enabling echnologiest - emerald insight
TRANSCRIPT

Access this journal onlinewww.emeraldinsight.com/loi/jet Volume 11 Number 3 2017
ISSN 2398-6263
Journal of
Enabling TechnologiesUser inclusion in health, support, social care and education
Volume 11 Number 3 2017
Contents
Journal of
Enabling Technologies User inclusion in health, support, social care and education
Number 3 73 Editorial
75 Researching telecare: the importance of contextKate Hamblin, Sue Yeandle and Gary Fry
85 A technology-aided program for helping persons with Alzheimer’s disease perform daily activitiesGiulio Lancioni, Nirbhay Singh, Mark O’Reilly, Jeff Sigafoos, Fiora D’Amico, Katia Pinto, Floriana De Vanna and Alessandro Caffò
92 Graphic symbols terminology: a call for a consensusEliada Pampoulou
101 Augmentative and alternative communication (AAC) training provision for professionals in EnglandSamantha Wallis, Steven Bloch and Michael Clarke
113 “A child with autism only has one childhood”: main themes and questions for research from the “Digital Bubbles” seminar seriesSarah Parsons, Nicola Yuill, Mark Brosnan and Judith Good

Certificate Number 1985ISO 14001
ISOQAR certified Management System,awarded to Emerald for adherence to Environmental standard ISO 14001:2004.
EDITORSarah ParsonsThe University of Southampton, UKE-mail [email protected]
DEPUTY EDITORJohn WoolhamKings College London, UKE-mail [email protected]
ASSOCIATE EDITORKevin DoughtyUniversity of York, UK
REVIEWS EDITORCheryl DobbsIndependent Consultant, Australia
ISSN 2398-6263© 2017 Emerald Publishing Limited
EDITORIAL BOARDChris AbbottKing’s College London, UKMaria BurtonSheffield Hallam University, UKDonna CowanChailey Heritage Clinical Services, UK Guy DewsburyThe Florence Nightingale School of Nursing and Midwifery, King’s College London, UK Paul DoyleHereward College, UKFern FauxNational Star College, UKMalcolm J. FiskCoventry University, UKKaren GuldbergUniversity of Birmingham, UKPetri IlmonenFinnish Association of Intellectual and Developmental Disabilities, FinlandWendy Keay-BrightCentre for Applied Research in Inclusive Arts and Design, Cardiff Metropolitan University
Martin KnappPersonal Social Services Research Unit (PSSRU), The London School of Economics, UK Jeremy LinskellNinewells Hospital, NHS Tayside, UK Katerina MavrouUniversity of Cyprus, CyprusKlaus MiesenbergerUniversity of Linz, AustriaMaurice MulvennaUniversity of Ulster, Ireland Nigel NewbuttUniversity of the West of England, UKSarah ParsonsUniversity of Southampton, UK Jeremy PorteusHousing Learning and Improvement Network, UKJane SealeOpen University, UKNick TylerUniversity College London, UK Tracey WilliamsonUniversity of Salford, UKPeter ZentelHeidelberg University Germany
Emerald Publishing LimitedHoward House, Wagon Lane, Bingley BD16 1WA, United KingdomTel +44 (0) 1274 777700; Fax +44 (0) 1274 785201E-mail [email protected] more information about Emerald’s regional offices please go to http://www.emeraldgrouppublishing.com/officesCustomer helpdesk :Tel +44 (0) 1274 785278; Fax +44 (0) 1274 785201E-mail [email protected], subscription and missing claims enquiries:E-mail [email protected] +44 (0) 1274 777700; Fax +44 (0) 1274 785201
Missing issue claims will be fulfilled if claimed within six months of date of despatch. Maximum of one claim per issue.Hard copy print backsets, back volumes and back issues of volumes prior to the current and previous year can be ordered from Periodical Service Company. Tel +1 518 537 4700; E-mail [email protected] For further information go to www.periodicals.com/emerald.htmlReprints and permissions serviceFor reprint and permission options please see the abstract page of the specific article in question on the Emerald web site (www.emeraldinsight.com), and then click on the “Reprints and permissions” link. Or contact: E-mail [email protected] Publisher and Editors cannot be held responsible for errors or any consequences arising from the use of information contained in this journal; the views and opinions expressed do not necessarily reflect those of the Publisher and Editors, neither does the publication of advertisements constitute any endorsement by the Publisher and Editors of the products advertised.No part of this journal may be reproduced, stored in a retrieval system, transmitted in any form or by any means electronic, mechanical, photocopying, recording or otherwise without either the prior written permission of the publisher or a licence permitting restricted copying issued in the UK by The Copyright Licensing Agency and in the USA by The Copyright Clearance Center. Any opinions expressed in the articles are those of the authors. Whilst Emerald makes every effort to ensure the quality and accuracy of its content, Emerald makes no representation implied or otherwise, as to the articles’ suitability and application and disclaims any warranties, express or implied, to their use.Emerald is a trading name of Emerald Publishing LimitedPrinted by CPI Group (UK) Ltd, Croydon, CR0 4YY
Journal of Enabling Technologiesis indexed and abstracted in:American Sociological Association Publishing Options Database,British Nursing IndexCINAHLCPA's AgeInfoCPA's New Literature on Old AgeIllustrataScopusSocial Care Online
Guidelines for authors can be found at:www.emeraldgrouppublishing.com/jet.htm

Sarah Parsons and John Woolham
Context is key
This is an issue of the Journal of Enabling Technologies that strongly illustrates the importanceand complexity of context in research and practice in our field. There are two research papersthat focus on enabling technologies in care contexts for the elderly, and two research papers thatfocus on augmentative and alternative communication (AAC) for professionals, albeit fromdifferent – though complementary – perspectives. The fifth paper is the final short report from theDigital Bubbles seminar series on innovative technologies for autism, in which the authorsconsider the overall context for future research in this area.
First, Hamblin, Yeandle and Fry place a very helpful methodological lens on context by criticallyevaluating their “everyday life analysis” (ELA) grounded within ethnographic principles.Their paper focusses on exploring the very individual and personal circumstances and factorsthat enable or constrain the use of telecare by older people in their homes. This is a paper thatseeks to dig beneath the standardised “outcome measures” to find out what matters most to theusers of technology in their everyday lives – a core area of interest for this journal of course.By using multiple methods with multiple informants, the authors were able to build up richinsights into experiences over time. The methods included an individualised and inclusive“ELA Box”, which enabled elderly participants to write diaries and/or take photographs of dailyexperiences depending on their preferences. It is clear from the findings that technologyimplementation – however well intentioned – can have substantial impacts on the aspects ofidentity fundamental to well-being, especially relating to independence, autonomy and control.
Ensuring that people can maintain independence and autonomy in their daily lives is, of course,vitally important and one of the main overall objectives of enabling technologies. The paper byLancioni and colleagues is a good example of a small-scale, but promising, evaluation of usingtechnology applications for supporting people with Alzheimer’s disease in their own homes.The authors developed a simple approach based on a tablet PC coupled with a Bluetoothearpiece and a talking alarm clock app that provided timed prompts and basic instructions tohelp people initiate and complete practical daily activities, such as preparing coffee and settingthe table. Over a short period of time, all of the eight participants were significantly supported toinitiate and complete many more activities during the day without staff intervention.As the authors note, this was a small sample and more research is needed to understandmore about the acceptability and satisfaction felt by the participants and their families. However,as an initial demonstration of what can be achieved with a simple set-up, this is an interesting andaccessible idea.
While these two papers target the views and experiences of the “end users”, the next two researchpapers come from the other direction of supporting the understanding and training of professionalsin the field of AAC. Pampoulou presents an insightful conceptual analysis of the diversity of thetypes of graphic symbols. The author shows that it is valuable to dig beneath commonly held viewsor assumptions to take a deeper look at how different symbol sets are constructed and, therefore,how they might be specifically beneficial in practice. In other words, symbol sets have differentways of conveying meaning and these different ways are likely to be important for supporting thecommunication needs and preferences of individuals. Being able to share a commonunderstanding and language around graphic symbols across multiple contexts andmulti-disciplinary teams is likely to be important for strengthening research and practice in this area.
Developing the knowledge and understanding of the professionals using AAC is the primaryconcern of the paper by Wallis, Bloch and Clarke. The authors surveyed 98 clinical service
DOI 10.1108/JET-07-2017-0024 VOL. 11 NO. 3 2017, pp. 73-74, © Emerald Publishing Limited, ISSN 2398-6263 j JOURNAL OF ENABLING TECHNOLOGIES j PAGE 73
Editorial

training providers in England to identify the current context for post-qualification AAC training.The findings showed strongly that there tends to be a medical model approach to current trainingthat focuses on the individual’s impairment and activities. There were also limited current trainingopportunities for understanding the wider context of technology use and the factors that mayimpede the uptake of AAC; crucial features of use highlighted by Hamblin and colleagues’ papernoted above. However, many service providers aspired to providing a more social modelapproach that focused on creating an enabling and inclusive environment, rather than targetingindividual impairments. The fact that there was an awareness of the need to prioritise anunderstanding of this wider context in future training provides at least some encouragement thatinclusive strategies are on the radar even if not yet widely implemented in training.
Finally, Parsons, Yuill, Brosnan and Good present the final short report in a series of paperspublished in this journal on the ESRC-funded “Digital Bubbles” seminar series that took placefrom 2014 to 2016. This paper summarises the main themes that emerged from the previous sixseminars and were used as a framework for discussion at the final, seventh seminar. The paperalso presents some ideas for directions for future research in the field, focussing on: ethics andresponsible innovation, learning and pedagogy, technology-enabled social interaction andengagement. It is clear that there is a very strong impetus coming from the autism community forresearch to move well beyond technologically deterministic approaches and narrowly definedoutcome measures. In the wider field of enabling technologies more generally, such conclusionsare well known. However, making the shift in research and practice is challenging and soit is always helpful to have repeated reminders about the value and importance of taking intoaccount the wider context, and critically reflecting on research aims and practices.
PAGE 74 j JOURNAL OF ENABLING TECHNOLOGIES j VOL. 11 NO. 3 2017

Researching telecare: the importanceof context
Kate Hamblin, Sue Yeandle and Gary Fry
Abstract
Purpose – The purpose of this paper is to present a research method which offers insights into the factorswhich affect the optimal use and implementation of telecare, or which may lead to its rejection by older peoplewith support needs – factors pertinent to those involved in the design and delivery of both telecare researchstudies and of services.Design/methodology/approach – The methodology outlined, influenced by Chicago School and Scienceand Technology Studies, emphasises the importance of context when examining social phenomena, such asthe use of technology. The multi-method approach identified key patterns which provide insights into howtelecare was used by a sample of older adults, including information on its suboptimal use and rejection.Findings – The study of telecare use in real-life situations – and the investigation of other complex socialinterventions – requires an approach which fully considers the importance of context in explainingsocial phenomena. The main value of the method and findings lies in the insights offered to designers of largerstudies which seek to generalise results, including telecare randomised control trials, as well as for thoseinvolved in the delivery of telecare services to achieve optimal adoption and use.Originality/value – The study methods described combined ethnographic, longitudinal and qualitativemethodologies and creative research tools in an innovative way to allow exploration of how context affectsthe uptake and use of telecare.
Keywords Interviews, Ethnography, Observations, Science and technology studies, Chicago School,Telecare
Paper type Research paper
Introduction: telecare and the “evidence” debate
In their paper on methodological approaches to evaluating telecare and telehealthinterventions, Davies and Newman (2011) propose a hierarchy of research types, in whichthey rank “case studies and qualitative research” second lowest, and place randomised controltrials (RCTs) just beneath the pinnacle of the systematic review. When the project that is thefocus of this paper began, the research team were often told that there was “no evidence”of the effectiveness or usefulness of telecare. At that time, findings from the largest RCT oftelecare in the UK (the Whole System Demonstrator project[1]) were not available and mostresearch on telecare came from small-scale, qualitative or pilot studies, some undertaken bytelecare providers. Such research was not considered rigorous enough to draw conclusions,and calls for more “robust” evidence persisted (ADASS, 2014).
It has been argued, however, that the lack of “evidence” about the effectiveness of telecare is amatter of disciplinary politics in a multidisciplinary field characterised by “territorial disputes aboutwhose knowledge is authoritative” (Williams et al., 2003, p. 52). Avoiding setting differentapproaches against one another, this paper argues that, while qualitative methods offer analternative, insightful approach in their own right, they also provide essential information, both forthe design of RCTs and other large-scale research, and for those commissioning and deliveringtelecare services. Positivistic research can obscure the complexity and context within which thedevices involved are situated (Greenhalgh and Swinglehurst, 2011); indeed, qualitative interviewswith service users who declined to participate in, or withdrew from, the Whole Systems
Received 25 April 2017Revised 3 July 2017Accepted 9 July 2017
© Kate Hamblin, Sue Yeandle andGary Fry. Published by EmeraldPublishing Limited. This article ispublished under the CreativeCommons Attribution (CC BY 4.0)licence. Anyone may reproduce,distribute, translate and createderivative works of this article( for both commercial &non-commercial purposes),subject to full attribution to theoriginal publication and authors.The full terms of this licence may beseen at http://creativecommons.org/licences/by/4.0/legalcode
The authors thank the TechnologyStrategy Board (TSB), theEconomic and Social ResearchCouncil (ESRC) and the NationalInstitute for Health Research(NIHR) for funding the research(Project No. 2592-25185) onwhich this paper is based, and thewider project consortium for theircontributions. In addition, theauthors thank Dr EmanuelaBianchera, Dr Chrissy Buse andDr Emma-Reetta Koivunen for theircontributions to the researchdesign and fieldwork and ProfessorPete Buckle for his comments onearlier drafts of this paper. Theauthors also offer their thanks tothe research participants for theirgenerosity and insights.
Kate Hamblin is a SeniorResearch Fellow at the OxfordInstitute of Population Ageing,University of Oxford, Oxford, UK.Sue Yeandle is a Professor ofSociology at the CIRCLE,University of Sheffield,Sheffield, UK.Gary Fry is based at the Schoolof Dementia Studies, Universityof Bradford, Bradford, UK.
DOI 10.1108/JET-04-2017-0016 VOL. 11 NO. 3 2017, pp. 75-84, Emerald Publishing Limited, ISSN 2398-6263 j JOURNAL OF ENABLING TECHNOLOGIES j PAGE 75
Demonstrator Sites project found that many complex factors influenced their rejection of telecare(Sanders et al., 2012) – factors which designers of RCTs and of telecare services should considerwhen assessing the impacts of these devices. This paper presents a multi-method approach tothe study of telecare; this could also be applied to the investigation or delivery of other complexsocial interventions where context and social interactions play a role in shaping outcomes.We first outline a methodology utilised by the (Aktive) project, designed to capture thecomplexities of the context within which telecare devices were situated, then we use researchfindings to demonstrate the importance of this context in mediating the adoption and useof telecare.
Telecare research: an alternative approach
It is widely accepted that research methods should be selected on the basis of their suitabilityfor examining a particular phenomenon. In health and social care settings, experimental andquasi-experimental research designs are traditionally seen as the “gold standard”, producingrobust, generalisable findings. However, it has been argued (Morgan-Trimmer and Wood, 2016)that such studies adopt a linear approach and aim to establish relationships between variables,and do not analyse how people’s responses to interventions are mediated by prior experiences,attitudes or by the interplay of different social actors in the situation. This, and the distancebetween the researcher and the data, underpins speculation about why particular outcomesoccurred or an intervention was successful (or not) (Morgan-Trimmer andWood, 2016). When anexperimental or quasi-experimental approach to telecare research is used, the technology tendsto be conceptualised as an objective, predictable phenomenon, ignoring the role of the user andthe context; both affect outcomes and the technology itself (Williams and Edge, 1996).By contrast, the approach adopted in science and technology studies (STS) conceptualisestechnology as a social phenomenon which cannot be studied in isolation from its social context.STS emerged in the 1960s, arguing that technology both shapes (making some things possible,or impossible) and is shaped by (humans can engage with, and can disable/enable its functions)context and interactions (Greenhalgh and Swinglehurst, 2011; Williams and Edge, 1996). STS issituated within the “contextualist paradigm” advocated by the Chicago School sociologists, whoargued that “one cannot understand social life without understanding the arrangements ofparticular social actors in particular social times and places […] Nothing that ever occurs in thesocial world occurs ‘“net of other variables’” (Abbott, 1997, p. 1152). The STS approach to datacollection is flexible, responsive, iterative and does not provide a “snapshot” of one point in time.It can also help explain why expected and actual outcomes are not aligned (Greenhalgh andSwinglehurst, 2011). This contextualist approach cannot identify the importance of specific“crucial variables”, but can reveal patterns of action likely to occur in similar contexts.The identification of these patterns, through the examination of the context within which acomplex intervention such as telecare is situated, is, we will argue, an important stage in thedesign of any research, including RCTs, and can assist those designing and delivering services[2]to ensure they are provided in a way that promotes optimal usage and outcomes.
The on-going search for an appropriate methodology for the study of how older people(and others) use telecare needs also to recognise that, as an intervention, telecare has many of thefeatures of the “complex social programmes” described in discussions of evidence-basedpolicymaking: it involves a “long implementation chain”, with many and varied stakeholders and endusers; it is embedded in complex and divergent social systems; it is “implemented amid theturbulence of other interventions”; and it is introduced and overseen by practitioners who“work constantly to improve the delivery of interventions”, disrupting uniformity of implementation inthe process (Pawson et al., 2011, p. 519). The range of actors likely to interact with telecare is large,and telecare systems are both extremely complex and continuously in flux at the macro level(in England, for example, local authority telecare services are typically recommissioned every fewyears) and at the micro level (individual telecare users’ needs are likely to be reassessed annually,or when an individual’s circumstances change) (Yeandle et al., 2014; Buckle, 2014). Furthermore,“telecare” is not a single product, but an array of equipment which has emerged across different“generations” of product development (Scottish Government, 2008). Even if a single device(e.g. a personal “pendant alarm”, of the type worn continuously on the body, requiring the user to
PAGE 76 j JOURNAL OF ENABLING TECHNOLOGIES j VOL. 11 NO. 3 2017

press a button to send an alert and linked to a remote monitoring centre) is isolated to evaluate itseffects, in reality the device is likely to be delivered to users in many, and variable, ways by a varietyof providers, including (often) a mix of third sector, private and local authority organisations indifferent localities, in a variety of combinations with other services (De Leonibus et al., 2013). Supplyand charging policies vary, too; in some areas local authorities provide a telecare service as a freeservice, while others levy fees (e.g. both examples were seen in AKTIVE). Telecare users’ lives arealso complex, “messy” and in flux, and research needs to reflect and capture this complexity, ratherthan impose artificial “order”, and seek to draw conclusions applicable to wider contexts.
The perspectives of STS and the Chicago School suggest that the methods used to exploretelecare as a subset of technology need to be capable of exploring the contexts and socialinteractions in which it is embedded (Greenhalgh and Swinglehurst, 2011). This paper describesa methodology developed to explore these contextual factors, which shape users’ experiencesand have the potential to “disrupt” the performance of telecare interventions. This complexity,the study revealed, has implications for health and social care professionals working with telecare(Sanders et al., 2012); for researchers planning experimental or quasi-experimental studies oftelecare (whose protocols should take account of this), and for commissioners, manufacturersand suppliers, who need an understanding of the real world context in which telecare is providedto assess the advantages and disadvantages of introducing it.
Everyday life analysis (ELA): bringing the social context back in
The aim of the AKTIVE was to develop new knowledge relating to the use of telecare and to thebarriers affecting its uptake and successful use[3]. The research design included a literaturesearch (AKTIVE Consortium 2013) and preliminary interviews (Yeandle et al., 2014), whichshowed that different stakeholders (policy-makers, telecare commissioners, academics, careworkers and unpaid carers) had varied perspectives on the purpose of telecare. Taking accountof this, the research team sought to include the views of both older telecare users and thoseinvolved in their care (e.g. care workers or carers) in the central element of the study, its ELA visitsto the homes of older people who had been supplied with telecare equipment as research withinthe contextualist paradigm suggests that the perspectives of users, and those involved in theircare, may be critical to understanding barriers to telecare adoption and use and the next sectionoutlines our method and approach.
Our fieldwork targeted people aged 65+who had been assessed as “susceptible to falls”, or hada diagnosis (or were displaying some symptoms) of cognitive impairment, or both. Our datacollection strategy involved visiting each participant four to six times over a period of six to ninemonths, typically with about four to six weeks between visits. Recruitment was arranged inpartnership with two English local authorities[4]. The research design enabled any familymembers, friends, neighbours, carers or care workers providing support to be included (with theolder person’s consent), providing additional contextual information. The final sample comprised60 participants who remained in the study long enough for longitudinal analysis; 16 were in boththe “falls” and “cognitive impairment” categories; 35 were in the former only; and nine were inthe latter only.
By taking important contextual information into account, critical observations can provide insightinto causal chains (Scriven, 2008); further, ethnographic studies often require researchers toembed themselves in the field for an extended period to observe interactions (Morley andSilverstone, 1991). Based on established methodological guidance (Silverstone et al., 1991),tools were developed for the specificity of the research context, and key ethnographicprinciples – observing and noting “routine” behaviour in “natural settings” and drawing inferences(Lull, 1987) – were adopted. The approach involved a carefully applied ethical framework designedto avoid intrusiveness or upsetting the older people studied, many of whomwere aged 85 or older,and living alone. Ethnography has become an established methodology within telecareresearch (cf. Greenhalgh and Swinglehurst, 2011; Mair et al., 2008: Pols and Willems, 2011;Milligan et al., 2011). The study team’s ELA visits varied in length (averaging about an hour) andwere used to observe participants in various settings in and around their homes and local areas,as they negotiated their surroundings and engaged in everyday activities (such as making tea or
VOL. 11 NO. 3 2017 j JOURNAL OF ENABLING TECHNOLOGIES j PAGE 77

