eliminating lateral violence in the ambulatory...
TRANSCRIPT
Eliminating Lateral Violence inthe Ambulatory Setting: OneCenter’s Strategies
TINA J. DIMARINO, BSN, RN, CNORed by onee harmfuline of thes of lateral
first stepmaintain
pectations. Use of athat arisely combat© AORN,
ence, dis-ork
ABSTRACT
Lateral violence (eg, disruptive, disparaging, or uncivil behavior inflictpeer on another) creates an unpleasant work environment that can haveffects on individual nurses, team members, patients, and the bottom lhealth care organization. Educating nurses about the most common formviolence and strategies for handling inappropriate behavior can be thetoward eliminating this behavior. Effective nursing leaders develop anda “zero-tolerance” culture that includes clear and concise behavioral exand consequences for employees who exhibit unprofessional behaviorcode of conduct, open communication, and quick resolution of issuesare strategies that one ambulatory surgery center has used to successfullateral violence in the workplace. AORN J 93 (May 2011) 583-588.Inc, 2011. doi: 10.1016/j.aorn.2010.10.019
Key words: lateral violence, horizontal violence, nurse-to-nurse violruptive behaviors, code of conduct, zero-tolerance culture, healthy wenvironment.
orizoence,
creaas hasafebee
nce iallo
y, inlega
indivrage
iors s
viors rang-rolling orcal abuse.3,4
t commonnclude non-ping, under-otage, in-failure to
ces.5,6
nsequencesold chil-break your
it.”7(p101)
Lateral violence, also called hviolence, nurse-to-nurse violity, and disruptive behavior,1
unpleasant work environment and heffects on individual nurses, patienthealth care organizations. Much hasten about the effects of lateral violeworkplace. When lateral violence isexist, it affects everyone at a facilitpatients. Lateral violence is definedoccurring “when oppressed groups/internalize feelings such as anger andmanifest their feelings through behav
gossip, jealousy, putdowns, and blaming.”doi: 10.1016/j.aorn.2010.10.019
© AORN, Inc, 2011
ntalincivil-tes anrmfulty, andn writ-n thewed tocludinglly asiduals, anduch as
Lateral violence encompasses behaing from nonverbal acts such as eye-eyebrow raising to extremes of physiResearchers have found that the mosforms of lateral violence in nursing iverbal innuendo, verbal insults, gossimining, withholding information, sabfighting, scapegoating, backstabbing,respect privacy, and broken confiden
Vega and Comer emphasize the coof lateral violence by paraphrasing andren’s rhyme, “sticks and stones maybones, but words can break your spir
2 Nurses who are subjected to lateral violence in
May 2011 Vol 93 No 5 ● AORN Journal 583

nt.4,7-
verag.8 Inrganid witities amem
d teamsely a
easedtimidaors ay conmes.1
pe oftcomeerious
oftenrly.10
lenceth phess frr loseffe
deprer expembebehav
e neehe amas inolenc
enseRatheue, mal viomem
eral violences as negative.14 This rec-inating the
lateral vio-and singlesinates dif-lence is. Forther nurse’sa secondas lateralentify lateralrespectfulreduces con-sociated withprove workehavior.4
nurse withe when
organiza-romote aent.16 Effec-ntain a “zero-
bers of therofessionaloral expecta-ment of pro-tly, there is
ences forl behavior.11
icies andramount.9
e reportingof reprisalinappropriatenteredre vital.17
promote ature culti-
May 2011 Vol 93 No 5 DIMARINO
the workplace often leave employmeturnover can cost an institution, on atween $22,000 and $64,000 per nursetion to the financial burdens on the oremaining staff members are burdeneing to shoulder additional responsibiltrain replacements.10 Remaining staffmay have little trust in each other anmay suffer, which in turn may adverpatient safety and outcomes.10,11
In 2008, the Joint Commission reltinel Event Alert emphasizing that indisruptive, and unprofessional behavisuitable in a culture of safety and mato preventable negative patient outcoganizations that allow or ignore this tyior risk experiencing these negative ouLateral violence has been called a “sin the delivery of safe care.”10(p400)
Nurses affected by lateral violencethe enthusiasm to do their jobs propedition, nurses subjected to lateral vioence stress that can manifest itself boand emotionally.12 Physically, the streral violence can cause weight gain olessness, and illnesses, to name a fewEmotionally, the nurse may becomefeel anxious, have low self-esteem, olow morale.9,12,13 Over time, staff mcome to consider these unacceptableroutine.10,13
Education and strong leadership arhelp curtail inappropriate behavior. Ttory surgery center in which I work hseveral strategies to combat lateral viimprove the work environment.
