AD, Flachskampf FA, Pellikka PA and Evangelista A. Recommendations for the evaluation of left ventricular diastolic function by echocardiography. J Am Soc Echocardiogr. 2009;22:107-33.
29. Zoghbi WA, Enriquez-Sarano M, Foster E, Grayburn PA, Kraft CD, Levine RA, Nihoyannopoulos P, Otto CM, Quinones MA, Rakowski H, Stewart WJ, Waggoner A and Weissman NJ. Recommendations for evaluation of the severity of native valvular regurgitation with two-dimensional and Doppler echocardiography. J Am Soc Echocardiogr. 2003;16:777-802.
30. Manunta P, Stella P, Rivera R, Ciurlino D, Cusi D, Ferrandi M, Hamlyn JM and Bianchi G. Left ventricular mass, stroke volume, and ouabain-like factor in essential hypertension. Hypertension. 1999;34:450-6.
31. Pierdomenico SD, Bucci A, Manunta P, Rivera R, Ferrandi M, Hamlyn JM, Lapenna D, Cuccurullo F and Mezzetti A. Endogenous ouabain and hemodynamic and left ventricular geometric patterns in essential hypertension. Am J Hypertens. 2001;14:44-50.
32. Hayashi T, Ijiri Y, Toko H, Shimomura H, Okabe M, Terasaki F, Kitaura Y and Kawamura K. Increased digitalis-like immunoreactive substances in patients with hypertrophic cardiomyopathy. Eur Heart J. 2000;21:296-305.
33. Fedorova OV, Talan MI, Agalakova NI, Lakatta EG and Bagrov AY. Coordinated shifts in Na/K-ATPase isoforms and their endogenous ligands during cardiac hypertrophy and failure in NaCl-sensitive hypertension. Journal of Hypertension. 2004;22:389-97.
34. Gottlieb SS, Rogowski AC, Weinberg M, Krichten CM, Hamilton BP and Hamlyn JM. Elevated concentrations of endogenous ouabain in patients with congestive heart failure. Circulation. 1992;86:420-5.
J. 2008;29:2506-13. JJ27. Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF, 3rd, Feldman HI,I,I, KKKusssekekek JJJW,W,W
Eggers P, Van Lente F, Greene T, Coresh J and Ckd EPI. A new equation to estststimimimatatateeeglg omomererullara ffilililtrtration rate. Ann Intern Med. 200909;150:604-12.
288. NaNaNagug eheheh SSSF,F AAAppppleton CP, Gillebert TC, Mariiinnno PN, Oh JK, SmSmmiseth hh OOOA, Waggoner AD, FFFlachskampmpmpfff FAFAF ,,, PePePellllllikikikkakk PPPA A A ananand dd EvEvEvannngegegelill staaa AA. RRRecececomomommemeennndatatatioioi nsnsns ffforo thehehe eeevavavalulul atatatioioion n n ofofof lllefeventricular ddidiaaastoliliic ffunctctctiooon bybyby eechhhooocardddiooograaaphhy.ff JJJ AmAmm SSSocc EEEchocararardidiogogogrr. 2000090909;2; 222:11107-7--33
29299. ZZoZ ghbi WWA,A, EEEnriqqqueez-SaSaararaano MMM,, FFFossster EE, Grrrayyburururnn n PAPAA,, Krrafafafttt CD,,, LLLevvvinnene RAAA, NiNiNihohohoyayayannnnnnopopopouououlololosss P,P,P, OOOttoo CMCMCM,,, QuQQ ininnonononeseses MMMA,A,A, RaRaRakokokowswswskikiki HHH, StStStewewewararartt t WJWJWJ, , WaWaWaggggggonononererr AAA aaandndnd Weissman NJ. Recommendattioioionsnsn for evalalaluauau tititiononon ooof f f thththe severity of native valvular regurgitation with two-dimennsisisionononalalal aaandndnd DDDopoppplplplererer eeechchchocococarara didid ogogography. J Am Soc Echocardiogr. 20200303;1;1; 6:6:77777-7 80802.2.
30 Manunta P Stella P Rivera R Ciurlino D Cusi D Ferrandi M Hamlyn JM and Bianchi G
by guest on May 19, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

