endoscopic retrograde cholangiopancreatographyuu.diva-portal.org › smash › get › diva2:1421436...
TRANSCRIPT
ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2020
Digital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1665
Endoscopic retrogradecholangiopancreatography
Perforation and long-term outcomes afterendoscopic sphincterotomy
ANN LANGERTH
ISSN 1651-6206ISBN 978-91-513-0937-8urn:nbn:se:uu:diva-408046

Dissertation presented at Uppsala University to be publicly examined in Hedstrandsalen,Entrance 70 Ground Floor, Uppsala University Hospital, Uppsala, Saturday, 30 May 2020 at09:00 for the degree of Doctor of Philosophy (Faculty of Medicine). The examination willbe conducted in Swedish. Faculty examiner: Professor Riadh Sadik (Gothenburg University,Department of Medical Science).
AbstractLangerth, A. 2020. Endoscopic retrograde cholangiopancreatography. Perforation and long-term outcomes after endoscopic sphincterotomy. Digital Comprehensive Summaries ofUppsala Dissertations from the Faculty of Medicine 1665. 66 pp. Uppsala: Acta UniversitatisUpsaliensis. ISBN 978-91-513-0937-8.
Endoscopic retrograde cholangio pancreatography (ERCP) is a commonly used procedurein various disorders of the pancreatobiliary tract. When extracting common bile duct stones(CBDS), the major duodenal papilla is divided using a papillotome to perform an endoscopicsphincterotomy (ES). Adverse events occurring shortly after ES are well-known and includeperforation which, however, is difficult to investigate due to its low frequency. ES is oftenused in elderly and/or infirm patients with gallstone pancreatitis and cholangitis, to preventrelapse in biliary events linked to CBDS. Subsequent cholecystectomy in these patients remainscontroversial. What happens in the long term after ES is still partially unknown.
In Paper I, we found an increased risk for both cholangitis and pancreatitis after ES for CBDS,without synchronic relapse of CBDS and when compared with the general population was found.In Paper II, we retained the ES group, but replaced the control group with controls with a historyof gallstone disease. The increased risk for both cholangitis and pancreatitis without relapse ofCBDS still remains but, no higher risk for malignancy in the pancreatobiliary tract was noted.
We conducted study III, a prospective follow-up after ES, to evaluate to what extent ESprevents relapse into biliary events after cholangitis and pancreatitis caused by bile duct stones.We included 100 patients who did not have earlier gallbladder surgery and who were treatedfor pancreatitis and/or cholangitis. The patients then underwent ES but not cholecystectomyand were followed for a mean of 42 months. None of the patients had recurrent pancreatitisand one had cholangitis. This indicates that ES alone is an alternative to cholecystectomy in theprevention of further attacks of acute pancreatitis and cholangitis.
Paper IV consists of 52,140 ERCPs that were registered with GallRiks, a Swedish populationbased register. A total of 376 cases were registered as perforations and 75 patients had a fataloutcome. These data showed that sphincterotomy in the pancreatic duct increased the risk ofdeath from perforation but the risk of death was reduced when ERCP was performed at a Q4centre.
Keywords: Long-term outcome, ERCP, perforation, endoscopic sphincterotomy
Ann Langerth, Department of Surgical Sciences, Upper Abdominal Surgery, Akademiskasjukhuset ing 70 1 tr, Uppsala University, SE-751 85 Uppsala, Sweden.
© Ann Langerth 2020
ISSN 1651-6206ISBN 978-91-513-0937-8urn:nbn:se:uu:diva-408046 (http://urn.kb.se/resolve?urn=urn:nbn:se:uu:diva-408046)

“Learn from yesterday, live for today, hope for tomorrow. The important thing is not to stop questioning.”
-Albert Einstein
To my dear family

List of Papers
This thesis is based on the following papers, which are referred to in the text by their Roman numerals.
I Langerth A, Brandt L, Ekbom A, Karlson B-M. (2014). Late
complications following sphincterotomy: A Swedish Popula-tion-Based Study. Hindawi Publishing Corporation. Diagnostic and Therapeutic Endoscopy. Volume 2014, Article ID 745790, 5 pages.
II Langerth A, Sandblom G, Karlson B-M. Long-term risk for acute pancreatitis, cholangitis, and malignancy more than 15 years after endoscopic sphincterotomy: a population-based study. Endoscopy, 2015. 47(12): p. 1132-6.
III Langerth A, Isaksson B, Ljungdahl M, Urdzik J, Karlson B-M. Endoscopic sphincterotomy is an effective method for prevent-ing recurrent pancreatitis and cholangitis with the gallbladder left in situ - a prospective study. Manuscript
IV Langerth A, Isaksson B, Karlson BM, Urdzik J, Linder S. ERCP-related perforations: a population-based study of inci-dence, mortality and risk factors. Surgical Endoscopy, 2019. https://doi.org/10.1007/s00464-019-06966-w
Reprints were made with permission from the respective publishers.


Contents
Introduction ................................................................................................... 11
Background ................................................................................................... 13 Anatomy ................................................................................................... 13
Endoscopic Retrograde Cholangiopancreatography ............................ 16 Direct cholangiopancreatoscopy .......................................................... 18
Papillotomy .............................................................................................. 19 Pancreatic sphincterotomy ................................................................... 19
Short-term complications after ERCP ...................................................... 19 Pancreatitis ........................................................................................... 19 Perforation ........................................................................................... 20 Cholangitis ........................................................................................... 21 Cholecystitis ........................................................................................ 21 Bleeding ............................................................................................... 21
Long-term complications after ERCP ...................................................... 21 Gallstone disease ...................................................................................... 22
Common bile duct stone ...................................................................... 22 Benign biliary strictures ........................................................................... 24 Benign pancreatic diseases ....................................................................... 25 Malignant pancreatobiliary obstruction .................................................... 25
Pancreatic cancer ................................................................................. 25 IPMN ................................................................................................... 26 Cholangiocarcinoma ............................................................................ 27 Cancer of the major duodenal papilla .................................................. 27 Duodenal adenocarcinoma ................................................................... 28
Statistics ................................................................................................... 28 Hazard Ratio (HR) ............................................................................... 28 Confidence interval .............................................................................. 28 Cox regression ..................................................................................... 28 Life table plot ....................................................................................... 29
Registries .................................................................................................. 29 The Swedish Population Register ........................................................ 29 The Swedish National Inpatient Register - IPR ................................... 29 The Swedish Cause of Death Register ................................................. 29 The Swedish Cancer Register .............................................................. 29

National Swedish Register for Gallstone Surgery and Endoscopic Retrograde Cholangiopancreatography (GallRiks) ............................. 30
Epidemiology ........................................................................................... 30 Bias ...................................................................................................... 30 Cohort study ........................................................................................ 30 Endpoint ............................................................................................... 30 Confounding ........................................................................................ 30
Aims of the thesis.......................................................................................... 31 Specific aims: ........................................................................................... 31
Summary of Papers ....................................................................................... 32 Late complications after ES ..................................................................... 32
Patients and methods ........................................................................... 32 Results ................................................................................................. 33
Confirming the results from the first study .............................................. 33 Patient and methods ............................................................................. 33 Results ................................................................................................. 34
The papillotomy study .............................................................................. 35 Patients ................................................................................................. 35 Methods ............................................................................................... 36 Results ................................................................................................. 36
The perforation study ............................................................................... 37 Patients and methods ........................................................................... 37 Results ................................................................................................. 41
Discussion ..................................................................................................... 45 Recurrence of CBDS after ES .................................................................. 45 Cholangitis after ES ................................................................................. 46 Pancreatitis after ES ................................................................................. 46 Benign bile duct stricture after ES ........................................................... 46 Malignancy after ES ................................................................................. 47 Overall morbidity and mortality after ERCP ........................................... 47 ES as a prevention of recurrent gallstone pancreatitis and cholangitis with the gallbladder left in situ ................................................................. 48 Perforations associated with ERCP .......................................................... 49 Clinical relevance ..................................................................................... 50
Conclusions ................................................................................................... 51 Paper I ...................................................................................................... 51 Paper II ..................................................................................................... 51 Paper III .................................................................................................... 51 Paper IV ................................................................................................... 51

Future aspects ............................................................................................... 52
Svensk sammanfattning ................................................................................ 53 Delarbete I ................................................................................................ 54 Delarbete II ............................................................................................... 54 Delarbete III ............................................................................................. 54 Delarbete IV ............................................................................................. 55 Sammanfattning ....................................................................................... 55
Acknowledgements ....................................................................................... 56
References ..................................................................................................... 58
Abbreviations
AE Adverse event CBD Common bile duct CBDS Common bile duct stone CI Confidence interval CT Computed tomography ERCP Endoscopic retrograde cholangiopancreatography ES Endoscopic sphincterotomy EUS Endoscopic ultrasound EPBD Endoscopic papillary balloon dilatation FCSEMS Fully covered self-expandable metallic stent GallRiks National Swedish Registry for Gallstone Surgery and
Endoscopic Retrograde Cholangiopancreatography HR Hazard ratio IPMN Intraductal papillary mucinous neoplasm IPR The Swedish National Inpatient Registry LC Laparoscopic cholecystectomy MRCP Magnetic resonance cholangiopancreatography OR Odds ratio PD Pancreatic duct PEP Post-ERCP pancreatitis PSC Primary sclerosing cholangitis PTBD Percutaneous transhepatic biliary drainage RR Relative risk SEMS Self-expandable metallic stent SOD Sphincter of Oddi dysfunction US Ultrasound
11
Introduction
Endoscopic retrograde cholangiopancreatography (ERCP) is a common pro-cedure for treating various diseases of the biliary and pancreatic ducts. It is often referred to as safe. In recent decades, the use of therapeutic ERCP has increased 30-fold 1.
In Sweden, about 9,000 ERCPs are performed every year. Most of them are for the indication of common bile duct stones (CBDS), www.ucr.uu.se/gallriks. Together with direct cholangiopancreatoscopy, ERCP is also used to investigate complex pancreatobiliary diseases such as bile duct strictures and intraductal papillary mucinous neoplasms of the pan-creas 2. This increase in procedure complexity increases the requisite exper-tise needed to complete the procedure successfully and probably also in-creases the risk of adverse events. Thus, understanding the factors associated with failed ERCP interventions is of great interest. Cannulation success is reported to be 92% and the perioperative complica-tion rate 2-3% 3. Postoperative complications, which studies suggest are up to 12% 4, include incidents within 30 days of the intervention and also events not due to the actual procedure, such as myocardial infarction, heart failure and pulmonary emboli.
In the short run, the most common complications have been studied and well defined and there are many articles dealing with this topic 3, 5, 6. Howev-er, more uncommon complications adjacent to the intervention, such as per-foration are less easy to evaluate 7.
In the long run, there are many papers discussing the frequency of recur-rence in CBDS 8-11, but only a few focus on other diagnoses following ES 12-
14. Due to the increase in the number of ERCPs being performed, especially in the younger population, it is vital to ensure, that we do not create an in-creased risk for, for example, malignancy in the long-run.
13
Background
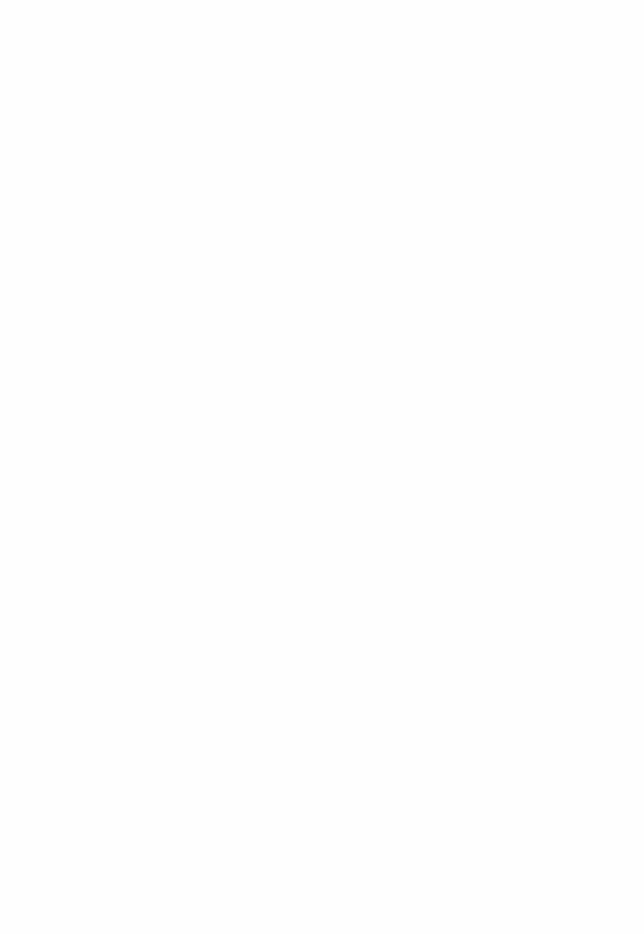
Figure 1. Anatomy of the upper gastrointestinal tract including important landmarks when performing ERCP
Anatomy The anatomy of the periampullary tract is special in many ways, in particular because of the individual variations that may be present. Demonstrated here is the most commonly occurring anatomy in this region [Figure1].
Duodenum The duodenum is the first part of the small intestine. It measures about 25-30cm and is formed as a C-shaped loop, meanders around the head of the pancreas. Except for the first 3cm, it is situated entirely retroperitoneally. The duodenum is divided into four different parts, related to the vertebral columns. The second part – duodenum descendens - passes parallel to and to the right of the inferior vena cava and lies on the medial part of the right
14
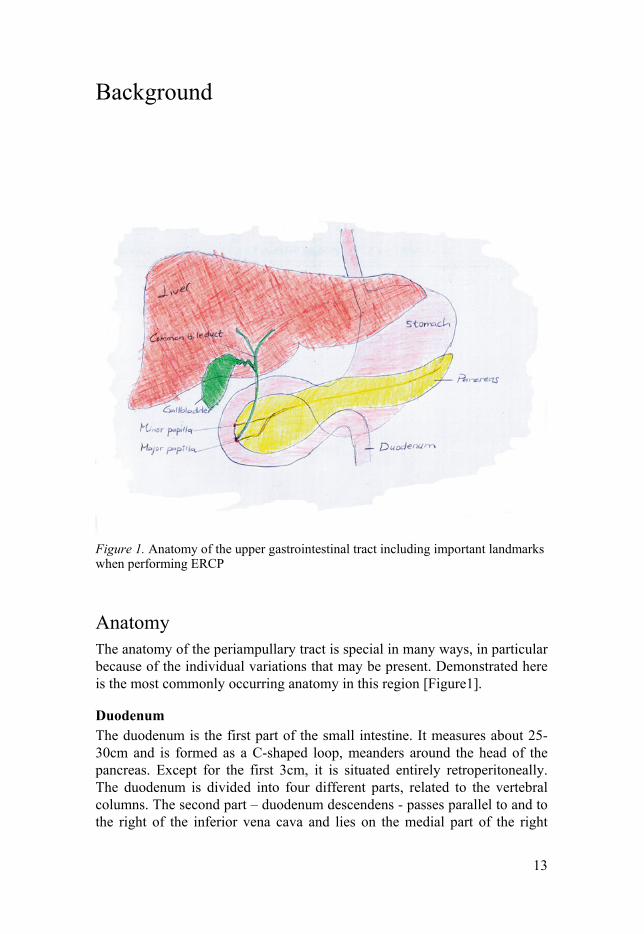
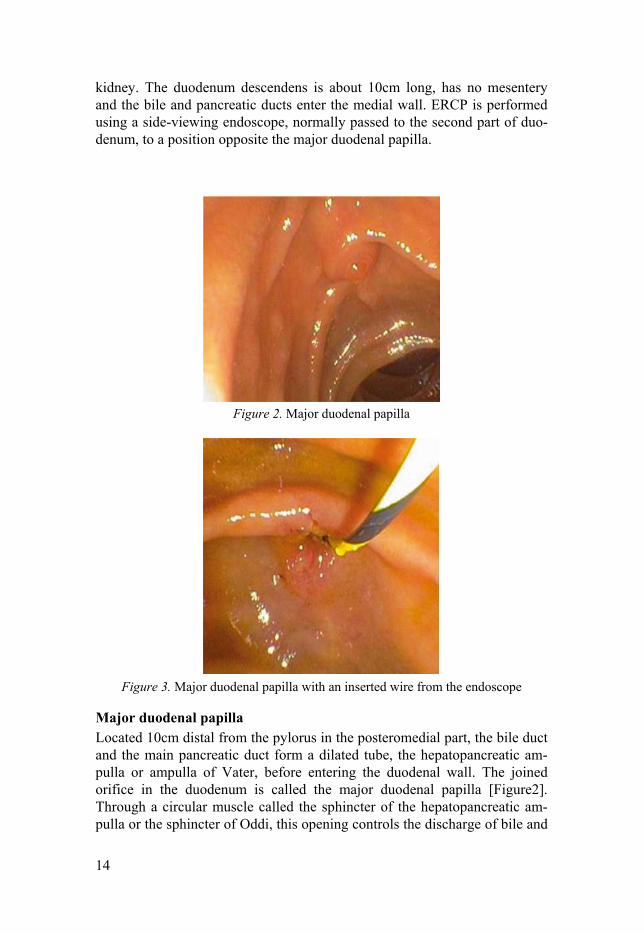
kidney. The duodenum descendens is about 10cm long, has no mesentery and the bile and pancreatic ducts enter the medial wall. ERCP is performed using a side-viewing endoscope, normally passed to the second part of duo-denum, to a position opposite the major duodenal papilla.
Figure 2. Major duodenal papilla
Figure 3. Major duodenal papilla with an inserted wire from the endoscope
Major duodenal papilla Located 10cm distal from the pylorus in the posteromedial part, the bile duct and the main pancreatic duct form a dilated tube, the hepatopancreatic am-pulla or ampulla of Vater, before entering the duodenal wall. The joined orifice in the duodenum is called the major duodenal papilla [Figure2]. Through a circular muscle called the sphincter of the hepatopancreatic am-pulla or the sphincter of Oddi, this opening controls the discharge of bile and

