endocardium in wolff-parkinson-white syndrome type a, with and
TRANSCRIPT
British Heart Journal, I973, 35, 594-600.
Arrival of excitation at right ventricular apicalendocardium in Wolff-Parkinson-White syndrometype A, with and without right bundle-branch block'
Cesar A. Castillo, Agustin Castellanos, Jr., B. Befeler, Robert J. Myerburg,Abdul S. Agha, and M. Celeste VagueiroFrom the Cardiovascular Laboratory, Veterans Administration Hospital, and the Division of Cardiology,Department of Medicine, University of Miami School of Medicine, Miami, Florida, U.S.A.
Filtered bipolar right ventricular apical (RVA) and His bundle electrograms, using electrodes only i mm
apart, were recorded in two patients with intermittent WPW type A with and without 'complete' rightbundle-branch block. In beats with exclusive normal pathway conduction and 'complete' right bundle-branchblock, the HV and V-RVA intervals represented His-to-left ventricular endocardial and left ventricularendocardial-RVA conduction times, respectively. The H-RVA interval was determined by addition of thesetwo intervals. In 'fusion' beats resulting from AV conduction through both normal and accessory pathways,the duration of the H-RVA interval was similar to that of beats with exclusive normal pathway conduction,suggesting that though the ventricles were pre-excited through an accessory pathway the RVA was stillactivated via the impulse emerging from the right bundle-branch. In beats with exclusive, or predominant,accessory pathway conduction and a WPW type A morphology, the H-RVA 'interval' was 'shorter-than-normal', suggesting that the RVA was not activated by the impulse traversing the normal pathway but bythe one propagating from the pre-excited site. The corresponding V-RVA intervals (giving a rough estimateof conduction time from pre-excited site to RVA) were longer (Iio and I20 msec, respectively) than in twoother patients with WPW type B. Intracardiac recordings have enhanced our knowledge of the ventricularactivation process in WPW type A, either pure or associated with 'complete' right bundle-branch block.
The diagnosis of right bundle-branch block inpatients with Wolff-Parkinson-White syndrome(WPW) has been a subject of considerable debateand speculation (Pick and Fisch, I958; Robertsonet al., I963; Laham, I969; Schamroth, I97i). Theintroduction of specialized techniques for obtainingintracardiac electrograms has offered a new ap-proach to the analysis of ventricular pre-excitation.This will be shown in the present communicationwhich deals with the arrival of excitation at severalrecording sites in patients having WPW type Aassociated with persistent, or intermittent, 'com-plete' right bundle-branch block.
Subjects and methodsThe technique for obtaining His bundle and local ven-
Received 8 November I972.1 This study was supported in part by Institutional ResearchFunds (Part II) provided by the Veterans AdministrationHospital, Miami, Florida, U.S.A.
tricular electrograms used in our department has beendiscussed in other communications (Castellanos, Cas-tillo, and Myerburg, I97I; Castellanos and Castillo,I972; Castellanos et al., I972a). After explaining theprocedure and obtaining consent from the patient,catheter electrodes were introduced to stimulate thehigh right atrium and to record from the His bundlearea and the right ventricular apex (RVA). Filtered(4o-400 Hz), bipolar electrograms, using electrodes imm apart, were obtained simultaneously with leads I,II, III, and Vi, at paper speeds of ioo mm/sec. Datafrom two patients withWPW type A in whom 'complete'right bundle-branch block also occurred will be pre-sented.The significance and duration of the various intervals
measured are discussed in the corresponding casedescription.
