emergency medical services for children plan program evaluation
TRANSCRIPT

Emergency Medical Services Agency
Emergency Medical Services for Children Plan Program Evaluation and Update
January 1, 2009


TABLE OF CONTENTS ___________________________________________________________________________ Introduction ......................................................................................................... 1 I. Authority and Purpose ........................................................................................ 2
II. Summary of the Contra Costa EMSC Plan......................................................... 3 III. Planning Basis: Then and Now........................................................................... 5 IV. Organizational Structure Update 2009 ............................................................. 18 V. EMS for Children System Design and Resources............................................ 22 VI. EMSC Program Monitoring and Evaluation ...................................................... 28
VII. Next Steps: EMSC……………………………………………………………………30 VIII. Appendices ....................................................................................................... 31
A. EMSC Advisory Group Stakeholder List B. EMS Plan Update Process: Activity Timeline C. 2009 Pediatric Field Treatment Notes and Protocols D. ALS/BLS Equipment EMSC Equipment Survey
E. Contra Costa County Paramedic Accreditation Policy F. Emergency Department Consultation Visit Survey tool and Results
G. Contra Costa County Injury Prevention Resource List
H. Contra Costa EMSC Pediatric Emergency Training Programs
This document has been prepared in collaboration with the Contra Costa EMSC Advisory Group and is respectfully submitted by
Contra Costa EMSC Coordinator Pat Frost RN, MS, PNP

Contra Costa Emergency Medical Service Agency Page 1 EMS for Children Plan January 1, 2009
Introduction ___________________________________________________________________________ In early 1999 the Contra Costa Emergency Medical Service (EMS) Agency identified integrated emergency and critical care services for children within the county as a priority. The California Emergency Medical Services for Children (EMSC) Model provided the ideal framework for development and implementation of a system that could provide these essential services. To this end, the county pursued and was granted in July 2000, funding from the California EMS Authority to plan, develop, and implement a comprehensive EMSC system for Contra Costa County. Over the course of the two-year project, special care was taken to develop an EMSC program that would meet the unique needs required of the county's pediatric population. As an end result, Contra Costa EMS designed an EMSC system that would ensure accessibility and availability of services to all children in need of emergency and critical care. In February 2007 Contra Costa EMS began the process of updating the EMSC Program Plan. The EMSC plan update began with a comprehensive re-assessment of the Contra Costa County current EMSC Plan and pediatric capabilities of our EMS stakeholders. The previous plan was reviewed and opportunities for improvement identified. The chronology of this process is defined in the EMS Plan Update Activity Timeline. The EMSC Advisory Committee was re-identified and new members were recruited in this process. EMSC capabilities of our Emergency Departments and stakeholder agencies were re-explored with the intention of supporting an integrated system of EMSC activities for our EMS system. Surveys and site visits were completed and retrospective prehospital data was collected and articulated in the EMSC Plan review document “The State of EMSC for Contra Costa County.” The Contra Costa County EMSC Program wishes to acknowledge the EMSC Advisory Committee and our committed EMS stakeholders who have spent countless hours in the support of the EMSC program in Contra Costa County. This group contributed their time and expertise to this project and should be credited for their on-going commitment to improve the quality of pediatric emergency care to the children of Contra Costa County.

Contra Costa Emergency Medical Service Agency Page 2 EMS for Children Plan January 1, 2009
I. Authority and Purpose ___________________________________________________________________________ Authority The Contra Costa Emergency Medical Services Agency under the authority of California Health and Safety Code Division 2.5 and the Contra Costa County Board of Supervisors has the authority to develop, implement, and monitor the Emergency Medical Services for Children (EMSC) Plan. Mission Statement To ensure that quality emergency medical services are available for all people in Contra Costa County and that emergency medical care is provided in a coordinated, professional and timely manner. Purpose of the Emergency Medical Services for Children Program The purpose of Contra Costa County's EMS for Children Program is to establish, monitor and maintain a coordinated and comprehensive EMSC system that promotes high quality, contemporary pediatric care for the children of Contra Costa County.
Numbers correspond to Supervisorial Districts

Contra Costa Emergency Medical Service Agency Page 3 EMS for Children Plan January 1, 2009
II. Summary of the Contra Costa EMSC Plan ___________________________________________________________________________ Prior to the inception of the Contra Costa EMSC Program, prehospital and hospital services for children existed without the benefit of a specific organized plan for Pediatric Emergency Care. The 2000 EMSC Plan provided a comprehensive framework for the ongoing efforts by the Contra Costa EMS Agency to address the emergency medical needs of the county's children. The EMSC Plan assisted the Agency in promoting high quality care in the prehospital setting, ED, trauma and tertiary care centers, and interfacility transfer arena. The 2009 EMSC Plan will further enhance these efforts by facilitating the ongoing integration of the EMSC system throughout the EMS system in addition to the promotion of illness and injury prevention and educational activities. This document describes the area and populations served, organization, planning basis, resources, challenges, activities, monitoring mechanisms, and other features of the EMSC program. Definitions The following are definitions of terms that will be used throughout the Contra Costa EMSC Plan and system component documents. PEDIATRIC PATIENT is defined for the Contra Costa County prehospital setting as a patient fourteen years or less. PEDIATRIC CRITICAL CARE CENTER is a center that has met the established standards as set forth by Contra Costa EMS and undergone a formal site review and designation process. PEDIATRIC INTENSIVE CARE UNIT (PICU) is a pediatric-specific critical care unit in a licensed acute care hospital specially staffed and equipped to provide critical care services to children. Standards for PICUs have been defined by the California Children's Services (CCS) Program and adopted by Contra Costa EMS. PEDIATRIC TRAUMA CENTER is licensed acute care hospital which usually treats (but not limited to) persons fourteen (14) years of age or less; that is approved as part of the Contra Costa County's Trauma Care System Implementation Plan, meets all relevant criteria, and has been designated as a pediatric trauma center, in accordance with the California Code of Regulations, Title 22, Division 9, Chapter 7 100255. PEDIATRIC EDUCATION FOR PREHOSPITAL PERSONNEL (PEPP) is a training program sponsored by the American Academy of Pediatrics, which encompasses the majority of emergencies encountered in pediatric patients. EMERGENCY NURSING PEDIATRIC COURSE (ENPC) is an educational program developed for RNs by the Emergency Nurses Association to standardize the approach to pediatric emergency care by nurses. PEDIATRIC ADVANCED LIFE SUPPORT COURSE (PALS) is an educational program developed for all emergency health care providers (MDs, RNs, EMT-Ps) by the American Heart Association and Academy of Pediatrics to standardize the approach to pediatric resuscitation.

Contra Costa Emergency Medical Service Agency Page 4 EMS for Children Plan January 1, 2009
PEDIATRIC EMERGENCY ASSESSMENT, RECOGNITION, AND STABILIZATION (PEARS) is an educational program developed for health care providers who do not routinely deal with pediatric emergencies (MDs, RNs, EMT-Ps) by the American Heart Association and Academy of Pediatrics to standardize the approach to assessment and management of the pediatric pre-arrest state. ADVANCED PEDIATRIC LIFE SUPPORT COURSE (APLS) is an educational program developed for all emergency health care providers (MDs, RNs, EMT-Ps) by the American College of Emergency Physicians and Academy of Pediatrics to standardize the initial assessment and early treatment of ill and injured children. EMS for CHILDREN (EMSC) ADVISORY GROUP is a multi-disciplinary advisory group that contributes to primary pediatric policy, procedure, protocol, and guideline development, monitors contemporary pediatric practices and other issues, and makes recommendations to Contra Costa EMS concerning the EMSC Program. TRAUMA SYSTEM is a regional system for field care and transport, destination determination, ED care, tertiary care and quality assurance of patients sustaining major trauma.
Contra Costa Emergency Medical Service Agency Page 5 EMS for Children Plan January 1, 2009
III. Planning Basis: Then and Now ___________________________________________________________________________ EMSC Program Overview The Contra Costa County EMSC Program seeks to promote contemporary and high quality emergency care throughout the county by providing tools to support practitioners at all levels to provide appropriate care of children and get these children to the facilities that best meet their EMS needs. Concurrent promotion of injury and illness prevention efforts is recognized as the most promising means to keep children healthy and out of the EMS system. Specific Issues and Areas for Improvement Identified in Contra Costa County The following are specific issues and areas for improvement that were identified by Contra Costa EMS in 1999 prior to the planning and implementation of the current EMSC system. The EMSC Program plans from1999 are in blue text. Since implementation of the EMSC Program in 2000 significant progress has been met. Progress and opportunities are captured under “Outcomes to Date”. EMSC Administrative and Organizational Structure Then and Now In order to plan, develop, and implement an EMSC system in Contra Costa County, an administrative and organizational structure with appropriate EMSC staff and resources has been identified as a need. Developing an on-going structure for maintaining the system when the grant has ended is included in the grant objectives. The State EMSC guidelines for “System Planning, Implementation and Management Model for the Integration of EMSC in Local EMS Systems” are being used as a guide for developing this structure. Outcomes To Date: The initial EMSC Task Force & Advisory Committee was established in 2000. An EMSC Role has continued since first inception. The current EMSC Program Coordinator was assigned in January 2007 to update of local EMSC program plan. The EMSC Advisory Committee was re-identified, new members recruited and electronic consultation, feedback and networking mechanisms were established. EMSC Plan Then and Now While prehospital and hospital services for children do exist in Contra Costa County, neither a specific EMSC Plan nor system is in place locally. A plan for development of an integrated EMSC system in Contra Costa will be adopted and incorporated into the local agency’s EMS System Plan. A comprehensive plan for an EMSC system that includes implementation and maintenance of all major components of the EMSC system, and that integrates the EMSC system with the overall EMS system, is to be developed. Outcomes to Date: Current EMSC plan was reviewed and progress of stakeholders assessed based on 2008 national and state EMSC goals and objectives. This process included re-education of EMSC system participants on the new EMSC guidelines for equipment and emergency department care of children. Contra Costa EMSC Plan now integrates all EMSC state guidelines as part of local EMSC plan. When variations exist

Contra Costa Emergency Medical Service Agency Page 6 EMS for Children Plan January 1, 2009
between local and state guidelines, those areas are evaluated for opportunities for improvement if applicable to the local EMS System. 1. Prehospital Services Then and Now Various studies in both California and the nation have indicated that many prehospital services are adult oriented and are often inadequate in providing pediatric care. They do not always have appropriate pediatric equipment and supplies, pediatric protocols, or sufficient pediatric training for prehospital personnel. Contra Costa is committed to assuring that prehospital services meet the needs of critically ill and injured children. This commitment includes assessment of equipment and skills, revision of treatment guidelines and protocols, and development and provision of specialized training for prehospital personnel to adequately prepare them to care for our younger population. Outcomes to Date: Surveys conducted in 2008 demonstrate that appropriate pediatric emergency equipment is in place throughout the system. All prehospital agencies and Emergency Departments have effectively implemented ongoing pediatric training programs on pediatric emergencies. Variations exist in type of courses and training mechanisms used to accomplish these objectives based on the needs and preferences of stakeholders. All courses are national pediatric emergency care curriculums of value in our EMS system. An information course comparison sheet was created by EMS in 2008 and distributed to stakeholders as a resource of the types of programs currently available for emergency personnel. Information on a new curriculum “Pediatric Emergency Assessment, Recognition & Stabilization” (PEARS) was introduced to stakeholders as part of the EMSC update. This curriculum is particularly exciting with its strong focus on pediatric emergency assessment and robust course materials. This program’s focus is on the new national standard for pediatric emergency assessment developed by the American Heart Association (AHA) and American Academy of Pediatrics (AAP). The new assessment model is called Assess, Categorize, Decide and Act (ACDA). This new assessment standard is already taught in Pediatric Advanced Life Support (PALS). All Contra Costa EMS stakeholders have been encouraged to integrate ACDA as a component to current pediatric emergency care training. Adoption of this new assessment model would provide a tremendous opportunity for EMS system providers to “speak the same language” when it comes to pediatric assessment. It would enable Contra Costa to use one assessment model throughout county for the identification and assessment of the pre-arrest state in children. Evidence-based medicine consistently demonstrates that assessment and early management of the pre-arrest state is key to improving outcomes in critically ill children. Prehospital Pediatric Protocols were established in 2000 and have been consistently updated based on current Pediatric Advanced Life Support standards and evidence-based medicine. As part of the Contra Costa EMSC update comparisons were made between National EMSC, State EMSC and Contra Costa prehospital protocols. Opportunities for new protocols were identified and will be one area of focus for future EMSC activities. In addition the EMSC Coordinator actively participates on the State EMSC Coordinator Group which has been updating the State pediatric protocols. These protocols serve as a

Contra Costa Emergency Medical Service Agency Page 7 EMS for Children Plan January 1, 2009
resource and model to the EMS community in California. Contra Costa pediatric protocols are consistent with those updated protocols. 2. Pediatric Capabilities of Emergency Departments (EDs): Then and Now In the absence of local EMSC standards or guidelines, emergency departments vary in training, equipment and supplies available for the evaluation, stabilization and transfer/transport (when indicated) of children. Emergency departments are particularly important in pediatric EMS systems because ill and injured children are brought directly to the ED in local hospitals by their parents or caretakers. Relatively few children are transported to EDs through the EMS system. Therefore, it is imperative that all ED’s have appropriately trained staff, equipment, and supplies for the evaluation, stabilization and transfer/transport (when indicated) of children. Guidelines for community hospital EDs will be developed with implementation and site visits to follow. Contra Costa has eight acute care facilities capable of receiving ALS patients. Local facility designation of receiving hospitals is based solely on State requirements for approval as a basic or comprehensive emergency department. There is strong support for the development and implementation of Pediatric ED guidelines from all hospitals, the EMCC and many other groups in the County. Outcomes to Date: In 2000, Contra Costa County established separate Pediatric ED guidelines consistent with EMS authority EMSC guidelines. Upon review of the 2000 Local EMSC guidelines and the 2008 State EMSC guidelines, local guidelines were determined to be redundant the and the state guidelines were adopted as our local guidelines. In 2008 the State EMSC guidelines were used to survey each receiving hospital in the system. The current State EMSC guidelines were distributed to all facilities along with their facilities previous 2000 EMSC self-assessments if they participated. This allowed each hospital to evaluate their own progress during this period of time and recognize “how far they had come” in implementing the EMSC guidelines. Each facility completed a written self-assessment survey and participated in an educational site visit to discuss their status with new guidelines and to identify opportunities for improvement. See addendum for hospital survey and summary. In 2007 Kaiser Antioch opened a new hospital in our community increasing our receiving facilities to nine for the county. All hospitals were found to be in compliance and common opportunities for improvement were identified in the area of training, disaster preparedness and quality improvement. EMSC program coordinator will act as facilitator to provide information and consultation to hospitals working on improvement in these areas. 5. Inter-facility Pediatric Consultation/Transfer Guidelines and Transfer Agreements
Then and Now Children identified as critically ill or injured require the expertise available through pediatric consultation and/or transfer, yet guidelines and agreements for consultation or transfer are not standardized or necessarily in place locally. The State EMSC project as well as other EMSC projects in California has developed pediatric consultation/transfer guidelines to assist physicians and hospitals in identifying children who might benefit from consultation

Contra Costa Emergency Medical Service Agency Page 8 EMS for Children Plan January 1, 2009
with pediatric critical care or trauma specialists. Such guidelines help to promote appropriate consultation and transfer when indicated to pediatric critical care and trauma referral hospitals. Pediatric interfacility transfer agreements also help to establish closer working relationships between referral centers and community hospitals. In Contra Costa County some centers and community hospitals have developed such agreements, but a number have not. Studies conducted by the Pediatric Intensive Care Network of Northern and Central California show that transports of critically ill and injured children from community hospitals to pediatric referral centers are significantly greater for designated centers that are part of an organized EMSC system and have signed transfer agreements with community hospitals. The EMSC project will develop pediatric interfacility consultation and transfer guidelines with the intent for them to be adopted by the receiving facilities within Contra Costa County. This will include developing and implementing interfacility transfer agreements with pediatric critical care centers and trauma centers. Outcomes To Date: Since 2000, formal and informal interfacility transfer agreements have been well established between referral centers and community hospitals. Formal transfer agreements are not global. The need for formal agreements is highly influenced by insurance and reimbursement patterns not within the EMS jurisdiction or influence. However all facilities have mechanisms in place to facilitate timely transfer of pediatric patients and do so accountably within the current system. In 2009, timely interfacility transfer will be increasingly scrutinized by other regulatory agencies such as Joint Commission. Incentives for compliance with timely appropriate transport of children to a higher level of care will be supported by these new Joint Commission standards on an ongoing basis. 6. Pediatric Interfacility Transport Services Then and Now
Interfacility critical care transport services guidelines do not currently exist in Contra Costa County. Children brought directly to EDs by their parents may require a higher level of care or specialized services not available at community hospitals. To obtain optimal care, these children may need to be transferred from the receiving ED to pediatric critical care centers or trauma centers. In addition, the condition of pediatric patients already admitted to community
hospitals may deteriorate and they may also require transfer to these specialized centers. Interfacility transport of critically ill and injured children involves mobile intensive care for a variety of complex pediatric medical and trauma conditions, and interfacility transport providers should have appropriately trained personnel and the capabilities for the management of pediatric patients during transport. Specialized pediatric center-based transport teams provide inter-facility transports when receiving a critically ill child. However, private ground and air transport providers are also involved in Contra Costa County. These include contracted ALS provider and air ambulance services. Guidelines will be developed and implemented for pediatric interfacility ground and air transport programs and assuring that all interfacility transport providers meet these guidelines. Outcomes To Date: As part of the EMSC plan development Contra Costa developed pediatric critical and trauma interfacility consultation and transfer guidelines in 2002. As of

Contra Costa Emergency Medical Service Agency Page 9 EMS for Children Plan January 1, 2009
2008 these guidelines were felt to be redundant and all facilities had transfer processes and/or agreements that were consistent with State EMSC standards. For that reason Contra Costa’s 2009 EMSC plan will adopted the State EMSC guidelines to evaluate EMSC performance issues within our county. Within our EMSC system both air and ground transport providers such as AMR, CALSTAR, REACH, and Pediatric Critical Care Center Transport Teams are involved in inter-facility transport of children. Our base hospital, John Muir Medical Center-Walnut Creek is a resource in facilitating transfer of critically ill pediatric patients transported to Children’s Hospital Oakland or other Pediatric Critical Care facilities. The 2008 EMSC Emergency Department survey summary demonstrates that each facility has identified appropriate pediatric transfer centers and mechanisms to facilitate timely transport of children requiring a higher level of care. In the fall 2008 Contra Costa EMS acted to support the collection of public comment among the EMSC stakeholders on the revised State EMSC Guidelines for Pediatric Inter-facility Transport Programs (#181) and Interfacility Pediatric Trauma and Critical Care Consultation and/or Transfer Guidelines (#183). Monitoring of these issues occurs as part of the Contra Costa Trauma Continuous Quality Improvement (CQI) process, Helicopter utilization oversight and EMS Event reporting (Contra Costa EMS patient safety reporting system). 7. Pediatric Referral Centers – Pediatric Critical Care and Trauma Centers Then and
Now Contra Costa County does not have a medical center with separate distinct pediatric intensive care units (PICUs). Critically ill and injured patients are for the most part transferred to out-of-county facilities, primarily Children’s Hospital and Research Center at Oakland, the regional pediatric treatment and trauma center for this catchment area. Children’s Hospital serves as a referral center for critically ill and injured children. However, the designation or official recognition as the specialized center is not fully integrated into an organized system of care for all critically ill and injured
children in Contra Costa. Standards for Pediatric Critical Care Centers (PCCC) have been developed by the state and used locally in the designation of the PCCC in Alameda County. A more formal integration into the neighboring EMSC system including referral to the PCCC/trauma center by each receiving facility within Contra Costa will occur as part of this grant project. Outcomes To Date: The recent EMSC survey of our receiving hospitals showed a significant decrease in the number of general care pediatric beds in Contra Costa. Contra Costa Regional Medical Center (CCRMC), Doctors San Pablo, John Muir Medical-Concord Campus (formerly known as Mount Diablo Hospital) have closed their pediatric units. The costs associated with providing trained pediatric nursing personnel with access to pediatric physician coverage in those communities have been prohibitive. In addition evidenced based pediatric care studies support directing pediatric care to pediatric specialty providers and facilities to improve outcomes. Pediatric care in our community has become quite consolidated.

Contra Costa Emergency Medical Service Agency Page 10 EMS for Children Plan January 1, 2009
Hospitals who have preserved pediatric services have augmented them with pediatric hospitalists available for 24/7 consultations. Overall all hospitals in our county have increasingly relied on moving children to facilities with definitive care for children. Children’s Hospital and Research Center at Oakland (CHO) located in Alameda County serves as the primary regional pediatric treatment and trauma center for our EMS system. The Contra Costa/Alameda County EMS Trauma Advisory Committee (TAC) provides appropriate oversight for Pediatric Trauma Triage. Each hospital in our EMS system has mechanisms in place to appropriately transfer pediatric patients requiring higher levels of care to CHO or other facilities if beds are not available. Transport of children typically occurs using a variety of resources including Pediatric Transport Teams sent from the receiving facility, Critical Care Transport, Air Transport and Ground Transport with trained specialists. The requirement for using these resources is very infrequent consistent with the low incidence of pediatric critical patients seen in our county. In addition the Contra Costa EMS system supports patient choice of facilities. This enables transport of pediatric special needs or chronically ill patients established at a particular pediatric center to be transported where they receive their care. Other pediatric/neonatal critical care facilities that receive patients from our facilities include: UC Davis Lucile Salter Packard Children’s Hospital at Stanford UCSF Kaiser Oakland, San Francisco, Sacramento and Santa Clara Santa Clara Valley Medical Center Shriners Sacramento California Pacific Medical Center Saint Francis Burn Center
8. Pediatric Rehabilitation Resources Then and Now
The provision of quality health care does not stop in the emergency department or upon discharge from hospital admission, yet specific pediatric rehab resources are not identified locally. The continuum of care would include the rehabilitation and additional supportive care provided to those in need of such services. State recommendations for pediatric rehabilitation programs will be reviewed in conjunction with the PCCC standards and recommendations for referral guidelines will be developed.
Outcomes To Date: Pediatric Rehabilitation Resources are highly specialized services accessed through referral and consultation with appropriate Pediatric Specialists and Pediatric Referral Centers. Currently pediatric patients who qualify for California Children’s Services (CCS) and/or Regional Center Services have rehabilitation and special services available to them. Access to these services is facilitated by appropriate CCS authorized

Contra Costa Emergency Medical Service Agency Page 11 EMS for Children Plan January 1, 2009
physicians and nurse specialists. Each facility in Contra Costa County has appropriate mechanisms in place to facilitate referral of pediatric patients to these resources. 9. Illness and Injury Prevention Programs/Public Information and Education Then and Now
At the inception of Contra Costa EMSC Plan a number of agencies had active illness and injury prevention programs, these programs were not integrated component of the EMSC system. Contra Costa County has had a strong commitment to illness and injury prevention programs. Many agencies, organizations, institutions, and providers in Contra Costa had worked for a number of years to improve emergency and critical care services for children. The Childhood Injury Prevention Coalition (CIPC) of Contra Costa County was key to those injury prevention efforts at the time. CIPC made considerable progress in identifying predominate injury
prevention issues and target areas for education and injury prevention efforts. CIPC was active in drowning prevention, home and crib safety, and passenger, bicycle and pedestrian safety. Contra Costa was the first county to pass a Countywide Action Plan to Prevent Violence, a comprehensive blueprint that was approved by 78.8% of the voters in 1994. A series of county residential pool-fencing ordinances to prevent child drowning was championed by CIPC in partnership with the Drowning Prevention Foundation. Both coalitions worked for a county ordinance covering the county’s unincorporated areas, which was followed by a majority of Contra Costa cities each passing similar ordinances for their areas. The county’s trauma center, John Muir Medical Center Walnut Creek has had a long-standing active and progressive injury prevention service, which includes a model Child Passenger Safety Program, and collaborates with the county’s services. EMS staff participates on the Child Death Review team that reviews pediatric deaths in the County. Recommendations for injury and illness prevention programs were developed in conjunction with existing prevention programs and integrated into the EMSC system. Outcomes To Date: Contra Costa EMSC provides information, referral, data and resources for stakeholders in Health Services, and our EMSC community to facilitate awareness and participation in a wide variety of pediatric injury prevention programs. Prevention activities are detailed in the addendum of this document. Prehospital data is available and provides information for injury prevention activities. This data is reported to appropriate constituencies within the EMS system. EMS staff are assigned to participate on Contra Costa County’s Child Death Review Team. This multidisciplinary team is responsible for the review of pediatric deaths in the County. After 2000 the Childhood Injury Prevention Coalition (CIPC) became inactive, but work has continued in the targeted area of bicycle and pedestrian injury prevention. In 2007 Contra Costa EMS joined the East-Bay Childhood Injury Prevention Network (EBCIPN). This inclusive organization supports opportunities for collaborative pediatric injury prevention activities including advocacy and facilitating public awareness. Its vision is to “create a safer world for all children by reducing preventable injuries.” Members represent a wide variety of interdisciplinary child injury prevention individuals and agencies throughout the East Bay Area. Contra Costa County has several stakeholders who participate regularly in this group.

