e&m coding guidelines - university of nevada, reno …€¢ cdi e l i & m s i b d coding an...
TRANSCRIPT

Evaluation & Management Documentation and Coding Documentation and Coding GuidelinesPresented by: Kristi A. Gutierrez CCS-P, CPC, CEMC

Objectives
• Participants will gain a working knowledge of Medicare’s 1995 Evaluation & Management Medicare s 1995 Evaluation & Management Documentation Guidelines.
• Participants will be able to apply the knowledge in everyday situations while seeing patients in y y g porder to utilize the correct level of Evaluation & Management Service and document that service
di ’ id lito meet Medicare’s Guidelines.

Agenda
• Medicare’s ‘95 Documentation Guidelines (DG) for Providers
• New and Established Patient Visits
• Consultations
• Hospital Services
C di E l i & M S i B d • Coding an Evaluation & Management Service Based on Time

Overview
• Medicare’s 1995 guidelines were developed to assist providers in choosing a level of service assist providers in choosing a level of service. Per Medicare’s DG the visit is made up of three (3) key components:(3) key components:▫ History;
▫ Physical Exam; and
M di l D i i M ki▫ Medical Decision Making.

What does Medicare need documented to bill a level of service?bill a level of service?• History▫ Chief Complaint (CC)▫ Chief Complaint (CC)▫ History of Present Illness (HPI)▫ Review of Systems (ROS)Review of Systems (ROS)▫ Past, family and/or social history (PFSH)
• Examination• Medical Decision Making (MDM)

Medical Decision Making (MDM)
• Medical Decision Making refers to the complexity of establishing a diagnosis and/or complexity of establishing a diagnosis and/or selecting a management option as measured by:

MDM Cont’d
• Number of possible diagnoses and/or number of management options that must be considered;management options that must be considered;
• The amount and/or complexity of medical records, diagnostic tests, and/or other information that must be obtained, reviewed and analyzed; and
• The risk of significant complications, morbidity d/ t lit ll biti i t d and/or mortality, as well as co-morbities, associated
with the patients presenting problem(s), the diagnostic procedure(s) and/or the possible g p ( ) / pmanagement options.

Number of Management Options/Diagnoses
• Self limited/minor (max 2 problems) or Est prob stable/improved = 1 pointEst prob stable/improved = 1 point
• Established Problem worsening = 2 points• New problem; no additional work up planned • New problem; no additional work up planned
(max 1 prob) = 3 points• New problem; additional work up planned (max p b ; p p (
1 prob) = 4 points


Scoring the Number of Diagnoses or Management OptionsManagement Options• 1 point = Minimal
• 2 points = Limited
• 3 points = Multiple
• 4 points or more = Extensive

Amount or complexity of data reviewed• Review and/or order of clinical lab tests =1 point (max)
• Review and/or order radiology tests =1 point (max)
R i d/ d 90000 i t t 1 i t ( )• Review and/or order 90000 series tests =1 point (max)
• Discussion of test results w/performing physician =1 point
• Decision to obtain old records and/or obtain history Decision to obtain old records and/or obtain history from someone other than the patient =1 point
• Review and summarization of old records and/or obtaining history from someone other than h i d/ di i f i h the patient and/or discussion of case with
another health care provider =2 points
• Independent visualization of image, tracing or specimen itself (not simply reviewing report) =2 pointsspecimen itself (not simply reviewing report) =2 points


Scoring the Amount or Complexity of Data ReviewedReviewed• 1 point = Minimal
• 2 points = Limited
• 3 points = Moderate
• 4 points or more = Extensive