Case IFour types of beats were observed in this 22-year-oldman with intermittent WPW type A. These respectivelyresulted from: (a) exclusive normal (AV) pathway con-
Arrival of excitation at right ventricular apical endocardium 595
A _II
III
VI
H St
HBE in wmi -LRA . LRA
RVA
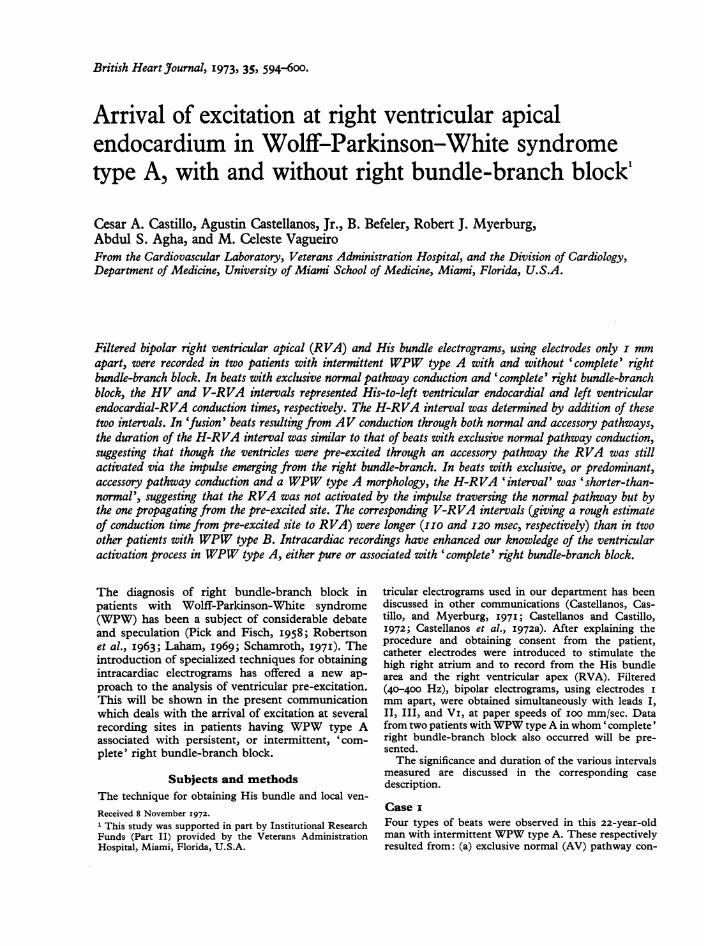
FIG. I Case i. Surface and intracardiac recordingsduring exclusive conduction through the normal AVpathway. The duration and significance of intervalsmeasured from this beat are shown in Table i. HBE,His (H) bundle bipolar electrogram; RVA, right ven-tricular apical bipolar electrogram; St, electric stimu-lus (delivered to the high right atrium).
In this, and all Figures, paper speed was IOOmm/sec.
.'iL
H '
4. -A ..-
o
V.Vlr
__
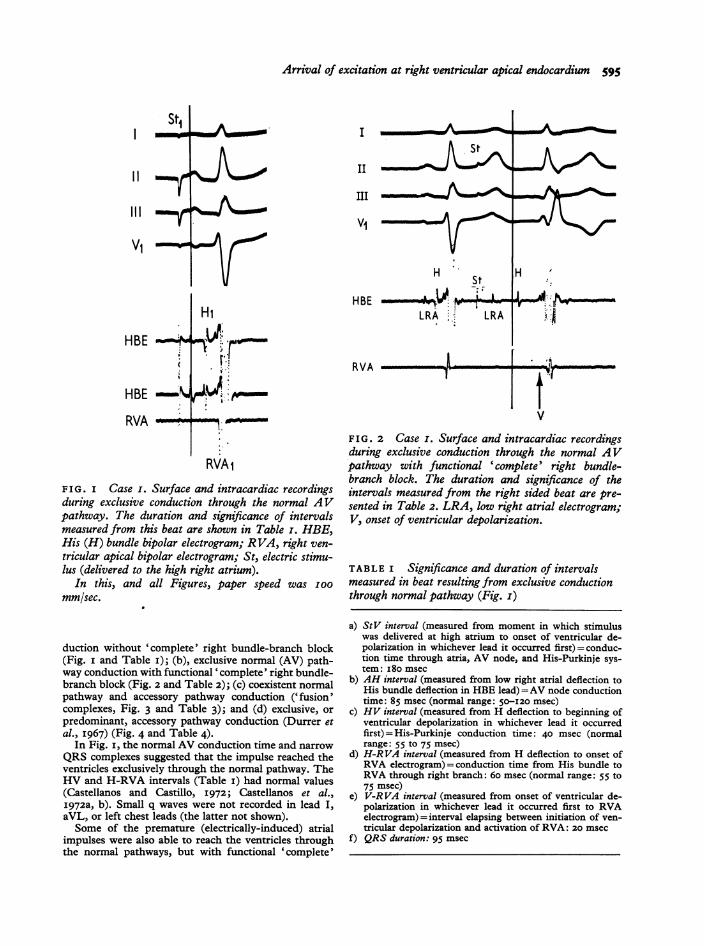
FIG. 2 Case i. Surface and intracardiac recordingsduring exclusive conduction through the normal AVpathway with functional 'complete' right bundle-branch block. The duration and significance of theintervals measured from the right sided beat are pre-sented in Table 2. LRA, low right atrial electrogram;V, onset of ventricular depolarization.
TABLE i Significance and duration of intervalsmeasured in beat resulting from exclusive conductionthrough normal pathway (Fig. i)
duction without 'complete' right bundle-branch block(Fig. I and Table i); (b), exclusive normal (AV) path-way conduction with functional 'complete' right bundle-branch block (Fig. 2 and Table 2); (c) coexistent normalpathway and accessory pathway conduction ('fusion'complexes, Fig. 3 and Table 3); and (d) exclusive, orpredominant, accessory pathway conduction (Durrer etal., I967) (Fig. 4 and Table 4).