walking their dog). Four field researchers made, in total, over 400 ELA visits; in each case the olderperson studied was visited by the same researcher. An observational template was used tocapture: researchers’ thoughts prior to each research visit; what happened during the visit; andto ensure issues discussed or observed were reported, including how the telecare was being usedand any issues not apparent from recorded conversation during the visit, such as relevant featuresof their home; and dynamics observed between persons present during the visit.
The interview approach chosen for the “guided conversations” (Downs, 1997) with participantsgenerated data on participants’ attitudes, opinions and activities. As part of the longitudinal researchdesign, different “topic guides” were developed for each visit to help explore participants’ everydaylives and to encourage a focus on the life course. The first ELA session with each participant focusedon installation of the telecare equipment, the rationale for acquiring it and explored participants’biographies, aiming to give them the freedom to “dictate those events and experiences that havedetermined the course of their lives” (Bornat and Bytheway, 2010, p. 6). For subsequent visits,the topic guides (covering social networks; homes and environments; education and employmenthistories; health and well-being; and attitudes towards technology) were tailored to individualparticipants’ experience, and updates on events since the previous visit were collected, withparticular reference to use of, and experiences with, the telecare equipment. While six to ninemonths is a relatively “compressed” timeframe for longitudinal research, it worked well in a study ofolder people with impairments and mobility limitations, and was adequate and appropriate for thestudy objectives, research questions and conceptual framework. Most research visits wereconducted when the older person was alone, but some took place when a family/friend carer,relative or care worker was present, sometimes creating joint interviews.
Within this multi-method approach, and where appropriate, participants were offered an “ELA box”,tailored to their circumstances, typically including a notebook, a disposable camera, and paper andstamped-addressed envelopes ( for writing to researchers). By individually tailoring the ELA boxes,the researchers could also tactfully navigate issues relating to literacy or to physical/sensorydisabilities. These creative methods were inspired by their effective use in team members’ previousresearch, and similar approaches have been used in other telecare research (Wherton et al., 2012).ELA participants were given flexible instructions to support completion of their diaries and on takingphotographs focused on their home, relationships, activities and any incidents involving theirtelecare devices. There was variation in the information recorded in the diaries, with some recordingtheir daily activities, concerns and feelings at length, while others made bullet point-style notes; bothformats provided insight into their daily lives and use of telecare. The photographs were printed anddiscussed with the participants at the next ELA visit.
Telecare acceptance and use: the importance of context
The ELA method provided crucial information relevant to the efficiency and effectiveness ofeach specific telecare intervention or package, and patterns observed in the data were used toidentify what “successful” use of telecare was, and what it meant, both to those using theequipment and those supporting them. Their criteria for success often differed from those usedby professionals/commissioners in the health and social care system, but paying attention toolder people’s perceptions, and to the contextual issues which affected their interactions withtelecare (and other outcomes) generated important insights. Using STS-influencedethnographic methods thus helped us to explain why expected and actual outcomes fortelecare often do not align (Greenhalgh and Swinglehurst, 2011). The following sectionshowcases the data collected using the ELA methodology, demonstrating that patterns ofbehaviour and attitudes related to telecare interventions are complex, and spatio-temporallylocated, enabling us to draw inferences capable of being tested in other contexts.
During the study, the research team rarely observed, or heard about, failures of telecare devicescaused by mechanical problems with the product. When used as intended, devices did nottrigger an alert to the designated response centre/responder. Study participants often mentionedincidents in which they could have used their telecare devices (especially pendant alarms),but had instead opted not to activate them to summon help. This “rejection” of the devices(either total or partial), and why it occurred, is relevant to the appraisal of telecare as “successful”
PAGE 78 j JOURNAL OF ENABLING TECHNOLOGIES j VOL. 11 NO. 3 2017

or “unsuccessful”, as without such understanding it is hard to assess the impact or effectivenessof telecare- here the ELA method proved invaluable.
Those who retained their devices, but did not use them as expected or directed, tended todistinguish between different types of fall: falls they could recover from alone (often withsubstantial effort or long periods on the floor), and those for which they needed their pendantalarm to get help. The decision to activate the alarm was mediated by several importantcontextual factors. Those who had not previously activated their device spoke of feeling confusedabout would happen: would they need to get to the response box to give instructions? Whowould be summoned to help them – would it be a carer/neighbour/family member, the police, anambulance or an emergency response service? These uncertainties, plus a desire to choose aresponse they felt suitable to the situation (e.g. not a family member late at night; not a “stranger”if security was a concern), could give participants pause, or deter their use of the pendant.Although these issues had usually been discussed when the equipment was installed, users andthose caring for them explained that this had often been at a time of heightened stress, linked todischarge from hospital or living alone for the first time after the death of a spouse, and for manyhad been the first time they had been in contact with social services. In these circumstances,instructions were easily misunderstood or forgotten, and some had felt overwhelmed by visitsfrom different services, so found it hard to disentangle who they should contact for advice. Someof the participants were inducted into the study when their telecare devices were installed.The research team was therefore able to observe the advice and information they received.There were a few instances in which the information provided was unclear or incorrect(e.g. whether the device could be worn in the shower, the cost of the service and eligibility criteriafor funded telecare). The assessors, installers, monitoring and response centre staff weretherefore all an important part of the context the telecare was situated in, and as such affectedhow participants viewed and used their devices. This embeddedness in social contextsmeant that devices were not neutral, predictable phenomena whose outcomes could easily becaptured in isolation.
Among those who had previously activated their pendant or other telecare device, pastexperience affected their later decisions. Some had found their previous experience negative andabandoned their device(s) to a drawer or other “safe place”. In some cases the previous responsehad surprised them – they had expected a family member to attend, but a response service cameinstead; for others, a long wait time had left them distrustful and reluctant to activate their alarm.By collecting data about these experiences longitudinally, the researchers could capturechanging attitudes towards the telecare devices over time, including, in a few cases, their removalfollowing false alerts or if the cost of the service was felt to be too significant.
Broader contextual issues also affected successful use of telecare. The study had the flexibility tocapture perspectives of people within an older person’s caring network (Yeandle, 2014) and theseshowed the importance of the interpersonal relationships within which telecare was situated;the participants were keen not to be “burdensome” to those who provided support by activatingtheir device too regularly or at particular times. Telecare was often initially installed (and accepted byparticipants) because it offered reassurance to those supporting them, but this had to be balancedwith their concerns about actually using their devices. Tensions could arise about wearing andusing the device between the older person and those providing their care (including, in some cases,care workers attending them at home); others reported that their telecare device(s) had improvedrelationships by providing reassurance between visits and forging stronger links betweenneighbours listed as responders.
The ELA method, and its emphasis on participants’ life histories, gave research participants anopportunity to reflect on their biographies, exploring how their past and present identities werebound up with roles they had taken in life. When telecare was installed as a response to a suddenevent (such as a fall or prior to hospital discharge) some participants experienced considerablechange. Some felt it was “out with the old” (activities and interests), and “in with new”(interventions and aids, introduced to reduce risk and provide assistance). Not all were happyabout or accepting of these developments and this was especially acute for those who felt theyhad had little say in the decision making involved. However, well-intentioned changes to theirhomes had been, or indeed how useful they were, some felt adaptions and the introduction of
VOL. 11 NO. 3 2017 j JOURNAL OF ENABLING TECHNOLOGIES j PAGE 79

telecare devices or other aids were markers of “old age”. Some thought telecare devices worn onthe body were unsightly, or not in keeping with how they wished to present themselves, andpreferred to keep devices such as pendant alarms “within reach” (e.g. on walking frames ortables, or worn concealed under clothing) which, in reality, made them potentially difficult toactivate in an emergency.
Others viewed telecare much more positively, arguing that it provided the vital “back-up”they needed to feel confident about living independently in the community (or being “allowed”by others to continue doing this). As their bodily frailty had increased, many participantshad identified areas of their homes as potentially “risky” or “out of bounds”; for some,telecare enabled these “high risk” areas, such as gardens, staircases and upper floors,to remain accessible. It also meant they felt safer and more secure in their homes (especially ifliving alone) and gave reassurance to their families and friends, often impacting positivelyon family relationships. Control, and the degree to which the older person felt empoweredin decisions about care and support, were critical in shaping their perspectives about telecare.
The ELA method in AKTIVE thus highlighted how context affects the lived experience of telecareand other technologies and changes designed to support older people who become frail.It demonstrated the significance of choice and control when packages of support, includingtelecare, are developed, and revealed the “trade-off” between how telecare can make people feeland its capacity to help them continue activities which help them to be and feel active,independent and embedded in valued places and communities. When introduced as part ofwider (often unwelcome) changes in their lives or homes (home care, home adaptations,the identification of some areas as “risky”), telecare could be hard to reconcile with valuedidentities as independent and active persons, however.
Strengths and limitations of the ELA approach
As methods which embrace ethnography and social constructivist approaches generate datavery different from those collected in experimental/quasi-experimental research, to compare their“quality” would be to compare apples and oranges. That said, the ELA approach produced validdata, collected in naturalistic settings which could be confirmed in the repeat nature of the visitsand, in relevant cases, from others involved in the older person’s life and/or care. Our findingswere context specific, but enabled patterns and common behaviours or attitudes to be observed,and used to generate theories and hypotheses.
The longitudinal aspect of the ELA method allowed the researchers to observe changeover time and ensured they did not merely capture “one-off” events; it was also flexible enough toensure the researchers were not closed off to “unexpected” data (Silverstone et al., 1991).Spreading research contact over an extended period also meant data could be collected in a lessintrusive and intense manner, appropriate for the study’s frail older participants, and allowedresearchers to factor in “good” and “bad” days, which was particularly important for respondentswhose health was variable, or who had cognitive impairment. The ELA visits also allowed theresearchers to build trust and rapport, facilitate understanding and create opportunities to clarifymaterial discussed in earlier visits. Ethnographic interviews yielded much information aboutparticipants’ use of and feelings about telecare, but also provided insights into the everyday livesof older people. The participants could also be observed demonstrating how they usedtheir telecare devices, sometimes with great difficulty, and researchers could note how theirhomes had changed over time, as frailty increased or, in some cases, devices and aids wereremoved as they recovered.
Reflecting on study visits, researchers felt the combination of open, “conversational” questionsand additional creative exercises and techniques enabled most participants (sometimes withthe assistance of their carers) to voice their opinions about telecare, as well as to discusspast and present events and share their general concerns and aspirations. The ELA topicguides allowed researchers to explore older people’s lives in ways which were enjoyable forboth parties and which produced material relevant to the study, although, due to the adaptablenature of the guides, it could sometimes be challenging to keep participants “on topic”.Where applicable, the joint interviews also produced insight into interpersonal dynamics,
PAGE 80 j JOURNAL OF ENABLING TECHNOLOGIES j VOL. 11 NO. 3 2017

interactions and relationships (Arksey, 1996). Some carers were able to re-word questions orcomments, helping with comprehension, but joint interviews could also be challenging ifcarers tried to “take over” the conversation, a particular problem in one case where theparticipant had dementia. The research team used techniques such as redirecting questions tothe older person (even if the other person present had already responded to it). If carers“spoke over”, answered on behalf of the older person, or corrected them to provide what theyfelt were the “facts” (Pratt, 2002), the researcher suggested an additional, separate interviewwith the carer, to enable them to tell “their side of the story” without devaluing or demoralisingthe older person.
The creative aspects of the ELA methodology were used by many, though not all participants(in total, 21 participants used diaries and eight took photographs). Diaries, frequently used insocial science and health research to record time use, social interaction and perceptionsof health over time, have some limitations, as participants can feel uneasy about recordingpersonal thoughts, or may lack confidence in their ability to write in a “correct” way(Välimäki et al., 2007). To mitigate this risk, the guidance was flexible in its approach,suggesting topics for notes which could be expressed in whatever format the participant feltcomfortable with. The diaries were valuable as they relied on short-term memory and reducedrecall errors, and allowed the researchers to triangulate the data. Research visits often beganwith the participant – particularly if they were unable to leave their home alone – stating that“nothing had happened” since the previous visit. However the diaries often sparked memories,clarifying points which had become confused, or provided insight into the participants’perceptions. They also kept the participants engaged with the project between visits and couldprompt the participants to feel a sense of achievement afterwards, and provided theopportunity for the participants to “say” things they perhaps felt uncomfortable aboutmentioning to the researcher. Fewer participants used photographs, and the cameras raisedsome practical issues for the research team due to difficulties in getting photos developedquickly enough for the pictures to still resonate with the participants. Those who did takephotographs tended to focus on three aspects of their everyday experience: the people in theirlives; places (typically their home or localities they visited); and things which helped them,including their telecare devices and other equipment.
The ELA method produced a large volume of data, comprising approximately 400 transcriptsin addition to fieldwork notes, and the diary and photographic data. This potentiallyoverwhelming amount of data were managed using an analytical strategy which employedthematic analysis (identified and cross-checked by all researchers) and computer-aidedtechniques for data mark-up and retrieval, plus various indexing and summarising techniquesto help the whole team acquire and retain a “picture” of each participant, includingthose they had not personally met. In line with an STS and contextualist approach, the analysisfocused on the processes at work, as opposed to the relationships between, or the relativeimportance of, variables; the focus was therefore on identifying patterns of actions which couldbe applied to similar contexts (Abbott, 1997). The analysis was nonetheless a challenging task,and required more time than originally allocated to it in the project plan. Due to thequalitative nature of the study, a representative sample of the wider population of telecare userswas not the aim[5]. It could be argued, therefore, that this limits the generalisability of thefindings, yet though the findings could be context specific, the in-depth methodologyprovided a valuable “thick description” and valid picture of the use of telecare by older people inthese two authorities, and the patterns we observed can be explored elsewhere and used togenerate theory.
Conclusion
This paper has described an innovative methodological approach applied in telecare research.The dominant methodological debate in this field has been inclined towards RCTs as the “goldstandard” for “robust evidence”. Telecare is a complex social intervention, however, affected bya myriad of confounding variables which may influence outcomes and compromisemeasurement of effects. A multidisciplinary and longitudinal approach is thus essential tofully address the importance of context in mediating the experience and use of telecare.
VOL. 11 NO. 3 2017 j JOURNAL OF ENABLING TECHNOLOGIES j PAGE 81

The research team developed a methodology to permit careful observation of the biographicaland social context in which the telecare equipment was situated, and to examine its effect on howusers and those involved in their care perceived and engaged with it. Influenced by STS and theChicago School, the methods chosen for the ELA were primarily ethnographic observationsand interviews with a biographical or thematic focus; these were supplemented by photographsand diaries to produce a nuanced overview of older people’s everyday lives and of the role oftelecare within them.
While labour-intensive in terms of data collection and analysis, the ELA approach yieldedimportant insights which other methods could not have achieved, including data thathighlighted the importance of the context within which the telecare was situated. They alsoprovided understanding of broader issues related to ageing, including challenges to identity, theimpact of physical or mental health problems, changes in relationships, care and support andsocial isolation. Understanding of these issues is very important for interpreting the factors whichaffect how telecare devices are received and used, with implications for whether these can bejudged “successful” or worth investing in. The ELA method, with its emphasis on eachparticipant’s “life history” in the first session, offered research participants an opportunity to reflecton their biographies, exploring how their past and present identities were bound up with rolesthey had taken in life. Many research participants felt “lost” within their social relationships as theystruggled to shift their identity from “carer” to “cared for”; many expressed a desire not to becomea “burden” to their families. It was often within these contexts, with painful changes on-going,that telecare was introduced. Few in the sample had telecare installed as a preventative measure(although a small minority acquired it as standard when entering supported housing); it wasgenerally installed in response to a sudden event such as a fall, loss of a co-resident spouse orhospitalisation, and as a result, some participants felt upset or unsettled. These feelings affectedtheir interactions with their telecare devices. For those who felt control over their daily lives andliving environment had been taken away, the decision about whether to wear, or to activate, theirdevices was significant.
These are important issues. They mediate the use of telecare devices by older adults, and need tobe considered both in the design of research to evaluate its outcomes, and by those developingand delivering telecare services and products to promote their optimal use. For example, a RCTstudy could be designed to take adequate account of the context in which telecare is installed,and to ensure that, prior to the assessment of outcomes, it is introduced and delivered in amanner broadly comparable across the intervention group.
Notes
1. The Whole Systems Demonstrator is the largest RCT of telecare and telehealth conducted in the UK todate, although other studies had been conducted in the years prior to its launch (e.g. Opening Doors forOlder People, Bowes and McColgan, 2006).
2. See (Hamblin, 2017).
3. More information on the AKTIVE, including the working papers can be found here: www.aktive.org.uk
4. Recruitment support was also provided by the Thames Valley Dementia and NeurodegenerativeDiseases Research Network and the Oxford Health NHS Foundation Trust.
5. An accurate picture of this wider population was not possible, as the data collected by the localauthorities on their telecare users did not permit this.
References
Abbott, A. (1997), “Of time and space: the contemporary relevance of the Chicago School”, Social Forces,Vol. 75 No. 4, pp. 1149-82.
ADASS (2014), “Better Care Technology Survey 2014 Report”, ADASS, London.
AKTIVE Consortium (2013), “The role of telecare in meeting the care needs of older people: themes, debatesand perspectives in the literature on ageing and technology”, AKTIVE Research Report Vol. 1, CIRCLE,University of Leeds, Leeds.
PAGE 82 j JOURNAL OF ENABLING TECHNOLOGIES j VOL. 11 NO. 3 2017

Arksey, H. (1996), “Collecting data through joint interviews”, Social Research Update, Vol. 15, pp. 1-4.
Bowes, A. and McColgan, G. (2006), Smart Technology and Community Care for Older People: Innovation inWest Lothian, Age Concern Scotland, Edinburgh.
Bornat, J. and Bytheway, B. (2010), “Perceptions and presentations of living with everyday risk in later life”,British Journal of Social Work, Vol. 40 No. 4, pp. 1118-34.
Buckle, P. (2014), “Human factors that influence the performance of the telecare system”, AKTIVEresearch report, Working Paper No. 7, Vol. 2, University of Leeds, Leeds.
Davies, A. and Newman, S. (2011), “Evaluating telecare and telehealth Interventions”, WSDAN briefing paper,Kings Fund, London.
De Leonibus, V., Bartosova, R. and Lewis, E. (2013), “ALT market in the UK – AKTIVE market report:initial overview”, AKTIVE research report, CIRCLE, University of Leeds, Leeds.
Downs, M. (1997), “The emergence of the person in dementia research”, Ageing and Society, Vol. 17 No. 5,pp. 597-607.
Greenhalgh, T. and Swinglehurst, D. (2011), “Studying technology use as social practice: the untappedpotential of ethnography”, BMC Medicine, Vol. 9 No. 45, pp. 1-7.
Hamblin, K. (2017), “Telecare, obtrusiveness, acceptance and use: an empirical exploration”, British Journalof Occupational Therapy, Vol. 80 No. 2, pp. 132-8.
Lull, J. (1987), World Families Watch Television, Sage, Newbury Park, CA.
Mair, F.S., Hiscock, J. and Beaton, S.C. (2008), “Understanding factors that inhibit or promote the utilizationof telecare in chronic lung disease”, Chronic Illness, Vol. 4 No. 2, pp. 110-17.
Milligan, C., Roberts, C. and Mort, M. (2011), “Telecare and older people: who cares where?”, Social Science &Medicine, Vol. 72 No. 3, pp. 347-54.
Morgan-Trimmer, S. and Wood, F. (2016), “Ethnographic methods for process evaluations of complex healthbehaviour interventions”, Trials, Vol. 17 No. 232, pp. 1-11.
Morley, D. and Silverstone, R. (1991), “Communication and context: ethnographic perspectives on the mediaaudience”, in Jankowski, N.W. and Jensen, K. (Eds), A Handbook of Qualitative Methodologies for MassCommunication Research, Routledge, London, pp. 149-62.
Pawson, R., Wong, G. and Owen, L. (2011), “Known knowns, known unknowns, unknown unknowns:the predicament of evidence-based policy”, American Journal of Evaluation, Vol. 32 No. 4, pp. 518-46.
Pols, J. and Willems, D. (2011), “Innovation and evaluation: taming and unleashing telecare technology”,Sociology of Health & Illness, Vol. 33 No. 3, pp. 484-98.
Pratt, R. (2002), “Nobody’s ever asked how I felt”, in Wilkinson, H. (Ed.), The Perspectives of People withDementia: Research Methods and Motivations, Jessica Kingsley Publishers, London, pp. 165-82.
Sanders, C., Rogers, A., Bowen, R., Bower, P., Hirani, S., Cartwright, M., Fitzpatrick, R., Knapp,M., Barlow, M.,Hendy, J., Chrysanthaki, T., Bardsley, M. and Newman, S. (2012), “Exploring barriers to participation andadoption of telehealth and telecare within the whole system demonstrator trial: a qualitative study”, BMC HealthServices Research, Vol. 12 No. 1, p. 220.
Scottish Government (2008), Seizing the Opportunity: Telecare Strategy 2009-2010, Scottish Government,Edinburgh.
Scriven, M. (2008), “A summative evaluation of RCT methodology: & an alternative approach to causalresearch”, Journal of Multidisciplinary Evaluation, Vol. 5 No. 9, pp. 11-24.
Silverstone, R., Hirsch, E. and Morley, D. (1991), “Listening to a long conversation: an ethnographic approachto the study of information and communication technologies in the home”, Cultural Studies, Vol. 5 No. 2,pp. 204-27.
Välimäki, T., Vehviläinen‐Julkunen, K. and Pietilä, A.M. (2007), “Diaries as research data in a study on familycaregivers of people with Alzheimer’s disease: methodological issues”, Journal of Advanced Nursing, Vol. 59No. 1, pp. 68-76.
Wherton, J., Sugarhood, P., Procter, R., Rouncefield, M., Dewsbury, G., Hinder, S. and Greenhalgh, T.(2012), “Designing assisted living technologies ‘in the wild’: preliminary experiences with cultural probemethodology”, BMC Medical Research Methodology, Vol. 12 No. 188, pp. 1-13.
VOL. 11 NO. 3 2017 j JOURNAL OF ENABLING TECHNOLOGIES j PAGE 83