EDUCATIONEducation serves as a first line of deftering a healthy work environment.4
allowing negative behaviors to continers and directors educated about laterand conflict resolution can help staff
achieve positive outcomes. Educating nurs584 AORN Journal
9 Thise, be-addi-
zation,h hav-ndberswork
ffect
a Sen-ting,
re un-tribute
1 Or-behav-s.11
barrier
lackIn ad-experi-ysicallyom lat-s, sleep-cts.12
ssed,eriencers mayiors as
ded tobula-
stitutede and
for fos-r thananag-lence
bers
about the most common forms of lathelps them to recognize the behaviorrather than accepting them as normalognition is often the first step in elimbehavior.15
Knowledge about what constituteslence calls attention to the behaviorsthem out as unacceptable. It also elimfering opinions about what lateral vioexample, one nurse may attribute anoincivility to being stressed out, whilenurse may define that same behaviorviolence.14 Helping staff members idviolence (ie, chronic disruptive or disbehavior versus a one-time reaction)fusion. Educational intervention is asincreasing nurses’ commitment to imrelationships and eradicate negative bFurthermore, education provides thethe tools to cope or confront someonnecessary.4
LEADERSHIPLeaders have a responsibility to theirtion, staff members, and patients to pprofessional, positive work environmtive nursing leaders develop and maitolerance” culture by holding all memhealth care team accountable for unpbehavior.11 Clear and concise behavitions are paramount in the encouragefessional behavior.11 Just as importana need for clear and concise consequemployees who exhibit unprofessiona
In addition to having written polconsequences, communication is paStaff members who feel comfortablproblems to managers without fearwill not remain silent witnesses tobehavior.4,10 Work relationships cearound mutual respect and caring aRespectful and caring relationshipspositive culture.14,15 A positive cul
es vates professional behavior.17
in crThes state neeo fosom och ans prol thers eqstero wato beironm.
my teverbaehaviery cereceies, In othrsontimsto mmes,entilong
other orgafor lave wors an
a heaOur eting thy theorkaddi
onduct fo-nication,r codexpectationsy furtherptable be-tified bydisruptive
of conduct,tarting pointding policy.n and pro-
f memberss, or talkese discus-sure stafft have work-aff member. Over time,managers
oicing their
iolence to allce programs.everyonets on the em-ization. Wenual basis sois accept-
ASC. As afind andterials into
clearly iden-deviationses need tozation byen employ-ur expecta-of conductrds. We ac-
LATERAL VIOLENCE www.aornjournal.org
The nurse manager is instrumentalpositive culture in an organization.14
can Organization of Nurse Executive“collaboration and communication arhealthy workplace.”6(p88) Leaders whteamwork, autonomy, and freedom frsive behaviors also aid in creating suronment.9,17 Effective nurse managerclear expectations for behavior, modeior consistently, hold all staff membeaccountable for their behavior, and focommunication for staff members whaddress problems. All nurses deservewith respect and to practice in an envconducive to the safe care of patients
OUR CENTER’S STRATEGYI experienced lateral violence duringa perioperative nurse. Backstabbing,nonverbal innuendo, and infighting bwere rampant at the ambulatory surg(ASC) where I worked. I was on theend of this behavior and, at other timobserver or witness to its infliction oremember thinking, “How is this peget away with such behaviors?” Viccluding me, reported the behaviorswith little or no resolution. Many tiers dismissed the behavior by comm“Oh, that’s just the way he is.” I nowork at that ASC.
