energy techniques (met) before looking at met and the ... · therapist (isometric contraction)....
TRANSCRIPT
Sport | MET
26 Issue 97 July 2011 InternatIonal therapIst www.fht.org.uk
Muscle Energy Techniques
An additional tool for the physical therapist’s ‘manual therapy toolbox’,
Muscle Energy Techniques (MET) can help to release and relax muscles, and promote the body’s own healing mechanisms.
MET is unique in its application as the client provides the initial effort while the practitioner facilitates the process. The primary force originates from the contraction of soft tissue, which is then utilised to assist and correct the presenting musculoskeletal dysfunction.
MET is generally classified as a direct technique – as opposed to indirect – because the muscular effort is from a controlled position, in a specific direction, against a distant counter force (usually the practitioner). One of the main uses of this method is to normalise joint range, rather than increase flexibility, and techniques can be used on any joints with restricted range of motion (ROM) identified during the passive assessment.
The benefits of MET may include:l Restoring normal tone in hypertonic musclesPhysical therapists use MET to try to help relax the hypertonic shortened muscles. If a joint has limited ROM, then through the initial identification of the hypertonic structures, techniques can help to achieve normality in the tissues. MET applied in conjunction with massage therapy can be very beneficial in helping to achieve this relaxation effect.l Strengthening weak musclesMET can be used to help strengthen weak, or even flaccid, muscles, with the client advised to contract the muscle classified as weak against a resistance applied by the therapist (isometric contraction). Timing of techniques can be varied, for example, the client resists the movement to approximately 20 to 30 per cent of their capability for five to 10 seconds, resting for 10 to 15 seconds, and then repeating the process five to eight times. This can be improved over time.l Preparing muscle for subsequent stretchingIn some circumstances, the sport a client participates in may affect joint ROM. Most people can benefit from improved flexibility, and although the focus of MET is to reach ‘normal’ ROM, a more intensive
MET approach can be employed to improve flexibility beyond this. This might involve the client contracting beyond the standard 10 to 20 per cent of the muscle’s capability. Once MET has been incorporated into the treatment plan, a flexibility programme could follow.l Improved joint mobility‘A stiff joint can become a tight muscle and a tight muscle can become a stiff joint’. When used correctly, MET can improve joint mobility, even when you are relaxing the muscles initially. A relaxation period follows the muscle contraction, which then helps to achieve the ‘new’ ROM.
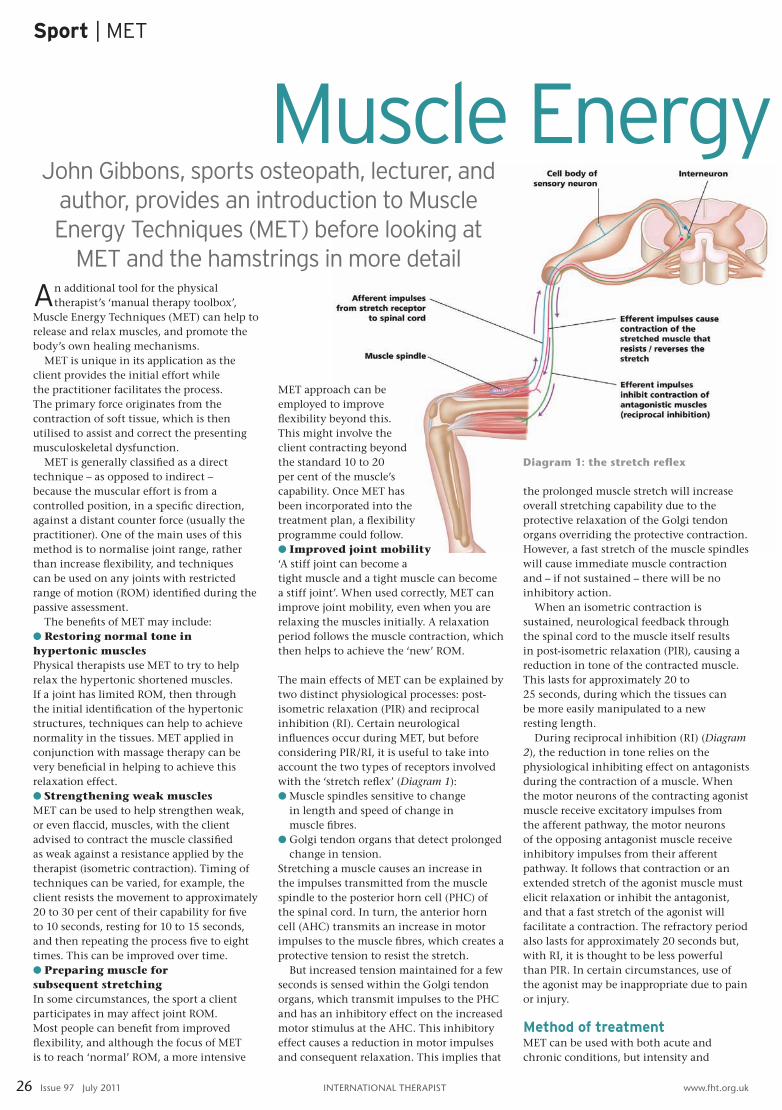
The main effects of MET can be explained by two distinct physiological processes: post- isometric relaxation (PIR) and reciprocal inhibition (RI). Certain neurological influences occur during MET, but before considering PIR/RI, it is useful to take into account the two types of receptors involved with the ‘stretch reflex’ (Diagram 1):l Muscle spindles sensitive to change
in length and speed of change in muscle fibres.
