emergency department ultrasound at auckland hospital fast and aaa: the first year
TRANSCRIPT

Emergency Department Ultrasound at Auckland Hospital
FAST and AAA: The first year

Objectives
• The role of FAST
• History of ED ultrasound at Auckland Hospital
• The ultrasound credentialling process
• How we performed in the first year
• How we compare to the rest of the world
• Where we go from here
FAST
• Focused
• Assessment
• Sonography
• Trauma
FAST
• Integral part of initial trauma workup
• Proven– Quick– Safe– Reliable– Reproducible– Repeatable

FAST
• Pitfalls – Poor sonographer– Poor scan
• Air
• Obesity
– Negative FAST doesn’t exclude injury!– Failure to serially examine the patient

History
• 1998 Purchased portable ultrasound machine
• 1998 First Australasian FAST course
• 1999-2001 Sporadic use of ultrasound
• Dec 2000 Formal Emergency Ultrasound credentialling program
• Feb 2001 1st credentialled ED sonographers

The Credentialling Process - Background
RadiologistClinician
RadiologistClinician

The Credentialling Process - Background
• Much debate in literature last 10 years
• Consensus meeting • Each department decide own credentialling process
• 200 scans and ongoing audit
• Subsequent literature – Shackford 1999 4 yr experience
• 50 scans
• Suggests acceptable error rates

The Credentialling Process - Background
• Workshop beneficial– Rozycki 1996
• Exit exam– Sisley 1999

The Credentialling Process - Background
• American College of Emergency Physicians 2001– 8 workshop hours– 25 scans in each of 6 areas– Can be partially credentialled
• Only 1/76 departments met criteria– Boulanger 2000

The Credentialling Process - Background
• Australasian College for Emergency Medicine– 16 workshop hours– 25 Accurate scans for FAST– 15 Accurate scans for AAA– >50% clinically indicated– Proctored by credentialled/ultrasound qualified
person– Exit exam

Auckland ED• Adopted ACEM guideline December 2000• 4 sonographers
– Satisfied workshop requirement– Scans should not alter management– All measured against ‘gold standard’– Proctored by radiologist
– Standardised form– Monthly/bimonthly
– Modified criteria for scans– 100% clinically indicated
– Exit examination February 2001

Results FAST
• 1 ED registrar ‘credentialled’ by June 2001– 79% Indicated scans
• 2/3 ED Specialists credentialled by Feb 2002– All scans clinically indicated

Results FAST
• For Detection Any Free Fluid
• 113 scans in 102 patients over 13 months– 9 scanned by 2 sonographers– 1 scanned by 3 sonographers
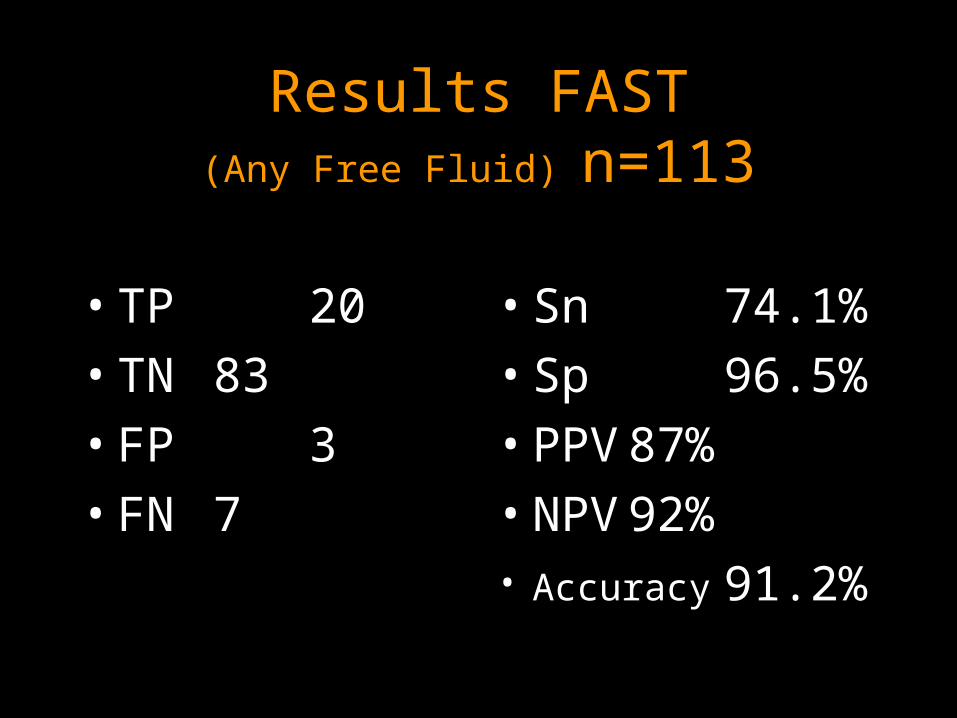
Results FAST(Any Free Fluid) n=113
• TP 20
• TN 83
• FP 3
• FN 7
• Sn 74.1%
• Sp 96.5%
• PPV 87%
• NPV 92%• Accuracy 91.2%