35. Bagrov A, Fedorova OV, Maslova MN, Roukoyatkina NI, Ukhanova MV and Zhabko EP. Endogenous plasma Na,K-ATPase inhibitory activity and digoxin like immunoreactivity after acute myocardial infarction. Cardiovasc Res. 1991;25:371-7.
36. Bagrov AY, Kuznetsova EA and Fedorova OV. Endogenous digoxin-like factor in acute myocardial infarction. J Intern Med. 1994;235:63-7.
37. Fridman AI, Matveev SA, Agalakova NI, Fedorova OV, Lakatta EG and Bagrov AY. Marinobufagenin, an endogenous ligand of alpha-1 sodium pump, is a marker of congestive heart failure severity. J Hypertens. 2002;20:1189-94.
38. Pitzalis MV, Hamlyn JM, Messaggio E, Iacoviello M, Forleo C, Romito R, de Tommasi E, Rizzon P, Bianchi G and Manunta P. Independent and incremental prognostic value of endogenous ouabain in idiopathic dilated cardiomyopathy. Eur J Heart Fail. 2006;8:179-86.
39. Stella P, Manunta P, Mallamaci F, Melandri M, Spotti D, Tripepi G, Hamlyn JM, Malatino LS, Bianchi G and Zoccali C. Endogenous ouabain and cardiomyopathy in dialysis patients. J Intern Med. 2008;263:274-80.
40. Fedorova OV, Agalakova NI, Talan MI, Lakatta EG and Bagrov AY. Brain ouabain stimulates peripheral marinobufagenin via angiotensin II signalling in NaCl-loaded Dahl-S rats. Journal of Hypertension. 2005;23:1515-23.
41. Dmitrieva RI, Bagrov AY, Lalli E, Sassone-Corsi P, Stocco DM and Doris PA. Mammalian bufadienolide is synthesized from cholesterol in the adrenal cortex by a pathway that Is independent of cholesterol side-chain cleavage. Hypertension. 2000;36:442-8.
42. Priyadarshi S, Valentine B, Han C, Fedorova OV, Bagrov AY, Liu J, Periyasamy SM, Kennedy D, Malhotra D, Xie Z and Shapiro JI. Effect of green tea extract on cardiac hypertrophy following 5/6 nephrectomy in the rat. Kidney Int. 2003;63:1785-90.
43. Kennedy DJ, Chen Y, Huang W, Viterna J, Liu J, Westfall K, Tian J, Bartlett DJ, Tang WH, Xie Z, Shapiro JI and Silverstein RL. CD36 and Na/K-ATPase-alpha1 form a proinflammatory signaling loop in kidney. Hypertension. 2013;61:216-24.
44. Wenceslau CF, Davel AP, Xavier FE and Rossoni LV. Long-term ouabain treatment impairs vascular function in resistance arteries. J Vasc Res. 2011;48:316-26.
45. Pope AJ, Druhan L, Guzman JE, Forbes SP, Murugesan V, Lu D, Xia Y, Chicoine LG, Parinandi NL and Cardounel AJ. Role of DDAH-1 in lipid peroxidation product-mediated inhibition of endothelial NO generation. Am J Physiol Cell Physiol. 2007;293:C1679-86.
46. Kennedy DJ, Vetteth S, Xie M, Periyasamy SM, Xie Z, Han C, Basrur V, Mutgi K, Fedorov V, Malhotra D and Shapiro JI. Ouabain decreases sarco(endo)plasmic reticulum calcium ATPase activity in rat hearts by a process involving protein oxidation. Am J Physiol Heart Circ Physiol. 2006;291:H3003-11.
47. Kennedy DJ, Elkareh J, Shidyak A, Shapiro AP, Smaili S, Mutgi K, Gupta S, Tian J, Morgan E, Khouri S, Cooper CJ, Periyasamy SM, Xie Z, Malhotra D, Fedorova OV, Bagrov AY and Shapiro JI. Partial nephrectomy as a model for uremic cardiomyopathy in the mouse. Am J Physiol Renal Physiol. 2008;294:F450-4.
48. El-Okdi N, Smaili S, Raju V, Shidyak A, Gupta S, Fedorova L, Elkareh J, Periyasamy S, Shapiro AP, Kahaleh MB, Malhotra D, Xie Z, Chin KV and Shapiro JI. Effects of cardiotonic steroids on dermal collagen synthesis and wound healing. J Appl Physiol. 2008;105:30-6.
49. Tian J, Shidyak A, Periyasamy SM, Haller S, Taleb M, El-Okdi N, Elkareh J, Gupta S, Gohara S, Fedorova OV, Cooper CJ, Xie Z, Malhotra D, Bagrov AY and Shapiro JI.
41. Dmitrieva RI, Bagrov AY, Lalli E, Sassone-Corsi P, Stocco DM and Doris PA... MaMaMammmmmmalaaliaianbufadienolide is synthesized from cholesterol in the adrenal cortex by a pathwwwayayy tthahahat t t IsIsIs independent of cholesterol side-chain cleavage. Hypertension. 2000;36:442-8.
42. Priyiyyadadarshshi S,S,S, Valentine B, Han C, Fedorova OVOVV, Bagrov AY, Liu JJ, , , PeP riyasamy SM, KeKeKennn edededy yy D,D, MMMalhotra D, Xie Z and Shapiro JIJIJI. EEffect of green n n tet a exexxtrtrtract on cardiachhhypertrophphphy y y fofofollowowowinining g g 5/55 6 6 nenenephphphrerer ctctctomomomy y y ininin the raat. KiKiKidndndneyeyey Intntnt. 202020030303;6;6;63:33 177858585-9-9-90.0.0.
434 . Kennedy DJJ,,, CCChennn YYY, HuHuuaanang W,WW VVViteeernaaa JJJ, Liuuu JJJ, WWWeesestftftfallll K,K,, TTTian JJJ, BBBararrtlllett DJDJDJ, TaTaanggg WWWHH,H XXiX e Z, Shaapiiirooo JI aanandd Sillvlveererstein n n RRLL... CDDD36 annnd Na/a/a/K-K-K ATATATPassse---alphaaa1 fooormmm a prprproioioinfnfnflalalammmmmmaatatororory y y sisisigngngnalaa inng g g lololoopopop in kikikidndndneyeyey... HyHyHypepepertrtrtenenensisisiononon. 20202013133;6;6;61:1:1:2121216-6-6-242424.
44. Wenceslau CF, Davel AP, Xaaavivivieree FE and d d RoRoossssssono i i i LVLVL . Longgg-term ouabain treatment impairsvascular function in resistanceee aaartrtrterererieieiess.s. JJ J VVVascscsc RRReseses.. 202020111111;4;4;48:8:8:316-26.
4545. . PoPopepep AAJ,J,, DDruruhahan n L,L,, GGuzuzmaman n JEJE,,, FoForbrbeses SSP,P,, MuMururugegeg sasan n V,V,, LLu u D,D,, XXiaia YY, , , ChChicicoioinene LLG,G,, Parinandi NL and Cardounel AJ Role of DDAH-1 in lipid peroxidation product-mediated
by guest on May 19, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