In Fig. i, the normal AV conduction time and narrowQRS complexes suggested that the impulse reached theventricles exclusively through the normal pathway. TheHV and H-RVA intervals (Table i) had normal values(Castellanos and Castillo, I972; Castellanos et al.,I972a, b). Small q waves were not recorded in lead I,aVL, or left chest leads (the latter not shown).Some of the premature (electrically-induced) atrial
impulses were also able to reach the ventricles throughthe normal pathways, but with functional 'complete'
a) StV interval (measured from moment in which stimuluswas delivered at high atrium to onset of ventricular de-polarization in whichever lead it occurred first) = conduc-tion time through atria, AV node, and His-Purkinje sys-tem: i8o msec
b) AH interval (measured from low right atrial deflection toHis bundle deflection in HBE lead) =AV node conductiontime: 85 msec (normal range: 50-120 msec)
c) HV interval (measured from H deflection to beginning ofventricular depolarization in whichever lead it occurredfirst) = His-Purkinje conduction time: 40 msec (normalrange: 55 tO 75 msec)
d) H-RVA interval (measured from H deflection to onset ofRVA electrogram)=conduction time from His bundle toRVA through right branch: 60 msec (normal range: 55 to75 msec)
e) V-RVA interval (measured from onset of ventricular de-polarization in whichever lead it occurred first to RVAelectrogram)=interval elapsing between initiation of ven-tricular depolarization and activation of RVA: 20 msec
f) QRS duration: 95 msec
I_
IIIlit --rVH
HBE ;
RVA
Hi
2:r.RVA
..
RVAi
56 Castillo, Castellanos, Befeler, Myerburg, Agha, and Vagueiro
TABLE 2 Significance and duration of intervalsmeasured in beat resulting from exclusive AV con-duction through normal pathway with functional' complete' right bundle-branch block (Fig. 2)
a) StV interval= 3 I0 msecb) AH interval= I50 msecc) HV interval= conduction time from His bundle to left
ventricular endocardium through left bundle system: 120msec
d) V-RVA interval=conduction time from left ventricularendocardium to right ventricular endocardium (RVA)through septum: 55 msec
e) H-RVA interval=HV interval (I20 msec) +V-RVA inter-val (55 msec): I75 msec
f) QRS duration = I 50 msec
ST2I r\_
IIIVI o_p
ViWNV1Kr
HBE -W..
HBE
RVA mm
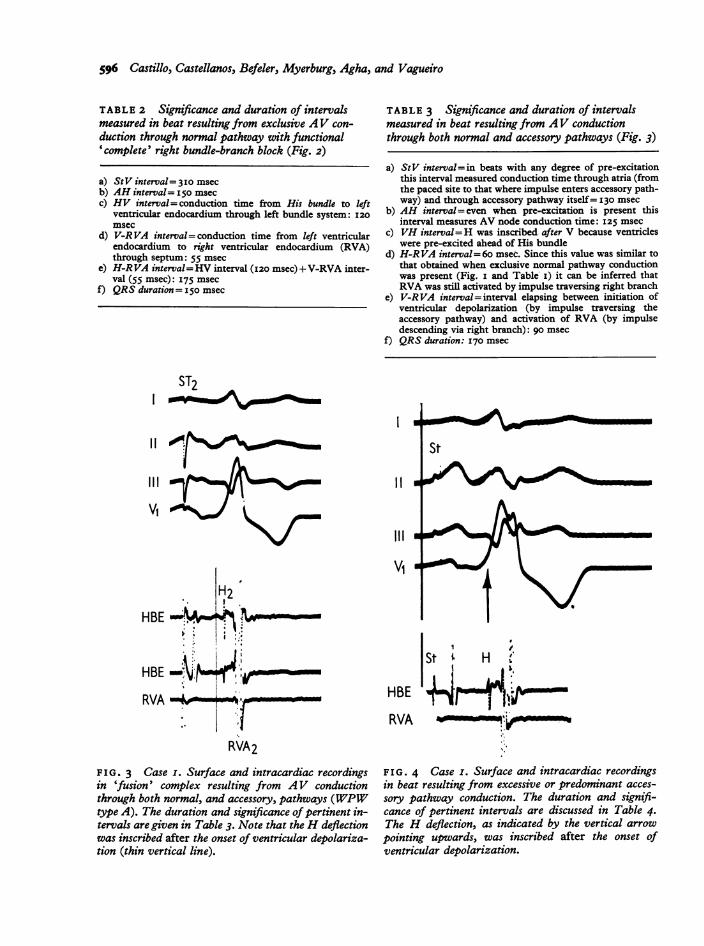
TABLE 3 Significance and duration of intervalsmeasured in beat resulting from AV conductionthrough both normal and accessory pathways (Fig. 3)
a) StV interval= in beats with any degree of pre-excitationthis interval measured conduction time through atria (fromthe paced site to that where impulse enters accessory path-way) and through accessory pathway itself= 130 msec
b) AH interval=even when pre-excitation is present thisinterval measures AV node conduction time: I25 msec
c) VH interval=H was inscribed after V because ventricleswere pre-excited ahead of His bundle
d) H-RVA interval= 60 msec. Since this value was similar tothat obtained when exclusive normal pathway conductionwas present (Fig. i and Table i) it can be inferred thatRVA was still activated by impulse traversing right branch
e) V-RVA interval=interval elapsing between initiation ofventricular depolarization (by impulse traversing theaccessory pathway) and activation of RVA (by impulsedescending via right branch): go msec
