enamel mineralization disturbances in 12-year-old children with known early exposure to fluorides
TRANSCRIPT
Oral Epidemiology
Enamel mineralization disturbances in12-year-old children with known earlyexposure to fluoridesANNA-KARIN HOLM AND ROLAND ANDERSSON
Department of Pedodonties, University of Umed, Umed, and Department of Preventive Dentistry Publie Dental Health Serviee, County ofVdslernorrland, Sund.svatt, Sweden
Holm, A,-K. & Andersson, R.: Enamel riiineralizaliorr dislurbanccs in 12-yeaj'-old children withknown early exposur'e to lluorides. Community Dent. Oral Epidemiol, 1982: 10: 335-339.
.•\bsli'acl - Enamel changes and caries experience were studied in 134 12-year-old children wilh aknowrr early exposur'e to fluoride tablets and/or llrror'ide contairring toothpaste. The influence ofbirth weight and breast-feeding per'iod was also analyzed. A clinical intact enamel was found irr32% ofthe children. Enamel llrioiosis was fouird irr 45% and localized opacities or' hyjjoplasias in40 %. Childr'en who had corrsrirricd lluoride tablets for a period of at least 12 months from the age of6 months ran a 5.4 times greater risk of developirrg enamel lluorosis than children with no suchconsumption. No such r'isk could be shown in childr'en who at 6 or 12 rrronths of agestar'ted to usefluor'ide toothpaste. There was no statistically significant reduction in ihe prevalence of smoothsru'face car-ies or' fillirrgs in children with an exposure to flrroride tablets.
Key woi'ds: erianrcl lluorosis: (luoride lablels; fluoride toothpaste.
^-.1 Anrra-Kai'iri Holm. Departrrrerit of Pedodonlics, Norrlarrdsgatarr 18 B. S-902 48 Umea, Sweden.
Accei3ted for ])ublication 23 May 1982.
The Swedish National Board of Health and Wel-fare recommends parents to give their childrenfluoride tablets (0.25 mg F) v\'hen the Ouoridecontent of the dritiking water is low (Table 1). InUmea, a town iti the tiorth of Sweden whosedrinking water formerly had a fluoride content ol0.2 mg/1, children were thus recommended thehigher dosage shown in the Table. Recomtnenda-tions were given that the tablets should be taketi atthe same titne as toothbitishitig was perfortned,'which means mornitigs and/or evenings.
The use of fluotide toothpaste, is, however, notrecommended utitil the child is 4 years old based otithe assumption that at this age he can conttols-wallowing atid the enamel mineralization o^ thepermanent iticisots is nearly completed.
In a study performed by ANDER.SSON & GRAH-
NEN (1) no sigtiiftcant elfeel on enamel mineraliza-tion could be shown after an intake of Otioridetablets according to Swedish t-eeommendatiotis. Iti
eontrast, A.\,SENDEN & PEEBLE.S (2) and THVLSTRfPet al. (3) showed that early ttse of fluoride tabletsiticreased the pt-evalence of etiamel nuorosis.
Since then, new light has been shed upon theeffect of fluoride on etiamel formatioti (4) andfurthertnore a new classification system for fltioro-tic enatnel changes has been developed and de-scribed (3). In ot-der to collect mor-e detailedinfortnation on the eflect of the therapeutic dailydose of fluoride used in Sweden a group of 12-year-old children with a relatively well-known e.xposut-eto fltiorides was examined. The aim was to find otitif the exposut-e to fluorides, in the form of eithertablets or toothpaste or iti combinatioti, fiad led todisturbances in the mineralization of the enamel.Tfie aim was also to atialyze certain backgroitndfactot-s sue)] as the importance of a low birth weightand of a short bi-east-feeding period. Caries statuswas also included.