Spironolactone attenuates experimental uremic cardiomyopathy by antagonizing marinobufagenin. Hypertension. 2009;54:1313-20.
by guest on May 19, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

Table. Baseline Characteristics (n=245).
Variable Value
Demographics:
Age (years) 58 ± 13
Male gender, n (%) 164 (67%)
Body mass index (kg/m2) 30 ± 6
African American, n (%) 45 (18%)
Heart failure history:
Ischemic etiology, n (%) 92 (39%)
NYHA class III or IV, n (%) 95 (66%)
Co-morbidities:
Hypertension, n (%) 130 (54%)
Diabetes mellitus, n (%) 92 (38%)
Echocardiographic indices:
LV mass index (g/m2) 159 ± 57
LV end-diastolic volume index (mL/m2) 97 ± 42
LV ejection fraction (%) 31 ± 13
Mitral E/e’ ratio 22 ± 12
Mitral E/A ratio 1.9 ± 1.0
Mitral DT (ms) 160 ± 52
Tricuspid E/e’ ratio 7.1 ± 3.8
LA volume index (mL/m2) 41 ± 17
RV end-diastolic area (cm2) 26 ± 9
NYHA class III or IV, n (%) 95 (((666666%)%)%)
CoCoCo-m-m-morororbibibididitititiesee :
Hypertenenensssioonon, n nn (%(%(%))) 131313000 (5(5(54%4%4%)))
Diabbetetetesee mmmellitttusss, n (%)%)%) 929292 (3888%%%)
Echocardiographic indices:
LVLVLV mass iiindddex (((g///m222))) 151515999 ±±± 575757
by guest on May 19, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