15
pancreatic secretions into the duodenum. When the endoscope is in position, the biliary tree or the pancreatic duct are accessed by using a hollow cannula with a guide wire that is passed through the working channel of the endo-scope into the duct of choice [Figure 3].
Minor duodenal papilla The minor duodenal papilla is located about 2cm above and to the right of the major papilla into which the accessory pancreatic duct opens. If promi-nent it can be mistaken for the major papilla. In about 1% of people the main pancreatic duct has no connection with the duct draining the head of the pancreas – the pancreas divisum. Cannulation of minor papilla may some-times be indicated but the success rate is lower than that for the major papil-la.
The common bile duct The bile duct passes posterior to the superior part of the duodenum and the head of the pancreas, occupying a groove in the head of the pancreas or em-bedded in it. Together with the pancreatic duct, the bile duct ends up in the major duodenal papilla, and drains via the common bile duct, through the major duodenal papilla into the second part of duodenum. The anatomy of the biliary tree allows good access to the biliary system with an endoscope.
Pancreas The pancreas is divided into four parts: head, body, neck and tail. It is 12-15cm long and is situated behind the stomach. It originates from the duode-num to witch it is anchored. The anterior surface is covered with peritoneum and the superior mesenteric vessels are situated in tight behind the neck of the pancreas. This gland is very important due to its production of insulin, glucagon and pancreatic juice. The main pancreatic duct begins in the tail of the pancreas and unites with the bile duct into the major duodenal papilla.
16
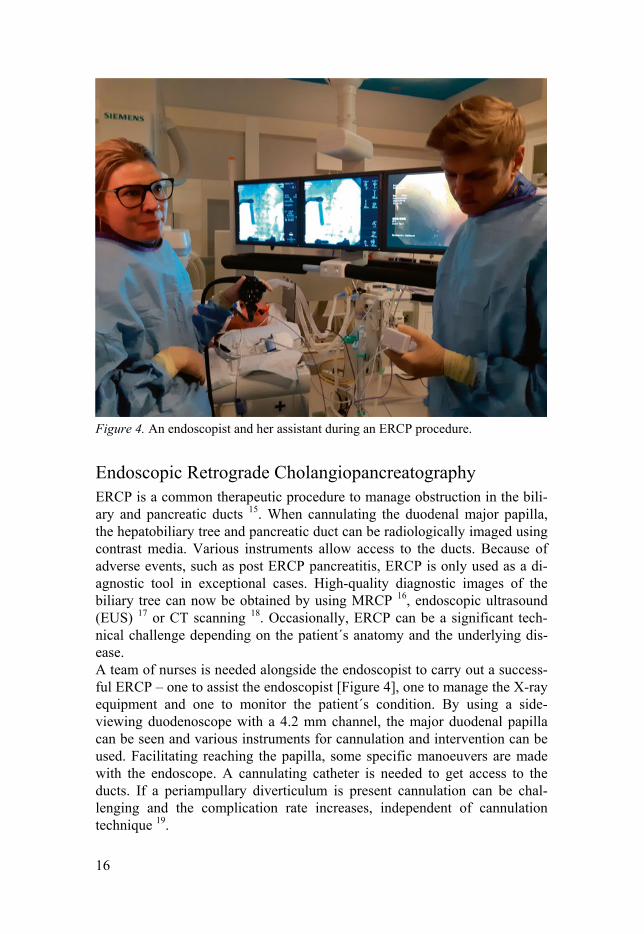
Figure 4. An endoscopist and her assistant during an ERCP procedure.
Endoscopic Retrograde Cholangiopancreatography ERCP is a common therapeutic procedure to manage obstruction in the bili-ary and pancreatic ducts 15. When cannulating the duodenal major papilla, the hepatobiliary tree and pancreatic duct can be radiologically imaged using contrast media. Various instruments allow access to the ducts. Because of adverse events, such as post ERCP pancreatitis, ERCP is only used as a di-agnostic tool in exceptional cases. High-quality diagnostic images of the biliary tree can now be obtained by using MRCP 16, endoscopic ultrasound (EUS) 17 or CT scanning 18. Occasionally, ERCP can be a significant tech-nical challenge depending on the patient´s anatomy and the underlying dis-ease. A team of nurses is needed alongside the endoscopist to carry out a success-ful ERCP – one to assist the endoscopist [Figure 4], one to manage the X-ray equipment and one to monitor the patient´s condition. By using a side-viewing duodenoscope with a 4.2 mm channel, the major duodenal papilla can be seen and various instruments for cannulation and intervention can be used. Facilitating reaching the papilla, some specific manoeuvers are made with the endoscope. A cannulating catheter is needed to get access to the ducts. If a periampullary diverticulum is present cannulation can be chal-lenging and the complication rate increases, independent of cannulation technique 19.
17
In a minority of cases, even the most skilled endoscopist will fail to achieve cannulation. Combined procedures such as percutaneous insertion of a catheter into the biliary system via the intrahepatic ducts or gall bladder, through which a guidewire is introduced into the duodenum, may be rele-vant. EUS-guided biliary drainage combined with ERCP has also been de-scribed as an alternative 20.
When ERCP fails, percutaneous transhepatic biliary drainage (PTBD) or surgical bypass procedures are performed as salvage therapies 21. Percutane-ous access and surgical options are associated with morbidity, mortality, and expense and therefore EUS-guided biliary drainage has gained in popularity worldwide 22, 23 and has a reported adverse events rate of around 5% 24. ERCP’s success rate varies markedly between institutions 25. Lower endos-copist volumes are associated with a higher ERCP failure rate, and a greater need for post-procedure hospitalizations 26. An association between low en-doscopist volume and high adverse event rates has also been noted 27.
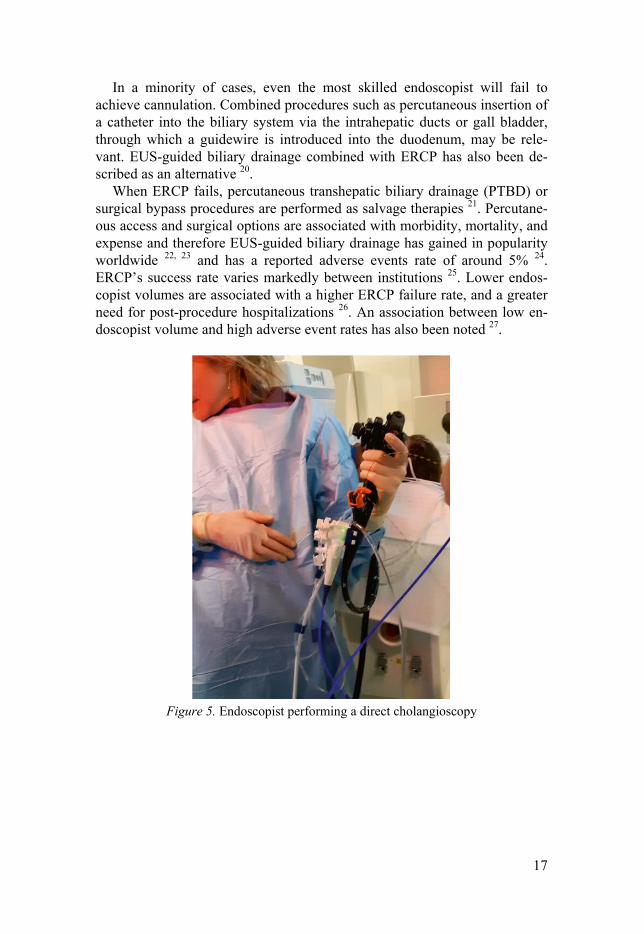
Figure 5. Endoscopist performing a direct cholangioscopy

18
Figure 6. Biopsy taken during direct cholangioscopy
Direct cholangiopancreatoscopy Direct cholangiopancreatoscopy enables the user to see directly into the bili-ary tree to the second- or third order ducts. Spyglass™ [Figure 5] can be handled by a single endoscopist when the fibre optic cable passes into the bile duct or pancreatic duct over a wire, through the endoscope’s working channel. A clearer view of a stricture can be obtained and biopsied under direct vision [Figure 6] thereby improving the yield of diagnostic histology to about 80% 28, 29. In cases of large stone disease, direct electrohydraulic or laser lithotripsy can also be performed when conventional methods have failed 30.
Figure 7. Papillotomy
19
Papillotomy Papillotomy or Endoscopic Sphincterotomy (ES) [Figure 7] is usually per-formed to manage common bile duct stones (CBDS), but also to facilitate stent insertion or the insertion of a cholangioscope into the biliary or pancre-atic ducts for direct visualization. An assortment of sphincterotomes is avail-able for improved precision and a guidewire is often used to cannulate the papilla. Contrast medium is injected to confirm the position of the sphincter-otome or the guidewire.
The optimal position is when the sphincterotome cuts in the 11 o´clock direction and the limit for upper extent is the transverse duodenal fold at the upper margin of the papilla.
If cannulation fails, a precut can be performed. However, this is associat-ed with an increased risk for perforation of the duodenum. The goal of a precut technique is to open the roof of the papilla in order to expose the bili-ary or pancreatic ductal orifice for selective ductal cannulation. Most often a needle-knife sphincterotome, consisting of a diathermic needle that protrudes 5 mm from the tip of the catheter, is used.
Pancreatic sphincterotomy Because the intramural segment of the pancreatic duct is shorter than that of the bile duct, the risk of perforation is higher. If selective pancreatic duct cannulation fails, a preliminary biliary sphincterotomy may help to identify the pancreatic duct orifice, which is typically located caudal and to the right of the bile duct orifice. In the case of a symptomatic pancreas divisum, sphincterotomy of the minor papilla can be performed to improve drainage 31.
Short-term complications after ERCP Complication rates must be interpreted with caution because definitions dif-fer between studies. There are other rare complications not discussed below, such as impacted baskets and gallstone ileus.
Pancreatitis With an incident rate of around 5% 32-34, post-ERCP pancreatitis (PEP) is the most common serious short-term complication. Both patient and procedure related factors are important in determining PEP. Risk factors are prior PEP, suspected sphincter of Oddi dysfunction (SOD), female gender, normal se-rum bilirubin, biliary sphincter balloon dilation, difficult cannulation, pan-creatic sphincterotomy and injections of contrast to the pancreatic duct 35, 36.

20
A combination of patient risk factors increases the risk for PEP 36, 37. NSAIDs can be given before the procedure to prevent PEP in high risk pa-tients 38 and/or a temporary stent can be placed in the pancreatic duct if can-nulated 39.
Figure 8. Arrows showing different, common locations for perforation injuries caused by the ERCP procedure.
Perforation Perforation caused by the ERCP procedure [Figure 8] is a feared, but fortu-nately, an uncommon complication reported at a frequency of around 1% 7, 40-43. It is most often associated with ES but can occur anywhere that endo-scopes travel. Perforation should always be considered if there is marked distress soon after the procedure. Risk factors associated with perforations are not clearly identified due to their low incidence. However, perforations induced by ES are more common when using the precut method and in pa-tients with SOD 44, 45. Early detection and finding the location of the perfo-ration are most crucial for the patients outcome 46. If a periampullary perfo-ration is detected during ERCP, a fully covered self-expandable metallic stent (FCSEMS) can be used 47 rather than an uncovered SEMS, as the lat-ter tends to embed in the duct, making it difficult to remove 48. Stapfer et al 49 suggested a classification system for ERCP-induced duodenal perfora-tion. It is the most commonly used system and is based on the anatomical location and mechanism of injury. Surgical indications of perforations in-clude haemodynamic instability, signs of peritonitis, continuing leakage, septic conditions, and a perforation of large size.