0301-.5661/82/060335-05 S02.50/0 «- 1982 Munksgaard, Copenhagen
336 HOLM AND ANDERSSON
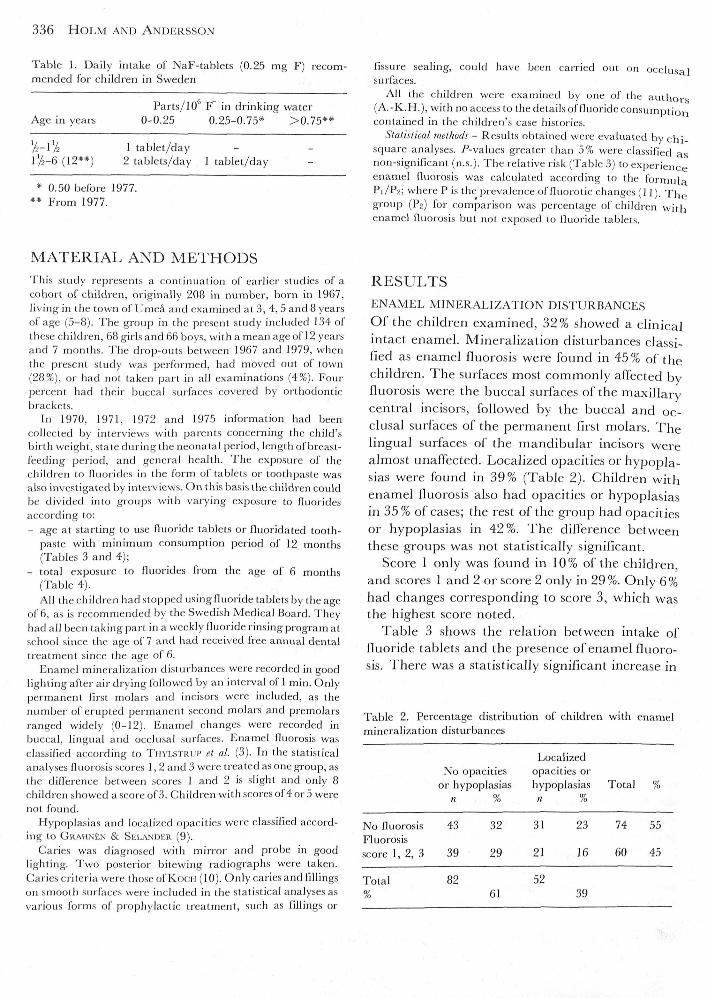
Table I. Daily intake of NaF-tablets (0.25 mg F) recom-mended for children in Sweden
Parts/10 F in drinking waterAge in years 0-0.25 0.25-0.75* >0.75**
/^-l/^ 1 tablet/day172-6 (12**) 2 tablets/day I tablet/day
* 0.50 before 1977.** From 1977.
fissure sealing, could have been carried out on occhi.salsurfaces.
All the children were exar-nined by one of the authors(A.-K.H.), with no access to the details of lluoride consurnptioncontained in the children's case histories.
Statisticat methods - Results obtained were evaluated by chi-square analyses, /"-values greater than 5% were classified asnon-significant (n.s.). The relative risk (Table 3) to exper-ienceenamel fluorosis was calculated according to the formulaPr/P2; where Pis the pr-evalence offluorotic charrges (11), Thegroup (P2) for compar'ison was per'centage of children withenamel fluorosis but nol exposed to fluoride tablets.
MATERIAL AND METHODSThis study repre.sents a continuation of earlier studies of acohort of children, originally 208 in number, born in 1967,living in the town of Umea and examined at 3, 4, 5 and 8 yearsof age (5-8). The group in the present study included 134 ofthe.se childr-en, 68gir-lsand 66 boys, with a mean age of 12 year-sand 7 months. The dr-op-outs between 1967 and 1979, whenthe present study was perfor-med, had moved out of town(28%), or had not taken part in all examinations (4%). Fourpercent had their buccal surfaces covered by orthodonticbrackets.
In 1970, 1971, 1972 and 1975 information had beencollected by interviews with parerrls concerning the child'sbirth weight, state during the neonatal period, length of breast-feeding period, and general health. The exposure of thechildren to fluorides in the form of tablets or toothpaste wasalso investigated by interviews. On this basis the children couldbe divided into groups with varying exposure to fluor'idesaccording lo:- age at starting to use fluoride tablets or fluoridated tooth-
paste with minimum consumption period of 12 months(Tables 3 and 4);
- total exposure to fluorides from the age of 6 months(Table 4).All the children had stopped using fluoride tablets by the age
of 6, as is r-ecommerrded by the Swedish Medical Board. Theyhad all been taking part in a weekly lluoride rinsing progr'am atschool since the age of 7 and had received free annual dentaltreatment since the age of 6.