RV s’ (cm/s) 9 ± 3
RV Fractional area change 34 ± 12
Tricuspid DT (ms) 189 ± 61
RA volume index (mL/m2) 34 ± 18
Medications:
Angiotensin converting enzyme inhibitors or angiotensin
receptor blockers, n (%)
143 (61%)
Beta-blockers, n (%) 171 (73%)
Spironolactone, n (%) 87 (37%)
Loop diuretics, n (%) 151 (64%)
Digoxin, n (%) 70 (30%)
Laboratory data:
MBG (pM) 583 [383, 812]
Myeloperoxidase (pM) 124 [77- 253]
BNP (pg/mL) 431 [97, 1417]
eGFR (mL/min/1.73m2) 71 ± 32
Cystatin C (mg/L) 1.85 [1.31 – 2.61]
ADMA ( M) 1.05 [0.82 – 1.33]
SDMA ( M) 1.70 [1.05 – 2.96]
MMA (nM) 50 [34 – 92]
Abbreviation: NYHA, New York Heart Association; LV, left ventricular; RV, right ventricular; MBG, marinobufagenin (MBG); eGFR, estimated glomerular filtration rate; BNP, B-type natriuretic peptide, ADMA, Asymmetric dimethylarginine; SDMA, symmetric dimethylarginine; MMA, mono methyl arginine.
Loop diuretics, n (%) 151 (6(6(64%4%4%)))
DiDiDigogogoxixixin, nnn (%) 70 (30%)
LLLaboratoryyy dddaaata:a:a:
MBG G G (p(( M)M)M) 58883 [3[ 8333, 8881222]
Myeloperoxidase (pM) 124 [77- 253]
BNBNBNPPP (((p //g/ LLmL))) 434343111 [9[9[9777, 1114141417]7]7]
by guest on May 19, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

Figure Legends
Figure 1. Marinobufagenin levels in heart failure. Comparison of plasma marinobufagenin
levels between non-heart failure (non-HF) participants and HF participants with reduced ( 40)
or preserved (>40) left ventricular ejection fraction (EF). ** p <0.001 vs control, by Student’s
t-test with Bonferroni’s correction.
Figure 2. Kaplan-Meier analysis of major adverse cardiac events (MACE) in participants
with heart failure. (A) Heart failure patients (n=245) stratified according to optimal cutoff for
plasma marinobufagenin (MBG) as follows: “Low” MBG (<574 pM) or “High” MBG ( 574
pM). (B) Subgroup analysis of heart failure patients (n=115) with serial blood draws from
admission to pre-discharge at 48-72 hours stratified according to optimal cutoff for change in
plasma MBG as follows: “decreasing” MBG (<5%) or “increasing” MBG ( 5%).
Figure 3. Elevated MBG levels contribute to nitrative stress. Echocardiographic measures of
cardiac ejection fraction (A) and Diastolic Left Ventricular Internal Dimension (LVIDd) (B)
after 4 weeks of either LAD ligation (LADx) or MBG infusion. Gene expression of calcium
handling proteins sarcoplasmic reticulum calcium ATPase (SERCA2a) (C) and sodium calcium
exchanger (NCX-1) (D), and hypertrophic markers beta myosin heavy chain ( MHC) (E) and
atrial natriuretic peptide (ANP) (F) after 4 weeks of LADx. Plasma MBG (G) levels are
increased 4 weeks after LAD ligation in a post myocardial infarction heart failure model. (H)
Adrenal tissue MBG levels 1 week after LAD ligation. P values were calculated using the Mann-
Whitney U test.
pM). (B) Subgroup analysis of heart failure patients (n=115) with serial bllooooooddd drdrdrawawaws s s frf om
admisssioion n too preee-ddischarge at 48-72 hours stratififiede according to optiimamm l cutoff for change in
plplplasssma MBGGG aasss fofofollowowows:s:s: ““dedd crcrreaeaeasisisingngng”” MMMBGBGG (((<5< %%%) or “i“iincncncrerereasininin ”g”g” MMMBGBGBG ( 555%)%)%)...
Figure 3. Elevated MBG levels s s cococontn ributeee to o nininitrt atatativivive stress. Echocardiographic measures o
cacardrdiaiac c ejejjecectitionon ffraractctioion n (A(A( ))) anand d DiDiasastotolilic c LeLeftft VeVentntriricuculalar r InInteternrnalal DDimimenensisionon (((LVLVIDIDd)d)) (((BB
by guest on May 19, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