Contra Costa Emergency Medical Service Agency Page 12 EMS for Children Plan January 1, 2009
10. Prehospital and Hospital Information Management/Data Then and Now System assessment and indications for improvement are realized through review of outcomes and other data, yet specific data on pediatric emergency care is not thoroughly collected. In 1999, the Contra Costa EMS Agency received a Prevention 2000 block grant to implement a prehospital information integration and management data system. The EMS Agency is committed to fund the continuation of this resource. The EMS Agency also currently collects some hospital outcome data utilized in its trauma system and first responder defibrillation program reviews. Coordination will
be established between the EMSC project, the prehospital data linkage project and hospital outcome data collection to compile appropriate pediatric EMS data needed to monitor the system. Outcomes to Date: Since 2000, EMS has successfully implemented two electronic prehospital care record (ePCR) systems in our County. American Medical Response ePCR system called “MEDS” is used by our EMS contract transport service and represents approximately 90% of all 911 transports in the system. This other ePCR has been in use in our county for about 10 years. Fire agencies utilize the “Zoll” electronic patient care record system. Zoll data generated from this ePCR system represents Fire first responders and Fire transport providers. This program was launched system-wide in 2007 and is in the process of being fully implemented. In 2008 we started to collect limited data from that ePCR system for process improvement. Contra Costa EMS has used both these electronic data systems to access information about pediatric prehospital patient care since 2007. Contra Costa EMS has also participated in the California State EMSC Performance Measures (CQI) study during in early 2007 and the National EMSC Performance Measures Project in early 2008. Our county had 100% participation with data collection on the National EMSC Performance Measures Project. This project supported California EMS Authority EMS for Children Program efforts to meet their funding outcome requirements as part of the National EMSC Program. Overall Contra Costa EMS has made extraordinary progress in this area and has fully integrated pediatric indicators into all EMS CQI processes. We continue to work to refine our pediatric performance measures. Pediatric EMS performance and descriptive data are captured in the document “The State of EMSC for Contra Costa County.” EMS continues to explore opportunities for prehospital data linkages to hospital outcome data. At this time outcome data continues to rely on the “human” interface to successfully obtain and compile successfully. Contra Costa EMS is well positioned to be successful with linking to data networks yet to be established to facilitate outcome analysis in the prehospital arena for children.
11. Continuous Quality Improvement Then and Now Any healthcare system or program implemented in an area requires an on-going review and assessment for adherence to standards, enhancement of quality of service, and need for revision or additions to the program. Thus EMSC system review must be incorporated into the existing local CQI program. Contra Costa is committed to developing a

Contra Costa Emergency Medical Service Agency Page 13 EMS for Children Plan January 1, 2009
total system Continuous Quality Improvement (CQI) program, which will include review and assessment of the EMSC program, developed for the county. Throughout the two and a half year grant process, Contra Costa EMSC Program developed and implemented EMSC system components and materials that provide a wide variety of tools and incentives necessary to achieve widespread excellence in pediatric care. These efforts include:
• Policies, procedures and protocols • Facility guidelines and standards • Consultation, recognition, and designation of specialty centers • Educational training and materials • Other assistance as needed Outcomes to Date: Since 2000 Contra Costa EMS has successfully implemented the EMSC system components supporting CQI as bulleted above. Pediatrics has been a strong focus of EMS System CQI activities and is now fully integrated as part of our CQI program. Annual EMS system prehospital provider needs assessments have consistently demonstrated that providers have ongoing needs for pediatric training and education. In response to these identified needs curriculums on pediatric emergency topics have been developed and standardized throughout the prehospital providers facilitated by the Contra Costa Fire EMS Training Consortium. Contra Costa “EMS Best Practices” newsletter routinely focuses on pediatric emergency care. CQI performance reports incorporating pediatric data to Emergency Medical Care Committee, Medical Advisory Committee, Facilities and Critical Care Committee and Fire EMS Training Consortium have strengthened efforts to provide information and awareness. Tools such as the new Prehospital Pediatric Color Coded Medication Cards facilitating safe pediatric field medication delivery have been developed. Improved processes to notify our emergency department stakeholders have been established to provide quick access to updates from the State EMSC, National EMSC and other groups such as the American Heart Association and the American Academy of Pediatrics. Contra Costa EMS Event (patient safety) Reporting System is designed to capture data as part of the QA process for QI analysis. Variations in pediatric prehospital protocol and skills success are monitored at appropriate intervals to identify opportunities for improvement. Examples of evidence-based changes taken based on CQI issues in our pediatric population include: Removal of Pediatric Intubation Removal of Charcoal for Pediatric Ingestions Instituting use of D10W for the treatment of pediatric hypoglycemia Instituting EZIO for pediatric use Adoption of ACDA assessment model Development of pediatric medication cards consistent with Color Length-Based Tape
Dosing (e.g. Broselow) Opportunities for improvement will continue to be identified and pediatric performance measures monitored moving forward.

Contra Costa Emergency Medical Service Agency Page 14 EMS for Children Plan January 1, 2009
Optimal EMSC System Design Then and Now In 2000 an optimal EMSC Program and System design for Contra Costa County was described as including the following features. As of 2009 the EMS System Design status is:
2000EMSC Design Recommendations 2009 EMSC System Design Opportunities An administrative and organization structure within the Contra Costa EMS would be established to oversee the activities of the EMSC Program.
EMSC Coordinator designated and function supported within the EMS Agency. EMSC Program oversight in place and well integrated in current advisory forums.
A multi-disciplinary EMSC Task Force would be established to facilitate the efforts of the EMS Agency for effective monitoring, evaluation and updating of the EMSC Program.
EMSC Advisory Group re-established. Networking and EMSC program update mechanisms put in place. Efforts to establish Emergency Department Physician and Nurse “EMSC Champions” throughout the community to facilitate EMSC program goals and objectives explored.
An organized system of Pediatric Advanced Life Support capabilities accessible throughout the county.
PEPP is the approved Pediatric Prehospital Provider training program. PALS, APLS, ENPC, and PEARS are all appropriate programs for ED providers based on provider role and responsibilities. All hospitals in compliance with appropriate training based on EMSC state guidelines. 2008 Survey revealed opportunities for additional training needs to be considered due to shrinking opportunity to maintain pediatric hospital expertise in the community. Pediatric general care and specialty beds have been significantly reduced since 2000. This trend is expected to continue placing new demands for improved pediatric skills in pediatric assessment, triage and appropriate treatment by emergency department professionals. Emergency Departments will increasingly be on the front lines of pediatric emergency care and need to be “ready” to rapidly assess, recognize, stabilize and transport the child in extremis. These events while rare require high-level pediatric skills. Contra Costa EMSC moving forward is positioned to continue to encourage and support training critical to the development and maintenance of those skills.

Contra Costa Emergency Medical Service Agency Page 15 EMS for Children Plan January 1, 2009
2000 EMSC Design Recommendations 2009 EMSC System Design Opportunities All levels of field personnel would be well trained and practiced in pediatric assessment and treatment skills.
ACDA “Assess, Categorize, Decide, Act” 2008 National Pediatric Emergency Assessment Model approved by the American Heart Association and American Academy of Pediatrics adopted as the county assessment standard for EMS system providers. A limited program of pediatric simulation training is currently in place for prehospital providers facilitated by the Fire-EMS Training Consortium. Simulation training has also been incorporated into some PEPP training for Fire-EMS providers. Opportunities for expanded pediatric simulation training resources for emergency department personnel are being explored. Interest in simulation training is growing in the emergency department and hospital community. EMS is committed to supporting an ongoing dialogue with the hospital community on creating opportunities for these resources to be developed.
Contemporary and practical pediatric field treatment protocols/guidelines would be maintained.
Prehospital pediatric protocols are currently up to date and in line with national standards and evidenced based medicine. Ongoing evaluation of protocols will emphasize evidence-based practice, patient safety and recognition of the pediatric pre-arrest state with rapid transport to definitive care. New protocols and resources in development.
All emergency departments would meet or exceed the recommended minimum criteria of the Administration, Personnel and Policy Guidelines for the Care of Pediatric Patients.
Facilities completed a self-assessment and participated in a site visit as part of EMSC program plan update. All facilities in compliance with current 2008 guidelines. See details in the survey results in the addendum of this document.
A minimum of one Pediatric Critical Care Center and one Pediatric Trauma Center would be designated for the County.
Children’s Hospital Oakland is the designated Pediatric Critical Care and Pediatric Trauma Center for Contra Costa County. Collaborative relationships in place to facilitate appropriate follow-up on CQI pediatric issues and trauma cases.

Contra Costa Emergency Medical Service Agency Page 16 EMS for Children Plan January 1, 2009
2000 EMSC Design Recommendations 2009 EMSC System Design Opportunities A comprehensive data collection system that includes the collection of recommended pediatric data would be established.
Comprehensive data collection system for review and evaluation of prehospital pediatric care implemented with reporting on pediatric performance measures. These include prehospital skills, pain, glucose, seizure, and medication safety.
Efforts of existing Contra Costa County injury prevention and public education programs would be supported.
Funding sources for injury prevention activities continue to be shrinking. This requires increasing improved collaboration among injury prevention stakeholders in their activities. Opportunities exist for EMSC to participate and support injury prevention by providing leadership, data, awareness and advocacy. In 2007, an EMSC web page was created as part of the Contra Costa County EMS website to improve access to information and resources about EMSC to our community. Enhancements are planned to add information and resources for emergency providers and the public in the areas of injury prevention, special needs, emergency first aid for schools as part of Contra Costa ongoing support of EMSC activities. Internet resources will continue to be explored and improvements implemented as opportunities are identified with the input of constituent groups.
Conclusion EMSC Program for Contra Costa County has met or exceeded 2000 program design objectives with opportunities for future innovative EMSC program enhancements.

Contra Costa Emergency Medical Service Agency Page 17 EMS for Children Plan January 1, 2009
In 2000, the initial development of Contra Costa’s EMSC created a free standing system of EMSC program coordination, oversight and advisory process. This model was very effective in establishing the EMSC program in Contra Costa but over time this program development model was unable to be sustained in its original configuration. Lack of EMSC dedicated personnel, resources & created barriers for stakeholders to fully participate. Instead the work of EMSC became integrated as part of other groups including Medical Advisory Committee, Facilities and Critical Care and Trauma Advisory Committee. The plans and objectives set out by the original EMSC plan succeeded with the commitment of numerous individuals within the EMS system during those years. The EMSC plan of 2000 successfully positioned Contra Costa EMSC stakeholders in effectively implementing a wide array of pediatric resources to improve emergency care for the children of our community.
Moving forward, the new EMSC program will continue to use an “integrated” approach to EMSC advocacy while supporting and recruiting “EMSC Champions” within our community. This approach is supported by our EMS stakeholders and is recommended as a best practice model to maintain and enhance the EMSC programs for all communities. Our EMSC workflow process model is below.
EMS-C Program
Pediatric Event
Review
Child Death
Review
Pediatric QI
Indicator Reports
California EMS-C
Program
Pediatric Trauma
PreTac & TACEMS QI Committee
Medical Advisory Committee
Facilities & Critical Care
EMS Medical Director
Prehospital Care
Coordinators
Fire-EMS Stakeholder QI Coordinators
EMS-C Coordinator
EMS-C Advisory
Committee
ED-EMSC Liaisons
Fire-EMS Training Consortium
Injury Prevention
Groups
Pediatric EMS-C Issue Identification
EMS for Children Improvement Process
Contra Costa EMS-C Program Workflow“Getting the Business of EMS-C Done”

Contra Costa Emergency Medical Service Agency Page 18 EMS for Children Plan January 1, 2009
IV. Organizational Structure Update 2009 ___________________________________________________________________________ Contra Costa County Geographic Characteristics Contra Costa is one of the nine counties comprising the Bay Region in Northern California. It is the ninth most populated county in California with a population of 1,051,677 as of January 1, 2008 and a geographical area of 732.5 square miles. There are nineteen incorporated cities within the County. Contra Costa is divided into three distinct sub-regions defined by topographic features: the bay plan and series of valleys in the western region; hills that separate the western region, the eastern plain and delta area in the eastern region. The delta lowlands have miles of waterways for recreation; the bay and river shorelines are traversed by rail lines and dotted with many heavy industries including major petrochemical facilities. Nine major highways connect Contra Costa with adjacent counties and are heavily traveled, particularly during commute periods. There are several two-lane county roads which traverse the hills and rural areas in a winding fashion and which have provided the scene for many severe motor vehicle crashes. Contra Costa has several Bart stations traveling through the county. Bart functions as the high-speed commuter rail system for the East Bay. There are two airports in the county Buchanan Field: located in Concord, and Byron Airport, located two miles south of Byron. Demographic Characteristics
Ethnic statistics reflect the increasingly diverse ethnic distribution of Contra Costa’s pediatric population. As of 2007 Contra Costa is home to approximately 255,915 children, ages 0-17, which is 3 % of California’s child population TPF
1FPT. As the table demonstrates, Contra
Costa’s pediatric population is ethically diverse and between 2001 and 2008 Racial/Ethnic data remained stable while the proportion of Caucasian/White children fell from 48% in 2001 to 43% in 2008.TPF
2FPT During that same period of time Hispanic/Latino children increased
from 25% to 32%.P
2P
TP
1PT Children Now, “Contra Costa County”, 2007 California County Data Book, childrennow.org
TP
2PT Kidsdata.org website, (2008) retrieved 10/20/08, from wwwkidsdaa.org

Contra Costa Emergency Medical Service Agency Page 19 EMS for Children Plan January 1, 2009
Center for Social Services Research
UC BerkeleyTPF
3FPT
Totals
Black White Hispanic Asian PI
Native Other
Total 255,915 23,041 (9%)
111,941 (43.7%)
78,582 (30.7%)
28,721 (11.2%)
822 (0.3%)
12,808 (5%)
< 1 yr 13,104 (5%)
1,177 (0.5%)
5,374 (2.1%)
4,531 (1.7%)
1,730 (0.7%)
33 (0.01%)
259 (0.1%)
1-2 yrs 26,233 (10.3%)
2,176 (0.9%)
10,296 (4%)
9,036 (3.5%)
3,108 (1.2%)
45 (0.02%)
1,572 (0.6%)
3-5 yrs 40,138 (15.7%)
2,917 (0.9%)
17,007 (6.6%)
12,734 (5%)
3,885 (1.5%)
46 (0.02%)
3,549 (1.4%)
6-10 yrs 68,515 (26.8%)
5,926 (2.3%)
29,597 (11.6%)
21,442 (8.4%)
7,422 (2.9%)
209 (0.8%)
3,919 (1.5%)
11-15 yrs 75,597 (29.5%)
7,383 (2.9%)
34,322 (13.4%)
22,290 (8.7%)
8,732 (3.4%)
329 (0.1%)
2,541 (1%)
16-17yrs 32,328 (12.6%)
3,462 (1.4%)
15,345 (6%)
8,549 (3.3%)
3,844 (1.5%)
160 (0.06%)
968 (0.4%)
Percentages reflect ethnic group by age/total number of children < 17 years
Between 2002-2006, 432 children less than 14 years of age died in Contra Costa County; 23% of those deaths were associated with preventable injury. TPF
4FPT Among the national leading
causes of death the most common cause of death in Contra Costa County in all ages groups was unintentional injury, followed by assault/homicide. In 2005 unintentional injuries resulted in 429 injury hospitalizations in children less than 15 years of age. TPF
5FPT Overall the
Bay Area injury hospitalization rate has declined since 1993 by more than 25%. Bay Area injury prevention programs supported by EMS for Children and other injury prevention groups have certainly played a roll in this decline. However one disturbing trend noted over since 2000 has been the incidence of gang violence in West and East Counties. Violence has steadily increased in these communities resulting in an increase in pediatric victims. Injury prevention efforts directed at violence need to developed and supported in order to reduce this trend. Child Deaths in Contra Costa and Injuries 2002-2006TPF
6FPT
Age of Decedent All Injuries Homicide Unintentional Self Inflicted 0-14 years 86 21 62 1
<1 year 21 4 16 0
1-4 years 25 7 18 0
5-14 years 40 10 28 1
TP
3PT Needell, B., et.al. (2007). Child Welfare Services Reports for California, Retrieved 3/28/08, from
www.csssr.Berkeley.edu/CWSCMSreports TP
4PT Department for Health Services, Death Statistical Data, retrieved on 10/21/08 from www.applications .dhs.ca.gov/vsq
TP
5PT State of California Department of Public Health, EPIC branch, retrieved from Kidsdata.org on 10/21/08.
TP
6PT California Department of Public Health, Vital Statistics Death Statistical Master File, retrieved on 10/21/08 from
www.applications.dhs.ca.gov/epic
Contra Costa Emergency Medical Service Agency Page 20 EMS for Children Plan January 1, 2009
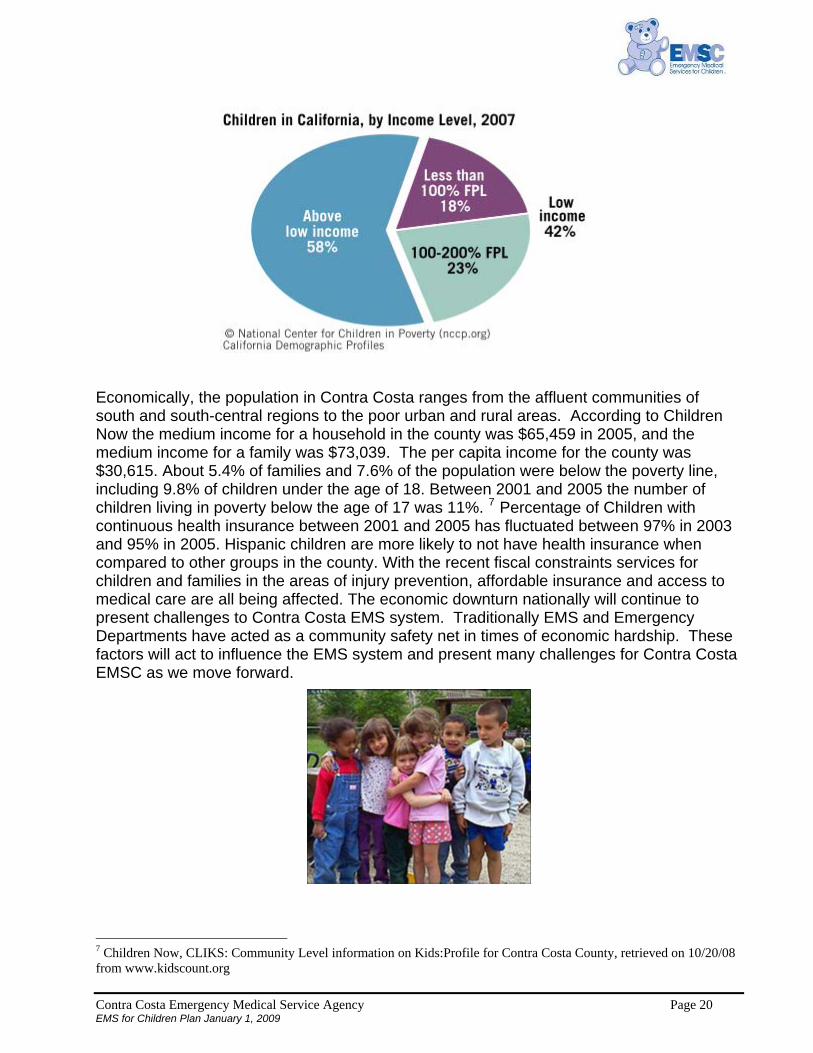
Economically, the population in Contra Costa ranges from the affluent communities of south and south-central regions to the poor urban and rural areas. According to Children Now the medium income for a household in the county was $65,459 in 2005, and the medium income for a family was $73,039. The per capita income for the county was $30,615. About 5.4% of families and 7.6% of the population were below the poverty line, including 9.8% of children under the age of 18. Between 2001 and 2005 the number of children living in poverty below the age of 17 was 11%. TPF
7FPT Percentage of Children with
continuous health insurance between 2001 and 2005 has fluctuated between 97% in 2003 and 95% in 2005. Hispanic children are more likely to not have health insurance when compared to other groups in the county. With the recent fiscal constraints services for children and families in the areas of injury prevention, affordable insurance and access to medical care are all being affected. The economic downturn nationally will continue to present challenges to Contra Costa EMS system. Traditionally EMS and Emergency Departments have acted as a community safety net in times of economic hardship. These factors will act to influence the EMS system and present many challenges for Contra Costa EMSC as we move forward.
TP
7PT Children Now, CLIKS: Community Level information on Kids:Profile for Contra Costa County, retrieved on 10/20/08
from www.kidscount.org

Contra Costa Emergency Medical Service Agency Page 21 EMS for Children Plan January 1, 2009
EMSC System Overview 2009 EMS Agency
The Contra Costa Health Services Emergency Medical Services Agency was established in 1983 and has provided leadership and support in the development of the EMS system for the county. The Agency is an integral part of the Contra Costa Health Services system. This system also includes the Contra Costa Regional Medical Center, the Contra Costa Health Centers, Community
Substance Abuse Services, the Contra Costa Health Plan, Environmental Health, Hazardous Materials Programs, Homeless Programs, Mental Health, and Public Health. The inclusion of all of these services under one umbrella has resulted in closer communication and integration of EMS services and other related County health care programs and activities. The EMS Agency is charged with the overall planning, implementation and evaluation of emergency medical services within Contra Costa County. The EMS Director, EMS Medical Director and Agency Staff carry out the EMS functions of Health Services. The EMS Medical Director has statutory responsibilities to oversee medical aspects of the EMS program. Emergency Medical Care Committee An Emergency Medical Care Committee (EMCC) provides advice regarding EMS matters to the Board of Supervisors, to Health Services and to the EMS Agency. This committee consists of representatives from 21 key participating system organizations, as well as, five consumers. The EMCC meets quarterly and all meetings of the EMCC and its subcommittees are open to the public. Prehospital Services
First responder services are provided by the County’s nine fire services, six of which provide paramedic level staffing to some or all of their units. One private and two fire service agencies provide emergency paramedic ambulance service to the County. Air ambulance services are available and provided primarily by CALSTAR and REACH, though additional services are available in surrounding counties.
Receiving Hospitals and Specialty Centers The EMS system further consists of nine receiving hospitals. John Muir Medical Center-Walnut Creek is the county's designated Level II Trauma Center and is also the base hospital providing on-line medical direction to the County’s paramedics. The County has also made provisions to treat critically ill and injured children by recognizing Children's Hospital Oakland as a Pediatric Trauma Center (PTC) and Pediatric Critical Care Center (PCCC).

Contra Costa Emergency Medical Service Agency Page 22 EMS for Children Plan January 1, 2009
V. 2009 EMSC for Children System Design and Resources ___________________________________________________________________________ Program Organization and Management The EMS Agency has the overall responsibility for planning, implementing, maintaining, and evaluating the EMS system and related programs, including the County EMSC Program. A member of agency's permanent staff is assigned oversight of the EMSC program. Responsibilities include coordinating program activities, and acting as the agency's liaison with the EMSC Task Force, system participants, the California EMS Authority and other groups interested in pediatric- related issues. 1. EMS for Children Advisory Committee
In 1999, the Contra Costa EMSC Task Force was appointed and served as the primary advisory group to the EMS Agency on issues related to pediatric emergency care, injury prevention, and other issues, during the Program's developmental and implementation stages. An EMSC Advisory Committee was established in 2000 to undertake the role and responsibility of advising the EMS Agency on EMSC program and system monitoring, evaluation and
maintenance. EMSC Advisory Committee membership consisted of representatives from key participants in the Contra Costa EMS and pediatric community. The EMSC coordinator in collaboration with the EMS Medical Director acts as the facilitator and coordinator for the group. The EMSC membership reviews EMSC issues electronically and the feedback is appropriately addressed and integrated as part of established standing EMS work groups. These EMS work groups include Quality Improvement, Medical Advisory Committee, East Bay Injury Prevention Network, Child Death Review, Fire EMS Training Consortium and Emergency Medical Care Committee of Contra Costa County. Secretarial and support services for the EMSC projects are to be provided by EMS Agency Staff. The EMSC Coordinator and EMSC Advisory activities have included:
• Adoption of State EMSC guidelines and standards for EMSC system components: Administration, Personnel, and Policy Guidelines for the Care of Pediatric Patients in the Emergency Department, Pediatric Critical Care and Trauma Consultation and Interfacility Transfer Guidelines
• Organization of EMSC consultation visits to all County emergency departments • Oversight of EMSC projects and activities • Review and revision of all pediatric-related ALS/BLS polices and treatment protocols • Participation in Contra Costa County prehospital education, and childhood injury and
illness prevention efforts
• Supporting the adoption of common standards in pediatric emergency assessment and training throughout the EMS system.
2. Facilities and Services Receiving Hospitals: • Contra Costa Regional Medical Center • Doctors Hospital, San Pablo

Contra Costa Emergency Medical Service Agency Page 23 EMS for Children Plan January 1, 2009
• John Muir Medical Center-Walnut Creek Campus • Kaiser Medical Center, Walnut Creek • Kaiser Medical Center, Richmond • Kaiser Medical Center, Antioch • John Muir Medical Center-Concord Campus • San Ramon Regional Medical Center • Sutter Delta Medical Center Base Hospitals: • John Muir Medical Center-Walnut Creek Trauma Center: • John Muir Medical Center- Walnut Creek
3. Pediatric Specialty Centers and Services Children's Hospital Oakland serves as the main pediatric referral center for Contra Costa County as well as other counties in Northern California. Pediatric trauma, critical care, and rehabilitation services are only a few of the specialized services offered at this facility. Shriner’s Hospital in Sacramento and Saint Francis Medical Center in San Francisco are receiving
facilities for burn patients. 4. Interfacility Linkages and Transfers EMTALA has eliminated the need for specific transfer agreements when the patient needs a higher level of care. To facilitate consistent, appropriate and orderly consultation and transfer of pediatric patients, Contra Costa 2008 Survey found that all facilities had policies or processes consistent with EMSC Interfacility Consultation and Transfer Guidelines. (Appendix) 5. Prehospital Care
First Responder Programs • Contra Costa County Fire Protection District • Crockett-Carquinez Fire Protection District • East Contra Costa Fire • Pinole Fire Department and Protection District • El Cerrito Fire Department • Richmond Fire Department • San Ramon Valley Fire Protection District • Rodeo-Hercules Fire Protection District • Moraga-Orinda Fire Protection District • East Bay Regional Parks Paramedic-First Responder Programs • Moraga-Orinda Fire Protection District • American Medical Response - Byron/Discovery Bay/Oakley and Crockett

Contra Costa Emergency Medical Service Agency Page 24 EMS for Children Plan January 1, 2009
• Contra Costa County Fire Protection District • San Ramon Valley Fire Protection District • El Cerrito Fire Department • Rodeo-Hercules Fire Protection District • Pinole Fire Department • California Highway Patrol Emergency Ambulance Providers • American Medical Response • San Ramon Valley Fire Protection District • Moraga-Orinda Fire Protection District Air Ambulance Providers • CALSTAR • REACH • Services available in surrounding counties include: Stanford Life Flight, Palo Alto;
UC Davis LIFE FLIGHT, Sacramento; Medi-Flight, Modesto; and Air Med Team, Stanislaus
Rescue Aircraft Providers • California Highway Patrol • East Bay Regional Parks • U.S. Coast Guard
6. Critical Illness and Injury Prevention Programs Injuries are a major cause of significant death and disability to children in our EMS system. This is well known to the stakeholders who have been active since 2000 in creating effective programs like “Every 15 Minutes” a nationally renowned program educating teens to the danger of driving under the influence creating “acted out” simulations of the deadly consequences for high schools throughout our community. The Contra Costa Trauma Program at John Muir
Medical Center-Walnut Creek leads this tremendously effective injury prevention effort. Injuries are a major cause of hospitalization in Contra Costa in children less than 18 years of age. Leading Causes of Hospitalized Non-fatal Injuries in Contra Costa County 0-18 years Top 5 Causes of Injury 2003 2004 2005 2006 Unintentional-Fall 233 238 212 164 Unintentional-MVT, Occupant 84 78 63 50 Homicide/Assault 58 60 60 61 Suicide/Self Inflicted 87 52 68 54 Unintentional-Struck by an object 49 51 32 40 Source: California Department of Public Health, Vital Statistics Death Statistical Master File, retrieved on 10/21/08 from www.applications.dhs.ca.gov/epic

Contra Costa Emergency Medical Service Agency Page 25 EMS for Children Plan January 1, 2009
From 1991-1997, a total of 104 youth ages 0-14 died from injuries in Contra Costa County, an average of 14.8 children per year. During 2002-2006 the average number of deaths associated with injury increased to15.8 per year. TPF
8FPT While these numbers are small they
represent preventable deaths in our EMS system and demonstrate the importance of the ongoing need for effective injury prevention activities. All stakeholders are involved in injury prevention in our system, however, many opportunities exist for improved injury prevention networking and coordination of activities. EMS has the opportunity to play a key role in supporting collaboration with injury prevention coalitions, networks and specialists throughout the system. The Contra Costa County EMSC Program participates with a number of local organizations and programs to promote childhood injury and illness activities. These include the East Bay Childhood Injury Prevention Network and Child Death Review. 7. Pediatric Rehabilitation Services
Children's Hospital Oakland has a pediatric rehabilitation service that has been approved by the Children's Services (CCS) Division of the California Department of Health Services. Children throughout Northern California are referred to Children's Hospital Oakland for rehabilitation. In addition, John Muir Medical Center is an approved CCS rehabilitation facility for children over the age of fourteen.
8. Public Education Public education is conducted by a number of entities in the county and works in tandem with injury prevention activities. The designated Pediatric and Adult Trauma Centers provide public injury prevention educational programs and activities. Historically, the fire services have also been active to promote fire-related injury prevention programs to the county's schools and the general public. With increasing numbers of medical and traumatic injury responses, fire agency injury prevention services have broadened beyond just fire safety. In the last five years the national recognition of childhood obesity as a factor in cardiovascular disease and diabetes risk has galvanized many in
our community to improve resources and information on the benefits of good nutrition and regular exercise. Contra Costa Health Services is a leader in our community supporting healthy lifestyle activities and programs.
Weight and Physical Fitness (7P
thP grade students meeting all fitness standards)
2003 2004 2005 2006 28.8% 32.3% 33.3% 31.5%
Source: Children Now: Contra Costa County Summary, retrieved on 10/20/08 from www.kids.data.org TP
8PT California Department of Public Health, Vital Statistics Death Statistical Master File, retrieved on 10/21/08 from
www.applications.dhs.ca.gov/epic

Contra Costa Emergency Medical Service Agency Page 26 EMS for Children Plan January 1, 2009
9. Professional Education Emergency ambulance service providers are responsible for assuring that paramedic employees have specialized training in caring for ill or injured pediatric patients. In addition, on-going continuing education in topics related to pediatrics is highly recommended though not mandated. In 2000 as part of the initial EMSC Program planning, the Pediatric Education for Prehospital Professionals (PEPP) course was introduced. This program received excellent evaluations and was adopted as the training standard for prehospital care providers since 2003. Since then, new programs such as Pediatric Advanced Life
Support (PALS) have come on to the scene and some stakeholders have required their providers to enhance their skills further by supporting tuition for attending these programs. EMS has a process of continuous review of training and works collaboratively with the Contra Costa Fire EMS Training Consortium to update and evaluate standards for prehospital pediatric training. Efforts to improve the standards in pediatric prehospital education will continue to be a focus for the EMSC program. Contra Costa EMSC recommends that pediatric continuing education for all levels of emergency department be consistent with the State EMSC guidelines Administration, Personnel, and Policy Guidelines for the Care of Pediatric Patients in the Emergency Department (EMSA # 182 revised in 2008). In addition, the Contra Costa County Trauma Center contract includes specific educational requirements for specialty services staff that are also consistent with State EMSC guidelines. 10. Quality Improvement and Evaluation Activities
Contra Costa EMS Quality Improvement program was approved by EMSA in April of 2008. This program is designed to fully integrate pediatric CQI throughout the EMS system using data analysis and supporting QA/QI activities of stakeholder agencies. CQI Programs currently exist at each of the emergency ambulance transport agencies and most first responder agencies as well as at Contra Costa County Fire Protection District, the County’s largest first responder agency.
In 2007 a comprehensive countywide EMS safety event reporting system was implemented based on best practices and provides mechanisms for timely reporting, review and appropriate corrective measures implemented. Identification of problem issues or system improvements can now be made at any level within the system including anonymously. These are communicated to EMS through prehospital care coordinators and the EMS Medical Director. Identified system issues that merit study or action are discussed at the Quality Improvement Committee. Action items and work groups are appropriately established as needed. The EMSC coordinator collaborates with appropriate groups to facilitate process improvement and support the development of programs, tools and resources for pediatric emergency care.

