employment of the combat support · pdf filefm 8-10-14 employment of the combat support...
TRANSCRIPT

FM 8-10-14
EMPLOYMENT OF THE COMBAT SUPPORT
HOSPITAL ____________________________________________
TACTICS, TECHNIQUES, AND PROCEDURES
HEADQUARTERS, DEPARTMENT OF THE ARMY
DISTRIBUTION RESTRICTION: Approved for public release; distribution is unlimited.
Manual Provided by eMilitary Manuals - http://www.emilitarymanuals.com

Manual Provided by eMilitary Manuals - http://www.emilitarymanuals.com

Manual Provided by eMilitary Manuals - http://www.emilitarymanuals.com
Manual Provided by eMilitary Manuals - http://www.emilitarymanuals.com

Manual Provided by eMilitary Manuals - http://www.emilitarymanuals.com

Manual Provided by eMilitary Manuals - http://www.emilitarymanuals.com

FM 8-10-14
CHAPTER 1
HOSPITALIZATION SYSTEM IN A THEATER OF OPERATIONS
1-1. Combat Health Support in a Theaterof Operations
a. A theater of operations (TO) is thatportion of an area of war necessary for militaryoperations and for the administration of suchoperations. The scenario depicts the size of theTO and the US Forces to be deployed. The theateris normally divided into a combat zone (CZ) anda communications zone (COMMZ). In someinstances, the COMMZ may be outside the TOand located in offshore support facilities, ThirdCountry support bases, or in the continentalUnited States (CONUS). The CZ begins at theArmy/corps rear boundary and extends forwardto the extent of the commander’s area ofinfluence. The COMMZ begins at the corps rearboundary and extends rearward to include thearea(s) needed to provide support to the forces inthe CZ.
b. The mission of the AMEDD is toconserve the fighting strength. This mission ofCHS is a continuous and an integrated functionthroughout the TO. It extends from the CZ backthrough the COMMZ and ends in CONUS.Combat health support maximizes the system’sability to maintain presence with the supportedsoldier, return injured, sick, and wounded soldiersto duty, and to clear the battlefield of soldierswho cannot return to duty (RTD). Patients areexamined, treated, and identified as RTD ornonreturn to duty (NRTD) as far forward as ismedically possible. Early identification is per-formed by the treating primary care provider andcontinues in the evacuation chain with constantreassessment. Patients requiring evacuation outof the division who are expected to RTD within
the theater evacuation policy are evacuated to acorps and/or COMMZ hospital. Those patientsclassified as NRTD follow the evacuation chainfor trauma care and stabilization for evacuationout of the theater.
1-2. Echelons of Combat Health Support
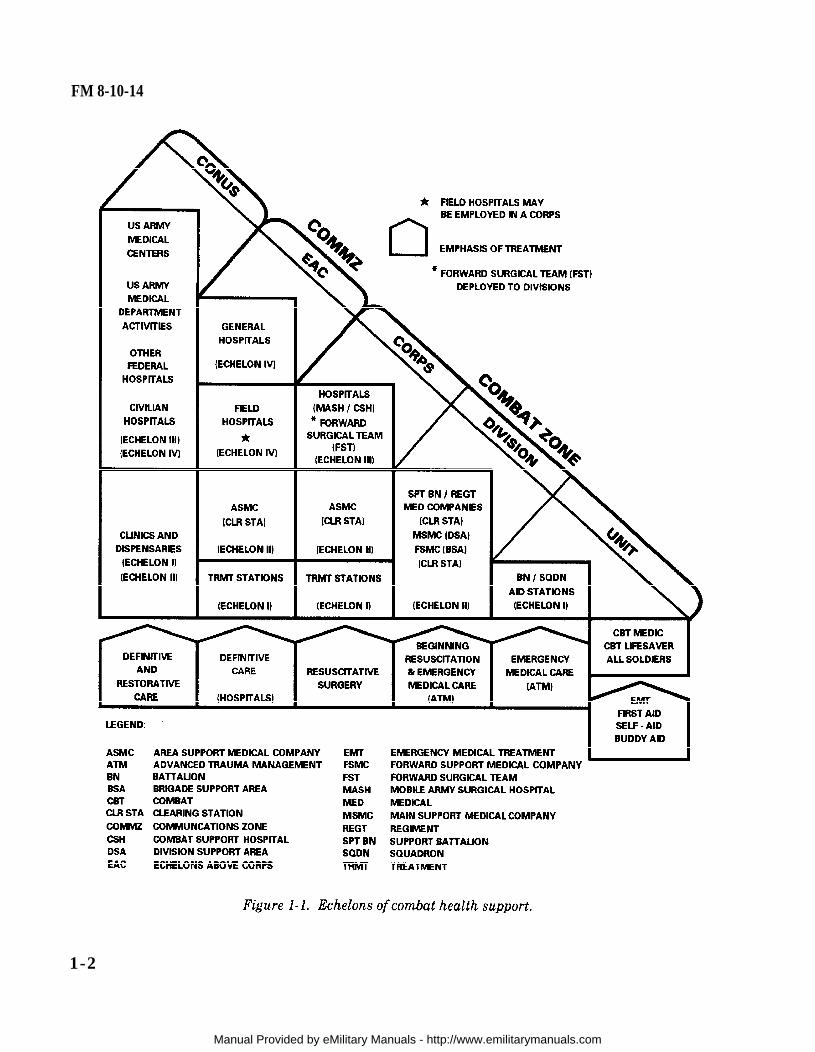
The CHS system within a TO is organized intofour echelons of support which extend rearwardthroughout the theater (see Figure l-l). Thesystem is tailored and phased to enhance patientidentification, evacuation, treatment, and RTD asfar forward as the tactical situation will permit.Hospital resources will be employed on an areabasis to provide the utmost benefit to themaximum number of personnel in the area ofoperations (AO). Each echelon reflects anincrease in capability, with the function of eachlower echelon being contained within thecapabilities of the higher echelon. Wounded, sick,or injured soldiers will normally be treated,returned to duty, and/or evacuated to CONUS(Echelon V) through these four echelons:
a. Echelon 1. This echelon is alsoknown as unit level. Care is provided by desig-nated individuals or elements organic to combatand combat support (CS) units and elements ofthe area support medical battalion (ASMB).Major emphasis is placed on those measuresnecessary to stabilize the patient (maintainairway, stop bleeding, prevent shock) and allowfor evacuation to the next echelon of care.
(1) Combat medic. This is the firstindividual in the CHS chain who makes medically
1-1
Manual Provided by eMilitary Manuals - http://www.emilitarymanuals.com
FM 8-10-14
1-2
Manual Provided by eMilitary Manuals - http://www.emilitarymanuals.com

FM 8-10-14
substantiated decisions based on medical militaryoccupational specialty (MOS)-specific training.The combat medic is supported by first-aidproviders in the form of self-aid and buddy aidand the combat lifesaver.
(a) Self-aid and buddy aid.The individual soldier is trained to be proficientin a variety of specific first-aid procedures withparticular emphasis on lifesaving tasks. Thistraining enables the soldier, or a buddy, to applyimmediate care to alleviate a life-threateningsituation.
(b) Combat lifesaver. En-hanced medical training is provided to selectedindividuals who are called combat lifesavers.These individuals are nonmedical unit membersselected by their commander for additionaltraining to be proficient in a variety of first-aidprocedures. A minimum of one individual persquad, crew, team, or equivalent-sized unit istrained. All combat units and some CS andcombat service support (CSS) units have combatlifesavers. The primary duty of these individualsdoes not change. The additional duties of combatlifesavers are performed when the tacticalsituation permits. These individuals provideenhanced first-aid care for injuries prior totreatment by the combat medic. The training isnormally provided by medical personnel assignedor attached to the unit. The training program ismanaged by a senior medical person designatedby the commander.
(2) Treatment squad. The treat-ment squad consists of a field surgeon, aphysician assistant (PA), two noncommissionedofficers (NCOs), and four medical specialists.The personnel are trained and equipped toprovide advanced trauma management (ATM)to the battlefield casualty. Advanced traumamanagement is emergency care designed toresuscitate and stabilize the patient for
evacuation to the next echelon of care. Eachsquad can split into two trauma treatment teams.These squads are organic to medical platoons/sections in maneuver battalions and designatedCS units and medical companies of separatebrigades, divisions, and echelons above divisionin the ASMB. Treatment squads (treatmentteams) may be employed anywhere on thebattlefield. When not engaged in ATM, theseelements provide routine sick call services on anarea basis. Echelon I care for units not havingorganic Echelon I capability is provided on anarea basis by the organization responsible in thesector.