21
Cholangitis The rate of post-ERCP cholangitis is reported at around 1% 32, 33, 35. Risk factors for cholangitis after ERCP consist primarily of failed or incomplete biliary drainage 50 but other risk factors include the use of combined percu-taneous-endoscopic procedures, stent placement in malignant strictures and low case volume 32. There is a lack of evidence concerning prophylactic antibiotics except with selected patients such as after liver transplantation 51.
Cholecystitis Cholecystitis complicates approximately 0.2% to 0.5% of ERCPs 32, 33 and it may be unclear whether this is a complication of the ERCP or merely the natural history of gallbladder stones. Placement of SEMS may increase the risk of cholecystitis, particularly if the stent is covered and the cystic duct is obstructed 52.
Bleeding Bleeding is a serious adverse event and is most commonly the result of en-doscopic biliary and/or pancreatic sphincterotomy. It occurs in approximate-ly 0.3% to 2% of cases after ERCP 32, 53. Correction of coagulopathy before ERCP is essential. Endoscopic papillary balloon dilation (EPBD) is associat-ed with a decreased risk of bleeding compared with ES 54. However, the risk of post-ERCP pancreatitis is increased in patients who undergo EPBD with-out initial endoscopic sphincterotomy 55.
Long-term complications after ERCP Since the ERCP era started at the end of the 1960s, it has become an increas-ingly common procedure. Initially used more as a diagnostic examination, it is nowadays eligible as a strictly therapeutic intervention, because of its known short-term complications and its unknown long-term complications due to ES.
Some long-term follow-up studies after ES have shown that the procedure is safe and effective, but depending on the underlying diagnosis, recurrence of CBDS may occur, especially if the gallbladder is still left in situ. A few studies discuss stenosis and cholangitis after ES. However, due to the lack of large studies with sufficient long-term follow-up, adverse events cannot be ruled out , even a long time after ES 12-14.
After dividing the sphincter of Oddi, there is no return. The possibility of unrestricted duodenal content reflux is now established 56. Moreover, reflux from the pancreatic duct to the bile duct and vice versa is enabled. This may
22
lead to infection and inflammation in the short-term and some studies indi-cate the development of cancer in the long term 57.
Gallstone disease Gallstone disease is a common gastrointestinal disorder in Western countries and represents a major public health problem. It is by far the most costly digestive disorder, mainly due to the surgical procedures associated with it 58,
59. The natural history of gallstone diseases has been reported as benign for both asymptomatic and symptomatic patients 60. Epidemiological studies have shown that 80% of subjects with stones are asymptomatic 61, 62. Seven to eight per cent will develop symptoms over the course of a five-year period 63. The most important risk factors for developing gallstone diseases are in-creasing age, female gender, heredity and obesity 64. Alcohol consumption has been shown to be associated with a lower prevalence of both symptomat-ic 65 and asymptomatic gallstone disease 66. Biliary colic arises when a gallstone impacts the neck of the gallbladder leading to obstruction of the cystic duct. This is typically centred in the right upper quadrant or epigastrium, with radiation to the right lower chest or the lower pole of the scapula. The pain of biliary colic often lasts between 30 minutes and 2 hours. The most common complication is cholecystitis and while other complications such as pancreatitis, cholangitis, obstructive jaun-dice and carcinoma of the gallbladder are more infrequent 67. Laparoscopic cholecystectomy (LC) is the method of choice for managing symptomatic gallbladder stones 68 (GallRiks, www.ucr.uu.se/gallriks). The identification of gallstones is fundamental before an operation and ultrasonography (US) is the most established form for detection.
Common bile duct stone The prevalence of CBDS in patients with symptomatic gallstones is between 10% and 20% 69, 70. Incidence is reported to be <5% in patients with no clini-cal suspicion of ductal stones prior to surgery 71, 72. The complications of CBDS are potentially life threatening and include pain, obstructive jaundice, cholangitis, hepatic abscesses and pancreatitis. Combined transabdominal ultrasound and liver function tests are helpful tools for investigating the probability of existing CBDS 73. When there is a persistent suspicion of CBDS and the results are non-diagnostic, further investigation maybe neces-sary, preferably with MRCP – a noninvasive modality 74. ERCP is highly sensitive in the detection of CBDS, with reported rates of over 90% 75. It also permits therapeutic removal of stones at the same time.
23
ES is often performed so that stones can be extracted with a Dormia basket or balloon catheter. Endoscopic papillary balloon dilatation (EPBD) can also be performed but because of the increased risk of post procedure pancreatitis it should be avoided as a stand-alone procedure 76. However, sphincterotomy together with EPBD for the removal of large CBDS has similar safety levels but superior efficiency to conventional treatment with sphincterotomy alone 77. Biliary stenting can be used in the management of retained common bile duct stones, permitting adequate biliary drainage prior to further endoscopy or surgery. The use of biliary stents as a sole treatment is recommended only for high risk patients or those with limited life expectancy 78.
An intraoperative rendezvous ERCP technique can be used when CBDS are detected by intraoperative cholangiography during cholecystectomy. An antegrade guidewire is then inserted by the surgeon through the cholangi-ography catheter and advanced through the major duodenal papilla. Simulta-neously, a duodenoscope is passed into the duodenum, and the guidewire is caught with a polypectomy snare and pulled gently through the working channel of the duodenoscope. This technique has gained popularity in Swe-den in recent years, as a single-session procedure, which shortens hospital stays and reduces PEP 79. If there is no endoscopist available at the time, the surgeon can leave the guidewire in place and anchor it with clips on the cyst-ic duct. The patient is then scheduled for ERCP within a day or two. Postop-erative rendezvous ERCP constitutes an acceptable alternative where ERCP resources are lacking or limited 80.
Other options when CBDS are detected during cholecystectomy are trans cystic or trans ductal laparoscopic bile duct exploration. Open surgery bile duct exploration and percutaneous radiological stone extraction should be reserved for the small number of patients for whom all other techniques have failed or are not possible. Percutaneous CBDS extraction is usually achieved by establishing a transhepatic biliary fistula through which catheter and cholangioscopic interventions are performed. A typical procedure will in-volve balloon dilation of the papilla, which allows stones to be pushed in an antegrade fashion into the duodenum. Completion rates are high but major adverse events occur in approximately 7% of patients 81. A number of ductal stones will spontaneously pass into duodenum before or after cholecystec-tomy 82, 83. If CBDS are left in situ, the risk for unfavourable outcomes is reported as 25% over a follow-up period from 0 to 4 years 84. However, ex-pectant management seems to be effective for the treatment of patients with acute gallstone pancreatitis and bile duct stones that are equal to or less than 5 mm 85.

24
Figure 9. A patient with PSC and a CBDS
Benign biliary strictures Differentiating benign from malignant biliary strictures is clinically im-portant, and this often presents a significant diagnostic challenge. Imaging plays a critical role. The situation in patients with benign biliary strictures is different from those with malignant strictures because of the potential for extended survival. Benign biliary strictures can be caused, for example, by chronic pancreatitis, postoperative strictures and primary sclerosing cholan-gitis (PSC) [Figure 9]. Temporary cholestasis can respond favourably to placement of a single 10 Fr plastic stent in the acute situation. However, plastic stents are limited by their short stent patency and the need for repeat-ed endoscopic procedures to achieve stricture resolution. Multiple 10 Fr stents have, however, been associated with a higher long-term success 86. FCSEMS have similar clinical success rates compared with plastic stents. They reduce the need for multiple endoscopic sessions and may also be as-sociated with fewer adverse events, shorter hospital stays, and reduced costs. Acceptable short-term safety profiles have been demonstrated, although stent migration proves to be a major issue 87. Balloon dilatation of a benign stric-ture is usually combined with stenting and rarely performed in isolation. The main indication for balloon dilatation alone is in the setting of PSC with a dominant stricture 88. Routine administration of prophylactic antibiotics be-fore ERCP in patients with PSC is strongly recommended 89. Percutaneous transhepatic cholangiography (PTC) may be indicated in patients with com-plicated tight hilar strictures, where reaching the distal end of the stricture is incomplete.
25
Benign pancreatic diseases ERCP can provide evaluation of pancreatic duct (PD) abnormalities, includ-ing strictures, stones, leaks, communicating pancreatic pseudocysts and side branch changes. In patients with painful chronic pancreatitis with ductal obstruction, both endoscopic and surgical management provide adequate drainage. However, significantly better pain control was found after surgery in a long time follow-up study 90. Obstructing PD stones can be removed by using stone extraction balloons or baskets but often lithotripsy is needed to fragment the stones 91. Pancreatic pseudocyst drainage is recommended in patients with symptoms 92. Endo therapy provides a less invasive approach than surgical drainage and a trans papillary approach can be performed if there is a relatively small pseudocyst communicating with the main pancre-atic duct.
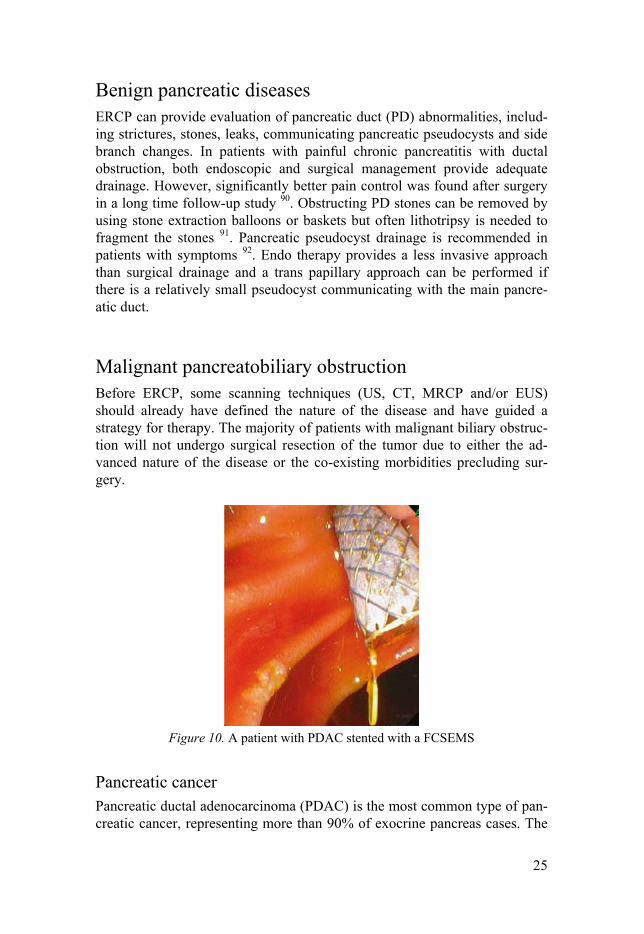
Malignant pancreatobiliary obstruction Before ERCP, some scanning techniques (US, CT, MRCP and/or EUS) should already have defined the nature of the disease and have guided a strategy for therapy. The majority of patients with malignant biliary obstruc-tion will not undergo surgical resection of the tumor due to either the ad-vanced nature of the disease or the co-existing morbidities precluding sur-gery.
Figure 10. A patient with PDAC stented with a FCSEMS
Pancreatic cancer Pancreatic ductal adenocarcinoma (PDAC) is the most common type of pan-creatic cancer, representing more than 90% of exocrine pancreas cases. The
26
other 10% of exocrine tumours are mucinous tumours, mixed adenosqua-mous tumours and acinar cell tumours 93. Endocrine neoplasms contribute approximately 5% of total pancreatic cancer cases.
Pancreatic cancer is associated with a very poor prognosis and 5-year sur-vival is less than 5% 94. Most patients are asymptomatic until the disease develops to an advanced stage. Only up to 20% of patients are eligible for initial resection and even after potentially curative resection most patients will eventually have recurrence 95. Five-year survival of completely resected patients is around to 25% 94, 96. Cigarette smoking is the leading environmen-tal cause of PDAC, with a relative risk =2 compared to non-smokers 97. In early stage pancreatic cancer, jaundice is the only physical finding if the lesion is located in the pancreatic head 98. ERCP with stenting [Figure10] is the mainstay therapy for biliary decompression but routine preoperative bili-ary drainage may be associated with increased complications 99.
IPMN Intraductal papillary mucinous neoplasms (IPMN) are epithelial tumours that arise from the main pancreatic duct or the branch ducts causing ductal dila-tion from mucin production. The identification of asymptomatic cystic le-sions of the pancreas has increased, thanks to the increasing use of high-quality, cross-sectional imaging. The radiographic classification of IPMN into main-duct, branch-duct and mixed variant has formed the backbone of the IPMN management paradigm. The presence of a discrete mass or solid component should be a concern for malignancy. As many as 60% of the main-duct type are malignant and should undergo resection 100. ERCP for cytology may be beneficial for patients with a worrisome feature and main pancreatic duct dilatation, but is not recommended as routine, especially not for branch duct IPMN 101. Direct visualization of a stricture or filling defect by pancreatoscopy is helpful in discriminating malignant from benign intra-ductal lesions.
27
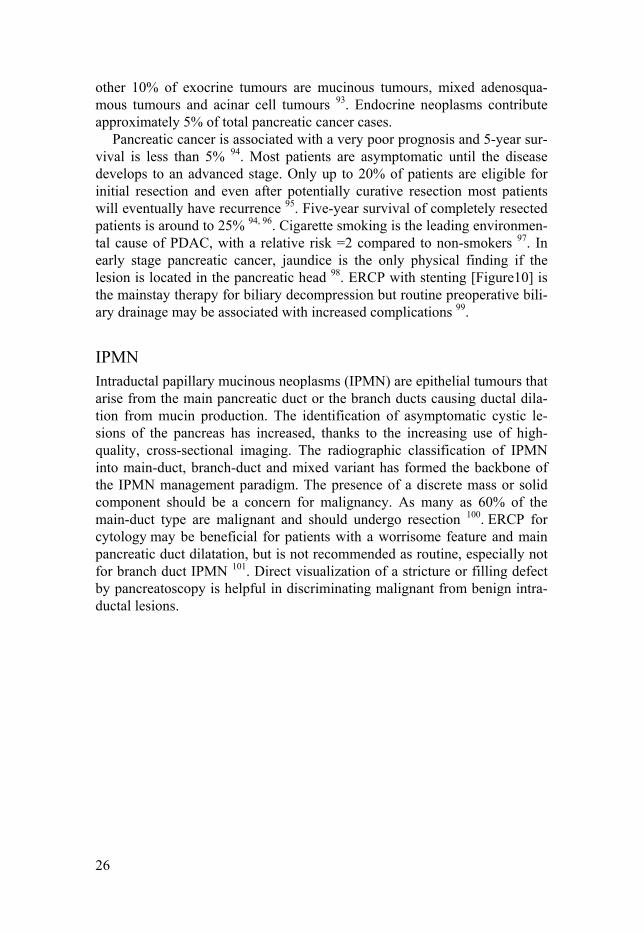
Figure 11. A patient with a perihilar cholangiocarcinoma received two endoprosthe-ses
Cholangiocarcinoma Cholangiocarcinoma is rare and makes up approximately 3% of all gastroin-testinal tract cancers 102. The incidence of intrahepatic cholangiocarcinoma is rising worldwide 103 while cases of extrahepatic cholangiocarcinoma are decreasing 104.This suggests that the tumours may have different etiological factors despite similar microscopic morphology. Perihilar cholangiocarci-noma is commonly diagnosed as an advanced disease at initial presentation. It is difficult to treat and resection is associated with high morbidity and mortality. Biliary drainage with stent placement [Figure 11] can be particu-larly difficult in those with advanced complex strictures. Evaluation with noninvasive imaging (i.e., MRCP) to delineate the anatomy is mandatory for preprocedural planning and helps limit the use of contrast injection during the ERCP and the risk of contaminating undrainable segments. Dilation of ductal strictures before drainage is sometimes necessary to gain access to the ducts. Brush cytology and/or direct cholangioscopic biopsies can then be performed.
Jaundice can be relieved when approximately 25% to 30% of the liver is adequately drained while drainage of greater than 50% is associated with a longer median survival 105.
Cancer of the major duodenal papilla Neoplasms of the papilla may have predominantly intestinal or pancreatobil-iary features or patterns may be mixed. Adenocarcinomas are the most common malignancies of the papilla 106. They can arise from the CBD, pan-creas or duodenum, and secondarily invade the papilla, and be mistaken for a

28
primary tumour. They are often relatively small when detected, presumably because of early obstructive symptoms. At diagnosis, almost 20% are less than 1 cm, and more than 75% are less than 4 cm.
Duodenal adenocarcinoma Duodenal adenocarcinoma is a rare malignancy, which comprises less than 1% of gastrointestinal tumours. More than 50% are periampullary 107. Other malignancies, including carcinoid, lymphoma, and gastrointestinal stromal tumours, may also occur within the duodenum, although these lesions are seen with much greater frequency elsewhere in the small bowel. ERCP can be extremely challenging when there is an overgrowth of cancer within the papilla.
Statistics Hazard Ratio (HR) The hazard ratio is commonly used when presenting survival data e.g. in clinical trials 108. When used in survival analyses it sometimes reflect the time to an event. Time to an event is rarely normally distributed. A hazard is a ratio at which events happens.
The assumption in proportional hazard models for survival analysis is that the hazard in one group is a constant proportion of the hazard in the other group. This proportion is the hazard ratio. It is used to show how many peo-ple can reach a certain point in time without experiencing an event or con-versely determining the number that do.
The hazard ratio differs from relative risk (RR) and odds ratio (OR) be-cause RR and OR are cumulative over a specific time, while HR represents instantaneous risk over a specific time.
Confidence interval This is the interval where the true value is located, with a specific probabil-ity. Confidence intervals measure the degree of uncertainty or certainty in a sampling method. The confidence interval probability is often set to 95% and the narrower the interval, the more certain is the accuracy of the result.
Cox regression The Cox model is a statistical technique for analysing survival data. Survival analysis studies the time between entry into a study and a subsequent event (such as death). The model allows us to isolate the effects of treatment from

29
the effects of other variables and will yield an equation for the hazard as a function of these variables 109.
Life table plot Life tables are one of the oldest statistical techniques and are used to meas-ure the survival outcome or any other well-defined endpoint in different groups over time 109.
Registries The Swedish Population Register All residents in Sweden have been registered since 1968. This is made pos-sible by each person’s unique national registration number 110. The register includes information about every resident’s address, civil status, country of birth, cause of death etc. The Swedish Tax Agency is responsible for the registry but Statistics Sweden, a Swedish government agency, processes data retrieval.
The Swedish National Inpatient Register - IPR More than 99% of all hospital discharges are registered in the IPR, which includes surgical procedures, and about 85-95% of diagnoses are validated 111. The Swedish National Board of Health and Welfare is responsible for this register. The long follow-up makes the register particularly suitable for large- scaled population- based research.
The Swedish Cause of Death Register This register contains data about every person registered in Sweden since 1961 at the time of death and is updated every year. The purpose is to an-swer a variety of questions such as: which deaths could have been avoided? The register can also be available for research.
The Swedish Cancer Register The Swedish Cancer Register is used to chart the occurrence of different cancer diagnoses in Sweden, how they differ over time and how they differ from other places in the world. This register is often used in research pro-jects.

