em waves for therapy
TRANSCRIPT

8/11/2019 EM Waves for Therapy
http://slidepdf.com/reader/full/em-waves-for-therapy 1/33
ELECTROMAGNETIC WAVES FOR THERAPY 271
11 Electromagnetic Waves for TherapyWe saw, in chapter 9, that Maxwell's equations predict that whenever charges areaccelerated electromagnetic waves are produced. In this chapter we consider theelectromagnetic waves used in therapy: how they are produced and why they areuseful to physiotherapists.
Ultraviolet and infrared radiation have low penetration depth but areuseful for therapy inapplications other thandiathermy.
Three main kinds of electromagnetic wave are used in therapy: microwaves, infraredand ultraviolet radiation. Of these, only microwaves are able to penetrate tissuesignificantly and so be classed as diathermic.
The different therapeutic applications of these radiations arise from their differingeffect on tissue. These effects, in turn, are determined by the wavelength (or frequency) of the waves. Before considering the effect on tissue we examine the wayin which each kind of electromagnetic wave is produced: this gives a first insight into
their physical and physiological effects.
PRODUCTION OF WAVES AROUND OPTICAL FREQUENCIES
In what follows we consider the way in which infrared and ultraviolet radiation areproduced for therapy. Both kinds of radiation are normally produced by similar apparatus: more fundamental are the similarities in the molecular processesinvolved.
Production of Ultraviolet Radiation
When discussing ultraviolet radiation it is a commonconvention to talk in terms of wavelength rather than
frequency.
Electromagnetic waves with frequencies from 0.75 x 1015 Hz to 3.00 x 1015 Hz areclassified as ultraviolet radiation (see figure 9.5). Their frequencies are above thoseof visible light and below those of X-rays. Ultraviolet radiation has wavelengthsbetween 400 nm and 100 nm. The wavelengths used in therapy are restricted to thehigh end of this range: 190 nm to 400 nm, as wavelengths less than 190 nm are
strongly absorbed in air.
By international convention the ultraviolet spectrum is divided into three regions.
to table of contents

8/11/2019 EM Waves for Therapy
http://slidepdf.com/reader/full/em-waves-for-therapy 2/33
ELECTROMAGNETIC WAVES FOR THERAPY 272
When deciding whether to
use UV for therapy, theclinician must, as with all interventions, weigh thebenefits against the risks.
Indeed, we have evidence for
gaseous conduction at normal temperature and pressure with every lightning flash in a thunderstorm.
These are:* UV-A: wavelengths between 400 nm and 315 nm
* UV-B: wavelengths between 315 nm and 280 nm
* UV-C: wavelengths between 280 nm and 100 nm.
UV-C radiation is used to sterilize things when you don't want to boil them. This isbecause UV-C, at sufficiently high intensities, destroys bacteria. It does this bydamaging the bacterial DNA. UV-C exposure will also damage human cells in thesame way and can produce malignancies (cancer). UV-C and, in fact, UV-B and -Ahave an extremely low penetration depth, so most of the absorption of UV is by theskin. The low penetration depth of UV is the reason that UV exposure (in particular,exposure to UV-C) is associated with skin cancer.
The usual means of producing ultraviolet light is by the passage of an electric current
through an ionized gas or vapour. Gases at normal temperature and pressure arevery poor conductors. They can, however, be made to conduct at high temperature or low pressure in the presence of a sufficiently strong electric field.
Ultraviolet radiation for therapeutic application is usually produced by current flowthrough mercury vapour. Mercury under reduced pressure is contained in a sealedenvelope of quartz or special glass with an electrode inserted in each end. The deviceis similar to the strip-lights (fluorescent lights) commonly found in the
kitchen at home and the office or tutorial room. The difference is that UVlights operate at lower pressures than household or business lights. Thismeans that more energy is required to initiate conduction and charges areaccelerated over greater distances so that when they collide, the energyrelease is larger and, as a result of the higher energies, UV rather thanvisible light is produced. The arrangement used with a mercury vapour lamp is shown in figure 11.1.
Figure 11.1Schematic diagram of a mercury vapour lamp.
to table of contents
8/11/2019 EM Waves for Therapy
http://slidepdf.com/reader/full/em-waves-for-therapy 3/33
8/11/2019 EM Waves for Therapy
http://slidepdf.com/reader/full/em-waves-for-therapy 4/33
ELECTROMAGNETIC WAVES FOR THERAPY 274
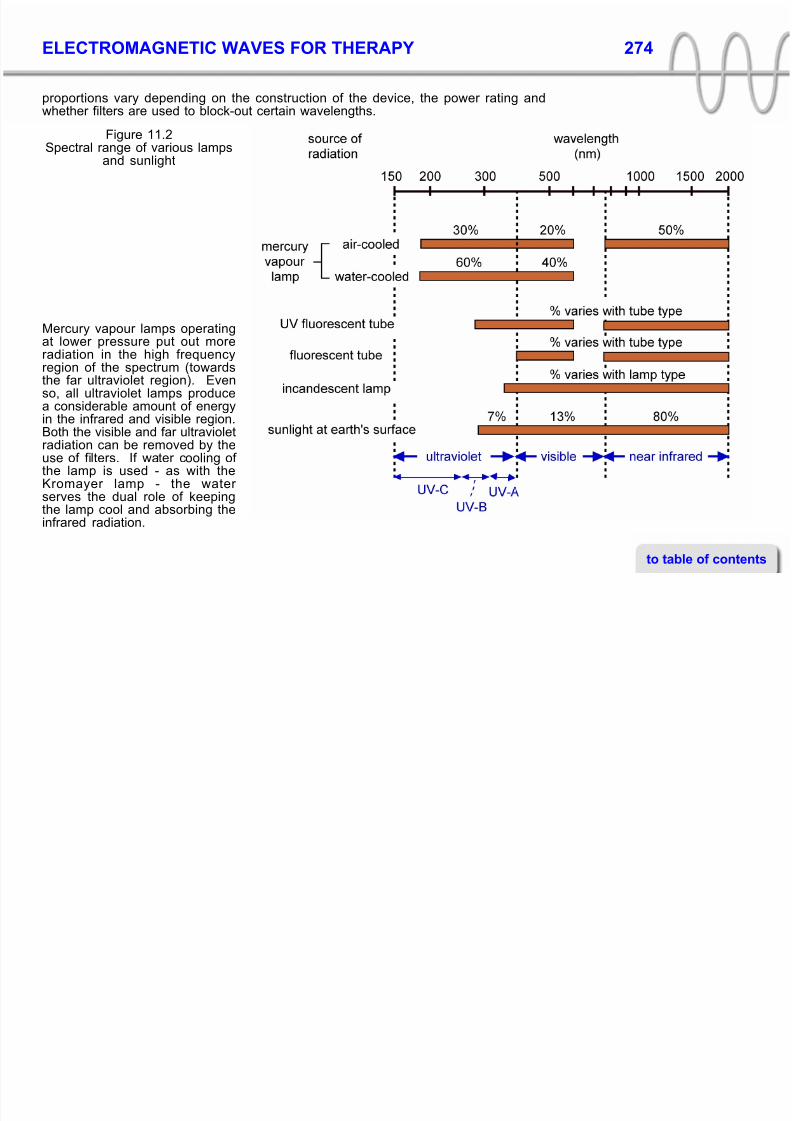
proportions vary depending on the construction of the device, the power rating andwhether filters are used to block-out certain wavelengths.
Figure 11.2Spectral range of various lamps
and sunlight
Mercury vapour lamps operatingat lower pressure put out moreradiation in the high frequencyregion of the spectrum (towardsthe far ultraviolet region). Evenso, all ultraviolet lamps producea considerable amount of energyin the infrared and visible region.Both the visible and far ultravioletradiation can be removed by theuse of filters. If water cooling of the lamp is used - as with theKromayer lamp - the water serves the dual role of keepingthe lamp cool and absorbing theinfrared radiation.
to table of contents
8/11/2019 EM Waves for Therapy
http://slidepdf.com/reader/full/em-waves-for-therapy 5/33