Enamel mineralization disturbances were recorded in goodlighting after air drying followed by an interval of 1 min. Onlypermanent fir'st molars and incisors were included, as thenumber of erupted perrrranent second molars and premolarsranged widely (0-12). Enamel changes were recorded inbueeal, lingual and occlu.sal surfaces. Enamel fluorosis wasclassified according to THVLSTRLIP et al. (3), In the statisticalanaly.ses Ilrrorosis scores 1, 2 and 3 were treated as one gr'oup, asthe diller'cnce between scor'es 1 and 2 is slight and only 8children showed ascoreof3. Children with scores ol 4 or 5 werenot found.
Hypoplasias and localized opacities were classified accord-ing to GRAHN£N & SELANDER (9).
Caries was diagnosed with mirror and probe in goodlighting. Two posterior bitewing radiographs wer'e taken.Caries cr'iteria were those of K(x:it (10). Only caries and fillingson smooth surfaces were included in the statistical analyses asvarious forms of prophylactic treatment, such as fillings or
RESULTSENAMEL MINERALIZATION DLSTURBANCES
Of the children examined, 32% showed a clinicalintact enamel. Mineralization disturbanees classi-fied as enamel fluorosis were found in 45 % of thechildt-en. The suifaces most commonly affected byfluotosis were the buccal surfaces ofthe maxillarycentral incisors, followed by the buccal and oc-clusal sutfaces of the permanent fit-st molars. Thelingual surfaces of the mandibular incisors wet-ealmost unaffected. Localized opacities or hypopla-sias were found in 39% (Table 2). Childt-en withenamel fluorosis also had opacities or hypoplasiasin 35 % of cases; the rest of the group had opacitiesor hypoplasias in 42%. The difference betweenthese groups was not statistically significant.
Score 1 only was found in 10% ofthe childreti,and scores 1 and 2 or score 2 only in 29%. Only 6%had changes corresponding to score 3, which wasthe highest score noted.