Contra Costa Emergency Medical Service Agency Page 27 EMS for Children Plan January 1, 2009
11. Coordination with Neighboring EMS Systems The EMSC program has worked closely with the California EMS Authority, and neighboring counties, in particular Alameda County, since its inception and is committed to continuing to do so. Currently our Trauma Advisory Committee is a Bi-County group providing trauma oversight in our system for both pediatric and adult trauma issues. Our EMSC program coordinator sits on the State EMSC Coordinator Committee as an active participant
and supports the States Annual EMSC conferences. State EMSC coordinators have been active in updating the State EMSC prehospital treatment guidelines and supporting many other collaborative EMSC projects. Contra Costa EMSC is an active participant in the East-Bay Childhood Injury Prevention Network.
Contra Costa Emergency Medical Service Agency Page 28 EMS for Children Plan January 1, 2009
VI. EMSC 2009 Program Monitoring and Evaluation ___________________________________________________________________________ General EMSC Coordinator in conjunction with the EMS Medical Director oversees activities of the EMSC Program. Pediatric Quality Improvement activities are integrated into the Agency's EMS QI Program. The EMSC Advisory Committee provides consultation as part of these activities on an ongoing basis. Protocols, guidelines and other EMSC products will be reviewed in accordance with the Agency's scheduled reviews to ensure that pediatric-related practices remain evidence-based and responsive to the needs of the county's children and system participants. An EMSC Program report will be provided to the California Emergency Medical Services Authority at appropriate intervals. EMSC System Components 1. Emergency Departments
ED Guidelines and Consultation Visits In 2000 Contra Costa EMS created separate ED guidelines for EMSC to facilitate implementation. Upon review of those guidelines and the states updated 2008 guidelines it was found that it was no longer necessary to create and maintain a separate guideline document. Effective 2007 Contra Costa EMSC adopted the State EMSC guidelines as the model to evaluate the pediatric emergency preparedness in our community.
The EMSC Coordinator will review State EMSA Emergency Department Guidelines and update the Contra Costa EMSC Emergency Department self-assessment tool at appropriate intervals. The EMSC coordinator will advise the EMS Agency of any suggestions or recommendations that should be presented to the receiving facilities on an ongoing basis. A facility self-assessment tool will be developed and updated by the EMSC coordinator based on the document “ Administration, Personnel and Policy for the Care of Pediatric Patients in the Emergency Department” (EMSA # 182 guideline). It is recommended that the survey be conducted at minimum with each update of the EMSA (#182) guidelines. Facility consultations should be conducted with each EMSA update and on an as needed basis. The EMS Agency staff member assigned the EMSC Project will be responsible for the scheduling of ED consultation visits and may engage the services of pediatric specialists to participate in these consultations.
2. Prehospital Pediatric Field Care Protocols Maintaining standards in Prehospital pediatric care is a critical function of the EMSC program. Protocols will continue to be monitored on an ongoing basis. EMSC Advisory members and other stakeholders may make recommendations at any time. Protocols will be reviewed annually or as needed. Recommendations for changes will be submitted to EMS Agency for consideration.

Contra Costa Emergency Medical Service Agency Page 29 EMS for Children Plan January 1, 2009
Prehospital Equipment and Supplies Pediatric equipment and supplies will be reviewed with any update of State or National EMSC equipment guidelines. They will also be reviewed in conjunction with changes to pediatric field treatment protocols or as determined by the EMSC Coordinator working with constituent advisory groups. Recommendations for changes will be submitted to EMS Agency for consideration.
Prehospital Pediatric Education
Since 2003 Contra Costa EMS has required current PEPP course certification of all prehospital providers. PEPP will continue to be the foundation of county prehospital provider training. The EMS will evaluate new pediatric
courses for opportunities to improved prehospital training in pediatric populations on an ongoing basis. Specific educational programs in addition to PEPP may be identified and developed based on needs identified through the Contra Costa Quality Improvement Program.
3. Specialty Centers Contra Costa County will continue its recognition and work collaboratively with Children's Hospital Oakland as the system's primary pediatric critical care and trauma center. Joint reviews with Alameda County EMS are part of our Trauma Review Process. The EMS Agency will periodically review the availability and location of other specialty care for pediatric patients.
4. Data Collection Computerized EMS data collection in Contra Costa is implemented and in use. Contra Costa EMS has a required data set that is consistent with CEMSIS. Contra Costa EMS data standards will use and collaborate with the State EMSC in the refinement of prehospital data standards for pediatrics and pediatric trauma.
5. Quality Improvement
Pediatric QI is integrated into the Contra Costa Quality Improvement Program. EMS stakeholders actively participate on all levels. EMS works collaboratively with stakeholders to support and implement pediatric EMS system performance through annual review and update of prehospital pediatric protocols. EMS staff participate in prehospital and emergency department pediatric education and training regularly. Stakeholders are

Contra Costa Emergency Medical Service Agency Page 30 EMS for Children Plan January 1, 2009
welcome to send comments and make recommendations to EMS through formal and informal communications. Plans and outcomes of pediatric QI activities are routinely communicated to the EMSC Advisory Group, Medical Advisory Committee and EMCC at appropriate intervals. Pediatric safety reporting is also integrated into EMS CQI program reports.
6. Illness and Injury Prevention
Contra Costa EMS continues to support and promote quality pediatric emergency care and injury prevention throughout the county. This includes collaborating with the East Bay Childhood Injury Prevention Network and other existing programs to promote the prevention of childhood illness' and injuries throughout the county and state. EMS will continue to be an active participant with assigned staff to the Child Death Review Committee.

Contra Costa Emergency Medical Service Agency Page 31 EMS for Children Plan January 1, 2009
VII. 10 Key Next Steps for Contra Costa EMSC
Contra Costa EMSC in the next 3-5 years will:
1. Support timely communication and feedback among EMSC system stakeholders through email, newsletters and outreach visits with stakeholders.
2. Support networking and collaboration among EMSC system stakeholders by
providing opportunities for participation and collaboration on local, state and national EMSC issues.
3. Maintain a current list of EMSC Champions and support activities within the
resources of the Local EMS agency.
4. Identify and distribute information and resources to improve stakeholder and public access to resources on pediatric injury prevention and childhood emergencies.
5. Explore and establish opportunities for joint stakeholder pediatric emergency
training.
6. Improve pediatric simulation training opportunities within EMS Local resources.
7. Maintain and support ongoing pediatric prehospital continuing education through curriculum development and the development and implementation of pediatric training standards for pediatric emergency assessment (ACDA) and pediatric trauma & medical protocols.
8. Evaluate innovative equipment and tools to increase safety and improve pediatric
prehospital care.
9. Maintain staff support for participation in local, state and regional EMSC activities.
10. Identify and distribute EMS stakeholder resources in the care for children in a disaster.
Contra Costa Emergency Medical Service Agency Page 32 EMS for Children Plan January 1, 2009
VIII. Appendices ___________________________________________________________________________
I. EMSC Advisory Group Stakeholder List J. EMS Plan Update Process: Activity Timeline K. 2009 Pediatric Field Treatment Notes and Protocols L. ALS/BLS Equipment EMSC equipment survey and updated equipment lists M. Contra Costa County Paramedic Accreditation Policy N. Emergency Department Consultation Visit Survey tool and survey results O. Contra Costa County Injury Prevention Resource List


Northern California EMS, Inc. EMS for Children Plan November, 1998
Appendix A: Acknowledgements: EMS for Children Advisory Group
Joe Barger MD Medical Director Contra Costa EMS
Art Lathrop Director Contra Costa EMS
Lauren Kovaleff RN Assistant Director EMS Contra Costa EMS
Pat Frost RN, MS, PNP EMSC Coordinator Contra Costa EMS
Pam Dodson RN Prehospital Care Coordinator Contra Costa EMS
Jim Betts MD Trauma Surgeon Children’s Hospital Medical Center Oakland
Stacey Hanover RN ED Director Children’s Hospital Medical Center Oakland
Kacey Hansen RN Trauma Coordinator John Muir Medical Center Walnut Creek
Nancy Daniel RN QI Coordinator Moraga Orinda Fire
Greg Sekera EMT-P QI Coordinator Pinole Fire
Ellen Leng MD ED Physician & EMCC Chair John Muir Medical Center Walnut Creek
Lori Altabet RN Base Coordinator John Muir Medical Center Walnut Creek
Karen Hamilton RN, CES AMR Contra Costa County
Dave George EMT-P Captain Contra Costa Fire
Dawn Reis RN ED Manager Kaiser Antioch
Paul Harper EMT-P CES AMR Contra Costa County
Keith Cormier EMS Chief Contra Costa Fire
Randy Lyman QI Coordinator REACH
Renee Juster RN ED Director John Muir Medical Center Concord
Monica Teves EMT-P AMR Contra Costa County
Judy Smith RN Trauma Coordinator Contra Costa EMS
Paul Naas QI Coordinator CALSTAR
Jay Colas RN ED Manager Kaiser Walnut Creek
Peter Fromm RN InterimED Director Contra Costa Regional Medical Center
Sam Bradley EMT-P QI Coordinator East Contra Costa Fire
Maria Beza RN Interim ED Director San Ramon Regional Medical Center
Andy Swartzell RN QI Coordinator San Ramon Valley Fire
Chris Eberle RN EMS Training Coordinator San Ramon Valley Fire
Jeff Burris EMT-P EMS Chief East Contra Costa Fire
Phyllis McClanahan RN ED Director Sutter Delta Medical Center
Gary Hashimoto MD ED Director Kaiser Walnut Creek
Jeanne Mills RN QI Coordinator Contra Costa Fire
Chuck Coleman EMT-P QI Coordinator Rodeo-Hercules Fire
Terri Pillow-Noriega RN ED Director Kaiser Richmond
Jim Carpenter MD Chair Child Death Review Contra Costa Health Services
Susan Ancell RN ED Director Doctors San Pablo Medical Center
Dave Gibson EMT-P EMS Chief El Cerrito Fire
Nancy Baer MSW Manager Injury Prevention & Physical Activity Promotion Projects. Contra Costa Health Services
Amy Buoncristiani MD ED Physician EMSC Liaison Physician Contra Costa Regional Medical Center
Cathy Seithel RN ED Nurse Educator Kaiser Walnut Creek
Greg Kennedy RN QI Coordinator Contra Costa Fire
Bob Buehl MD ED Medical Director San Ramon Regional Medical Center
Anita Fligge RN, MSN,CEN,MICN ED Nurse Educator Pediatric Liaison Nurse John Muir Medical Center Walnut Creek
Ross Fay Program Director CALSTAR
Hope Freidman RN Outreach Nurse Children’s Hospital and Medical Center Oakland
Charlene Boyer RN Director of Emergency Services Kaiser Walnut Creek
Jenna Timm MD Pediatric Liaison Physician Kaiser Richmond
Julie Crouse RN Director of Emergency Services John Muir Medical Center Walnut Creek

Northern California EMS, Inc. EMS for Children Plan November, 1998
EMS for Children Advisory Group (continued)
Jack Choi MD ED Physician & Pediatric Liaison Physician Kaiser Walnut Creek & Kaiser Antioch
Bev Jacobs Director of Clinical Programs Contra Costa Health Plan
Bev Jones Senior VP for Patient Care Services John Muir Medical Center Walnut Creek
William Mills MD Pediatric Liaison Physician John Muir Medical Center Walnut Creek
Lowry Mitchell, RN Emergency Services Director Kaiser Antioch/Diablo Service Area
Vicki Loftquist RN, MS,PNP Clinical Nurse Specialist & Pediatric Nurse Manager San Ramon Regional Medical Center
Kathy O’Brien Director of Regulatory Compliance Kaiser Walnut Creek
Sean Russell Program Director REACH
Bernice Rodriguez MD ED Physician & Pediatric Liaison Physician John Muir Medical Center Walnut Creek
Dr. Khoury MD ED Medical Director John Muir Medical Center Walnut Creek
Desmond Carson MD ED Medical Director Doctors Medical Center San Pablo
Mary Shaw RN Executive Director Nursing Doctors Medical Center San Pablo
Laurel Hodgson MD ED Assistant Medical Director Doctors Medical Center San Pablo
Robert Mooney MD ED Physician Kaiser Walnut Creek
Michael Lucas MD ED Physician Kaiser Antioch
Keith Harris RN Pediatric Liaison Nurse Kaiser Antioch
Pam Pshea Chief Nursing Officer San Ramon Regional Medical Center
Nicholas Giardini MD Director Pediatric Hospitalist San Ramon Regional Medical Center
David Birdsall MD ED Medical Director John Muir Medical Center Concord
Jeff Leinan MD ED Medical Director Sutter Delta Medical Center
Dr. Sen MD Chief Pediatric Hospitalist Sutter Delta Medical Center
Richard Leahy MD ED Medical Director Kaiser Richmond
David Goldstein MD ED Medical Director Contra Costa Regional Medical Center
Noel Luiz EMT-P Captain/Paramedic Contra Costa County Fire
Leslie Mueller Director of Operations AMR Contra Costa County
Adriene Clark-Wilkenson RN Nurse Educator Sutter Delta Medical Center Assistant Nurse Manager Kaiser Antioch
Rebecca Rozen Regional Vice President Hospital Council of Northen California
Gene Hern MD Medical Director AMR Contra Costa County
Alvin Tang MD ED Physician Kaiser Richmond
Constance Donovan RN ED Program Manager Contra Costa Regional Medical Center
Jen Gossett RN ED Informatics Nurse Contra Costa Regional Medical Center
Dr. Sen Pediatric Hospitalist Sutter Delta Medical Center
This document has been prepared and is respectfully submitted by
Pat Frost RN, MS, PNP EMS for Children Coordinator
Quality Improvement Coordinator Contra Costa Emergency Medical Services
Questions and comments should be submitted to [email protected]

Appendix B
EMSC Plan Update Process
Activity Timeline


1/1/
2007
1/30
/200
9
Act
ivity
Tim
elin
e
7/1/
2007
EM
SC
Adv
isor
y G
roup
Re-
iden
tifie
d &
Sta
keho
lder
s in
form
ed o
f up
date
pro
cess
The
EM
SC
Adv
isor
y C
omm
ittee
con
sist
s of
mul
tidis
cipl
inar
y re
pres
enta
tives
from
the
Con
tra C
osta
EM
S &
ped
iatri
c co
mm
unity
.Th
e co
mm
ittee
act
s to
revi
ew a
nd s
uppo
rt th
e C
ontra
Cos
ta C
ount
y E
MS
C p
rogr
am.
The
com
mitt
ee w
as fo
rmed
in 1
999
to
deve
lop
the
2002
Con
tra C
osta
EM
S P
lan.
Mem
bers
hip
incl
udes
med
ical
and
nur
sing
repr
esen
tativ
es fr
om re
ceiv
ing
hosp
itals
, ped
iatri
cian
s an
d pe
diat
ric e
mer
genc
y an
d tra
uma
depa
rtmen
t exp
erts
, pre
-hos
pita
l firs
t res
pond
er a
nd tr
ansp
ort a
genc
ies
and
inte
rest
ed c
omm
unity
gro
ups.
Th
e co
mm
ittee
is c
oord
inat
ed b
y an
EM
SC
coo
rdin
ator
in c
olla
bora
tion
with
the
EM
S M
edic
al D
irect
or. I
n 20
07 th
e E
MS
C A
dvis
ory
Com
mitt
ee w
as re
-est
ablis
hed
and
revi
ews
issu
es e
lect
roni
cally
. EM
SC
Adv
isor
y fe
edba
ck is
app
ropr
iate
ly a
ddre
ssed
and
inte
grat
edas
par
t of e
stab
lishe
d st
andi
ng E
MS
wor
k gr
oups
. The
se in
clud
e Q
ualit
y Im
prov
emen
t, Fa
cilit
ies
Crit
ical
Car
e C
omm
ittee
, Med
ical
A
dvis
ory
Com
mitt
ee, C
ontra
Cos
ta/A
lam
eda
Chi
ld P
reve
ntio
n N
etw
ork,
Chi
ld D
eath
Rev
iew
, Con
tra C
osta
Cou
nty
Fire
-EM
S C
onso
rtium
an
d th
e E
mer
genc
y M
edic
al C
are
Com
mitt
ee o
f Con
tra C
osta
Cou
nty.
3/25
/200
8S
take
hold
er
PE
AR
S
prev
iew
2/23
/200
7C
CE
MS
EM
SC
C
oord
inat
or d
esig
nate
d
1/31
/200
8-4
/30/
2008
EM
SC
Pla
n S
take
hold
er
Re-
educ
atio
n &
Pub
lic C
omm
ent P
erio
d
3/29
/200
820
08 E
MSA
Equ
ip G
uide
lines
st
akeh
olde
r dis
tribu
tion
and
Ped
i inf
o re
ques
tdu
e 4/
30/0
83/27
/200
8C
CE
MS
Ped
i Tra
nsfe
r G
uide
lines
doc
re
view
to
advi
sory
par
ticip
ants
du
e 4/
30/0
8
4/2/
2008
ED
Sel
f Ass
essm
ent
Dis
tribu
ted
Dea
dlin
e 8/
1/08
8/1/
2008
ED
EM
SC
O
n-si
te s
urve
ype
riod
begi
ns
3/3/
2008
Ped
i Cou
rse
Com
paris
on D
evel
oped
fo
r sta
keho
lder
s1/23
/200
8E
MS
A A
nnua
lE
MS
C C
onfe
renc
e
1/26
/200
8-3
/13/
2008
NE
DA
RC
Sur
vey
Par
ticip
atio
n
3/23
/200
7-6
/11/
2007
Sta
te E
MSC
CQ
I In
dica
tor S
tudy
P
artic
ipan
t
8/1/
2007
CA
EM
SC
C
oord
inat
or M
tg
4/9/
2008
CA
EM
SC
per
form
ance
m
easu
re &
ped
i pro
toco
l in
put s
ubm
itted
1/7/
2008
EM
SC
web
reso
urce
s ad
ded
to E
MS
web
site
3/1/
2007
-1/3
0/20
0820
02 E
MS
C p
lan
docu
men
ts a
nd in
trodu
ctor
y si
te v
isits
con
duct
ed
9/1/
2008
ED
Sta
keho
lder
s E
MS
C
surv
ey d
ata
com
pile
d
1/30
/200
9E
MS
C p
lan
& re
port
Subm
itted
for
stat
e ap
prov
al
11/1
1/20
08M
AC
pre
sent
atio
n
10/1
/200
8-1
/15/
2009
Loca
l EM
SC
Pla
n ap
prov
al p
erio
d
6/11
/200
8E
MC
C re
port
EM
SC
up
date
pro
cess
12/1
1/20
08E
MC
C p
rese
ntat
ion
3/2/
2008
-8/6
/200
8S
tate
EM
SC
Pro
toco
l Rev
iew
7/7/
2008
MA
C p
edi e
quip
upda
te in
put
12/9
/200
8E
MS
C S
ite
Vis
its C
ompl
ete
10/1
/200
8E
MS
C G
uide
lines
18
1 &
183
D
istri
bute
d to
st
akeh
olde
rs fo
r com
men
t
12/1
/200
818
1 &
183
Gui
delin
e co
mm
ents
to
EM
SA
11/4
/200
8-1
2/4/
2008
EM
SC
Pla
n P
ublic
Com
men
t

Appendix C
Contra Costa Emergency Medical Services
2009
Pediatric Field Treatment Notes
And
Protocols


2008
-200
9 C
ompa
riso
n of
Ped
iatr
ic P
re-h
ospi
tal P
roto
cols
/Pro
cedu
res/
Gui
delin
es
Nat
iona
l, St
ate,
and
Con
tra
Cos
ta C
ount
y N
atio
nal
Stat
e C
ontr
a C
osta
Cou
nty
Gen
eral
pat
ient
car
e Pe
diat
ric p
rimar
y su
rvey
P1
:Rou
tine
Med
ical
Car
e
PHC
M: N
otes
on
Pedi
atric
Pat
ient
s Tr
aum
a Pe
diat
ric tr
aum
a B
lunt
trau
ma
Pene
tratin
g tra
uma
P14:
Tra
uma
patie
nts (
high
risk
) P1
5: M
inor
Tra
uma
P1
6: T
raum
atic
Arr
est
Bur
ns
Pedi
atric
bur
ns
Ther
mal
El
ectri
cal
Che
mic
al
P17:
Bur
ns
PHC
M: N
otes
on
Bur
ns
Fore
ign
body
airw
ay o
bstru
ctio
n Pe
diat
ric re
spira
tory
dis
tress
U
pper
airw
ay o
bstru
ctio
n Lo
wer
airw
ay o
bstru
ctio
n N
on o
bstru
ctiv
e
P12:
Airw
ay O
bstru
ctio
n PH
CM
: ALS
Not
es
Res
pira
tory
dis
tress
, fai
lure
, or a
rres
t Pe
diat
ric re
spira
tory
dis
tress
U
pper
airw
ay o
bstru
ctio
n Lo
wer
airw
ay o
bstru
ctio
n N
on o
bstru
ctiv
e
P13:
Acu
te re
spira
tory
dis
tress
; Cro
up/E
pigl
ottis
, A
cute
Ast
hma/
Bro
ncho
spas
m
Res
pira
tory
Dis
tress
in th
e ch
ild o
n ve
ntila
tory
supp
ort
PH
CM
: ALS
Not
es
Res
pira
tory
dis
tress
in th
e ch
ild w
ith a
tra
cheo
stom
y
PHC
M: A
LS N
otes
Bro
ncho
spas
m
P1
3: A
cute
resp
irato
ry d
istre
ss; C
roup
/Epi
glot
tis,
Acu
te A
sthm
a/B
ronc
hosp
asm
N
ewbo
rn re
susc
itatio
n N
eona
tal r
esus
cita
tion
P2: N
eona
tal R
esus
cita
tion
Bra
dyca
rdia
Pe
diat
ric b
rady
card
ia
P4: B
rady
card
ia
Tach
ycar
dia
Pedi
atric
tach
ycar
dia
P5: T
achy
card
ia S
tabl
e, u
nsta
ble
SVT
Poss
ible
V
Tach
N
on-tr
aum
atic
car
diac
arr
est
Pedi
atric
car
diac
arr
est
Asy
stol
e/PE
A; V
Fib/
Puls
eles
s Vta
ch
P3:C
ardi
ac a
rres
t- no
n-tra
umat
ic; s
ectio
n Pr
imar
y th
erap
y
Vas
cula
r Acc
ess:
Intra
osse
ous
PH
CM
: ALS
Not
es
PFro
st E
MS
QI
Page
1
12/2
3/20
08