30
National Swedish Register for Gallstone Surgery and Endoscopic Retrograde Cholangiopancreatography (GallRiks) GallRiks was established in 2005 and uses a data internet platform (Gall-Riks, www.ucr.uu.se/gallriks) with online data registration of procedures and 30-day follow-up information. Since its inception, there has been continuing validation resulting in high consistency between the register and medical records. The data registered here represent almost all cholecystectomies and more than 90% of all ERCPs performed in Sweden 4. Many publications are based on data from GallRiks. Hospitals performing ERCPs report to the register continuously. Each year, the number of procedures and reported complications increases.
Epidemiology Bias Bias is a systematic error, providing false results that cannot be corrected in the final analysis of data.
Cohort study A cohort study is a type of longitudinal observational study of a group of people who share the same characteristics or who have experienced a com-mon event. It is often undertaken to obtain evidence to try to refute the exist-ence of a suspected association between cause and effect in a specific inter-val of time.
Endpoint Endpoint refers to any clinical outcome which has been specified in advance.
Confounding Confounding is when something other than the exposure affects the groups studied in different ways and in the end affects the outcome.

31
Aims of the thesis
The overall aims of the thesis were to investigate long-term adverse events after ES, the frequency and causes of perforation associated to ES as well as the outcome after ES, when the gallbladder is still left in situ, as a prophy-laxis after CBDS caused cholangitis and pancreatitis.
Specific aims: I To assess long-term morbidity and mortality after ES for
CBDS compared to the general population. II To investigate whether the results of increased risk for cholan-
gitis and pancreatitis a long time after ES for CBDS, from Study I, remain when compared with other patients with gall-stone diseases.
III To evaluate the outcome of ES after CBDS related cholangitis and pancreatitis, when the gallbladder is still in situ.
IV To analyse the frequency of perforations associated with ERCP and to verify the risk factors for death due to the perfo-ration.

32
Summary of Papers
Late complications after ES Paper I: Late Complications following Endoscopic Sphincterotomy for Cho-ledocholithiasis: a Swedish Population-Based Study
This first paper assesses long-term adverse events after ES for CBDS. The controls were retrieved from the general population.
Patients and methods Patients The study included all patients in central Sweden, who had undergone ERCP with ES for CBDS between 1977 and 1990. A total of 1113 patients were identified through local prospectively completed registers in six different hospitals. These were the only units performing ERCP in this region, at that time. Accordingly, this cohort is population based. The patients´ records were systematically reviewed in order to exclude all procedures performed for indications other than CBDS. Patients with strictures/stenosis were ex-cluded.
Controls Using the Swedish Population Register we were able to identify five age and gender matched controls from the general population, for each patient in the ES cohort. By using the national registration numbers, record links were made to the Inpatient Register.
Methods All patients were followed until December 31, 1999, or until death, or until the patients last control was dead. The first year of follow-up was excluded to avoid morbidity due to a nearby ERCP, such as undiagnosed malignancy. Thus the study consisted of 964 patients available for follow-up. Total mor-bidity was defined as all sicknesses requiring inpatient care. We retrieved information about cholangitis, pancreatitis, CBDS, cholecystitis, jaundice, advanced alcoholism and death. The local registries had no information about whether the patients had undergone cholecystectomy before the ES and the information is therefore lacking.

33
Results Mortality was higher in the ES group, among both men and women 65-79 years old, compared to the control group, HR 1.29 and 1.30 respectively and for men younger than 50, HR 3.22. Total morbidity in the ES group was higher in all age groups except in men older than 80, compared to the control group. Twenty-eight patients in the ES group, 11 with and 17 without con-comitant CBDS, developed acute cholangitis, HR 36. Acute pancreatitis was diagnosed in 26 of the ES patients, only one with CBDS at the same time, HR 6.2. Acute pancreatitis occurred most frequently during the first eight years of the study [Fig 12]. Advanced alcohol abuse was higher in the back-ground population.
Figure 12. Cumulative incidence of pancreatitis 12 months and more after ES.
Confirming the results from the first study Paper II: Long-term risk for acute pancreatitis, cholangitis and malignancy more than 15 years after endoscopic sphincterotomy – a population-based study.
To confirm the results from study I, we retained the ES group, but re-placed the control group to controls with a history of gallstone disease.
Patient and methods Patients The patient cohort was the same as in Paper I.
34
Controls For each patient, six age and gender matched controls, were identified from the Inpatient Register. These were assembled into two cohorts. Group A consisted of patients who had undergone cholecystectomy but not ES, while Group B consisted of patients who had undergone choledochotomy +/- chol-ecystectomy but not ES.
Methods All patients were followed until December 31, 2010, or until the patient or one of the controls died. Events during the first year were excluded to avoid bias due to a diagnosis other than CBDS requiring ES. After the first year 1065 ES patients in Group A and 1,062 ES patients in Group B were availa-ble for follow-up.
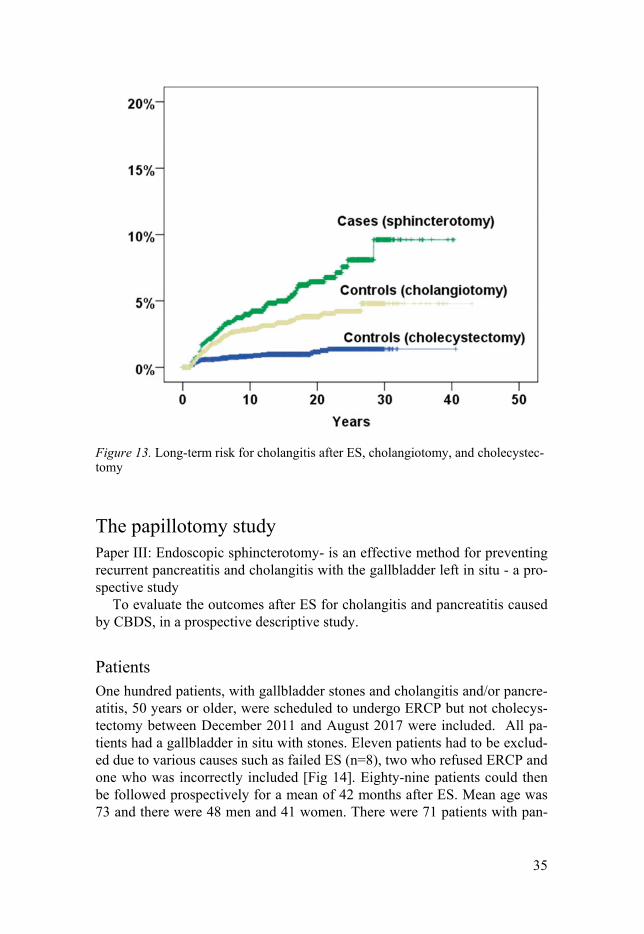
Results The risk for cholangitis [Fig 13], pancreatitis and bile duct stricture was sig-nificantly higher in the ES group when compared with both Group A and Group B containing patients with gallstones diseases who had not undergone ES. No significant increase in risk was seen for the malignant diagnoses. The total morbidity and mortality risks were no higher for the ES group than the control groups.
35
Figure 13. Long-term risk for cholangitis after ES, cholangiotomy, and cholecystec-tomy
The papillotomy study Paper III: Endoscopic sphincterotomy- is an effective method for preventing recurrent pancreatitis and cholangitis with the gallbladder left in situ - a pro-spective study
To evaluate the outcomes after ES for cholangitis and pancreatitis caused by CBDS, in a prospective descriptive study.
Patients One hundred patients, with gallbladder stones and cholangitis and/or pancre-atitis, 50 years or older, were scheduled to undergo ERCP but not cholecys-tectomy between December 2011 and August 2017 were included. All pa-tients had a gallbladder in situ with stones. Eleven patients had to be exclud-ed due to various causes such as failed ES (n=8), two who refused ERCP and one who was incorrectly included [Fig 14]. Eighty-nine patients could then be followed prospectively for a mean of 42 months after ES. Mean age was 73 and there were 48 men and 41 women. There were 71 patients with pan-

36
creatitis, 23 with cholangitis plus an additional five patients with both diag-noses. Thirty-six patients had a CBDS during their ERCP.
Methods A total of 135 patients were identified and extracted from our hospital data base with gallstone cholangitis or/and pancreatitis and of these, 48 missed inclusion in our study. The frequency of diabetes mellitus was higher among the missed patients than among the study patients, but otherwise the baseline characteristics did not differ between the groups. Phone calls to the study patients were made every three months during the first year and then once annually. The median time from the patients’ hospitalization to performed ERCP was 36 days. Gallstone size and amount in the gallbladder and bile duct were measured using ERCP, CT and US images. The largest gallstone was measured. Gallstones 5mm or less were counted as small and the others as big. Three gallstones or fewer were regarded as “single” and more as “multiple”.
Results The study period consisted of a total of 314 patient years at risk. There were no recurrences of gallstone pancreatitis throughout this period. One patient had an episode of cholangitis and underwent a subsequent ERCP. This pa-tient had cholangitis after ES and underwent a laparotomy in an attempt to perform a cholecystectomy, but the surgery was interrupted due to adher-ences. This patient underwent a subsequent ERCP. Due to recurrent CBDS with biliary colic, an additional patient needed an ERCP. It is noteworthy that 11 patients had a recurrence of cholangitis or pancreatitis before their ERCP could be performed in a total of 1.5 patient years. Of the 25 patients that underwent a cholecystectomy, 17 patients had cholecystitis and eight had biliary colic. Fourteen patients with biliary symptoms were treated con-servatively. Among those patients who needed a cholecystectomy, seven were converted from laparoscopic to open surgery. The patients who under-went a cholecystectomy had a mean age significantly lower than that of the patients who did not undergo surgery, 69 and 75 years (p-value <0.001), respectively. The 41 patients with biliary symptoms were also younger than the 48 asymptomatic patients, 70 years old compared to 76 (p-value 0.001). Neither the gallstone size nor amount differed between the pancreatitis and cholangitis patients.

37
Figure 14. Flowchart depicting excluded patients and some follow-up data
The perforation study Paper IV: ERCP-related perforations: a population-based study of incidence, mortality and risk factors
Evaluation of the risk of death after a perforation associated with ERCP, frequency, mechanisms, actions undertaken and patient outcomes.
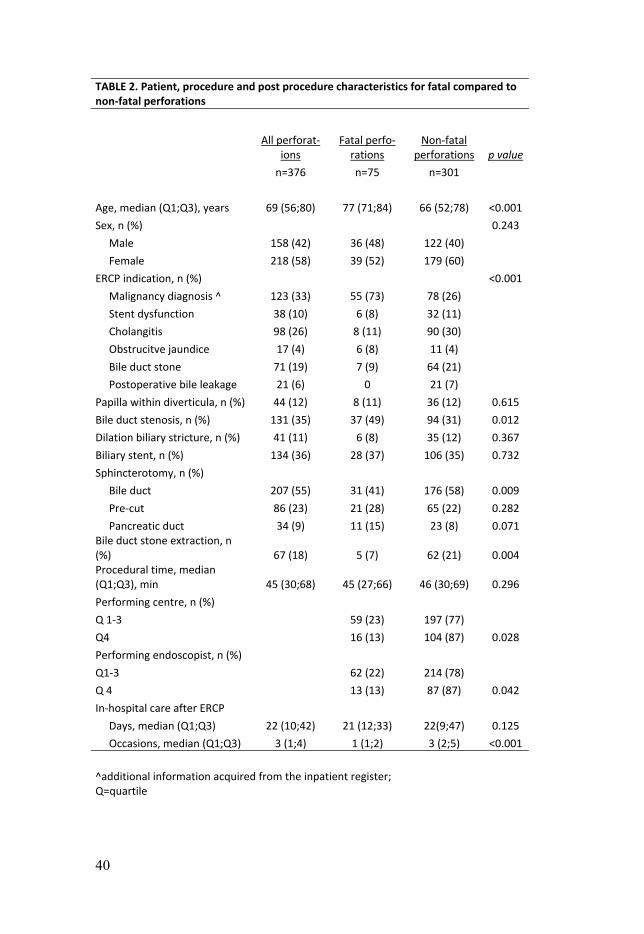
Patients and methods The GallRiks register listed 52,140 patients between May 2005 and to the end of 2013. Among these, 376 (0.72%) perforations were noted. Through the Inpatient Register and the Cause of Death Register we could then identi-fy 75 (0.14%) patients who had died within 90 days or at the index hospitali-zation. Complementary data concerning all ERCPs during the study period were extracted from GallRiks [Table 1]. The 75 dead patients’ records were requested from each hospital that had performed the ERCP. Thirteen patients had to be excluded for various reasons [Fig 1]. The 75 dead patients were defined as the fatal group and were then compared with the patients without deadly perforations, denoted as the non-fatal group [Table 2]. The case vol-

38
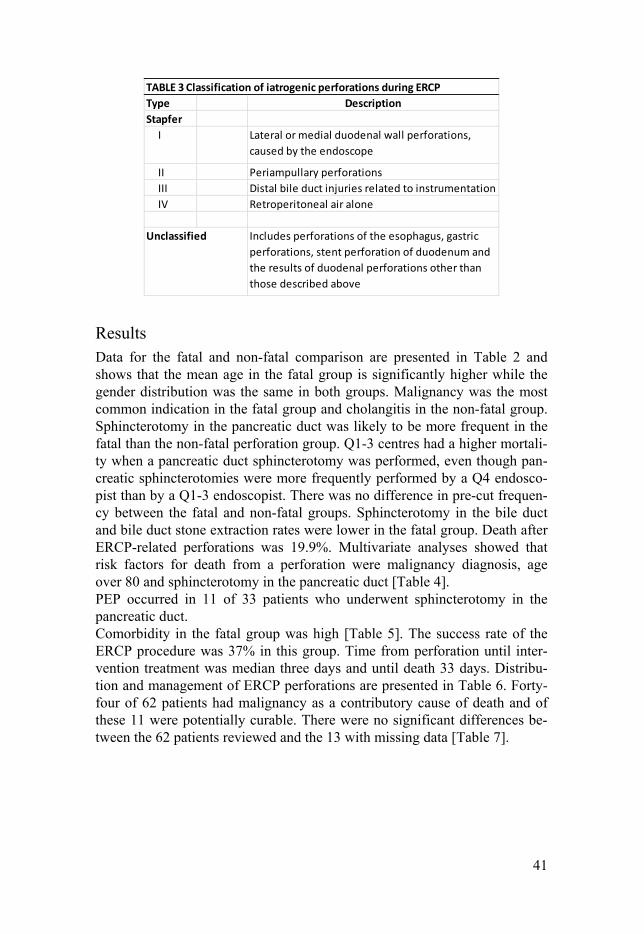
ume of centres and endoscopists was divided into the upper quartile (Q4) and the lower three quartiles (Q1-3) groups. We used the Stapfer classifica-tion system of duodenal perforations after ERCP in order to stratify the inju-ries. The group of injuries that could not be included in the classification system was named unclassified [Table 3].
TABLE 1. Patient and procedure characteristics for all ERCPs performed during study period
All ERCPs n=52 140
Age, mean ± SD, years 67 ± 17 Sex, n (%) Female 28 070 (54) ERCP indication, n (%) Malignancy diagnosis 4 957 (10) Stent dysfunction 2 632 (5) Cholangitis 4 192 (8) Obstrucitve jaundice 11 151 (21) Bile duct stone 16 828 (32) Postoperative bile leakage 1 404 (3) Papilla within diverticula, n (%) 5 543 (11) Bile duct stenosis, n (%) 10 729(21) Sphincterotomy, n (%) Bile duct 27 971 (54) Pre-cut 4 166 (8) Pancreatic duct 1 044 (2) Bile duct stone extraction, n (%) 16 130 (31) Procedural time, mean ± SD, min 36 ± 25