8/11/2019 EM Waves for Therapy
http://slidepdf.com/reader/full/em-waves-for-therapy 6/33
ELECTROMAGNETIC WAVES FOR THERAPY 276
Carbon arcs are rarely used today in physiotherapy departments: they have beenlargely superseded by mercury vapour lamps which are cleaner and easier to operate.
Production Of Infrared Radiation
Infrared radiation - sometimes referred to as radiant heat - is produced (andabsorbed) by all materials at temperatures above absolute zero.
Absorption of infrared radiation results in changes in molecular and atomic motion of a material; the continuous agitation and changes in the motion of molecules, andwithin molecules also results in the emission of infrared radiation. For example,chemical bonds in molecules can absorb energy and 'stretch', changing the bondlength and thus the energy of the bonding electrons. When the bond reverts to itsoriginal size, infrared radiation is produced at a frequency characteristic of the bond.
Any object will be emitting and absorbing infrared radiation on an ongoing basis. Whether emissionoutweighs absorptiondepends on the temperatureof the object relative to its
surroundings.
Any molecule may, as a result of absorption of radiation or collision, change its stateof rotation or vibration, or both simultaneously. On changing to a rotation or vibrationstate of lower energy, infrared radiation is produced. A particular kind of molecule hasvery many possible states of rotation and vibration and therefore many options for going from one state to some other.
At a given temperature a body will emit a continuous spectrum of radiation - themaximum intensity occurring at a particular frequency but with significant intensitiesextending over a wide range of frequencies. The frequency of maximum production of radiation is directly proportional to the absolute temperature of the source. Sincewavelength and frequency are inversely related (by equation 9.1, v = f.λ), it follows thatthe wavelength of maximum production of radiation is inversely proportional to theabsolute temperature of the source. (This is called Wien's Law).
As the source of radiation becomes progressively warmer, the wavelength of
maximum emission becomes progressively shorter: thus an iron bar turns from blackto 'red-hot' to 'white hot' to 'blue hot' as its temperature increases. In the black to red-hot temperature range both near infrared (770 to about 4000 nm) and far infrared
to table of contents

8/11/2019 EM Waves for Therapy
http://slidepdf.com/reader/full/em-waves-for-therapy 7/33

8/11/2019 EM Waves for Therapy
http://slidepdf.com/reader/full/em-waves-for-therapy 8/33
ELECTROMAGNETIC WAVES FOR THERAPY 278
From a penetration depth of a few millimetres at 1200 nm there is a decrease to about0.1 mm at 3000 nm. Wavelengths above 3000 nm are absorbed by moisture on thesurface of the skin. The trend does not continue indefinitely and we find that in the far infrared region from 10 000 to 40 000 nm, the penetration depth increases to severalcentimetres. In effect, the tissues become much more transparent.
Figure 11.3
Penetration of radiation into skin in theinfrared to ultraviolet region of the
electromagnetic spectrum
Over the whole of the near infrared spectrum andup to about 20 000 nm in the far infrared, reflectionis minimal. Close to 95 per cent of energyincident perpendicular to the skin is absorbed -only about 5 per cent is reflected. To a reasonableapproximation then, we can consider infraredradiation to be wholly absorbed by tissue.
The region of the ultraviolet spectrum of interest intherapy extends from about 180 nm to 390 nm.From figure 11.3 we can see that most of thisradiation is absorbed in the epidermis. In theregion from 220 nm to 300 nm about 5 to 8 per cent of incident radiation is reflected. Thereflectance increases to about 20 per cent at 390
nm. Within the range there are regions of very lowreflectance corresponding to specific absorptionby particular molecules in the skin - for example,
to table of contents

8/11/2019 EM Waves for Therapy
http://slidepdf.com/reader/full/em-waves-for-therapy 9/33
ELECTROMAGNETIC WAVES FOR THERAPY 279
nucleic acids absorb strongly at frequencies between 250 and 260 nm and at 280 nm.
Heating by Infrared Radiation
The physiological effects ofinfrared radiation differ fromthose of other forms of
heating (e.g. shortwavediathermy) only in thelocation of heat production.
From the foregoing discussion it is clear that the major effect of infrared radiation isthermal: to increase the temperature of cutaneous tissue. The penetration depth isvery small but some heat will be transferred to the subcutaneous tissues via thecapillaries.
The main effects of treatment are:
* An increase in metabolic rate in the superficial tissues. This is the direct effect of temperature on the rate of chemical reactions generally. As a result there will bean increased demand for oxygen and an increased output of waste products.
* Dilatation of capillaries and arterioles due directly to the heating and also as a
reflex reaction to the presence of increased concentrations of metabolites. Theflow of blood to the superficial tissues is thus increased producing a reddeningof the skin (erythema) and an increased supply of oxygen and nutrients. Theerythema produced by infrared therapy, unlike that resulting from ultraviolettreatment, appears quite rapidly and begins to fade soon after treatment ceases.
The effects of infrared radiation are not damaging unless the temperatureelevation is too high.
* Sensory sedation. Mild heating has a 'sedatory' effect on sensory nerves and isthus useful for the relief of pain.
* Muscle spasm relief. This results from both the effect of heat on nerve fibres andthe direct effect of heat which is transferred to muscle from the superficialtissues.
Effects of Ultraviolet Radiation
The effects of ultraviolet radiation are mainly non-thermal and due to cellular damage
and protective responses. While damage might seem an undesirable consequence,there are therapeutic benefits of treatment. Five principal effects of therapeuticsignificance are found to result from treatment with ultraviolet radiation:
to table of contents
8/11/2019 EM Waves for Therapy
http://slidepdf.com/reader/full/em-waves-for-therapy 10/33