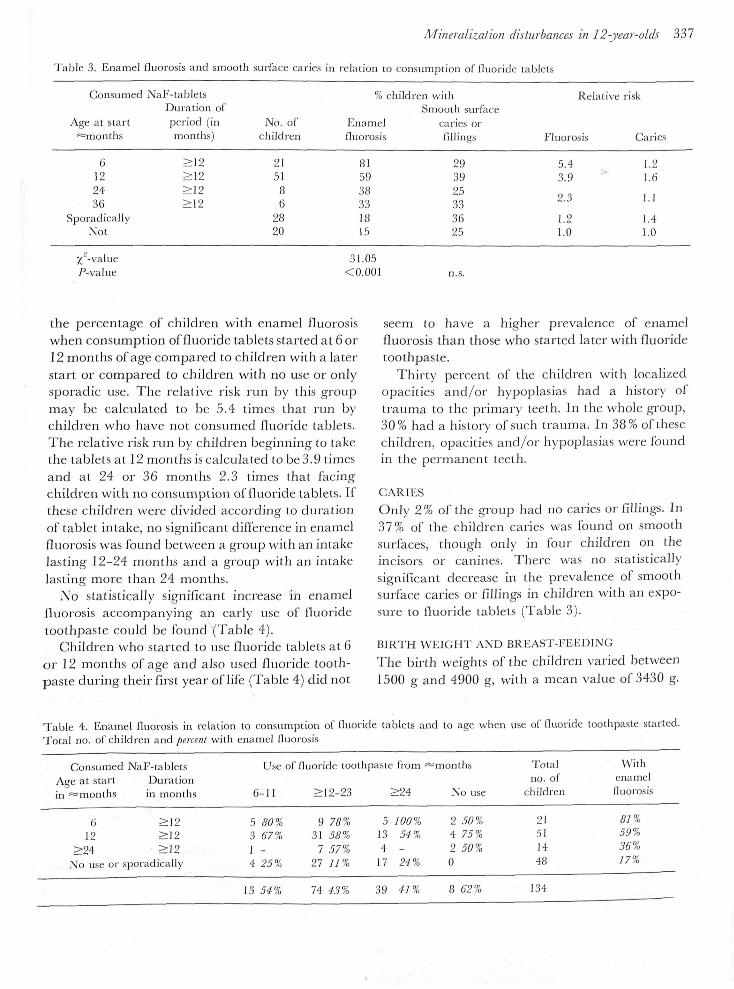
Table 3 shows the relation between intake offluoride tablets and the presence of enamel fluoro-sis. There was a statistically significant increase in
Table 2. Percentage distribution of children with enamelmineralization disturbances
LocalizedNo opacities opacities or
or hypoplasias hypoplasias Total %n % n %
No fluorosisFluorosisscore 1, 2, 3
43
39
32
29
31
21
23
16
74
60
55
45
Total 82 5261 39
Mineralization disturbances in 12-year-olds 337
Table 3. Enamel lluor-osis and srrrooth surface caries in relatiorr to corrsumptiorr ol'lluor'ide tablet.s
Consumed
Age at start^months
6122436
SporadicallyNot
x'-vahre/^-value
NaF-tabletsDuration ofper'iod (inmonths)
>12>12
>r2
No. ofehildren
215186
2820
% child
Enamelfluorosis
8159
' 3 833IS15
31.05<0.001
Iren withSmooth sur'face
caries orfillings
293925333625
n.s.
Relative
Fluor'osis
5.43.9
2.3
1.21.0
risk
Caries
1.21.6
1.1
1.41.0
the percentage of children with enamel fluorosiswhen consumption of fluoride tablets started at 6 or12 months of age eompared to children with a laterstart or compared to children with no use or onlysporadic use. Tfie relative risk run by this gt-oupmay be calculated to be 5.4 times that run bycfiildten wfio have not consumed fluotide tablets.The relative risk ritn by childt-en beginning to takethe tablets at 12 months is calculated to be 3.9 timesand at 24 or 36 motiths 2.3 times that facingchildren with no consumption of fluoride tablets. Ifthese children were divided according to durationof tablet intake, no significant difference in enamelfluorosis was found between a grottp with an intakelasting 12-24 months and a group with an intakefasting more than 24 months.
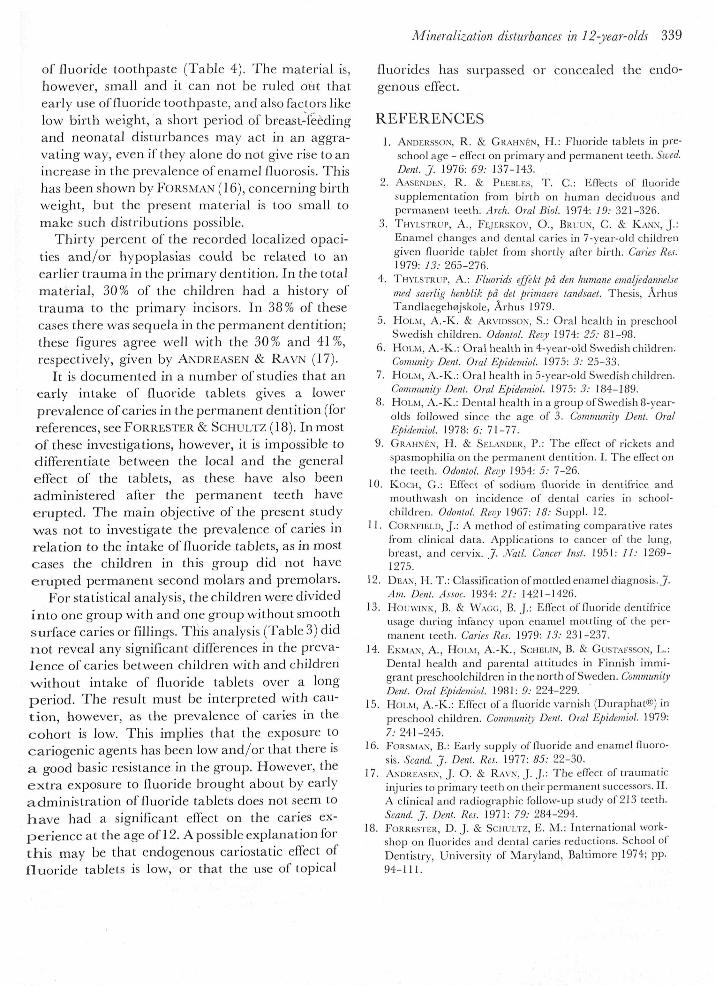
No statistically significant increase in enamellluorosis accompanying an early use of fluoridetoothpaste could be found (Table 4).