f) QRS duration: I70 msec
I. ;St; H .
HBE 4 i-RVA - W,-
FIG. 4 Case I. Surface and intracardiac recordingsin beat resulting from excessive or predominant acces-sory pathway conduction. The duration and signifi-cance of pertinent intervals are discussed in Table 4.The H deflection, as indicated by the vertical arrowpointing upwards, was inscribed after the onset ofventricular depolarization.
11
III
VIH2
.
I :,'
I_
RVA2
FIG. 3 Case I. Surface and intracardiac recordingsin 'fusion' complex resulting from AV conductionthrough both normal, and accessory, pathways (WPWtype A). The duration and significance of pertinent in-tervals are given in Table 3. Note that the H deflectionwas inscribed after the onset of ventricular depolariza-tion (thin vertical line).
I
Arrival of excitation at right ventricular apical endocardium 597
TABLE 4 Significance and duration (msec) ofintervals measured in beat resulting from exclusive orpredominant accessory pathway conduction (Fig. 4)
a) StV interval* = 130 msecb) AH interval*= I50 msecc) VH interval* =H was inscribed after V because ventricles
were pre-excited ahead of His bundled) H-RVA interval= differences between activation time of
bundle (by impulse traversing the AV node) and RVA: 45msec
Since this interval was shorter than normal (6o msecin Fig. I and Table i), RVA could not have been depolar-ized by impulse descending through right branch. HenceRVA was most probably activated by impulse propagatingfrom pre-excited area
Therefore:e) The V-RVA interval of iIo msec represented conduction
time from pre-excited area to RVAf) QRS duration: i85 msec
* As defined in Table 3.
right bundle-branch block and prolonged AV conduc-tion time (Fig. 2). The HV interval measured I20 msec
(Table 2), suggesting that there was an associated con-
duction delay through the left bundle system.Fig. 3 shows a 'fusion' complex (with WPW type A
morphology) which occurred when the atrial impulsereached the ventricles through both normal and acces-sory pathways. This diagnosis was suggested, as shownin Table 3, by: (a) shortening of the StV interval;(b) increase in QRS duration with appearance of a deltawave; (c) inscription of the H deflection after the onsetof ventricular depolarization (Castillo and Castellanos,I970), and (d) H-RVA interval similar to that in normalbeats.The slightly wider QRS complex shown in Fig. 4
had a similar (short) StV interval. Though the mor-
phology in lead Vi resembled that of 'complete' rightbundle-branch block, inscription of the H deflectionafter the beginning of ventricular depolarization sug-gested that this beat resulted from exclusive, or pre-dominant, accessory pathway conduction (Durrer et al.,I967). Due to the reasons discussed in Table 4, it wasassumed that the RVA was not activated from the rightbranch but from the pre-excited area.