8/11/2019 EM Waves for Therapy
http://slidepdf.com/reader/full/em-waves-for-therapy 11/33
ELECTROMAGNETIC WAVES FOR THERAPY 281
The degree of erythema production is used to characterize the dose in ultra-violettherapy using UV-B fluorescent tubes or mercury vapour lamps. The reaction isgraded into four levels:
* A first-degree erythema is a slight reddening of the skin which takes from six toeight hours to develop. The erythema has faded in about twenty four hoursleaving the skin apparently unchanged. A minimum erythema dose (MED) is also
a slight reddening which takes from six to eight hours to develop but in this casethe erythema is still just visible at twenty four hours.
* A second-degree erythema is a more marked reddening of the skin (resemblingmild sunburn). There is a slight soreness. The reaction fades in about two daysand is followed by pigmentation. After one or two weeks desquamation (peeling,usually powdery) occurs.
* A third-degree erythema resembles severe sunburn. The skin may begin toshow the effects as soon as two hours after treatment. The reaction is severe andthe skin becomes hot, sore and oedematous. Effects subside gradually over several days and the skin often peels off in sheets or flakes.
The counter-irritation effect of a fourth degree erythema has
been used in the past as aquick and effective method of relieving pain from joints and other deep structures indegenerative arthritis and rheumatic conditions.
* A fourth-degree erythema is similar to a third-degree reaction but exudation andoedema are so marked that blisters form. Production of a third or fourth degreeerythema in a small localized area results in a counter-irritation effect.
Dose characterization in this way is appropriate for sources which produce anappreciable proportion of UV-B radiation. When using UV-A fluorescent tubes,dosage can not be assessed in this way as erythema production is minimal except atextremely high dose levels. In practice this is not a problem as the principal use of UV-A is in conjunction with a photosensitizing drug, 8-methoxy-psoralen, for thetreatment of psoriasis. For psoralen - UV-A, therapy a special procedure is used for
dose characterization. The procedure is described in chapter 12.
to table of contents

8/11/2019 EM Waves for Therapy
http://slidepdf.com/reader/full/em-waves-for-therapy 12/33

8/11/2019 EM Waves for Therapy
http://slidepdf.com/reader/full/em-waves-for-therapy 13/33
ELECTROMAGNETIC WAVES FOR THERAPY 283
production of electromagnetic waves (chapter 9) which are beamed by the reflector.
Figure 11.4Schematic diagram: microwave
apparatus
The frequency of the microwaves is equal to the frequency of the AC produced by themagnetron. This is determined by the physical construction of the magnetron and isfixed during manufacture.
A number of differently shaped antennas and reflectors may be used for directing thebeam. Each gives a different beam shape though none gives a perfectly uniformbeam. To obtain a collimated uniform beam (like a searchlight) would require aparabolic reflector with a point source of radiation as shown in figure 11.5(a). If a pointsource of radiation is placed at the focus of the parabola the beam emerges with auniform cylindrical shape as shown.
In the case of microwaves used by physiotherapists, the most common frequency is2450 MHz and the wavelength in air is 12 cm. The source of radiation is normally ahalf-wave antenna; a rod shaped conductor about 6 cm long. Placed in a smallparabolic reflector the antenna would produce a highly non-uniform beam (figure11.5b). To produce a reasonably uniform beam the antenna would need to be placedin a reflector very much larger than its 6 cm length. A reflector with a focal length of a
to table of contents

8/11/2019 EM Waves for Therapy
http://slidepdf.com/reader/full/em-waves-for-therapy 14/33
ELECTROMAGNETIC WAVES FOR THERAPY 284
metre or more and a diameter of several metres would be needed - producing abeam which is metres in diameter.
Figure 11.5(a) a uniform beam from a parabolic reflector and
point source, (b) a non-uniform beam from aparabolic reflector and extended source
For therapeutic application, a microwave beam only 10to 20 cm in diameter is desirable, in order to localize
the microwave energy. Reflectors 10 or 20 cm indiameter with antennas about 6 cm in length cannotproduce a uniform beam but can be designed toproduce a diverging beam. The beams obtained fromreflectors presently used in therapy divergeconsiderably - the wave intensity decreasing rapidlywith distance from the reflector. The reflectors must bedesigned this way: if a less divergent beam is
produced part of the beam will be divergent, part will beparallel and part focussed at some point in front of thereflector as in figure 11.5(b). This has the obvious riskof producing a local hot-spot in the patient's tissue andcausing tissue damage.
Microwave applicators are available to produce a number of beam patterns. Thepattern is not obvious from inspection of the shape of the reflector but themanufacturers do supply this information.
to table of contents

8/11/2019 EM Waves for Therapy
http://slidepdf.com/reader/full/em-waves-for-therapy 15/33
ELECTROMAGNETIC WAVES FOR THERAPY 285
EFFECT OF MICROWAVES ON TISSUEThe penetration depth of microwaves (table 9.1) indicates that the waves are useful for diathermy.
The three factors determining the depth efficiency of waves generally are (chapter 9)the penetration depth (δ) of the waves in a particular tissue and the extent of reflectionand refraction at tissue interfaces.
Considering first penetration depth, we make the observation that tissues with highvalues of dielectric constant (ε) and conductivity (σ) absorb electromagnetic radiationmore rapidly than tissues with low values of ε and σ. The reasons were given inchapter 9 previously. Values of ε and σ are significantly different at microwavefrequencies to those appropriate to shortwave diathermy at 27 MHz (table 6.2). Table11.1 lists the values applicable at microwave frequencies.
Notice that fatty tissue and bonemarrow have quite similar values of ε and σ - this explains why thepenetration depth of microwaves(table 9.1) is almost the same inboth tissues. The relatively highvalues of ε and σ for muscle resultin a greater rate of microwave
absorption and hence a lower value for the penetration depth inthis tissue.
The extent of reflection at aninterface is calculated fromequation 9.5: it is determined by themismatch in impedance of the
tissues. Since we are talking aboutelectromagnetic waves the imped-
Table 11.1
Dielectric constant and conductivity of tissueat microwave frequencies.
to table of contents