Children who started to use fluoride tablets at 6or 12 montfis of age and also used fltioride tooth-paste during their first year of life (Table 4) did not
seem to have a higher prevalence oi enamelfluorosis than those who started later with fluoridetoothpaste.
Thirty percent of the children with localizedopacities and/or hypoplasias had a history oftrauma to the primai-y teeth. In the whole gt-oup,30% had a history of such trauma. In 38% of thesechildt-en, opacities and/or hypoplasias were fbundin the permanent teeth.
CARIESOnly 2% of the group had no caries or fillings. In37% of the children caries was found on smoothsurfaces, though only in four children on theincisors or canines. There was no statisticallysignificant decrease in the prevalence of smoothsurface caries or fillings in children with an expo-stare to lluoride tablets (Table 3).
BIRTH WEIGHT AND BREAST-FEEDINCThe birth weights of the children varied between1500 g and 4900 g, with a mean value of 3430 g.
Table 4. Enamel fluorosis in relation to consumption of fluoride tablets and to age when use of fluoride toothpaste started.Total no, of childr'en and pereent with enamel fluor'osis
Consumed NaF-tabletsAge at start Durationin =monlhs ir-r months
Use of fluor'ide toothpaste from
6-11 >12-23 >24 Notr.se
Totalno. of
children
Withenamelfluorosis
612
>24No use
>J2>12
, , -ai:2:,. ' ' / •" •or sporadically
53I4
80%67%_25%
931
727
78%58%57%11%
5134
17
100%54%-24%
2420
50%75%50%
215114,48
81%59%36%17%
13 54% 74 43'! 39 41 % 8 62% 134

338 HOLM AND ANDERSSON
The length of the breast-feeding period variedbetween 0 and 8 months, with an average of 1.8months. Sixty-nine percent had been breast-fed foronly 1-3 months and 16% were entirely bottle-fed.There was no statistically significant relationshipbetween birth weight and prevalence of enamelfluorosis or prevalence of opacities and hypoplasias,nor could any such relationship be shown betweenprevalence of enamel fluorosis and period of breast-feeding. The number of children wilh variousneonatal disturbances stich as temporary asphyxiaor icterus did not differ significantly betweengroups with and without enamel fluorosis.
DISCUSSIONThe estimate of the time ofthe children's exposureto fluorides may be regarded as reasonably reliablein this study because the repeated interviews madeit possible to check more carefully the veracity ofthe parents' information than would otherwisehave been the case. The effect of lapses of memoryhas also been reduced.
Recording and classification of enamel mineral-ization disturbances entails manifest methodologieproblems. As the extent of the mineralizationdisturbances which might occur with the fluorideconsumption involved here was considered small,the index proposed by DEAN (12) was not regardedas sufficiently sensitive and discriminatory. How-ever, by utilizing the index of THYLSTRUP et al. (3)even minor changes involving perikymata pat-terning are included. This may be one explanationfor the fact that children who had not had an intakeof fluoride tablets or used fluoride toothpaste alsodisplayed mineralization disturbances which wereclassified as enamel fluorosis (Table 3).
There are also difficulties in reliably and cor-rectly classifying and differentiating betweenchanges representing score 1 and score 2. There-fore, the material was divided for statistical analysisinto one group with fluorosis (scores 1, 2 and 3) andone group without fluorosis, in order to give greaterreliability. We thus excluded the possibility ofdetermining whether a longer period of tabletconsumption would increase the severity of thechanges. However, this question, too, is of minorimportance with the slight changes involved.