Nat
iona
l St
ate
Con
tra
Cos
ta C
ount
y V
entri
cula
r fib
rilla
tion
or p
ulse
less
ve
ntric
ular
tach
ycar
dia
Pedi
atric
car
diac
arr
est
Asy
stol
e/PE
A
VFi
b/Pu
lsel
ess V
tach
P3: C
ardi
ac a
rres
t - n
on-tr
aum
atic
; sec
tion
Ven
tricu
lar f
ib/p
ulse
less
VTa
ch
Asy
stol
e an
d pu
lsel
ess e
lect
rical
act
ivity
Pe
diat
ric c
ardi
ac a
rres
t A
syst
ole/
PEA
; VFi
b/Pu
lsel
ess V
tach
P3
: Car
diac
arr
est -
non
-trau
mat
ic; s
ectio
n A
syst
ole
& P
EA
Alte
red
men
tal s
tatu
s Pe
diat
ric a
ltere
d le
vel o
f co
nsci
ousn
ess
P7: A
ltere
d le
vel o
f con
scio
usne
ss
Seiz
ures
Pe
diat
ric se
izur
es
P8: S
eizu
res
Non
-trau
mat
ic h
ypop
erfu
sion
(sho
ck)
Pedi
atric
shoc
k P6
: Hyp
oten
sion
/sho
ck
Ana
phyl
actic
shoc
k/al
lerg
ic re
actio
n Pe
diat
ric a
llerg
ic re
actio
n/ a
naph
ylax
is
P10:
Ana
phyl
axis
/alle
rgic
reac
tion
P11:
Ana
phyl
actic
Sho
ck
Ana
phyl
actic
shoc
k tre
ated
with
aut
o-in
ject
or d
evic
e
NA
: Aut
o-in
ject
ors n
ot p
art o
f loc
al sc
ope
Toxi
c ex
posu
re
Pedi
atric
toxi
c ex
posu
re
P9: P
oiso
ning
N
ear-
drow
ning
Pe
diat
ric N
ear-
drow
ning
N
o cu
rren
t PH
CG
Pedi
atric
Env
ironm
enta
l em
erge
ncie
s H
ypot
herm
ia
Hea
t illn
ess
Loca
l col
d in
jury
No
curr
ent P
HC
G
Pain
man
agem
ent
Pedi
atric
Pai
n A
sses
smen
t and
M
anag
emen
t P1
9: P
ain
Man
agem
ent (
nont
raum
atic
) PH
CM
: Pai
n ev
alua
tion
and
treat
men
t le
ngth
-bas
ed c
olor
cod
ed m
edic
atio
n ca
rds
Dea
th o
f a c
hild
No
curr
ent P
HC
G
Polic
y: D
eter
min
atio
n of
Dea
th
Pe
diat
ric B
ehav
iora
l Em
erge
ncie
s (n
ew 2
009
ID)
No
curr
ent P
HC
G
A
LTE
(new
200
9 ID
) P1
8: A
LTE/
Nea
r mis
s SID
S
Chi
ld A
buse
& N
egle
ct
(new
200
9 ID
) N
o cu
rren
t PH
CG
Po
licy:
Abu
se a
nd A
ssau
lt re
porti
ng
ID=
In d
evel
opm
ent
PFro
st E
MS
QI
Page
2
12/2
3/20
08












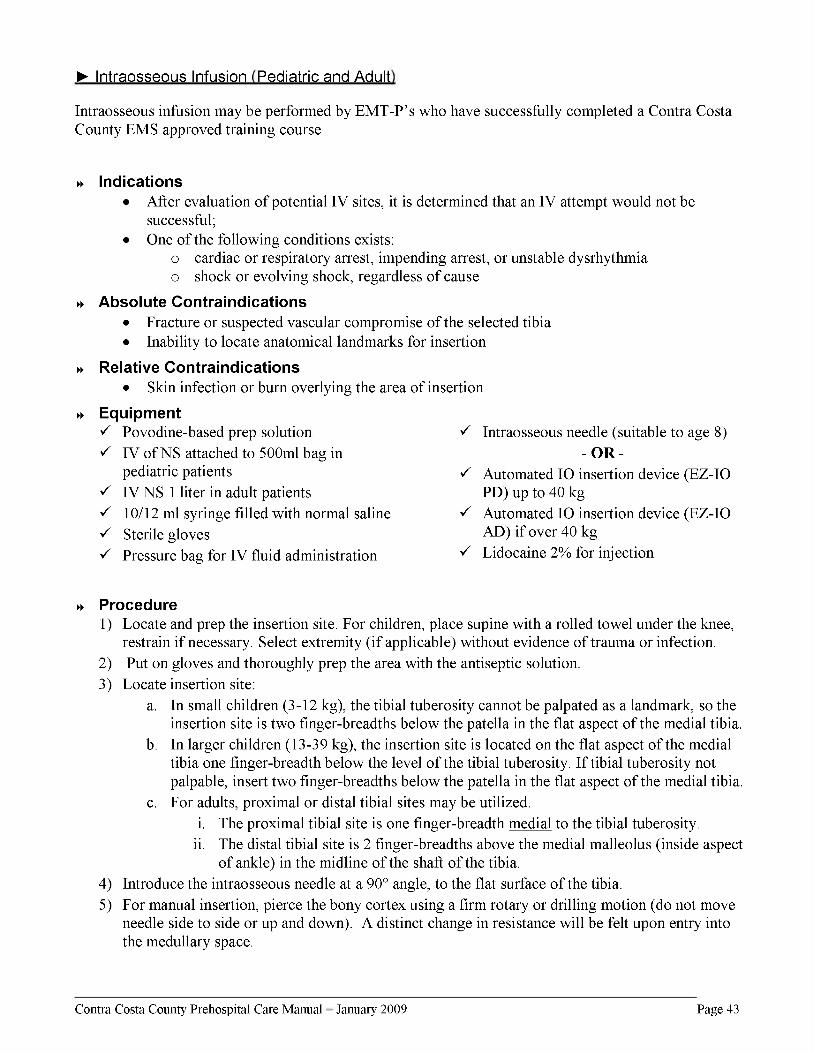






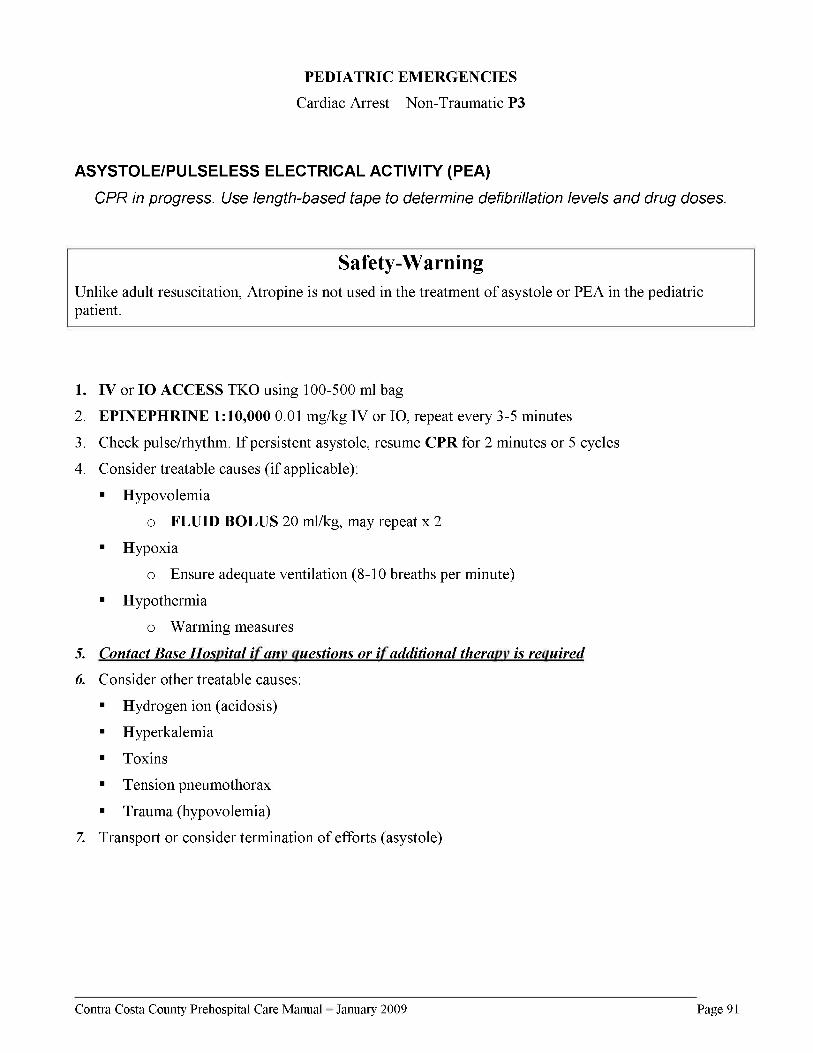



















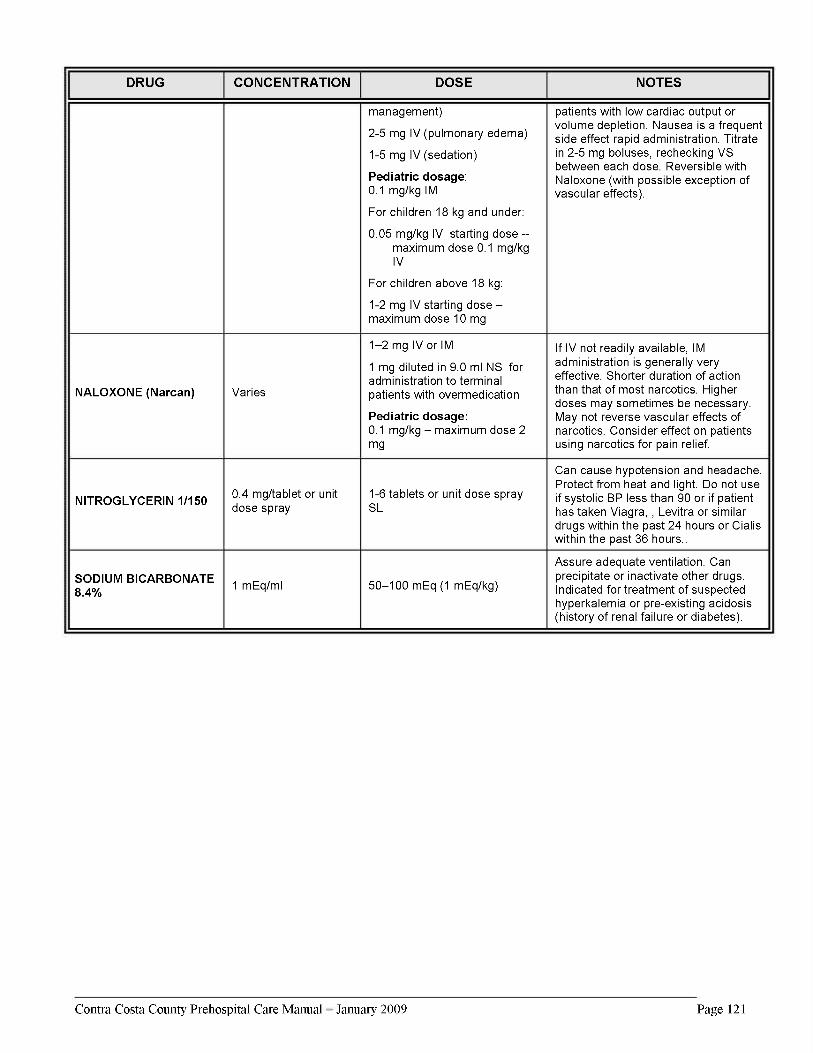










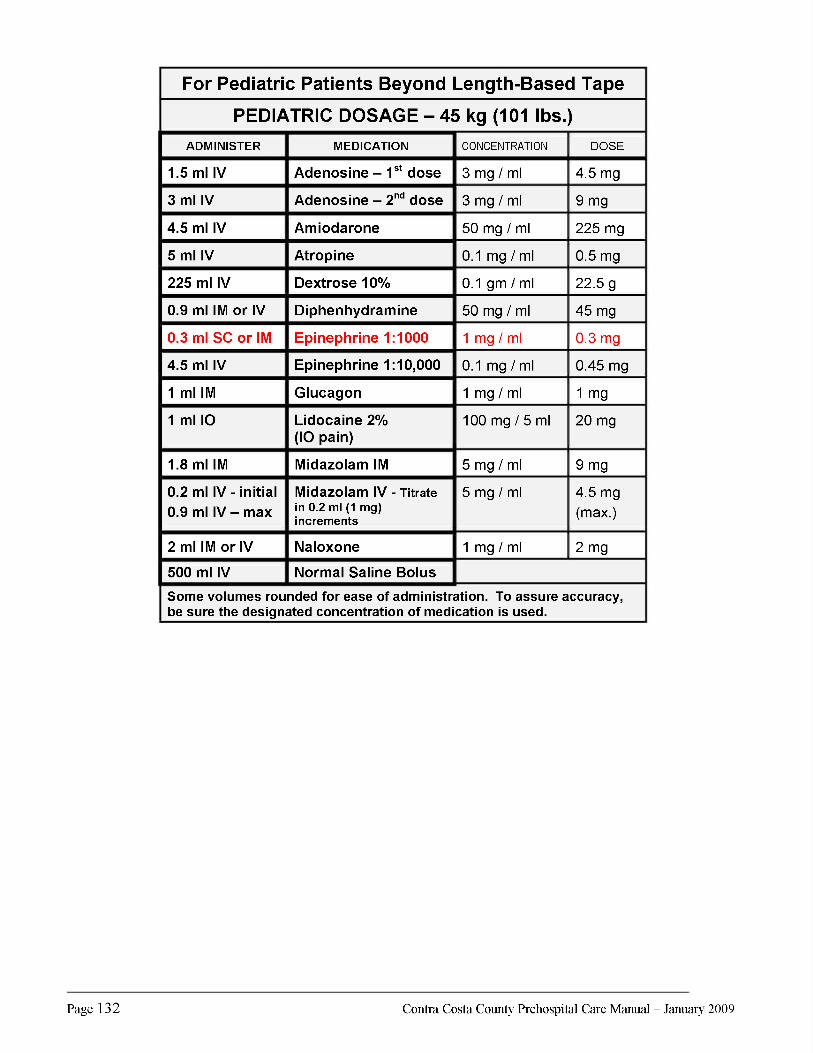


Appendix D
Prehospital
ALS/BLS Equipment
Survey Summary
and
Updated Equipment Lists


Con
tra
Cos
ta E
mer
genc
y M
edic
al S
ervi
ces
EM
S Fo
r C
hild
ren
Prog
ram
Ped
iatr
ic E
quip
men
t Lis
t Rev
iew
20
08 P
reho
spita
l Equ
ipm
ent L
ist A
sses
smen
t and
Upd
ate
Rec
omm
enda
tions
As p
art o
f Con
tra
Cos
ta 2
008
EM
S fo
r C
hild
ren
(EM
SC) u
pdat
e pr
oces
s, an
ass
essm
ent w
as d
one
of th
e pr
ehos
pita
l pro
vide
rs p
edia
tric
equ
ipm
ent.
The
follo
win
g ite
ms w
ere
iden
tifie
d as
NO
T p
art o
f 200
7 C
ontr
a C
osta
’s m
anda
tory
BL
S/A
LS
Prov
ider
equ
ipm
ent l
ist.
This
list
of i
tem
s was
com
pile
d af
ter c
ompa
ring
our
Loca
l EM
S Eq
uipm
ent L
ist t
o up
date
d 20
08 re
com
men
datio
ns o
f the
Cal
iforn
ia E
MSC
Tec
hnic
al A
dvis
ory
Com
mitt
ee a
nd N
atio
nal E
MSC
gui
delin
es.
Alth
ough
man
y of
thes
e ite
ms w
ere
not o
n ou
r cur
rent
cou
nty
EMS
equi
pmen
t lis
t, it
was
kno
wn
that
maj
ority
of i
tem
s wer
e al
read
y in
use
thro
ugho
ut o
ur E
MS
syst
em.
Surv
ey P
roce
ss: A
ped
iatri
c eq
uipm
ent s
urve
y w
as c
ondu
cted
am
ong
a re
pres
enta
tive
sam
ple
of C
ontra
Cos
ta
preh
ospi
tal p
rovi
der g
roup
s. Th
ese
grou
ps in
clud
ed a
mbu
lanc
e ba
sed
trans
port
BLS
/ALS
pro
vide
r: A
MR
, firs
t re
spon
der f
ire B
LS/A
LS p
rovi
der:
Con
tra C
osta
Fire
and
com
bine
d fir
e fir
st re
spon
der a
nd tr
ansp
ort p
rovi
der:
San
Ram
on V
alle
y Fi
re.
Each
age
ncy
revi
ewed
thei
r cur
rent
equ
ipm
ent a
nd a
nsw
ered
the
follo
win
g qu
estio
ns.
This
in
form
atio
n w
as th
en u
sed
to u
pdat
e an
d re
vise
to o
ur lo
cal E
MS
equi
pmen
t lis
t for
BLS
/ALS
pro
vide
rs.
1.
Doe
s you
r ag
ency
alr
eady
car
ry th
is it
em(s
) eve
n if
it is
not
spec
ified
on
our
equi
pmen
t lis
t? If
so
plea
se sp
ecify
wha
t siz
es y
ou d
o ca
rry
if di
ffer
ent t
han
wha
t is o
n st
ated
. 2.
If t
he e
quip
men
t ite
m is
not
one
cur
rent
ly c
arri
ed is
ther
e a
need
to c
arry
this
pie
ce o
f equ
ipm
ent?
C
onsi
der
cost
and
freq
uenc
y of
use
as t
he m
ajor
fact
ors i
n yo
ur r
ecom
men
datio
ns.
3.
If y
ou d
o no
t rec
omm
end
carr
ying
an
item
stat
e yo
ur r
atio
nale
. As p
art o
f the
upd
ate
of o
ur E
MSC
pl
an if
var
iatio
ns e
xist
from
the
stat
e re
com
men
datio
ns it
is n
eces
sary
to c
aptu
re th
e re
ason
s why
. Pa
t Fro
st E
MSC
Coo
rdin
ator
Pa
ge 1
12
/30/
2008

Con
tra
Cos
ta E
mer
genc
y M
edic
al S
ervi
ces
EM
S Fo
r C
hild
ren
Prog
ram
Ped
iatr
ic E
quip
men
t Lis
t Rev
iew
20
08 P
reho
spita
l Equ
ipm
ent L
ist A
sses
smen
t and
Upd
ate
Rec
omm
enda
tions
EM
SC p
rogr
am 2
008
pedi
atri
c ad
ditio
ns to
Con
tra
Cos
ta E
MS
BL
S/A
LS
equi
pmen
t lis
ts a
re n
oted
in th
e la
st c
olum
n.
Pe
di E
quip
men
t not
list
ed o
n ou
r re
quire
d cu
rren
t man
dato
ry E
MS
equi
pmen
t lis
t for
BLS
/ALS
pro
vide
rs.
Item
s ar
e no
ted
as c
omin
g fro
m B
LS o
r A
LS s
tate
/nat
iona
l gui
delin
es
Che
ck if
car
ry n
ow
2008
EM
SC U
pdat
e R
ecom
men
datio
ns
M=
Man
dato
ry L
ist A
dditi
on
N=N
ot re
com
men
ded
ratio
nale
incl
uded
SR
VFPD
CC
CFP
DA
MR
Late
x fr
ee e
quip
men
t?
Y Y
Y M
(B
LS) P
edi N
asop
hary
ngea
l airw
ays
(fren
ch)
18,2
0,22
,24,
26 A
re a
ll si
zes
avai
labl
e an
d in
us
e?
Y Y
Y M
(BLS
) Por
tabl
e su
ctio
n w
ith re
gula
tor h
igh/
low
se
tting
s (lo
w s
ettin
gs m
ay b
e ap
prop
riate
for
pedi
-all
prov
ider
s ha
ve b
ut n
eed
to s
peci
fy
to m
eet s
tate
gui
delin
es)
Y Y
Y M
(BLS
) Sph
ygm
oman
omet
er o
r oth
er B
/P
mea
surin
g de
vice
s pe
di/a
dult
(reg
ular
and
la
rge)
cuf
fs fo
r exa
mpl
e th
igh
size
s w
e ha
ve?
Y Y
Y M
(BLS
) Tem
pera
ture
mea
surin
g de
vice
-opt
iona
l ite
m
Y Y
N
N
Opt
iona
l ite
m a
nd fr
eque
ncy
of u
se d
oes
not
just
ify m
anda
tory
equ
ipm
ent r
equi
rem
ent
(BLS
) Inf
ant n
asal
can
nula
s
Y Ex
cept
in
fant
siz
e
Y Ex
cept
in
fant
siz
e
Y M
=Ped
i N
=Inf
ant
Blo
w-b
y m
ore
effe
ctiv
e in
infa
nt a
nd fr
eque
ncy
of
use
& c
ost o
f car
ryin
g do
es n
ot ju
stify
man
dato
ry
equi
pmen
t req
uire
men
t (B
LS) W
ide
bore
tubi
ng fo
r por
tabl
e su
ctio
n
Y Y
Y M
(B
LS) S
uctio
n ca
thet
er a
dd 6
fren
ch
Y Y
Y M
Pat F
rost
EM
SC C
oord
inat
or
Page
2
12/3
0/20
08

Con
tra
Cos
ta E
mer
genc
y M
edic
al S
ervi
ces
EM
S Fo
r C
hild
ren
Prog
ram
Ped
iatr
ic E
quip
men
t Lis
t Rev
iew
20
08 P
reho
spita
l Equ
ipm
ent L
ist A
sses
smen
t and
Upd
ate
Rec
omm
enda
tions
(BLS
) AE
D w
ith p
edi c
apab
ilitie
s –s
trong
ly
reco
mm
ende
d if
do n
ot h
ave
acce
ss to
ALS
re
com
men
ded
porta
ble
defib
/mon
itor
Y Y
N
M
All
BLS
age
ncie
s ha
ve A
ED
with
ped
iatri
c ca
pabi
litie
s or
acc
ess
to m
anua
l def
ibril
lato
rs w
ith
capa
bilit
ies
via
ALS
sup
port.
(B
LS) a
rm s
plin
ts s
peci
fy p
edia
tric/
adul
t (Jo
e th
inks
that
pro
vide
rs h
ave
pedi
siz
es b
ut
not s
ure)
Y N
Y
M
Spe
cify
as
splin
ts th
at c
an b
e ac
com
mod
ated
for
infa
nts
& p
edia
tric
patie
nts.
(B
LS) C
hild
saf
e re
stra
ints
-opt
iona
l ite
m
Y N
Y
M
For t
rans
port
prov
ider
s.
(BLS
) ped
i bac
kboa
rd (K
ED a
ccep
tabl
e)
Y Y
Y M
(B
LS) t
ract
ion
splin
ts lo
wer
ext
rem
ities
pe
diat
ric/a
dult
Y Y
Y M
(B
LS) P
ain
asse
ssm
ent t
ool (
in o
ur tr
eatm
ent
guid
elin
es b
ut n
eed
to s
peci
fy to
mee
t sta
te
guid
elin
es) –
optio
nal i
tem
N
Y Y
M
Add
ing
to p
edia
tric
colo
r bas
ed d
rug
refe
renc
e ca
rds
effe
ctiv
e 1/
1/20
09
(BLS
Nat
iona
l) na
sal s
alin
e dr
ops
for i
nfan
ts
(sal
ine
pillo
ws
coul
d be
use
d)
N
N
N
N
Freq
uenc
y of
use
doe
s no
t jus
tify
cost
s to
m
anda
te.
(BLS
) Bul
b sy
ringe
(Cur
rent
ly li
sted
as
item
in
obs
tetr
ical
kit.
Sho
uld
we
or d
o w
e in
clud
e se
para
tely
so
peop
le d
o no
t nee
d to
op
en k
its to
acc
ess
bulb
syr
inge
)
Y O
nly
in
OB
kit.
Y O
nly
in
OB
kit.
Y M
(O
B ki
t acc
ess
suffi
cien
t)
(ALS
) Nee
dle
size
s 24
gau
ge (?
nee
d)
Smal
ler
need
les s
o ra
rely
use
d ?
nece
ssity
Y Y
Y M
Li
st a
s 24
-25
gaug
e ne
edle
s. M
anuf
actu
rers
su
ppor
t onl
y 25
G
(ALS
) IV
cat
hete
r siz
es 2
4 ga
uge
(? n
eed)
Sm
alle
r IV
cat
hete
rs so
rar
ely
used
?
nece
ssity
Y Y
Y M
P
revi
ousl
y on
list
will
re-a
dd.
(ALS
) Vol
ume
limiti
ng d
evic
e /IV
adm
in s
ets
(vol
utro
ls n
ot u
sed,
min
i bag
s, m
icro
drip
de
vice
s to
lim
it flo
w in
use
)
Y Y
Y/N
M
M
ini b
ags
and
mic
ro d
evic
es p
rovi
de s
uffic
ient
sa
fety
con
trols
. Cos
ts a
nd fr
eque
ncy
of u
se d
o no
t ju
stify
vol
utro
ls.
Pat F
rost
EM
SC C
oord
inat
or
Page
3
12/3
0/20
08