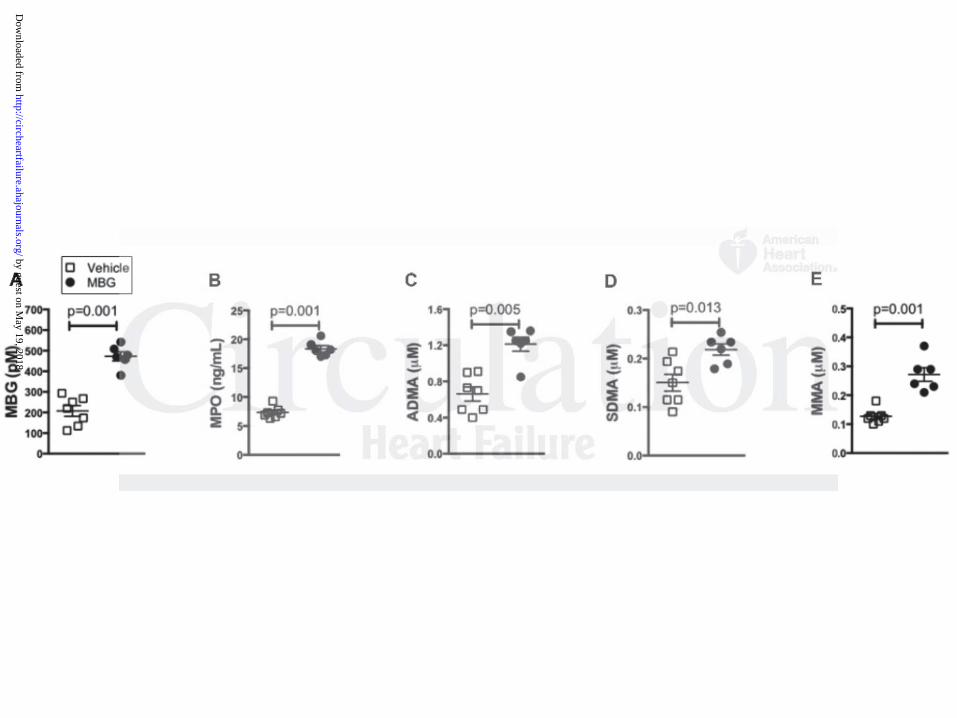
Figure 4. Elevated MBG levels contribute to nitrative stress. After 4 week infusion of MBG,
plasma levels of MBG (A) and MPO (B), as well as methylated arginine metabolites asymmetric
dimethylarginine (ADMA, C), symmetric dimethylarginine (SDMA, D), and mono methyl
arginine (MMA, E) are increased vs vehicle treated mice. P values were calculated using the
Mann-Whitney U test.
Figure 5. Elevated MBG levels contribute to fibrosis. Representative picosirius red histology
(A) and quantitative morphometry (B) from mouse hearts after 4 week MBG infusion. Scale bar
represents 100 um. P values were calculated using the Mann-Whitney U test.
by guest on May 19, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

by guest on May 19, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
by guest on May 19, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

by guest on May 19, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
by guest on May 19, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