I now serve as administrator for anMy experience with incivility and oution’s commitment to zero toleranceviolence has helped to create a positivironment at our center. Administratoagers at this facility want to providework atmosphere for staff members.have resulted in staff members repormorale is at an all-time high. They sacoming to work and that the ASC’s wronment is pleasant and enjoyable. In
have not experienced any turnover relatedeating aAmeri-es thatded in aterppres-envi-
videbehav-
uallyopennt to
treatedent
nure asl andorsnter
vingwas aners. Iable to
, in-anagersmanag-
ng,er
r ASC.niza-
teralrk en-d man-lthyffortsat theiry enjoyenvi-tion, we
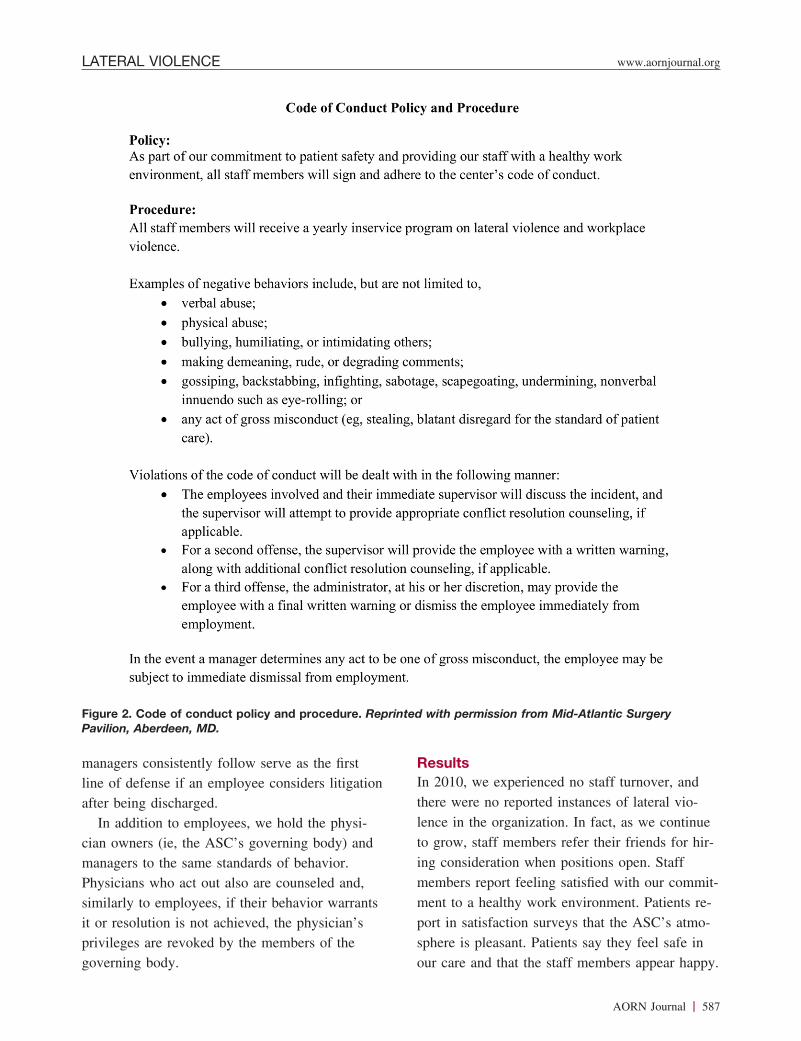
eral violence incidents. Our code of ccuses on the values of caring, commurespect, and teamwork (Figure 1). Ouclearly and succinctly describes our eof acceptable behavior, and our policidentifies the consequences of unaccehavior (Figure 2). The resources idenLongo,4 such as the steps to combatbehaviors and tips for drafting a codewere helpful in providing us with a sto create this code and the correspon
Managers encourage communicatiomote an open-door policy where stafcan express concerns, vent frustrationabout whatever is on their minds. Thsions are confidential. Managers reasmembers that the discussions will norelated repercussions, even when a stis voicing concerns about a coworkerstaff members have come to trust theand learned to be more open about vconcerns.