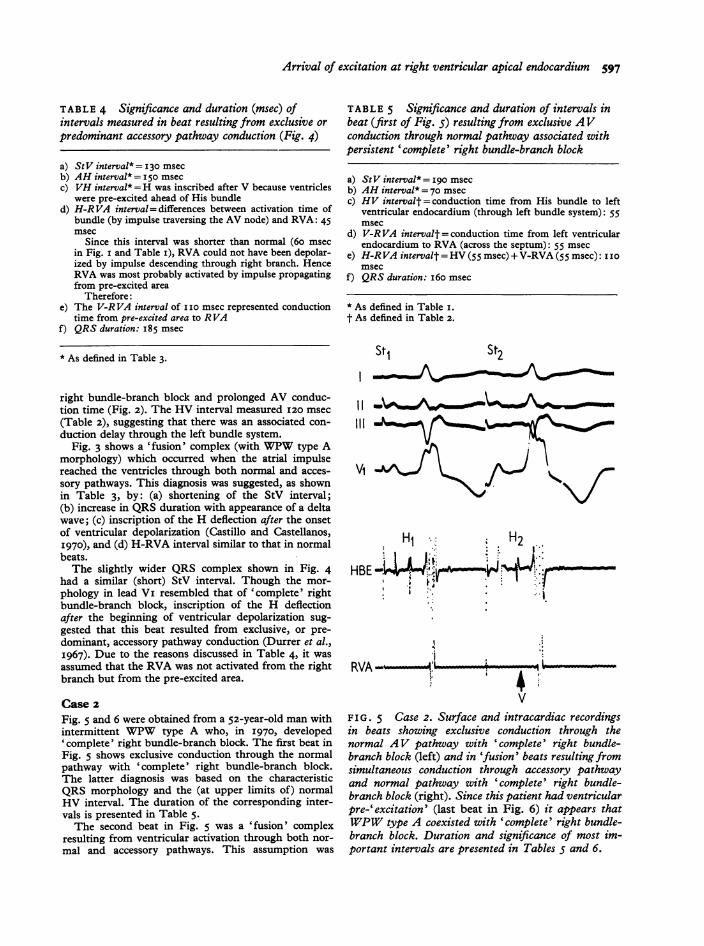
Case 2Fig. 5 and 6 were obtained from a 52-year-old man withintermittent WPW type A who, in I970, developed'complete' right bundle-branch block. The first beat inFig. 5 shows exclusive conduction through the normalpathway with 'complete' right bundle-branch block.The latter diagnosis was based on the characteristicQRS morphology and the (at upper limits of) normalHV interval. The duration of the corresponding inter-vals is presented in Table 5.The second beat in Fig. 5 was a 'fusion' complex
resulting from ventricular activation through both nor-
mal and accessory pathways. This assumption was
TABLE 5 Significance and duration of intervals inbeat (first of Fig. .5) resulting from exclusive AVconduction through normal pathway associated withpersistent 'complete' right bundle-branch block
a) StV interval*= I90 msecb) AH interval* = 70 msecc) HV intervalt= conduction time from His bundle to left
ventricular endocardium (through left bundle system): 55msec
d) V-RVA intervalt= conduction time from left ventricularendocardium to RVA (across the septum): 55 msec
e) H-RVA intervalt =HV (55 msec) + V-RVA (55 msec): i Iomsec
f) QRS duration: i6o msec
* As defined in Table i.t As defined in Table 2.
St, St2
VI
HlHBE444S
I...
RVA 4;L ;
FIG. 5 Case 2. Surface and intracardiac recordingsin beats showing exclusive conduction through thenormal AV pathway with 'complete' right bundle-branch block (left) and in 'fusion' beats resulting fromsimultaneous conduction through accessory pathwayand normal pathway with 'complete' right bundle-branch block (right). Since this patient had ventricularpre-'excitation' (last beat in Fig. 6) it appears thatWPW type A coexisted with 'complete' right bundle-branch block. Duration and significance of most im-portant intervals are presented in Tables 5 and 6.
598 Castillo, Castellanos, Befeler, Myerburg, Agha, and Vagueiro
TABLE 6 Significance and duration (msec) ofintervals measured in beat (last in Fig. 5) resultingfrom AV conduction through both normal (withcomplete right bundle-branch block) and accessorypathways
a) StV interval* = I65 msecb) AH interval*= 95 msecc) VH interval*= H was inscribed with V because of ven-
tricular pre-excitation ahead of His bundled) H-RVA interval= conduction time from His bundle to left
ventricular endocardium through left bundle system (55msec in Table 5) and from the left ventricular endocardiumto RVA (across septum: 55 msec in Table 5): II0 msec
Since this value is similar to that obtained in beats with-out pre-excitation (Table 5), RVA must have been activatedas in these beats
e) V-RVA interval= elapsing between initiation ofventriculardepolarization (by impulse traversing accessory pathway)and activation of RVA (following sequence expressed indefinition of H-RVA interval): 75 msec
f) QRS duration: I90 msec
* As defined in Table 3.