by guest on May 19, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

Alexei Y. Bagrov and W.H. Wilson TangMichael Finucan, Alaa Gabi, Charles M. Medert, Kristen Westfall, Allen Borowski, Olga Fedorova,
David J. Kennedy, Kevin Shrestha, Brendan Sheehy, Xinmin S. Li, Anuradha Guggilam, Yuping Wu,Right Ventricular Dysfunction and Nitrative Stress in Heart Failure
Elevated Plasma Marinobufagenin, An Endogenous Cardiotonic Steroid, Is Associated with
Print ISSN: 1941-3289. Online ISSN: 1941-3297 Copyright © 2015 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation: Heart Failure published online August 14, 2015;Circ Heart Fail.
http://circheartfailure.ahajournals.org/content/early/2015/08/14/CIRCHEARTFAILURE.114.001976World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circheartfailure.ahajournals.org/content/suppl/2015/08/14/CIRCHEARTFAILURE.114.001976.DC1Data Supplement (unedited) at:
http://circheartfailure.ahajournals.org//subscriptions/
is online at: Circulation: Heart Failure Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information about thisEditorial Office. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculation: Heart Failure Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on May 19, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
1
SUPPLEMENTAL MATERIAL
Quantitative Histologic Techniques. Mason’s trichome and picosirius red staining was
performed on deparafinized 5 µm serial heart sections. The sections were mounted
under a Leica DM 2500 microscope and digitized with a QImaging MicroPublisher 5.0
RTV camera. Quantitative morphometric analysis was performed on fields (at least 8
from each animal) and the collagen volume was determined using automated and
customized algorithms/scripts for batch analysis (ImageIQ Inc., Cleveland, OH) written
for Image Pro Plus 7.0. Briefly, a set of representative images were chosen that
demonstrated a wide range of staining intensities and prevalence. In an automated
script, these "training" images were loaded one after another prompting the user to
delineate pixels representing positive collagen staining using an interactive color picking
tool. An iterative color profile or classifier was generated and subsequently applied to all
images in a given directory using a fully automated algorithm. Positive pixels, as defined
by the color profile, were segmented and summed to provide positive staining area.
Total tissue area was determined by extracting the "saturation" channel, applying a lo-
pass filter, and thresholding the result. Any area within the general tissue boundary that
was empty (i.e. white) was removed by converting the original image to grayscale and
applying a fixed threshold for non background pixels on adequately white-balanced
images. Finally, total tissue area and total stained area were exported to Excel. For
post-processing verification, segmented regions were superimposed onto the original
image (green outlines) for each image analyzed.

2
Transthoracic Echocardiography. Comprehensive 2-dimensional echocardiography was
performed in standard parasternal and apical views on all participants by an American
Society of Echocardiography registered research sonographer using a Vivid 7
echocardiography machines (GE Healthcare, Waukesha WI) equipped with a phased-
array transducer. Standard 2-dimensional and Doppler data, triggered to the QRS
complex, was digitally stored in a cine-loop format. The Simpson biplane method was
used to measure left ventricular ejection fraction (LVEF), left ventricular end-systolic
volume index (LVESVI), and left atrial volume index (LAVI). Ventricular volume and
mass measurements were indexed to body surface area. Right ventricular systolic
pressure (RVSP) was calculated from the Doppler estimated tricuspid valve regurgitant
jet velocity using the Bernoulli equation. Assessment and classification of diastolic
parameters, mitral inflow patterns, and quantification of mitral regurgitation were made
following the American Society of Echocardiography recommendations1, 2. Small animal
echocardiography was performed using a Vivid 7 ultrasound machine (GE Medical)
equipped an il3L linear probe operated at 14 MHz in order to obtain 2-D (parasternal
long- and short-axis views) and M-mode images as we have previously published3, 4. All
echocardiographic measurements were averaged over three cardiac cycles.

3
Supplemental Table 1. Univariate correlations between marinobufagenin (MBG) and clinical and echocardiographic characteristics MBG (pM)
Spearman’s r p-value
Age (years) 0.06 0.392
Body mass index (kg/m2) 0.02 0.768
Echocardiographic Indices
LV Structure
LV mass index (g/m2) 0.15 0.073
LVEDVi (mL/m2) -0.05 0.552
LV Systolic function
LV ejection fraction (%) -0.04 0.585
LV Diastolic function
Mitral E/e’ ratio
Mitral E/A ratio
0.13
0.12
0.136
0.202
Mitral DT (ms) -0.24 0.007
LA volume index (mL/m2) -0.04 0.551
RV Structure
RV end-diastolic area (cm2) 0.21 0.023
RV Systolic function
RV s' (cm/s) -0.39 <0.0001
RV Fractional area change -0.42 <0.0001
RV Diastolic Function
Tricuspid E/e' ratio 0.22 0.027

4
Tricuspid DT (ms) -0.38 0.002
RA volume index (mL/m2) 0.22 0.013
Laboratory Data
Myeloperoxidase (pM) 0.42 <0.0001
BNP (pg/mL) 0.25 0.001
eGFR (mL/min/1.73m2) -0.06 0.345
Cystatin C (mg/L) 0.06 0.485
ADMA (μM) 0.32 <0.001
SDMA (μM) 0.34 <0.001
MMA (μM) 0.40 <0.0001
Abbreviation: ADMA, Asymmetric dimethylarginine; SDMA, symmetric dimethylarginine;
MMA, monomethyl arginine