b. Echelon II. This echelon may alsobe known as division level. Care at this echelonis rendered at the clearing station (division orcorps). Here the casualty is examined and hiswounds and general status are evaluated todetermine his treatment and evacuationprecedences, as a single casualty among othercasualties. Those patients who can RTD within 1to 3 days are held for treatment. Emergencymedical treatment (EMT) (including beginningresuscitation) is continued and, if necessary,additional emergency measures are instituted;but they do not go beyond the measures dictatedby the immediate necessities. The divisionclearing station has blood replacement capability,limited x-ray and ambulatory services, patientholding capability, and emergency dental care.Clearing stations provide Echelon I CHSfunctions on an area basis to those units withoutorganic medical elements. Echelon II CHS alsoincludes preventive medicine (PVNTMED)activities and combat stress control (CSC). Thesefunctions are performed typically by company-sized medical units organic to brigades, divisions,and ASMBs.
c. Echelon III. The first hospitalfacilities are located at this echelon. Within theCZ, the mobile army surgical hospital (MASH)and the CSH are staffed and equipped to provide
1-3
Manual Provided by eMilitary Manuals - http://www.emilitarymanuals.com
FM 8-10-14
resuscitation, initial wound surgery, and post-operative treatment. Although the MASH isan Echelon III facility, it is designed to beemployed within the division area. At the CSH,patients are stabilized for continued evacuation,or returned to duty. Those patients who areexpected to RTD within the theater evacuationpolicy are regulated to a facility that has thecapability for reconditioning and rehabilitating.
d. Echelon IV. At this echelon, thepatient may be treated at the general hospital(GH) or the field hospital (FH). The GHs arestaffed and equipped for general and specializedmedical and surgical care. Those patients notexpected to RTD within the theater evacuationpolicy are stabilized and evacuated to CONUS.At the FH, reconditioning and rehabilitatingservices are provided for those patients who willbe RTD within the theater evacuation policy.
e. Echelon V. This echelon of care isprovided in CONUS. Hospitalization is providedby DOD hospitals (military hospitals of thetriservices) and Department of Veterans Affairs(DVA) hospitals. Under the National DisasterMedical System, patients overflowing DOD andDVA hospitals will be cared for in designatedcivilian hospitals.
1-3. Theater Hospital System
a. Medical Force 2000 is the modern-ization effort to restructure the CHS systemincluding hospitalization in support of a TO. Thissystem consists of four hospitals, a medicalcompany, holding, and six medical/surgical teams.The two corps hospitals are the MASH and theCSH. The two COMMZ hospitals are the FH andthe GH. In addition to these hospitals, themedical company, holding, provides a 1,200-cotconvalescent capability. For a detailed discussion
on the Medical Force 2000 hospital system, referto FM 8-10.
(1) Mobile army surgical hospital.This hospital is a 30-bed facility with the primarymission of providing lifesaving surgical andmedical care to stabilize patients for furtherevacuation, either to the CSH or to COMMZhospitals. Patients are held approximately 24 to36 hours until considered stable enough totolerate a bed-to-bed transfer without incurringfurther risk to their condition. The MASH willbe employed in the corps area or forward in thedivision rear area. This hospital is not DeployableMedical Systems (DEPMEDS)-equipped. It is 100percent mobile with organic vehicles.
(2) Forward surgical team. Aforward surgical team (FST) will replace the twosurgical squads in each of the following: theairborne division; the air assault division; and the2d Armored Cavalry Regiment (ACR). The FSTswill also replace the medical detachment(surgical) and the 30-bed MASH. This team willbe a corps augmentation for divisional andnondivisional medical companies. It will provideemergency/urgent initial surgery and nursingcare after surgery for the critically wounded/injured patient until sufficiently stable forevacuation to a theater hospital. The FSTs notorganic to divisions and the 2d ACR will beassigned to a medical brigade or group andnormally attached to a corps hospital when notoperationally employed and further attachedfor support to a divisional/nondivisional medicalcompany.
(3) Combat support hospital. Thishospital is addressed in detail in the followingchapters of this publication.