Williams, R. and Edge, D. (1996), “The social shaping of technology”, Research Policy, Vol. 25 No. 6,pp. 865-99.
Williams, T., May, C., Mair, F., Mort, M. and Gask, L. (2003), “Normative models of health technologyassessment and the social production of evidence about telehealth care”, Health Policy, Vol. 64 No. 1,pp. 39-54.
Yeandle, S. (2014), “Frail older people and their networks of support: how does telecare fit in?”, AKTIVEresearch report, Vol. 2, Working Paper No. 2, University of Leeds, Leeds.
Yeandle, S., Buckle, P., Fry, G., Hamblin, K., Koivunen, E.-R. and McGinley, C. (2014), “The AKTIVE project’ssocial, design and prospective hazard research: research methods”, AKTIVE research report, Vol. 3, Leeds:CIRCLE, University of Leeds, Leeds.
Corresponding author
Kate Hamblin can be contacted at: [email protected]
For instructions on how to order reprints of this article, please visit our website:www.emeraldgrouppublishing.com/licensing/reprints.htmOr contact us for further details: [email protected]
PAGE 84 j JOURNAL OF ENABLING TECHNOLOGIES j VOL. 11 NO. 3 2017

A technology-aided program for helpingpersons with Alzheimer’s disease performdaily activities
Giulio Lancioni, Nirbhay Singh, Mark O’Reilly, Jeff Sigafoos, Fiora D’Amico, Katia Pinto,Floriana De Vanna and Alessandro Caffò
Abstract
Purpose – Persons with mild and moderate Alzheimer’s disease experience increasing activity engagementfailures, with consequent cognitive, social, and physical drawbacks. The purpose of this paper is to assess atechnology-aided program to help these persons to independently start and carry out daily activities at theappropriate times.Design/methodology/approach – The program was implemented with eight participants according to anadapted non-concurrent multiple baseline design across participants. The program provided eachparticipant with: timely reminders about the activities to carry out, verbal instructions about the activity steps,and brief encouragements and praise.Findings – All participants showed improvement during the program, that is, they managed toindependently start the activities at the scheduled times and perform those activities with satisfactory levels ofaccuracy (i.e. with mean percentages of correct steps nearing or exceeding 90).Originality/value – A technology-aided program, such as that used in this study, may help persons withmild and moderate Alzheimer disease engage in daily activities, with possible benefits for their cognitivefunctioning, social image, and physical condition.
Keywords Tablet, Assistive technology, Instructions, Reminders, Alzheimer’s disease, Daily activities
Paper type Research paper
Background
Alzheimer’s disease is a neurodegenerative disorder that causes a progressive decline in thepersons’ condition (Bernick et al., 2012; Kim, 2015; Wilson et al., 2012). For example, duringthe mild and moderate stages of the disease, persons begin to show activity engagementproblems, with a tendency to be gradually more passive and inaccurate (Boyd et al., 2017;Lancioni et al., 2015). They do not seem to be fully aware of time and fail to start daily activitieswhen these are due (Brown et al., 2011; Spíndola and Dozzi Brucki, 2011). Likewise, they donot seem to recall all the activity steps, with an increasing deterioration of their performance(Campos et al., 2016; Khosravi and Ghapanchi, 2016).
In contrast with the aforementioned decline, engagement in daily activities is considered vitallyrelevant from a cognitive and social standpoint and it also constitutes a practical opportunity forphysical exercise (Hernández et al., 2015; Law et al., 2014; Letts et al., 2011). Indeed,the performance of daily activities may involve motor responses such as, arms and legs stretching,body bending and balancing, weight lifting and carrying, and walking, which are highly valued inphysical exercise programs for elderly people (Hernández et al., 2015; Hoffmann et al., 2013).Thus, there is wide consensus on the need to foster such activities in persons with Alzheimer’sdisease and supply these persons with assistive technology to boost their independencefrom staff/caregivers (Boyd et al., 2017; Czarnuch et al., 2016; Wang et al., 2017). Technologysolutions have normally been used either to remind the persons of simple activities to perform
Received 19 March 2017Revised 1 May 2017Accepted 2 May 2017
Declaration of interest: the authorsreport no conflicts of interest. Theauthors alone are responsible for thecontent and writing of the paper.
Giulio Lancioni is a Professorat the Department ofNeuroscience and SenseOrgans, University of Bari,Bari, Italy.Nirbhay Singh is a Professor ofPsychiatry at the Department ofPsychiatry, Augusta University,Augusta, Georgia, USA.Mark O’Reilly is a Professor atthe University of Texas atAustin, Austin, Texas, USA.Jeff Sigafoos is a Professor at theVictoria University of Wellington,Wellington, New Zealand.Fiora D’Amico is a Psychologistat the S. Raffaele Medical CareCenters, Bari, Italy.Katia Pinto is aNeuropsychologist at the OperaDon Uva, Alzheimer CenterBisceglie, Bisceglie, Italy.Floriana De Vanna is aPsychotherapist at the MemoryDrops Day Center,Giovinazzo, Italy.Alessandro Caffò is anAssistant Professor at theDipartimento di Scienze dellaFormazione PsicologiaComunicazione, Universitadegli Studi di Bari, Bari, Italy.
DOI 10.1108/JET-03-2017-0011 VOL. 11 NO. 3 2017, pp. 85-91, © Emerald Publishing Limited, ISSN 2398-6263 j JOURNAL OF ENABLING TECHNOLOGIES j PAGE 85

(e.g. taking medication) or to provide the persons with instructions for the steps of complex, dailyactivities (e.g. preparing food recipes) started after staff/caregiver reminders (Kamimura et al., 2012;Lancioni et al., 2012; Oriani et al., 2003; Perilli et al., 2013).
This pilot study was aimed at assessing a technology-aided program that provided eightparticipants with mild or moderate Alzheimer’s disease with timely reminders about the dailyactivities to carry out, verbal instructions concerning the steps included in those activities, as wellas simple encouragements and praise. In essence, the study was to determine whetherthe program could support the participants’ independent start and successful performance of theactivities scheduled and motivate the participants to maintain their functional engagement overtime. A positive outcome of the study would be considered practically encouraging and suggestbasic intervention guidelines for contexts dealing with the wellbeing of these people.
Methods
Participants and setting
The eight participants included in the study (seven women and one man) were deemed to be inthe mild or moderate stages of the disease, and represented a convenience sample (Pedhazurand Schmelkin, 1991). Staff/caregivers’ reports and direct observations indicated that theparticipants had difficulties with daily activities (i.e. failing to remember the times at which theywere due and the steps involved) and underlined differences in the participants’ abilities to followverbal instructions for performing the activities. Some participants seemed more skilled thanothers in following small strings of instructions (i.e. instructions presented in succession andreferring to sequences of activity steps). Based on those apparent differences, the participantswere divided into two groups of four. The members of the first group (with the pseudonyms ofKim, Carole, Kathie, and Fred) were 64-77 (M¼ 71) years old, had scores of 21-25 (M¼ 23)on the Mini-Mental State Examination (Folstein et al., 1975), and were considered to function at ahigher level than those of the second group. The members of the second group (with thepseudonyms of Donna, Nancy, Pam, and Beth) were 66-79 (M¼ 75) years old, and hadMini-Mental scores of 15-22 (M¼ 19). All participants tended to be fairly passive unless instructedby staff/caregivers, and had verbalized their interest in using a device such as that adopted in thisstudy when staff showed it to them. While this interest was seen as consent to the study, theirreported inability to (reliably) read and sign a consent form had led their families to sign such formfor them. The study complied with the 1964 Helsinki declaration and its later amendments andwas approved by a relevant ethics committee. The activity and care centers that the participantsregularly attended served as the setting for the study.
Activities, technology, and sessions
For each participant, 12 or 14 daily activities of practical relevance were selected (e.g. preparingcoffee, setting the table, watering plants, bringing paper and soap to different toilet rooms,preparing a toast, and making photocopies). The activities included a mean of 18 steps for thefirst four participants and 14 steps for the second group of participants. Specific verbalinstructions were recorded for the single activity steps and presented to the participants duringthe intervention with the technology-aided program (see below). The technology included a tabletdevice with Android operating system and the Talking Alarm Clock application as well as awireless Bluetooth earpiece. The Talking Alarm Clock application was highly suitable to schedulethe activities with related instructions, as well as encouragement/praise statements. Six or sevenactivities were scheduled over 2- or 3-hour morning or afternoon periods representing thesessions of the study.
Scheduling an activity consisted of recording a time and a verbal reminder for the activity, specificinstructions to guide the participant through the activity steps, and encouragement/praisestatements. When the time for an activity was reached, the participant was reminded to start thatactivity and thereafter he or she was presented with the instructions for it. For the first fourparticipants, the instructions were presented in strings of three to five (i.e. without breaksbetween them) to cover sets of as many steps, such as, “take the container, put paper and soap
PAGE 86 j JOURNAL OF ENABLING TECHNOLOGIES j VOL. 11 NO. 3 2017

in it, and start moving to the first toilet.” The instruction strings were separated by intervals of30-90 s (with variations across participants and activities based on preliminary observations ofparticipants’ step performance), during which short verbal encouragement/praise statementscould occur. For the participants of the second group, the instructions were typically presented instrings of two to cover sets of as many steps. Again, encouragement/praise statements couldoccur in between instruction strings. The participants received the reminders, the instructions,and the encouragement/praise statements through the aforementioned, wireless Bluetoothearpiece linked to the tablet. The earpiece was easy to wear and allowed the tablet to be kept in aremote place.
Experimental conditions
The study included two baseline phases without technology and an intervention phase with thetechnology. The numbers of sessions the participants received within the two baseline phasesvaried according to an adapted non-concurrent multiple baseline design across participants(Kazdin, 2011).
Baseline I and II. During the first baseline, each session started with the participant receivinga printed list of six or seven activities that he or she was expected to carry out and the times atwhich the activities were due. A research assistant familiar to the participant, and speciallyprepared on the implementation of the experimental conditions, read those activities andtimes and placed the list on the table before the participant. This phase served to determinehow many of the scheduled activities the participant would start independently. During eachsession of the second baseline, the research assistant asked the participant to carry outsix or seven activities (i.e. one at a time). This phase served to determine how many steps ofeach activity the participant carried out correctly. The research assistant would intervene tocorrect a step only if an error on that step precluded the adequate continuation of the activity.At the end of an activity, the research assistant praised the participant for his or her willingnessand efforts.
Intervention. At the beginning of each session of the intervention phase, the participant wasprovided with the wireless Bluetooth earpiece, and the technology-aided program was set towork as described above. The initial three or four sessions served as familiarization and practicesessions, with the participant receiving explanations and guidance from the research assistantand gaining independent activity performance. During the subsequent sessions, the participantreceived no specific help from the research assistant and error corrections would occur as duringthe second baseline phase. At the end of the activities, the research assistant would praise theparticipant (see above). The intervention phase served to determine how many of the activitiesscheduled within the sessions the participant started independently and how many steps ofthose activities the participant carried out correctly. In essence, the intervention phase was toclarify the impact of the program and its likely practical implications.
Data recording
Data recording concerned the number of activities the participants started as scheduled withinthe sessions (across the first baseline and the intervention phase) and the number of steps theparticipants performed correctly for the activities started in the sessions (during the second baselineand the intervention phase). Interrater agreement was assessed in about 25 percent of the sessions.Percentages of agreement were computed on the single sessions for the first measure and singleactivities for the second measure by dividing the number of activities or steps with agreement bythe total number of activities or steps and multiplying by 100 percent. The percentages were in the80-100 range, with means exceeding 95 on both measures for all participants.
Results
Table I reports the participants’ mean percentages of activities started independently and theirmean percentages of activity steps carried out correctly across the baseline and interventionsessions. During the first baseline phase, which included between three and five sessions
VOL. 11 NO. 3 2017 j JOURNAL OF ENABLING TECHNOLOGIES j PAGE 87

per participant, the participants’ mean percentages of activities started independently werebetween 0 and 14. During the second baseline phase, which also included between threeand five sessions per participant, the participants’mean percentages of activity steps carried outcorrectly were always below 35. During the intervention phase, which included between34 and 78 sessions ( following the three or four introductory sessions), the participants’mean percentages of activities started independently were (close to) 100. That is,the participants responded to all the technology-regulated reminders or missed only very fewof them (i.e. a maximum of six in the case of Donna) throughout the phase. The overall meanpercentages of correct steps were near or above 90 for all participants. The Kolmogorov-Smirnovtest (Siegel and Castellan, 1988) indicated that the differences between the baseline andintervention session values were statistically significant (po0.01) on both measures (i.e. activitiesstarted independently and activity steps carried out correctly) for all participants.
Discussion
The participants’ successful start and accurate performance of the activities scheduled during theintervention sessions emphasize the effectiveness of the technology-aided program. Indeed,the program’s components (i.e. reminders, instructions, and encouragements/praise) appearedsuitable to ensure the participants’ timely and appropriate engagement in those activitiesindependent of any specific supervision. Moreover, the participants seemed to enjoy the sessionsand their activity engagement with the support of the technology, as indicated by a number ofinformal reports underlying their eagerness to be involved in the sessions and their satisfactionwith their activity performance.
Although caution is required in interpreting the results of this study (given the small number ofparticipants), such results seem to meaningfully extend the evidence provided by previousstudies in the area. In fact, earlier studies were basically concerned with promoting theindependent start and execution of simple activities (e.g. taking medication) or the performance ofcomplex activities whose start relied on staff/caregiver reminders (Kamimura et al., 2012; Kerkhofet al., 2016; Lancioni et al., 2014). Enabling persons with mild or moderate Alzheimer’s disease tostart and carry out daily activities independently, without specific demands on staff/caregivertime, may also be critical to allow them a higher level of activity engagement during the day(Hernández et al., 2015; Imbeault et al., 2014).
Regular activity engagement can have a positive impact in terms of cognitive stimulation (i.e. byfostering the practice of perceptual and communication functions), from a social standpoint(i.e. by improving the participants’ social status and relationship with families and staff ), as well asin terms of physical exercise (Eggermont et al., 2010; Hernández et al., 2015; Law et al., 2014).With regard to the last point, it is important to note that daily activities, like those used in this
Table I Participants’ mean percentages of activities started independently and meanpercentages of activity steps carried out correctly
Baseline I Baseline II InterventionIndependent Correct Independent CorrectActivities Steps Activities Steps
Participants Sessions Means Sessions Means Sessions Means Means
Kim 4 0 4 33 66 100 96Carole 4 14 5 30 78 100 98Kathy 3 0 4 30 41 99 87Fred 5 0 3 29 75 100 90Donna 3 10 5 18 74 99 96Nancy 4 4 4 31 34 100 97Pam 4 0 4 32 49 100 95Beth 5 3 3 26 43 99 93
Note: Mean percentages are rounded to the nearest full number value
PAGE 88 j JOURNAL OF ENABLING TECHNOLOGIES j VOL. 11 NO. 3 2017

study, can involve motor responses, such as ambulating, body bending and balancing, arms andlegs stretching, arms lifting, and weight carrying. All these responses would be consideredrelevant in a program of mild physical exercise for these persons (Canonici et al., 2012; De Vreedeet al., 2005; Maliszewska-Cyna et al., 2017).
Conclusion
In conclusion, a technology-aided program, such as that used in this study, seems to be aneffective resource with multiple practical implications. Before general statements can be drawn,however, new research is needed to address the main limitations of the present study andspecifically verify whether the results reported above can be replicated across larger groups ofparticipants (Kazdin, 2011; Makel and Plucker, 2014), gather formal evidence about the level ofsatisfaction the participants experience with the program conditions and their performance (i.e.by recording their program preferences or indices of happiness) (Sidani et al., 2009), anddetermine the overall acceptability of the program within daily contexts as well as any perceptionof risks/drawbacks associated with its application (i.e. by using social validation assessments)(Luiselli et al., 2010).
References
Bernick, C., Cummings, J., Raman, R., Sun, X. and Aisen, P. (2012), “Age and rate of cognitivedecline in Alzheimer disease: Implications for clinical trials”, Archives of Neurology, Vol. 69 No. 7, pp. 901-5.
Boyd, H.C., Evans, N.M., Orpwood, R.D. and Harris, N.D. (2017), “Using simple technology to promptmultistep tasks in the home for people with dementia: an exploratory study comparing prompting formats”,Dementia (London), Vol. 16 No. 4, pp. 424-42.
Brown, P.J., Devanand, D.P., Liu, X. and Caccappolo, E. (2011), “Functional impairment in elderly patientswith mild cognitive impairment and mild Alzheimer disease”, Archives of General Psychiatry, Vol. 68 No. 6,pp. 617-26.
Campos, C., Rocha, N.B., Vieira, R.T., Rocha, S.A., Telles-Correia, D., Paes, F., Yuan, T., Nardi, A.E.,Arias-Carrion, O., Machado, S. and Caixeta, L. (2016), “Treatment of cognitive deficits in Alzheimer’s disease:a psychopharmacological review”, Psychiatria Danubina, Vol. 28 No. 1, pp. 2-12.
Canonici, A.P., Andrade, L.P., Gobbi, S., Santos-Galduroz, R.F., Gobbi, L.T. and Stella, F. (2012), “Functionaldependence and caregiver burden in Alzheimer’s disease: a controlled trial on the benefits of motorintervention”, Psychogeriatrics, Vol. 12 No. 3, pp. 186-92.
Czarnuch, S., Ricciardelli, R. and Mihailidis, A. (2016), “Predicting the role of assistive technologies in the livesof people with dementia using objective care recipient factors”, BMCGeriatrics, Vol. 16, p. 143, doi: 10.1186/s12877-016-0314-2.
De Vreede, P.L., Samson, M.M., Van Meeteren, N.L., Duursma, S.A. and Verhaar, H.J. (2005), “Functional-task exercise versus resistance strength exercise to improve daily function in older women: a randomized,controlled trial”, Journal of the American Geriatric Society, Vol. 53 No. 1, pp. 2-10.
Eggermont, L.H., Gavett, B.E., Volkers, K.M., Blankevoort, C.G., Scherder, E.J., Jefferson, A.L.,Steinberg, E., Nair, A., Green, R.C. and Stern, R.A. (2010), “Lower-extremity function in cognitively healthyaging, mild cognitive impairment, and Alzheimer’s disease”, Archives of Physical Medicine and Rehabilitation,Vol. 91 No. 4, pp. 584-8.
Folstein, M., Folstein, S.E. and McHugh, P.R. (1975), “Mini-mental State” a practical method for grading thecognitive state of patients for the clinician”, Journal of Psychiatric Research, Vol. 12 No. 3, pp. 189-98.
Hernández, S.S., Sandreschi, P.F., da Silva, F.C., Arancibia, B.A., da Silva, R., Gutierres, P.J. and Andrade, A.(2015), “What are the benefits of exercise for Alzheimer’s disease? A systematic review of the past 10 years”,Journal of Aging and Physical Activity, Vol. 23 No. 4, pp. 659-68.
Hoffmann, K., Frederiksen, K.S., Sobol, N.A., Beyer, N., Vogel, A., Simonsen, A.H., Johannsen, P., Lolk, A.,Terkelsen, O., Cotman, C.W., Hasselbach, S.G. and Waldemar, G. (2013), “Preserving cognition, quality oflife, physical health and functional ability in Alzheimer’s disease: the effect of physical exercise (ADEX trial) –Rationale and design”, Neuroepidemiology, Vol. 41 Nos 3-4, pp. 198-207.
VOL. 11 NO. 3 2017 j JOURNAL OF ENABLING TECHNOLOGIES j PAGE 89