8/11/2019 EM Waves for Therapy
http://slidepdf.com/reader/full/em-waves-for-therapy 16/33
ELECTROMAGNETIC WAVES FOR THERAPY 286
Clearly if we wish to calculatethe pattern of heating intissue we must take account
of both the penetration depthin each tissue and theamount of reflection and refraction at each tissueinterface. Each factor will have a significant effect onthe heating pattern.
See the chapter by Schwanin: Licht, S H, Therapeutic Heat and Cold, (2nd Edition),
New Haven (1968).
ance of interest is the electrical impedance - determined by the dielectric constant (ε)and conductivity (σ) of the tissue. Reflection of microwaves at the fat/muscle and
muscle/bone interfaces will be pronounced due to the difference in electricalproperties (changed by a factor of 10) on either side of the boundary concerned.
The amount of refraction at an interface is calculated from equation 9.12: it isdetermined by the mismatch in wave velocity of the tissues. The wave velocity in turnis determined by the dielectric constant and conductivity of the tissue.
Because of the large difference in the electrical properties (ε and σ) of air, fatty tissue,muscle and bone, refraction effects will be significant unless the microwave beamstrikes each boundary at a right angle (zero angle of incidence).
The Fraction of Total Energy Absorbed
A knowledge of the dielectric constant and conductivity of each tissue enables us to
calculate the relative rate of heating of each tissue. This information alone does notallow us to predict the actual amount of heat produced since much of the microwaveenergy is reflected at the air/skin interface.
The significant difference in the electrical properties of air (for which ε ≈ 1 and σ ≈ 0)and soft tissue will result in a considerable amount of the energy incident upon theskin being reflected. The total percentage of microwave energy absorbed deeper inthe body tissues and hence converted into heat also depends on the thickness of the
skin/fatty tissue layer. This is because a proportion of the wave energy reflected fromthe fat/muscle interface will penetrate the skin and be re-radiated into the air.
Some decades ago, H. P. Schwan (see Licht (1968)) calculated the percentage of total energy reflected at different frequencies and various thicknesses of skin and fat.His results show that:
* At frequencies less than 1000 MHz, 60 to 70% of the energy is reflected this
almost independently of skin and fat thickness.
to table of contents

8/11/2019 EM Waves for Therapy
http://slidepdf.com/reader/full/em-waves-for-therapy 17/33
ELECTROMAGNETIC WAVES FOR THERAPY 287
* Between 1000 and 3000 MHz reflection depends critically and in a complex wayon tissue thickness. Between 0 and 80% of the energy is reflected.
* Above 3000 MHz around 60% of the energy is reflected - again almostindependently of tissue thickness.
Another practical implicationof the large amount of
reflection is the need to avoid unintentional exposure of body parts (including those of the therapist).
One major implication of the above results is that at a frequency of 2450 MHz theeffective dosage is virtually impossible to determine in a clinical situation, due to the
practical difficulty in establishing skin and fat thickness which may vary considerablyin the treated area. Clearly a frequency above or below the range 1000 to 3000 MHz isto be preferred on these grounds. As we will see in what follows, a lower frequency ispreferable.
The Distribution of Absorbed Energy
We examine now the absorption of the proportion of microwave energy which is not
reflected by the skin or re-radiated. Consider a 2 cm fatty tissue layer adjoiningmuscle tissue. For simplicity we begin by making two assumptions:
* that no bone is present. We will take bone into account in subsequent examples.
* that refraction can be ignored. In other words the angle of incidence is assumedto be zero. Refraction effects will be described separately.
The relative rate of heating can be calculated from the dielectric constant andconductivity of each tissue: the two factors which determine the amount of reflectionand the penetration depth. The method of calculation is described by Schwan (seeLicht (1968)).
Figure 11.6 shows the pattern of heat production for microwaves at the relatively highfrequency of 8500 MHz (wavelength 3.5 cm in air). A standing-wave pattern (seechapter 9) is produced in the fatty tissue: this is because of reflection at the fat/muscle
interface.
to table of contents
8/11/2019 EM Waves for Therapy
http://slidepdf.com/reader/full/em-waves-for-therapy 18/33
ELECTROMAGNETIC WAVES FOR THERAPY 288
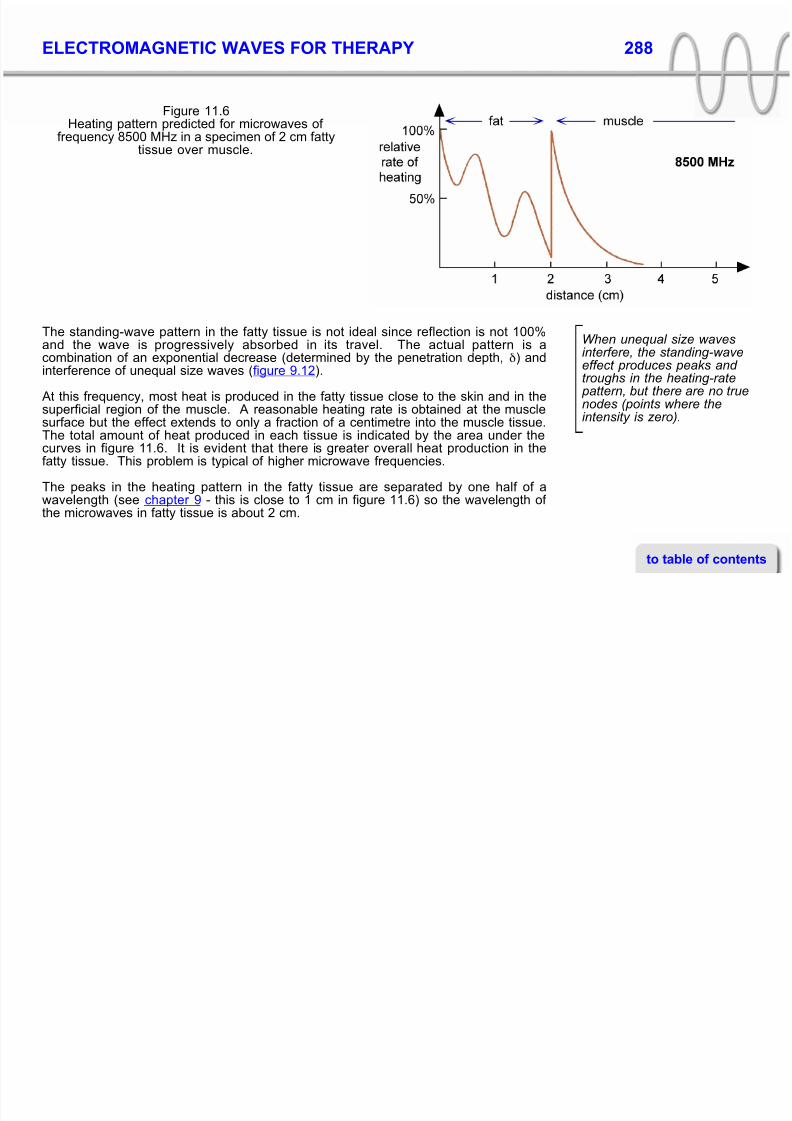
Figure 11.6Heating pattern predicted for microwaves of
frequency 8500 MHz in a specimen of 2 cm fattytissue over muscle.
When unequal size wavesinterfere, the standing-waveeffect produces peaks and troughs in the heating-rate pattern, but there are no true
nodes (points where theintensity is zero).
figure 9.12).
At this frequency, most heat is produced in the fatty tissue close to the skin and in the
superficial region of the muscle. A reasonable heating rate is obtained at the musclesurface but the effect extends to only a fraction of a centimetre into the muscle tissue.The total amount of heat produced in each tissue is indicated by the area under thecurves in figure 11.6. It is evident that there is greater overall heat production in thefatty tissue. This problem is typical of higher microwave frequencies.
The peaks in the heating pattern in the fatty tissue are separated by one half of awavelength (see chapter 9 - this is close to 1 cm in figure 11.6) so the wavelength of the microwaves in fatty tissue is about 2 cm.
The standing-wave pattern in the fatty tissue is not ideal since reflection is not 100%and the wave is progressively absorbed in its travel. The actual pattern is acombination of an exponential decrease (determined by the penetration depth, δ) andinterference of unequal size waves (
to table of contents
8/11/2019 EM Waves for Therapy
http://slidepdf.com/reader/full/em-waves-for-therapy 19/33
ELECTROMAGNETIC WAVES FOR THERAPY 289
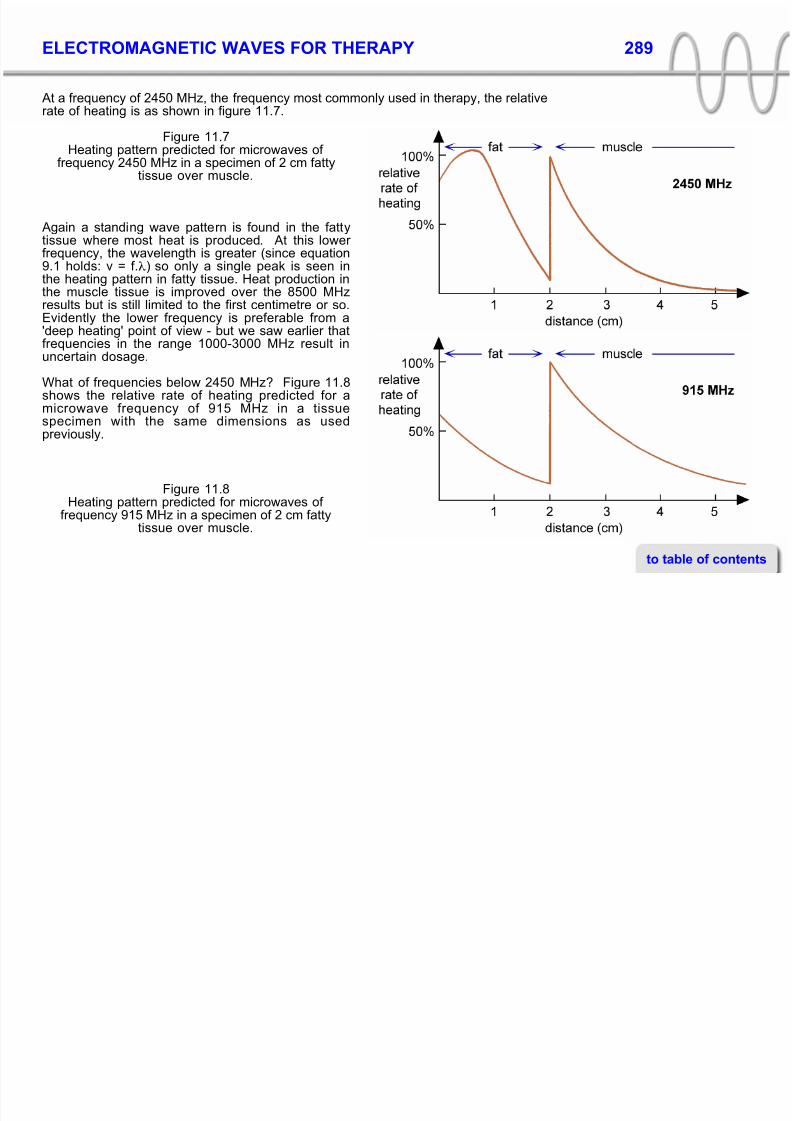
At a frequency of 2450 MHz, the frequency most commonly used in therapy, the relativerate of heating is as shown in figure 11.7.
Figure 11.7Heating pattern predicted for microwaves of
frequency 2450 MHz in a specimen of 2 cm fattytissue over muscle.
Again a standing wave pattern is found in the fattytissue where most heat is produced. At this lower frequency, the wavelength is greater (since equation9.1 holds: v = f.λ) so only a single peak is seen inthe heating pattern in fatty tissue. Heat production inthe muscle tissue is improved over the 8500 MHz
results but is still limited to the first centimetre or so.Evidently the lower frequency is preferable from a'deep heating' point of view - but we saw earlier thatfrequencies in the range 1000-3000 MHz result inuncertain dosage.
What of frequencies below 2450 MHz? Figure 11.8shows the relative rate of heating predicted for a
microwave frequency of 915 MHz in a tissuespecimen with the same dimensions as usedpreviously.
Figure 11.8
Heating pattern predicted for microwaves of frequency 915 MHz in a specimen of 2 cm fattytissue over muscle.
to table of contents