39
Figure 15. Flowchart detailing all included ERCPs and perforations
40
TABLE 2. Patient, procedure and post procedure characteristics for fatal compared to non-fatal perforations
All perforat-
ions Fatal perfo-
rations Non-fatal
perforations p value
n=376 n=75 n=301
Age, median (Q1;Q3), years 69 (56;80) 77 (71;84) 66 (52;78) <0.001
Sex, n (%) 0.243
Male 158 (42) 36 (48) 122 (40)
Female 218 (58) 39 (52) 179 (60)
ERCP indication, n (%) <0.001
Malignancy diagnosis ^ 123 (33) 55 (73) 78 (26)
Stent dysfunction 38 (10) 6 (8) 32 (11)
Cholangitis 98 (26) 8 (11) 90 (30)
Obstrucitve jaundice 17 (4) 6 (8) 11 (4)
Bile duct stone 71 (19) 7 (9) 64 (21)
Postoperative bile leakage 21 (6) 0 21 (7)
Papilla within diverticula, n (%) 44 (12) 8 (11) 36 (12) 0.615
Bile duct stenosis, n (%) 131 (35) 37 (49) 94 (31) 0.012
Dilation biliary stricture, n (%) 41 (11) 6 (8) 35 (12) 0.367
Biliary stent, n (%) 134 (36) 28 (37) 106 (35) 0.732
Sphincterotomy, n (%)
Bile duct 207 (55) 31 (41) 176 (58) 0.009
Pre-cut 86 (23) 21 (28) 65 (22) 0.282
Pancreatic duct 34 (9) 11 (15) 23 (8) 0.071 Bile duct stone extraction, n (%) 67 (18) 5 (7) 62 (21) 0.004 Procedural time, median (Q1;Q3), min 45 (30;68) 45 (27;66) 46 (30;69) 0.296
Performing centre, n (%)
Q 1-3 59 (23) 197 (77)
Q4 16 (13) 104 (87) 0.028
Performing endoscopist, n (%)
Q1-3 62 (22) 214 (78)
Q 4 13 (13) 87 (87) 0.042
In-hospital care after ERCP
Days, median (Q1;Q3) 22 (10;42) 21 (12;33) 22(9;47) 0.125
Occasions, median (Q1;Q3) 3 (1;4) 1 (1;2) 3 (2;5) <0.001
^additional information acquired from the inpatient register; Q=quartile
41
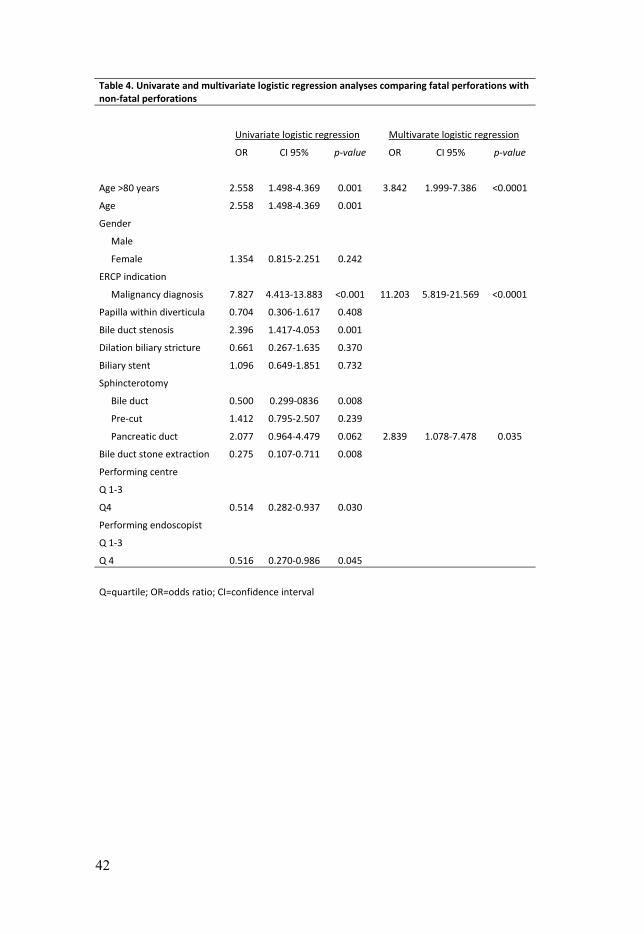
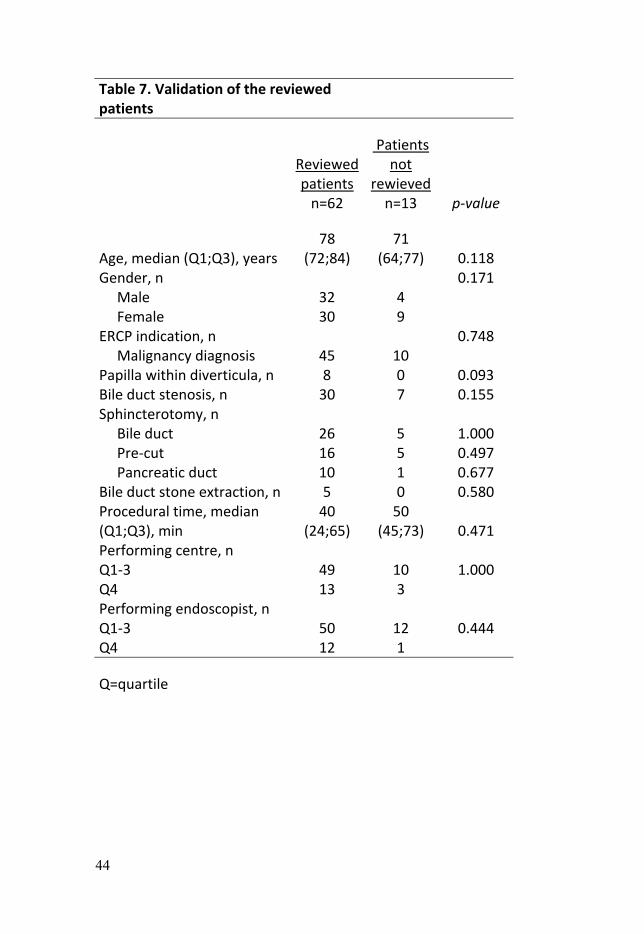
Results Data for the fatal and non-fatal comparison are presented in Table 2 and shows that the mean age in the fatal group is significantly higher while the gender distribution was the same in both groups. Malignancy was the most common indication in the fatal group and cholangitis in the non-fatal group. Sphincterotomy in the pancreatic duct was likely to be more frequent in the fatal than the non-fatal perforation group. Q1-3 centres had a higher mortali-ty when a pancreatic duct sphincterotomy was performed, even though pan-creatic sphincterotomies were more frequently performed by a Q4 endosco-pist than by a Q1-3 endoscopist. There was no difference in pre-cut frequen-cy between the fatal and non-fatal groups. Sphincterotomy in the bile duct and bile duct stone extraction rates were lower in the fatal group. Death after ERCP-related perforations was 19.9%. Multivariate analyses showed that risk factors for death from a perforation were malignancy diagnosis, age over 80 and sphincterotomy in the pancreatic duct [Table 4]. PEP occurred in 11 of 33 patients who underwent sphincterotomy in the pancreatic duct. Comorbidity in the fatal group was high [Table 5]. The success rate of the ERCP procedure was 37% in this group. Time from perforation until inter-vention treatment was median three days and until death 33 days. Distribu-tion and management of ERCP perforations are presented in Table 6. Forty-four of 62 patients had malignancy as a contributory cause of death and of these 11 were potentially curable. There were no significant differences be-tween the 62 patients reviewed and the 13 with missing data [Table 7].
TABLE 3 Classification of iatrogenic perforations during ERCP
Type Description
Stapfer
I Lateral or medial duodenal wall perforations,
caused by the endoscope
II Periampullary perforations
III Distal bile duct injuries related to instrumentation
IV Retroperitoneal air alone
Unclassified Includes perforations of the esophagus, gastric
perforations, stent perforation of duodenum and
the results of duodenal perforations other than
those described above
42
Table 4. Univarate and multivariate logistic regression analyses comparing fatal perforations with non-fatal perforations
Univariate logistic regression Multivarate logistic regression
OR CI 95% p-value OR CI 95% p-value
Age >80 years 2.558 1.498-4.369 0.001 3.842 1.999-7.386 <0.0001
Age 2.558 1.498-4.369 0.001
Gender
Male
Female 1.354 0.815-2.251 0.242
ERCP indication
Malignancy diagnosis 7.827 4.413-13.883 <0.001 11.203 5.819-21.569 <0.0001
Papilla within diverticula 0.704 0.306-1.617 0.408
Bile duct stenosis 2.396 1.417-4.053 0.001
Dilation biliary stricture 0.661 0.267-1.635 0.370
Biliary stent 1.096 0.649-1.851 0.732
Sphincterotomy
Bile duct 0.500 0.299-0836 0.008
Pre-cut 1.412 0.795-2.507 0.239
Pancreatic duct 2.077 0.964-4.479 0.062 2.839 1.078-7.478 0.035
Bile duct stone extraction 0.275 0.107-0.711 0.008
Performing centre
Q 1-3
Q4 0.514 0.282-0.937 0.030
Performing endoscopist
Q 1-3
Q 4 0.516 0.270-0.986 0.045
Q=quartile; OR=odds ratio; CI=confidence interval

43
TABLE 6. Feature of injury and management of the 62 reviewed patients according to classification
Stapfer Total Management
Early treatment
Late treat-ment
Best sup-portive care/No
treatment
I 2 (3) 2 (100) 0 (0) 0 (0)
II 21 (34)
6 (28) 10 (48) 5 (24)
III 20 (32)
10 (50) 4 (20) 6 (30)
IV 0 (0) 0 (0) 0 (0) 0 (0)
Unclassified 19 (31)
7 (37) 10 (53) 2 (10)
% in parentheses; p-value 0.161
44
Table 7. Validation of the reviewed patients
Reviewed patients
Patients not
rewieved n=62 n=13 p-value
Age, median (Q1;Q3), years 78
(72;84) 71
(64;77) 0.118 Gender, n 0.171 Male 32 4 Female 30 9 ERCP indication, n 0.748 Malignancy diagnosis 45 10 Papilla within diverticula, n 8 0 0.093 Bile duct stenosis, n 30 7 0.155 Sphincterotomy, n Bile duct 26 5 1.000 Pre-cut 16 5 0.497 Pancreatic duct 10 1 0.677 Bile duct stone extraction, n 5 0 0.580 Procedural time, median (Q1;Q3), min
40 (24;65)
50 (45;73) 0.471
Performing centre, n Q1-3 49 10 1.000 Q4 13 3 Performing endoscopist, n Q1-3 50 12 0.444 Q4 12 1
Q=quartile

45
Discussion
It is fundamental that health care professionals carry out ERCP as safely as possible. They must have detailed patient information and understand the procedural factors that contribute to risk so they can minimize their impact. This includes careful evaluation of the clinical situation, consideration of whether ERCP is the best way to manage the problem and whether it is worth the risk for the indications. They must also take into account the sup-port team and endoscopist volumes and skills. An experienced team, under-standing and managing the risk factors, can keep adverse events to a mini-mum but cannot rule them out completely.
Recurrence of CBDS after ES Patients diagnosed with CBDS should be offered stone extraction if possible. The benefit is greatest for symptomatic patients 78. ES, EPBD and surgical management are all techniques used in the treatment of CBDS. However, EPBD has a higher rate of acute pancreatitis as an early complication 112. It is recommended in patients undergoing laparoscopic cholecystectomy that transcystic or transductal laparoscopic bile duct exploration (LBDE) and perioperative ERCP are appropriate techniques which are considered equally valid treatment options 78. Long-term results after LBDE have shown a low recurrent stone rate of 2% 113. In Papers I and II the recurrence of CBDS after ES was 4.1% and 5% respectively. In both these studies the first year after ES was excluded and the rates could therefore have been even higher. Reports of recurrent CBDS after ERCP with ES vary between 3.5% and 14% in different studies 114, 115. In some of these studies, long-term results were defined as 30 days or longer after ES. However, stones can be missed during ERCP and left in the common bile duct (CBD). If the gallbladder is left in situ, new stones can also move from the gallbladder throughout ductus cysti-cus to the CBD. It has been suggested that bacterial infection following abla-tion of the sphincter mechanism may play a role in the new formation of stones in the CBD 116. The presence of pneumobilia, which indicates signifi-cant reflux of duodenal contents into the CBD, seems to be a risk factor for recurrent CBDS 117. Patients with dilated bile ducts were especially prone to forming new stones 118. In Papers I and II we had no access to information about eventual pneumobilia or whether the bile duct was dilated.
46
Cholangitis after ES Cholangitis usually occurs along with CBDS, but there are reported cases of cholangitis without concomitant CBDS after ES 11, 114. In Papers I and II, 61% and 91.5%, respectively, of the patients with cholangitis had no recur-rences of CBDS at the same time. In both Papers I and II, cholangitis oc-curred during the entire study period. After ES, the opening between the CBD and duodenum can permit duodenal contents to enter into the biliary tree and cause contamination. However, if we cannot close the gate com-pletely after stone extraction, as occurs with EPBD, we can prevent it from remaining wide open. The use of performing a limited ES, followed by EPBD, can be a successful half-way measure, perhaps reducing the likeli-hood of duodenobiliary reflux and its complications 119. However, a limited sphincterotomy of the duodenal papilla may lead to symptomatic stenosis of the bile duct and main pancreatic duct orifices 120. Contrary to our results in Papers I and II, there were no recurrences of cholangitis without CBDS in Paper III, which reviewed 314 patient years at risk after ES.
Pancreatitis after ES A long-term increased risk for acute pancreatitis after ES for CBDS was noted in both Papers I and II. The increased risk was not explained by con-comitant CBDS. No further reports on the subject have been published since our studies. We had the same theory for this occurrence of pancreatitis in our Papers I and II as in the appearance of cholangitis without concomitant CBDS, namely the possibility of the reflux of duodenal contents up in the pancreatic duct after opening up the sphincter of Oddi with an ES. Another explanation could be the possibility of a stone migration from CBDS into the duodenum before ERCP. A transient ampullary obstruction caused by a mi-gratory stone is a generally accepted pathogenesis in acute gallstone pan-creatitis 121.
Benign bile duct stricture after ES The incidence of bile duct stricture after ES for CBDS is low and includes stenosis of the papilla. It may also occur after inflammation such as pancrea-titis and cholangitis. It is obvious that the risk for stricture is higher among patients who have had a stone sickness compared to the background popula-tion (Paper I) but the risk remains when comparing ES patients to other gall-stone sick patients who did not undergo ES (Paper II). The increased risk may be due to a stenosis of the papilla after ES. This was more common in the early days of the ERCP era because fear of perforation limited the use of

47
ES. Biliary injury associated with ERCP may be difficult to assess since guidewires and accessories can pass through the wall of the ducts unnoticed during the procedure but may cause a stricture after extension when healing. Chronic inflammation caused by prolonged duodenal reflux can also cause biliary strictures.
Malignancy after ES In Paper II, we assessed malignancy in the bile duct, pancreas and the major duodenal papilla after ES. No increased cancer risk was seen when compar-ing ES patients with other gallstone patients who did not undergo ERCP with ES. According to these results, the first population-based study, per-formed in 1997 12 demonstrated no increased risk of cancer following ES with a median follow-up of 9 years. In 2008 and 2016, Stömberg et al 14, 122 presented long-term follow-up studies showing an increased risk of malig-nancy in the pancreatobiliary tract after ERCP in benign disease but ES did not affect that risk. The risk also seemed to decrease over the follow-up pe-riod. Similar results were obtained by Mortensen et al. 123. The gradual de-crease in the rate of cholangiocarcinoma over time following ERCP indicat-ed that, in some of these patients, malignancy may have been present at the time of ERCP but not diagnosed until after the procedure. Patients who had undergone cholecystectomy irrespective of ES, had a lower risk of malig-nancy than those who had not undergone cholecystectomy 14. This finding suggests that the process of carcinogenesis in these patients might be con-nected with gallstone disease. However, cancer of the bile duct is a rare ma-lignancy with a low expected incidence limiting the analyses of cancer risk by follow-up duration. Malignant transformation of the choledochal epitheli-um under exposure to digestive enzymes and bacteria will need a longer time to be verified 124 than the completed studies to day can offer.
Overall morbidity and mortality after ERCP In Paper I, the overall morbidity and mortality after ES was significantly increased compared to the background population. These results could not be confirmed in Paper II when comparing ES patients with other patients with gallstone diseases, indicating that the increased overall morbidity and mor-tality after ES in Paper I may be caused by the underlying gallstone disease per se. It is difficult to analyse the reported deaths after ERCP as the spectra of patients and procedures differ as well as the time after ERCP. Attributing mortality between concurrent illness, active complications and complications due to other procedures required after ERCP failure can be a great challenge. One large meta-analysis included 21 prospective studies and reported ERCP-