(4) Field hospital. This hospital isa 504-bed facility with the mission of providinghospitalization for patients and for reconditioningand rehabilitating those patients who can RTD
1-4
Manual Provided by eMilitary Manuals - http://www.emilitarymanuals.com

FM 8-10-14
within the theater evacuation policy. Themajority of patients within this facility will be inthe convalescent care category. The FH isnormally located in the COMMZ, but could beused in the corps rear when geographicaloperational constraints dictate. It is 20 percentmobile with organic vehicles.
(5) General hospital. This organi-zation is a 476-bed facility with the mission ofproviding stabilization and hospitalization forpatients who require either further evacuationout of the TO, or who can RTD within the theaterevacuation policy. The GH will normally belocated in the COMMZ. Its mobility is 10 percentwith organic vehicles.
(6) Medical company, holding.This unit provides reconditioning and rehabili-tation for up to 1,200 convalescent care patients.This unit may be located in the corps or COMMZ.It is used to augment the CSH when operationalnecessity dictates. It may also be used in the
3-week CSC reconditioning program. This unitis staffed and equipped to provide care forminimal category (self-care) patients.
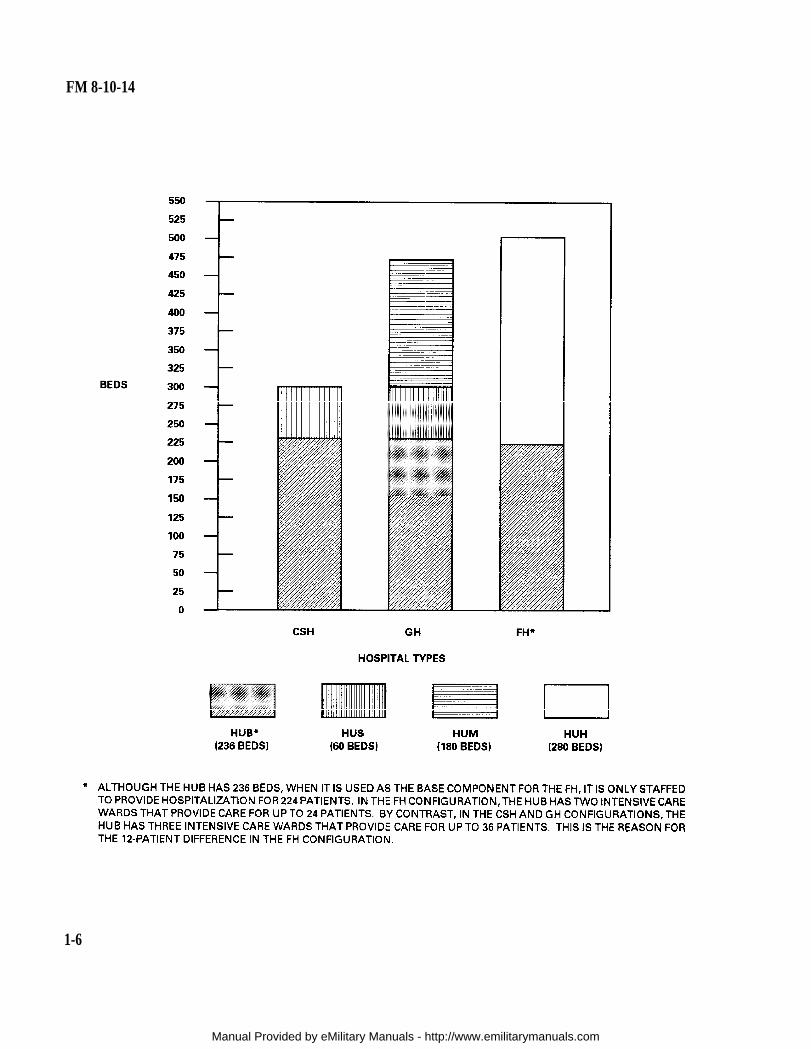
b. The CSH, FH, and GH are designedusing the following four modules:
(1) Hospital unit, base (HUB).
(2) Hospital unit, surgical (HUS).
(3) Hospital unit, medical (HUM).
(4) Hospital unit, holding (HUH).
They are configured using the appropriate com-bination of these modules. The HUB can operateindependently, is clinically similar, and is locatedin each hospital as the initial building block. Theother three mission-adaptive modules (HUS,HUM, and HUH) are dependent upon the HUB(see Figure 1-2, page 1-6.