Table of RiskPresenting Problem(s) Diagnostic Proc.Ordered Management Option(s)
SelectedLevel of Risk
One self limited or minor problem e.g. cold insect bite tinea corporis
Lab tests req. venipuncture, chest X-rays EKG-EEG UA
Rest
G lMinimalcold, insect bite, tinea corporis. chest X rays, EKG EEG, UA,
Ultrasound, e.g. echo, KOH prep.
Gargles
Elastic bandages
Superficial dressings
2 or more self-limited or minor problems
Physiologic tests not under stress
OTC drugs
Minor surg no risksLowproblems
1 stable chronic illness
Acute uncomp illness or inj
stress
Non-cardiovascular imaging
Superficial needle biopsies
Minor surg no risks
PT/OT
IV fluids no additives
1 or more chronic illnesses w/ mild exacerbation
Physiologic tests under stress
Diagnostic endoscopies
Minor surg w/ risks
Elective major surgModerateexacerbation
2 or more stable chronic illnessesDiagnostic endoscopies
Deep needle biopsies
Elective major surg
Rx drug manage
IV fluid w/ additives
1 or more chronic illnesses w/ severe exacerbation
Cardiovascular imaging
Cardiac EP studies
Elec. major surg w/ risks
Emerg major surgHighexacerbation
Acute or chronic illness w/ threat to life/limb
Cardiac EP studies
Diagnostic endo w/risks
Discography
Emerg major surg
Parenteral controlled Rx
g
**** This is an abbreviated Table of Risk. Use Medicare guidelines for full Table of Risk


Scoring the Table of Risk
• The highest level of risk from any column is the level to chooselevel to choose.

Scoring the Overall MDM
Number Diagnoses or Management
Options
Amount or Complexity of
Data ReviewedRisk MDM Level
p
Minimal Minimal Minimal Straightforward
Limited Limited Low Low
Multiple Moderate Moderate Moderate
Extensive Extensive High High
Circle the score for each area of the MDM. Two (2) out of three (3) must meet or exceed the level chosen.


History
• The history portion of the chart is made up of four (4) componentsfour (4) components▫ Chief Complaint (CC)▫ History of Present Illness (HPI)History of Present Illness (HPI)▫ Review of Systems (ROS)▫ Past, Family and/or Social History (PFSH)
• The HPI, ROS and PFSH must all meet or exceed the scoring for the overall level chosen f h i i f h hfor the History portion of the chart.

Chief Complaint (CC)
• Every patient visit needs to list a CC.The CC is a concise statement describing the • The CC is a concise statement describing the symptom, problem, condition, diagnosis, provider recommended return or other factor provider recommended return or other factor that is the reason for the encounter.

Scoring the CC
• Per Medicare’s DG there is no “scoring” of the CC although the guidelines do state that the CC CC although the guidelines do state that the CC needs to be present.

History of Present Illness (HPI)
• The HPI is a chronological description of the development of the patient’s present illness from development of the patient s present illness from the first sign and/or symptom or from the previous encounter to the present.previous encounter to the present.

HPI Cont’d
• Per Medicare DG the HPI includes:▫ Location ▫ Location ▫ Quality ▫ Severity Severity ▫ Duration ▫ Timing ▫ Context ▫ Modifying factors
d d▫ Associated signs and symptoms.

Scoring the HPI
• Count the number of elements the provider documented for the HPIdocumented for the HPI.
▫ One (1) to three (3) elements constitutes a Brief One (1) to three (3) elements constitutes a Brief HPI
▫ Four (4) or more elements constitutes an Extended HPI


Review of Systems (ROS)
• A ROS is an inventory of the body systems obtained through a series of questions seeking to obtained through a series of questions seeking to identify signs and/or symptoms which the patient may be experiencing or has experienced.
h b b i d b ill ff b• The ROS may be obtained by ancillary staff or by a form the patient fills out (this may also be obtained by Medical Students.)obtained by Medical Students.)
• It must be evidenced that it was reviewed by the provider and any information supplementing or
fi i h b d dconfirming the ROS must be documented.