8/11/2019 EM Waves for Therapy
http://slidepdf.com/reader/full/em-waves-for-therapy 20/33
ELECTROMAGNETIC WAVES FOR THERAPY 290
The wavelength in fatty tissueat 915 Mhz is about 18 cm soa peak and a trough would beseparated by 4.5 cm (onequarter of a wavelength).
At 915 MHz, a standing wave pattern is still produced in the fatty tissue but thewavelength is so large that no peaks are evident.
Figure 11.9 shows the relative rate of heating predicted for a microwave frequency of 434 MHz in the same tissue specimen.
Figure 11.9Heating pattern predicted for microwaves of frequency 434 MHz in a specimen consisting
of 2 cm fatty tissue over muscle.
The depth efficiency of lower frequency microwavesis apparent from figures 11.8 and 11.9. Bothfrequencies give maximum heating in the musclewith much the same decrease in heating rate withdistance into the tissue. The lowest frequency (434MHz) produces least heating of fatty tissue; thedifference being most noticeable near the tissuesurface.
Both frequencies give a heating pattern which issuitable for diathermy and dosage is reasonablypredictable.
The heating of the fatty tissue surface with 915 MHz microwaves can be compensatedfor by using a contact applicator with surface cooling. The microwave director (applicator) is designed to be used in direct contact with the patient. Cooling air isblown through the applicator and on to the patients' skin during treatment in order tominimize the temperature elevation of superficial tissues.
to table of contents

8/11/2019 EM Waves for Therapy
http://slidepdf.com/reader/full/em-waves-for-therapy 21/33
ELECTROMAGNETIC WAVES FOR THERAPY 291
Figure 11.10Heating pattern predicted for a microwave
frequency of 2450 MHz in a tissue combinationof 2 cm fat, 2 cm muscle and 2 cm bone.
Figure 11.11Heating pattern predicted for a microwave
frequency of 915 MHz in a tissue combinationof 2 cm fat, 2 cm muscle and 2 cm bone.
When we consider the three-layer system of fat/muscle/bone we predict reflection at boththe fat/muscle interface and at themuscle/bone interface. In consequence acomplex heating pattern is produced in boththe fat and muscle tissue. Figures 11.10,11.11 and 11.12 show the patterns predictedfor frequencies of 2450 MHz, 915 MHz and
434 MHz respectively. Tissue dimensions arethe same as those chosen to illustrate theheating pattern for ultrasound (figures 10.6and 10.7).
to table of contents