St1* St2
VLI
HBE - (4m9
:BH
RVA _
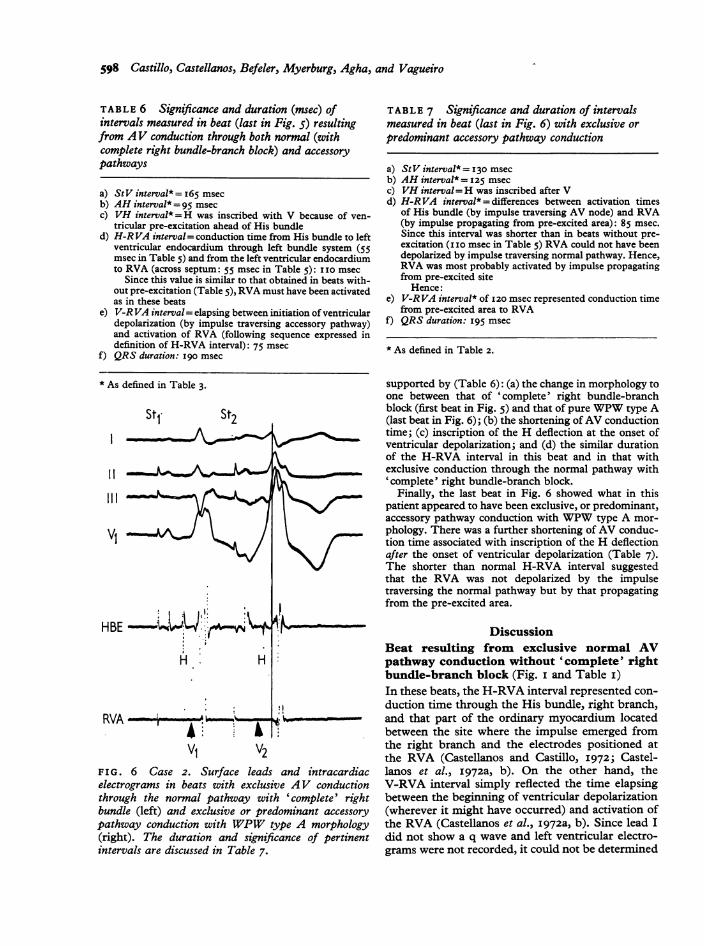
V: V2F I G. 6 Case 2. Surface leads and intracardiacelectrograms in beats with exclusive AV conductionthrough the normal pathway with 'complete' rightbundle (left) and exclusive or predominant accessorypathway conduction with WPW type A morphology(right). The duration and significance of pertinentintervals are discussed in Table 7.
TABLE 7 Significance and duration of intervalsmeasured in beat (last in Fig. 6) with exclusive orpredominant accessory pathway conduction
a) StV interval* = 130 msecb) AH interval* = 125 msecc) VH interval=H was inscribed after Vd) H-RVA interval* = differences between activation times
of His bundle (by impulse traversing AV node) and RVA(by impulse propagating from pre-excited area): 85 msec.Since this interval was shorter than in beats without pre-excitation (i I0 msec in Table 5) RVA could not have beendepolarized by impulse traversing normal pathway. Hence,RVA was most probably activated by impulse propagatingfrom pre-excited site
Hence:e) V-RVA interval* of 120 msec represented conduction time
from pre-excited area to RVAf) QRS duration: I95 msec
* As defined in Table 2.
supported by (Table 6): (a) the change in morphology toone between that of 'complete' right bundle-branchblock (first beat in Fig. 5) and that of pure WPW type A(last beat in Fig. 6); (b) the shortening ofAV conductiontime; (c) inscription of the H deflection at the onset ofventricular depolarization; and (d) the similar durationof the H-RVA interval in this beat and in that withexclusive conduction through the normal pathway with'complete' right bundle-branch block.
Finally, the last beat in Fig. 6 showed what in thispatient appeared to have been exclusive, or predominant,accessory pathway conduction with WPW type A mor-phology. There was a further shortening of AV conduc-tion time associated with inscription of the H deflectionafter the onset of ventricular depolarization (Table 7).The shorter than normal H-RVA interval suggestedthat the RVA was not depolarized by the impulsetraversing the normal pathway but by that propagatingfrom the pre-excited area.
DiscussionBeat resulting from exclusive normal AVpathway conduction without 'complete' rightbundle-branch block (Fig. i and Table i)In these beats, the H-RVA interval represented con-duction time through the His bundle, right branch,and that part of the ordinary myocardium locatedbetween the site where the impulse emerged fromthe right branch and the electrodes positioned atthe RVA (Castellanos and Castillo, I972; Castel-lanos et al., I972a, b). On the other hand, theV-RVA interval simply reflected the time elapsingbetween the beginning of ventricular depolarization(wherever it might have occurred) and activation ofthe RVA (Castellanos et al., I972a, b). Since lead Idid not show a q wave and left ventricular electro-grams were not recorded, it could not be determined
I
Arrival of excitation at right ventricular apical endocardium 599
whether the supraventricular impulse reached theleft ventricular endocardium before the right, thelatter before the former, or both at more or less thesame time.