l Golgi tendon organs that detect prolonged change in tension.
Stretching a muscle causes an increase in the impulses transmitted from the muscle spindle to the posterior horn cell (PHC) of the spinal cord. In turn, the anterior horn cell (AHC) transmits an increase in motor impulses to the muscle fibres, which creates a protective tension to resist the stretch.
But increased tension maintained for a few seconds is sensed within the Golgi tendon organs, which transmit impulses to the PHC and has an inhibitory effect on the increased motor stimulus at the AHC. This inhibitory effect causes a reduction in motor impulses and consequent relaxation. This implies that
the prolonged muscle stretch will increase overall stretching capability due to the protective relaxation of the Golgi tendon organs overriding the protective contraction. However, a fast stretch of the muscle spindles will cause immediate muscle contraction and – if not sustained – there will be no inhibitory action.
When an isometric contraction is sustained, neurological feedback through the spinal cord to the muscle itself results in post-isometric relaxation (PIR), causing a reduction in tone of the contracted muscle. This lasts for approximately 20 to 25 seconds, during which the tissues can be more easily manipulated to a new resting length.
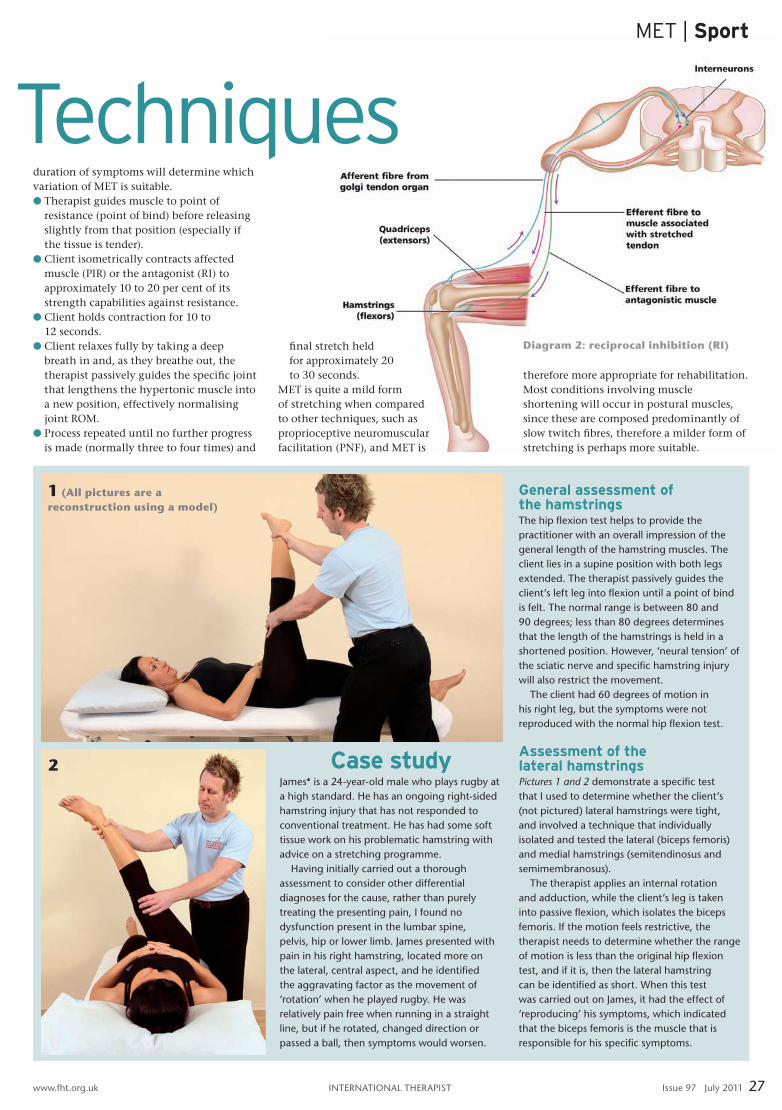
During reciprocal inhibition (RI) (Diagram 2), the reduction in tone relies on the physiological inhibiting effect on antagonists during the contraction of a muscle. When the motor neurons of the contracting agonist muscle receive excitatory impulses from the afferent pathway, the motor neurons of the opposing antagonist muscle receive inhibitory impulses from their afferent pathway. It follows that contraction or an extended stretch of the agonist muscle must elicit relaxation or inhibit the antagonist, and that a fast stretch of the agonist will facilitate a contraction. The refractory period also lasts for approximately 20 seconds but, with RI, it is thought to be less powerful than PIR. In certain circumstances, use of the agonist may be inappropriate due to pain or injury.