8/11/2019 EM Waves for Therapy
http://slidepdf.com/reader/full/em-waves-for-therapy 22/33
ELECTROMAGNETIC WAVES FOR THERAPY 292
Figure 11.12Heating pattern predicted for a microwave
frequency of 434 MHz in a tissue combinationof 2 cm fat, 2 cm muscle and 2 cm bone.
For each frequency, heat production in bone isminimal. Both 915 and 434 MHz microwavesproduce maximum heating in the muscle layer:the lower frequency having greater depthefficiency. Not too much significance can beattributed to the actual positions of maximaand minima of heat production as these vary
with the tissue dimensions and electricalproperties assumed. The general implicat-ions of the figures are, however, clear:frequencies below 1000 MHz are needed if tissues located beneath a few centimetres of fat are to be effectively heated. For treatingstructures located closer to the skin surface -for example a knee or elbow joint which is not
covered by a thick layer of fat - a frequency of 2450 MHz is adequate, though the dose will besomewhat unpredictable. More deeply locatedstructures - for example, the hip joint - are notheated appreciably at this frequency.
TISSUE GEOMETRY AND REFRACTION EFFECTS
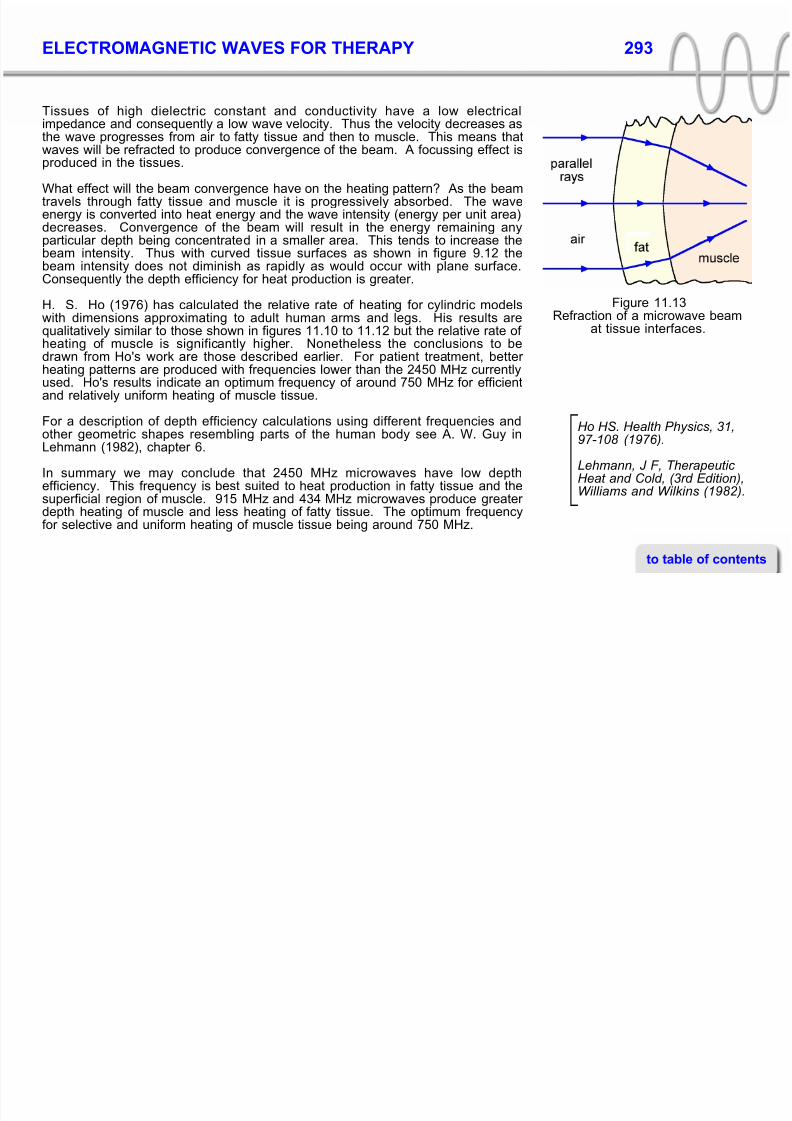
The heating patterns shown in figures 11.6 to 11.12 were calculated ignoringrefraction effects. This is appropriate for a uniform microwave beam incident upon aplane surface with tissues of constant thickness beneath. When microwaves areincident upon a curved surface then, even if the beam is uniform, refraction will occur.This is illustrated in figure 11.13, where reflected waves are omitted for clarity.
The amount of refraction depends on the curvature of the tissue surfaces an theelectrical characteristics of the tissues. When the curvature of the tissues ispronounced, as for example with an arm or leg, the amount of refraction isconsiderable. The smaller is the radius of the limb, the greater is the refraction effect.
to table of contents
8/11/2019 EM Waves for Therapy
http://slidepdf.com/reader/full/em-waves-for-therapy 23/33
ELECTROMAGNETIC WAVES FOR THERAPY 293
Tissues of high dielectric constant and conductivity have a low electricalimpedance and consequently a low wave velocity. Thus the velocity decreases asthe wave progresses from air to fatty tissue and then to muscle. This means thatwaves will be refracted to produce convergence of the beam. A focussing effect isproduced in the tissues.
What effect will the beam convergence have on the heating pattern? As the beam
travels through fatty tissue and muscle it is progressively absorbed. The waveenergy is converted into heat energy and the wave intensity (energy per unit area)decreases. Convergence of the beam will result in the energy remaining anyparticular depth being concentrated in a smaller area. This tends to increase thebeam intensity. Thus with curved tissue surfaces as shown in figure 9.12 thebeam intensity does not diminish as rapidly as would occur with plane surface.Consequently the depth efficiency for heat production is greater.
Figure 11.13Refraction of a microwave beamat tissue interfaces.
H. S. Ho (1976) has calculated the relative rate of heating for cylindric modelswith dimensions approximating to adult human arms and legs. His results arequalitatively similar to those shown in figures 11.10 to 11.12 but the relative rate of heating of muscle is significantly higher. Nonetheless the conclusions to bedrawn from Ho's work are those described earlier. For patient treatment, better heating patterns are produced with frequencies lower than the 2450 MHz currentlyused. Ho's results indicate an optimum frequency of around 750 MHz for efficientand relatively uniform heating of muscle tissue.
Ho HS. Health Physics, 31,97-108 (1976).
Lehmann, J F, Therapeutic Heat and Cold, (3rd Edition),Williams and Wilkins (1982).
For a description of depth efficiency calculations using different frequencies andother geometric shapes resembling parts of the human body see A. W. Guy inLehmann (1982), chapter 6.
In summary we may conclude that 2450 MHz microwaves have low depthefficiency. This frequency is best suited to heat production in fatty tissue and thesuperficial region of muscle. 915 MHz and 434 MHz microwaves produce greater depth heating of muscle and less heating of fatty tissue. The optimum frequencyfor selective and uniform heating of muscle tissue being around 750 MHz.
to table of contents