Imbeault, H., Bier, N., Pigot, H., Gagnon, L., Marcotte, N., Fulop, T. and Giroux, S. (2014), “Electronic organizerand Alzheimer’s disease: fact or fiction?”, Neuropsychological Rehabilitation, Vol. 24 No. 1, pp. 71-100.
Kamimura, T., Ishiwata, R. and Inoue, T. (2012), “Medication reminder device for the elderly patients withmild cognitive impairment”, American Journal of Alzheimer’s Disease and Other Dementias, Vol. 27 No. 4,pp. 238-42.
Kazdin, A.E. (2011), Single-Case Research Designs: Methods for Clinical and Applied Settings, 2nd ed.,Oxford University Press, New York, NY.
Kerkhof, Y.J., Graff, M.J., Bergsma, A., de Vocht, H.H. and Dröes, R.M. (2016), “Better self-management andmeaningful activities thanks to tablets? Development of a person-centered program to support people withmild dementia and their carers through use of hand-held touch screen devices”, InternationalPsychogeriatrics, Vol. 28 No. 11, pp. 1917-29.
Khosravi, P. and Ghapanchi, A.H. (2016), “Investigating the effectiveness of technologies appliedto assist seniors: a systematic literature review”, International Journal of Medical Informatics, Vol. 85 No. 1,pp. 17-26.
Kim, S. (2015), “Cognitive rehabilitation for elderly people with early-stage Alzheimer’s disease”, Journal ofPhysical Therapy Science, Vol. 27 No. 2, pp. 543-6.
Lancioni, G.E., Perilli, V., Singh, N.N., O’Reilly, M.F., Sigafoos, J., Cassano, G., Cordiano, N., Pinto, K.,Minervini, M. G. and Oliva, D. (2012), “Technology-aided pictorial cues to support the performance of dailyactivities by persons with moderate Alzheimer’s disease”, Research in Developmental Disabilities, Vol. 33 No. 1,pp. 265-73.
Lancioni, G.E., Singh, N.N., O’Reilly, M.F., Sigafoos, J., D’Amico, F., Ferlisi, G., Denitto, F., De Vanna, F. andBelardinelli Olivetti, M. (2015), “Patients with moderate Alzheimer’s disease engage in verbal reminiscencewith the support of a computer-aided program: a pilot study”, Frontiers in Aging Neuroscience, Vol. 7, p. 109,doi: org/10.3389/fnagi.2015.00109.
Lancioni, G.E., Singh, N.N., O’Reilly, M.F., Sigafoos, J., Renna, C., Pinto, K., De Vanna, F., Caffo, A.O. andStasolla, F. (2014), “Persons with moderate Alzheimer’s disease use simple technology aids to manage dailyactivities and leisure occupation”, Research in Developmental Disabilities, Vol. 35 No. 9, pp. 2117-28.
Law, L.L., Barnett, F., Yau, M.K. and Gray, M.A. (2014), “Effects of functional tasks exercise on older adultswith cognitive impairment at risk of Alzheimer’s disease: a randomized controlled trial”, Age and Ageing,Vol. 43 No. 6, pp. 813-20.
Letts, L., Edwards, M., Berenyi, J., Moros, K., O’Neill, C., O’Toole, C. and McGrath, C. (2011),“Using occupations to improve quality of life, health and wellness, and client and caregiver satisfaction forpeople with Alzheimer’s disease and related dementias”, American Journal of Occupational Therapy, Vol. 65No. 5, pp. 497-504.
Luiselli, J.K., Bass, J.D. and Whitcomb, S.A. (2010), “Teaching applied behavior analysis knowledgecompetencies to direct-care service providers: outcome assessment and social validation”, BehaviorModification, Vol. 34 No. 5, pp. 403-14.
Makel, M.C. and Plucker, J.A. (2014), “Facts are more important than novelty: Replication in the educationsciences”, Educational Researcher, Vol. 43 No. 6, pp. 304-16.
Maliszewska-Cyna, E., Lynch, M., Oone, J.J., Nagy, P.M. and Aubert, I. (2017), “The benefits of exercise andmetabolic interventions for the prevention and early treatment of Alzheimer’s disease”, Current AlzheimerResearch, Vol. 14 No. 1, pp. 47-60.
Oriani, M., Moniz-Cook, E., Binetti, G., Zanieri, G., Frisoni, G.B., Geroldi, C., De Vreese, L.P. and Zanetti, O.(2003), “An electronic memory aid to support prospective memory in patients in the early stages ofAlzheimer’s disease: a pilot study”, Aging & Mental Health, Vol. 7 No. 1, pp. 22-7.
Pedhazur, E. and Schmelkin, L. (1991), Measurement Design and Analysis: An Integrated Approach,Psychology Press, New York, NY.
Perilli, V., Lancioni, G.E., Hoogeveen, F., Caffó, A., Singh, N.N., O’Reilly, M.F., Sigafoos, J., Cassano, G. andOliva, D. (2013), “Video prompting versus other instruction strategies for persons with Alzheimer’s disease”,American Journal of Alzheimer’s Disease and Other Dementias, Vol. 28 No. 4, pp. 393-402.
Sidani, S., Epstein, D.R., Bootzin, R.R., Moritz, P. and Miranda, J. (2009), “Assessment of preference fortreatment: Validation of a measure”, Research in Nursing & Health, Vol. 32 No. 4, pp. 419-31.
PAGE 90 j JOURNAL OF ENABLING TECHNOLOGIES j VOL. 11 NO. 3 2017

Siegel, S. and Castellan, N.J. (1988), Nonparametric Statistics for the Behavioral Sciences, 2nd ed.,McGraw-Hill, New York, NY.
Spíndola, L. and Dozzi Brucki, S.M. (2011), “Prospective memory in Alzheimer’s disease and mild cognitiveimpairment”, Dementia & Neuropsychologia, Vol. 5 No. 2, pp. 64-8.
Wang, R.H., Sudhama, A., Begum, M., Huq, R. and Mihailidis, A. (2017), “Robots to assist daily activities:Views of older adults with Alzheimer’s disease and their caregivers”, International Psychogeriatrics, Vol. 29No. 1, pp. 67-79.
Wilson, R.S., Segawa, E., Boyle, P.A., Anagnos, S.E., Hizel, L.P. and Bennett, D.A. (2012), “The naturalhistory of cognitive decline in Alzheimer’s disease”, Psychology and Aging, Vol. 27 No. 4, pp. 1008-17.
Corresponding author
Giulio Lancioni can be contacted at: [email protected]
For instructions on how to order reprints of this article, please visit our website:www.emeraldgrouppublishing.com/licensing/reprints.htmOr contact us for further details: [email protected]
VOL. 11 NO. 3 2017 j JOURNAL OF ENABLING TECHNOLOGIES j PAGE 91

Graphic symbols terminology: a call for aconsensus
Eliada Pampoulou
Abstract
Purpose – Graphic symbols, such as the Picture Communication Symbols, Makaton and Widgit, have beentraditionally used in the field of augmentative and alternative communication (AAC) in order to support peoplewith little or no functional speech. The paper aims to discuss these issues.Design/methodology/approach – However, given the fact that the terminology remains contested in theexisting literature as well as the multidisciplinary nature surrounding graphic symbols, in more recent years andthe number of terms used in different fields, it is vital that the terminology of graphic symbols is revisited again.Findings – In the last section of the paper, a definition of graphic symbols is proposed.Originality/value – The value of this paper lies in the fact that while field of graphic symbols have been usedin the AAC for more than 30 years, there is still no consensus regarding the meaning of the terminology used.
Keywords Semiotics, Definition, AAC, Graphic symbols, Manual symbols, Spoken symbols
Paper type Conceptual paper
1. Introduction
The field of augmentative and alternative communication (AAC) is concerned with a range of toolsandmethods to support people who have difficulties in communicating through verbal speech, andsymbols are one of the means that are used (Beukelman and Mirenda, 2013). The importance ofconsistent terminology has been highlighted within the AAC community for several years now, for itis argued that the lack of it can cause miscommunication and confusion among professionalsworking in the field (Lloyd and Blischak, 1992; Pampoulou, 2015). However, there is not a cleardefinition of what graphic symbols stand for, as this is a term that encompasses different types ofsymbols such as objects, miniatures, photographs, Picture Communication Symbols (PCS),Makaton, Widgit, Sclera and Mulberry symbols (Beukelman and Mirenda, 2013;Pampoulou, 2015). The focus of this paper is on those graphic symbols chosen by experts torepresent language concepts, such as Widgit, Sclera and Mulberry symbols. These symbols havebeen traditionally used in the field of AAC (Pampoulou, 2015, 2017); however, they are also found inother disciplines and, thus, it would be beneficial where a common terminology is to be establishedacross the different disciplines, including linguistics, education, speech and language therapy, AACand psychology. If this were to be achieved, then all the stakeholders involved could open upchannels of communication by referring to commonly agreed terms. Hence, the focus of this paperis to discuss the current literature pertaining to the definition of graphic symbols and to propose acommon terminology of these symbols in order to initiate a discussion towards establishing anagreed terminology that could be utilised across different disciplines. The discussion that unfolds inthe following sections is outlined in Figure 1 and it is primarily focused on the literature of semioticsand AAC, as these are the two key fields where the debates about symbols have been taking place.
2. Definition of the term “symbol” based on the AAC and semiotics fields
When discussing the terminology of symbols, it is important to refer to the literature on semioticsas this “might provide clarity and precision to AAC terminology. In order to avoid terminological
Received 24 February 2017Revised 12 May 201710 July 2017Accepted 10 July 2017
The author wishes to thank MaxHarris for his valuable commentson previous drafts of this paper.
Eliada Pampoulou is a ScientificCollaborator at the Departmentof Rehabilitation Science,Cyprus University ofTechnology, Limassol, Cyprus.
PAGE 92 j JOURNAL OF ENABLING TECHNOLOGIES j VOL. 11 NO. 3 2017, pp. 92-100, © Emerald Publishing Limited, ISSN 2398-6263 DOI 10.1108/JET-02-2017-0008

confusion, overall similarities and a few critical differences must be clarified” (Soto and Olmstead,1993, p. 137). Prior to discussing the terminology of symbols in the AAC and semiotic fields, it isimportant to refer to the etymological definition of symbols, because “being attentive to theetymological origins of words may sometimes put us in touch with an original form of life wherethe terms still had living ties to the lived experiences from which they originally sprang”(Van Manen, 1990, p. 59). Additionally, it is important to refer to the symbol definitions given inmore recent dictionaries, because “etymologies, however, do not necessarily tell the truth-or, atleast, they tell the truth, in terms of historical, not of structural, semantics” (Eco, 1984, p. 130).Whilst it is not the purpose here to refer to the definition of symbols regarding their structuralsemantic aspects, Eco’s (1984) point that etymologies refer to historical terms is important.Etymologically, the term symbol, originating from the word σύμβολον, comes from συμβάλλω, “tothrow together” (Skeat, 1958, p. 537), thus implying that it refers to “that which by custom orconvention represents something else” (Geddie, 1956, p. 117). That is, a symbol can be “a token,pledge, a sign by which one infers a thing” (Skeat, 1958, p. 537). This characteristic of asymbol as representing something else is also found in more recent dictionaries, with the OxfordConcise Dictionary, for instance, defining one as “a thing conventionally regarded as typifying,
Figure 1 Developing a common terminology for linguistic graphic symbols
EtymologiesDictionaries
Semiotics Augmentative and AlternativeCommunication
General definition
Type of relation Type of relation
Symbol definition General definition
A symbol refers to a relation that exists between a symbol and something else
A symbol is the interpretation that a person creates for the relation that existsbetween a symbol and its referent
Spoken, manual, graphic symbols
Definition of referentDefinition of referent
Symbols focused on in this paper, can be identified as iconic or symbolic signs
Symbols focused on this paper are visual, aided graphic symbols, but differ from othertypes of graphic symbols in terms of the referents they represent
The symbols focused on in this paper carry linguistic information and they have theflexibility to represent different numbers of referents. They have been created in a
systematic way in order to have the capacity to represent language (such as nouns,verbs and modifiers) as words or in phrases when used in conjunction with each other
Proposed Definition: Linguistic graphic symbols refer to the interpretation that aperson has regarding the relation that exists between a symbol and its referent. These
aided, visual symbols have been created in a systematic way in order to have thecapacity to represent language (such as nouns, verbs and modifiers) as words or
phrases, when used in conjunction with each other
VOL. 11 NO. 3 2017 j JOURNAL OF ENABLING TECHNOLOGIES j PAGE 93

representing, or recalling something, esp. an idea or quality” (Thompson, 1995, p. 1411).Regarding the definition of symbols, within the AAC field, “symbols (are) used to representobjects, actions, relationships, etc.” (Fristoe and Lloyd, 1979, p. 402; cited in Lloyd and Fuller,1986, p. 167) and a similar definition published a few years later stated that a “symbol refers toa represent-ta-tion to a referent” [sic] (Lloyd and Blischak, 1992, p. 107). Both definitions referto a relation that exists between a symbol and something else, which aligns with the definitionsgiven in dictionaries.
In the discipline of semiotics, Saussure refers to linguistic signs as the relationship between thesignifier and the signified, where the former denotes the mental concept that someone has inhis/her mind and the signified sound pattern. The nature of this relation is dependent on the socialand cultural conventions in the form of a general consensus by members of one linguisticcommunity (Chandler, 2002). According to this author, whilst for Saussure the term “sign” relatesto language, more specifically the speech (and writing) that people use in order to connect themental concept with the sound pattern (the psychological impression of a sound), the signifiedcan also take other forms, such as material items (e.g. tree or paper). As Chandler (2002,pp. 18-19) comments “The signifier is now commonly interpreted as the material (or physical)form of the sign – it is something which can be seen, heard, touched, smelled or tasted” [sic].Thus, based on Saussure’s dyadic model, the sign is the relationship that exists between thesignifier (mental concept) and the signified (acoustic pattern, materials) and symbols terms,the latter is the referent. Whilst both Saussure and Peirce refer to signs, only Peirce (1931) usesthe term symbols as part of his theory and, hence, several links with the AAC field can bemade through his theory of signs (Soto and Olmstead, 1993; Chandler, 2002).
For Peirce (1931), still within the semiotics tradition, “a sign, or representamen, is somethingwhich stands to somebody for something in some respect or capacity” (Peirce, 2.228[1]).Similarly, in the AAC definition, the symbol (the sign in semiotics) represents the referent (theobject in semiotics). At this point it would appear reasonable to contend that under bothdefinitions (AAC and semiotics) there is a dual relation, whereby the symbol (or the sign)represents something else. However, Peirce (1931) adds a third element: the interpretant which isthe “sense-making” (Chandler, 2002, p. 35) or, in other words, the idea that is evoked in the mind.This happens because: “The sign opens up the object so that it (the object) can spawn a thought”(Corrington, 1993, p. 148). Thus, the relation between the sign and the object creates aninterpretant. For Peirce, the interpretant (idea evoked, the thought) is important because:“The meaning of a sign is not contained within it, but arises in its interpretation” (Chandler, 2002,p. 35). However, the interpretant (the idea evoked in mind) depends on the “interpreter – thoughPeirce doesn’t feature that term in his triad” (Chandler, 2002, p. 35). Despite the fact that the AACsymbol definitions cited above include neither an interpretant (interpretation/ the idea evoked) noran interpreter (person who interprets), both elements (a term borrowed from Chandler, 2002) areimportant in AAC research. Accordingly, it would seem reasonable to conclude that the notion oficonicity (visual resemblance of the symbol to its referent) within AAC parallels the interpretant andthe interpreter perspectives under semiotics and, hence, this information needs to be included inthe AAC symbols definition. In particular, the literature surrounding iconicity focuses on aperson’s previous experiences with symbols, among other things (Sevcik et al., 1991).Consequently, it would be reasonable to contend that a symbol is the interpretation that a personcreates for the relation that exists between a symbol and its referent.
It is also important to consider Peirce’s (1931) second triad of signs with the type of symbols that existin the AAC field; first, because he does refer to symbols, albeit this term carries a different meaningfrom that assigned in the AAC field. Second, the three types of signs are related to the type ofsymbols that the AAC community focuses upon, although using a different terminology. Third, it is inaccordance with Venkatagiri’s (2002) perspective that the discussion of icons, symbols and signs“can provide a framework for clinical decisions and choices related to AAC” (Venkatagiri, 2002, p. 45).Peirce’s (1931) second triad of signs is based on the relation that exists between the sign and theobject, where the former can be icons, indices or symbols (Soto and Olmstead, 1993). An icon is asign that represents an object, “mainly by its similarity” (Peirce, 2.276), through physicalcharacteristics, such as colour, shape, texture, smell, sound, or even a functional relationship to itsobject (such as a picture or photograph of a fire to denote hot). Regarding the type of graphic
PAGE 94 j JOURNAL OF ENABLING TECHNOLOGIES j VOL. 11 NO. 3 2017

symbols that I focus on in this paper, they frequently bear physical resemblance to what theyrepresent in terms their colour, shape and/or size. Actually, Venkatagiri (2002) specifically refers toRebus, Picsym and PCS symbols as icons. Beukelman and Mirenda (2013) categorise the symbolsas pictorial symbols, which can infer that they share the same qualities as those in pictures, suchas the physical resemblance of objects. As explained earlier, in semiotics pictures are identified asicons. An important characteristic of icons and, thus, AAC symbols is that “the association of iconswith their referents requires some learning” (Venkatagiri, 2002, p. 51). Nevertheless, “the meaning ofan icon is inherent in the icon itself; accordingly, its acquisition usually requires a minimal amount oflearning” (Venkatagiri, 2002, p. 51). The learnability of icons is in fact directly related to thewell-researched topic of iconicity (Venkatagiri, 2002).
In the AAC literature, “iconicity refers to the visual relationship of a symbol to its referent. Whilesome symbols have little or no visual resemblance to their referents, others are very close visualapproximations” (Fuller and Lloyd, 1991, p. 216). Transparent symbols have a strong visualresemblance to their referents and for this reason the observer is able to understand therelationship between the symbols and their referents, even if the object is not present, for,as indicated in the literature, “transparency implies guessability” (Fuller, 1997, p. 30). Similarly,Venkatagiri (2002) states that transparent icons are those “that are intuitively meaningful, becausethey look, sound, or otherwise closely resemble the referent they signify (e.g. a picture of a sun isused to represent the sun)” (Venkatagiri, 2002, p. 48). In relation to AAC graphic symbols, thesecan be those that represent concrete vocabulary, such as an apple or a chair. Based on theiconicity literature, translucent symbols fall between transparent and opaque ones (Fuller, 1997).In such cases, the relationship between the symbol and referent can be understood when bothare presented together, because the person can understand the relation that exists betweenthem (Fuller, 1997). Sevcik et al. (1991, p. 164) point out that “the relationship between the symboland its referent is revealed through some form of instruction”.
Opaque symbols have no visual relationship between the symbol and the referent even whenboth are presented together (Fuller and Lloyd, 1991; Sevcik et al., 1991). This arbitrary relationbetween a symbol and its referent is also found in Peirce’s (1931) discussion of symbolic signsin which he states that the relation between the sign and its object is based on conventional laws.As indicated above, one example is natural languages, which are manifested in both verbal(such as spoken speech) and written (such as traditional orthography) forms, with a personneeding to learn the relation that exists between the symbolic signs and their objects. FindingsfromMirenda and Locke (1989) illustrate this relationship. These scholars explored the iconicity ofdifferent types of symbols in 40 subjects with various types of disabilities (cognitive, social andcommunication), who had no functional speech and their results showed that the least opaquesymbols were Blissymbols and traditional orthography. Peirce (1931) defines traditionalorthography as symbolic signs, whilst Venkatagiri (2002) terms Blissymbols as such and basedon this information it is contended that opaque symbols (based on iconicity as in AAC) can beregarded as being equivalent to symbolic signs (in semiotic terms).
Continuing the discussion about Peirce’s triadic taxonomy (icons, symbols and indices), indicesare not related to graphic symbols and, hence, are outside of the scope of this paper. This isbecause an indexic sign has an inseparable relation (direct, causal or real) to its object and, thus, itis impossible for an index to exist without that object (Goudge, 1969). An example to illustrate thispoint is the bullet hole as an index of the passage of a bullet (Soto and Olmstead, 1993).According to Venkatagiri (2002), in AAC, indices can be, for instance, related to different reflexivevocalisations, such as cries, babbling, and moans; facial expressions such as a smile; and bodyposture, such as being slumped. In regard to the third type of signs, “a symbol is arepresentamen whose representative character consists precisely in its being a rule that willdetermine its interpretant” (Peirce, 2.292). In other words, the relationship between therepresentamen (sign) and the object is arbitrary, without any natural relation and, therefore, theassociation depends on the virtue of a law, habit or convention (Peirce, 1931; Silverman, 1983;Chandler, 2002). Natural languages (including the traditional orthography) and notational systemsare entirely symbolic (Peirce, 1931). In the field of AAC, for Venkatagiri (2002), symbolic signs canbe some of the graphic symbols in Blissymbols. This is because the Blissymbol system isgoverned by rules, which when put in practice can allow the person to combine different symbols
VOL. 11 NO. 3 2017 j JOURNAL OF ENABLING TECHNOLOGIES j PAGE 95

in order to create a new meaning (Smith, 2006). However, even within this collection “a smallnumber of Blissymbols are icons” as there is a physical resemblance between the symbol and thereferent (Venkatagiri, 2002, p. 49). Consequently, based on Peirce’s triadic taxonomy, thegraphic symbols focused on in this paper can be identified as iconic signs (such as the PCS set)or symbolic signs (such as Blissymbols).
2.1 Spoken, manual and graphic symbols
In order to clarify the definition of graphic symbols within the AAC field, it is vital to distinguish thesefrom spoken and manual symbols and, accordingly, it is important that “the type of symbol shouldalways be specified to avoid confusion” (Lloyd and Blischak, 1992, p. 107). One of the maindifferences between the three types of symbols is the modality through which they areimplemented, that is, “while spoken symbols are conveyed through the auditory-vocal modality,graphic and manual symbols are conveyed through the visual modality” (Fristoe and Lloyd, 1979,cited in Lloyd and Fuller, 1986, p. 167). Despite the fact that both manual and graphic symbols areconveyed through the visual modality they differ in terms of the demands needed for theirproduction. Specifically, whilst manual symbols (such as gestures, eye blinking and sign language)do not require anything additional from the person’s body for the meaning to be conveyed, in thecase of graphic symbols (such as photographs, pictures, PCS and Makaton symbols) these needto be deployed on flashcards, printed communication books or communication devices.
One example of spoken symbols is natural speech (Lloyd, 1985), which is conveyed through thevocal modality. One of the differences between spoken symbols and graphic ones is that theformer are segmentable, because “a restricted set of meaningless segments are capable ofmultiple combinatorial possibilities yielding new linguistic signs” (Smith, 2006, p. 152).For instance, the combination of the phonemes “p”, “o”, and “t” can give two new linguisticsigns “pot” and “top”, whereas the combination of more phonemes can increase the number ofcombinatorial possibilities so that new linguistic signs can be produced. Conversely, graphicsymbols “vary in their potential for segmentation” (Smith, 2006). One collection of symbols thathas the flexibility of segmentation and, thus, can produce new meanings is Blissymbols, as it is astructured system through which, when the rules are learnt, the user can create an infinite numberof messages (Bliss, 1965; Jones and Cregan, 1986; Smith, 2006). On similar lines, Minspeaksymbols are used semantically in order to allow the person to create meanings for the purposesof communicating with others (Mathisen et al., 2009). In other collections of graphic symbols, thissegmentation is not present. For instance, PCS has a fixed number of symbols and there are norules that can allow the creation of new ones (Smith, 2006). Hence, it can be argued that spokenand graphic symbols are not equivalent because flexible segmentation is not usually present withthe latter. Furthermore, spoken symbols differ from graphic ones in that a relationship existsbetween the former and its referent. Spoken symbols “exist in an arbitrary relationship with theirreferents; these sign-meaning relationships are consistent and unique” (Smith, 2006, p. 152).This point is further discussed in the last section of the paper.
Turning to graphic symbols, these are aided symbols, whereby some additional inputs areneeded in order for the person to convey the intended meaning. These can include real objects,photographs, pictures, traditional orthography, and graphic symbols, such as those of MakatonandWidgit (Fuller et al., 1997; Beukelman and Mirenda, 2005). Fuller et al. (1997, p. 49) created atable in which they classified graphic symbols based on their functional similarities into differentcategories. Among others, they make the distinction between “Primarily picture-based symbolswithout linguistic characteristics” and “Partially picture-based symbols with linguisticcharacteristics”. Whilst these scholars do not provide any explanation of what they mean by“picture-based symbols”, it could be interpreted that this is related to the degree to which oneaided symbol links to the functions of a picture. That is, there are those symbols that have closelinks to the functions of the pictures (such as photographs and PCS) and those that have partiallypicture-based relations (such as PICSYMS and Blissymbol). Additionally, it can be argued thatwhether symbols are partially or wholly picture based is related to their iconicity. This is becauseiconicity pertains to the degree to which one symbol resembles its referent. Regarding this,findings by Mirenda and Locke (1989) show that the most iconic aided symbols are objects orcolour photographs, whereas the least are Blissymbols and traditional orthography.
PAGE 96 j JOURNAL OF ENABLING TECHNOLOGIES j VOL. 11 NO. 3 2017