Beat resulting from exclusive normal AVpathway conduction with functional 'com-plete' right bundle-branch block (Fig. 2 andTable 2)In Fig. 2, the presence of (true) 'complete' rightbundle-branch block was suggested by the prolongedAV conduction time, the wide QRS complexes,the triphasic pattern in lead Vi, the preterminal-terminal slurring, and the absence of initial delay.Since the HV interval measured I20 msec, anassociated conduction delay must have been presentwithin the left bundle-branch. Assuming that theblock in the right branch was 'complete', the HVinterval most probably represented conduction timefrom His bundle to left ventricular endocardium(through the left bundle system). Moreover, theV-RVA interval could be used as a rough measure-ment of conduction time from the left ventricularendocardium to the RVA: left-to-right transseptalconduction time. Therefore, the H-RVA intervalgave an estimate of conduction time from His bundleto left ventricular endocardium and from the latterarea to the RVA.
Beat resulting from AV conduction throughboth normal and accessory pathways without'complete' right bundle-branch block (Fig. 3and Table 3)In Fig. 3, pre-excitation of the ventricles throughthe accessory pathway occurred before that of theHis bundle. Thus, the H deflection was inscribedafter the onset of the delta wave. However, the RVAwas activated by the impulse traversing the rightbranch (from the His bundle) since the duration ofthe H-RVA interval (6o msec) was similar to that ofthe beat with exclusive normal pathway conductionand narrow QRS complexes (Fig. i and Table i).Though this beat was a 'fusion' complex, the pre-dominantly positive (wide and monophasic) de-flection in lead Vi suggested that the impulse arisingin the pre-excited area activated most parts of bothventricles. Yet, it reached the RVA after this areahad already been depolarized by the activation frontemerging from the right bundle-branch.
Beat resulting from exclusive accessory path-way conduction (Fig. 4 and Table 4)In contrast to what occurred in Fig. 3 (where a'fusion' complex was present), Fig. 4 showed thatthe H-RVA 'interval' was reduced from 6o to 45
msec. This suggests that the RVA was not activatedby the impulse emerging from the right branchpossibly because the RVA had already been depolar-ized by the impulse propagating from the pre-excited site. Therefore, the V-RVA interval couldbe used as a rough measurement of conductiontime from pre-excited area to RVA.
Beat resulting from exclusive, or predomin-ant, accessory pathway associated with organic'complete' right bundle-branch block (Fig. 5and Table 5)If the block in the right bundle-branch was com-plete (and persistent), the HV interval gave anindication of His-to-left ventricular endocardiumconduction time. In consequence, the V-RVArepresented left-to-right transseptal conductiontime. The duration of the H-RVA interval was cal-culated by adding the HV (H-left ventricular endo-cardial) and the V-RVA (left ventricular endocar-dial-right ventricular apical endocardial) conductiontimes (Fig. 2 and 5, Tables 2 and 5).
'Fusion' beat resulting from AV conductionthrough normal pathway (with persistent'complete' right bundle-branch block) andthrough accessory pathway (Fig. 5 and Table 6)In this beat the impulse propagating from the pre-excited site probably did not reach the left ventricu-lar endocardial areas first depolarized by the impulseemerging from the left bundle system in time torender them refractory since the H-RVA interval(determined by the addition of the H-to-left ven-tricular endocardial and left ventricular endocardialto RVA conduction times) had a similar value (iIOmsec) to the beat without pre-excitation. A 'fusion'complex was possible because some (anterior) rightventricular regions were not activated from the pre-'excited area but by the impulse which, afterdescending through the left bundle system, propa-gated in a left-to-right direction across the septum.
Beat resulting from predominant, or exclusive,accessory pathway conduction without 'com-plete' right bundle-branch block (Fig. 6 andTable 7)The shorter-than-normal H-RVA interval suggestedthat the RVA was not activated by the impulsereaching the ventricles through the His bundle.Assuming 'complete' block in the right branch,depolarization of the RVA was most probably afunction of the impulse propagating from the pre-excited region. Thus, the V-RVA interval of 120msec represented conduction time from the lattersite to the RVA.

6oo Castillo, Castellanos, Befeler, Myerburg, Agha, and Vagueiro
Conduction time from pre-excited area toendocardial surface of RVAAlthough the pathways that the impulse followed inpropagating from one site to the other are notknown, the morphology of the QRS complexes sug-gested an anteroposterior and left-to-right sequenceof activation (Rosenbaum et al., I945).The conduction times from pre-excited site to
RVA endocardium in these two patients with WPWtype A (II0-120 msec, respectively) were longerthan those recorded in two other cases of WPWtype B (40-50 msec, respectively) (Castellanos et al.,I972b). However, these findings do not imply thatdifferent values might not be recorded in otherpersons with this syndrome, depending on the vari-able location of the accessory pathways.