5
Supplemental Table 2. Cox proportional hazards analyses of adverse long-term
clinical outcomes.
HR (95% CI) p-value
MBG 1.58 (1.10 – 2.31) 0.014
Adjusted for age, male gender 1.55 (1.07 – 2.26) 0.019
Adjusted for age, gender, LVEF 1.51 (1.04 – 2.21) 0.031
Adjusted for age, gender, LVEF, ischemic etiology 1.48 (1.01 – 2.17) 0.042
Adjusted for age, gender, ischemic etiology, diabetes
mellitus
1.50 (1.04 – 2.19) 0.031
Adjusted for age, gender, smoking, diabetes mellitus 1.47 (1.02 – 2.14) 0.040
Adjusted for eGFR 1.43 (0.99 – 2.08) 0.060
Adjusted for ischemic etiology 1.53 (1.06 – 2.24) 0.023
Adjusted for mitral E/e' ratio 1.65 (0.97 – 2.87) 0.066
Adjusted for RV s' 1.36 (0.76 – 2.51) 0.305
Adjusted for tricuspid E/e' 1.36 (0.77 – 2.46) 0.290
Adjusted for BNP 1.40 (0.87 – 2.31) 0.169
*HRs represent the risk associated with MBG levels ≥ 574 pM

6
Supplemental Table 3. Net reclassification analysis 5
Discrimination Analysis Percentage 95% CI P-value
AUC
Model with MBG 60.7% 0.33
Model without MBG 57.8%
IDI 3% <0.001
NRI 33.6% 9.3%-57.8% 0.007
Events correctly reclassified 41.9%
Non-events correctly reclassified -8.3%
Abbreviation: AUC, Area under the curve; IDI, integrated discrimination improvement;
NRI, net reclassification index; CI, confidence interval.
Both models were adjusted for age, gender, ischemic etiology, and diabetes. The risk of
mortality was estimated using the Cox model.

7
Supplemental Table 4. Cox proportional hazards analyses by quartiles for adverse
long-term clinical outcomes.
HR (95% CI) P-value
MBG Quartile 4 vs Quartile 1 1.57 (0.91 – 2.75) 0.102
MBG Quartile 3 vs Quartile 1 2.14 (1.27 – 3.68) 0.004
MBG Quartile 2 vs Quartile 1 1.43 (0.81 – 2.55) 0.222
8
Supplemental References
1. Nagueh SF, Appleton CP, Gillebert TC, Marino PN, Oh JK, Smiseth OA, Waggoner AD, Flachskampf FA, Pellikka PA and Evangelista A. Recommendations for the evaluation of left ventricular diastolic function by echocardiography. J Am Soc Echocardiogr. 2009;22:107-33.
2. Zoghbi WA, Enriquez-Sarano M, Foster E, Grayburn PA, Kraft CD, Levine RA, Nihoyannopoulos P, Otto CM, Quinones MA, Rakowski H, Stewart WJ, Waggoner A and Weissman NJ. Recommendations for evaluation of the severity of native valvular regurgitation with two-dimensional and Doppler echocardiography. J Am Soc Echocardiogr. 2003;16:777-802.
3. Kennedy DJ, Vetteth S, Periyasamy SM, Kanj M, Fedorova L, Khouri S, Kahaleh MB, Xie Z, Malhotra D, Kolodkin NI, Lakatta EG, Fedorova OV, Bagrov AY and Shapiro JI. Central role for the cardiotonic steroid marinobufagenin in the pathogenesis of experimental uremic cardiomyopathy. Hypertension. 2006;47:488-95.
4. Kennedy DJ, Elkareh J, Shidyak A, Shapiro AP, Smaili S, Mutgi K, Gupta S, Tian J, Morgan E, Khouri S, Cooper CJ, Periyasamy SM, Xie Z, Malhotra D, Fedorova OV, Bagrov AY and Shapiro JI. Partial nephrectomy as a model for uremic cardiomyopathy in the mouse. Am J Physiol Renal Physiol. 2008;294:F450-4.
5. Pencina MJ, D'Agostino RB, Sr. and Steyerberg EW. Extensions of net reclassification improvement calculations to measure usefulness of new biomarkers. Stat Med. 2011;30:11-21.