In a more recent publication about categorising the different aided symbols, Beukelman andMirenda (2013) divide them into four broad categories: “tangible symbols” (such as real andminiature objects), “representational symbols” (photographs and line-drawing symbols, such asPCS), “abstract symbol systems” (such as the Yerkish lexigrams) and “orthography andorthographic symbols” (such as Braille and word codes). Of particular interest for this research isthat these authors include photographs and graphic symbols in the same category(“representational symbols”). In regard to the type of symbols this paper is focused on,Beukelman and Mirenda (2013) refer to these as “representational symbols” and once again theirrepresentation element is illustrated (as in AAC and semiotics definitions, as discussed in the firstsection). Additionally, a distinction is made based on the design, such as for instance PCS andMakaton being designed as line-drawings and, thus, they differ in terms of design from “tangiblesymbols” (such as real and miniature objects). This is an important element to consider whenfocusing on a graphic symbols definition in that they have been purposively designed by expertsto represent language for different fields, such as AAC and education (Pampoulou, 2015).
In this paper, it is also vital to consider pictograms. This is because the graphic symbols(e.g. Mulberry, SymbolStix and PCS) discussed are often labelled as such by different stakeholders,including symbol developers, AAC specialists and special educators (Pampoulou, 2015). In addition,the term pictograms is already used in one of the existing graphic symbols sets. That is, Pictogramsis a Swedish set that was purposively drawn to include white-on-black symbols so as to reduce thediscrimination of the figure-ground. Regarding the definition of pictograms, according to ChambersDictionary a pictograph (defined as the same as a pictogram) is “a picture used as a symbol for aword or phrase; a pictorial representation of values, statistics etc.” It can be argued that this definitionaligns with those discussed in the first section of this paper based on the semiotics and AAC fields,as symbols are the representation of something else. However, as has been discussed in thissection, the graphic symbols this paper is focused on are not just pictures, for they can be also takethe form of line-drawings (e.g. PCS, Makaton and Widgit), albeit it can be argued that both picturesand line-drawings represent something else. It is contended here that a common terminologyis needed to refer to all different collections of symbols (such as PCS, Widgit, Sclera , etc.) and thus,it is important to decide whether to use the terms pictograms, graphic symbols or an alternativeoption, if it is deemed the most appropriate.
3. Definition of referents
Turning to the definition of referents, these are the symbols representations, such that a “symbolrefers to a re-present-ta-tion to a referent” [sic] (Lloyd and Blischak, 1992, p. 107), where thesecan be objects, actions and relationships, amongst others (Lloyd, 1985). However, in the AACfield, apart from the above information, there is no direct explanation regarding the meaning ofreferents. Even within an article entitled “AAC terminology policy and issues update” there is lackof information about what the term referent means (Lloyd and Blischak, 1992). One reason for thiscould be due to the different types of symbols that exist within the AAC community. For instance,in relation to spoken symbols, the referent can be either individual phonemes or words, whereasfor manual ones it can be a sign (here the term refers to sign language and not to the definitiongiven in semiotics) represented by words or letters. Nevertheless, it can be argued that if “we usethe term symbol to reflect to some form of representation level, we have automatically infused averbal component to it” (Blau, 1987, p. 98). For instance, Vinson (2001) proposed thatphotographs can be used as symbols for nouns, albeit the representation is not as effective forverbs and modifiers. In contrast, because graphic symbols are line-drawings in which arrows areused and different rules are deployed to convey the meaning, these can be more effectivesymbols for representing certain linguistic information.
Smith (2006) focused on the linguistic relation between spoken and graphic symbols withtheir referents:
[…] language users evolve and retain a consistent relationship between words and their meanings-aone-word, one-meaning approach. Such relationships are essential for mutual intelligibility.By contrast, flexibility in interpretation of graphic symbols may be an important element in the efficientuse of aided communication [21, 22]. Given the vocabulary constraints implicit in communication boards
VOL. 11 NO. 3 2017 j JOURNAL OF ENABLING TECHNOLOGIES j PAGE 97

for example, efficient communication may require the use of the same symbol to represent multiplemeanings. DRINKmay represent “I am thirsty; milk please; more 7UP; juice; I’d love a coffee; it’s been ahard day” or may even refer to a TV sitcom, Father Ted (Smith, 2006, p. 153).
The author supported the perspective that in spoken symbols there is a “one-word, one-meaningapproach” in order for both communicative partners to understand mutually what is said. Regardinggraphic symbols, for Smith (2006), a single one can represent a number of referents, especially whenthere is the communication need to use one graphic symbol (such as DRINK) to represent a numberof different referents (such as “I am thirsty; milk please”). Another possible example is the graphicsymbol for LIBRARY, which can evoke a number of referents, such as lots of books, study, studentand reading. Hence, one graphic symbol is capable of representing a number of different referents,not simply one. It is vital here to refer back to the first section of the paper and focus on Peirce’s(1931) definition about signs and, in particular, on the importance of the interpretant (idea evoked inmind), which is dependable on the interpreter. Hence, it can be argued that the referent in AAC is theidea evoked in mind, i.e., the “sense-making” of an individual regarding the relationship that existsbetween the symbol and the object. Additionally, it can also be the concept (mental idea) thatinstructors teach the person to learn for a specific symbol. For instance, the Pragmatic OrganisationDynamic Display books contain a set of graphic symbols (the size of the symbols varies dependingon the person’s skills), which are learned and used for communication purposes initially throughsystematic receptive language input (Porter, personal communication). In sum, it can be argued thatgraphic symbols are flexible in terms of the number of referents that they represent depending uponthe interpretant and/or instructor’s understanding and goals.
4. Operational definition
Based on the discussion above, an operational definition of the type of graphic symbols(e.g. Makaton, Mulberry and Sclera) discussed in this paper is provided as a template for future work:
Linguistic graphic symbols refer to the interpretation that a person has for the relation that existsbetween a symbol and its referent. These aided visual symbols have been created in a systematic wayin order to have the capacity to represent language (such as nouns, verbs and modifiers) as words orphrases, when used in conjunction with each other.
In particular, the relation that exists between the symbol and its referent depends on theinterpretation that is created between the two. Most of these symbols lack the segmentationability that characterises natural speech. However, they have the flexibility to represent a variety ofconcepts depending upon the chosen link created between the symbol and its referent. Thesesymbols have been mainly designed by companies and charities and they often encompassedspecific rules in order to meet the needs of individuals who can benefit from their deployment.
5. Conclusions
The importance of consistent terminology has been highlighted within the AAC community forseveral years now, for it is argued that the lack of it can cause miscommunication and confusionamong professionals working in this and other fields (Lloyd and Blischak, 1992; Fuller et al., 1992;Pampoulou, 2015). This led to the writing of this paper aimed at developing an operationaldefinition in order to contribute to the existing literature as well as to support practice.
Focusing, first, on academia, the current work has the objective of initiating a discussion on this topicthat can bring together different disciplines on a discussion board aimed at developing a commonterminology when referring to the type of symbols that form the subject of this paper. This can,subsequently, lead to a more in-depth discussion about the characteristics of these symbols by alsotaking account of the constant and rapid advancement of technology. Hence, it is proposed that aworking group (scholars and practitioners from different disciplines) be formedwithin the appropriateprofessional organisation, for example, the International Society of Augmentative and AlternativeCommunication. The working group would develop a glossary of standardised terms andcharacteristics of symbols, which would then be disseminated through different activities (such aspublications, conferences and workshops) and in this way all the interested stakeholders would beinformed about a common terminology that should be used across different disciplines.
PAGE 98 j JOURNAL OF ENABLING TECHNOLOGIES j VOL. 11 NO. 3 2017

Shifting the focus to practice, the current work aims to stimulate the debate about defining linguisticgraphic symbols amongst all interested stakeholders, including practitioners (e.g. speech andlanguage therapists and teachers), carers (e.g. parents) and symbol developers. To this end, theworking definition provided above as a result of the prior discussion, it is believed, can provide auseful starting point for such a debate. In addition, it is important to disseminate the notion thatwhilst other types of graphic symbols (e.g. photographs and pictures) are capable of representingparts of language, albeit, mainly nouns, linguistic graphic symbols can do so in a moresophisticated way than other symbol types. Specifically, they can represent language either asindividual meanings (represent one word or a phrase) or in compounded ones (when these symbolsare put together in a sentence). Additionally, some of these linguistic graphic symbol sets havesegmentation ability that is always present in spoken symbols, but not found in other graphicsymbols (e.g. objects). The provided operational definition has the purpose of highlighting that therelationship between the symbol and its referent is based on the individual’s interpretation or that ofthe instructor or even a combination of the two. Despite the fact that this work in this paper and,hence, the operational definition, is based on the well-established fields of semiotics and AAC,morework is needed in developing a common terminology amongst the different disciplines.
Note
1. In this paper, I follow the quoting system that many scholars use when referring to Peirce’s (1931) work.Specifically, the first digit refers to the number of the Volume (book) of the Collected Papers of CharlesSanders Peirce and the digits after the dot indicate the page number on which that the quotation canbe found.
References
Beukelman, D.R. and Mirenda, P. (2005), Augmentative and Alternative Communication: Supporting Childrenand Adults with Complex Communication Needs, 3rd ed., Paul H. Brookes Publishing Co., Baltimore, MD.
Beukelman, D.R. and Mirenda, P. (2013), Augmentative and Alternative Communication: Supporting Childrenand Adults with Complex Communication Needs, 4th ed., Paul H. Brookes Publishing Co, Baltimore, MD.
Blau, A.F. (1987), “A response to Lloyd and Fuller: toward an augmentative and alternative communicationsymbol taxonomy: a proposed superordinate classification”, Augmentative and Alternative Communication,Vol. 3 No. 2, pp. 97-9.
Bliss, C.K. (1965), Semantography (Blissymbolics) A Simple System of 100 Logical Pictorial Symbols,Which Can be Operated and Read like 1+ 2¼3 in all Languages, Semantography (Blissymbolics)Publications, Sydney.
Chandler, D. (2002), Semiotics: The Basics, Routledge, London and New York, NY.
Corrington, R.S. (1993), An introduction to C.S. Peirce Philosopher, Semiotician, and Ecstatic Naturalist,Rowman and Littlefield, Michigan, MD.
Eco, U. (1984), Semiotics and the Philosophy of Language, Macmillan, London.
Fristoe, M. and Lloyd, L.L. (1979), “Nonspeech communication”, in Ellis, N.R. (Ed.), Handbook of mentaldeficiency: Psychological theory and research, 2nd ed., Lawrence Erlbaum Associates, New York, NY,pp. 401-430.
Fuller, D. (1997), “Initial study into the effects of translucency and complexity on the learning of blissymbols bychildren and adults with normal cognitive abilities”, Augmentative and Alternative Communication, Vol. 13No. 1, pp. 30-9.
Fuller, D.R. and Lloyd, L.L. (1991), “Toward a common usage of iconicity terminology”, Augmentative andAlternative Communication, Vol. 7 No. 3, pp. 215-20.
Fuller, D.R., Lloyd, L.L. and Schlosser, R.W. (1992), “Further development of an augmentative andalternative communication symbol taxonomy”, Augmentative and Alternative Communication, Vol. 8 No. 1,pp. 67-74.
Fuller, D.R., Lloyd, L.L. and Stratton, M. (1997), “Aided AAC symbols”, in Lloyd, L.L., Fuller, D. and Arvidson, H.(Eds), Augmentative and Alternative Communication: Handbook of Principles and Practice, Allyn and Bacon,Needham Heights, MA, pp. 48-79.
VOL. 11 NO. 3 2017 j JOURNAL OF ENABLING TECHNOLOGIES j PAGE 99

Geddie, W. (1956), Chambers’s Twentieth Century Dictionary, W.&R. Chambers, Edinburgh.
Goudge, T.A. (1969), The Thought of C.S. Peirce, University of Toronto Press, Toronto.
Jones, P.R. and Cregan, A. (1986), Sign and Symbol Communication for Mentally Handicapped People,Croom Helm, London and Dover.
Lloyd, L.L. (1985), “Comments on terminology”, Augmentative and Alternative Communication, Vol. 1 No. 3,pp. 95-97.
Lloyd, L.L. and Blischak, D.M. (1992), “AAC terminology policy and issues update”, Augmentative andAlternative Communication, Vol. 8 No. 2, pp. 104-9.
Lloyd, L.L. and Fuller, D.R. (1986), “Toward an augmentative and alternative communication symboltaxonomy: a proposed superordinate classification”, Augmentative and Alternative Communication, Vol. 2No. 4, pp. 165-71.
Mathisen, B., Arthur-Kelly, M., Kidd, J. and Nissen, C. (2009), “Using MINSPEAK: A case study of a preschoolchild with complex communication needs”, Disability and Rehabilitation: Assistive Technology, Vol. 4 No. 5,pp. 376-83.
Mirenda, P. and Locke, P.A. (1989), “A comparison of symbol transparency in nonspeaking persons withintellectual disabilities”, Journal of Speech and Hearing Disorders, Vol. 54 No. 2, pp. 131-40.
Pampoulou, E. (2015), “The use of graphic symbols in inclusive primary schools an exploration of teachers’and speech and language therapists’ experiences of graphic symbols”, unpublished thesis, King’s CollegeLondon, London.
Pampoulou, E. (2017), “Exploring speech and language therapists and teachers’ experiences when choosinggraphic symbol set(s) for their students in inclusive primary schools in England and Cyprus”, Journal ofEnabling Technologies, Vol. 11 No. 2, pp. 49-58.
Peirce, C.S. (1931), in Hartshome, C., Weiss, P. and Burks, A.W. (Eds), Collected Papers of Charles SandresPeirce, Vol. II, Harvard University Press, Cambridge, MA.
Sevcik, R.A., Romski, M.A. and Wilkinson, K.M. (1991), “Roles of graphic symbols in the language acquisitionprocess for persons with severe cognitive disabilities”, Augmentative and Alternative Communication, Vol. 7No. 3, pp. 161-70.
Silverman, K. (1983), The Subject of Semiotics, Oxford University Press, New York, NY.
Skeat, W.W. (1958), An Etymological Dictionary of the English language, Clarendon Press, Oxford.
Smith, M. (2006), “Speech, language and aided communication: connections and questions in adevelopmental context”, Disability and Rehabilitation, Vol. 28 No. 3, pp. 151-7.
Soto, G. and Olmstead, W. (1993), “A semiotic perspective for AAC”, Augmentative and AlternativeCommunication, Vol. 9 No. 2, pp. 134-41.
Thompson, D. (1995), The Concise Oxford Dictionary (Edited by Della Thompson), Oxford University Press,Oxford.
Van Manen, M. (1990), Researching Lived Experience: Human Science for an Action Sensitive Pedagogy,Althouse Press, London.
Venkatagiri, H.S. (2002), “Clinical implications of an augmentative and alternative communication taxonomy”,Augmentative and Alternative Communication, Vol. 18 No. 1, pp. 45-57.
Vinson, B.P. (2001), Essentials for Speech-Language Pathologists, Singular Thomson Learning, Albany, NY.
Corresponding author
Eliada Pampoulou can be contacted at: [email protected]
For instructions on how to order reprints of this article, please visit our website:www.emeraldgrouppublishing.com/licensing/reprints.htmOr contact us for further details: [email protected]
PAGE 100 j JOURNAL OF ENABLING TECHNOLOGIES j VOL. 11 NO. 3 2017

Augmentative and alternativecommunication (AAC) trainingprovision for professionals in England
Samantha Wallis, Steven Bloch and Michael Clarke
Abstract
Purpose – The purpose of this paper is to document augmentative and alternative communication (AAC)training provision by clinical services in England.Design/methodology/approach – A questionnaire was used to obtain the following information concerningAAC training provision; frequency, length, type, content and cost, trainee occupations and numbers, andfuture training priorities, and information concerning training providers – service type, geographical area.Findings – In total, 98 clinical service training providers in England responded. Services commonly reportedproviding AAC training to speech and language therapists, teaching assistants and teachers. Training around“use of specific AAC products, systems and technology” and “introducing/awareness raising of AAC products”were rated as high priority for future training and were two of the three subject areas where services reportedthe highest percentage of training. Training was predominantly provided at a foundation (basic) level.Originality/value – There is no consensus on the amount or content of AAC training which professionals inEngland must receive. Evidence suggests that AAC training for pre-qualification professionals is limited andthis paper has identified variation in the amount and type of post-qualification AAC training. While knowledgeconcerning specific AAC systems is necessary, focussing training primarily on this area may not addresscritical gaps in knowledge. There is a need for specific recommendations regarding AAC training forprofessionals in this field, to ensure professionals can fully support people who use AAC.
Keywords Training, Survey, Augmentative and alternative communication,Continuing professional development, International classification of functioning, disability and health, Therapists
Paper type Research paper
1. Introduction
Augmentative and alternative communication (AAC) refers to communication methods that eithersupplement or substitute an individual’s speech and/or writing (Clarke et al., 2016). These maybe unaided (such as the use of manual signs) or aided (involving the use of communicationdevices external to the body, such as communication aid technologies). AAC strategies andtools are part of a fluid, multi-modal repertoire of resources that are used in every daycommunication interactions. It is estimated that approximately 0.5 per cent of the population ofEngland requires AAC intervention (Communication Champion, 2011; Creer et al., 2016).
The importance of AAC to the lives of children and adults is reflected through current educationand healthcare funding and service delivery guidelines in England and Wales (Department forEducation, 2013; National Institute for Health and Care Excellence, 2016), through the reportedexperiences of people using AAC (Clarke and McConachie, 2001) and a growing body of researchevidence (Light and McNaughton, 2012; Ganz, 2015). Consequently, there is an increasingrequirement for professionals to maintain and enhance their knowledge and skills in supportingpeople using AAC. During the last 20 years there has been a marked growth in the diversity of AACtechnology, partly due to the rapid expansion and adaptation of mainstream technologies, andongoing developments in specialist technologies (Communication Matters, 2012).
Received 16 October 2016Revised 30 March 201720 June 2017Accepted 21 June 2017
The questionnaire data collectiontook place as part of aDepartment for Education-fundedAAC Grant (2012-2013) toproduce proposals for a model offuture AAC service provision.The data presented in the presentpaper are that collected forobjective 8 of the AAC Grantprogramme; “National AACTraining and Learning”.
Samantha Wallis is a SpecialistSpeech and LanguageTherapist and Steven Blochand Michael Clarke are SeniorLecturers, all at UniversityCollege London, London, UK.
DOI 10.1108/JET-10-2016-0023 VOL. 11 NO. 3 2017, pp. 101-112, © Emerald Publishing Limited, ISSN 2398-6263 j JOURNAL OF ENABLING TECHNOLOGIES j PAGE 101