1-5
Manual Provided by eMilitary Manuals - http://www.emilitarymanuals.com
FM 8-10-14
1-6
Manual Provided by eMilitary Manuals - http://www.emilitarymanuals.com
FM 8-10-14
CHAPTER 2
THE COMBAT SUPPORT HOSPITAL
2-1. Mission and Allocation
The mission of this hospital is to provideresuscitation, initial wound surgery, post-operative treatment, and RTD those soldiers inthe CZ who fall within the corps evacuationpolicy, or to stabilize patients for further evacua-tion. This hospital is capable of handling all typesof patients. It has a basis of allocation of 2.4hospitals per division.
2-2. Assignment and Capabilities
a. The CSH is assigned to the Head-quarters and Headquarters Company (HHC),Medical Brigade, TOE 08-422L100. The hospitalmay be further attached to the Headquartersand Headquarters Detachment (HHD), MedicalGroup, TOE 08-432L000.
b. This unit provides hospitalizationfor up to 296 patients. The hospital has eightwards providing intensive nursing care for up to96 patients, seven wards providing intermediatenursing care for up to 140 patients, one wardproviding neuropsychiatric (NP) care for up to 20patients, and two wards providing minimalnursing care for up to 40 patients.
c. Surgical capacity is based on eightoperating room (OR) tables for a surgical capacityof 144 OR table hours per day.
•
d. Other capabilities include—
• Consultation services forpatients referred from other medical treatmentfacilities (MTFs).
• Unit-level CHS for organicpersonnel only.
• Pharmacy, clinical laboratory,blood banking, radiology, physical therapy, andnutrition care services.
• Medical administrative andlogistical services to support work loads.
• Dental treatment to staff andpatients and oral and maxillofacial surgery sup-port for military personnel in the immediate areaplus patients referred by the area CHS units.
2-3. Hospital Support Requirements
In deployment and sustainment of operations,this unit is dependent upon appropriate elementsof the corps for—
• Personnel
• Finance.
administrative services.
• Mortuary affairs and legal services.
• Transportation services (unit is 35percent mobile with organic assets).
• Laundry services for other thanpatient-related linen.
Security and enemy prisoner of war(EPW) security during processing and evacu-ation.
• Transportation for discharged pa-tients.
• Class I supplies (rations) to includethe Medical B Rations required for patient feed-ing.
• Engineer supporttion, waste disposal, and minor
for site prepara-construction.
2-1
Manual Provided by eMilitary Manuals - http://www.emilitarymanuals.com

FM 8-10-14
• Veterinary support for zoonoticdisease control and investigation; inspection ofmedical and nonmedical rations, to includesuspected contaminated rations and dispositionrecommendations; and animal bites.
• PVNTMED support for food facilityinspection, vector control, and control of medicaland nonmedical waste.
2-4. Hospital Organization and Func-tions
The CSH is a modular-designed facility whichconsists of a HUB and HUS. It can be furtheraugmented with specialty surgical/medical teamsto increase its capabilities. It may become adesignated specialty center as the work load ormission dictates (Figure 2-1).
2-2
Manual Provided by eMilitary Manuals - http://www.emilitarymanuals.com

FM 8-10-14
a. The HUB is a 236-bed facility whichhas 36 intensive, 140 intermediate, 40 minimal,and 20 NP care beds. It has two OR modules, onesurgical and the other orthopedic, which arestaffed to provide a total of 72 OR table hours perday. It also allows for attachment of specialtysurgical teams. The HUB is an independentorganization which includes all hospital services(Figure 2-2).
b. The HUS is comprised of 60 intensivecare beds, two OR modules, one x-ray module,one triage/preoperative/EMT module, and theappropriate staffs (Figure 2-3, page 2-5). TheHUS is dependent on the HUB for food service,maintenance, and administration.
c. When the HUB and HUS are em-ployed to form a single hospital, half of the ORtables are staffed for two 12-hour shifts with theother half only staffed for one 12-hour shift perday.
2-5. The Hospital Unit, Base
The HUB provides a solid infrastructure for theCSH operations. The HUB contains the followingsections:
a. Hospital Headquarters Section.This section provides internal command andcontrol (C2) and management of all hospitalservices. Personnel of this section supervise andcoordinate the surgical, nursing, medical,pastoral, and administrative services. Stafflngincludes the HUB commander, the chiefs ofsurgery, nursing, and medicine, an executiveofficer (XO), a chaplain, a command sergeantmajor (CSM), and an administrative specialist(Table 2-1). When the HUB and the HUS jointo function as a CSH, the HUB commander isthe CSH commander unless otherwise desig-nated.