We provide education on lateral vstaff members through annual inserviThese sessions serve as reminders toabout negative behavior and its effecployees, patient safety, and the organreview our code of conduct on an anthat there is no confusion about whatable or unacceptable behavior in ourresult of this yearly review, we oftenincorporate additional educational maour policies.
ExpectationsProfessional behavior is required andtified. We do not overlook or acceptfrom professional behavior. Employebecome team members of our organiadhering to our code of conduct. Whees are hired, we review with them otions and ask them to sign our codeand pledge adherence to these standa
to lat- tively discourage gossiping and disruptive or rude
AORN Journal 585

g to o
utmo
embe
We a
ng a
care.
d or
ent t
re en
ions a
yees
fessio
use o
mat
ager a
t caus
flicts
ing pe
ame or find-
pproach to
ing the code
s clarify mis-
and discuss
on ground.
fy and ac-
h party is
ior. If the
s to discuss
erbal or writ-
esolving the
nship with
nd may
r experience,
ether and
fill the va-
nagers main-
ractions in-
and all
policies that
May 2011 Vol 93 No 5 DIMARINO
behaviors by reinforcing and adherin
code of conduct. Teamwork is of the
importance.
ActionsManagers, nurse leaders, and staff m
held accountable for their behaviors.
problems as quickly as possible, as lo
so does not negatively affect patient
experience, matters that go unresolve
to escalate create a negative environm
fects team performance. Employees a
aged to report code of conduct violat
as possible. Managers counsel emplo
not acting in a respectful, caring, pro
manner by providing guidance in the
propriate communication skills. If the
conflict between employees, the man
the employees in discovering the roo
problem. In our experience, most con
result of miscommunication or differ
Figure 1. Code of conduct. Reprinted with p
586 AORN Journal
ur
st
rs are
ddress
s doing
In our
are left
hat af-
cour-
s soon
who are
nal
f ap-
ter is a
ssists
e of the
are a
rcep-
tions. Without resorting to placing bl
ing fault, managers use a proactive a
help ensure that employees are follow
of conduct. Managers help employee
communications and misperceptions
these with both parties to reach comm
We encourage employees to identi
complish appropriate resolutions. Eac
held accountable for his or her behav
manager makes at least three attempt
the problem or gives the employee v
ten warnings and is unsuccessful in r
conflict, we dissolve the work relatio
the employee. This is often difficult a
leave us short-staffed. It has been ou
however, that team members pull tog
work harder while steps are taken to
cant position. It is imperative that ma
tain proper documentation of all inte
volving the counseling of employees
verbal and written warnings. Written
ermission from Mid-Atlantic Surgery Pavilion, Aberdeen, MD.
s theers li
the pbod
havioseledior whysicrs of
over, andateral vio-we continueends for hir-n. Staffour commit-Patients re-SC’s atmo-eel safe in
rgery
LATERAL VIOLENCE www.aornjournal.org
managers consistently follow serve aline of defense if an employee considafter being discharged.
In addition to employees, we holdcian owners (ie, the ASC’s governingmanagers to the same standards of bePhysicians who act out also are counsimilarly to employees, if their behavit or resolution is not achieved, the pprivileges are revoked by the membe
Figure 2. Code of conduct policy and pPavilion, Aberdeen, MD.
governing body.
firsttigation
hysi-y) andr.and,arrantsian’sthe
ResultsIn 2010, we experienced no staff turnthere were no reported instances of llence in the organization. In fact, asto grow, staff members refer their friing consideration when positions opemembers report feeling satisfied withment to a healthy work environment.port in satisfaction surveys that the Asphere is pleasant. Patients say they f
ure. Reprinted with permission from Mid-Atlantic Su
rocedour care and that the staff members appear happy.