ROS Cont’d
▫ Constitutional ▫ Musculoskeletal
Per Medicare DG the following systems are recognized:
▫ Eyes ▫ Ears, nose, mouth,
h
▫ Integumentary▫ Neurological
throat ▫ Cardiovascular ▫ Respiratory
▫ Psychiatric ▫ Endocrine
H t l i /L h ti ▫ Respiratory ▫ Gastrointestinal ▫ Genitourinary
▫ Hematologic/Lymphatic ▫ Allergic/Immunologic
Genitourinary

ROS Cont’d
• If a template is used to document the ROS, each box must be individually marked and all positive box must be individually marked and all positive systems must be commented on.
• When documenting the patient record, the statement “all other systems reviewed and negative” is considered a complete ROS after negative is considered a complete ROS after commenting on the systems with positive responses. The statement “non contributory” is
ffi i d i fnot sufficient documentation of a ROS.
Scoring the ROS
• Count the number of elements documented in the ROSthe ROS.▫ One (1) element is a Problem Pertinent ROS▫ Two (2) to nine (9) elements is an Extended ROSTwo (2) to nine (9) elements is an Extended ROS▫ Ten (10) or more elements is a Complete ROS


Past, Family, Social History (PFSH)
• The PFSH consists of a review of three areas:▫ Past history (the patient’s past experiences with ▫ Past history (the patient s past experiences with
illnesses, surgeries, injuries, etc) ▫ Family history (the patient’s review of significant y y ( p g
family medical events) ▫ Social history (an age appropriate review of past
d i i i )and current activities)

PFSH Cont’d
• The PFSH may be obtained by ancillary staff or through a form the patient fills out (this too may through a form the patient fills out (this too may be obtained by a Medical Student.)
• It must be evidenced that it was reviewed by the provider and any information supplementing or p y pp gconfirming the PFSH must be documented.

Scoring the PFSH
• Count the number of elements documented for the PFSH▫ One (1) element from any of the three (3) areas
constitutes a Pertinent PFSH▫ One (1) element from two (2) of the three (3) areas
tit t C l t PFSH fconstitutes a Complete PFSH for:established patients, ED, subsequent nursing facility care, domiciliary care (est. pt),or home care (est. pt)
▫ One (1) element from all of the three (3) areas ▫ One (1) element from all of the three (3) areas constitutes a Complete PFSH for:
new patients, hospital observation services, hospital inpatient services initial care, consults, comprehensive inpatient services initial care, consults, comprehensive nursing facility evals, domiciliary care (new pt) or home care (new pt)


Scoring the Overall HistoryHPI ROS PFSH Overall History
Brief N/A N/A Problem Focused
Brief Problem Pertinent N/A Expanded Problem Focused
Extended Extended Pertinent DetailedExtended Extended Pertinent Detailed
Extended Complete Complete Comprehensive
Circle the score in each column.
All three (3) must meet or exceed the level of service chosen.( )


ExamMedicare’s DG recognize the following body areas and organ systems:
▫ Head, including the face ▫ Neck ▫ Chest, including the breasts &
▫ Constitutional (e.g. vitals, appearance)
▫ Eyes axillae
▫ Abdomen ▫ Genitalia, groin, buttocks
▫ Ears, nose, mouth and throat ▫ Cardiovascular ▫ Respiratory
▫ Back, including spine ▫ Each extremity
▫ Gastrointestinal

Exam Cont’d
▫ Genitourinary ▫ Musculoskeletal ▫ Musculoskeletal ▫ Skin ▫ Neurologic Neurologic ▫ Psychiatric ▫ Hematologic/lymphatic/immunologic
Exam Cont’d
• Specific abnormal and relevant negative findings of the affected area should be documentedof the affected area should be documented.
• A notation of abnormal without elaboration is not sufficient.not sufficient.
• A brief statement or notation noting negative or normal is sufficient for unaffected/asymptomatic areas.