1.1 Training need
In the UK, policy and research recommendations for AAC frequently reference the needfor training of professionals as a component of their continuing professional development(Enderby et al., 2013; Communication Champion, 2010). Specific training for professionalsworking with children with severe/complex speech, language and communication needs is alsowidely recommended (Department for Children, Schools and Families, 2008). More widely,professionals and parents have reported that training contributes to positive outcomes for AACusers (Soto et al., 2001). For example, in a survey of AAC users and family members, training forfamilies and teachers was identified as a critical factor facilitating positive outcomes in AACsystem use (Lund and Light, 2007). McMillan (2008) has also reported that AAC training forteachers was associated with positive outcomes for students using AAC. McMillian documentedan increased rate of initiation using AAC and generalisation and maintenance of AAC device usefor two months post-training.
The shift to supporting children with special educational needs in mainstream schoolshas increased the proportion of professionals likely to encounter children who use AAC(Matthews, 2001). Speech and language therapists (SLTs) are often key in managingAAC system use, however, in a survey of 320 SLTs, Matthews (2001) found that only 57 per centof therapists in the UK had received undergraduate training in AAC. Additionally, most SLTsclassified their knowledge in supporting AAC technologies as either “none” (31 per cent) or“general knowledge/awareness” (37 per cent). It is reported that UK SLT undergraduatestypically receive only six to ten hours of AAC training (Communication Champion, 2010).This suggests a high and growing level of need for post-qualification training.
1.2 Current training recommendations
A range of recommendations have beenmade on UK provision of AAC services (Enderby et al., 2013;Communication Champion, 2010; Communication Matters, 2012). As yet, no consensusexists for the amount, delivery mode and content of AAC training for professionals.Recommendations by the Royal College of Speech and Language Therapists (RCSLT, 2011)focus primarily on training in relation to supporting AAC technology use. Enderby et al. (2013)explored the theme of AAC training, suggesting that training concentrates on “AAC strategies,research and practice; AAC systems, methods and techniques and how to access and implementthem; AAC equipment and potential customisation and access options; and how to use and preparethe equipment for use” (p. 76). Similarly, Communication Matters (2012), the UK chapter of theInternational Society for AAC highlighted the need to train professionals on software, hardware,vocabulary and communication strategies.
Others have recommended training on enhancing the AAC user’s communicative environment.Costigan and Light (2010) discussed a need to train professionals in supporting the widerrange of participatory skills needed by an AAC user. They recommended that pre-qualificationAAC training should develop professional skills in areas including assessment, intervention, AACsymbols and systems, cultural competence, problem-solving and collaborative skills, highlightinga likely need to train professionals in areas of AAC support beyond the operational knowledge ofAAC technologies.
Recognition of the potential benefits of specifying aspects of training need is seen in thedevelopment of a framework for informing and profiling AAC knowledge and skills in staff acrosshealth, education and social services (IPAACKS; NHS Education for Scotland, 2014). Developed inScotland, this framework was developed through review of relevant literature and consultation withkey stakeholders including people with AAC. It outlines core values that should underpin the workof those supporting people who use AAC, and provides information on competency levels for staffacross four skill levels, within eight skills areas, two of which focus on issues related to AACtechnology (e.g. AAC technology preparation, adaption and implementation; AAC technologymanagement of resources). The authors suggest that this broad-based framework can be used byindividuals and/or organisations to appraise and monitor staff skills sets. Another approach toframing the scope of AAC training is the World Health Organisation’s International Classification ofFunctioning, Disability and Health (ICF; World Health Organisation, 2001). The ICF has been used
PAGE 102 j JOURNAL OF ENABLING TECHNOLOGIES j VOL. 11 NO. 3 2017

widely to assess communication difficulties and their impact on daily life for people using AAC(Clarke et al., 2012; Price and Clarke, 2011; Threats and Worrall, 2004). This biopsychosocialmodel has been applied to many aspects of communication impairment and examines theinteractions between an individual’s health conditions, body functions and structures, activities andparticipation. Furthermore, it considers environmental and personal factors that may influence anindividual (World Health Organisation (WHO) 2001).
More recently, the International Classification of Functioning, Disability and Health – Children andYouth Version (ICF-CY;WHO, 2007) has been used as a framework for assessment of children andyoung people who use AAC (Rowland et al., 2012; Clarke et al., 2012; Griffiths and Price, 2011).Rowland et al. proposed that using the ICF-CY in the AAC field may encourage professionalsworking in AAC to consider a wider range of environmental factors that influence youngcommunicators, as well as the functional communication skills needed for activity and participation.The ICF has also been used to frame recommendations for training provision in AAC, computeraccess and environmental control, reflecting multiple issues in effective support for AAC usersbeyond knowledge of AAC devices themselves (Gresswell and Hoogerwerf, 2007).
1.3 Summary and research question
There is a lack of consensus on the quantity or content of AAC training for professionals workingwith people using AAC. Consequently, there is a risk that needs may not be understood or fullymet. Evidence suggests that AAC training for pre-qualification professionals is limited and there isno information on the content or quantity of AAC post-qualification training delivered forprofessionals across England. This paper therefore sought to address the following question:what is the current overview of AAC training provision in England?
2. Methodology
2.1 Questionnaire measure
The questionnaire was developed through expert consensus in the research team anda stakeholder focus group, comprising service users, service providers, suppliers and aservice commissioner. It was then piloted with four clinical AAC services and adaptedin response to feedback from this group. This method was chosen because it enabled alarge number of organisations to respond promptly and allowed national data to be collectedeasily and accurately.
The survey comprised two sections: information concerning AAC training provision – trainingfrequency, length, type, content and cost, trainee occupations and numbers and future trainingpriorities, and information concerning the survey respondents – service type, geographical area.Responses were made largely via closed multiple choice or rating scales, to enable comparisonbetween responses. Areas of training content presented in multiple choice options reflected theICF framework’s domains. The first author linked the training content with ICF categories andestablished 71 per cent agreement with the other researchers, with 100 per cent agreementfollowing further discussion. A copy of the questionnaire is available from the authors on request.
2.2 Procedure
Participants were identified via Communication Matters charity specialist AAC provider database,and from the national AAC service database concurrently being developed under the auspices ofthe Department for Education-funded AAC Grants Project (2012-2013), which aimed to locateand survey all services providing AAC in England. An invitation to engage in the study wase-mailed to all services identified and a series of reminders were sent. Participants were directedto the online survey, which was open for eight weeks. Data were anonymised as appropriate andstored securely. Participants were informed that completing the questionnaire gave consent forstorage of responses by submitting the survey. Ethical review for the project was sought from theuniversity ethics board. The ethics board advised that, given the methods involved in the study,review was not required because the study involved no change to standard clinical service.
VOL. 11 NO. 3 2017 j JOURNAL OF ENABLING TECHNOLOGIES j PAGE 103

2.3 Participants
The questionnaire was sent to 187 service providers in England. Responses were received from98 clinical services. Commercial AAC services, independent AAC services and higher educationinstitutes were also invited to engage in the study. The responses provided by theseorganisations are not contained within this paper.
2.4 Data Analysis
All questionnaire responses were collated and stored directly in a SurveyMonkeyTM database.The questionnaire data were transferred to Microsoft Excel for quantitative and qualitativeanalysis. Free text entries were analysed by the research team. Key issues identified werecompared in order to agree final themes. While prevalence of need for AAC in the UK is estimatedat 0.5 per cent, accurate information is not available for the actual population currently served byAAC services. Therefore, an a priori assumption was made that that need for training is broadlyequivalent across regions.
3. Results
3.1 Respondent demographics
In total, 98 clinical service training providers in England responded to the survey, including NHS,education and charities providing established clinical services (n¼ 98; adult services¼ 38 per cent;paediatric services¼ 48 per cent, combined adult and paediatric services¼ 13 per cent;unspecified¼ 1 per cent).
Table I shows the geographical distribution of responses across the ten specialisedcommissioning hub (SCH) regions in England. The survey received responses from eachregion, however, the number of services represented in each SCH region varies.
Clinical services classified the reach of their service as local, regional or national (local¼ 51 per cent,regional¼ 11 per cent, national¼ 6 per cent, other/unspecified¼ 32 per cent). Where respondentsclassified their service reach at more than one level, the widest reach level only was recorded.
Services predominantly delivered AAC training to professionals in their own service or regionalcatchment area only (only professionals within the service/organisation¼ 36 per cent, onlyprofessionals within the regional catchment area¼ 38 per cent, professionals from anywhere¼9 per cent, other¼ 7 per cent, no response¼ 10 per cent).
The distribution of training to specific professional groups is shown in Table II. The four mostcommonly trained professional groups for each subgroup of clinical services are highlighted.
Table I Geographical distribution of responses across the ten specialised commissioninghub (SCH) regions in England
Specialised commissioning hub (SCH) regions in England Number of responding services
East Midlands 5East of England 6London 19North East, North Cumbria and the Hambleton and Richmondshiredistricts of North Yorkshire 4North West 6South East Coast 7South West 16Thames Valley and Wessex 9West Midlands 9Yorkshire and the Humber 12All of England 5Total 98
PAGE 104 j JOURNAL OF ENABLING TECHNOLOGIES j VOL. 11 NO. 3 2017

Over half of the responding clinical services delivered training to SLTs, teaching assistantsand teachers, with 95 per cent of paediatric clinical services delivering training toteaching assistants. Over a third of clinical services for adults provided training to nurses;a smaller proportion of paediatric services trained this population (34 per cent of adult services,7 per cent of paediatric services). A fifth or less of the responding clinical servicesdelivered training to nurses, physiotherapists, managers, clinical technicians, socialworkers, psychologists, commissioners or doctors, with just 6 per cent of total servicestraining doctors.
3.2 AAC training content
The proportion of training delivered by service providers in each specified contenttopic are shown in Table III, in order of percentage response from high to low. The mostcommon area of training concerned use of specific AAC products, systems andtechnologies (27 per cent), although the proportion of training delivered on this topic variednotably across the sample (range 0-100 per cent). Introducing/awareness raising of AACproducts, systems and technology (13 per cent) and aspects of language developmentand learning through AAC (12 per cent) were also subject areas which received relatively highlevels of attention. In comparison, all other subject areas were poorly represented, with thepercentage of training in outcome measurement markedly low, at less than 1 per cent ofoverall training activity.
The areas of training content were categorised as relating to the impairment, activity, participationor environment of an AAC user, as follows (Table IV ).
These definitions were based on the ICF model (WHO, 2001). Measuring outcomes was found tofall outside the specific components of the ICF model, as outcomes might relate to any aspect ofimpairment, activity, participation or environment.
As shown in Table III, whilst a large percentage of training was delivered on specific areasof the environment, training was also frequently provided on aspects of the AAC user’simpairment and activity. Notably, training on the participation of AAC users appeared to be lessfrequently delivered.
Table II Percentage of training delivered to specific professional groups
Percentage ofoverall clinical
services providingtraining to each
profession (n¼85)
Percentage of adultclinical services
providing training toeach profession
(n¼32)
Percentage ofpaediatric clinicalservices providingtraining to each
profession (n¼ 42)
Percentage of mixedclinical services
providing training toeach profession
(n¼ 11)
Speech andlanguagetherapists 62 47 64 100Teachingassistants 60 13 95 64Teachers 53 9 83 64Care assistants 48 66 33 55Occupationaltherapists 36 38 31 55Other 24 19 29 18Nurses 20 34 7 27Physiotherapists 20 19 19 27Managers 16 16 12 36Social workers 13 25 5 9Clinicaltechnicians 12 9 10 27Psychologists 9 13 7 9Commissioners 7 3 5 27Doctors 6 3 5 18
VOL. 11 NO. 3 2017 j JOURNAL OF ENABLING TECHNOLOGIES j PAGE 105

3.3 Perceived priorities for future training
Respondents ranked 15 subject areas for priority for future training provision (1¼ highest priority,15¼ lowest priority). Overall, the subject area receiving the highest priority ranking was use ofspecific AAC products, systems and technology (mean ranking score¼ 5.35). Other highlyranked subject areas were adapting the environment to facilitate AAC use (mean ranking
Table III Proportion of training delivered by service providers in each specified content topic
Overall clinical services Adult services Paediatric services Mixed services
Use of specific AAC products,systems and technology: 27%
Use of specific AAC products,systems and technology: 27%
Use of specific AAC products,systems and technology: 30%
Use of specific AAC products,systems and technology: 21%
(E) (E) (E) (E)Introducing/awareness raising ofAAC products, systems andtechnology: 13%
Introducing/awareness raising ofAAC products, systems andtechnology: 14%
Language development andlearning through AAC: 19%
Introducing/awareness raising ofAAC products, systems andtechnology: 15%
(E) (E) (A) (E)Language development andlearning through AAC: 12%
AAC use for daily living activities:11%
Introducing/awareness raising ofAAC products, systems andtechnology: 11%
Language development andlearning through AAC: 12%
(A) (A) (E) (A)Cognition and language: 7% Cognition and language: 9% Adapting the environment to
facilitate AAC use: 8%Cognition and language: 9%
(I) (I) (E) (I)AAC use for daily living activities:6%
Developing the interpersonalinteraction skills of significantothers: 9%
Developing the interpersonalinteraction skills of people usingAAC: 6%
Seating and positioning for AACuse: 7%
(A) (P) (P) (A)Adapting the environment tofacilitate AAC use: 6%
Developing the interpersonalinteraction skills of people usingAAC: 6%
Motor and sensory function: 6% AAC service delivery and funding:6%
(E) (P) (I) (E)Developing the interpersonalinteraction skills of people usingAAC: 6%
Adapting the environment tofacilitate AAC use: 5%
Cognition and language: 5% Developing the interpersonalinteraction skills of significantothers: 6%
(P) (E) (I) (P)Developing the interpersonalinteraction skills of significantothers: 6%
Supporting social/communityparticipation of people who useAAC: 5%
Developing the interpersonalinteraction skills of significantothers: 4%
Adapting the environment tofacilitate AAC use: 5%
(P) (P) (P) (E)Motor and sensory function: 4% Motor and sensory function: 4% Seating and positioning for AAC
use: 4%Supporting social/communityparticipation of people who useAAC: 5%
(I) (I) (A) (P)Seating and positioning for AACuse: 3%
AAC service delivery and funding:3%
AAC use for daily living activities:3%
AAC use for daily living activities:4%
(A) (E) (A) (A)Supporting social/communityparticipation of people who useAAC: 3%
Language development andlearning through AAC: 3%
Supporting social/communityparticipation of people who useAAC: 2%
Developing the interpersonalinteraction skills of people usingAAC: 4%
(P) (A) (P) (P)AAC service delivery and funding:2%
Acceptance, rejection andabandonment of AAC: 2%
Managing others’ attitudes towardspeople who use AAC: 1%
Acceptance, rejection andabandonment of AAC: 2%
(E) (A) (E) (A)Acceptance, rejection andabandonment of AAC: 1%
Seating and positioning for AACuse: 1%
Measuring outcomes: 1% Managing others’ attitudes towardspeople who use AAC: 2%
(A) (A) (E)Managing others’ attitudes towardspeople who use AAC: 1%
Managing others’ attitudes towardspeople who use AAC: o1%
AAC service delivery andfunding: o1%
Motor and sensory function: 2%
(E) (E) (E) (I)Measuring outcomes: o1% Measuring outcomes: o1% Acceptance, rejection and
abandonment of AAC: o1%Measuring outcomes: o1%
(A)
Notes: Key, I, impairment; A, activity; P, participation; E, environment
PAGE 106 j JOURNAL OF ENABLING TECHNOLOGIES j VOL. 11 NO. 3 2017
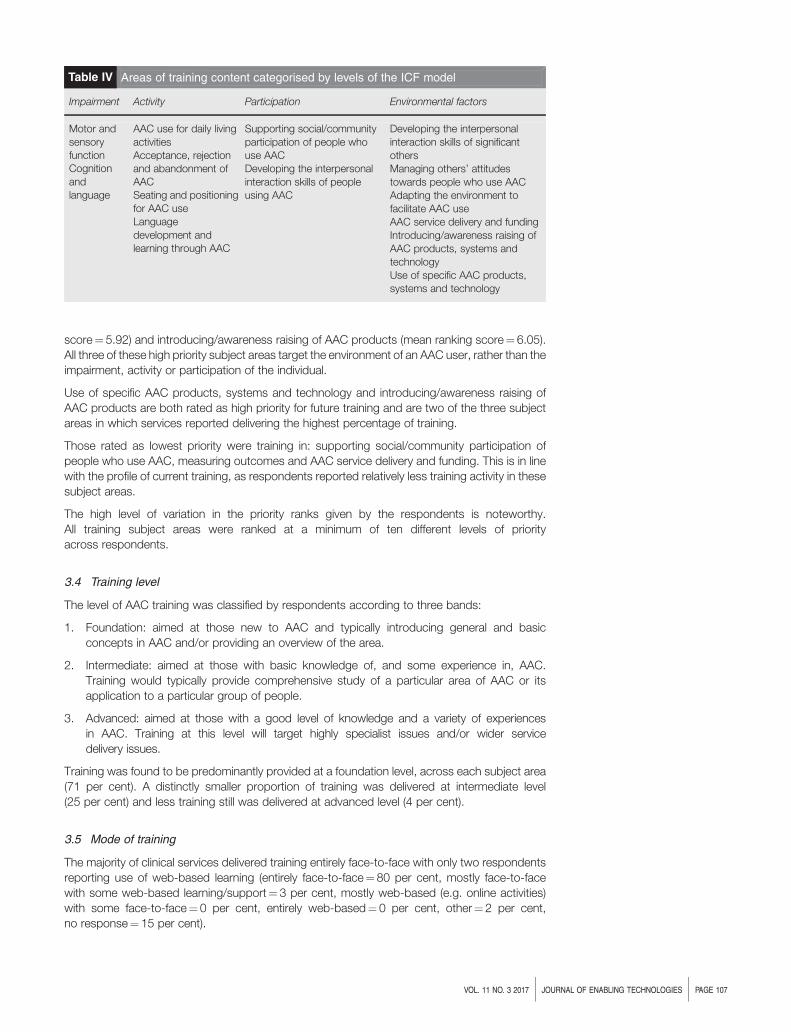
score¼ 5.92) and introducing/awareness raising of AAC products (mean ranking score¼ 6.05).All three of these high priority subject areas target the environment of an AAC user, rather than theimpairment, activity or participation of the individual.
Use of specific AAC products, systems and technology and introducing/awareness raising ofAAC products are both rated as high priority for future training and are two of the three subjectareas in which services reported delivering the highest percentage of training.
Those rated as lowest priority were training in: supporting social/community participation ofpeople who use AAC, measuring outcomes and AAC service delivery and funding. This is in linewith the profile of current training, as respondents reported relatively less training activity in thesesubject areas.
The high level of variation in the priority ranks given by the respondents is noteworthy.All training subject areas were ranked at a minimum of ten different levels of priorityacross respondents.
3.4 Training level
The level of AAC training was classified by respondents according to three bands:
1. Foundation: aimed at those new to AAC and typically introducing general and basicconcepts in AAC and/or providing an overview of the area.
2. Intermediate: aimed at those with basic knowledge of, and some experience in, AAC.Training would typically provide comprehensive study of a particular area of AAC or itsapplication to a particular group of people.
3. Advanced: aimed at those with a good level of knowledge and a variety of experiencesin AAC. Training at this level will target highly specialist issues and/or wider servicedelivery issues.
Training was found to be predominantly provided at a foundation level, across each subject area(71 per cent). A distinctly smaller proportion of training was delivered at intermediate level(25 per cent) and less training still was delivered at advanced level (4 per cent).
3.5 Mode of training
The majority of clinical services delivered training entirely face-to-face with only two respondentsreporting use of web-based learning (entirely face-to-face¼ 80 per cent, mostly face-to-facewith some web-based learning/support¼ 3 per cent, mostly web-based (e.g. online activities)with some face-to-face¼ 0 per cent, entirely web-based¼ 0 per cent, other¼ 2 per cent,no response¼ 15 per cent).
Table IV Areas of training content categorised by levels of the ICF model
Impairment Activity Participation Environmental factors
Motor andsensoryfunctionCognitionandlanguage
AAC use for daily livingactivitiesAcceptance, rejectionand abandonment ofAACSeating and positioningfor AAC useLanguagedevelopment andlearning through AAC
Supporting social/communityparticipation of people whouse AACDeveloping the interpersonalinteraction skills of peopleusing AAC
Developing the interpersonalinteraction skills of significantothersManaging others’ attitudestowards people who use AACAdapting the environment tofacilitate AAC useAAC service delivery and fundingIntroducing/awareness raising ofAAC products, systems andtechnologyUse of specific AAC products,systems and technology
VOL. 11 NO. 3 2017 j JOURNAL OF ENABLING TECHNOLOGIES j PAGE 107

4. Discussion
The aim of this paper was to identify the profile of post-qualification AAC training delivered byclinical services in England. This was based on the recognition that AAC services andtechnologies are evolving rapidly and that available evidence does not provide robustunderstanding of the amount and type of training being provided and the learningsupport needs for professionals who may encounter AAC in their clinical work. The resultsindicate variability in the training delivered, together with a tendency towards face-to-facefoundation level training.
4.1 Training content and perceived priorities
Approximately one-third of training across services focussed on using specific AACtechnology; however, the range of training priorities was diverse. This may be due to thelimited policy and recommendations available to guide priorities for training, or may reflectthe heterogeneous nature of the client group and variable training needs for AAC professionals.Notably, whilst “adapting the environment to facilitate AAC use” received a relatively highpriority rating from respondents, this area was reported to receive very little attention duringtraining provision.
4.2 Focus on training to support technology use
Recommendations for post-qualification AAC training often focus on the use of specific AACtechnologies (e.g. Enderby et al., 2013; RCSLT, 2011). However, other essential aspects ofknowledge and skill in relation to supporting the holistic needs of people who use AAC are,it seems, not fully addressed. The content most frequently covered in post-qualification trainingdid not fully reflect the breadth of areas covered in the ICF model, and thus the full potential needsof AAC users and their families.
The emphasis on AAC technology, operational skills and/or an introduction to AAC correspondswith data on the content of pre-qualification courses in the USA (Costigan and Light, 2010).This is of relevance as AAC researchers report concerns that the focus on technology is beingprioritised over the focus on the communication skills and needs of the individual (Light andMcNaughton, 2013). Indeed, in a study of long-term outcomes of AAC provision, five out of sevenpeople using AAC who were interviewed reported that AAC can function as a barrier tocommunication, and that intervention should best be driven by participation goals, rather thantechnology use (Lund and Light, 2007).
4.3 Supporting the environment and participation of the AAC user
Limited training appeared to be provided for many environmental and participation factors suchas supporting interactions with significant others, adapting the environment, AAC for daily livingand the acceptance, and rejection and abandonment of AAC. There is currently little research onthe effectiveness of AAC training for professionals across the ICF model’s various domains,however, some evidence suggests that environmental training on topics beyond use of AACtechnology can result in maintained improvement of AAC use in the short term (McMillan, 2008).Furthermore, research has suggested that AAC training focusing on elements of participationsuch as the attitudes and skills of conversation partners may be beneficial. The attitudes of family,peers, professionals and society are understood to impact on participation levels for AAC users(McCarthy and Light, 2005). According to Lund and Light (2007), it is likely that positive attitudesto AAC use will result in expectations of success and a supportive and inclusive environment.This suggests that training professionals to advocate positive attitudes towards AAC use in theirsettings may result in better outcomes for AAC users. However, as an increasing range ofmainstream technology is used to provide AAC options, several researchers have proposed thatthere is increased public awareness and social acceptance of AAC (McNaughton andLight, 2013; Shane et al., 2012). Questions remain as to the potential shifts in societal attitudestowards AAC and people who use AAC as mainstream technologies are used for AAC purposes,and the ways in which training may promote positive attitudinal change.
PAGE 108 j JOURNAL OF ENABLING TECHNOLOGIES j VOL. 11 NO. 3 2017