Results FAST(Laparotomy or Extra Investigation) n=107
• TP 11
• TN 89
• FP 5
• FN 2
• Sn 84.6%
• Sp 94.7%
• PPV 68.8%
• NPV 97.8%• Accuracy 93.5%

Results FAST Existing literature
• vs gold standard, novice sonographers• 3 studies
• Sn 69-79%
• Sp 96-98%
• vs clinical observation and experienced sonographers
• Sn 80-98%
• Sp >90%

Errors FAST
• 7 FN– 5/7 Trivial fluid, conservative management– 1 penetrating trauma with minor injury– 1 blunt trauma bladder injury, stable
• All views adequate and correct interpretation according to radiologist

Errors FAST
• 3 FP– 1 “ascites”– 1 “?pericardial effusion”– 1 Retroperitoneal and abdominal wall
haematomas
• Adequate views but incorrect interpretation

Result of errors FAST
• 1 CT scan thorax for “?Pericardial effusion”

Emergency Department Ultrasound for AAA
• 2 Case series in literature

Results AAA
• 66 Scans in 58 Patients in 12 months– 5 Scanned by 2 sonographers– 1 Scanned by all 4
• 3/4 sufficient scans to meet requirement

Results AAAn=66
• TP 26
• TN 39
• FN 1
• FP 0
• Sn 96.3%
• SP 100%
• PPV 96.3%
• NPV 97.5%• Accuracy 98.3%

“Error” AAA
• Free air obscured 6cm AAA
• Free fluid detected in Morison’s and Splenorenal recesses
• Found to have perforated DU
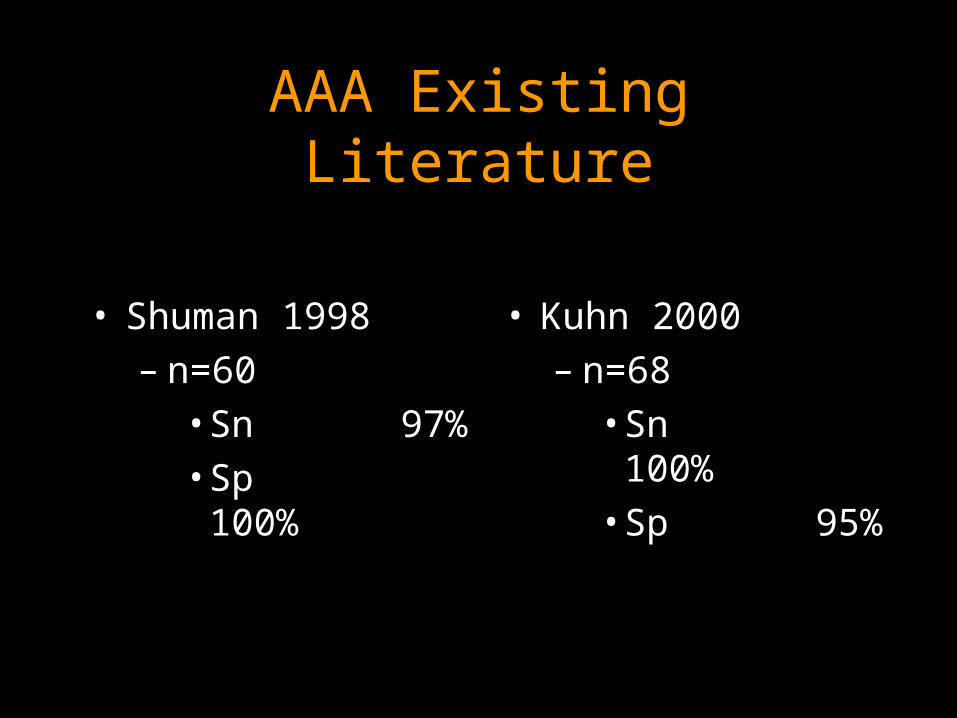
AAA Existing Literature
• Shuman 1998– n=60
• Sn 97%• Sp
100%
• Kuhn 2000– n=68
• Sn100%
• Sp 95%