(1) Hospital commander (60A00).Command and control is the process throughwhich the activities of the hospital are directed,coordinated, and controlled to accomplish themission. This process begins and ends with thecommander. An effective commander must havea thorough knowledge and understanding ofplanning and implementing CHS (FM 8-55). Heis decisive and provides specific guidance to hisstaff in the execution of the mission. The success-ful commander delegates authority and fostersan organizational climate of mutual trust, co-operation, and teamwork. He has the overallresponsibility for coordination of CHS within thehospital’s AO. Additionally, he is responsible forthe structural layout of the hospital.
(2) Chief, surgical service (61J00).The chief surgeon is the principal advisor to thehospital commander for surgical activities. Heprovides supervision and control over the surgi-cal services to include the ORs. He prescribescourses of treatment and surgery for patientshaving injuries or disorders with surgical condi-tions and participates in surgical procedures asrequired. He coordinates and is responsible forall matters pertaining to the evaluation, manage-ment, and disposition of patients received by thesection. He is responsible for the evaluation andtraining programs for his professional staff. Healso functions as the Deputy Commander forProfessional Services.
2-3
Manual Provided by eMilitary Manuals - http://www.emilitarymanuals.com

FM 8-10-14
2-4
Manual Provided by eMilitary Manuals - http://www.emilitarymanuals.com

FM 8-10-14
(3) Chief nurse (66A00). The chiefnurse is the principal advisor to the hospitalcommander for nursing activities. This officerplans, organizes, supervises, and directs nursingcare practices and activities of the hospital. Thisofficer is also responsible for the orientation andprofessional development programs for thenursing staff.
(4) Chief, medicine services(61F00). This officer is responsible for the exami-nation, diagnoses, and treatment, or recom-mended course of management for patients with
medical illnesses. He controls the length of patientstay through continuous patient evaluation, earlydetermination of disposition, or evacuation to thenext echelon of care.
(5) Executive officer (67A00). Thehospital XO advises the commander on matterspertaining to health care delivery. He plans,directs, and coordinates administrative activitiesfor the hospital. He provides guidance to thetactical operations center (TOC) staff in planningfor future operations. He also functions as theChief, Administrative Service.
2-5
Manual Provided by eMilitary Manuals - http://www.emilitarymanuals.com

FM 8-10-14
(6) Hospital chaplain (56A00).The chaplain functions as the staff officer for allmatters in which religion impacts on commandprograms, personnel, policy, and procedures. Heprovides for the spiritual well-being and moraleof patients and hospital personnel. He also pro-vides religious services and pastoral counselingto soldiers in the AO.
(7) Command sergeant major(00Z50). The CSM is the principal enlistedrepresentative to the commander. He advises thecommander and staff on all matters pertaining towelfare and morale of enlisted personnel in termsof assignment, reassignment, promotion, anddiscipline. He provides counsel and guidance toNCOs and other enlisted personnel of thehospital. He is also responsible for the receptionof newly assigned enlisted personnel into theunit. The CSM evaluates the implementation ofindividual soldier training on common soldiertasks and supervises the hospital’s NCO pro-fessional development.
(8) Administrative specialist(71L20). The administrative specialist performstyping, clerical, and administrative duties for thehospital headquarters. He proofreads corre-spondence for proper spelling, grammar, punc-tuation, format, and content accuracy. Heestablishes and maintains files, logs, and otherstatistical information for the command. He isthe light-vehicle driver and radio operator for thecommand section.
b. Hospital Operations Section. Thissection is responsible for communications (in-ternal and external), security, plans and opera-tions, deployment, and relocation of the hospital.The staff is composed of a medical operationsofficer, a field medical assistant, an operationsNCO, a nuclear, biological, and chemical (NBC)NCO, an administrative specialist, and appro-priate communications personnel (Table 2-2).The authorization for the field medical assistantis counted in the HUS.
(1) Medical operations officer(70H67). This officer is responsible to the XO forthe Intelligence Officer/Operations and TrainingOfficer (S2/S3) functions of the hospital. Hesupervises all tactical operations conducted bythe hospital to include planning and relocation.He is responsible for the formulation of the tacti-cal standing operating procedures (TSOP) andhospital planning factors (refer to Appendix A foran example of a TSOP format and Appendix B foran estimate of hospital planning factors).