Method of treatmentMET can be used with both acute and chronic conditions, but intensity and
John Gibbons, sports osteopath, lecturer, and author, provides an introduction to Muscle Energy Techniques (MET) before looking at
MET and the hamstrings in more detail
Diagram 1: the stretch reflex
Case studyJames* is a 24-year-old male who plays rugby at a high standard. he has an ongoing right-sided hamstring injury that has not responded to conventional treatment. he has had some soft tissue work on his problematic hamstring with advice on a stretching programme.
having initially carried out a thorough assessment to consider other differential diagnoses for the cause, rather than purely treating the presenting pain, I found no dysfunction present in the lumbar spine, pelvis, hip or lower limb. James presented with pain in his right hamstring, located more on the lateral, central aspect, and he identified the aggravating factor as the movement of ‘rotation’ when he played rugby. he was relatively pain free when running in a straight line, but if he rotated, changed direction or passed a ball, then symptoms would worsen.
General assessment of the hamstringsthe hip flexion test helps to provide the practitioner with an overall impression of the general length of the hamstring muscles. the client lies in a supine position with both legs extended. the therapist passively guides the client’s left leg into flexion until a point of bind is felt. the normal range is between 80 and 90 degrees; less than 80 degrees determines that the length of the hamstrings is held in a shortened position. however, ‘neural tension’ of the sciatic nerve and specific hamstring injury will also restrict the movement.
the client had 60 degrees of motion in his right leg, but the symptoms were not reproduced with the normal hip flexion test.
Assessment of the lateral hamstringsPictures 1 and 2 demonstrate a specific test that I used to determine whether the client’s (not pictured) lateral hamstrings were tight, and involved a technique that individually isolated and tested the lateral (biceps femoris) and medial hamstrings (semitendinosus and semimembranosus).
the therapist applies an internal rotation and adduction, while the client’s leg is taken into passive flexion, which isolates the biceps femoris. If the motion feels restrictive, the therapist needs to determine whether the range of motion is less than the original hip flexion test, and if it is, then the lateral hamstring can be identified as short. When this test was carried out on James, it had the effect of ‘reproducing’ his symptoms, which indicated that the biceps femoris is the muscle that is responsible for his specific symptoms.
MET | Sport
InternatIonal therapIst www.fht.org.uk www.fht.org.uk InternatIonal therapIst Issue 97 July 2011 27
Muscle Energy Techniquesduration of symptoms will determine which variation of MET is suitable.l Therapist guides muscle to point of
resistance (point of bind) before releasing slightly from that position (especially if the tissue is tender).
l Client isometrically contracts affected muscle (PIR) or the antagonist (RI) to approximately 10 to 20 per cent of its strength capabilities against resistance.
l Client holds contraction for 10 to 12 seconds.
l Client relaxes fully by taking a deep breath in and, as they breathe out, the therapist passively guides the specific joint that lengthens the hypertonic muscle into a new position, effectively normalising joint ROM.
l Process repeated until no further progress is made (normally three to four times) and
final stretch held for approximately 20 to 30 seconds.
MET is quite a mild form of stretching when compared to other techniques, such as proprioceptive neuromuscular facilitation (PNF), and MET is
therefore more appropriate for rehabilitation. Most conditions involving muscle shortening will occur in postural muscles, since these are composed predominantly of slow twitch fibres, therefore a milder form of stretching is perhaps more suitable.