48
related mortality of 0.33% 125. The most common complications causing death after ERCP result from pancreatitis, bleeding, perforation, infection and cardiopulmonary events. Delay in the diagnosis of perforation is a con-tributing cause of death 126. In Paper IV, the fatal ERCP group had multiple comorbidities, making them particularly susceptible to complications. This group also had a low ERCP success rate (37%). Completion of the intended ERCP procedure has been found to decrease mortality 43. Not surprisingly, older patients with comorbid conditions, e.g. cancer, have increased post-ERCP mortality 127-129.
ES as a prevention of recurrent gallstone pancreatitis and cholangitis with the gallbladder left in situ In Paper III, we showed the usefulness of ES in the a prevention of recurrent gallstone pancreatitis and cholangitis, when the gallbladder is left in situ. In total, we studied 314 patient years and saw no recurrence of gallstone pan-creatitis and only one case of cholangitis. This result is similar to many other studies on this subject 130-137. Twenty-eight per cent of the patients in Paper III needed a cholecystectomy after ES and an additional 18 % had biliary symptoms. Patients needing surgery and patients with biliary symptoms after ES were significantly younger. Earlier studies have noted a lower incidence of acute cholecystitis in patients older than 80 years than in the younger pa-tients 138. Some studies have shown greater complication rates following laparoscopic cholecystectomy in the elderly population 139, associated with a higher conversion rate, increased morbidity, and a longer hospital stay. Nev-ertheless, most studies suggest that, given an acceptable perioperative risk profile, elderly patients with symptomatic gallstone disease should be treated surgically 140. However, following ES some RCTs have been published, the first by Hammarström 141, suggesting ES alone as a feasible treatment for elderly and high-risk patients. This is in line with our conclusions, and we therefore suggest cholecystectomy for the younger population. However, despite the good prevention of the recurrence of pancreatitis and cholangitis, there is a high incidence of other gallstone-related sicknesses and a high risk of having to convert the laparoscopic procedure to open surgery. In Paper III, acute cholecystitis was the most common gallstone sickness to relapse into. If cholecystitis is treated conservatively and the gallbladder is left in situ, there is a 22% risk of developing recurrent gallstone-related disease within a period of two years [139]. There has been a recent discussion as to whether it is safer to leave the gallbladder in situ after a mild attack of cholecystitis, as this has a success rate of 96% 142.

49
Perforations associated with ERCP Paper IV showed a high proportion of sphincterotomies in the pancreatic duct, in the fatal group. Both precut and sphincterotomy in the pancreatic duct are valuable complements in difficult cannulations 143 and have been discussed as risk factors for perforations in earlier studies 44, 45. However, when precut is used by experienced endoscopists the risk appears to be lower 144. A meta-analysis of six trials comparing early precut versus persistent attempts at standard cannulation showed that the overall rate of adverse events was 5% after early precut, which is not significantly different from 6% in the control group 145. It is unknown whether only experienced endos-copists participated in those trials. In a systematic review and meta-analysis, demonstrating a correlation between high endoscopist volume and a low number of adverse events 27, we found that endoscopist and centre volume definitions varied widely between studies. Thus, there is no agreed number of procedures that count as high or low. It is necessary to have international discussion and agreement in this matter to create a clear definition, as to how many procedures must be performed before reaching a safe ERCP proce-dure.
Earlier studies have discussed the high risk of pancreatitis after sphincter-otomy in the pancreatic duct 146. In our study a high number of patients (33%) developed pancreatitis after perforation due to a sphincterotomy in the pancreatic duct. However, this is not surprising considering the location of the perforation. The paucity of cases with perforation after sphincterotomy of the pancreatic duct and the lack of published studies on the subject should inspire additional studies to explore this issue. The longer procedure time in the perforation group shows that this group had more complex procedures throughout their ERCPs than the all-ERCP group.
In Paper IV, we found a high proportion of deaths after perforation (19.9%) in comparison to earlier studies, which have reported around 10% 147-150. The fatal perforation group consisted of significantly older patients with a higher comorbidity and malignancy was diagnosed more frequently than in the non-fatal perforation group. This has probably contributed strong-ly to these patients’ mortality. Earlier studies have shown increased post-ERCP mortality in older patients with comorbid conditions e.g. cancer 127-129. The success rate of ERCP completion was only 37% in the fatal group. Car-rying out the intended ERCP procedure is important for patient outcomes as this has been found to decrease mortality 43. It is also important to detect and manage perforations as soon as possible after they occur 46. In the fatal group the time to detection and further management was long. We could not com-pare this with the non-fatal perforations since we did not have access to pa-tient records in this group. The fact that patients with malignancy, even when the cancer was potentially curable, may have contributed to a less ac-tive approach in this group and thus a worse outcome.

50
Clinical relevance With Papers I and II, implementation of the study result in clinical practice can be difficult. It is seldom possible to avoid sphincterotomy when an ERCP is being performed and CBDS is found. In those cases, leaving the stones behind is not an option. Also, a sphincterotomy is usually performed even if CBDS is not found during the procedure. Patients with gallstone-related diseases and long life expectancy, and with the gallbladder still left in situ should therefore be scheduled for a cholecystectomy instead, and if CBDS is found, a perioperative ERCP can be carried out. Study III strength-ens this opinion. Older patients with shorter life expectancy and with comor-bidities can be treated advantageously with sphincterotomy and not be ini-tially scheduled for surgery for their CBDS, cholangitis and/or pancreatitis. Unfortunately complications sometimes occur during ERCP and Study IV demonstrates that if a perforation related to sphincterotomy in the pancreatic duct happens at a Q1-3 centre the patient has a worse outcome than if the perforation happens at a Q4 centre. This indicates that a patient should be transported from a Q1-3 centre to a Q4 centre, if a perforation associated with sphincterotomy in the pancreatic duct occurs.
51
Conclusions
Paper I In this register cohort study, comparing ES patients with controls from the general population, both acute pancreatitis and cholangitis seem to be proba-ble long-term complications after ES. Mortality was not affected in all age groups. This was partly in line with our hypothesis.
Paper II This long-term follow-up study, comparing ES patients with controls treated for gallstone disease without undergoing ES, shows a significantly increased risk for both acute cholangitis and pancreatitis after ES but not for cancer in the pancreatobiliary tract. This was partly in line with our hypothesis.
Paper III ES prevents recurrences of gallstone pancreatitis and cholangitis when the gallbladder is left in situ. Aged and/or infirm patients can benefit from being treated with ES alone and without an initially planned cholecystectomy. This was in line with our hypothesis.
Paper IV The frequency of ERCP related perforations is low but it carries a high mor-tality rate. Age above 80, a malignancy diagnosis and sphincterotomy in the pancreatic duct are risk factors for death after a perforation. Q1-3 centres had a higher fatal outcome than Q4 centres after a perforation due to a sphincter-otomy in the pancreatic duct. This was in line with our hypothesis.
52
Future aspects
It is important to continue long-term follow-up after ERCP with ES concern-ing the possible development of malignancy due to chronic inflammation in the biliary tract. The follow-up period in the studies so far has been too short and too few patients have been included in the studies. A longer follow-up after ES of the patients studied in Paper III is necessary, to further explore whether there are cases of pancreatitis and/or cholangitis both with and without concomitant recurrences of bile duct stones.
Perforations associated with ERCP are uncommon and it is difficult to do large studies on the subject. We are planning a review of all patient records concerning ERCP perforations registered in GallRiks between 2005 and 2013. We also plan to further examine perforation cases caused by stent migration. The risk for pancreatitis after a perforation related to sphincterotomy in the pancreatic duct is high. It would be interesting to investigate the outcome of all sphincterotomies in the pancreatic duct in order to calculate whether it is the perforation per se or whether the sphincterotomy in the pancreatic duct causes a higher risk of pancreatitis.

53
Svensk sammanfattning
ERCP är en av de mest komplexa av de olika endoskopiska procedurer som finns tillgängliga och sedan introduktionen 1968 utförs allt fler undersök-ningar världen över. ERCP används både för att åtgärda vanliga sjukdomar och för att utreda mer komplicerade sjukdomar i gallvägarna och bukspott-körtelgången. De terapeutiska procedurerna har ökat 30-faldigt de senaste decennierna medan de diagnostiska undersökningarna minskat något. Detta dels på grund av att nya moderna undersökningsmetoder såsom magnetka-mera och endoskopiskt ultraljud finns tillgängliga allt oftare men också för de komplikationer som uppstår i samband med ERCP.
Korttidskomplikationerna är välkända och den vanligaste är inflammation i bukspottkörteln och förekommer i ungefär 5 % av fallen. Blödning, infekt-ioner och skador på tolvfingertarmen förekommer i varierande grad i sam-band med ERCP. Både faktorer kopplade till patienten och proceduren är viktiga att känna till för att minska frekvensen av komplikationer.
Papillotomi innebär att man delar muskeln mellan gallgången och tolv-fingertarmen så att t.ex. stenar i gallgången kan avlägsnas lättare. Papillo-tomi ökar risken för komplikation främst i form av perforation. När det är svårt att komma in i gallgången används ibland en speciell form av papillo-tomi s.k. precut, som i vissa studier ger ökad risk för perforation. Det gäller också papillotomi i pankreasgången som ibland behövs för att t.ex. avlägsna stenar. Perforation i samband med ERCP är ett allvarligt och livshotande tillstånd. Det är viktigt att så snabbt som möjligt diagnostisera en perforation så att patienten kan få adekvat behandling.
En papillotomi görs ibland för att förebygga återinsjuknande i gallstensor-sakad inflammation i bukspottkörteln då gallstenar som hamnar i gallgången i senare skede lättare kan passera ut i tarmen. Det är fortfarande omtvistat ifall dessa patienter även behöver en efterföljande gallblåseoperation.
Långtidseffekten efter en papillotomi är inte så välstuderad men det finns studier som visar att det blir ett backflöde av tarminnehåll upp i gall och pankreasgång efter muskeldelningen av papillen. Det kan i sin tur ge en ökad risk för både infektion i gallgången och inflammation i bukspottkörteln utan samtidig återinsjuknande av sten i gallgången. Att kronisk inflammation kan trigga cancer är välkänt. Kopplingen mellan cancer och genomgången papil-lotomi är ännu inte helt utesluten på grund av för kort uppföljningstid i de studier som publicerats. I början av ERCP eran utfördes undersökningen främst på äldre patienter med hög samsjuklighet men numer används meto-
54
den på unga för övrigt friska patienter. Det är därför viktigt att veta att vi inte skapar en ökad cancerrisk hos de patienter som papillotomeras.
Delarbete I I denna studie ingår 1113 patienter som genomgick ERCP med papillotomi på något av de sex sjukhus i Mellansverige där ERCP genomfördes åren 1977 till 1990. Alla patienterna fick ålders och köns matchade kontroller från normalbefolkningen via svenska befolkningsregistret och följdes sedan tills patienten dog, alla kontrollerna var döda eller tom år 1999. Resultatet visade att det förekom högre grad av både infektion i gallgången och in-flammation i bukspottkörteln hos de patienter som genomgått ERCP med papillotomi även om de inte hade återinsjuknande i gallgångssten.
Delarbete II Vi använde samma patienter som i delarbete I men matchade med nya kon-troller som delades in i två grupper, tre i varje. Kontrollgrupp A bestod av patienter som genomgått galloperation men inte papillotomi och kontroll-grupp B som genomgått öppning av gallgången med borttagning av sten men inte papillotomi. Det visade sig att patientgruppen som genomgått ERCP med papillotomi hade högre risk att få infektion i gallgången och inflammat-ion i bukspottkörteln än båda kontrollgrupperna. Dock var inte risken för cancer i bukspottkörteln, gallgången eller papillen förhöjd.
Delarbete III I denna studie inkluderades 100 st. patienter med akut gallstens orsakad in-flammation i bukspottkörteln och/eller infektion i gallvägarna och som hade gallblåsan kvar. De fick inte ha haft eller ha en pågående inflammation i gallblåsan och de skulle vara 50 år eller äldre. Alla planerades för ERCP med papillotomi. 89st var tillgängliga för uppföljning då 11 st. behövde ex-kluderas av olika anledningar, men de flesta pga. misslyckad ERCP. Dessa patienter följdes sedan i genomsnitt 42 månader genom telefonsamtal var tredje månad första året och därefter en gång per år. Det som efterfrågades var uppkomna gallrelaterade besvär och genomgångna ERCPer och operat-ioner. Ingen av dessa patienter återinsjukande i inflammation i bukspottkör-teln och endast en patient i infektion i gallvägarna. Av dessa 89 patienter behövde 25 st. operera bort sin gallblåsa varav en stor andel blev komplice-rade och krävde öppen operation.

55
Delarbete IV GallRiks, som är ett nationellt register för gallstensoperationer och ERCPer, söktes igenom efter de patienter som blivit registrerade med en perforation antingen under själva ERCP ingreppet eller inom 30 dagar efter undersök-ningen. Bland 52140 ERCPer fanns 376 registrerade som perforationer mel-lan åren 2005 och 2013. Av dessa dog 75 st. inom en tre månaders period eller inom indexvårdtillfället och deras journalkopior beställdes från respek-tive sjukhus. Några journalkopior kunde inte återfinnas och ytterligare några exkluderades då perforation inte kunde bekräftas. Det återstod 62 st. patien-ter som kallades dödlig perforationsgrupp och kunde jämföras med övriga perforationer. Bakgrundsdata på alla 52140 ERCPer extraherades också från GallRiks. Dödligheten efter en perforation var 20 %. Ålder över 80 år, ma-lignitets diagnos och papillotomi i pankreasgången visade sig öka risken att dö efter en perforation. Risken att dö efter en perforation i buksottkörtel-gången minskade om den inträffade på ett Q4 center.
Sammanfattning ERCP med papillotomi ökar risken för inflammation i bukspottkörteln och infektion i gallvägarna på lång sikt.
ERCP med papillotomi kan förebygga återinsjuknande i gallstensrelaterad bukspottkörtelinflammation och gallgångs infektion då gallblåsan inte opere-ras bort.
Dödligheten efter en ERCP relaterad perforation är hög. Risken att dö i en perforation är högre för patienter äldre än 80, om det förekommer en malign diagnos och om patienten genomgått en papillotomi i pankreasgången. Ris-kan att dö efter en perforation relaterad till en papillotomi i pankreasgången minskade om patienten befann sig på ett Q4 center.
56
Acknowledgements
I would like to express my deepest gratitude to the following people who have supported this thesis in different ways:
Britt-Marie Karlson, my main tutor for introducing me to the wonderful world of science, ERCP and pancreatic surgery. Thank you for believing in me and for encouraging further research.
Bengt Isaksson, co-tutor, for giving excellent advice and for your encour-agement. Per Hellman, co-tutor, for support in various ways.
Ulf Haglund, for giving me the opportunity to do this thesis.
Gabriel Sandblom, co-author for help with analysing data and for your valu-able comments.
Stefan Linder, co-author for giving brilliant comments and linguistic im-provements of the manuscript and for being a fantastic clinician and friend. Anders Ekbom, co-author, for your excellent comments and for invaluable help in handling data in Paper I.
Mikael Ljungdahl, co-author, for help with collecting patients for Paper III.
Magnus Sundbom, for support in various ways and for providing time.
Jozef Urdzik for helping me with statistical issues.
Petter Frühling for assisting with the translation of Paper III. My past and current colleagues at the HPB unit: Christopher Månsson, Ag-neta Norén, Arne Eklund, Frans Duraj, Maria Johansson, Peter Moberger, Eva-Lena Syrén, Laura Zarantonello, Hanna Sternby, Christoph Ansorge, Farima Brandt

57
Former and current Heads of the Department of Surgery, Uppsala University Hospital, Ewa Lundgren, Staffan Wollert, Claes Juhlin and Kristna Ahlgren, and Olle Nilsson, former Head of the Department of Surgical Sciences, Upp-sala University. My dear colleagues with whom I share an office: Maria Söderström, Bjarni Vidarson and Branislav Climácek.
Håkan Andreasson, Åsa Collin, Lana Ghanipour, David Edholm, Malin Enblad, Willhelm Graf, Jakob Hedberg, Gustav Linder, Eduardo Sima, Mar-tin Löfling Skogar, Sara Artursson, Khalid Elias, Henrik Benoni for all the discussions at the seminars, and Joakim Folkesson for making them possible.
All my other fellow colleagues at the Department of Surgery, Uppsala Uni-versity Hospital for all the joy of working together. All colleagues and co-workers in Gävle and Bollnäs and a special thanks to Michael Krog and Jörgen Block for being fantastic teachers and role-models early in my surgical career. My childhood friend, Anna-Lena Wirén, for always being there.
My brother Roger and his daughters Agnes and Alice for all the happy times we have had over the years.
Naimy, my dear mother in law for always helping with so many things. Last but certainly not least I want to thank my beloved and wonderful fami-ly: my husband, Torbjörn, for always supporting me in everything and for serving delicious dinners and our children Viktor, Johannes, Anna and Dan-iel, together with their beloved ones, for bringing us so much joy and happi-ness in life.