4.4 Outcome measurement in AAC
The Department for Children, Schools and Families (2008) found that insufficient measurementsexist to provide service commissioners with evidence of outcomes in speech and languagetherapy, and recommended continual evaluation of progress to ensure positive outcomes forclients. Outcome measurement was reported to be given minimal attention in the trainingprovided by survey respondents in this study. This limited focus on outcome measurement hasalso been previously noted (Lund and Light, 2007). Furthermore, Lund and Light (2007) reportedthat AAC users and family members highlighted limited attention to goals and over-focus onintervention as a barrier to positive outcomes for people using AAC during interviews. The lowpriority given to training in AAC outcome measurement may reflect a need for this training to bedeveloped and delivered in this area. It is also possible that the low reported training on outcomesspecific to AAC but be a consequence of the respondents applying established service-wideprocedures for outcome measurement to the AAC context. Given the multifaceted and specificdemands of AAC intervention, it may be reasonable to suggest that reflection on outcomemeasurement in the AAC context would benefit from specific consideration by service providers.
4.5 Training level
The respondents reported that they primarily delivered foundation level training. As the topics ofAAC equipment, language development and learning, and some aspects of the environment andwere most commonly delivered in training by the survey respondents, this may reflect a model ofAAC training delivery where knowledge of these topics is regarded as foundation or basicknowledge of AAC. This suggests that elements of the environment such as supportinginteractions with significant others and adapting the environment; elements of participationsuch as AAC for daily living, and acceptance, rejection and abandonment of AAC, andoutcome measurement comprise the more intermediate/advanced knowledge related to AAC.Further multidisciplinary work will be required to identify the need for, and potential content of,intermediate and advanced training in AAC. Given that continuing professional development isintegral to professions working with individuals who use AAC, the lack of training at anintermediate or advanced level is an area of considerable concern.
4.6 Delivery mode
With the growing use of information technology in the workplace, a rising trend towards web-based learning for post-qualification professionals has been observed. However, only a smallproportion of the training delivered by the survey respondents in this study was given online.
Advantages of web-based learning are well purported; in particular, that web-based learning canbe achieved regardless of distance from trainer, that participants can access training according totheir own schedule and opportunities for individualised learning where participants progress attheir own pace (Cook, 2007). Web-based training can also support increased training reach(Lebel et al., 2005). This may be of specific benefit in the field of AAC, where specialist services aregeographically remote from the services that they may support. In these instances, web-basedlearning could result in significant savings relating to length and cost of travel. This is an area thatwould benefit from further exploration, in order to maximise professional efficiency andopportunities for staff development in the area of AAC.
4.7 Limitations
Limitations for this study include the sample method, as sampling was self-selected and theresearchers did not contact non-respondents to establish why they did not contribute tothe survey. With no register of clinical AAC services in England, it was not possible to calculate thepercentage of eligible services which responded to the questionnaire. Furthermore, there was abias in the distributional spread of responses with a greater number of responses from Londonand the South West. Nevertheless, the study did retain a large sample size and the surveyhas revealed some important insights into the training provision for professionals working inEngland with children and adults using AAC.
VOL. 11 NO. 3 2017 j JOURNAL OF ENABLING TECHNOLOGIES j PAGE 109

It is possible that clinical services are focussing on aided technology training and that the area ofunaided or low tech training may be receiving less attention (Iacono et al., 2011). This would benefitfrom further exploration in future research. Additionally, information was not collected regarding theprofessionals working in the teams surveyed, and it may be that the make-up of professionals inthose teams influenced their views on training priorities. A further limitation is that information ontraining to parents, carers and people who use AACwas not gathered. More research into this areamay provide valuable insights into the support parents, carers and users receive.
Professionals responding to the questionnaire were not asked to document the amount oftraining they provide on using AAC to access social media. However, as a growing area of interestwith potential benefits for AAC users (Raghavendra et al., 2015), it warrants consideration in post-and pre-qualification professional training.
4.8 Conclusion
There is no consensus on the amount or content of AAC training which professionals in Englandmust receive in order to provide best possible services to people using AAC. Existing researchsuggests that AAC training for pre-qualification professionals is limited and this paper hasidentified significant variation in the amount and type of post-qualification AAC training providedby clinical services. Training provided by respondents was predominantly face-to-face anddelivered at a foundation level. Respondents reported diverse priorities for future AAC training;notably, these priorities did not consistently match the current training content.
There is potential for the re-examination of AAC training provision to professionals across a broadrange of areas. Costigan and Light (2010) have recommended that specific and measurablecompetencies for AAC training should be established in order to enhance professionalknowledge and skills against recognised benchmarks, and frameworks such as the IPACCKS(NHS Education for Scotland, 2014) have been developed for this purpose. Recommendationsfor effective training delivery models and length and dosage of training in AAC would allowprofessionals to ensure they have the training to support AAC users. To develop AAC training inEngland, further information is needed on whether current AAC training is effective, to determinethe maintenance of skills learnt and the impact of this training. In particular, evidence relating tothe efficacy of AAC training across ICF domains would seem to support recommendations forpotential AAC training content for professionals.
References
Clarke, M.T. and McConachie, H. (2001), “Views of young people using augmentative and alternativecommunication systems”, International Journal of Language and Communication Disorders, Vol. 36 No. 1,pp. 107-15.
Clarke, M.T., Price, K. and Griffiths, T. (2016), “Augmentative and alternative communication for children withcerebral palsy”, Paediatrics and Child Health, Vol. 26 No. 9, pp. 373-7.
Clarke, M.T., Newton, C., Petrides, K.V., Griffiths, T., Lysley, A. and Price, K. (2012), “An examination ofrelations between participation, communication and age in children with complex communication needs”,Augmentative and Alternative Communication, Vol. 28 No. 1, pp. 44-51.
Communication Champion (2010), “Augmentative and alternative communication: a report on provisionfor children and young people in England”, a report from the Office of the Communication Champion andCouncil, London.
Communication Champion (2011), “Specialised AAC provision: commissioning national services”, a reportfrom the Office of the Communication Champion and Council, London.
Communication Matters (2012), “AAC service standards”, a report from Communication Matters, Leeds.
Cook, D.A. (2007), “Web-based learning: pros, cons and controversies”,Clinical Medicine, Vol. 7 No. 1, pp. 37-42.
Costigan, A. and Light, J. (2010), “A review of preservice training in augmentative and alternativecommunication for speech-language pathologists, special education teachers, and occupational therapists”,Assistive Technology: The Official Journal of RESNA, Vol. 22 No. 4, pp. 200-12.
PAGE 110 j JOURNAL OF ENABLING TECHNOLOGIES j VOL. 11 NO. 3 2017

Creer, S., Enderby, P., Judge, S. and John, A. (2016), “Prevalence of people who could benefit fromaugmentative and alternative communication (AAC) in the UK: determining the need”, International Journal ofLanguage and Communication Disorders, Vol. 51 No. 6, pp. 639-53.
Department for Children, Schools and Families (2008), “The Bercow report: a review of services for childrenand young people (0-19) with speech, language and communication needs”, a report from Department forChildren, Schools and Families, London.
Department for Education (2013), “The future of AAC services in England: a framework for equitable andeffective commissioning”, a report from the Department for Education, London.
Enderby, P., Judge, S., Creer, S. and John, A. (2013), “Examining the need for, and provision of, AAC in theUnited Kingdom”, a report from Communication Matters, Leeds.
Ganz, J.B. (2015), “AAC interventions for individuals with autism spectrum disorders: state of the science andfuture research directions”, Augmentative and Alternative Communication, Vol. 31 No. 3, pp. 203-14.
Gresswell, A. and Hoogerwerf, E. (2007), “Guidelines for lifelong learning in assistive technology.Communication, computer access and environmental control”, KPT Consortium, AIAS Bologna Onlus,Bologna, available at: www.at4inclusion.org/kpt/book+guidelines_ENG.pdf (accessed 19 August 2016).
Griffiths, T. and Price, K. (2011), “A proposed framework for decision-making for assistive communicationtechnology support: many perspectives, but one common goal”, Journal of Assistive Technologies, Vol. 5No. 4, pp. 242-8.
Iacono, T., Lyon, K. and West, D. (2011), “Non-electronic communication aids for people withcomplex communication needs”, International Journal of Speech Language Pathology, Vol. 13 No. 5,pp. 399-410.
Lebel, T., Olshtain, E. and Weiss, P. (2005), “Teaching teachers about augmentative and alternativecommunication: opportunities and challenges of a web-based course”, Augmentative and AlternativeCommunication, Vol. 21 No. 4, pp. 264-77.
Light, J. and McNaughton, D. (2012), “Supporting the communication, language, and literacy development ofchildren with complex communication needs: state of the science and future research”, Assistive Technology,Vol. 24 No. 1, pp. 34-44.
Light, J. and McNaughton, D. (2013), “Putting people first: re-thinking the role of technology in augmentativeand alternative communication intervention”, Augmentative and Alternative Communication, Vol. 29 No. 4,pp. 299-309.
Lund, S. and Light, J. (2007), “Long-term outcomes for individuals who use augmentative and alternativecommunication: part III – contributing factors”, Augmentative and Alternative Communication, Vol. 23 No. 4,pp. 323-35.
McCarthy, J. and Light, J. (2005), “Attitudes towards individuals who use augmentative andalternative communication: research review”, Augmentative and Alternative Communication, Vol. 21 No. 1,pp. 41-55.
McMillan, J. (2008), “Teachers make it happen: from professional development to integration of augmentativeand alternative communication technologies in the classroom”, Australasian Journal of Special Education,Vol. 32 No. 2, pp. 199-211.
McNaughton, D. and Light, J. (2013), “The iPad and mobile technology revolution: benefits and challenges forindividuals who require augmentative and alternative communication”, Augmentative and AlternativeCommunication, Vol. 29 No. 2, pp. 107-16.
Matthews, R. (2001), “A survey to identify therapists’ high-tech AAC knowledge, application and training”,International Journal of Language and Communication Disorders, Vol. 36, pp. 64-9.
National Institute for Health and Care Excellence (2016), “Motor neurone disease: assessment andmanagement (NG42)”, a report from NICE, London.
NHS Education for Scotland (2014), “IPAACKS: informing and profiling AAC knowledge and skills”,a framework from NHS Education for Scotland, Edinburgh.
Price, K. and Clarke, M.T. (2011), “Developing total communication systems for children with oro-motordisorders”, in Roig Quilis, M. and Pennington, L. (Eds),Oro-Motor Disorders in Childhood, Viguera, Barcelona,pp. 285-98.
VOL. 11 NO. 3 2017 j JOURNAL OF ENABLING TECHNOLOGIES j PAGE 111

Raghavendra, P., Newman, L., Grace, E. and Wood, D. (2015), “Enhancing social participation in youngpeople with communication disabilities living in rural Australia: outcomes of a home-based intervention forusing social media”, Disability and Rehabilitation, Vol. 37 No. 17, pp. 1576-90.
RCSLT (2011), “Resource manual for commissioning and planning services for SLCN: augmentative andalternative communication (AAC)”, a report from the RCSLT, London.
Rowland, C., Fried-Oken, M., Steiner, S., Lollar, D., Phelps, R., Simeonsson, R. and Granlund, M. (2012),“Developing the ICF-CY for AAC profile and code set for children who rely on AAC”, Augmentative andAlternative Communication, Vol. 28 No. 1, pp. 21-32.
Shane, H., Laubscher, E., Schlosser, R., Flynn, S., Sorce, J. and Abramson, J. (2012), “Applying technologyto visually support language and communication in individuals with autism spectrum”, Disorders Journal ofAutism and Developmental Disorders, Vol. 42 No. 6, pp. 1228-35.
Soto, G., Muller, E., Hunt, P. and Goetz, L. (2001), “Critical issues in the inclusion of students who useaugmentative and alternative communication: an educational team perspective”, Augmentative andAlternative Communication, Vol. 17 No. 2, pp. 62-72.
Threats, T.T. and Worrall, L. (2004), “Classifying communication disability using the ICF”, Advances inSpeech – Language Pathology, Vol. 6 No. 1, pp. 53-62.
World Health Organisation (2001), “International classification of functioning, disability and health”, a reportfrom the World Health Organisation, Geneva.
World Health Organisation (2007), “International classification of functioning, disability and health:children & youth version: ICF-CY”, A report from the World Health Organisation, Geneva.
Further reading
Clarke, M.T. and Price, K. (2012), “Augmentative and alternative communication for children with cerebralpalsy”, Paediatrics and Child Health, Vol. 22 No. 9, pp. 367-71.
Clarke, M.T., Price, K. and Jolleff, N. (2012), “Augmentative and alternative communication”, in Kersner, M.and Wright, J. (Eds), Speech and Language Therapy: The Decision Making Process When Working withChildren, Fulton, London, pp. 201-9.
Hynan, A., Goldbart, J. and Murray, J. (2015), “A grounded theory of internet and social media use by youngpeople who use augmentative and alternative communication (AAC)”, Disability and Rehabilitation, Vol. 37No. 17, pp. 1559-75.
Mirenda, P. (2003), “Toward functional augmentative and alternative communication for students with autism:manual signs, graphic symbols, and voice output communication aids”, Language, Speech, and HearingServices in Schools, Vol. 34 No. 3, pp. 203-16.
Corresponding author
Michael Clarke can be contacted at: [email protected]
For instructions on how to order reprints of this article, please visit our website:www.emeraldgrouppublishing.com/licensing/reprints.htmOr contact us for further details: [email protected]
PAGE 112 j JOURNAL OF ENABLING TECHNOLOGIES j VOL. 11 NO. 3 2017

“A child with autism only has onechildhood”: main themes and questionsfor research from the “Digital Bubbles”seminar series
Sarah Parsons, Nicola Yuill, Mark Brosnan and Judith Good
Abstract
Purpose – The purpose of this paper is to present an overview of the main messages and key questions forfurther research arising from the seven-seminar series entitled, “Innovative technologies for autism: criticalreflections on digital bubbles”, funded by the Economic and Social Research Council in the UK.Design/methodology/approach – A synthesis of the main ideas is presented, drawing on thepresentations, discussions, participant feedback, and short papers from across the seminar series, whichtook place between November 2014-2016.Findings – There were many positive examples where technologies were positioned and used as facilitative“bridges” between ideas, communities, understanding, and experiences. Researchers and communitystakeholders also emphasised the importance of taking different perspectives and working in strongerpartnerships with each other. Four overarching research questions were developed from these themes toprovide a roadmap for future research, relating to: responsible innovation, technology-enabled socialinteraction, learning and pedagogy, and engagement.Originality/value – The findings and methodologies produced by the Digital Bubbles seminar series,available on the project website (http://digitalbubbles.org.uk/) and in a series of short papers, provide a richrepository of state-of-the-art thinking in the field of autism and technology that is being utilised nationally andinternationally in teaching and learning. This paper suggests some valuable future research directions andhighlights the importance of establishing and maintaining multi-disciplinary research teams, with autisticpeople and their families at their core.
Keywords State-of-the-art, Autism, Multi-disciplinary, Innovative technologies, Future research,Co-construction
Paper type Viewpoint
Introduction
Interest in the development, application, and evaluation of a range of technologies forsupporting children and adults on the autism spectrum, and their families and friends,remains very strong. In this journal alone, some of the most downloaded papers reportresearch situated in this field (e.g. Mintz, 2013; Tunney and Ryan, 2012). Media reportsabound, highlighting both dire warnings and miraculous interventions when using technologiesfor people with autism (e.g. see examples in Parsons et al., 2015; Parsons, 2015a), andresearch interest in this area has shown very strong growth in recent years (Ploog et al., 2013).It was this expanding interest in the field, along with our own experiences of many years ofrelevant research, which provided the catalyst for proposing a series of seminars that wouldcritically evaluate and discuss research and practice in autism and technology. We wereinterested in probing (or “popping” in the nomenclature of the series) the “bubbles” that tend toexist in the field. That is, we had observed tendencies for ideas, critiques, and teams to work in
Received 13 July 2017Revised 13 July 2017Accepted 18 July 2017
© Sarah Parsons, Nicola Yuill,Mark Brosnan and Judith Good.Published by Emerald PublishingLimited. This article is publishedunder the Creative CommonsAttribution (CC BY 4.0) licence.Anyone may reproduce, distribute,translate and create derivativeworks of this article ( for bothcommercial & non-commercialpurposes), subject to fullattribution to the originalpublication and authors. The fullterms of this licence may be seenat http://creativecommons.org/licences/by/4.0/legalcode
The seminar series “Innovativetechnologies for autism: criticalreflections on digital bubbles” is acollaboration between theUniversities of Southampton,Sussex and Bath, funded by theESRC (No. ES/M002624/1). Allsummaries of feedback obtainedduring the seminar series areavailable on the website http://digitalbubbles.org.uk. The authorswould like to thank everyone whotook part in the seminar series aswell as the many friends andcolleagues who provided invaluablesupport behind the scenes.
The authors affiliation’s can befound at the end of this article.
DOI 10.1108/JET-07-2017-0023 VOL. 11 NO. 3 2017, pp. 113-119, Emerald Publishing Limited, ISSN 2398-6263 j JOURNAL OF ENABLING TECHNOLOGIES j PAGE 113

isolation from each other without cross-fertilising research agendas and practice. We wantedto examine these bubbles and try to bring them together in meaningful ways throughdiscussion, participation, and engagement. This endeavour was funded by the Economicand Social Research Council (ESRC) in the UK for the seminar series: “Innovative technologiesfor autism: critical reflections on digital bubbles”, which took place over two years between2014-2016, with the series website being our main communication and dissemination tool(http://digitalbubbles.org.uk/).
The “Digital Bubbles” seminar series was designed around six core themes with an opportunityfor synthesis and further reflection at the seventh, final seminar. We have previously reported onthe main discussions that took place, and the questions that arose, from the six themed seminarsas summarised in Table I.
The final seminar was named “The Cauldron of Many Bubbles” to reflect its role in bringingtogether the main ideas from the previous six seminars, highlighting key themes, and identifyingpriorities and questions for future research. The seminar took place at Cumberland Lodge,Berkshire, UK in November 2016. This short paper provides an overview of these aspects fromthe final seminar and summarises the main outcomes of the series, both practical and intellectual.We first address the knowledge gained, followed by the practical aspects that supported thedevelopment of a multi-disciplinary network through the series of seminars.
Key themes and questions for the field from the seminar series
There was an absolutely central question that underpinned many discussions, and which wasposed directly by one of the delegates at the very first seminar:
Whenever you’re trying to develop technologies, think about whether it will really improve someone’slife – or do you just think it will?
Table I Summary of the six themed seminars in the series “Innovative technologies forautism: critical reflections on digital bubbles”
Seminar Date and location Main focus or question(s) addressedRelatedpublication
Seminar 1: TheSocial Bubble
University ofSouthampton,November 2014
Whether technologies create a social bubbleand, if so, do they increase social isolation,or provide helpful ways of engaging with otherpeople in a remote way?
Parsons et al.(2015)
Seminar 2: TheDevelopmentalBubble
University ofSussex, March2015
How can developmental psychology informapproaches to understanding of autism(and approaches to intervention)?
Yuill et al. (2015)
Seminar 3: TheMethodologicalBubble
University of Bath,July 2015
What are the useful strategies as well aschallenges that have been found in developing,researching and evaluating technologies forautism?
Brosnan et al.(2016)
Seminar 4: TheTechnologyBubble
University ofSouthampton,November 2015
How do different kinds of technology supportinteraction and communication? What are thebenefits and costs of the development and useof different types of innovative technologies(e.g. virtual reality; tangible devices; augmentedreality)?
Good, Parsons,Yuill and Brosnan(2016)
Seminar 5: TheDisciplinaryBubble
University ofSussex, March2016
What is it that we are trying to achieve withtechnology and how can we collaborateconstructively across these disciplines to realiseour goals?
Parsons et al.(2017)
Seminar 6: TheDiversity Bubble
University of Bath,July 2016
What can we learn from research beingconducted with other groups of users and howmight awareness of such diversity inform awider agenda of social inclusion?
Brosnan et al.(2017)
PAGE 114 j JOURNAL OF ENABLING TECHNOLOGIES j VOL. 11 NO. 3 2017
The importance of ensuring that technologies adequately address this question was alsosummed up very powerfully by the following statement of one of the speakers (a parent andresearcher) at the sixth seminar:
A child with autism only has one childhood.
This was a crucial reminder that children with autism are children first and not experimentalparticipants. We have to be clearer about what we are trying to aim for in research and practice inorder to ensure that needs and expectations are appropriately met and that valuable time is notwasted on enterprises that may not be useful, engaging or fun. The same applies to adultsparticipating in, or collaborating with, research of course.
In synthesising the core of the discussions across the series, there was a repeated and helpfulmetaphor, both explicit and implicit, that characterised many ideas, i.e. digital technologies as“bridges”, for example:
■ to interactions between people, and between contexts;
■ across gaps in understanding, for enabling people to understand and experience differentperspectives;
■ between real and virtual, in terms of making online connections and friendships as well asmoving more smoothly between real and virtual contexts;
■ between cultures, in relation to the positive representation and expression of autistic cultureonline and how this is raising awareness;
■ between research and practice, through applying tools that support and documentpractitioner involvement in research;
■ between communities, by establishing networks of interest and expertise that can be local,national, and international in nature;
■ between disciplines, by encouraging a focus on what projects need to do rather than who weare as researchers; and
■ between processes and outcomes, through questioning what an “appropriate outcome”looks like for individuals, and valuing participation in the process of engagement as much asany measured outcomes at the end of projects.
These bridges seemed to place an emphasis on the different roles that technologies can play aspractical tools for enabling connections, understanding, sharing, and greater awareness inthe field, and extended the initial idea of technologies as bridges proposed by Barnabear (2014),a self-described “Aspie and Software Engineer”, at the first seminar.
Beyond the nature of digital technologies as facilitative tools were core principles for research andresearchers that emerged from the presentations and discussions at the previous six seminars.First, there was a strong message about the need to “look up and outwards” with regard totechnology use and development for people with autism (particularly inspired by Yvonne Rogers’talk at the fifth seminar, see Parsons et al., 2017). This principle related both to researchers whoare encouraged to consider wider perspectives from outside their own disciplinary bubbles, andalso to how technologies can support engagement and creativity in a variety of ways.For example, some discussions across the series highlighted the need to “pop” the bubbleregarding concerns about unhealthy or socially isolating uses of technologies and instead toreflect and report on how technologies can connect individuals in important ways. Examplesprovided by seminar participants included sharing family discussions about Minecraft, or bymaking friends with others who share a special interest.
Second, there was recognition that, as a field, we often need to “stand back” from neurotypicalassumptions and expectations about the roles of technologies and how they could or should beused for supporting people with autism and their families. Technologies that focus onameliorating social and communication difficulties tend to dominate the field (e.g. Ploog et al.,2013; Wass and Porayska-Pomsta, 2014) reflecting a “medical model” approach that places anemphasis on fixing the impairment rather than on enabling the strengths, interests, and creativity
VOL. 11 NO. 3 2017 j JOURNAL OF ENABLING TECHNOLOGIES j PAGE 115