The results point to a positive correlation be-tween exposure to fluoride tablets and the occur-
rence of enamel iluorosis. Children who receivedtablets from the age of 6 months appeared to beparticularly liable to experience such changes(Table 3).
These observations support those published ear-lier by THVLSTRUP et al. (3). In an earlier retro-spective Swedish study (1), no significant differencewas found in the occurrence of enamel fluorosisbetween a group which had taken fluoride tabletsfor 4-5 years starting at 6 months of age, and acontrol group. In that study, however, the indexused was that of DEAN (12), according to which theoccurrence of perikymata patterning correspond-ing to score 1 as defined by THYLSTRUP et al. (3) isnot counted as dental fluorosis. The changes in theenamel found in the present study consist largely ofjust such perikymata patterning (scores 1 and 2)and may in the main be taken as evidence that theintake of even small amounts of fluorides appears tohave an effect on the mineralization ofthe enamel.No aesthetic judgment of the appearance of theenamel has been made.
The results of this study seem to show that earlyuse of fluoride containing toothpaste does notinduce elinieal changes ofthe enamel. This findingis in accordance with recent observations by Hou-wiNK & WAGG (13), who found no "hypoplasia ormottling" in teeth of 7-10-year-old children afterregular use of 2% sodium monofluorophosphatetoothpaste during the mineralization period ofthepermanent teeth. Thus the results from the presentstudy do not seem to support the recommendationsfrom the Swedish Medical Board that fluoridetoothpaste should not be used until the child is 4years old. The fact that as many as 94% of thechildren used such toothpaste before the age of 4years, despite the recommendations given, showsthat it is not practical to expect families withchildren to use toothpastes of different types. Thatfluoride toothpaste is also used by children youngerthan 4 years old had been confirmed by otherstudies (14, 15). The high number of children withenamel fluorosis among those who did not usefluoride toothpaste at all may be explained by thehigh number of fluoride tablet users in this group(100%).
When early start with fluoride tablets and eat-lyuse of fluoride toothpaste coincided, the prevalenceof enamel fluorosis was not higher than in the groupof children who had a somewhat later start with use
Mineralization disturbances in 12-year-olds 339
of fluoride toothpaste (Table 4). The material is,however, small and it can not be ruled out thatearly use of fluoride toothpaste, and also factors likelow birth weight, a short period of breast-feedingand neonatal disturbances may act in an aggra-vating way, even if they alone do not give rise to anincrease in the pt-evalence of enamel fluorosis. Thishas been shown by FORSMAN (16), concerning birthweight, but the present material is too small tomake such distributions possible.
Thirty percent of the recorded localized opaci-ties and/or hypoplasias could be related to anearlier trauma in the primaty dentition. In the totalmaterial, 30% of the children had a history oftrauma to the primary incisors. In 38% of theseeases thet-e was sequela in the permanent dentition;these figures agree well with the 30% and 41%,respectively, given by ANDREASEN & RAVN (17).
It is documented in a number of studies that anearly intake of fluoride tablets gives a lowerprevalence of caries in the permanent dentition (forreferences, see FORRESTER & SGHULTZ (18). In mostof these investigations, however, it is impossible todifferentiate between the local and the generaleffect of the tablets, as these have also beenadministered after the permanent teeth haveerupted. The main objective of the present study-was not to investigate the prevalence of caries inrelation to the intake of fluoride tablets, as in mostcases the children in this group did not haveerupted permanent second molars and premolars.
For statistical analysis, the children were dividedinto one group with and one group without smoothsurface caries or fillings. This analysis (Table 3) didnot reveal any significant differences in the preva-lence of caries between children with and children-without intake of fluoride tablets over a longperiod. The result must be interpreted with cau-tion, however, as the prevalence of caries in thecohort is low. This implies that the exposure tocariogenic agents has been low and/or that there isa good basic resistance in the gt-oup. However, theextra exposure to fluoride brought about by earlyadministration of fiuoride tablets does not seem tohave had a significant effect on the caries ex-perience at the age of 12. A possible explanation forthis may be that endogenous cariostatic effect offluoride tablets is low, or that the use of topical
fiuorides has surpassed or concealed the endo-genous effect.