Scoring the Exam
• Count the number of elements documented as examined by the provider:by p▫ Problem Focused Examination - limited exam of
affected body area or organ system (1)▫ Expanded Problem Focused Examination - limited ▫ Expanded Problem Focused Examination - limited
exam of affected body area or organ system and other symptomatic related organ systems (2-7)
▫ Detailed extended exam of affected body areas or ▫ Detailed - extended exam of affected body areas or organ systems and other symptomatic or related organ systems (2-7)C h i l lti t ▫ Comprehensive - a general multi-system exam or complete exam of a single organ system (8 or more)


Scoring the Overall Chart• New patients▫ 3 out of 3 areas must meet or exceed the level of service chosenE t bli h d ti t• Established patients▫ 2 out of 3 areas must meet or exceed the level of service chosen
• Consultations▫ 3 out of 3 areas must meet or exceed the level of service chosen 3 out of 3 areas must meet or exceed the level of service chosen
• Initial Observation Services▫ 3 out of 3 areas must meet or exceed the level of service chosen
• Initial Hospital Servicesp▫ 3 out of 3 areas must meet or exceed the level of service chosen


New Patient Office Visits
• New Patient – A new patient is a patient who has not had a face to face encounter in the last threenot had a face to face encounter in the last threeyears:▫ By the same provider By the same provider
▫ By a provider of the same specialty in the same group
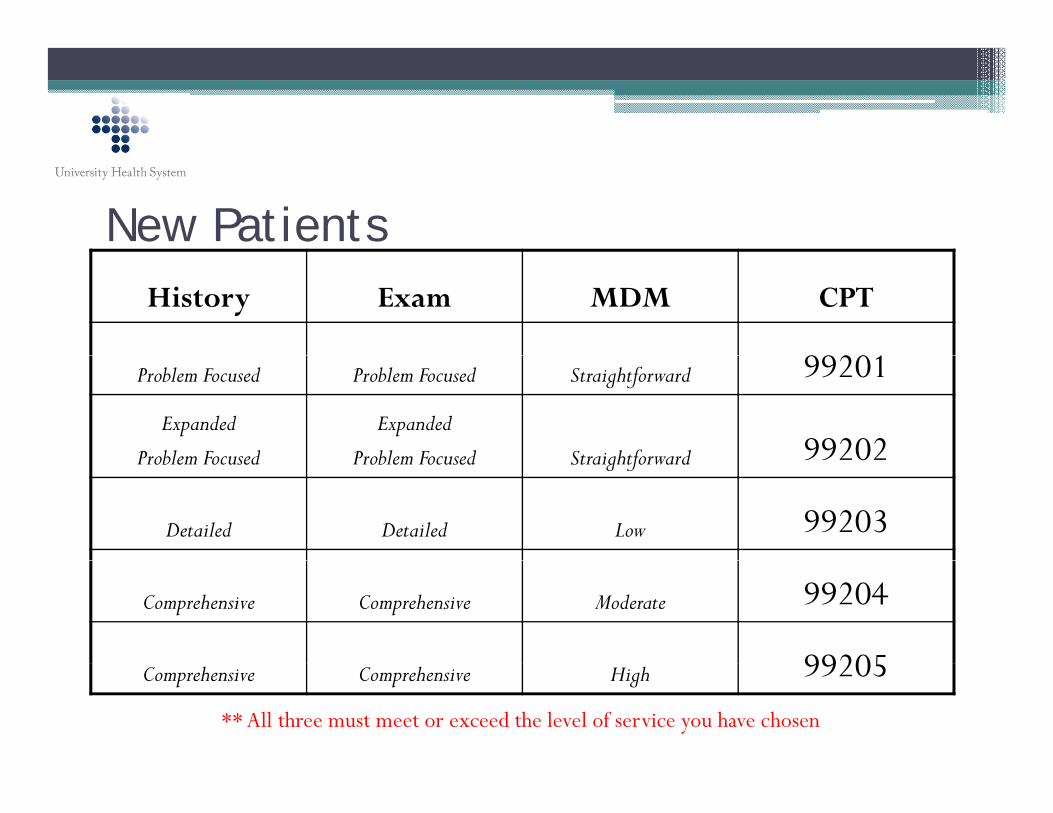
New PatientsHistory Exam MDM CPT
99201Problem Focused Problem Focused Straightforward 99201
Expanded
Problem Focused
Expanded
Problem Focused Straightforward 99202Problem Focused Problem Focused Straightforward 99202
Detailed Detailed Low 99203
Comprehensive Comprehensive Moderate 99204
99205Comprehensive Comprehensive High 99205** All three must meet or exceed the level of service you have chosen