Con
tra
Cos
ta E
mer
genc
y M
edic
al S
ervi
ces
EM
S Fo
r C
hild
ren
Prog
ram
Ped
iatr
ic E
quip
men
t Lis
t Rev
iew
20
08 P
reho
spita
l Equ
ipm
ent L
ist A
sses
smen
t and
Upd
ate
Rec
omm
enda
tions
(A
LS) E
TT c
uffe
d 6.
5 an
d 7.
5 ad
ditio
ns
N
Y Y
N
Freq
uenc
y of
use
doe
s no
t jus
tify
cost
s.
Ped
iatri
c in
tuba
tion
bein
g re
mov
ed fr
om lo
cal
scop
e ef
fect
ive
1/1/
2009
(ALS
) ETT
unc
uffe
d 6.
5 ad
ditio
n (s
tate
re
com
men
ds a
nd w
ould
be
appr
opria
te fo
r 40
kg
patie
nt) M
edic
al d
irect
or d
oes
not
wan
t to
add
sinc
e te
chno
logy
mov
ing
to
smal
ler t
ubes
with
cuf
fs
N
N
N
N
Freq
uenc
y of
use
doe
s no
t jus
tify
cost
s.
Ped
iatri
c in
tuba
tion
bein
g re
mov
ed fr
om lo
cal
scop
e ef
fect
ive
1/1/
2009
(ALS
) Mon
itor/D
efib
rilla
tors
(por
tabl
e) w
ith p
edi
and
adul
t def
ib p
ads/
padd
les
(cap
able
of
disc
harg
ing
belo
w 2
5 w
att s
econ
ds)
Y Y
Y M
(ALS
) Ped
i end
tida
l CO
2 de
tect
or
Y Y
Y M
(A
LS) p
ulse
oxi
met
er a
nd p
edi a
nd a
dult
prob
es
Y Y
Y M
(A
LS) 2
D10
W 2
50 m
l bag
s (n
ew b
ased
on
our u
pdat
es)
N
N
N
M
Cur
rent
trea
tmen
t gui
delin
es to
cha
nge
in 2
009
to
use
D10
for p
atie
nt s
afet
y (A
LS) C
olor
met
ric P
edi a
nd a
dult
end
tidal
CO
2 de
vice
s or
qua
ntita
tive
end-
tidal
CO
2 m
onito
rs
(opt
iona
l sco
pe it
em)
Y Y
Y M
Pat F
rost
EM
SC C
oord
inat
or
Page
4
12/3
0/20
08
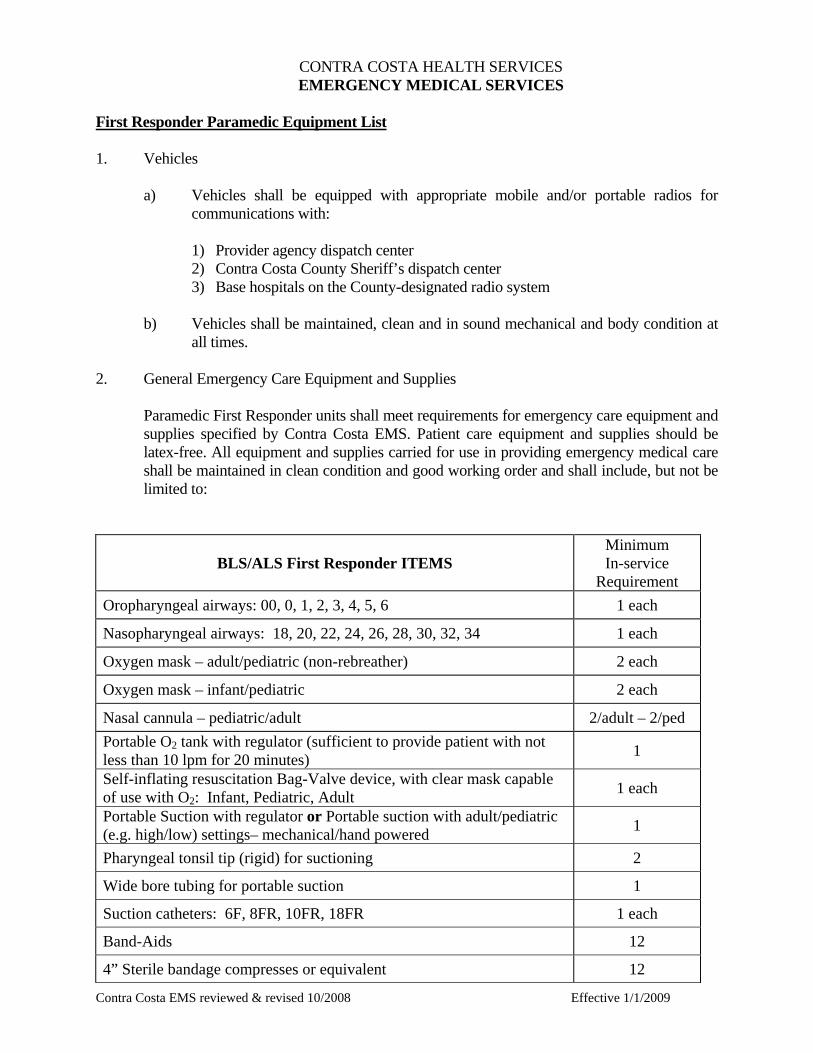
Contra Costa EMS reviewed & revised 10/2008 Effective 1/1/2009
CONTRA COSTA HEALTH SERVICES EMERGENCY MEDICAL SERVICES First Responder Paramedic Equipment List 1. Vehicles
a) Vehicles shall be equipped with appropriate mobile and/or portable radios for communications with: 1) Provider agency dispatch center 2) Contra Costa County Sheriff’s dispatch center 3) Base hospitals on the County-designated radio system
b) Vehicles shall be maintained, clean and in sound mechanical and body condition at
all times.
2. General Emergency Care Equipment and Supplies Paramedic First Responder units shall meet requirements for emergency care equipment and
supplies specified by Contra Costa EMS. Patient care equipment and supplies should be latex-free. All equipment and supplies carried for use in providing emergency medical care shall be maintained in clean condition and good working order and shall include, but not be limited to:
BLS/ALS First Responder ITEMS Minimum In-service
Requirement Oropharyngeal airways: 00, 0, 1, 2, 3, 4, 5, 6 1 each
Nasopharyngeal airways: 18, 20, 22, 24, 26, 28, 30, 32, 34 1 each
Oxygen mask – adult/pediatric (non-rebreather) 2 each
Oxygen mask – infant/pediatric 2 each
Nasal cannula – pediatric/adult 2/adult – 2/ped Portable O2 tank with regulator (sufficient to provide patient with not less than 10 lpm for 20 minutes) 1
Self-inflating resuscitation Bag-Valve device, with clear mask capable of use with O2: Infant, Pediatric, Adult 1 each
Portable Suction with regulator or Portable suction with adult/pediatric (e.g. high/low) settings– mechanical/hand powered 1
Pharyngeal tonsil tip (rigid) for suctioning 2
Wide bore tubing for portable suction 1
Suction catheters: 6F, 8FR, 10FR, 18FR 1 each
Band-Aids 12
4” Sterile bandage compresses or equivalent 12

Contra Costa EMS reviewed & revised 10/2008 Effective 1/1/2009
3x3” or 4x4” sterile gauze pads 4
2” or 3” rolled bandages 6
40” triangular bandages 4
10x30” or larger universal dressing 2
1”, 2” or 3” adhesive tape 2 rolls
Bandage shears 1
Vaseline gauze 2 Arm splints – with soft or cushioned surface or equivalent padded board, wrap around, wire ladder, inflatable or cardboard (able to accommodate adult/pediatric/infants)
2
Leg splints – with soft or cushioned surface or equivalent padded board, wrap around, wire ladder, inflatable or cardboard (able to accommodate adult/pediatric/infants)
2
Traction splints – with lower extremity limb support slings, padded ankle hitch traction strap and heel rest or equivalent (reel, sager or equivalent): Adult, Pediatric - (required on designated apparatus)
1 each
Spineboard – long with 4 straps (or equivalent) 1
Head immobilzer – disposable or impervious to bodily fluids 2
Cervical collars – Hard: sizes to fit all patients over one (1) year of age 2 each Optional: adjustable cervical collar (hard only – sizes to fit all patients
over one (1) year of age) 2
Blood pressure cuffs with sphygmomanometers (portable): Adult, Large arm (obese), Pediatric, Infant 1 each
Stethoscope: Adult/Pediatric combination 1 Burn sheets (sterile) – may be disposable or linen (with date of sterilization and expiration indicated) 1 set
Irrigation tubing 1
Sterile saline for irrigation 2000cc
Cold packs 2 Obstetrical Kit (sterile, to include minimum of umbilical cord tape or clamps (2), 1 scissors or scalpel, 1 aspirating bulb syringe, 1 pair gloves, 2 drapes, dressings & towels, clean plastic bag)
1
Newborn stocking cap 1
Emergency thermal blanket (reflective foil) or equivalent 2
Triage tags 20
Current Contra Costa EMS Field Treatment Guidelines and policies 1
Faces Pain scale (for adult & pediatric use) 1
Battery operated flashlight 1
Glucose paste 2

Contra Costa EMS reviewed & revised 10/2008 Effective 1/1/2009
AED with pediatric capabilities*. *Pediatric capabilities requirement may be met by responding ALS ambulance.
1

Contra Costa EMS reviewed & revised 10/2008 Effective 1/1/2009
First Responder Paramedic Equipment and Supplies: In addition to the BLS supply/equipment requirements, advanced life support units shall include, but not be limited to, the following:
ALS First Responder ITEMS Minimum In-service
Requirement Cellular telephone 1 Monitor/defibrillator (portable) – must have strip chart recorder and synchronized cardioversion capabilities. Defibrillator capable of discharging below 25 joules for pediatric use.
1
Pulse oximetry capable device 1
Pulse oximeter adult & pediatric probes 1 set each
Extra charged batteries for monitor/defibrillator 1
Defibrillator paddles/pads: Adult, Pediatric 1 set each
Laryngoscope handle 1
Laryngoscope blades: #0, 1, 2, 3, 4 Miller 1 each
Laryngoscope blades: #2, 3, 4 Macintosh 1 each
Endotracheal tubes: 6.0, 7.0, 8.0, 9.0 cuffed 2 each
Endotracheal tube introducer (e.g. Bougie) 1
Water soluble lubricant – individual packets 3
Magill forceps: Adult, Pediatric 1 each
Batteries (extra) for laryngoscope 1 set
Bulbs (extra) for laryngoscope 1
ETT securing device: Adult 1 each
Stylet: Adult 1 each
Pen light 1
End-Tidal CO2 (ETCO2) detector 2
ETT placement assessment device (bulb) 1 King Airway Kit
Tube – size 3, 4 and 5 Syringe Lubricant
1
Hand-held nebulizer for inhalation 2
ETT Nebulizer Adapter 1
Nebulizer mask – adult and pediatric 1 each Pleural Decompression/Needle Thoracostomy kit: (or equivalent)
Angiocatheter – 12 - 14ga Syringe – 30cc One-way valve
2 sets

Contra Costa EMS reviewed & revised 10/2008 Effective 1/1/2009
Rubber connecting tube Betadine swabs (4) Alcohol swabs (4) Vaseline gauze (2) Sterile gauze pads (2) Tape
IO insertion device e.g. EZIO 1
Intraosseous needle – adult/pediatric 2 each
Pressure bag for adult IO 1
Syringes: 1cc, 30cc 2
Syringes: 3cc, 5cc, 10cc or 12cc 2 each
Needles: 18ga 1”, 20ga 1”, 22ga 1”, 24 ga or 25ga” - 2 each
Medication-added labels 2
IV catheters: 16ga, 18ga, 20ga, 22ga, 24ga 4 each
Alcohol swabs 5
Tourniquet 2
Razor 1
Armboard(s) adaptable for infant, child, adult 1 each
Normal Saline solution – 500ml or 1000ml bags for adult patients 2 liters
Normal Saline solution – 100ml or 250mlbags for pediatric patients 2 each
Universal vial adapter/dispensing pin 2
Saline lock with extension tubing 2
IV tubing: mini drip (60gtt), macro drip (10/15gtt) or equivalent (4) 2 each
IV extension tubing 2
Secured drug box 1 Pediatric length-based weight determination tape e.g. Broselow or equivalent 1
Glucometer (with lancets and test strips) 1
Adenosine (6mg) 5
Albuterol (2.5mg/3ml unit dose ampule) 4
Amiodarone (150mg/3ml ampule) 3
Atropine (1mg preload) 4
Aspirin (81mg tablets) 1 bottle
Diphenhydramine (Benadryl) (50mg/1cc) 2

Contra Costa EMS reviewed & revised 10/2008 Effective 1/1/2009
Calcium Chloride (1 gm) 1
Dextrose 10 W (250 ml/bags) 2
Dextrose 50% (25gm/50cc) 2
Epinephrine 1:10,000 (1mg/10cc) 4
Epinephrine 1:1,000 (1mg/1cc) 2
Glucagon (1mg/1cc) 1
Lidocaine 2% for IO pain control 100 mg
Midazolam (Versed) (5mg/ml ampule/vial) 10 mg
Morphine Sulfate (10mg/1cc ampule/vial) 20 mg
Naloxone (Narcan) 4 mg
Nitroglycerin (0.4 mg/tab or multidose spray) 1 bottle
Sodium Bicarbonate (50mEq/50cc) 1

Contra Costa EMS reviewed & revised 10/2008 Effective 1/1/2009
CONTRA COSTA HEALTH SERVICES EMERGENCY MEDICAL SERVICES AMBULANCE EQUIPMENT AND SUPPLY REQUIREMENTS 1. Vehicles
a. Ambulance vehicles shall meet standards specified in Title 13, California Code of Regulations, and each shall possess a valid emergency vehicle permit issued by the California Highway Patrol.
b. Vehicles shall be maintained, clean and in sound mechanical and body condition at all times. c. All ambulances shall have adequate space in the patient care compartment to accommodate at least
one stretcher patient and two providers. There shall be sufficient space to allow for patient care activities during transport.
d. Vehicles shall be equipped with appropriate mobile and/or portable radios for communications with:
1) Provider agency dispatch center 2) Contra Costa County Sheriff’s dispatch center 3) Base hospitals on the County-designated radio system
2. Personal Protective Equipment (PPE)
All ambulance providers are encouraged to adhere to the California Emergency Medical Services Authority (EMSA) guideline #216 – Minimum Personal Protective Equipment (PPE) For Ambulance Personnel in California (see attachment). Those providers that have received equipment through the PPE grant project are required to adhere to this guideline.
3. General Emergency Care Equipment and Supplies Ambulances shall meet the State requirements for emergency care equipment and supplies. Patient
care equipment and supplies should be latex-free. All equipment and supplies carried for use in providing emergency medical care shall be maintained in clean condition and good working order and shall include, but not be limited to:
BLS/ALS Ambulance ITEMS Minimum In-service
Requirement Oropharyngeal airways: 00, 0, 1, 2, 3, 4, 5, 6 1 each
Nasopharyngeal airways: 18, 20, 22, 24, 26, 28, 30, 32, 34 1 each
Oxygen mask – adult/pediatric (non-rebreather) 2 each
Oxygen mask – infant/pediatric 2 each
Nasal cannula – pediatric/adult 2/adult – 2/ped
O2 tank – fixed in vehicle with regulator (M-tank or equivalent) 1 Portable O2 tank with regulator (sufficient to provide patient with not less than 10 LPM - for 20 minutes) 1
Self inflating resuscitation Bag-Valve device, with clear mask, capable of use with O2: Infant, Pediatric, Adult 1 each
Portable Suction with regulator or Portable suction with adult/pediatric (e.g. high/low) settings – mechanical/hand powered 1

Contra Costa EMS reviewed & revised 10/2008 Effective 1/1/2009
Wide bore tubing for portable suction 1
Pharyngeal tonsil tip (rigid) for suctioning 2
Suction catheters: 6F, 8FR, 10FR, 18FR 1 each
Band-Aids 12
4” Sterile bandage compresses or equivalent 12
3x3” or 4x4” sterile gauze pads 4
2” or 3” rolled bandages 6
40” triangular bandages 4 10x30” or larger universal dressing 2 1”, 2” or 3” adhesive tape 2 rolls Bandage shears 1 Vaseline gauze 2 Arm splints – with soft or cushioned surface or equivalent padded board, wrap around, wire ladder, inflatable or cardboard (able to accommodate adult/pediatric/infants)
2
Leg splints – with soft or cushioned surface or equivalent padded board, wrap around, wire ladder, inflatable or cardboard (able to accommodate adult/pediatric/infants)
2
Traction splints – with lower extremity limb support slings, padded ankle hitch traction strap and heel rest or equivalent (reel, sager or equivalent): Adult/Pediatric
1 each
Spineboard – long with 4 straps (or equivalent) 1 Spineboard : (pediatric capable) – short with 2 straps or equivalent (Kendrick Extrication Device) 1
Head immobilizer – disposable or impervious to bodily fluids 2
Cervical collars – Hard: sizes to fit all patients over one (1) year of age 2 each Optional: adjustable cervical collar (hard only): sizes to fit all patients over one (1) year of age 2
Scoop stretcher with straps (or equivalent) 1 Blood pressure cuffs with sphygmomanometers (portable): Adult, Large arm (obese), Pediatric, Infant 1 each
Stethoscope: Adult/Pediatric (or combination) 1 Burn sheets (sterile) – may be disposable or linen (with date of sterilization and expiration indicated) 1 set
Irrigation tubing 1
Saline for irrigation, sterile: 2000cc
Cold packs 2 Obstetrical Kit (sterile, to include minimum of umbilical cord tape or clamps (2), 1 scissors or scalpel, 1 aspirating bulb syringe, 1 pair gloves, 2 drapes, dressings & towels, clean plastic bag)
1

Contra Costa EMS reviewed & revised 10/2008 Effective 1/1/2009
Newborn Stocking Cap 1
Emergency thermal blanket (reflective foil) or equivalent 2 Ambulance gurney – capability for elevating the head and be adjustable, straps for securing patient to gurney, wheels, non-permeable covering material, means of securing gurney in vehicle.
1
Portable cardio-respiratory monitor with pulse oximetry capability 1
Pulse oximeter adult & pediatric probes 1 set each AED with pediatric capabilities*. *Pediatric capabilities requirement may be met by responding ALS ambulance. 1
Triage tags 20
Current map (within 2 years) of entire county or ambulance zone maps 1
Current Contra Costa EMS Field Treatment Guidelines and policies 1
Faces Pain Scale (for adult & pediatric use) 1
Ankle and wrist restraints (4 per set) 1 set
Child safe restraints (infant/pediatric) 1 set each
Battery operated flashlight 1
Emesis basin or disposable emesis bags and covered waste container 1
Linen – towels, sheets, pillow cases, blankets, pillows 2 each
Glucose Paste 1 tube

Contra Costa EMS reviewed & revised 10/2008 Effective 1/1/2009
ALS Ambulance Emergency Care Equipment and Supplies: In addition to the BLS ambulance supply/equipment requirements, advanced life support units shall include, but not be limited to, the following:
ALS Ambulance ITEMS Minimum In-service
Requirement Cellular telephone 1 Monitor/defibrillator (portable) – must have strip chart recorder, 12-lead and synchronized cardioversion & ETCO2 monitoring capabilities. Defibrillator capable of discharging below 25 joules for pediatric use.
1
Extra charged batteries for monitor/defibrillator 1
Defibrillator paddles/pads: Adult, Pediatric 1 set each
12-lead patches 2 sets
Laryngoscope handle 1
Laryngoscope blades: #0, 1, 2, 3, 4 Miller 1 each
Laryngoscope blades: #2, 3, 4 Macintosh 1 each
Endotracheal tubes: 6.0, 7.0, 8.0, 9.0 cuffed 2 each
Endotracheal tube introducer (e.g. Bougie) 1
Water soluble lubricant – individual packets 3
Magill forceps: Adult, Pediatric 1 each
Batteries (extra) for laryngoscope 1 set
Bulbs (extra) for laryngoscope 1
ETT securing device: Adult 2
Stylet: Adult, 1 each
Pen light 1
End-Tidal CO2 (ETCO2) detector 2 ETT placement assessment device (bulb) 1 ETT Nebulizer Adapter 2 King Airway Kit
Tube – size 3, 4 and 5 Syringe Lubricant
1
Hand-held nebulizer for inhalation 2 Nebulizer mask – adult and pediatric 2 each Pleural Decompression/Needle Thoracostomy kit: (or equivalent)
Angiocatheter – 12 - 14ga Syringe – 30cc
2 sets

Contra Costa EMS reviewed & revised 10/2008 Effective 1/1/2009
One-way valve Rubber connecting tube Betadine swabs (4) Alcohol swabs (4) Vaseline gauze (2) Sterile gauze pads (2) Tape
Continuous Positive Airway Pressure (CPAP) device 1
IO insertion device e.g. EZIO 1
Intraosseous needle – adult and pediatric 2 each
Pressure bag for adult IO 1
Syringes: 1cc, 30cc 2
Syringes: 3cc, 5cc, 10cc or 12cc 2 each
Needles: 18ga 1”, 20ga 1”, 22ga 1”, 25 or 24 ga ” 2 each
Medication-added labels 2
IV catheters: 16ga, 18ga, 20ga, 22ga, 24ga 4 each
Alcohol swabs 5
Tourniquet 2
Razor 1
Armboard(s) (adaptable for infant, child, adult) 1 each
Normal Saline solution – 500cc or 1000cc bag for adult patients 4 liters
Universal vial adapter/dispensing pin 2
Normal Saline solution – 100ml, 250ml for pediatric patients 2 each
Saline lock with extension tubing 2
IV tubing: mini drip (60gtt), macro drip (10/15gtt) or equivalent (8) 4 each
IV extension tubing 4
Glucometer (with lancets and test strips) 1
Secured drug box 1
Pediatric length-based weight determination tape e.g. Broselow or equivalent 1
Adenosine (6mg) 5
Albuterol (2.5mg/3ml unit dose ampule) 4
Amiodarone (150mg/3ml ampule) 6
Atropine (1mg preload) 4

Contra Costa EMS reviewed & revised 10/2008 Effective 1/1/2009
Aspirin (81mg tablets) 1 bottle
Diphenhydramine (Benadryl) (50mg/1cc) 2
Calcium Chloride (1 gm) 1
Dextrose 10% (250 ml) 2
Dextrose 50% (25gm/50cc) 2
Dopamine (400mg/250cc premixed bag) (or equivalent) 1
Epinephrine 1:10,000 (1mg/10cc) 4
Epinephrine 1:1,000 (1mg/1cc) 2
Glucagon (1mg/1cc) 1
Lidocaine 2% for IO pain control 100 mg
Midazolam (Versed) (5mg/ml ampule/vial) 10 mg
Morphine Sulfate (10mg/1cc ampule/vial) 20 mg
Naloxone (Narcan) 4 mg
Nitroglycerin (0.4 mg/tab or multidose spray) 1 bottle
Sodium Bicarbonate (50mEq/50cc) 1


Appendix E
Contra Costa County Paramedic Accreditation
Policy


POLICY #: 2
Contra Costa Emergency Medical Services
PAGE: 11 of 11
EFFECTIVE: 01/01/09
PARAMEDIC ACCREDITATION REVIEWED: 11/01/08
I. PURPOSE
To identify the process for paramedic accreditation in Contra Costa County. II. ACCREDITATION
A. All candidates shall meet the following accreditation requirements: 1) Possess a current California paramedic license. 2) Be employed as a paramedic with a designated ALS service provider or the EMS Agency. 3) Attend a Contra Costa EMS Orientation provided by the provider agency and approved by
the EMS Agency or provided by the EMS Agency. 4) Successfully complete the Contra Costa County EMS Optional Scope Skills Session
provided by the provider agency. 5) Complete an application form, available online or at the provider agency or the EMS
Agency. B. Documentation that the accreditation requirements have been met must be submitted to the
EMS Agency, by the applicant’s employer, with the candidate’s application and accreditation fee.
The EMS Agency shall notify individuals applying for accreditation of the decision to accredit within thirty (30) days of application.
III. MAINTAINING ACCREDITATION A. Accreditation to practice shall be continuous as long as: 1) State licensure is maintained, 2) Employment as a paramedic with a designated Contra Costa ALS service provider or the
EMS Agency is maintained, 3) A current and valid ACLS card, according to the standards of the American Heart
Association is maintained, 4) Verification of skills competency is completed every two years, and 5) Any other local requirements are met. B. Documentation that the above requirements to maintain accreditation have been met must be
submitted by the applicant or the applicant’s employer prior to expiration of the paramedic’s license.


Appendix F
Contra Costa EMSC Emergency Department
Consultation Visit Survey Tool and Results


Contra Costa County 2008 EMS for Children Emergency Department Self Assessment
“Approximately 30 million children are seen each year in our nation’s emergency departments (EDs). Most of these children (90%) will arrive by private car and 10% will arrive by ambulance. Each ED must be prepared with appropriate staff, equipment, supplies, and procedures to ensure quality care regardless of the patient’s age or presenting complaint.” Source: Joint policy statement American Academy of Pediatrics & American College of Emergency Physicians (2001) Introduction In 2002 the Contra Costa EMS Agency implemented the county’s first Emergency Medical Services for Children (EMSC) Plan. This plan helped establish many recommendations and guidelines to assist Emergency Departments in providing minimum and uniform administrative, personnel, and policy guidelines for the care of pediatric patients within the county. Our current EMSC Plan is due for review and update. The process will begin with each Emergency Department completing a self-assessment. This will allow the EMS Agency to evaluate the effectiveness of our current EMS for Children Program. It will be followed at a later date with a facility educational consultation and site visit. The site visits will further assist us in collecting information for our State mandated EMSC Plan review. Emergency departments in Contra Costa County vary in pediatric patient volume, education of staff caring for pediatric emergencies, and in availability of equipment to care for pediatric patients. This new self-assessment tool is based on the recently updated 2008 EMSC ED Guidelines for Pediatric Care (document #182). It is designed to further assist Emergency Departments in assessing their readiness to provide care for pediatric patients. It will also be helpful in preparation for the County EMSC facility educational consultation. This consultation should take about 2 hours. If you have any questions about this self-assessment or the EMSC facility educational consultations, please contact Pat Frost EMSC Coordinator at [email protected]. I will be contacting you to schedule the consultation site visit at a later date. Enclosed are the revised California State EMS Authority Guidelines for Administration, Personnel and policy for the Care of Pediatric Patients in the Emergency Department (document #182). Please compare these guidelines to your current practices and identify opportunities for improvement where applicable. This survey will be due by August 1, 2008.

Contra Costa County 2008 EMS for Children Emergency Department Self Assessment
Definitions and Terms used in this ED self-evaluation are consistent with EMSA document # 182 revised in 2008 and are listed here for your convenience. The numbers correspond to the endnotes dispersed throughout this survey document and are identical to the endnotes in EMSA document #182. 1 Personnel guidelines for a physician and a nurse coordinator for pediatric emergency medicine may be met by staff currently assigned other roles in the department and may be shared between EDs. 2 “Qualified specialist” means a physician licensed in California who has: 1) taken special postgraduate medical training, or has met other specified requirements, and 2) has become board certified within six years of qualification for board certification in the corresponding specialty, for those specialties that have board certification and are recognized by the American Board of Medical Specialties. For Standby Emergency Departments: A physician who is not a qualified specialist may perform the role if:
(1) the physician can demonstrate to the appropriate hospital body and the hospital is able to document that he/she has met requirements which are equivalent to those of the Accreditation Council for Graduate Medical Education (ACGME) or the Royal College of Physicians and Surgeons of Canada; (2) the physician can clearly demonstrate to the appropriate hospital body that he/she has substantial education, training, and experience in treating and managing pediatric patients which shall be tracked by the pediatric quality improvement program;
(3) the physician has successfully completed a residency program and (4) is current with Advanced Pediatric Life Support: The Pediatric Emergency Medicine Course (APLS) or Pediatric Advanced Life Support (PALS)
3 These guidelines do not promote or suggest that any particular continuing education course is required for competency. Competency as stated in this document is defined by local (hospital) credentialing requirements which should include requirements for all ages of patients from newborns through the elderly. 4 Refer to Section V of the Guidelines: Quality Improvement 5 For physicians staffing a general emergency department, a pediatric emergency department or for physicians staffing an emergency department in a children’s hospital, certification in Emergency Medicine or Pediatric Emergency Medicine is the preferred standard of competence. For all other situations or areas in which physician resources are limited, then a physician specialist as described in section ll.B.1. is desirable. 6 The Pediatric consultant should be a specialist in pediatrics or pediatric emergency medicine and may be board certified or prepared. Requirements may be fulfilled by supervised senior residents who are capable of assessing emergency situations in their respective specialties. When a senior resident is the responsible specialist: the senior resident shall be able to provide the overall control and leadership necessary for the care of the patient, including initiating care; the pediatric consultant shall be on-call and promptly7 available; the pediatric consultant shall be advised of all admissions, participate in major therapeutic decisions, and be present in the ED for major resuscitations. 7 May be met by PALS or APLS 8 Endtidal CO2 monitoring is considered the optimal method of assessing for and monitoring of endotracheal tube placement in the trachea, however for low patient volume hospitals, CO2 colorimetric detector devices could be substituted. Clinical assessment alone is not appropriate. 9 Feeding tubes (size 5F) may be utilized as a UVC catheter
10 A spinal stabilization device should be a device that can also stabilize the neck of an infant, child or adult in a neutral position. 11 2005 International Consensus Conference on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Recommendations (or most current)

Contra Costa County 2008 EMS for Children Emergency Department Self Assessment
Promptly available means being within the emergency department within a period of time that is medically prudent and proportional to the patient’s clinical condition and such that the interval between the arrival of the patient to the emergency department and the arrival of the respondent should not have a measurably harmful effect on the course of the patient management or outcome.
ADMINISTATION /COORDINATION Circle one Y N Medical Director for the ED. Name___________________________________
Y N Y N Y N
Physician coordinator for pediatric emergency medicine.1Name:________________________ This may be met by staff currently assigned other roles in the department and may be shared between EDs. Qualifications: 1. Qualified specialist2 in Pediatric Emergency Medicine or Emergency Medicine, of
MD who is a qualified specialist2 in Pediatrics or Family Medicine and is current in APLS or PALS training.
2. Demonstrates special interest, knowledge, and skill in emergency medical car of children as demonstrated by training, clinical experience, or focused continuing education.
3. Maintains competency3 in pediatric emergency care as defined by local (hospital) credentialing requirements.
Responsibilities: 1. Oversight of ED pediatric quality improvement (QI). 2. Liaison with appropriate hospital-based pediatric care committees 3. Liaison with pediatric critical care center, trauma centers, the local EMS agency,
base hospital, prehospital care providers, and community hospitals. 4. Facilitates ED physician pediatric emergency education and competency4
evaluations. 5. Ensure pediatric disaster preparedness for emergency department
Comments: Y N Y N
A Nursing Coordinator for pediatric emergency care.1 (eg: Pediatric Liaison Nurse) Name:_______________________________ This may be met by staff currently assigned other roles in the department and may be shared between EDs. Qualifications: 1. RN with at least two years experience in pediatrics or emergency nursing within the
previous five years. 2. Completion of PALS, ENPC, APLS, or other equivalent pediatric emergency course.