Time Taken to Scan
• FAST median 5min (1-20)
• AAA median 3.5 (1-16)
• Similar to literature published

FAST Learning Curve
• Debate about this
• Shackford only author to look at initial experience– Suggests 10 scans before proficient– Showed ‘Institutional learning curve’– 12 Individuals = wide variation in error rates– Only 4/12 had >25 scans in 4 years

FASTLearning CurvePooled Error Rates for EU
0.00
0.02
0.04
0.06
0.08
0.10
0.12
5 10 15 20 25 30 33
Number of Scans
Err
or
Ra
te
Any Free Fluid
Clinically Significant

FAST Learning Curve
• Error rate <10%
• Most ‘errors’ clinically insignificant
• Individual variation

Potential Bias
• Patients not consecutive – Opportunity for pre-selection of patients
• Individual sonographers could discard unsatisfactory scans prior to proctoring

Summary
• Emergency Department Ultrasound is established in Auckland Hospital
• Accuracy mirrors existing literature
• Pitfalls exist and should be considered

The future
• Credentialling continues
• Credentialled sonographers record in notes
• Clinical management may alter
• Ongoing audit
• Expanded indications– Unstable patient with abdominal pain
• Is there free fluid?
Case 1
• 37f
– 4hr Abdominal pain
– Collapse and seizure
– Shock
– Arrives ED 1755
– SLOH 1806

Case 1
• OT 1815

Case 2
• 28f
– 1/2 hr Abdominal pain
– HR 84, SBP 90, RR 16
– Arrives ED 0910
– S/B registrar 1000
– SLOH 1018

Case 2
• Urine pregnancy test 1025, positive
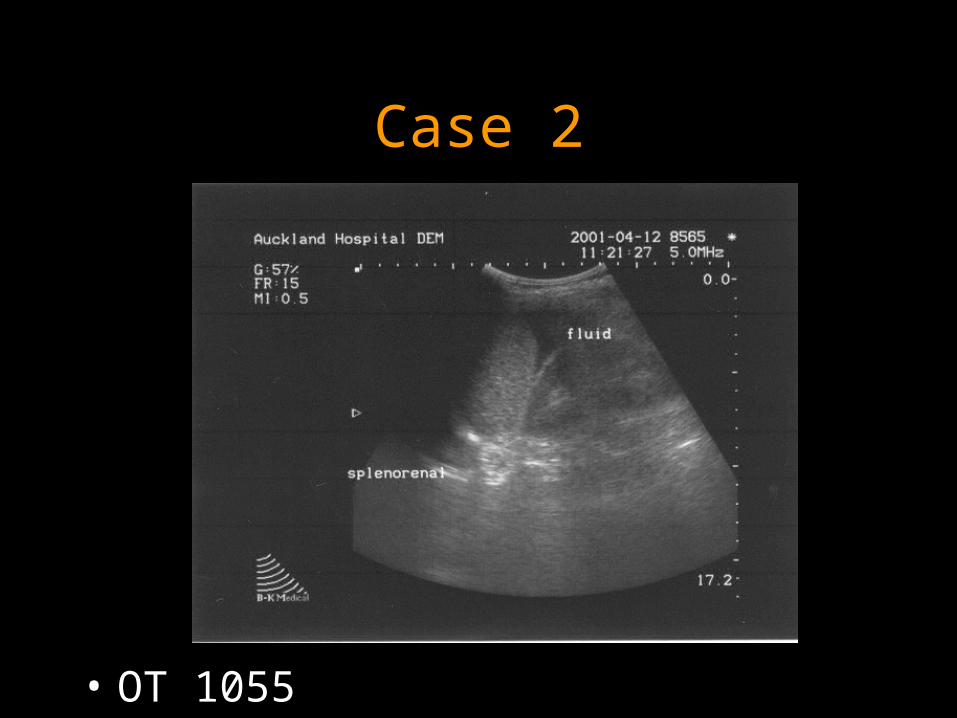
Case 2
• OT 1055

Case 3
• 19m– Fall from tree– Collapse at home– Fighting en route– Arrives ED 1635– FAST 1645

Case 3
• OT for thoracotomy