8/11/2019 EM Waves for Therapy
http://slidepdf.com/reader/full/em-waves-for-therapy 24/33
ELECTROMAGNETIC WAVES FOR THERAPY 294
Microwaves are intrinsically unsuited to heating of bone (see figures 11.10 to 11.12)because of its electrical characteristics: for this reason joints can only be heated whenthe overlying tissue layers are very thin. For heating of deeply located joints,ultrasound or shortwave diathermy would be more effective.
The difference betweenheating rate and rate of
temperature increase, and the relationship betweenthese quantities, wasdiscussed in chapter 7.
As a final point it should be stressed that the graphs shown in figures 11.6 to 11.12show where heat is produced but not the temperature increase in each tissue. The
temperature increase depends on such factors as the specific heat capacity of thetissue and heat transfer within and between tissues and to the bloodstream (seechapter 7).
LASERS
The acronym 'laser' stands for 'light amplification by stimulated emission of radiation'.Lasers are electromagnetic wave amplifiers which can produce beams of electro-
magnetic waves with two special properties:* the beam has very little divergence. It has a pencil-like shape.
* the beam is coherent. That is, all the waves in the beam are of exactly the samefrequency and wavelength and are synchronized with each other.
The divergence of a laser
beam is so small that abeam pointed at the mooncould illuminate a target lessthan a metre across.
The pencil-like beam of the laser means that the wave energy is always concentrated
on the same area: the intensity (which is the energy per unit area) does not decreasedappreciably with distance due to beam-spreading.
Production of a laser beam
Visible light can be produced by excitation of atoms. For example if crystals of acopper salt, such as copper sulphate, are heated in a flame, the flame turns blue.When strontium salts are heated, the flame turns violet. Sodium salts produce a
yellow colouration. This is because electrons in the copper, strontium or sodiumatoms are kicked from their 'ground state' orbitals by the heat energy of the flame and
to table of contents
8/11/2019 EM Waves for Therapy
http://slidepdf.com/reader/full/em-waves-for-therapy 25/33

8/11/2019 EM Waves for Therapy
http://slidepdf.com/reader/full/em-waves-for-therapy 26/33
ELECTROMAGNETIC WAVES FOR THERAPY 296
High power lasers are used to cut steel sheets several
centimetres thick. Muchlower powers are used inmicrosurgery, where focused beams are used to cut tiny regions of tissue.
Lasers are often applied withonly a thin film of plastic separating the laser from theskin surface, so beamdivergence is not important.
beams can be therapeutically beneficial. What has not been established is whether laser beams have any advantage over simpler (and cheaper) torch beams. Nocomparisons have yet been reported.
Beam Intensity
The output of a laser can vary from tens of milliwatts to tens of kilowatts, depending onthe type and the physical construction. Lasers used therapeutically have power levels
between these two extremes. They are typically of relatively low power and intensity.Intensities are normally in the range 1 mW.cm-2 to 50 mW.cm-2.
The beam diameter of the low power lasers used clinically is about 3 mm (an area of about 7 mm2). Thus if the output intensity is, for example, 20 mW.cm-2 and the area is7 mm2 = 0.07 cm2, the power of the beam is 20/0.07 mW ≈ 300 mW or 0.3 W.
By way of comparison, a torch might have a beam 8 cm in diameter (an area about 50
cm2) and use a 12 W light bulb. As far as visible light output is concerned, the bulb isabout 25% efficient (75% of the energy is emitted at infrared frequencies). Hence thepower of the visible light-beam is approximately 3 W. The visible-light beam intensityis 3/50 = 0.06 W.cm-2 or 60 mW.cm-2. The intensity of the infrared component isapproximately 180 mW.cm-2.
A torch beam thus has a similar and, if anything, a higher power and intensity than aclinical laser but is polychromatic. The wave energy is spread over a range of
frequencies. Any clinical significance of the polychromatic/monochromatic differencehas yet to be established.
Beam Divergence
Light from a light bulb can be formed into a pencil-like beam (as in a searchlight) byusing a parabolic reflector but the beam divergence is larger than that of a laser because of the practical difficulty of producing a perfectly shaped reflector. This
difference would be of no clinical significance for beams between a light source andthe patient, a distance of only a few centimetres or tens of centimetres.
to table of contents