Contra Costa County 2008 EMS for Children Emergency Department Self Assessment
Y N Responsibilities
1. Coordination with the pediatric physician coordinator for pediatric QI activities 2. Facilitation of ED nursing continuing education and competency3 evaluations in
pediatrics. 3. Liaison with pediatric critical care center, trauma centers, the local EMS agency,
base hospitals, prehospital care providers, and community hospitals. 4. Liaison with appropriate hospital-based pediatric care committees 5. Ensure emergency nursing preparedness for pediatric disasters.
Comments:
PERSONNEL Circle one Y N Y N Y N
Physicians staffing – ED physician on duty 24 hours/day as per Title 22: Ref. 70415. Qualifications/Education: 1. Qualified specialist2 in Pediatrics or Emergency Medicine, or 2. Physicians who are not qualified specialists2 in Emergency Medicine or Pediatric
Emergency Medicine should be current in PALS or APLS5. 3. Complete pediatric competency3 evaluations that are age specific and include
neonates, infants, children and adolescents as required by local credentialing.
Comments Y N Y N Y N
Back up MD Specialty Services: There is a plan for pediatric patients to receive specialized care 1. A designated pediatric consultant6 is available for in-house consultation or through
phone consultation and transfer agreements. 2. Pediatric specialty physicians available for in-house consultation or through phone
consultation and transfer agreements. Comments:
Nurses staffing the ED Qualifications:

Contra Costa County 2008 EMS for Children Emergency Department Self Assessment
Y N Y N Y N
1. At least one ED RN per shift with current completion of ENPC, PALS, APLS, or equivalent pediatric emergency nursing course.
2. All RNs regularly assigned to the ED complete four hours of CE in topics related to pediatrics every two years. This may be met through completion of ENPC, PALS, or APLS. 7
3. Complete pediatric competency3 evaluations that are age specific and include neonates, infants, children and adolescents as required by local credentialing.
Comments: Y N
MID LEVEL PRACTITIONERS (Physician Assistants, Nurse Practitioners) Qualifications:
1. All mid-level practitioners regularly assigned to the ED and who car for pediatric patients should demonstrate current completion of PALS, APLS, ENPC or other equivalent pediatric emergency care course.
2. Complete pediatric competency4 evaluations that are age specific and include neonates, infants, children, and adolescents as required by local credentialing.
Comments:

Contra Costa County 2008 EMS for Children Emergency Department Self Assessment
QUALITY IMPROVEMENT (QI)
Circle one Y N A Pediatric QI Plan should be established
This plan may be a component of the comprehensive ED QI plan. Y N Components of the plan include; a plan for interface with prehospital, ED, trauma, in-
patient pediatrics, pediatric critical care, hospital-wide QI activities. Y N Y N Y N Y N
The pediatric QI plan may include the following: 1. A periodic review of aggregate data of pediatric emergency visits 2. A review of prehospital and ED pediatric patient care. Select indicators which may
include: • Deaths • Transfers • Child Maltreatment cases • Cardiopulmonary or respiratory arrests • Trauma admissions from the ED • Operating room admissions from the ED • ICU admissions from the ED • Patient safety including adverse events involving medication delivery.
3. Mechanism to monitor professional credentialing, education and competencies • Airway management • Burn care • Critical care monitoring • Medication delivery and device/equipment safety • Pain assessment and treatment • Trauma care • Vascular access
4. A mechanism to provide for integration of findings from QI process and reviews into education and clinical competency evaluations of ED staff.
Comments:

Contra Costa County 2008 EMS for Children Emergency Department Self Assessment
POLICIES, PROCEDURES AND PROTOCOLS
Circle one Y N Check those P/P currently in place
Policies, procedures or protocols for emergency care of children are not limited to but should include the following: Pediatric policies, procedures or protocols may be a component of ED or hospital policy and procedure or may be addressed as separate pediatric specific documents.
1. Illness and injury triage 2. Pediatric Assessment 3. Physical or chemical restraint of patients 4. Child maltreatment 5. Safe surrender and child abandonment 6. Consent (including situations in which a parent is not immediately available) 7. DNR orders 8. Procedural sedation 9. Death in ED to include SIDS and care of the grieving family 10. Radiation dosage protocol 11. Scheduled resuscitation medical and supply inventory check 12. Immunization status 13. Mental health emergencies 14. Family Centered Care, including:
• Education of the patient, family and regular caregivers • Discharge planning and instruction • Family presence during care
15. Communication with patient’s primary health care provider. 16. Pain assessment and treatment 17. Disaster preparedness plan that addresses the following pediatric issues:
• A plan to minimize parent-child separation and improved methods for reuniting separated children from their families
• A plan that addresses pediatric surge capacity for both injured and non-injured
• A plan that includes access to specific medical and mental health therapies, as well as social services, for children in the event of a disaster.
• A plan which ensures that disaster drills include a pediatric mass casualty incident at least once every 2 years
• Decontamination 18. Medication safety
• Record all weights in kg • Process to solicit feedback from staff including medical error reporting • Involvement of families in medication safety process. • Medication orders that are clear and unambiguous
An Inter-facility Consultation and Transfer Plan for tertiary or specialized care
should include at a minimum the following:

Contra Costa County 2008 EMS for Children Emergency Department Self Assessment
Y N A plan for sub-specialty consultation (telephone or real-time telemedicine 24
hours/day) Y N Identification of transferring and receiving facilities’ responsibilities in compliance
with EMTALA. Establishment of inter-facility transfer agreements (including repatriation of the child
back to his/her community as appropriate) should include the following pediatric specialty referral resources.
• Medical and surgical pediatric intensive care • Trauma • Re-implantation (replacement of severed digits or limbs) • Burns • Psychiatric emergencies • Obstetric and perinatal emergencies • Child maltreatment
Comments/issues/areas for improvement:
GUIDELINES FOR SUPPORT SERVICES FOR THE ED Circle one Y N
Respiratory Care Practitioners (who respond to the ED) should include qualified staff and necessary equipment and supplies to care for children in the ED
Y N Respiratory Care Staffing: At least one Respiratory care or equivalent practitioner n house 24 hours/day Complete pediatric competency4 evaluations that are age specific and include
neonates, infants, children and adolescents as required by local credentialing Y N Radiology Services should include qualified staff and necessary equipment and
supplies to provide imaging studies of children including Protocols that include modification of radiation exposure of children based on
age and weight, pediatric radiation dosing and protective shielding of children for plain radiography and CT
Y N Clinical Laboratory Services should include qualified staff and necessary equipment and supplies to provide laboratory services and testing/analysis including but not limited to: Obtaining samples from children of all ages Micro-capabilities
Comments/issues/areas for improvement:
EQUIPMENT, SUPPLIES AND MEDICATIONS FOR THE CARE OF PEDIATRIC PATIENTS IN THE EMERGENCY DEPARTMENT
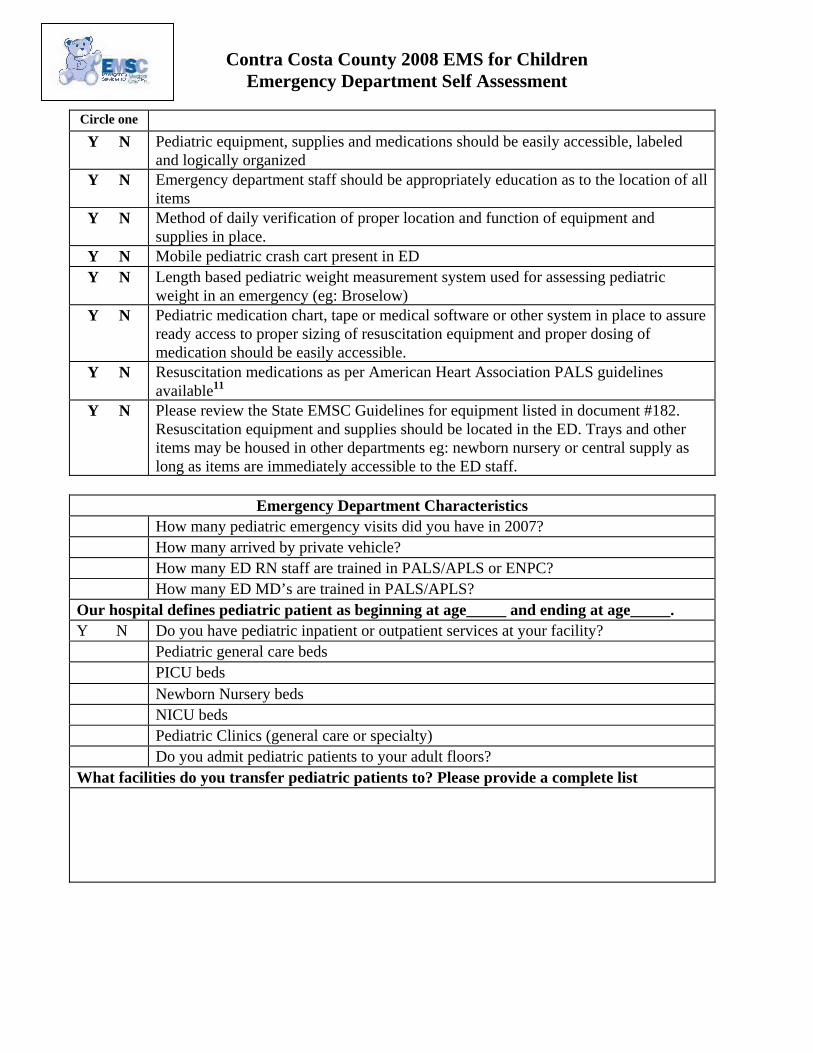
Contra Costa County 2008 EMS for Children Emergency Department Self Assessment
Circle one Y N Pediatric equipment, supplies and medications should be easily accessible, labeled
and logically organized Y N Emergency department staff should be appropriately education as to the location of all
items Y N Method of daily verification of proper location and function of equipment and
supplies in place. Y N Mobile pediatric crash cart present in ED Y N Length based pediatric weight measurement system used for assessing pediatric
weight in an emergency (eg: Broselow) Y N Pediatric medication chart, tape or medical software or other system in place to assure
ready access to proper sizing of resuscitation equipment and proper dosing of medication should be easily accessible.
Y N Resuscitation medications as per American Heart Association PALS guidelines available11
Y N Please review the State EMSC Guidelines for equipment listed in document #182. Resuscitation equipment and supplies should be located in the ED. Trays and other items may be housed in other departments eg: newborn nursery or central supply as long as items are immediately accessible to the ED staff.
Emergency Department Characteristics
How many pediatric emergency visits did you have in 2007? How many arrived by private vehicle? How many ED RN staff are trained in PALS/APLS or ENPC? How many ED MD’s are trained in PALS/APLS?
Our hospital defines pediatric patient as beginning at age_____ and ending at age_____. Y N Do you have pediatric inpatient or outpatient services at your facility? Pediatric general care beds PICU beds Newborn Nursery beds NICU beds Pediatric Clinics (general care or specialty) Do you admit pediatric patients to your adult floors? What facilities do you transfer pediatric patients to? Please provide a complete list

Contra Costa County 2008 EMS for Children Emergency Department Self Assessment
What pediatric prevention community activities or programs does your hospital or ED participate in? Please list and attach additional information if needed. Y N Would your ED be interested in joint ED/Prehospital resuscitation training using
a Pediatric Patient Simulator? Y N Have you heard about the new AHA and AAP National Standard in Pediatric
Emergency Assessment, Recognition and Stabilization? (Known as Assess Categorize Decide Act for ACDA). This new standard is currently being taught in PALS and the new AHA course focused on Pediatric Emergency Assessment called PEARS (Pediatric Emergency Assessment, Recognition and Stabilization).
Y N Would you be interested in a staff training 1-2 hours on this new assessment approach?
How can Contra Costa EMS Agency support your ED efforts to improve in the care of children? This survey was completed by: (name/title) Contra Costa County EMS thanks you for your participation in this survey. Results will be compiled and shared with our facilities as blinded data. Recommendations for improvement of pediatric prehospital care is always welcome and should be directed to Pat Frost at [email protected].

Con
tra
Cos
ta C
ount
y 20
08 E
MSC
Em
erge
ncy
Dep
artm
ent A
sses
smen
t Sum
mar
y*
* Sur
vey
and
site
vis
its w
ere
com
plet
ed b
etw
een
May
of 2
008
and
Dec
embe
r 200
8
A: CCRMC
B: Doctors-SP
C: JMMC-WC
D: Kaiser-R
E: Kaiser-WC
F: JMMC-C
G: Sutter Delta
H: SRVRMC
I: Kaiser-A
EMSC
Site
Vis
it C
ompl
eted
Y
Y Y
Y Y
Y Y
Y Y
AD
MIN
ISTR
ATI
ON
/CO
OR
DIN
ATI
ON
mee
ts 2
008
EMSA
gui
delin
es
M
edic
al D
irect
or fo
r ED
Y
Y Y
Y Y
Y Y
Y Y
Phy
sici
an C
oord
inat
or fo
r ped
iatri
c em
erge
ncy
med
icin
e Y
Y1Y
Y Y
Y Y
Y Y
Q
ualif
icat
ion
crite
ria m
et
Y
Y
Y
Y
Y
Y
Y
Y
Y
R
espo
nsib
ilitie
s m
et
Y Y
Y Y
Y Y
Y Y
Y N
ursi
ng C
oord
inat
or fo
r ped
iatri
c em
erge
ncy
care
Y
Y Y
Y2,3
Y Y
Y Y
Y
Qua
lific
atio
n cr
iteria
met
Y
Y
2Y
Y2,3
Y Y
Y Y
Y
Res
pons
ibilit
ies
crite
ria m
et
Y3Y
Y Y2,
3Y
Y2,3
Y2,3
Y Y
Foot
note
s:
1 Pos
ition
ass
umed
by
Med
ical
Dire
ctor
2 P
ositi
on; a
ssum
ed b
y E
D N
urse
Man
ger
3 Sh
ared
resp
onsi
bilit
y
PER
SON
NEL
mee
ts 2
008
EMSA
gui
delin
es
P
hysi
cian
Sta
ffing
ED
MD
sta
ffing
24
hrs/
day
Y Y
Y Y
Y Y
Y Y
Y Q
ualif
icat
ions
/Edu
catio
n
Y Y1
Y Y
Y Y
Y Y
Y
Qua
lifie
d sp
ecia
list
Y Y1
Y Y
Y Y
Y Y
Y
Non
spe
cial
ist-P
ALS
2 Y
Y1Y
Y Y
Y Y
Y Y
C
ompl
ete
Ped
i com
pete
ncy
in p
edia
trics
requ
ired
by c
rede
ntia
ling
Y
Y1
Y Y
Y Y
Y Y1
Y B
ack-
up M
D S
peci
alty
Ser
vice
s P
lan
for P
edia
tric
Pat
ient
s re
quiri
ng s
peci
aliz
ed c
are
Y Y3
Y Y
Y Y
Y Y
Y
Des
igna
ted
Ped
iatri
c C
onsu
ltant
in-h
ouse
/pho
ne c
onsu
lt &
tran
sfer
agr
eem
ents
Y
Y
3Y
Y Y
Y3Y3
Y Y
P
edia
tric
spec
ialty
phy
sici
ans
avai
labl
e fo
r in-
hous
e/ph
one
cons
ult &
tran
sfer
agr
eem
ents
Y
Y
Y
Y
Y
Y
3Y3
Y Y
Foot
note
s:
1 E
mer
genc
y M
edic
ine
CE
con
tain
s pe
diat
rics
2 Util
izes
PA
LS, A
PLS
or e
quiv
alen
t as
part
of q
ualif
icat
ions
/edu
catio
n 3 D
esig
nate
d pe
diat
ric h
ospi
tal s
peci
alis
ts u
sed
to fa
cilit
ate
spec
ialty
refe
rral
LE
GEN
D: Y
= Y
es
N
= N
o
NA
= N
ot A
pplic
able
Page
1
12
/24/
2008

Con
tra
Cos
ta C
ount
y 20
08 E
MSC
Em
erge
ncy
Dep
artm
ent A
sses
smen
t Sum
mar
y*
A: CCRMC
B: Doctors-SP
C: JMMC-WC
D: Kaiser-R
E: Kaiser-WC
F: JMMC-C
G: Sutter Delta
H: SRVRMC
I: Kaiser-A
PER
SON
NEL
mee
ts 2
008
EMSA
gui
delin
es
N
ursi
ng S
taffi
ng in
ED
Qua
lific
atio
ns/E
duca
tion
At l
east
one
ED
RN
/shi
ft cu
rrent
in P
ALS
, EN
PC
, AP
LS o
r equ
ival
ent p
edia
tric
nurs
ing
cour
se
Y2Y2
Y2Y2
Y2Y2
Y2Y2
Y2
A
ll R
N’s
regu
larly
ass
igne
d to
ED
com
plet
e fo
ur h
ours
CE
rela
ted
to P
eds
(incl
udes
: P
ALS
, EN
PC
or e
quiv
alen
t. Y2
Y2Y2
Y2Y2
Y2Y2
Y2Y2
C
ompl
ete
com
pete
ncy
eval
uatio
ns th
at a
re a
ge s
peci
fic a
nd in
clud
e: n
eona
tes,
in
fant
s, c
hild
ren
& a
dole
scen
ts a
s pe
r loc
al c
rede
ntia
ling
Y2Y2
Y Y
Y Y
Y2Y5
Y
MID
=LE
VE
L P
RA
CTI
TIO
NE
RS
(Phy
sici
an A
ssis
tant
s, N
urse
Pra
ctiti
oner
s)
Q
ualif
icat
ions
/Edu
catio
n
A
ll re
gula
rly a
ssig
ned
to E
D s
houl
d de
mon
stra
te c
urre
nt c
ompl
etio
n of
PA
LS, E
NP
C,
AP
LS o
r equ
ival
ent
NA
Y
N
Y
N
A
Y
Y
NA
N
A
C
ompl
ete
com
pete
ncy
eval
uatio
ns th
at a
re a
ge s
peci
fic a
nd in
clud
e: n
eona
tes,
in
fant
s, c
hild
ren
& a
dole
scen
ts a
s pe
r loc
al c
rede
ntia
ling
NA
Y
Y
Y
N
A
Y
Y
NA
N
A
QU
ALI
TY IM
PRO
VEM
ENT
mee
ts 2
008
EMSA
gui
delin
es
P
edia
tric
QI P
lan
shou
ld b
e es
tabl
ishe
d Y
Y Y
Y1,4
Y1,3
Y4Y
Y Y1,
3
Ped
i QI P
lan
inte
rface
s w
ith in
tern
al a
nd e
xter
nal p
reho
spita
l & h
ospi
tal-w
ide
QI a
ctiv
ities
Y
Y
Y
Y
Y
4Y4
Y Y
Y4
Ped
i QI p
lan
may
incl
ude
the
follo
win
g:
Y
Y
Y
Y
Y4
Y1Y
Y Y4
P
erio
dic
revi
ew o
f agg
rega
te d
ata
of p
edia
tric
emer
genc
y vi
sits
Y
Y
Y
Y
4Y4
Y1Y
Y Y4
R
evie
w o
f pre
hosp
ital &
ED
ped
i pat
ient
car
e in
dica
tors
whi
ch m
ay in
clud
e: d
eath
s,
trans
fers
, chi
ld m
altre
atm
ent,
arre
sts,
trau
ma,
sur
gica
l & IC
U c
ases
. Pat
ient
saf
ety
& m
edic
atio
n ad
vers
e ev
ents
.
Y Y
Y Y
Y4
Y Y
Y4
M
echa
nism
to m
onito
r pro
fess
iona
l cre
dent
ialin
g, e
duca
tion
and
com
pete
ncie
s Y
Y
Y
Y
Y
Y
Y
Y
Y
Mec
hani
sm to
pro
vide
for i
nteg
ratio
n of
find
ing
from
QI p
roce
ss a
nd re
view
s in
to
educ
atio
n an
d cl
inic
al c
ompe
tenc
y ev
alua
tions
of E
D s
taff.
Y
Y Y
Y Y4
Y1,4
Y Y
Y4
Foot
note
s:
1 P
edia
tric
plan
par
t of g
ener
al E
D Q
I Pla
n 2 E
xcee
ds re
quire
men
t: A
ll E
D R
N s
taff
curr
ent i
n P
ALS
/EN
PC
or e
quiv
alen
t 3 P
lan
to d
evel
op
4 Lim
ited
to c
ase
revi
ew
5 Ped
iatri
c co
mpe
tenc
y-ba
sed
prog
ram
in p
lace
Page
2
12
/24/
2008

Con
tra
Cos
ta C
ount
y 20
08 E
MSC
Em
erge
ncy
Dep
artm
ent A
sses
smen
t Sum
mar
y*
A: CCRMC
B: Doctors-SP
C: JMMC-WC
D: Kaiser- R
E: Kaiser-WC
F: JMMC-C
G: Sutter Delta
H: SRVRMC
I: Kaiser: A
POLI
CIE
S A
ND
PR
OC
EDU
RES
mee
ts 2
008
EMSA
gui
delin
es1
E
stab
lishe
d po
lices
and
pro
cedu
res
for p
edia
tric
emer
genc
y pa
tient
s ar
e no
t lim
ited
but
shou
ld i
nclu
de:
Y Y
Y Y
Y Y
Y Y
Y
Ill
ness
and
inju
ry tr
iage
Y
Y
Y
Y
Y
Y
Y
Y
Y
Pedi
atric
ass
essm
ent
Y Y
Y Y
Y Y
Y Y
Y
Phys
ical
or c
hem
ical
rest
rain
t of p
atie
nts
Y Y
Y
Y
Y
Y
Y
Y
Y
Chi
ld m
altre
atm
ent
Y Y
Y Y
Y Y
Y Y
Y
Saf
e su
rrend
er &
chi
ld a
band
onm
ent
Y
Y
Y
Y
Y
Y
Y
Y
Y
C
onse
nt (i
nclu
ding
situ
atio
ns in
whi
ch a
par
ent i
s no
t im
med
iate
ly a
vaila
ble)
Y
Y
Y
Y
Y
Y
Y
Y
Y
DN
R o
rder
s Y
Y1Y
Y Y
Y1Y
Y Y
P
roce
dura
l sed
atio
n Y
Y Y
Y Y
Y Y
Y Y
D
eath
in E
D to
incl
ude
SID
S &
car
e of
the
grie
ving
fam
ily
N5
N5
Y Y
Y N
5N
5Y
N5
R
adia
tions
dos
age
prot
ocol
Y
Y Y
Y Y
Y Y
Y Y
S
ched
uled
resu
scita
tion
med
ical
and
sup
ply
inve
ntor
y ch
eck
Y
Y
Y
Y
Y
Y
Y
Y
Y
Im
mun
izat
ion
stat
us
Y Y
Y Y
Y Y
Y Y
Y
Men
tal h
ealth
em
erge
ncie
s Y
Y
Y
Y
Y
Y
Y
Y
4Y
Fa
mily
Cen
tere
d C
are
incl
udin
g: p
atie
nt ,
fam
ily a
nd c
areg
iver
edu
catio
n, D
isch
arge
pl
anni
ng a
nd in
stru
ctio
n, fa
mily
pre
senc
e du
ring
care
. Y
Y Y
Y Y
Y Y
Y Y
C
omm
unic
atio
n w
ith p
atie
nt’s
prim
ary
heal
th c
are
prov
ider
. Y
5Y
Y Y
Y Y2
Y Y
Y
Pai
n as
sess
men
t and
trea
tmen
t Y
Y
Y
Y
Y
Y
Y
Y
Y
Dis
aste
r pre
pare
dnes
s pl
an a
ddre
ssin
g pe
diat
ric is
sues
: par
ent c
hild
sep
arat
ion
and
reun
ifica
tion,
ped
iatri
c su
rge
capa
city
, dis
aste
r med
ical
, men
tal &
soc
ial s
ervi
ces
for
child
ren,
dis
aste
r dril
ls in
clud
e pe
diat
ric m
ass
casu
alty
inci
dent
one
eve
ry 2
yea
rs &
de
cont
amin
atio
n.
Y3Y3
Y2,3
Y3Y3
Y1,4
Y3Y4
Y3
M
edic
atio
n sa
fety
: rec
ord
all w
eigh
ts in
kg,
med
ical
err
or re
porti
ng, f
amily
invo
lvem
ent i
n m
edic
atio
n sa
fety
pro
cess
, med
icat
ion
orde
rs c
lear
& u
nam
bigu
ous.
Y
Y Y
Y Y
Y Y
Y Y
Foot
note
s:
1 Thi
s lis
t was
exp
ande
d w
ith 2
008
upda
te o
f Sta
te E
MS
C g
uide
lines
. Ped
iatri
c po
licie
s, p
roce
dure
s or
pro
toco
ls m
ay b
e a
com
pone
nt o
f ED
or h
ospi
tal p
olic
y &
pro
cedu
re o
r may
be
addr
esse
d as
sep
arat
e pe
diat
ric s
peci
fic d
ocum
ents
. 2 P
lan
to d
evel
op
3 Has
gen
eric
dis
aste
r pla
n w
ith s
ome
or li
mite
d pe
diat
ric a
spec
ts
4 Add
ition
al p
edi a
nd a
dole
scen
t asp
ects
pla
nned
to e
nhan
ce c
urre
nt p
olic
ies,
pro
toco
ls &
gui
delin
es
5 E
stab
lishe
d in
form
al p
roce
sses
in p
lace
with
no
form
al p
edia
tric
polic
y
Page
3
12
/24/
2008