of individuals (Shakespeare, 2006). Instead, there is an opportunity to focus more onunderstanding the roles that technologies play in the everyday lives of people with autism andtheir families, and to value the meaning that they find in those uses and interactions.
Part of the “standing back”, therefore, also involves greater consideration and action regarding“taking the lead”. This means that researchers need to develop more inclusive and participatoryapproaches to projects and understand who should be involved, in what ways, and at what stagesof research. There is always a balance to be struck here: some people with autism and their familiesmay not want to be fully involved or to take the lead in projects, but may wish to contribute viewsand expertise in a range of ways (see Brosnan et al., 2016). The key is ensuring that participation isplanned for and enabled from the start of the project in ways that align with the core activities andresearch questions of the project, as well as with the needs and wishes of relevant stakeholders.
Finally, and overarching these three core principles, is the need for the field to develop moremulti-dimensional and holistic ways of researching and understanding how and where technologiescan be used, developed, and evaluated. This includes incorporating the perspectives of parents,friends, and siblings as well as the multiple other stakeholders whose views and expertise alsoshape and influence technology engagement. This also requires moving beyond narrowly definedoutcome measures in research in order to capture the richness and complexity of the contexts,practices, and pedagogies of technology use.
In reflecting on these core principles, we developed four key questions (and sub-questions) thatencapsulated what we had learned as well as signposted us towards a research agenda,informed by and formed with the many stakeholders who attended the series:
RQ1. What does responsible innovation mean in the autism and technology field?
RQ1a. How do we know that what we do really makes a difference or is valued?
RQ1b. For whom might it really make a difference or be valued? This could be from theperspectives of individuals with autism, parents and families, practitioners, as well as fromthe perspectives of professionals who may wish to use technologies to supportindividuals and families in a range of ways.
RQ1c. What is it that we are really trying to achieve with our work, and why?
RQ2. What does it mean to be social in a technology-enabled world?
RQ2a. Where or what is the “social deficit”? Where is the social isolation? In other words, it isimportant to question critically the idea that people with autismmay be particularly sociallydisadvantaged by engaging with technologies.
RQ2b. From whose perspective are we making these judgements? Much research and thinkingabout autism comes from a “neurotypical” perspective, but we need to strive for a betterunderstanding of the benefits and limitations of technologies from the perspectives of thepeople who use them.
RQ2c. How do we challenge normative assumptions, or start from a different place in ourthinking? Addressing this question presupposes that much stronger collaborativeworking is fundamental for moving the field forward.
RQ3. What could be the focus for learning and pedagogy?
RQ3a. How can we encourage “looking up and outwards”? In other words, how canresearchers and practitioners take a wider view of what is happening within and aroundthe technology to support e-inclusion (Abbott, 2007)? How can technologies be used toenable connections and interactions with others in a range of ways?
RQ3b. How can we enable fun, play, creativity, lightness, and subtlety? Much research in thisarea focuses on addressing social communication difficulties, but what are we missing bymaintaining this narrow focus? Broadening our ideas of positive engagement andindicators of success would enable a more holistic understanding of the person or child.
RQ3c. What role could technologies play in addressing the “double empathy problem” (Milton,2012)? This is the problem that people without autism have difficulties understanding the
PAGE 116 j JOURNAL OF ENABLING TECHNOLOGIES j VOL. 11 NO. 3 2017

world from the perspectives of people with autism, and vice versa. The affordances oftechnologies can be used to support sharing digital spaces and taking differentperspectives (e.g. Parsons, 2015b).
RQ4. How can we think more holistically about engagement?
RQ4a. Dowe need “bridges” at all? In other words, is it possible to think inmore inclusive ways abouthow people, working or interacting together, may use technologies for shared purposes?
RQ4b. How can we more effectively enable support and mediation through technologies? Thisquestion requires us to consider technologies as mediating tools that can supportengagement, interest, and communication in different ways, rather than simply as ameans for rehearsal or practice of behaviours that may be difficult. A good example of thisis from a Mum at the first seminar who described how her son’s love of Minecraft hadopened up dialogue between family members as they shared in his enjoyment.
RQ4c. How can we integrate experiences, processes and outcomes and adequately addresscomplexity and multiple perspectives within research and practice? This requires us tomove beyond narrowly defined or standardised outcome measures of behaviour orcommunication to try to capture the richness and diversity of experiences, preferences,and interactions that take place between multiple stakeholders.
We intend to use these questions to help guide our own future research endeavours and, ofcourse, share them here with the aim of generating further ideas, discussion, and debate. It isimportant to reflect that many of these questions are not necessarily autism-specific but couldhave more general applicability as a way of framing the value and usefulness of technology in avariety of contexts. The important point, though, is that these questions have emerged fromsustained and shared discussions with stakeholders from across the autism and technology field.In other words, we have already started from a different place in our thinking. We next reportbriefly on the practicalities of engagement through the series to highlight the foundation that wasestablished and upon which we can move forward with this research agenda.
Successful outcomes from the seminar series: engagement and co-construction
Through the seminars, we have developed a strong, multi-disciplinary community of academicresearchers and stakeholders (people with autism, families and carers, professionals andpractitioners) to review and critically evaluate ways that technology might support or impair thewellbeing of people on the autism spectrum. This community also includes internationalacademics, national and local autism organisations, representatives from the technologyindustry, and autism research funders. Over the seven seminars, 240 delegates attended and wesupported 50 travel bursaries to enable postgraduate research students (PGRs) and early careerresearchers (ECRs) and community stakeholders to participate. A particular success of the serieswas the sustained involvement of stakeholders, PGRs and ECRs throughout, enabling them tocontribute to and participate in these important discussions. We also developed an internationalperspective with colleagues attending from Spain, Turkey and the USA. Academics andpractitioners from an ERASMUS+ project entitled SMART-ASD (see SMART-ASD.EU) attendedone of the seminars as part of their development days.
We have also developed an interdisciplinary co-constructed body of knowledge and aninnovative method of e-participation for the autism and technology field (see below), both ofwhich inform our agenda for future research. First, the participation of stakeholders wassupported directly at the seminars through many opportunities for discussion and feedback, andcontinued through the website after each seminar. A simple, but effective, strategy at theseminars was to encourage delegates to note down questions and observations on Post-it notesduring the day and place these on the wall for other delegates to see. Delegates were asked atthe end of the seminar to spend five minutes writing down final reflections, including any keymessages they took from the day and/or any burning questions they were left with. These Post-itnotes were collated and shared through the website. They became an important source ofinformation since they provided evidence of scrutiny and reflection on the invited talks and
VOL. 11 NO. 3 2017 j JOURNAL OF ENABLING TECHNOLOGIES j PAGE 117

ensured that everyone who attended a “Digital Bubbles” seminar had the opportunity to voicetheir views or queries. This feedback from speakers and delegates was incorporated into theprevious six papers reporting on the discussions of the series (see Table I) and so became anessential mechanism for co-constructing key ideas and messages.
Second, we have developed and promoted a free innovative mobile app, ASCmeI.T., inspired bythe first seminar and jointly funded by each of the research team’s respective institutions fromEnterprise Budgets and Research Council (ESRC and EPSRC) Impact Acceleration Funds.ASCmeI.T. was co-developed with members of the autistic community who had attended thefirst seminar. The app is free to download (ascme-it.org.uk) and enables anyone to submit ideasabout “which technology for autism needs to be invented?”, either using their mobile phones, orthrough the ASCmeI.T., website. The autistic community can therefore input into the very firststages of the technology design process for the first time, and the app is a good example of ane-participation method that could be applied much more widely (Good, Yuill, Parsons,Brosnan and Austin, 2016; Parsons et al., 2016).
The seminar series website (http://digitalbubbles.org.uk) is now a rich repository of key messagesand short videos from national and international speakers about their research in the autism andtechnology field. This state-of-the-art resource is being used within teaching for studentsstudying autism-related topics at all three academic institutions represented by the DigitalBubbles team (Universities of Southampton, Sussex, Bath). In addition, the website is a keyresource within the SMART-ASD MOOC (Europe-wide in multiple languages) that has beendeveloped at the University of Bath for parents and practitioners of children with autism (www.bath.ac.uk/research/news/2017/02/27/autism-mooc/), thereby having international reach.
Next steps
It is important to us as a team that we make an active commitment to work with the key principlesand questions that have emerged for the autism and technology research field over the course ofthis two-year seminar series project. To that end, we have initiated a Call for Papers for a specialissue in Research in Autism Spectrum Disorders, entitled: “Look up! Digital technologies forautistic people to support interaction and embodiment in the real world”. This special issue will bepublished in 2018. We have also surveyed the attendees at the final seminar to establish theirpriorities for action (e.g. joint writing, joint projects) as well as their priorities for research, and wewill use this information as a starting point for conducting a survey with our wider group ofseminar participants to further inform the future research agenda. We will report on these findingsin due course. There have been numerous connections, activities, and projects undertaken as adirect result of people meeting each other at the seminars, and we hope that these ripples willcontinue to spread through and beyond this network. We will also be pursuing some of the ideasgenerated through the ASCmeI.T., app via workshops and small-scale projects with the aim ofbringing those ideas closer to reality. We would like to encourage any interested readers to get intouch and to watch this space (http://digitalbubbles.org.uk) for further developments.
References
Abbott, C. (2007), E-Inclusion: Learning Difficulties and Digital Technologies, Futurelab, Bristol, available at:www.nfer.ac.uk/publications/FUTL66 (accessed 11 July 2017).
Barnabear (2014), “A guided tour of autism and technology by Barnabear, Aspie and Software Engineer”,Digital Bubbles, 28 November, available at: http://digitalbubbles.org.uk/wp-content/uploads/2014/12/digital_bubbles_barnabear-Sem-1.pdf (accessed 27 February 2017).
Brosnan, M., Parsons, S., Good, J. and Yuill, N. (2016), “How can participatory design inform the design anddevelopment of innovative technologies for autistic communities?”, Journal of Assistive Technologies, Vol. 10No. 2, pp. 115-20.
Brosnan, M., Holt, S., Yuill, N., Good, J. and Parsons, S. (2017), “Beyond autism and technology: lessonsfrom neurodiverse populations”, Journal of Enabling Technologies, Vol. 11 No. 2, pp. 43-8.
Good, J., Parsons, S., Yuill, N. and Brosnan, M. (2016), “Virtual reality and robots for autism: moving beyondthe screen”, Journal of Assistive Technologies, Vol. 10 No. 4, pp. 211-16.
PAGE 118 j JOURNAL OF ENABLING TECHNOLOGIES j VOL. 11 NO. 3 2017
Good, J., Yuill, N., Parsons, S., Brosnan, M. and Austin, L. (2016), “Putting technology design into the handsof the users with the ASCmeI.T. App”, CHI 2016 Workshop on Autism and Technology: Beyond Assistanceand Intervention, San Jose, CA, available at: http://igw.tuwien.ac.at/chi16-autismtechnology/attachments/GoodEtAl.pdf (accessed 26 March 2017).
Milton, D. (2012), “On the ontological status of autism: the ‘double empathy problem’ ”, Disability and Society,Vol. 27 No. 6, pp. 883-7.
Mintz, J. (2013), “Can smartphones support inclusion for autism in mainstream?”, Journal of AssistiveTechnologies, Vol. 7 No. 4, pp. 235-42.
Parsons, S. (2015a), “Digital technologies for autism: moving past the headlines towards greater collaborationand partnership”, Blog post, 7 December, available at: www.autistica.org.uk/tech-for-autism/ (accessed26 March 2017).
Parsons, S. (2015b), “Learning to work together: designing a multi-user virtual reality game for socialcollaboration and perspective-taking for children with autism”, International Journal of Child-ComputerInteraction, Vol. 6, pp. 28-38.
Parsons, S., Yuill, N., Brosnan, M. and Good, J. (2015), “Innovative technologies for autism: critical reflectionson digital bubbles”, Journal of Assistive Technologies, Vol. 9 No. 2, pp. 116-21.
Parsons, S., Yuill, N., Brosnan, M. andGood, J. (2017), “Interdisciplinary perspectives on designing, understandingand evaluating digital technologies for autism”, Journal of Enabling Technologies, Vol. 11 No. 1, pp. 13-18.
Parsons, S., Yuill, N., Good, J., Brosnan, M., Austin, L., Singleton, C., Bossavit, B. and Barnabear (2016),“What technology for autism needs to be invented? Idea generation from the autism community via theASCmeI.T. App”, paper presented at the 15th ICCHP 2016 Conference, Linz, 13-15 July.
Ploog, B.O., Scharf, A., Nelson, D. and Brooks, P.J. (2013), “Use of computer-assisted technologies (CAT) toenhance social, communicative, and language development in children with autism spectrum disorders”,Journal of Autism and Developmental Disorders, Vol. 43 No. 2, pp. 301-22.
Shakespeare, T. (2006), “The social model of disability”, in Davis, L.J. (Ed.), The Disability Studies Reader,2nd ed., Routledge, Abingsdon, pp. 197-204.
Tunney, R. and Ryan, M. (2012), “Can iDevices help teaching assistants support pupils with ASD?”, Journal ofAssistive Technologies, Vol. 6 No. 3, pp. 182-91.
Wass, S.V. and Porayska-Pomsta, K. (2014), “The uses of cognitive training technologies in the treatment ofautism spectrum disorders”, Autism, Vol. 18 No. 8, pp. 851-71.
Yuill, N., Parsons, S., Good, J. and Brosnan, M. (2015), “Knowing me, knowing you: perspectives onawareness in autism”, Journal of Assistive Technologies, Vol. 9 No. 4, pp. 233-8.
Authors’ affiliations
Sarah Parsons is a Professor of Autism and Inclusion at the Southampton Education School,University of Southampton, Southampton, UK.
Nicola Yuill is a Senior Lecturer at the School of Psychology, University of Sussex, Sussex, UK.
Mark Brosnan is a Professor of Psychology at the Department of Psychology, University of Bath,Bath, UK.
Judith Good is a Reader in Informatics at the Department of Informatics, University of Sussex,Sussex, UK.
Corresponding author
Sarah Parsons can be contacted at: [email protected]
For instructions on how to order reprints of this article, please visit our website:www.emeraldgrouppublishing.com/licensing/reprints.htmOr contact us for further details: [email protected]
VOL. 11 NO. 3 2017 j JOURNAL OF ENABLING TECHNOLOGIES j PAGE 119

Emerald is excited to announce a recent partnership with Peerwith, a platform that provides authors with a variety of services.
The Emerald Peerwith site can be found here:https://authorservices.emeraldpublishing.com/
Peerwith connects academics seeking support for their work with a relevant expert to get their research submission-ready. Peerwith experts can help with the following: language editing, copy editing, scientific editing, translation services, statistical support, funding application support, visuals, video, publication support, literature search, peer review and indexing services. Authors post their assignments on the Peerwith site, experts provide a quote, and the fee and conditions are then agreed upon directly between the author and the expert.
While we are not, of course, guaranteeing publication upon use of Peerwith, we hope that being able to direct academics to this resource either before submission or during the peer review process will help authors further improve the quality of their papers and increase their chances of positive reviews and acceptance.
Academics with relevant expertise can sign up as an expert on the Peerwith system here:https://www.peerwith.com/services/offer
12750_PeerwithJournalAd_MF_v01.indd 1 01/03/2017 11:07:27

Certificate Number 1985ISO 14001
ISOQAR certified Management System,awarded to Emerald for adherence to Environmental standard ISO 14001:2004.
EDITORSarah ParsonsThe University of Southampton, UKE-mail [email protected]
DEPUTY EDITORJohn WoolhamKings College London, UKE-mail [email protected]
ASSOCIATE EDITORKevin DoughtyUniversity of York, UK
REVIEWS EDITORCheryl DobbsIndependent Consultant, Australia
ISSN 2398-6263© 2017 Emerald Publishing Limited
EDITORIAL BOARDChris AbbottKing’s College London, UKMaria BurtonSheffield Hallam University, UKDonna CowanChailey Heritage Clinical Services, UK Guy DewsburyThe Florence Nightingale School of Nursing and Midwifery, King’s College London, UK Paul DoyleHereward College, UKFern FauxNational Star College, UKMalcolm J. FiskCoventry University, UKKaren GuldbergUniversity of Birmingham, UKPetri IlmonenFinnish Association of Intellectual and Developmental Disabilities, FinlandWendy Keay-BrightCentre for Applied Research in Inclusive Arts and Design, Cardiff Metropolitan University
Martin KnappPersonal Social Services Research Unit (PSSRU), The London School of Economics, UK Jeremy LinskellNinewells Hospital, NHS Tayside, UK Katerina MavrouUniversity of Cyprus, CyprusKlaus MiesenbergerUniversity of Linz, AustriaMaurice MulvennaUniversity of Ulster, Ireland Nigel NewbuttUniversity of the West of England, UKSarah ParsonsUniversity of Southampton, UK Jeremy PorteusHousing Learning and Improvement Network, UKJane SealeOpen University, UKNick TylerUniversity College London, UK Tracey WilliamsonUniversity of Salford, UKPeter ZentelHeidelberg University Germany
Emerald Publishing LimitedHoward House, Wagon Lane, Bingley BD16 1WA, United KingdomTel +44 (0) 1274 777700; Fax +44 (0) 1274 785201E-mail [email protected] more information about Emerald’s regional offices please go to http://www.emeraldgrouppublishing.com/officesCustomer helpdesk :Tel +44 (0) 1274 785278; Fax +44 (0) 1274 785201E-mail [email protected], subscription and missing claims enquiries:E-mail [email protected] +44 (0) 1274 777700; Fax +44 (0) 1274 785201
Missing issue claims will be fulfilled if claimed within six months of date of despatch. Maximum of one claim per issue.Hard copy print backsets, back volumes and back issues of volumes prior to the current and previous year can be ordered from Periodical Service Company. Tel +1 518 537 4700; E-mail [email protected] For further information go to www.periodicals.com/emerald.htmlReprints and permissions serviceFor reprint and permission options please see the abstract page of the specific article in question on the Emerald web site (www.emeraldinsight.com), and then click on the “Reprints and permissions” link. Or contact: E-mail [email protected] Publisher and Editors cannot be held responsible for errors or any consequences arising from the use of information contained in this journal; the views and opinions expressed do not necessarily reflect those of the Publisher and Editors, neither does the publication of advertisements constitute any endorsement by the Publisher and Editors of the products advertised.No part of this journal may be reproduced, stored in a retrieval system, transmitted in any form or by any means electronic, mechanical, photocopying, recording or otherwise without either the prior written permission of the publisher or a licence permitting restricted copying issued in the UK by The Copyright Licensing Agency and in the USA by The Copyright Clearance Center. Any opinions expressed in the articles are those of the authors. Whilst Emerald makes every effort to ensure the quality and accuracy of its content, Emerald makes no representation implied or otherwise, as to the articles’ suitability and application and disclaims any warranties, express or implied, to their use.Emerald is a trading name of Emerald Publishing LimitedPrinted by CPI Group (UK) Ltd, Croydon, CR0 4YY
Journal of Enabling Technologiesis indexed and abstracted in:American Sociological Association Publishing Options Database,British Nursing IndexCINAHLCPA's AgeInfoCPA's New Literature on Old AgeIllustrataScopusSocial Care Online
Guidelines for authors can be found at:www.emeraldgrouppublishing.com/jet.htm

Access this journal onlinewww.emeraldinsight.com/loi/jet Volume 11 Number 3 2017
ISSN 2398-6263
Journal of
Enabling TechnologiesUser inclusion in health, support, social care and education
Volume 11 Number 3 2017
Contents
Journal of
Enabling Technologies User inclusion in health, support, social care and education
Number 3 73 Editorial
75 Researching telecare: the importance of contextKate Hamblin, Sue Yeandle and Gary Fry
85 A technology-aided program for helping persons with Alzheimer’s disease perform daily activitiesGiulio Lancioni, Nirbhay Singh, Mark O’Reilly, Jeff Sigafoos, Fiora D’Amico, Katia Pinto, Floriana De Vanna and Alessandro Caffò
92 Graphic symbols terminology: a call for a consensusEliada Pampoulou
101 Augmentative and alternative communication (AAC) training provision for professionals in EnglandSamantha Wallis, Steven Bloch and Michael Clarke
113 “A child with autism only has one childhood”: main themes and questions for research from the “Digital Bubbles” seminar seriesSarah Parsons, Nicola Yuill, Mark Brosnan and Judith Good