(2) Field Medical Assistant(70B67). This officer is responsible to the medicaloperations officer for planning and coordinatingsite selection and convoy operations duringhospital deployment and relocation. He alsofunctions as the operations security (OPSEC) andcommunications security (COMSEC) officer forthe hospital. The requirement for this position iscounted in the unit headquarters section (HUS).When the HUB and HUS form a CSH, the fieldmedical assistant, HUS becomes the field medicalassistant in this section.
2-6
Manual Provided by eMilitary Manuals - http://www.emilitarymanuals.com
FM 8-10-14
(3) Operations sergeant (91B40).The operations sergeant is responsible to themedical operations officer for physical security,to include the hospital defense plan; preparationof unit plans, operation orders (OPORDs) andmap overlays; and intelligence information andrecords. He also supervises subordinate staff.
(4) Section chief (31U40). ThisNCO serves as the principal signal advisor to thehospital commander and medical operations offi-cer on all communications matters. He is respon-sible to the medical operation and plans officersfor the planning, supervising, coordinating, andtechnical assistance in the installation, operation,management, and operator-level maintenance ofradio, field wire, and switchboard communica-tions systems. He supervises all subordinatecommunications personnel.
(5) Nuclear, biological, and chem-ical noncommissioned officer (54B40). This NCOis the technical advisor to the hospital command-er and medical operations officer on matters per-taining to NBC operations. He is responsible tothe medical operations officer for the planning,training, NBC decontamination (less patient),and other aspects of hospital NBC defensive op-erations.
(6) Electronic switch systems op-erator (31F20). This operator is responsible tothe section chief for the installation, operation,and operator-level maintenance of switchboardsand switching systems.
(7) Electronic switch systems op-erator (31FI0). These operators are responsibleto the section chief for the installation, opera-tion, and unit-level maintenance on switchboards,switching assemblages, and associated communi-cations equipment.
(8) Signal information service spe-cialist (31UIO). This individual is responsible to
the section chief for installation and operation ofunit wire systems, associated equipment, andfrequency modulated (FM) radios.
(9) Administrative specialist (7L10).This individual is responsible to the operationssergeant for general typing and administrativefunctions for the section.
(10) Signal support systems special-ist (31UI0). This individual is responsible to thesection chief for installing wire for field tele-phones and assisting in the operation of the hos-pital FM radios.
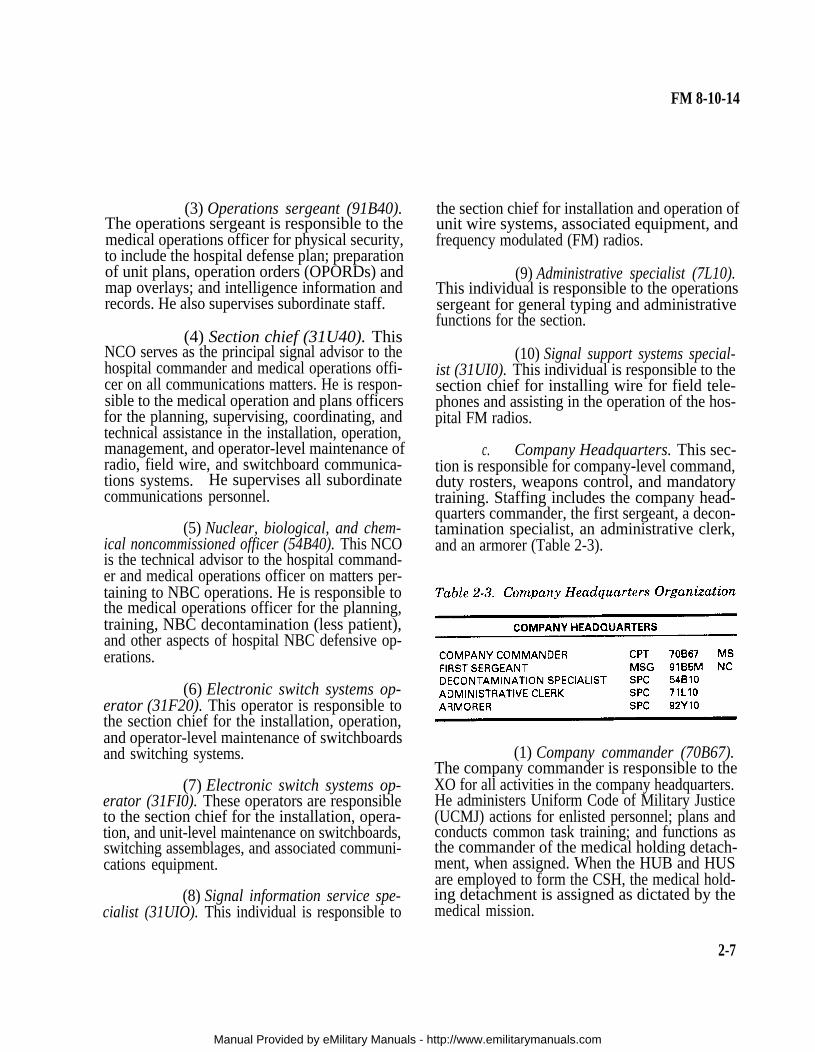
c. Company Headquarters. This sec-tion is responsible for company-level command,duty rosters, weapons control, and mandatorytraining. Staffing includes the company head-quarters commander, the first sergeant, a decon-tamination specialist, an administrative clerk,and an armorer (Table 2-3).