AORN Journal 587

itionarogra
dicatevironaccevioleanagwithreco
hey oexpeced a cis resed threateflou
n worrs Rev
http://dNovem
riate b. 2009
rs: stranline J
enuCatbleofCruptive, 2010as a sly lice:257-2ng: con
may break yourbullying in the
1-109.benefits ofrse retention.d.org/MainPeriodicals/o3Sept07/er 18, 2010.al violence.
violence in:399-403.atient safety.ointcommissiona_40.htm. Ac-
raw CA, Pagacerioperative
s: nurse-to-0;45(3):166-
Michel Y, Wel-e nursing07;28(11):1247-
risk? Tenn
date: we arerolina Nurse.
on M. Dealingzero tolerance.09;47(12):
R, is al Consul-
strator ofAberdeen,affiliationpotentialof this
May 2011 Vol 93 No 5 DIMARINO
Research has helped us discover addtional resources and strengthen our p
CONCLUSIONAs nursing professionals strive to erafessional behaviors from the work enignoring lateral violence is no longerResponsibility for eliminating lateralstarts with the owners, leaders, and mthe health care organization and endsstaff members, who must consistentlyand deal with these behaviors when tWith commitment, clearly identifiedand consistent actions, we have shapof caring and respect at our ASC. Thhas improved our organization, fosterdelivery of care to our patients, and cenvironment that allows our nurses toto practice excellent nursing.
References1. Johnson SL. International perspectives o
bullying among nurses: a review. Int Nu56(1):34-40.
2. Legal definition of lateral violence, 2010..uslegal.com/l/lateral-violence/. Accessed2010.
3. Kirchner B. Safety: addressing inappropin the perioperative workplace. AORN J177-180.
4. Longo J. Combating disruptive behaviopromote a healthy work environment. ONurs. http://www.nursingworld.org/MainMANAMarketplace/ANAPeriodicals/OJIN/TaVol152010/No1Jan2010/Combating-DisBehaviors.aspx. Accessed November 18
5. Griffin M. Teaching cognitive rehearsallateral violence: an intervention for newnurses. J Contin Educ Nurs. 2004;35(6)
6. Johnson SL, Rea RE. Workplace bullyi
nurse leaders. J Nurs Adm. 2009;39(2):84-90.588 AORN Journal
l educa-m.
unpro-ment,ptable.nceers ofitsgnizeccur.tations,ulturepecte safed anrish and
kplace. 2009;
efinitionsber 18,
ehavior;90(2):
tegies toIssues
egories/ontents/-.hield fornsed63.cerns for
7. Vega G, Comer DR. Sticks and stonesbones, but words can break your spirit:workplace. J Bus Ethics. 2005;58(1):10
8. Bland-Jones C, Gates M. The costs andnursing turnover: a business case for nuOnline J Issues Nurs. http://nursingworlMenuCategories/ANAMarketplace/ANAOJIN/TableofContents/Volume122007/NNurseRetention.aspx. Accessed Novemb
9. Longo J, Sherman R. Leveling horizontNurs Manage. 2007;38(3):34-37, 50-51.
10. Sheridan-Leos N. Understanding lateralnursing. Clin J Oncol Nurs. 2008;12(3)
11. Behaviors that undermine a culture of pSentinel Event Alert. 2008;40. http://www.j.org/Sentinelevents/Sentineleventalert/secessed November 18, 2010.
12. Bigony L, Lipke TG, Lundberg A, McGGL, Rogers A. Lateral violence in the psetting. AORN J. 2009;89(4):688-700.
13. Embree JL, White AH. Concept analysinurse lateral violence. Nurs Forum. 201173.
14. Stanley KM, Martin MM, Nemeth LS,ton JM. Examining lateral violence in thworkforce. Issues Ment Health Nurs. 201265.
15. Norris T. Lateral violence: is nursing atNurse. 2010;73(2):1, 7.
16. Dulaney P, Zager L. Lateral violence upstill listening & we thank you. South CaJuly-September 2010;11.
17. Cleary M, Hunt GE, Walter G, Robertswith bullying in the workplace: towardJ Psychosoc Nurs Ment Health Serv. 2034-41.
Tina J. DiMarino, BSN, RN, CNOnurse consultant for Custom Surgicatants, LLC, Street, MD, and adminithe Mid-Atlantic Surgery Pavilion,MD. Ms DiMarino has no declaredthat could be perceived as posing aconflict of interest in the publication
article.