58
References
1. Moffatt DC, Yu BN, Yie W, et al. Trends in utilization of diagnostic and therapeutic ERCP and cholecystectomy over the past 25 years: a population-based study. Gastrointest Endosc 2014;79:615-22.
2. Pereira P, Peixoto A, Andrade P, et al. Peroral cholangiopancreatoscopy with the SpyGlass(R) system: what do we know 10 years later. J Gastrointestin Liver Dis 2017;26:165-170.
3. Enochsson L, Swahn F, Arnelo U, et al. Nationwide, population-based data from 11,074 ERCP procedures from the Swedish Registry for Gallstone Sur-gery and ERCP. Gastrointest Endosc 2010;72:1175-84, 1184 e1-3.
4. Enochsson L, Thulin A, Osterberg J, et al. The Swedish Registry of Gallstone Surgery and Endoscopic Retrograde Cholangiopancreatography (GallRiks): A nationwide registry for quality assurance of gallstone surgery. JAMA Surg 2013;148:471-8.
5. Kanamori A, Kiriyama S, Tanikawa M, et al. Long- and short-term outcomes of ERCP for bile duct stones in patients over 80 years old compared to younger patients: a propensity score analysis. Endosc Int Open 2016;4:E83-90.
6. Wojtun S, Gil J, Gietka W, et al. Endoscopic sphincterotomy for choledocho-lithiasis: a prospective single-center study on the short-term and long-term treatment results in 483 patients. Endoscopy 1997;29:258-65.
7. Bill JG, Smith Z, Brancheck J, et al. The importance of early recognition in management of ERCP-related perforations. Surg Endosc 2018;32:4841-4849.
8. Sugiyama M, Atomi Y. Follow-up of more than 10 years after endoscopic sphincterotomy for choledocholithiasis in young patients. Br J Surg 1998;85:917-21.
9. Sugiyama M, Atomi Y. Risk factors predictive of late complications after endoscopic sphincterotomy for bile duct stones: long-term (more than 10 years) follow-up study. Am J Gastroenterol 2002;97:2763-7.
10. Schreurs WH, Juttmann JR, Stuifbergen WN, et al. Management of common bile duct stones: selective endoscopic retrograde cholangiography and endo-scopic sphincterotomy: short- and long-term results. Surg Endosc 2002;16:1068-72.
11. Costamagna G, Tringali A, Shah SK, et al. Long-term follow-up of patients after endoscopic sphincterotomy for choledocholithiasis, and risk factors for recurrence. Endoscopy 2002;34:273-9.
12. Karlson BM, Ekbom A, Arvidsson D, et al. Population-based study of cancer risk and relative survival following sphincterotomy for stones in the common bile duct. Br J Surg 1997;84:1235-8.
13. Langerth A, Sandblom G, Karlson BM. Long-term risk for acute pancreatitis, cholangitis, and malignancy more than 15 years after endoscopic sphincterot-omy: a population-based study. Endoscopy 2015;47:1132-6.

59
14. Stromberg C, Luo J, Enochsson L, et al. Endoscopic sphincterotomy and risk of malignancy in the bile ducts, liver, and pancreas. Clin Gastroenterol Hepa-tol 2008;6:1049-53.
15. Classen M, Demling L. [Endoscopic sphincterotomy of the papilla of vater and extraction of stones from the choledochal duct (author's transl)]. Dtsch Med Wochenschr 1974;99:496-7.
16. Vaishali MD, Agarwal AK, Upadhyaya DN, et al. Magnetic resonance chol-angiopancreatography in obstructive jaundice. J Clin Gastroenterol 2004;38:887-90.
17. Saftoiu A, Vilmann P. Role of endoscopic ultrasound in the diagnosis and staging of pancreatic cancer. J Clin Ultrasound 2009;37:1-17.
18. Zandrino F, Benzi L, Ferretti ML, et al. Multislice CT cholangiography with-out biliary contrast agent: technique and initial clinical results in the assess-ment of patients with biliary obstruction. Eur Radiol 2002;12:1155-61.
19. Karaahmet F, Kekilli M. The presence of periampullary diverticulum in-creased the complications of endoscopic retrograde cholangiopancreatog-raphy. Eur J Gastroenterol Hepatol 2018;30:1009-1012.
20. Giovannini M, Moutardier V, Pesenti C, et al. Endoscopic ultrasound-guided bilioduodenal anastomosis: a new technique for biliary drainage. Endoscopy 2001;33:898-900.
21. Bahra M, Jacob D. Surgical palliation of advanced pancreatic cancer. Recent Results Cancer Res 2008;177:111-20.
22. Guo J, Giovannini M, Sahai AV, et al. A multi-institution consensus on how to perform EUS-guided biliary drainage for malignant biliary obstruction. Endosc Ultrasound 2018;7:356-365.
23. Khan MA, Akbar A, Baron TH, et al. Endoscopic Ultrasound-Guided Biliary Drainage: A Systematic Review and Meta-Analysis. Dig Dis Sci 2016;61:684-703.
24. Itonaga M, Kitano M, Hatamaru K, et al. Endoscopic ultrasound-guided cho-ledochoduodenostomy using a thin stent delivery system in patients with un-resectable malignant distal biliary obstruction: A prospective multicenter study. Dig Endosc 2018.
25. Ekkelenkamp VE, de Man RA, Ter Borg F, et al. Prospective evaluation of ERCP performance: results of a nationwide quality registry. Endoscopy 2015;47:503-7.
26. Cote GA, Imler TD, Xu H, et al. Lower provider volume is associated with higher failure rates for endoscopic retrograde cholangiopancreatography. Med Care 2013;51:1040-7.
27. Keswani RN, Qumseya BJ, O'Dwyer LC, et al. Association Between Endos-copist and Center Endoscopic Retrograde Cholangiopancreatography Volume With Procedure Success and Adverse Outcomes: A Systematic Review and Meta-analysis. Clin Gastroenterol Hepatol 2017;15:1866-1875 e3.
28. Dwyer L, Polavarapu N, Hood S, et al. PWE-009 Per oral cholangioscopy: systematic evaluation in clinical practice. Gut 2010;59:A88-A89.
29. Aljabiri M, Lerman A, Kalaitzakis E, et al. PWE-005 Initial experience of spyglass per-oral cholangioscopy in a UK centre. Gut 2010;59:A87-A87.
30. Laleman W, Verraes K, Van Steenbergen W, et al. Usefulness of the single-operator cholangioscopy system SpyGlass in biliary disease: a single-center prospective cohort study and aggregated review. Surg Endosc 2017;31:2223-2232.
31. Zippi M, Familiari P, Traversa G, et al. Role of endoscopic sphincterotomy of the minor papilla in pancreas divisum. Clin Ter 2014;165:e312-6.

60
32. Freeman ML, Nelson DB, Sherman S, et al. Complications of endoscopic biliary sphincterotomy. N Engl J Med 1996;335:909-18.
33. Masci E, Toti G, Mariani A, et al. Complications of diagnostic and therapeu-tic ERCP: a prospective multicenter study. Am J Gastroenterol 2001;96:417-23.
34. Li GZ, Wang F, Fang J, et al. Risk Factors for Post-Endoscopic Retrograde Cholangiopancreatography Pancreatitis: Evidence from 1786 Cases. Med Sci Monit 2018;24:8544-8552.
35. Loperfido S, Angelini G, Benedetti G, et al. Major early complications from diagnostic and therapeutic ERCP: a prospective multicenter study. Gastroin-test Endosc 1998;48:1-10.
36. Freeman ML, DiSario JA, Nelson DB, et al. Risk factors for post-ERCP pancreatitis: a prospective, multicenter study. Gastrointest Endosc 2001;54:425-34.
37. Mehta SN, Pavone E, Barkun JS, et al. Predictors of post-ERCP complica-tions in patients with suspected choledocholithiasis. Endoscopy 1998;30:457-63.
38. Liu L, Li C, Huang Y, et al. Nonsteroidal Anti-inflammatory Drugs for En-doscopic Retrograde Cholangiopancreatography Postoperative Pancreatitis Prevention: a Systematic Review and Meta-analysis. J Gastrointest Surg 2018.
39. Fazel A, Quadri A, Catalano MF, et al. Does a pancreatic duct stent prevent post-ERCP pancreatitis? A prospective randomized study. Gastrointest En-dosc 2003;57:291-4.
40. Dubecz A, Ottmann J, Schweigert M, et al. Management of ERCP-related small bowel perforations: the pivotal role of physical investigation. Can J Surg 2012;55:99-104.
41. Preetha M, Chung YF, Chan WH, et al. Surgical management of endoscopic retrograde cholangiopancreatography-related perforations. ANZ J Surg 2003;73:1011-4.
42. Kim J, Lee SH, Paik WH, et al. Clinical outcomes of patients who experi-enced perforation associated with endoscopic retrograde cholangiopancrea-tography. Surg Endosc 2012;26:3293-300.
43. Srivastava S, Sharma BC, Puri AS, et al. Impact of completion of primary biliary procedure on outcome of endoscopic retrograde cholangiopancreato-graphic related perforation. Endosc Int Open 2017;5:E706-E709.
44. Enns R, Eloubeidi MA, Mergener K, et al. ERCP-related perforations: risk factors and management. Endoscopy 2002;34:293-8.
45. Cotton PB. Analysis of 59 ERCP lawsuits; mainly about indications. Gastro-intest Endosc 2006;63:378-82; quiz 464.
46. Cirocchi R, Kelly MD, Griffiths EA, et al. A systematic review of the man-agement and outcome of ERCP related duodenal perforations using a stand-ardized classification system. Surgeon 2017;15:379-387.
47. Lee SM, Cho KB. Value of temporary stents for the management of perivate-rian perforation during endoscopic retrograde cholangiopancreatography. World J Clin Cases 2014;2:689-97.
48. Garcia-Cano J, Taberna-Arana L, Jimeno-Ayllon C, et al. Use of fully cov-ered self-expanding metal stents for the management of benign biliary condi-tions. Rev Esp Enferm Dig 2010;102:526-32.
49. Stapfer M, Selby RR, Stain SC, et al. Management of Duodenal Perforation After Endoscopic Retrograde Cholangiopancreatography and Sphincteroto-my. Annals of Surgery 2000;232:191-198.