Importance of catheter recordingsPick and Fisch (I958) emphasized that the diagnosisof WPW type A associated with intermittent rightbundle-branch block was not difficult because thepre-excitation occurred in the chamber with theintact bundle-branch block, therefore allowing forthe delta wave to coexist with the late QRS changesproduced by right bundle-branch block. Unfor-tunately similar electrocardiographic changes areseen in beats with pure WPW type A when theright ventricle is activated after the left, not becausethe right branch is blocked but as a consequence ofthe specific modality of intraventricular conductioncharacteristic of an impulse propagating from theposterior part of the ventricles in an anteriordirection.
This communication stresses the importance ofintracardiac electrograms in establishing the correctdiagnosis. Moreover, a recent report from ourdepartment (Castellanos et al., 1972b) indicated howtheir value was enhanced by simultaneously recordedvectorcardiograms.
In beats with pure 'complete' right bundle-branch block a preterminal-terminal rightwardsoriented delay was associated with normal, or pro-longed PR (or StV), HV, and RVA intervals. Co-existing initial and rightwards oriented terminaldelays were seen in beats with WPW type A co-existing with 'complete' right bundle-branch blockas well as in those with pure WPW type A. Whereasin the former instances the initial delay was due topre-excitation and the terminal conduction abnor-malities to right bundle-branch block in pure WPWtype A (resulting from exclusive conduction throughthe accessory pathway), both types of delay were due
exclusively to the bizarre activation pattern seen inbeats propagating from an ectopic ventricular site,regardless of whether they reached this area (fromthe atria) through an accessory pathway, or whetherthey originated there (spontaneous or inducedextrasystoles).
Duration of StV intervalDuring high atrial pacing pre-excitation occurredeven when the StV intervals were within normallimits (greater than I20 msec), probably becausethis interval included conduction time through theaccessory pathway as well as through the atria, fromthe paced site to its upper entrance, which presum-ably was located somewhere in the left atrium.
ReferencesCastellanos, A., Jr., Agha, A. S., Befeler, B., and Castillo,
C. A. (1972a). A study of arrival of excitation at selectedventricular sites during human bundle branch block usingbipolar catheter electrodes. Chest. In the press.
Castellanos, A., Jr., Agha, A. S., Portillo, B., and Myerburg,R. J. (I972b). Usefulness of vectorcardiography combinedwith His bundle recordings and cardiac pacing in evalua-tion of the pre-excitation (Wolff-Parkinson-White) syn-drome. American Journal of Cardiology. 30, 623.
Castellanos, A., Jr., and Castillo, C. A. (1972). His bundlerecordings in right bundle-branch block coexisting withiatrogenic right ventricular pre-excitation. British HeartJournal, 34, 153.
Castellanos, A., Jr., Castillo, C. A., and Myerburg, R. J.(197I). Bipolar coronary sinus lead for left atrial and leftventricular recording. American Heart journal, gi, 832.
Castillo, C. A., and Castellanos, A., Jr. (1970). His bundlerecordings in patients with reciprocating tachycardias andWolff-Parkinson-White syndrome. Circulation, 42, 271.
Durrer, A., Schoo, L., Schuilenburg, R. M., and Wellens,H. J. J. (I967). The role ofpremature beats in the initiationand termination of supraventricular tachycardia in Wolff-Parkinson-White syndrome. Circulation, 36, 644.
Laham, J. (I969). Le Syndrome de Wolff-Parkinson-White,pp. 159-i68. Maloine, Paris.
Pick, A., and Fisch, C. (1958). Ventricular pre-excitation(WPW) in the presence of bundle branch block. AmericanHeartjournal, 55, 504.
Robertson, P. G. C., Emslie-Smith, D., Lowe, K. G., andWatson, H. (I963). The association of type B ventricularpre-excitation and right bundle branch block. BritishHeart Journal, 25, 755.
Rosenbaum, F. F., Hecht, H. H., Wilson, F. N., and John-ston, F. D. (1945). The potential variations of the thoraxand the esophagus in anomalous atrioventricular excitation(Wolff-Parkinson-White syndrome). American HeartJournal, 29, 28I.
Schamroth, L. (I97i). The Disorders of Cardiac Rhythm,p. 247. Blackwell Scientific Publications, Oxford.
Requests for reprints to Dr. A. Castellanos, Jr., Univer-sity of Miami School of Medicine, P.O. Box 875,Biscayne Annex, Miami, Florida 33152, U.S.A.