Con
tra
Cos
ta C
ount
y 20
08 E
MSC
Em
erge
ncy
Dep
artm
ent A
sses
smen
t Sum
mar
y*
A: CCRMC
B: Doctors-SP
C: JMMC-WC
D: Kaiser-R
E: Kaiser-WC
F: JMMC-C
G: Sutter Delta
H: SRVRMC
I: Kaiser-A
An
Inte
rfac
ility
Con
sulta
tion
and
tran
sfer
Pla
n fo
r ter
tiary
or s
peci
aliz
ed c
are
shou
ld in
clud
e at
a m
inim
um th
e fo
llow
ing
in li
ne w
ith 2
008
EMSA
gui
delin
es.
Pla
n fo
r sub
-spe
cial
ty c
onsu
ltatio
n (te
leph
one
or re
al-ti
me
tele
med
icin
e 24
/hrs
per
day
) Y
Y
Y
Y
Y
Y
Y
Y
Y
Id
entif
icat
ion
of tr
ansf
errin
g an
d re
ceiv
ing
faci
litie
s re
spon
sibi
litie
s in
com
plia
nce
with
EM
TALA
Y
Y
3Y
Y Y
Y Y
Y Y
Est
ablis
hmen
t of i
nter
-faci
lity
trans
fer a
gree
men
ts (i
nclu
ding
repa
triat
ion
of th
e ch
ild b
ack
to h
is/h
er
com
mun
ity a
s ap
prop
riate
) sho
uld
incl
ude
the
follo
win
g pe
diat
ric s
peci
alty
refe
rral
reso
urce
s:
M
edic
al a
nd s
urgi
cal p
edia
tric
inte
nsiv
e ca
re
Tr
aum
a
Re-
impl
anta
tion
(rep
lace
men
t of s
ever
ed d
igits
or l
imbs
)
Bur
ns
P
sych
iatri
c em
erge
ncie
s
Obs
tetri
c an
d pe
rinat
al e
mer
genc
ies
C
hild
mal
treat
men
t
Y2Y2
Y2Y2
Y2Y2
Y2Y2
Y2
Gui
delin
es fo
r Sup
port
Ser
vice
s fo
r the
ED
in li
ne w
ith 2
008
EMSA
gui
delin
es.
R
espi
rato
ry C
are
Prac
titio
ners
(who
resp
ond
to th
e E
D) s
houl
d in
clud
e qu
alifi
ed s
taff
and
nece
ssar
y eq
uipm
ent a
nd s
uppl
ies
to c
are
for c
hild
ren
in th
e E
D
Y Y
Y Y
Y Y
Y Y
Y
Res
pira
tory
Car
e S
taffi
ng
Y Y
Y Y
Y Y
Y Y
Y
At l
east
one
resp
irato
ry c
are
or e
quiv
alen
t pra
ctiti
oner
in h
ouse
24
hrs/
day
Y
Y
Y
Y
Y
Y
Y
Y
Y
C
ompl
ete
pedi
atric
com
pete
ncy
eval
uatio
ns th
at a
re a
ge s
peci
fic a
nd in
clud
e ne
onat
es,
infa
nts,
chi
ldre
n an
d ad
oles
cent
s as
requ
ired
by lo
cal c
rede
ntia
ling.
Y
Y Y
Y Y
Y Y
Y Y
Rad
iolo
gy S
ervi
ces
shou
ld in
clud
e qu
alifi
ed s
taff
& n
eces
sary
equ
ipm
ent &
sup
plie
s to
pro
vide
im
agin
g st
udie
s of
chi
ldre
n in
clud
ing:
Pro
toco
ls th
at in
clud
e m
odifi
catio
n of
radi
atio
n ex
posu
re o
f chi
ldre
n ba
sed
on a
ge a
nd
wei
ght,
pedi
atric
radi
atio
n do
sing
and
pro
tect
ive
shie
ldin
g of
chi
ldre
n fo
r pla
in ra
diog
raph
y an
d C
T
Y Y
Y Y
Y Y2
Y Y
Y
Clin
ical
Lab
orat
ory
Serv
ices
wou
ld in
clud
e qu
alifi
ed s
taff
and
nece
ssar
y eq
uipm
ent &
sup
plie
s to
pr
ovid
e la
bora
tory
ser
vice
s an
d te
stin
g/an
alys
is in
clud
ing
but n
ot li
mite
d to
:
Obt
aini
ng s
ampl
es fr
om c
hild
ren
of a
ll ag
es
M
icro
-cap
abilit
ies
Y Y
Y Y
Y Y
Y Y
Y
Foot
note
: 1 P
lan
is in
dev
elop
men
t 2 S
ome
com
pone
nts
liste
d m
ay n
ot b
e m
et
3 Info
rmal
agr
eem
ents
in p
lace
Page
4
12
/24/
2008

Con
tra
Cos
ta C
ount
y 20
08 E
MSC
Em
erge
ncy
Dep
artm
ent A
sses
smen
t Sum
mar
y*
A: CCRMC
B: Doctors-SP
C: JMMC-WC
D:Kaiser-R
E:Kaiser-WC
F: JMMC-C
G: Sutter Delta
H: SRVRMC
I: Kaiser-A
Equi
pmen
t, Su
pplie
s &
Med
iatio
ns fo
r the
Car
e of
Ped
i Pat
ient
s in
the
ED in
line
with
200
8 EM
SA g
uide
lines
.
Ped
iatri
c eq
uipm
ent,
supp
lies
& m
edic
atio
ns s
houl
d be
eas
ily a
cces
sibl
e, la
bele
d an
d lo
gica
lly
orga
nize
d Y
Y Y
Y Y
Y Y
YY
ED
sta
ff sh
ould
be
appr
opria
tely
edu
cate
d to
loca
tion
of a
ll ite
ms
Y
Y
Y
Y
Y
Y
Y
YY
Mob
ile p
edia
tric
cras
h ca
rt re
com
men
ded
in E
D
Y Y
Y Y
Y Y
Y Y
Y
Leng
th b
ased
ped
iatri
c w
eigh
t mea
sure
men
t sys
tem
use
d fo
r in
an e
mer
genc
y (e
g: B
rose
low
) Y
Y
Y
Y
Y
Y
Y
Y
Y
Ped
iatri
c m
edic
atio
n ch
art,
tape
or m
edic
al s
oftw
are
or o
ther
sys
tem
in p
lace
to a
ssur
e re
ady
acce
ss
to p
rope
r siz
ing
of re
susc
itatio
n eq
uipm
ent a
nd p
rope
r dos
ing
of m
edic
atio
n sh
ould
be
easi
ly
acce
ssib
le
Y Y
Y Y
Y Y
Y Y
Y
Res
usci
tatio
n m
edic
atio
n as
per
200
5 AH
A P
ALS
gui
delin
es a
vaila
ble
Y
Y
Y
Y
Y
Y
Y
YY
Res
usci
tatio
n eq
uipm
ent (
reco
mm
enda
tions
per
Sta
te E
MS
C g
uide
lines
) and
sup
plie
s sh
ould
be
loca
ted
in th
e ED
.
Tray
s &
oth
er it
ems
may
be
hous
ed in
oth
er d
epar
tmen
ts e
g: N
ewbo
rn n
urse
ry o
r cen
tral
supp
ly im
med
iate
ly a
cces
sibl
e if
need
ed.
Y Y
Y Y
Y Y
Y Y
Y
Con
clus
ions
Fa
cilit
ies
have
met
or e
xcee
ded
Con
tra C
osta
EM
SC
Pla
n 20
00 g
oals
and
exp
ecta
tions
. P
edia
tric
inpa
tient
bed
cap
acity
has
bee
n su
bsta
ntia
lly re
duce
d to
1 b
ed fo
r eve
ry 5
000
child
ren
< 14
yea
rs in
the
EM
S s
yste
m s
ince
200
0. T
his
is th
e re
sult
of e
limin
atio
n of
ped
iatri
c be
ds a
t Doc
tors
San
Pab
lo, C
CR
MC
& J
MM
C-C
onco
rd a
nd in
crea
sing
refe
rral
of s
ick
child
ren
to d
efin
itive
ped
iatri
c ca
re.
As
of J
anua
ry 1
, 200
9 th
ere
are
44 g
ener
al p
edia
tric
beds
, 47
new
born
nur
sery
bed
s an
d 48
NIC
U b
eds
in th
e C
ontra
Cos
ta E
MS
sys
tem
. O
ppor
tuni
ties
exis
t to
impr
ove
Con
tra C
osta
EM
SC
Pro
gram
in th
e fo
llow
ing
area
s:
P
edia
tric
CQ
I pro
cess
es.
P
olic
y an
d pr
otoc
ols
for m
anag
ing
pedi
atric
dea
th in
the
ED
incl
udin
g si
tuat
iona
l sup
port
for h
ealth
car
e pr
ovid
ers.
Enh
ance
d ed
ucat
ion
and
train
ing
in th
e ea
rly re
cogn
ition
and
inte
rven
tion
of th
e pe
diat
ric p
re-a
rres
t sta
te to
impr
ove
outc
omes
.
Dev
elop
men
t of c
riter
ia fo
r ped
iatri
c in
patie
nt c
onsu
ltatio
n w
ithin
eac
h fa
cilit
y.
P
edia
tric
disa
ster
pre
pare
dnes
s in
clud
ing
the
pedi
atric
sur
ge c
apab
ility
Enh
ance
d pr
ehos
pita
l and
em
erge
ncy
depa
rtmen
t col
labo
ratio
n on
ped
iatri
c em
erge
ncy
care
issu
es in
clud
ing
inju
ry p
reve
ntio
n Pa
ge 5
12/2
4/20
08

Con
tra
Cos
ta 2
008
EMSC
Sur
vey
Emer
genc
y D
epar
tmen
t Cha
ract
eris
tics
A: CCRMC
B: Doctors-SP
C: JMMC-WC
D: Kaiser-R
E: Kaiser-WC
F: JMMC-C
G: Sutter Delta
H: SRVRMC
I: Kaiser-A opened 11/07
Pedi
atric
Em
erge
ncy
Visi
ts in
200
7 6,
316
7,20
0
23%
of
ED
vis
its
6,42
3 6,
000
5,78
4 8,
024
18.2
% o
f E
D v
isits
15,0
006
25%
of E
D
visi
ts
2,89
5 23
% o
f E
D v
isits
4821
% A
rrivi
ng b
y pr
ivat
e ve
hicl
e 95
%
80%
?
? 90
.5%
55
2 ?
90%
?
90.4
%
4361
98%
10
0%
100%
410
0%
100%
10
0%
100%
10
0%
100%
%
ED
RN
sta
ff tra
ined
in P
ALS
/EN
PC
or
equi
vale
nt
100%
10
0%2
100%
10
0%
100%
10
0%2
100%
10
0%
100%
%
ED
MD
s tra
ined
in P
ALS
/AP
LS o
r eq
uiva
lent
P
edia
tric
patie
nt d
efin
ed a
s (a
ges)
0-
13 y
r 0-
18 y
r 0-
13 y
r 1d
–18
yr
0-18
yr
0-18
yr
0-18
yr
1d-1
8 yr
0-
18 y
r
Do
you
have
ded
icat
ed p
edia
tric
inpa
tient
or
out
patie
nt s
ervi
ces
Y
N
Y
N
Y
Y
Y
Y
Y
Do
you
have
ped
iatri
c ge
nera
l car
e be
ds
N
N
Y
17
bed
s N
Y
12
bed
s N
5Y
7
beds
Y
5
8 be
ds
N
PIC
U b
eds
N
N
N
N
N
N
N
N
N
New
born
Nur
sery
bed
s Y
6 be
ds
N
Y
19
-20
beds
N
Y
ro
om in
N
Y
ro
om in
Y
15
bed
s Y
6 be
ds
NIC
U b
eds
N
N
Y
4
beds
N
Y
28
bed
s N
Y
4
beds
Y
2
beds
Y
10 b
eds
Ped
iatri
c cl
inic
s: g
ener
al/s
peci
alty
car
e Y
N
Y
N
Y
N
N
N
Y
Adm
it pe
diat
ric p
atie
nts
to a
dult
units
? N
Y5
pts
>14
N
N
Y
pts
> 14
Y
5
pts
> 6
N
Y
Y
pts
> 14
W
hat f
acilit
ies
do y
ou tr
ansf
er p
edia
tric
patie
nts
to
CH
O
JMM
C-W
C
CH
O
KP
-OA
K
CC
RM
C3
CH
O
UC
SF
LPC
H
UC
Dav
is
Shr
iner
s S
t Fra
ncis
C
PM
D
JMH
-Pav
CH
O
KP
-OK
K
P-O
K
KP
-SA
C
KP
-SC
C
HO
U
CS
F LP
CH
CH
O
JMM
C-W
C
CC
RM
C3
LPC
H
UC
Dav
is
UC
SF
Kai
ser
CH
O
JMM
C-W
C
JMM
C-C
LP
CH
CH
O
JMH
-Pav
K
aise
r JM
MC
-C
Her
rick
LPC
H
CH
O
KP
-OK
U
CS
F
S
t Fra
ncis
Frem
ont
Hos
p
Page
6
12
/24/
2008

A: CCRMC
B: Doctors-SP
C: JMMC-WC
D: K/Richmond
E: K/Walnut Crk
F: JMMC-C
G: Sutter Delta
H: SRVRMC
I: K/Antioch opened 11/07
Invo
lved
in p
edia
tric
prev
entio
n ac
tiviti
es
Y
Y
Y
Y
Y
Y
Y
Y
Y
Inte
rest
ed in
Joi
nt E
D/P
reho
spita
l tra
inin
g us
ing
pedi
atric
pat
ient
sim
ulat
or
Y
Y
Y
Y
Y
Y
Y
N
Y
Hea
rd a
bout
new
AC
DA
ped
i em
erge
ncy
asse
ssm
ent m
odel
taug
ht in
PA
LS/P
EA
RS
N
N
Y
Y
Y
N
N
Y
Y
Y
Y
Y
Y
Y
Y
Y
N
Y
Inte
rest
ed in
a s
taff
train
ing
on th
is n
ew
appr
oach
Fo
otno
tes:
1 F
acili
ty o
pene
d in
Nov
200
8 2 A
ll M
Ds
train
ed in
itial
ly b
ut u
nkno
wn
how
man
y cu
rren
t 3 C
CR
MC
ped
iatri
c un
it cl
osed
in 2
008
4 With
in 6
mon
ths
of h
ire
5 Lic
ense
d as
med
/sur
g be
ds n
ot d
edic
ated
ped
iatri
c un
it 6 E
stim
ated
vol
umes
of p
edia
tric
patie
nts
Rec
omm
enda
tions
/com
men
ts fr
om fa
cilit
ies
to s
uppo
rt fo
r ED
effo
rts
to im
prov
e th
e ca
re o
f chi
ldre
n:
Ass
ist i
n pr
ovid
ing
EN
PC c
lass
es in
Con
tra C
osta
Cou
nty
Bet
ter p
reho
spita
l com
mun
icat
ion
Bet
ter r
espo
nse
to c
ritic
al c
are
trans
fers
B
y gi
ving
the
hosp
itals
add
ition
al a
ssis
tanc
e fo
r tra
inin
g an
d su
pplie
s th
roug
h m
oney
reso
urce
s an
d co
llabo
rativ
e pa
rtner
ship
s in
ord
er to
impr
ove
care
to p
edia
tric
patie
nts.
B
e aw
are
of li
mita
tions
O
pen
com
mun
icat
ion
betw
een
ED
& E
MS
. C
onst
ruct
ive
feed
back
onc
e cr
itica
l ped
iatri
c pa
tient
has
bee
n tra
nspo
rted
to th
e E
D.
Use
eve
ry o
ppor
tuni
ty to
lear
n fro
m o
ur c
ases
to c
ontin
uous
ly im
prov
e th
e ca
re d
eliv
ered
.
Page
7
12
/24/
2008

Appendix G
Contra Costa EMSC Injury Prevention
Resource List


PFro
st C
ontra
Cos
ta E
MSC
Coo
rdin
ator
12.
24.0
8
Con
tra
Cos
ta E
mer
genc
y M
edic
al S
ervi
ces
EM
S fo
r C
hild
ren
In
jury
Pre
vent
ion
Res
ourc
e L
ist
C
ontr
a C
osta
Cou
nty
has n
umer
ous l
ocal
res
ourc
es d
edic
ated
to in
jury
pre
vent
ion.
Thi
s lis
t is m
eant
to h
ighl
ight
s som
e of
the
reso
urce
s rea
dily
ava
ilabl
e in
the
com
mun
ity. T
he m
ajor
ity o
f the
se r
esou
rces
are
web
bas
ed p
rovi
ding
acc
ess t
o in
jury
pre
vent
ion
educ
atio
nal m
ater
ials
, res
ourc
es a
nd p
rogr
ams a
t any
time.
E
MS
Stak
ehol
ders
are
enc
oura
ged
to u
se th
ese
reso
urce
s. C
onta
ct C
ontr
a C
osta
EM
S to
add
you
r pr
ogra
m to
this
list
. N
ame
of O
rgan
izat
ion
Mis
sion
, Des
crip
tion
or P
urpo
se
Web
site
/Con
tact
Info
rmat
ion
Eas
t Bay
Chi
ld In
jury
Pr
even
tion
Net
wor
k (E
BC
IPN
)
Form
erly
Con
tra C
osta
Inju
ry P
reve
ntio
n C
oalit
ion.
Thi
s gr
oup
prov
ides
net
wor
king
opp
ortu
nitie
s to
inju
ry p
reve
ntio
n sp
ecia
lists
and
gro
ups t
o pr
omot
e ch
ild in
jury
pre
vent
ion
in
thei
r com
mun
ities
. Th
e vi
sion
of t
he E
BC
IPN
will
cre
ate
a sa
fer w
orld
for a
ll ch
ildre
n by
redu
cing
pre
vent
able
inju
ries.
Cha
ir Ja
ckW
alsh
39@
aol.c
om
Con
tra
Cos
ta H
ealth
Se
rvic
es In
jury
Pre
vent
ion
Proj
ect
Con
duct
cla
ssro
om b
icyc
le a
nd p
edes
trian
safe
ty
pres
enta
tions
, wal
king
eve
nts,
helm
et d
istri
butio
n an
d bi
ke
rode
os. W
orki
ng to
cre
ate
a sa
fer s
treet
and
com
mun
ity
envi
ronm
ent f
or w
alki
ng a
nd b
icyc
ling.
ww
w.c
chea
lth.o
rg/g
roup
s/pr
even
tion/
Kee
ping
Bab
ies S
afe
Kee
ping
Bab
ies S
afe
exis
ts to
pro
vide
lead
ersh
ip in
kee
ping
ba
bies
safe
from
pre
vent
able
inju
ries a
nd d
eath
s ass
ocia
ted
with
uns
afe
crib
s, da
nger
ous c
hild
ren'
s pro
duct
s and
uns
afe
slee
p en
viro
nmen
ts.
ww
w.k
eepi
ngba
bies
safe
.org
Chi
ldre
n’s H
ospi
tal &
R
esea
rch
Cen
ter
Oak
land
H
ere
to h
elp
if a
child
is in
jure
d. B
ut a
lso
focu
sed
on
prev
entin
g th
e in
jury
in th
e fir
st p
lace
. By
som
e es
timat
es,
90 p
erce
nt o
f uni
nten
tiona
l inj
urie
s can
be
avoi
ded.
The
w
ebsi
te p
rovi
des i
nfor
mat
ion
to k
eep
child
ren
out o
f har
m's
way
.
ww
w.c
hild
rens
hosp
italo
akla
nd.o
rg/h
ealth
car
e/de
pts/
keep
ings
afe.
asp
Safe
Kid
s A
nat
iona
l and
glo
bal n
etw
ork
of o
rgan
izat
ions
who
se
mis
sion
is to
pre
vent
acc
iden
tal c
hild
hood
inju
ry, a
lead
ing
kille
r of c
hild
ren
14 a
nd u
nder
.
ww
w.u
sa.sa
feki
ds.o
rgLo
cal C
oalit
ion
SA
FE K
IDS
Ala
med
a C
ount
y
510-
618-
2048

PFro
st C
ontra
Cos
ta E
MSC
Coo
rdin
ator
12.
24.0
8
Con
tra
Cos
ta E
mer
genc
y M
edic
al S
ervi
ces
EM
S fo
r C
hild
ren
In
jury
Pre
vent
ion
Res
ourc
e L
ist
Nam
e of
Org
aniz
atio
n M
issi
on, D
escr
iptio
n or
Pur
pose
W
ebsi
te/C
onta
ct In
form
atio
n D
row
ning
Pre
vent
ion
Foun
datio
n To
pre
vent
the
trage
dy o
f dro
wni
ngs t
hrou
gh p
ublic
info
rmat
ion,
ed
ucat
ion
and
polic
y ch
ange
w
ww
.dro
wni
ngpr
even
tionf
ound
atio
n.us
Con
tra
Cos
ta H
ealth
Se
rvic
es B
icyc
le &
Pe
dest
rian
Saf
ety
Proj
ect
Educ
atio
nal m
ater
ials
, hel
met
s; b
icyc
le ro
deo
equi
pmen
t; di
vers
ion
prog
ram
w
ww
.cch
ealth
.org
/topi
cs/c
hild
_saf
ety/
reso
urce
s.php
Con
tra
Cos
ta H
ealth
Se
rvic
es C
hild
Saf
ety
Res
ourc
es
Sour
ce fo
r web
site
s with
det
aile
d ho
me
safe
ty c
heck
lists
and
pr
even
tion
info
rmat
ion
ww
w.c
chea
lth.o
rg/to
pics
/chi
ld_s
afet
y/re
sour
ces.p
hp
Firs
t 5 C
ontr
a C
osta
Fi
rst 5
Con
tra C
osta
mak
es a
diff
eren
ce in
the
lives
of c
hild
ren
ages
0 to
5 a
nd th
eir f
amili
es b
y in
vest
ing
in lo
cal p
rogr
ams a
nd
serv
ices
des
igne
d to
hel
p ch
ildre
n re
ach
thei
r gre
ates
t pot
entia
l in
scho
ol a
nd li
fe. O
ur m
issi
on is
to h
elp
child
ren
grow
up
heal
thy,
re
ady
to le
arn,
and
supp
orte
d in
safe
, nur
turin
g fa
mili
es a
nd
com
mun
ities
.
ww
w.fi
rstfi
vecc
.org
Stre
et S
mar
ts
Cre
ated
in 2
004
this
inju
ry p
reve
ntio
n pr
ogra
m fo
cuse
s on
child
in
jury
pre
vent
ion
and
com
mun
ity e
duca
tion
by a
ddre
ssin
g tra
ffic
sa
fety
pro
blem
s at i
ts so
urce
: in
the
min
ds o
f driv
ers,
pede
stria
ns
and
cycl
ists
.
ww
w.st
reet
smar
ts-s
rv.c
om
Con
tra
Cos
ta H
ealth
Se
rvic
es V
iole
nce
Prev
entio
n
A v
arie
ty o
f pro
gram
s car
ried
out b
y C
CH
S, o
ften
in p
artn
ersh
ip
or in
con
junc
tion
with
com
mun
ity p
rovi
ders
to d
ecre
ase
and
prev
ent y
outh
vio
lenc
e an
d it’
s con
sequ
ence
s.
ww
w.c
chea
lth.o
rg/to
pics
/vio
lenc
e/
Con
tra
Cos
ta C
risi
s Cen
ter
To
kee
p pe
ople
in C
ontra
Cos
ta C
ount
y, C
alifo
rnia
aliv
e an
d sa
fe,
help
them
thro
ugh
cris
es, a
nd c
onne
ct th
em w
ith c
ultu
rally
re
leva
nt re
sour
ces i
n th
e co
mm
unity
to c
hild
ren
and
fam
ilies
. In
clud
es S
IDS
supp
ort,
yout
h vi
olen
ce &
suic
ide
prev
entio
n an
d ho
mel
ess s
ervi
ces.
ww
w.c
risis
-cen
ter.o
rg

PFro
st C
ontra
Cos
ta E
MSC
Coo
rdin
ator
12.
24.0
8
Con
tra
Cos
ta E
mer
genc
y M
edic
al S
ervi
ces
EM
S fo
r C
hild
ren
In
jury
Pre
vent
ion
Res
ourc
e L
ist
Nam
e of
Org
aniz
atio
n M
issi
on, D
escr
iptio
n or
Pur
pose
W
ebsi
te/C
onta
ct In
form
atio
n C
hild
Abu
se P
reve
ntio
n C
ounc
il of
Con
tra
Cos
ta
Cou
nty
Mis
sion
is to
pro
mot
e th
e sa
fety
of o
ur c
hild
ren,
rais
e co
mm
unity
aw
aren
ess,
influ
ence
pub
lic p
olic
y, e
duca
te o
ur c
omm
unity
and
fa
mili
es, p
rovi
de re
sour
ces a
nd su
ppor
t fam
ilies
ww
w.c
apc-
coco
.org
/pre
vent
ion-
inte
rven
tion.
htm
l
Cal
iforn
ia P
oiso
n C
ontr
ol
The
Cal
iforn
ia P
oiso
n C
ontro
l Sys
tem
(CPC
S) is
the
stat
ewid
e pr
ovid
er o
f im
med
iate
, fre
e an
d ex
pert
treat
men
t adv
ice
and
assi
stan
ce o
ver t
he te
leph
one
in c
ase
of e
xpos
ure
to p
oiso
nous
, ha
zard
ous o
r tox
ic su
bsta
nces
. Ava
ilabl
e to
ll-fr
ee, 2
4 ho
urs a
day
, 7
days
a w
eek,
365
day
s a y
ear
ww
w.c
alpo
ison
.org
Pois
on A
ctio
n Li
ne
1-80
0-22
2-12
22
Con
tra
Cos
ta C
ount
y O
ffic
e of
E
duca
tion
Con
tra C
osta
Cou
nty
Off
ice
of E
duca
tion
emer
genc
y pr
epar
edne
ss
Web
pag
e go
al is
to p
rovi
de c
hild
care
pro
vide
rs a
nd p
aren
ts w
ith
easy
acc
ess t
o pe
rtine
nt e
mer
genc
y pr
epar
edne
ss in
form
atio
n an
d re
sour
ces a
s the
y re
late
to sc
hool
s thr
ough
out t
he c
ount
y.
ww
w.c
ccoe
.k12
.ca.
us/a
bout
/reso
urce
s_em
erge
ncy.
htm
l
San
Ram
on V
alle
y Fi
re
Prot
ectio
n D
istr
ict
Fred
die
the
Fire
truc
k an
imat
ed w
ebsi
te h
elps
kid
s and
thei
r fa
mili
es le
arn
to st
ay sa
fe. H
elps
chi
ldre
n de
term
ine
thei
r saf
ety
awar
enes
s. A
dditi
onal
pre
vent
ion
prog
ram
s foc
us o
n fir
e an
d bu
rn
prev
entio
n, h
ome
haza
rds,
elec
trica
l saf
ety,
cho
king
haz
ards
, bas
ic
first
aid
, fal
ls p
reve
ntio
n, d
row
ning
pre
vent
ion,
poi
son
prev
entio
n,
holid
ay sa
fety
and
veh
icle
safe
ty. T
hese
pre
vent
ion
activ
ities
im
pact
ove
r 25,
000
child
ren
a ye
ar.
ww
w.sr
vfpd
.dst
.ca.
us/k
ids/
inde
x.ht
m
Eve
ry 1
5 m
inut
es
Supp
orte
d by
John
Mui
r Wal
nut C
reek
Tra
uma
Cen
ter i
n co
llabo
ratio
n w
ith m
any
EMS
agen
cies
thro
ugho
ut C
ontra
Cos
ta
Cou
nty
Eve
ry 1
5 M
inut
es is
a tw
o-da
y pr
ogra
m th
at fo
cuse
s on
high
scho
ol ju
nior
s and
seni
ors.
It ch
alle
nges
teen
s to
thin
k ab
out
the
resp
onsi
bilit
y of
mak
ing
mat
ure
deci
sion
s abo
ut d
rinki
ng a
nd
driv
ing
and
the
impa
ct th
at th
eir d
ecis
ions
hav
e on
fam
ily, f
riend
s an
d ot
her m
embe
rs o
f the
ir co
mm
unity
. Thi
s em
otio
nally
cha
rged
w
orks
hop
feat
ures
sim
ulat
ions
, ree
nact
men
ts, g
uest
spea
kers
and
di
scus
sion
gro
ups.
ww
w.e
very
15m
inut
es.c
om/e
nter
/ent
er.h
tml
ww
w.jo
hnm
uirh
ealth
.com
/inde
x.ph
p/jm
mdh
s_al
lianc
e_ou
r_pr
ogra
ms_
broa
der1
.htm
l