(1) Company commander (70B67).The company commander is responsible to theXO for all activities in the company headquarters.He administers Uniform Code of Military Justice(UCMJ) actions for enlisted personnel; plans andconducts common task training; and functions asthe commander of the medical holding detach-ment, when assigned. When the HUB and HUSare employed to form the CSH, the medical hold-ing detachment is assigned as dictated by themedical mission.
2-7
Manual Provided by eMilitary Manuals - http://www.emilitarymanuals.com

FM 8-10-14
(2) First sergeant (91B5M). Thefirst sergeant is responsible to the company com-mander for enlisted matters. He also assists insupervising company administration and trainingactivities. He provides guidance to the enlistedmembers of the company and represents them tothe company commander. He also functions asthe reenlistment NCO.
(3) Decontamination specialist(54B10). This specialist is responsible to the firstsergeant for training the company’s NBC teamson the operation of NBC detection and decontami-nation equipment and for the operator main-tenance on this equipment. He assists the NBCNCO in the establishment, administration, train-ing, and application of NBC defense measures.He also performs NBC reconnaissance and isdesignated as a light-vehicle operator.
(4) Administrative clerk (71LI0).The clerk-typist is responsible to the firstsergeant for providing the personnel and unitadministration support for the company head-quarters. His duties consist of general admin-istration and personnel actions.
(5) Armorer (92YI0). The armor-er’s primary duty is that of maintaining the wea-pons storage area, small arms, and ammunitionand performing small arms unit maintenance.He is designated as the light-vehicle operator forthe section.
d. Administrative Division. This divi-sion provides overall administrative services forthe hospital to include personnel administration,mail distribution, awards and decorations, leaves,and typing support. The staff is composed of thehospital adjutant, personnel sergeant, personneladministrative sergeant, an administrative spe-cialist, mail delivery clerks, and an administra-tive clerk (Table 2-4). This section coordinates withelements of corps support command (COSCOM)for finance, personnel, and administrative services.
(1) Hospital adjutant (70F67).This officer is responsible to the hospital XO forthe adjutant functions within the hospital. Healso advises the commander and staff in the areaof personnel management for patients and staff.
(2) Personnel sergeant (75240).The personnel sergeant is responsible to theadjutant for specific personnel functions whichinclude personnel management, records, actions,and preparation of Standard Installation/DivisionPersonnel System (SIDPERS) changes. He en-sures coordination between the medical brigadeand/or medical group Personnel and Adminis-tration Center (PAC) and the hospital. Headvises the hospital commander, adjutant, andother staff members on personnel administrativematters. He also supervises the activities ofsubordinate personnel.
(3) Personnel administrative ser-geant (75B20). This individual is responsible tothe personnel sergeant for personnel and admin-istrative functions for the hospital.
(4) Administrative specialists(71L10). These specialists are responsible to thepersonnel sergeant for general typing and admin-istrative functions for the division.
(5) Mail delivery clerks (71L10).These administrative specialists are responsible
2-8
Manual Provided by eMilitary Manuals - http://www.emilitarymanuals.com