Established PatientsHistory Exam MDM CPT
NA NA NA 9921199211
Problem Focused Problem Focused Straightforward 99212
Expanded Problem Focused
Expanded Problem Focused
Low 99213
Detailed Detailed Moderate 9921499214
Comprehensive Comprehensive High 99215
** Two out of the three elements must meet or exceed the level of service you have chosen

Consultations
• A consultation is distinguished from a visit because it is done at the request of a referring because it is done at the request of a referring provider and the consultant prepares a report of his/her findings that is provided to the referring his/her findings that is provided to the referring provider for his or her use in treatment of the patient.

The three “R”s of a Consultation
• Request - Documentation of the Request for consultation from the referring provider consultation from the referring provider
• Reason - The Reason for the consult which must • Reason The Reason for the consult which must be medically reasonable and necessary
• Report - The written Report by the consultant which was provided back to the referring physician


Outpatient Consultations
History Exam MDM CPT
Problem Focused Problem Focused Straightforward 99241
Expanded Problem Expanded Problem Straightforward 99242pFocused
pFocused
g f 99242
Detailed Detailed Low 99243
Comprehensive Comprehensive Moderate 99244
Comprehensive Comprehensive High 99245
**Three out of the three must meet or exceed the level of service you have chosen
Comprehensive Comprehensive High 99245

Inpatient ConsultationsHistory Exam MDM CPT
bl d bl d h f dProblem Focused Problem Focused Straightforward 99251
Expanded Problem Focused
Expanded Problem Focused
Straightforward 99252Focused Focused
Detailed Detailed Low 99253
Comprehensive Comprehensive Moderate 99254
Comprehensive Comprehensive High 99255
**Three out of the three must meet or exceed the level of service you have chosen


Initial Hospital Observation Services
History Exam MDM CPT
Detailed/ Comprehensive
Detailed/ Comprehensive
Straightforward/ Low
99218p p
Comprehensive Comprehensive Moderate 99219
Comprehensive Comprehensive High 99220
**Three out of the three must meet or exceed the level of service you have chosen

Initial Hospital Services
History Exam MDM CPTy
Detailed/ C h
Detailed/ C h
Straightforward/ L
99221Comprehensive Comprehensive Low
Comprehensive Comprehensive Moderate 99222p p
Comprehensive Comprehensive High 99223
**Three out of the three must meet or exceed the level of service you have chosen
p p g


Subsequent Hospital Services
History Exam MDM CPTy
Detailed/ C h i
Detailed/ C h i
Straightforward/ L
99231Comprehensive Comprehensive Low
Comprehensive Comprehensive Moderate 99232p p
Comprehensive Comprehensive High 99233
**Two out of the three must meet or exceed the level of service you have chosen

Observation or Inpatient Care Services
History Exam MDM CPT
Detailed/ Comprehensive
Detailed/ Comprehensive
Straightforward/ Low
99234p p
Comprehensive Comprehensive Moderate 99235
Comprehensive Comprehensive High 99236
**Three out of the three must meet or exceed the level of service you have chosen
These codes are for patients that are admitted and discharged on the same day.

Time Based Evaluation & Management ServicesServices• Time may be the controlling factor when
determining a level of service In order to use determining a level of service. In order to use time as the controlling factor, the provider must document the following:document the following:▫ The total face-to-face time spent with the patient▫ That over 50% of that time was spent in
counseling or coordination of care for the patient▫ The nature or content of the counseling and
coordination of carecoordination of care

Time Based Evaluation & Management Services cont’dServices cont d• Medicare expects that coding based on time is
the exception to the rule not a regular the exception to the rule not a regular occurrence.
• In order to determine what level of service was In order to determine what level of service was provided based on time, look at the average time spent for that level of service.
• For example, the average time spent (according to the CPT manual) for a 99214 is 25 minutes.

Now that I know how to document to Now that I know how to document to support coding based on time. Where can I find the average time spent for each visit?find the average time spent for each visit?


Thank You
Please click here to take h f hthe quiz for this course.