PFro
st C
ontra
Cos
ta E
MSC
Coo
rdin
ator
12.
24.0
8
Con
tra
Cos
ta E
mer
genc
y M
edic
al S
ervi
ces
EM
S fo
r C
hild
ren
In
jury
Pre
vent
ion
Res
ourc
e L
ist
Nam
e of
Org
aniz
atio
n M
issi
on, D
escr
iptio
n or
Pur
pose
W
ebsi
te/C
onta
ct In
form
atio
n Jo
hn M
uir
Com
mun
ity H
ealth
A
llian
ce
Obj
ectiv
es o
f the
pro
gram
incl
ude:
Uni
nsur
ed, u
nder
serv
ed a
nd
vuln
erab
le p
opul
atio
ns in
the
serv
ice
area
hav
e ac
cess
to h
ealth
ca
re. H
ealth
edu
catio
n, p
reve
ntio
n an
d ea
rly d
etec
tion
serv
ices
are
av
aila
ble
to re
side
nts w
ith p
hysi
cal,
men
tal a
nd d
enta
l hea
lth
cond
ition
s. C
hild
hood
supp
ort s
ervi
ces a
re a
vaila
ble
to p
aren
ts a
nd
scho
ols.
Res
iden
ts a
re sa
fe fr
om in
tent
iona
l and
uni
nten
tiona
l in
jurie
s.
ww
w.jo
hnm
uirh
ealth
.com
/inde
x.ph
p/jm
mdh
s_al
lianc
e_ou
r_pr
ogra
ms_
broa
der1
.htm
l
Kai
ser
Perm
anen
te C
ontr
a C
osta
Cou
nty
This
web
site
pro
vide
s a w
ealth
of h
ealth
pro
mot
ion
and
inju
ry
prev
entio
n m
ater
ials
for K
aise
r and
non
-Kai
ser m
embe
rs in
our
co
mm
unity
.
ww
w.m
embe
rs.k
aise
rper
man
ente
.org
/kpw
eb/c
lus
terQ
uery
.do?
clus
ter=
liveh
ealth
y
Con
tra
Cos
ta F
ire
Prev
entio
n D
istr
ict
CC
FPD
Pub
lic E
duca
tion
Uni
t goa
l is t
hat a
ll of
our
citi
zens
, fro
m
pres
choo
lers
to se
nior
citi
zens
, will
lear
n th
e pr
oper
act
ion
to ta
ke
in a
sudd
en fi
re o
r life
em
erge
ncy.
We
have
a n
umbe
r of p
rogr
ams
and
tool
s to
acco
mpl
ish
this
goa
l. O
ur v
isio
n is
a F
ire D
istri
ct
whe
re n
o on
e su
ffer
s fire
inju
ry o
r dea
th d
ue to
lack
of k
now
ledg
e or
pre
para
tion.
Web
site
pro
vide
s a w
ealth
of r
esou
rces
and
link
s to
inju
ry p
reve
ntio
n an
d di
sast
er p
repa
redn
ess r
esou
rces
.
http
://w
ww
.ccc
fpd.
org/
PubE
d/In
tro.h
tml
Ric
hmon
d E
mer
genc
y A
ctio
n C
omm
unity
Tea
ms (
RE
AC
T)
This
pro
gram
pro
vide
s fre
e tra
inin
g fo
r the
com
mun
ity to
“re
act”
an
d ke
ep sa
fe w
hen
emer
genc
ies a
rise.
w
ww
.poi
ntric
hmon
d.co
m/R
EAC
T/
Pino
le F
ire
Dep
artm
ent
Prov
ides
a n
umbe
r of l
ocal
pro
gram
s and
web
reso
urce
s to
prot
ect
child
ren
from
inju
ry.
ww
w.c
i.pin
ole.
ca.u
s/fir
e/pr
ogra
ms.h
tml
C
ontr
a C
osta
Chi
ld C
are
Cou
ncil
Prov
ides
supp
ort a
nd a
ssis
tanc
e fo
r par
ents
to p
rom
ote
heal
thy
child
-saf
e en
viro
nmen
ts. A
lso
prov
ides
info
rmat
ion
and
supp
ort
for c
hild
ren
with
spec
ial n
eeds
. Web
site
has
a la
rge
num
ber o
f re
sour
ces a
nd e
duca
tiona
l mat
eria
ls to
supp
ort i
njur
y pr
even
tion.
ww
w.c
ocok
ids.o
rg/

Appendix H
Contra Costa EMSC Pediatric Emergency Training Programs
Course Comparison Resource


Con
tra
Cos
ta E
MSC
Pe
diat
ric
Em
erge
ncy
Tra
inin
g Pr
ogra
m C
ompa
riso
n
Prog
ram
Ta
rget
A
udie
nce
Leng
th
Cre
ated
by
Pu
rpos
e Sk
ills
Test
ed
Com
plet
ion
Req
uire
men
ts
Inst
ruct
or
Req
uire
men
ts
ENPC
E
mer
genc
y N
urse
P
edia
tric
Cou
rse
Dire
cted
to
Em
erge
ncy
Roo
m N
urse
s.
Initi
al
cour
se
16 h
ours
w
ith 8
ho
ur
rene
wal
co
urse
. H
as
inst
ruct
or
cour
se
com
pone
nt
Em
erge
ncy
Nur
ses
Asso
ciat
ion
in
coop
erat
ion
with
AH
A
and
AA
P.
Inte
rnat
ion
ally
ap
prov
ed
curr
icul
um
from
the
EN
A
Pre
sent
s co
re le
vel
know
ledg
e to
and
ps
ycho
mot
er s
kills
as
soci
ated
with
nur
sing
ca
re fo
r chi
ldre
n in
the
emer
genc
y de
partm
ent.
Inco
rpor
ates
AH
A
stan
dard
s bu
t no
long
er h
as P
ALS
re
new
al o
ptio
n
Con
tent
incl
udes
: The
P
edia
tric
Pat
ient
Initi
al
Ass
essm
ent a
nd T
riage
R
espi
rato
ry D
istre
ss a
nd
Failu
re C
ardi
ovas
cula
r Em
erge
ncie
s M
edic
al
Emer
genc
ies
Chi
ld
Mal
treat
men
t To
xico
logi
c E
mer
genc
ies
Ped
iatri
c Tr
aum
a C
risis
Inte
rven
tion
The
Neo
nate
Sta
biliz
atio
n an
d Tr
ansp
ort
Ped
iatri
c C
onsi
dera
tions
: R
espi
rato
ry
Inte
rven
tions
, V
ascu
lar A
cces
s,
Pain
M
anag
emen
t an
d M
edic
atio
n A
dmin
istra
tion
and
Posi
tioni
ng
and
Imm
obiliz
atio
n Te
chni
ques
P
edia
tric
Mul
tiple
Tr
aum
a Pe
diat
ric
Res
usci
tatio
n
Eval
uatio
n M
etho
ds
Suc
cess
ful c
ompl
etio
n of
the
cour
se in
clud
es
scor
ing
a m
inim
um o
f 80
% o
n th
e 50
item
m
ultip
le c
hoic
e ex
amin
atio
n an
d de
mon
stra
ting
all
criti
cal s
teps
and
70%
of
the
tota
l poi
nts
in
the
eval
uate
d sk
ill st
atio
ns. P
artic
ipan
ts
have
the
abili
ty to
re
peat
the
writ
ten
exam
inat
ion
or a
ps
ycho
mot
or s
kill
stat
ion
if ne
eded
.
ENPC
Ver
ifica
tion
Ver
ifica
tion
will
be
issu
ed fr
om E
NA
with
su
cces
sful
com
plet
ion
of th
e co
urse
. V
erifi
catio
n re
mai
ns
curre
nt fo
r fou
r yea
rs.
EN
PC
app
rove
d co
urse
dire
ctor
, fa
culty
per
E
NP
C
Adm
inis
trativ
e G
uide
lines
. In
stru
ctor
s m
ust
com
plet
e in
stru
ctor
co
urse
and
be
mon
itore
d (m
uch
like
AH
A
prog
ram
facu
lty)
This
com
paris
on w
as c
ompi
led
afte
r rev
iew
of e
ach
cour
ses c
onte
nt a
nd w
eb si
te in
form
atio
n as
of M
arch
200
8
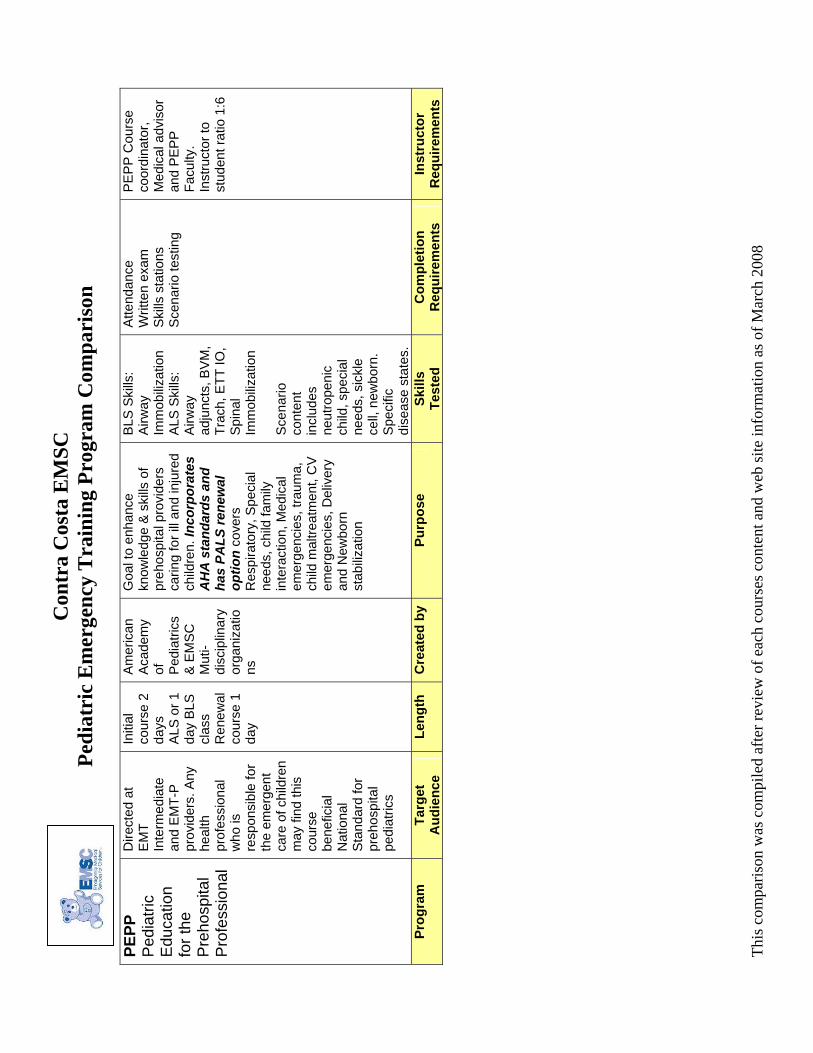
Con
tra
Cos
ta E
MSC
Pe
diat
ric
Em
erge
ncy
Tra
inin
g Pr
ogra
m C
ompa
riso
n
PEPP
P
edia
tric
Edu
catio
n fo
r the
P
reho
spita
l P
rofe
ssio
nal
Dire
cted
at
EM
T In
term
edia
te
and
EM
T-P
pr
ovid
ers.
Any
he
alth
pr
ofes
sion
al
who
is
resp
onsi
ble
for
the
emer
gent
ca
re o
f chi
ldre
n m
ay fi
nd th
is
cour
se
bene
ficia
l N
atio
nal
Sta
ndar
d fo
r pr
ehos
pita
l pe
diat
rics
Initi
al
cour
se 2
da
ys
ALS
or 1
da
y B
LS
clas
s R
enew
al
cour
se 1
da
y
Am
eric
an
Aca
dem
y of
P
edia
trics
&
EM
SC
M
uti-
disc
iplin
ary
orga
niza
tions
Goa
l to
enha
nce
know
ledg
e &
ski
lls o
f pr
ehos
pita
l pro
vide
rs
carin
g fo
r ill
and
inju
red
child
ren.
Inco
rpor
ates
A
HA
sta
ndar
ds a
nd
has
PALS
rene
wal
op
tion
cove
rs
Res
pira
tory
, Spe
cial
ne
eds,
chi
ld fa
mily
in
tera
ctio
n, M
edic
al
emer
genc
ies,
trau
ma,
ch
ild m
altre
atm
ent,
CV
em
erge
ncie
s, D
eliv
ery
and
New
born
st
abiliz
atio
n
BLS
Ski
lls:
Airw
ay
Imm
obiliz
atio
n A
LS S
kills
: A
irway
ad
junc
ts, B
VM
, Tr
ach,
ETT
IO,
Spi
nal
Imm
obiliz
atio
n S
cena
rio
cont
ent
incl
udes
ne
utro
peni
c ch
ild, s
peci
al
need
s, s
ickl
e ce
ll, n
ewbo
rn.
Spe
cific
di
seas
e st
ates
.
Atte
ndan
ce
Writ
ten
exam
S
kills
sta
tions
S
cena
rio te
stin
g
PE
PP
Cou
rse
coor
dina
tor,
Med
ical
adv
isor
an
d P
EP
P
Facu
lty.
Inst
ruct
or to
st
uden
t rat
io 1
:6
Prog
ram
Ta
rget
A
udie
nce
Leng
th
Cre
ated
by
Pu
rpos
e Sk
ills
Test
ed
Com
plet
ion
Req
uire
men
ts
Inst
ruct
or
Req
uire
men
ts
This
com
paris
on w
as c
ompi
led
afte
r rev
iew
of e
ach
cour
ses c
onte
nt a
nd w
eb si
te in
form
atio
n as
of M
arch
200
8

Con
tra
Cos
ta E
MSC
Pe
diat
ric
Em
erge
ncy
Tra
inin
g Pr
ogra
m C
ompa
riso
n
PEA
RS
Ped
iatri
c E
mer
genc
y A
sses
smen
t, R
ecog
nitio
n an
d S
tabi
lizat
ion
Dire
cted
at a
ll pr
ehos
ptia
l pe
diat
ric c
are
prov
ider
s, a
ll he
alth
car
e pr
ovid
ers
who
ar
e no
t tra
ined
in
ped
iatri
cs.
Prer
equi
site
be
pro
ficie
nt in
C
PR
and
read
an
d st
udy
the
PEAR
S pr
ovid
er
man
ual a
nd
stud
ent C
D
Initi
al
cour
se 1
da
y
AH
A a
nd
Am
eric
an
Aca
dem
y of
P
edia
trics
.
Focu
s is
on
the
rapi
d as
sess
men
t and
ear
ly
inte
rven
tion
of th
e pr
e-ar
rest
sta
te to
ef
fect
ivel
y PR
EVEN
T pe
diat
ric a
rres
t. N
ew
natio
nal s
tand
ard
for
pedi
atric
ass
essm
ent
and
reco
gniti
on
trai
ning
. Ta
kes
PALS
Ass
ess,
C
ateg
oriz
e, D
ecid
e &
A
ct M
odel
with
PA
T (P
edia
tric
A
sses
smen
t Tria
ngle
as
com
pone
nt o
f A
sses
s).
Use
s Pr
imar
y A
sses
smen
t, Se
cond
ary
Ass
essm
ent a
nd
Tert
iatr
y A
sses
smen
t ap
proa
ch to
car
e C
ateg
oriz
e ill
ness
by
type
and
sev
erity
(R
ecog
nitio
n) a
nd th
e im
plem
enta
tion
of
appr
opria
te
inte
rven
tions
Ski
lls: P
edia
tric
asse
ssm
ent,
resp
irato
ry
skills
sta
tion,
ci
rcul
ator
y ag
ency
, re
susc
itatio
n te
am c
once
pt,
Asse
ssm
ent
and
reco
gniti
on
key
skill
s ta
ught
Bef
ore
cour
se:
revi
ew te
xt a
nd
PE
AR
S s
tude
nt C
D
activ
ities
. Dur
ing
cour
se a
ctiv
ely
parti
cipa
te p
ract
ice,
&
com
plet
e al
l ski
lls
stat
ions
and
le
arni
ng s
tatio
ns.
Pas
s sk
ills
test
s in
ch
ild 1
resc
uer a
nd
infa
nt 1
& 2
resc
uer
CP
R/A
ED
. Pas
s a
vide
o-ba
sed
writ
ten
test
with
a m
inim
um
scor
e of
84%
PALS
In
stru
ctor
s P
ALS
Reg
iona
l Fa
culty
on
site
A
ppro
pria
te
pedi
atric
sp
ecia
lists
B
LS In
stru
ctor
In
stru
ctor
S
tude
nt R
atio
1:
8
Prog
ram
Ta
rget
A
udie
nce
Leng
th
Cre
ated
by
Pu
rpos
e Sk
ills
Test
ed
Com
plet
ion
Req
uire
men
ts
Inst
ruct
or
Req
uire
men
ts
This
com
paris
on w
as c
ompi
led
afte
r rev
iew
of e
ach
cour
ses c
onte
nt a
nd w
eb si
te in
form
atio
n as
of M
arch
200
8

Con
tra
Cos
ta E
MSC
Pe
diat
ric
Em
erge
ncy
Tra
inin
g Pr
ogra
m C
ompa
riso
n
PALS
P
edia
tric
Adv
ance
d Li
fe S
uppo
rt
Cur
rent
BLS
he
alth
car
e pr
ovid
er.
Dire
cted
for
pedi
atric
hea
lth
care
pro
vide
rs
(ped
iatri
cian
s,
pedi
atric
MD
sp
ecia
lists
, pe
diat
ric
inte
rns
resi
dent
s,
nurs
es) a
nd
emer
genc
y pe
rson
nel w
ho
treat
ped
iatri
c pa
tient
s in
clud
ing
preh
ospi
tal
prov
ider
s.
Con
tent
can
be
prio
ritiz
ed to
m
eet a
pa
rticu
lar t
arge
t au
dien
ce b
y co
urse
dire
ctor
.
Initi
al
cour
se 2
da
ys
Ren
ewal
co
urse
1
day
Lect
ures
de
liver
ed
via
vide
o fo
rmat
to
assu
re
all
cont
ent
deliv
ered
AH
A a
nd
Am
eric
an
Aca
dem
y of
P
edia
trics
Focu
s is
on
ALL
as
pect
s of
ped
iatri
c re
susc
itatio
n. N
atio
nal
stan
dard
for p
edia
tric
re
susc
itatio
n tr
aini
ng.
Cov
ers
Ove
rvie
w o
f PA
LS s
cien
ce.
CP
R/A
ED
, Ped
iatri
c A
sses
smen
t Tria
ngle
, M
anag
emen
t of
Res
pira
tory
E
mer
genc
ies,
Rhy
thm
di
stur
banc
es, C
ardi
ac
Arre
st, S
hock
and
R
espi
rato
ry C
ase
sim
ulat
ions
Ski
lls: H
igh
qual
ity C
PR
, S
yste
mat
ic
App
roac
h to
th
e pa
tient
. R
espi
rato
ry
skills
, Rhy
thm
di
stur
banc
es/E
lec
trica
l Th
erap
y,
Vas
cula
r ac
cess
, re
susc
itatio
n co
re
sim
ulat
ions
Fo
cus
is
com
preh
ensi
ve
reco
gniti
on a
nd
man
agem
ent o
f th
e ch
ild w
ith
mor
e em
phas
is
on re
susc
itatio
n an
d le
ss
emph
asis
on
reco
gniti
on a
nd
asse
ssm
ent
than
in y
ears
pa
st. S
trong
ho
spita
l bas
ed
emph
asis
.
Bef
ore
cour
se:
PALS
sel
f as
sess
men
t CD
. P
artic
ipat
ion
in
cour
se. P
ass
skills
ch
ild/in
fant
CP
R
and
AE
D. W
ritte
n ex
am p
ass
of 8
4%.
Pas
s 2
PA
LS c
ore
case
test
s as
team
le
ader
(ped
i cod
es)
AH
A F
acul
ty
Cou
rse
Dire
ctor
, M
D P
ALS
in
stru
ctor
, Lea
d P
ALS
inst
ruct
or,
Oth
er P
ALS
in
stru
ctor
s,
BLS
inst
ruct
or
optio
nal;
Spe
cial
ty
Facu
lty
Inst
ruct
or
Stu
dent
Rat
io
max
1:8
M
ust b
e af
filia
ted
with
A
HA
trai
ning
ce
nter
.
Prog
ram
Ta
rget
A
udie
nce
Leng
th
Cre
ated
by
Pu
rpos
e Sk
ills
Test
ed
Com
plet
ion
Req
uire
men
ts
Inst
ruct
or
Req
uire
men
ts
This
com
paris
on w
as c
ompi
led
afte
r rev
iew
of e
ach
cour
ses c
onte
nt a
nd w
eb si
te in
form
atio
n as
of M
arch
200
8
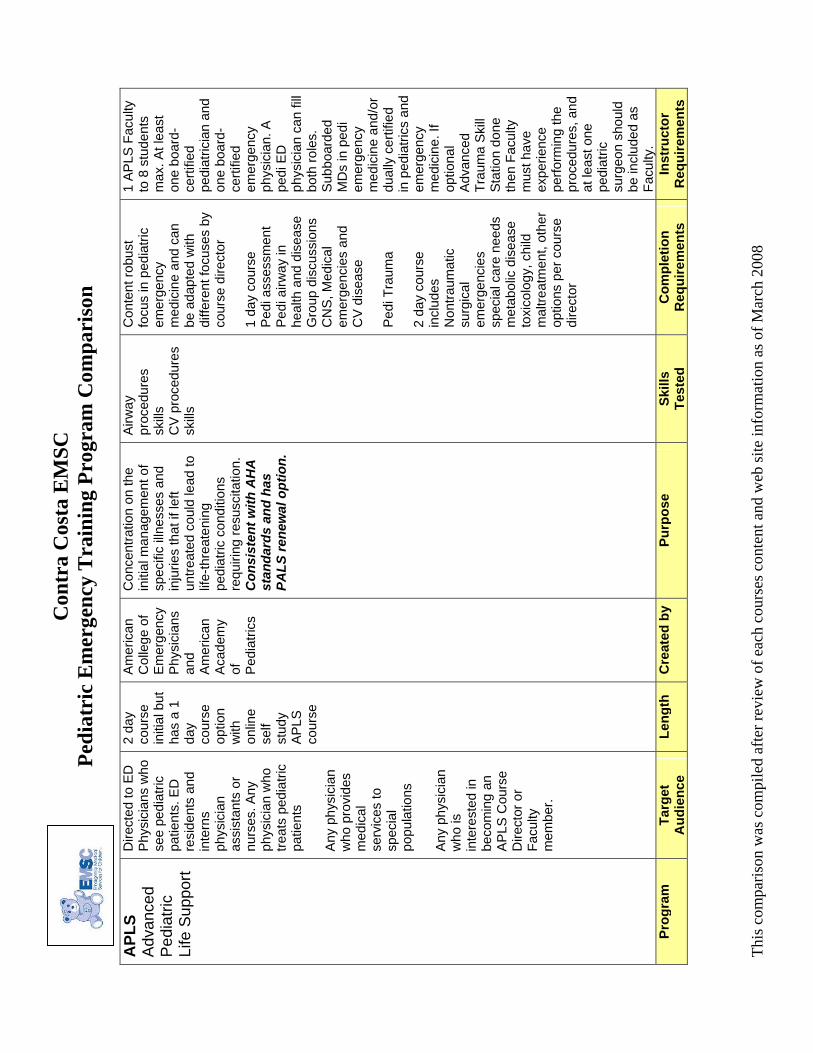
Con
tra
Cos
ta E
MSC
Pe
diat
ric
Em
erge
ncy
Tra
inin
g Pr
ogra
m C
ompa
riso
n
APL
S A
dvan
ced
Ped
iatri
c Li
fe S
uppo
rt
Dire
cted
to E
D
Phy
sici
ans
who
se
e pe
diat
ric
patie
nts.
ED
re
side
nts
and
inte
rns
phys
icia
n as
sist
ants
or
nurs
es. A
ny
phys
icia
n w
ho
treat
s pe
diat
ric
patie
nts
Any
phys
icia
n w
ho p
rovi
des
med
ical
se
rvic
es to
sp
ecia
l po
pula
tions
Any
phys
icia
n w
ho is
in
tere
sted
in
beco
min
g an
A
PLS
Cou
rse
Dire
ctor
or
Facu
lty
mem
ber.
2 da
y co
urse
in
itial
but
ha
s a
1 da
y co
urse
op
tion
with
on
line
self
stud
y AP
LS
cour
se
Am
eric
an
Col
lege
of
Em
erge
ncy
Phy
sici
ans
and
Am
eric
an
Aca
dem
y of
P
edia
trics
Con
cent
ratio
n on
the
initi
al m
anag
emen
t of
spec
ific
illne
sses
and
in
jurie
s th
at if
left
untre
ated
cou
ld le
ad to
lif
e-th
reat
enin
g pe
diat
ric c
ondi
tions
re
quiri
ng re
susc
itatio
n.
Con
sist
ent w
ith A
HA
st
anda
rds
and
has
PALS
rene
wal
opt
ion.
Airw
ay
proc
edur
es
skills
C
V p
roce
dure
s sk
ills
Con
tent
robu
st
focu
s in
ped
iatri
c em
erge
ncy
med
icin
e an
d ca
n be
ada
pted
with
di
ffere
nt fo
cuse
s by
co
urse
dire
ctor
1
day
cour
se
Ped
i ass
essm
ent
Ped
i airw
ay in
he
alth
and
dis
ease
G
roup
dis
cuss
ions
C
NS
, Med
ical
em
erge
ncie
s an
d C
V d
isea
se
Ped
i Tra
uma
2 da
y co
urse
in
clud
es
Non
traum
atic
su
rgic
al
emer
genc
ies
spec
ial c
are
need
s
met
abol
ic d
isea
se
toxi
colo
gy, c
hild
m
altre
atm
ent,
othe
r op
tions
per
cou
rse
dire
ctor
1 AP
LS F
acul
ty
to 8
stu
dent
s m
ax. A
t lea
st
one
boar
d-ce
rtifie
d pe
diat
ricia
n an
d on
e bo
ard-
certi
fied
emer
genc
y ph
ysic
ian.
A
pedi
ED
ph
ysic
ian
can
fill
both
role
s.
Sub
boar
ded
MD
s in
ped
i em
erge
ncy
med
icin
e an
d/or
du
ally
cer
tifie
d in
ped
iatri
cs a
nd
emer
genc
y m
edic
ine.
If
optio
nal
Adv
ance
d Tr
aum
a S
kill
Sta
tion
done
th
en F
acul
ty
mus
t hav
e ex
perie
nce
perfo
rmin
g th
e pr
oced
ures
, and
at
leas
t one
pe
diat
ric
surg
eon
shou
ld
be in
clud
ed a
s Fa
culty
. Pr
ogra
m
Targ
et
Aud
ienc
e Le
ngth
C
reat
ed b
y
Purp
ose
Skill
s Te
sted
C
ompl
etio
n R
equi
rem
ents
In
stru
ctor
R
equi
rem
ents
This
com
paris
on w
as c
ompi
led
afte
r rev
iew
of e
ach
cour
ses c
onte
nt a
nd w
eb si
te in
form
atio
n as
of M
arch
200
8