61
50. Motte S, Deviere J, Dumonceau JM, et al. Risk factors for septicemia follow-ing endoscopic biliary stenting. Gastroenterology 1991;101:1374-81.
51. Harris A, Chan AC, Torres-Viera C, et al. Meta-analysis of antibiotic prophy-laxis in endoscopic retrograde cholangiopancreatography (ERCP). Endosco-py 1999;31:718-24.
52. Suk KT, Kim HS, Kim JW, et al. Risk factors for cholecystitis after metal stent placement in malignant biliary obstruction. Gastrointest Endosc 2006;64:522-9.
53. Cotton PB, Garrow DA, Gallagher J, et al. Risk factors for complications after ERCP: a multivariate analysis of 11,497 procedures over 12 years. Gas-trointest Endosc 2009;70:80-8.
54. Feng Y, Zhu H, Chen X, et al. Comparison of endoscopic papillary large balloon dilation and endoscopic sphincterotomy for retrieval of choledocho-lithiasis: a meta-analysis of randomized controlled trials. J Gastroenterol 2012;47:655-63.
55. Tsujino T, Isayama H, Komatsu Y, et al. Risk factors for pancreatitis in pa-tients with common bile duct stones managed by endoscopic papillary bal-loon dilation. Am J Gastroenterol 2005;100:38-42.
56. Kamisawa T, Okamoto A. Biliopancreatic and pancreatobiliary refluxes in cases with and without pancreaticobiliary maljunction: diagnosis and clinical implications. Digestion 2006;73:228-36.
57. Sogaard KK, Erichsen R, Lund JL, et al. Cholangitis and subsequent gastro-intestinal cancer risk: a Danish population-based cohort study. Gut 2014;63:356-61.
58. Sandler RS, Everhart JE, Donowitz M, et al. The burden of selected digestive diseases in the United States. Gastroenterology 2002;122:1500-11.
59. Aerts R, Penninckx F. The burden of gallstone disease in Europe. Aliment Pharmacol Ther 2003;18 Suppl 3:49-53.
60. Festi D, Reggiani ML, Attili AF, et al. Natural history of gallstone disease: Expectant management or active treatment? Results from a population-based cohort study. J Gastroenterol Hepatol 2010;25:719-24.
61. Berger MY, van der Velden JJ, Lijmer JG, et al. Abdominal symptoms: do they predict gallstones? A systematic review. Scand J Gastroenterol 2000;35:70-6.
62. Barbara L, Sama C, Morselli Labate AM, et al. A population study on the prevalence of gallstone disease: the Sirmione Study. Hepatology 1987;7:913-7.
63. Halldestam I, Enell EL, Kullman E, et al. Development of symptoms and complications in individuals with asymptomatic gallstones. Br J Surg 2004;91:734-8.
64. Diehl AK. Epidemiology and natural history of gallstone disease. Gastroen-terol Clin North Am 1991;20:1-19.
65. Maclure KM, Hayes KC, Colditz GA, et al. Weight, diet, and the risk of symptomatic gallstones in middle-aged women. N Engl J Med 1989;321:563-9.
66. Volzke H, Baumeister SE, Alte D, et al. Independent risk factors for gallstone formation in a region with high cholelithiasis prevalence. Digestion 2005;71:97-105.
67. Friedman GD. Natural history of asymptomatic and symptomatic gallstones. Am J Surg 1993;165:399-404.
62
68. van Dijk AH, de Reuver PR, Besselink MG, et al. Assessment of available evidence in the management of gallbladder and bile duct stones: a systematic review of international guidelines. HPB (Oxford) 2017;19:297-309.
69. Houdart R, Perniceni T, Darne B, et al. Predicting common bile duct lithiasis: determination and prospective validation of a model predicting low risk. Am J Surg 1995;170:38-43.
70. Videhult P, Sandblom G, Rasmussen IC. How reliable is intraoperative chol-angiography as a method for detecting common bile duct stones? : A pro-spective population-based study on 1171 patients. Surg Endosc 2009;23:304-12.
71. Collins C, Maguire D, Ireland A, et al. A prospective study of common bile duct calculi in patients undergoing laparoscopic cholecystectomy: natural his-tory of choledocholithiasis revisited. Ann Surg 2004;239:28-33.
72. Nebiker CA, Baierlein SA, Beck S, et al. Is routine MR cholangiopancreatog-raphy (MRCP) justified prior to cholecystectomy? Langenbecks Arch Surg 2009;394:1005-10.
73. Jovanovic P, Salkic NN, Zerem E, et al. Biochemical and ultrasound parame-ters may help predict the need for therapeutic endoscopic retrograde cholan-giopancreatography (ERCP) in patients with a firm clinical and biochemical suspicion for choledocholithiasis. Eur J Intern Med 2011;22:e110-4.
74. Boraschi P, Gigoni R, Braccini G, et al. Detection of common bile duct stones before laparoscopic cholecystectomy. Evaluation with MR cholangi-ography. Acta Radiol 2002;43:593-8.
75. Caddy GR, Tham TC. Gallstone disease: Symptoms, diagnosis and endo-scopic management of common bile duct stones. Best Pract Res Clin Gastro-enterol 2006;20:1085-101.
76. Aiura K, Kitagawa Y. Current status of endoscopic papillary balloon dilation for the treatment of bile duct stones. J Hepatobiliary Pancreat Sci 2011;18:339-45.
77. Karsenti D, Coron E, Vanbiervliet G, et al. Complete endoscopic sphincter-otomy with vs. without large-balloon dilation for the removal of large bile duct stones: randomized multicenter study. Endoscopy 2017;49:968-976.
78. Williams E, Beckingham I, El Sayed G, et al. Updated guideline on the man-agement of common bile duct stones (CBDS). Gut 2017;66:765-782.
79. Noel R, Arnelo U, Swahn F. Intraoperative versus postoperative rendezvous endoscopic retrograde cholangiopancreatography to treat common bile duct stones during cholecystectomy. Dig Endosc 2018.
80. Syrén E-L, Sandblom G, Eriksson S, et al. Postoperative rendezvous endo-scopic retrograde cholangiopancreaticography as an option in the manage-ment of choledocholithiasis. Surgical Endoscopy 2019.
81. Ozcan N, Kahriman G, Mavili E. Percutaneous transhepatic removal of bile duct stones: results of 261 patients. Cardiovasc Intervent Radiol 2012;35:621-7.
82. Lefemine V, Morgan RJ. Spontaneous passage of common bile duct stones in jaundiced patients. Hepatobiliary Pancreat Dis Int 2011;10:209-13.
83. Balandraud P, Biance N, Peycru T, et al. Fortuitous discovery of common bile duct stones: results of a conservative strategy. Gastroenterol Clin Biol 2008;32:408-12.
84. Möller M, Gustafsson U, Rasmussen F, et al. Natural course vs interventions to clear common bile duct stones: Data from the swedish registry for gall-stone surgery and endoscopic retrograde cholangiopancreatography (gallriks). JAMA Surgery 2014;149:1008-1013.
63
85. Kim SB, Nam YJ, Kim KH, et al. Is endoscopic sphincterotomy beneficial for the treatment of acute gallstone pancreatitis with small bile duct stone? Eur J Gastroenterol Hepatol 2019;31:192-196.
86. Catalano MF, Linder JD, George S, et al. Treatment of symptomatic distal common bile duct stenosis secondary to chronic pancreatitis: comparison of single vs. multiple simultaneous stents. Gastrointest Endosc 2004;60:945-52.
87. Kaffes AJ, Liu K. Fully covered self-expandable metal stents for treatment of benign biliary strictures. Gastrointest Endosc 2013;78:13-21.
88. Kaya M, Petersen BT, Angulo P, et al. Balloon dilation compared to stenting of dominant strictures in primary sclerosing cholangitis. Am J Gastroenterol 2001;96:1059-66.
89. Aabakken L, Karlsen TH, Albert J, et al. Role of endoscopy in primary scle-rosing cholangitis: European Society of Gastrointestinal Endoscopy (ESGE) and European Association for the Study of the Liver (EASL) Clinical Guide-line. Endoscopy 2017;49:588-608.
90. Cahen DL, Gouma DJ, Nio Y, et al. Endoscopic versus surgical drainage of the pancreatic duct in chronic pancreatitis. N Engl J Med 2007;356:676-84.
91. Tandan M, Reddy DN, Santosh D, et al. Extracorporeal shock wave lithotrip-sy and endotherapy for pancreatic calculi-a large single center experience. Indian J Gastroenterol 2010;29:143-8.
92. Jacobson BC, Baron TH, Adler DG, et al. ASGE guideline: The role of en-doscopy in the diagnosis and the management of cystic lesions and inflam-matory fluid collections of the pancreas. Gastrointest Endosc 2005;61:363-70.
93. Cowgill SM, Muscarella P. The genetics of pancreatic cancer. Am J Surg 2003;186:279-86.
94. Siegel R, Ma J, Zou Z, et al. Cancer statistics, 2014. CA Cancer J Clin 2014;64:9-29.
95. Gillen S, Schuster T, Meyer Zum Buschenfelde C, et al. Preopera-tive/neoadjuvant therapy in pancreatic cancer: a systematic review and meta-analysis of response and resection percentages. PLoS Med 2010;7:e1000267.
96. https://www.cancercentrum.se/globalassets/cancerdiagnoser/bukspottkortel/ kvalitetsregister/pankreascancerarsrapport2018.pdf.
97. Lowenfels AB, Maisonneuve P. Epidemiology and prevention of pancreatic cancer. Jpn J Clin Oncol 2004;34:238-44.
98. De La Cruz MS, Young AP, Ruffin MT. Diagnosis and management of pan-creatic cancer. Am Fam Physician 2014;89:626-32.
99. van der Gaag NA, Rauws EA, van Eijck CH, et al. [Preoperative biliary drainage for pancreatic head tumours: more complications]. Ned Tijdschr Geneeskd 2010;154:A1883.
100. Lafemina J, Katabi N, Klimstra D, et al. Malignant progression in IPMN: a cohort analysis of patients initially selected for resection or observation. Ann Surg Oncol 2013;20:440-7.
101. Yoshioka T, Shigekawa M, Yamai T, et al. The safety and benefit of pancre-atic juice cytology under ERCP in IPMN patients. Pancreatology 2016;16:1020-1027.
102. Lazaridis KN, Gores GJ. Cholangiocarcinoma. Gastroenterology 2005;128:1655-67.
103. Olnes MJ, Erlich R. A review and update on cholangiocarcinoma. Oncology 2004;66:167-79.
64
104. Endo I, Gonen M, Yopp AC, et al. Intrahepatic cholangiocarcinoma: rising frequency, improved survival, and determinants of outcome after resection. Ann Surg 2008;248:84-96.
105. Vienne A, Hobeika E, Gouya H, et al. Prediction of drainage effectiveness during endoscopic stenting of malignant hilar strictures: the role of liver vol-ume assessment. Gastrointest Endosc 2010;72:728-35.
106. Albores-Saavedra J, Schwartz AM, Batich K, et al. Cancers of the ampulla of vater: demographics, morphology, and survival based on 5,625 cases from the SEER program. J Surg Oncol 2009;100:598-605.
107. Ross RK, Hartnett NM, Bernstein L, et al. Epidemiology of adenocarcinomas of the small intestine: is bile a small bowel carcinogen? Br J Cancer 1991;63:143-5.
108. Spruance SL, Reid JE, Grace M, et al. Hazard Ratio in Clinical Trials. Anti-microbial Agents and Chemotherapy 2004;48:2787-2792.
109. Cox DR. Regression Models and Life-Tables. Journal of the Royal Statistical Society. Series B (Methodological) 1972;34:187-220.
110. Lunde AS, Lundeborg S, Lettenstrom GS, et al. The person-number systems of Sweden, Norway, Denmark, and Israel. Vital Health Stat 2 1980:1-59.
111. Ludvigsson J, Andersson E, Ekbom A, et al. External review and validation of the Swedish national inpatient register. BMC Public Health 2011;11:1-16.
112. Baron TH, Harewood GC. Endoscopic balloon dilation of the biliary sphinc-ter compared to endoscopic biliary sphincterotomy for removal of common bile duct stones during ERCP: a metaanalysis of randomized, controlled tri-als. Am J Gastroenterol 2004;99:1455-60.
113. Quaresima S, Balla A, Guerrieri M, et al. A 23 year experience with laparo-scopic common bile duct exploration. HPB (Oxford) 2017;19:29-35.
114. Prat F, Malak NA, Pelletier G, et al. Biliary symptoms and complications more than 8 years after endoscopic sphincterotomy for choledocholithiasis. Gastroenterology 1996;110:894-9.
115. Bergman JJ, van der Mey S, Rauws EA, et al. Long-term follow-up after endoscopic sphincterotomy for bile duct stones in patients younger than 60 years of age. Gastrointest Endosc 1996;44:643-9.
116. Tanaka M, Takahata S, Konomi H, et al. Long-term consequence of endo-scopic sphincterotomy for bile duct stones. Gastrointest Endosc 1998;48:465-9.
117. Fujimoto T, Tsuyuguchi T, Sakai Y, et al. Long-term outcome of endoscopic papillotomy for choledocholithiasis with cholecystolithiasis. Dig Endosc 2010;22:95-100.
118. Pereira-Lima JC, Jakobs R, Winter UH, et al. Long-term results (7 to 10 years) of endoscopic papillotomy for choledocholithiasis. Multivariate analy-sis of prognostic factors for the recurrence of biliary symptoms. Gastrointest Endosc 1998;48:457-64.
119. Attasaranya S, Cheon YK, Vittal H, et al. Large-diameter biliary orifice bal-loon dilation to aid in endoscopic bile duct stone removal: a multicenter se-ries. Gastrointest Endosc 2008;67:1046-52.
120. Khandekar S, Disario JA. Endoscopic therapy for stenosis of the biliary and pancreatic duct orifices. Gastrointest Endosc 2000;52:500-5.
121. Acosta JM, Ledesma CL. Gallstone Migration as a Cause of Acute Pancreati-tis. New England Journal of Medicine 1974;290:484-487.
122. Stromberg C, Bockelman C, Song H, et al. Endoscopic sphincterotomy and risk of cholangiocarcinoma: a population-based cohort study in Finland and Sweden. Endosc Int Open 2016;4:E1096-e1100.

65
123. Mortensen FV, Jepsen P, Tarone RE, et al. Endoscopic sphincterotomy and long-term risk of cholangiocarcinoma: a population-based follow-up study. J Natl Cancer Inst 2008;100:745-50.
124. Kurumado K, Nagai T, Kondo Y, et al. Long-term observations on morpho-logical changes of choledochal epithelium after choledochoenterostomy in rats. Dig Dis Sci 1994;39:809-20.
125. Andriulli A, Loperfido S, Napolitano G, et al. Incidence Rates of Post-ERCP Complications: A Systematic Survey of Prospective Studies. Am J Gastroen-terol 2007;102:1781-1788.
126. Howard TJ, Tan T, Lehman GA, et al. Classification and management of perforations complicating endoscopic sphincterotomy. Surgery 1999;126:658-63; discussion 664-5.
127. Kalaitzakis E. All-cause mortality after ERCP. Endoscopy 2016;48:987-994. 128. Glomsaker T, Hoff G, Kvaloy JT, et al. Patterns and predictive factors of
complications after endoscopic retrograde cholangiopancreatography. Br J Surg 2013;100:373-80.
129. Bodger K, Bowering K, Sarkar S, et al. All-cause mortality after first ERCP in England: clinically guided analysis of hospital episode statistics with link-age to registry of death. Gastrointest Endosc 2011;74:825-33.
130. Schreurs WH, Vles WJ, Stuifbergen WH, et al. Endoscopic management of common bile duct stones leaving the gallbladder in situ. A cohort study with long-term follow-up. Dig Surg 2004;21:60-4; discussion 65.
131. Bignell M, Dearing M, Hindmarsh A, et al. ERCP and endoscopic sphincter-otomy (ES): a safe and definitive management of gallstone pancreatitis with the gallbladder left in situ. J Gastrointest Surg 2011;15:2205-10.
132. Sanjay P, Yeeting S, Whigham C, et al. Endoscopic sphincterotomy and interval cholecystectomy are reasonable alternatives to index cholecystecto-my in severe acute gallstone pancreatitis (GSP). Surg Endosc 2008;22:1832-7.
133. Vazquez-Lglesias JL, Gonzalez-Conde B, Lopez-Roses L, et al. Endoscopic sphincterotomy for prevention of the recurrence of acute biliary pancreatitis in patients with gallbladder in situ: long-term follow-up of 88 patients. Surg Endosc 2004;18:1442-6.
134. Welbourn CR, Beckly DE, Eyre-Brook IA. Endoscopic sphincterotomy without cholecystectomy for gall stone pancreatitis. Gut 1995;37:119-120.
135. Uomo G, Manes G, Laccetti M, et al. Endoscopic sphincterotomy and recur-rence of acute pancreatitis in gallstone patients considered unfit for surgery. Pancreas 1997;14:28-31.
136. Hernandez V, Pascual I, Almela P, et al. Recurrence of acute gallstone pan-creatitis and relationship with cholecystectomy or endoscopic sphincteroto-my. Am J Gastroenterol 2004;99:2417-23.
137. Kaw M, Al-Antably Y, Kaw P. Management of gallstone pancreatitis: chole-cystectomy or ERCP and endoscopic sphincterotomy. Gastrointest Endosc 2002;56:61-5.
138. Yasui T, Takahata S, Kono H, et al. Is cholecystectomy necessary after endo-scopic treatment of bile duct stones in patients older than 80 years of age? J Gastroenterol 2012;47:65-70.
139. Pavlidis TE, Marakis GN, Symeonidis N, et al. Considerations concerning laparoscopic cholecystectomy in the extremely elderly. J Laparoendosc Adv Surg Tech A 2008;18:56-60.

66
140. Leandros E, Alexakis N, Archontovasilis F, et al. Outcome analysis of lapa-roscopic cholecystectomy in patients aged 80 years and older with complicat-ed gallstone disease. J Laparoendosc Adv Surg Tech A 2007;17:731-5.
141. Hammarstrom LE, Holmin T, Stridbeck H. Endoscopic treatment of bile duct calculi in patients with gallbladder in situ: long-term outcome and factors. Scand J Gastroenterol 1996;31:294-301.
142. Loozen CS, Oor JE, van Ramshorst B, et al. Conservative treatment of acute cholecystitis: a systematic review and pooled analysis. Surg Endosc 2017;31:504-515.
143. Catalano MF, Linder JD, Geenen JE. Endoscopic transpancreatic papillary septotomy for inaccessible obstructed bile ducts: Comparison with standard pre-cut papillotomy. Gastrointest Endosc 2004;60:557-61.
144. Navaneethan U, Konjeti R, Venkatesh PG, et al. Early precut sphincterotomy and the risk of endoscopic retrograde cholangiopancreatography related com-plications: An updated meta-analysis. World J Gastrointest Endosc 2014;6:200-8.
145. Cennamo V, Fuccio L, Zagari RM, et al. Can early precut implementation reduce endoscopic retrograde cholangiopancreatography-related complication risk? Meta-analysis of randomized controlled trials. Endoscopy 2010;42:381-8.
146. Zhong H, Wang X, Yang L, et al. Modified transprepancreatic septotomy reduces postoperative complications after intractable biliary access. Medicine (Baltimore) 2018;97:e9522.
147. Machado NO. Management of duodenal perforation post-endoscopic retro-grade cholangiopancreatography. When and whom to operate and what fac-tors determine the outcome? A review article. JOP 2012;13:18-25.
148. Jin Y-J, Jeong S, Kim JH, et al. Clinical course and proposed treatment strat-egy for ERCP-related duodenal perforation: a multicenter analysis. Endosco-py 2013;45:806-812.
149. Alfieri S, Rosa F, Cina C, et al. Management of duodeno-pancreato-biliary perforations after ERCP: outcomes from an Italian tertiary referral center. Surg Endosc 2013;27:2005-12.
150. Fatima J, Baron TH, Topazian MD, et al. Pancreaticobiliary and duodenal perforations after periampullary endoscopic procedures: diagnosis and man-agement. Arch Surg 2007;142:448-54; discussion 454-5.


Acta Universitatis UpsaliensisDigital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1665
Editor: The Dean of the Faculty of Medicine
A doctoral dissertation from the Faculty of Medicine, UppsalaUniversity, is usually a summary of a number of papers. A fewcopies of the complete dissertation are kept at major Swedishresearch libraries, while the summary alone is distributedinternationally through the series Digital ComprehensiveSummaries of Uppsala Dissertations from the Faculty ofMedicine. (Prior to January, 2005, the series was publishedunder the title “Comprehensive Summaries of UppsalaDissertations from the Faculty of Medicine”.)
Distribution: publications.uu.seurn:nbn:se:uu:diva-408046
ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2020