8/11/2019 EM Waves for Therapy
http://slidepdf.com/reader/full/em-waves-for-therapy 27/33
ELECTROMAGNETIC WAVES FOR THERAPY 297
Beam Diameter
The beam diameter of the low power lasers used clinically (commonly referred-to as'low level lasers') is about 3 mm (an area of about 7 mm 2 = 0.07 cm2). Aconsequence is that if the area of the skin surface which is to be treated is severalcm2, the beam must be scanned over the area. This means that both the averageintensity and the energy delivered per unit area are reduced. For example, if the areato be treated is 5 cm x 5 cm (25 cm2), the reduction in average intensity and energy
delivered per unit area is 25/0.07 = 3500 times. By contrast, a torch beam wouldilluminate the same area with no reduction in intensity or energy delivered.
Coherence
Coherence is only possibleif waves have identical frequencies. If thefrequencies (and thus, thewavelengths) are different,they cannot stay in-phase.
The light from a light-globe is incoherent. The radiated waves have differentfrequencies (a spread of frequencies about some mean) and the waves are not 'insynch' with each other. Synchronization is impossible because the wavelengths are
different. The coherence of a laser beam is not likely to be of practical significance asbiological tissues are quite inhomogeneous at a microscopic level. This means thatwaves will be scattered and slowed to varying extents so coherence will be lost. Acoherent beam striking the skin surface will be incoherent after traversing a distancethrough tissue of only a few cell diameters. Although coherence is rapidly lost inbiological tissue, the beam remains monochromatic i.e. the waves still have identicalfrequencies.
Since coherence is lost when lasers are beamed through tissue, whether thelight source is a laser or superluminous diodeappears irrelevant.
Producing a coherent beam using diode lasers is technically difficult. Superluminousdiodes are easier to manufacture. These are devices which produce monochromatic,laser-like beams which are non-coherent. It should be noted that some diode 'lasers'used in physiotherapy produce relatively incoherent beams and should more correctlybe described as 'superluminous diodes'. The lack of coherence in the beam of radiation produced would appear to be of no clinical significance.
Laser Light Wavelengths
The particular wavelength of radiation emitted by a laser is determined by the physical
to table of contents
8/11/2019 EM Waves for Therapy
http://slidepdf.com/reader/full/em-waves-for-therapy 28/33
ELECTROMAGNETIC WAVES FOR THERAPY 298
The range of wavelengthswhich can be produced by laser action is quite large,from the microwave regionof the spectrum to the X-ray region.
design; in particular its chemical composition. Thus helium-neon lasers emit redlight with a wavelength of 632.8 nm. Ruby lasers, which consist of a cylindrical rod of synthetic ruby (a gemstone made of aluminium oxide) emit red light with a wavelengthof 694.3 nm.
Gallium aluminium arsenide (GaAlAs) diodes emit radiation at a frequencydetermined by the ratio of gallium to aluminium. The particular wavelength can bebetween 650 nm (in the visible, red part of the spectrum) and 1300 nm (in the near
infrared).Two types of lasers are commonly used in physiotherapy: helium-neon lasers, which,as noted above, produce red light of wavelength 632.8 nm and gallium aluminiumarsenide diode lasers, operating at near-infrared wavelengths (normally between 810and 850 nm).
Penetration Depth
The penetration depth of laser radiation is the same as ordinary electromagneticradiation of the same frequency. The wave coherence and the monochromatic natureof the laser beam make no difference. Thus the penetration depth of visible light froma helium-neon laser is a mm or so and most of the wave energy is absorbed in theepidermis (figure 11.3). The infrared radiation produced by commercial GaAlAsdiodes has greater penetration depth but most of the wave energy is absorbed in theepidermis and dermis.
Consideration of beam areaand average intensity indicates that torch-beamtherapy might be a cheaper and more effective treatment than laser therapy.
This perhaps explains why laser irradiation has been shown to be of value for treatingulcers and other skin conditions. What has not been shown, and is not likely to beshown, is that laser treatment is any better than shining a torch beam on the area.
Similar considerations indicate that laser irradiation is not likely to be of value for treating deeper tissue injuries.
The therapeutic benefit and relative cost effectiveness of laser therapy must thus bequestioned.
to table of contents
8/11/2019 EM Waves for Therapy
http://slidepdf.com/reader/full/em-waves-for-therapy 29/33
ELECTROMAGNETIC WAVES FOR THERAPY 299
EXERCISES
1 (a) What are the similarities and differences between infrared, ultraviolet andmicrowave radiation?
(b) State the wavelength range and frequency range of each kind of radiation.
2 Figure 11.1 shows a schematic diagram of a mercury vapour lamp.
(a) Describe the mechanism whereby ultraviolet radiation is produced in thelamp.
(b) Why must the power supply used for the lamp be current limiting?
(c) Why must special glass be used for the lamp envelope?
3 Compare the output of UV, visible and infrared radiation of air and water cooled
UV lamps and fluorescent tubes (figure 11.2).(a) Why do water-cooled lamps put out a negligible proportion of infrared
radiation?
(b) Why do fluorescent tubes put out a negligible amount of radiation atwavelengths less than 280 nm?
4 (a) Describe the process of production of infrared radiation by lamps and
electric heaters.(b) What effect does the use of a reflector have on the directionality and
wavelength of the radiation produced?
5 The filament of a light bulb is at a temperature of 3000 K and its wavelength of maximum emission is 960 nm. If the filament temperature was lowered to 1000K by decreasing the current what would be the new wavelength of maximum
emission? In what part of the electromagnetic spectrum is this wavelength?
to table of contents

8/11/2019 EM Waves for Therapy
http://slidepdf.com/reader/full/em-waves-for-therapy 30/33
ELECTROMAGNETIC WAVES FOR THERAPY 300
6 (a) Use figure 11.3 to describe the variation with frequency of the penetrationdepth of near infrared radiation.
(b) Describe the ways in which heat produced by near infrared radiation istransferred to subcutaneous tissue. Which would you expect to be themost efficient transfer mechanism?
7 Compare and contrast the principal effects of infrared and ultraviolet radiation on
tissue. How are the differences related to the wavelength of the radiation?
8 (a) What is meant by the term erythema as related to dosage in ultraviolettherapy?
(b) Briefly list the characteristics of a first, second, third and fourth-degreeerythema reaction to ultraviolet radiation.
9 Figure 11.4 shows a schematic diagram of apparatus used for the production of microwaves.
(a) Briefly describe the function of each subsection.
(b) Why is a magnetron valve rather than conventional electronic circuitry usedin microwave apparatus?
(c) What is the relationship between the size of the antenna in figure 11.4 andthe wavelength of the microwaves produced?
(d) What determines the frequency of the microwave radiation produced by theapparatus?
10 Figure 11.5 shows the beam produced by a point source of radiation positionedat the focus of a parabolic reflector. Draw diagrams to show the effect on thebeam shape of:
(a) mounting the point source between the focus and the reflector surface (stillon the central axis)
to table of contents
ELECTROMAGNETIC WAVES FOR THERAPY 301

8/11/2019 EM Waves for Therapy
http://slidepdf.com/reader/full/em-waves-for-therapy 31/33
ELECTROMAGNETIC WAVES FOR THERAPY 301
(b) mounting the point source on the central axis but further from the reflector than the focus.
11 (a) Explain why parabolic reflectors are not used with microwave diathermyapparatus.
(b) What are the most important factors determining the size and shape of thereflectors used with microwave diathermy apparatus?
12 (a) Give a brief explanation (in molecular terms) of why tissues with highdielectric constant and conductivity have low values of penetration depth for microwave radiation
(b) Refer to the figures given in table 11.1 and comment on the relative valuesof penetration depth for microwaves in fat, muscle and bone. Which tissueswould be expected to have similar values of penetration depth and why?
13 It has been said that a frequency of 2450 MHz represents a very poor choice for microwave radiation used in therapy because of the unpredictability of dosage.Explain.
14 Using data in table 11.1 determine the thickness of fat required to absorb 50% of the transmitted microwave energy at a frequency of:
(a) 1000 MHz
(b) 2000 MHz
(c) 4000 MHz
15 For microwaves of frequency 2000 MHz (table 9.1) calculate the fraction of energyremaining after travelling through
(a) 2 cm fat
(b) 2 cm muscle
(c) 2 cm bone.In which tissue is the energy absorbed most rapidly?
to table of contents

8/11/2019 EM Waves for Therapy
http://slidepdf.com/reader/full/em-waves-for-therapy 32/33
ELECTROMAGNETIC WAVES FOR THERAPY 303

8/11/2019 EM Waves for Therapy
http://slidepdf.com/reader/full/em-waves-for-therapy 33/33
ELECTROMAGNETIC WAVES FOR THERAPY 303
Complete the diagram to show the refraction effects. Briefly explain whathappens to waves at each boundary and why.
to table of contents