REFERENCES1, ANDI;R,S,SON, R . & CRAHMC.V, H . : Fluor-ide tablets in pr-e-
sehool age - eflect or-r primary and permanent teeth. Swed.Dent. J. 1976: 69: 137-143.
2. A.vsENUtiN, R. & Pta-.Bi.i-s, T. C : EfTects of fluoridestrpplemei'rtation Ir'om bir'th on htrmari deeiduotrs andpermanent teeth. Arch. Orat Bioi. 1974: 19: 321-326.
3. THVi.si'tiUP, A., Fi;|ERSKo\', O., BRiai.v, C. & K.VN.N, J.:Enamel changes and dental caries in 7-year'-oId childrengiven lluoride tablet fr-om shoi'tly after birth. Caries Res.1979: 13: 265-276.
4. TH\L.s'rRt>P, A.: Ftuorids effekt pd den humane emaljedannelsemed saerlig henblik pd det primaere tandsaet. Thesis. ArlrusTandlaegehojskole, Arhus 1979.
5. H()t.i\i, A.-K. & ARVtDS.soN, S.: Or-al health in pre.schoolSwedish children. Odontol. Revy 1974: 25: 81-98.
6. HOLM, A.-K.: Oral health in 4-year-old Swedish childr-en.Comunity Dent. Oral Epidemiol. 1975: .?.• 25-33.
7. HOLM, A , - K , : Or'al health in 5-year'-old Swedish childr'en.Community Dent. Oral Epidemiol. 1975:.?.' 184-189,
8. HOLM, A.-K,: Dental health irr a group of Swedish 8-year'-olds followed since the age oi 3. Community Dent. OralEpidemiol. 1978: 6: 11-11.
9. GR.AHNEN, H . & Sia.ANDicu. P.: The elTect of r-ickets andspasrnophilia on the permanent dentition. I. The eflect onthe teeth. Odontol. Revy 1954: 5: 7-26.
10. K<1CH, G.: Eflect of sodium fluoride in dentifrice andmouthwash on incider-rce of dental caries ir-r school-children. Odontot. Revy 1967: 18: Suppl. 12.
11. CORNFIELD, J.: A method of estimating comparative r-atesfr-om clinical data. Applications to cancer of the lung,br'east, and cervix. J. .Natl. Caneer Inst. 1951: //, ' 1269-1275.
12. DE,A\, H , T , : Classifrcatiorr of mottled enamel diagnosis. ,7..•im. Dent. As.soc. 1934: 21: 1421-1426.
13. HotiwtNK, B. & WAGG, B. J.: Eflect of fluoride dentifr'iceirsage durirtg infancy upon enamel mottlir-rg of the per-manent teeth. Caiies Res. 1979: 13: 231-237.
14. EisNtAN, A., HoL.\t, A.-K., SCHELIN, B, & GtisTAF,ssoN, L.:Dental health and par-ental attitudes in Finnish immi-gr-ant pr-eschoolchildren in the north of Sweden. CommunityDent. Oral Epidemiol. 1981: 9: 224-229.
15. HOLM, A.-K.: ElTect of a fluoride varnish (Duraphat®) inpr'eschool childr'en. Community Dent. Orat Epidemiot. 1979:
7.'241-245.16. F0R.SMAN, B.: Early supply of fluoride and enamel fluoro-
sis. Seand J . Dent^ Res. 1977: 85: 22-30.17. ANDREA.SEN, J. O. & RAVN, J. J.: The eflect of traumatic
injuries to primar-y teeth on their permanent successors. II.A clinical and radiographic follow-up study of 213 teeth.Seand J. Dent. Res. 1971: 79: 284-294.
18. FoRRra'rER, D. J, & SctttJLrz, E. M.: International work-shop on fluorides and dental caries redrrctions. School ofDentistr'y, Univer'sity of Maryland, Baltimor-e 1974; pp.94-111. '