2
1 (All pictures are a reconstruction using a model)
Diagram 2: reciprocal inhibition (RI)
Sport | MET
28 Issue 97 July 2011 InternatIonal therapIst www.fht.org.uk
pIc
ture
s: l
otu
s pu
blI
shIn
g
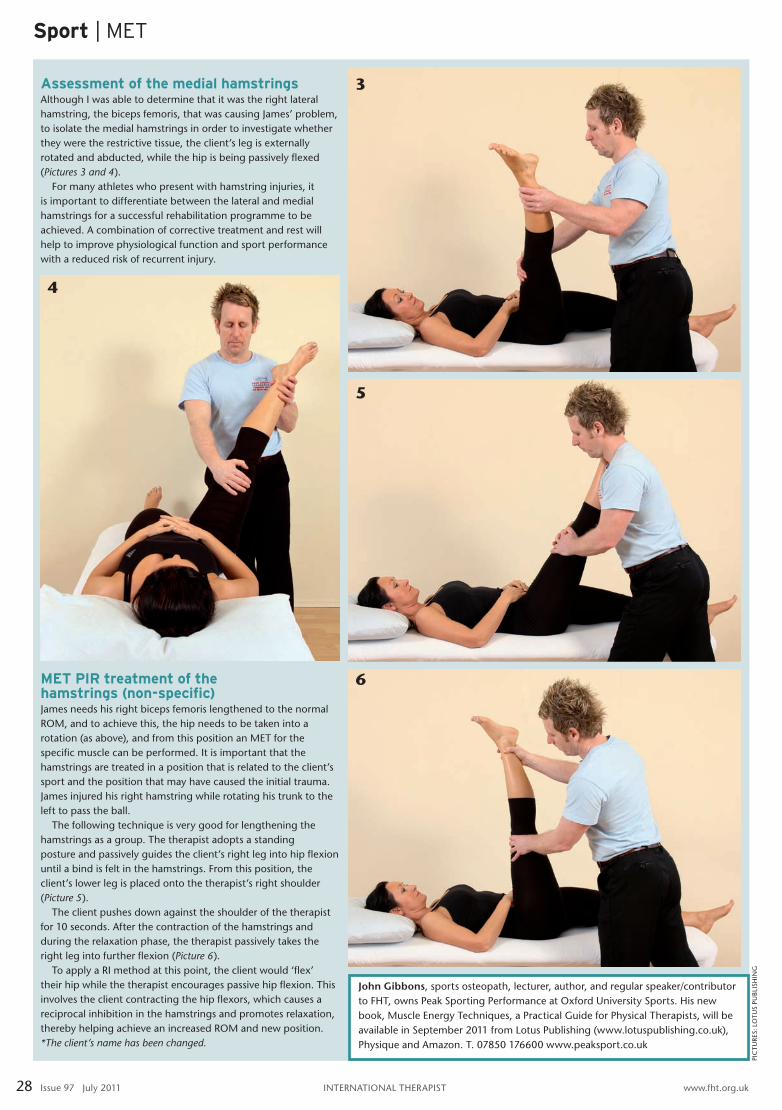
Assessment of the medial hamstringsalthough I was able to determine that it was the right lateral hamstring, the biceps femoris, that was causing James’ problem, to isolate the medial hamstrings in order to investigate whether they were the restrictive tissue, the client’s leg is externally rotated and abducted, while the hip is being passively flexed (Pictures 3 and 4).
For many athletes who present with hamstring injuries, it is important to differentiate between the lateral and medial hamstrings for a successful rehabilitation programme to be achieved. a combination of corrective treatment and rest will help to improve physiological function and sport performance with a reduced risk of recurrent injury.
John Gibbons, sports osteopath, lecturer, author, and regular speaker/contributor to Fht, owns peak sporting performance at oxford university sports. his new book, Muscle energy techniques, a practical guide for physical therapists, will be available in september 2011 from lotus publishing (www.lotuspublishing.co.uk), physique and amazon. t. 07850 176600 www.peaksport.co.uk
5
6
4
MET PIR treatment of the hamstrings (non-specific)James needs his right biceps femoris lengthened to the normal roM, and to achieve this, the hip needs to be taken into a rotation (as above), and from this position an Met for the specific muscle can be performed. It is important that the hamstrings are treated in a position that is related to the client’s sport and the position that may have caused the initial trauma. James injured his right hamstring while rotating his trunk to the left to pass the ball.
the following technique is very good for lengthening the hamstrings as a group. the therapist adopts a standing posture and passively guides the client’s right leg into hip flexion until a bind is felt in the hamstrings. From this position, the client’s lower leg is placed onto the therapist’s right shoulder (Picture 5).
the client pushes down against the shoulder of the therapist for 10 seconds. after the contraction of the hamstrings and during the relaxation phase, the therapist passively takes the right leg into further flexion (Picture 6).
to apply a rI method at this point, the client would ‘flex’ their hip while the therapist encourages passive hip flexion. this involves the client contracting the hip flexors, which causes a reciprocal inhibition in the hamstrings and promotes relaxation, thereby helping achieve an increased roM and new position.*The client’s name has been changed.
3