engineering the prevention of hospital acquired venous...
TRANSCRIPT

Christopher M. Masek, BSIE CSSBBVA Nebraska Western Iowa HealthcareSystem
Midwest Mountain Veterans EngineeringResource Center (VERC)
Engineering the Prevention of HospitalAcquired Venous Thromboembolism
Define Evaluate Design Implement Results Sustain Spread

Book Club
The Wisdom of Crowds. Surowiecki,J. New York: Anchor Books, 2005.
The Survivors Club. Sherwood, B.Grand Central Publishing 2010.
2

Objectives
What is Venous Thromboembolism(VTE)?
Lean Healthcare Implementation
Human Factors
Define Evaluate Design Implement Results Sustain Spread3

About the Presenter
BSIE University of Nebraska – Lincoln Dana Corporation Lucent/Avaya/Connectivity Solutions Mfg Goodyear Tire and Rubber Co./ Veyance
Inc. Veterans Affairs Nebraska Western Iowa
Healthcare System Midwest Mountain Veterans Engineering
Resource Center (VERC)
Define Evaluate Design Implement Results Sustain Spread4

AcknowledgementsVTE Team
Ann Polich, MD
Gale Etherton, MD
Jon Knezevich, PharmD
Peter A. Woodbridge, MD, MBA
Melissa Eggink
Pam Florea
Susan Hallbeck, PhD
Justin RousekDefine Evaluate Design Implement Results Sustain Spread
5

Veterans Affairs Nebraska WesternIowa Healthcare System
From 104 counties in Nebraska, westernIowa, portions of Kansas and Missouri
Total Veteran population: 167,000
FY08 Vested Users: 47,000
FY08 Outpatient Visits: 408,000
FY08 Inpatient Admits: 5,000
Define Evaluate Design Implement Results Sustain Spread6

Veterans Affairs Nebraska WesternIowa Healthcare System
Omaha, NE
In patient Care, Outpatient Care, ResidentialMental Health Programs, Research
Grand Island, NE
Outpatient Care, Community Living Center(nursing home), Residential Substance Abuse
Lincoln, NE
Large Community Based Outpatient Clinic(CBOC) providing Outpatient Care
Define Evaluate Design Implement Results Sustain Spread7
Veterans Affairs Nebraska WesternIowa Healthcare System
Community Based Outpatient Clinics(CBOCs)
North Platte, NE
Norfolk, NE
Holdrege, NE
Bellevue, NE
Shenandoah, IA
Define Evaluate Design Implement Results Sustain Spread8

Why is this important?
~44,000-98,000 Americans die eachyear from medical errors (IOM)
9Define Evaluate Design Implement Results Sustain Spread

10

Why?
“Medicine used to be simple, ineffectiveand relatively safe.
Now it is complex, effective anddangerous.”
11
Sir Cyril Chantler, former DeanGuy’s, King and St. Thomas’s Medicaland Dental School, Lancet 1999
Define Evaluate Design Implement Results Sustain Spread

Why?
“We are carrying the 19th century clinicaloffice into the 21st century world. It’s
time to retire it.”
Donald Berwick, MD
Institute for Healthcare Improvement
12Define Evaluate Design Implement Results Sustain Spread
VTE Background
#1 preventable hospital acquired death isdue to VTE
8 times more likely to acquire VTE whenhospitalized
VTE is a preventable problem which is notapproached uniformly across all patients
Define Evaluate Design Implement Results Sustain Spread13

What is VTE
Pulmonary embolism resulting fromdeep vein thrombosis (DVT) —collectively referred to as VTE — is themost common preventable cause ofhospital death. (Heit et al 2002,Tapson et al 2005,
Clagett et al 1995)
Define Evaluate Design Implement Results Sustain Spread14

What is VTE in plainlanguage
A blood clot that forms in the leg
The blood clot breaks free and movesthrough the bloodstream
The clot travels to the lung and blocks oneor more arteries in the lung
Needs prompt treatment
It is life threatening
Can be prevented
Define Evaluate Design Implement Results Sustain Spread15

16
Repenning QI Model *
* Repenning, N. and J. Sterman (2001). Nobody Ever Gets Credit for Fixing Defects that Didn't Happen:Creating and Sustaining Process Improvement, California Management Review, 43, 4: 64-88
ProcessReliability
Errosion inReliability
Investment inReliability
Define Evaluate Design Implement Results Sustain Spread

17
The “Work Harder” Loop
ProcessReliability
Errosion inReliability
Investment inReliability
ActualPerformance
PerformanceGap
DesiredPerformance
Time Spent onImprovement
+
+
-
+
Time SpentWorking
+
Pressure todo work
+
+
Work Harder
delay
Define Evaluate Design Implement Results Sustain Spread

18
The “Work Smarter” LoopProcess
ReliabilityErrosion inReliability
Investment inReliability
ActualPerformance
PerformanceGap
DesiredPerformance
Time Spent onImprovement
+
+
-
+
Time SpentWorking
+
Pressure todo work
+
+
Work Harder
Pressure toImprove
Capability+
+
Work Smarter
delay
Define Evaluate Design Implement Results Sustain Spread

Improvement Project
100 day Rapid Process ImprovementWorkshop (RPIW)
Lean Kaizen Event
Team focused
Highly scripted
Formal Charter
Education and Application of Lean tools
Define Evaluate Design Implement Results Sustain Spread19

Charter-Problem Statement
Currently patients are not assessed at admission or dailyfor VTE uniformly.
There is a section on the current Computer PhysicianOrder Entry (CPOE) system that is skipped over.
The occurrence of VTE/DVT is relatively low, but when itdoes occur, it can cause additional complications to thepatient.
This problem most affects patient length of stay, mortality.
A possible consequence of changes to this process mayincrease drug use/cost, increased staffing, adverse effectsfrom anticoagulants.
Define Evaluate Design Implement Results Sustain Spread20

Charter – Goal Statementand Scope
Goal
100% DVT VTE assessment onmedicine wards
Scope
Admitted Medicine patient, excludeSurgery patients
Define Evaluate Design Implement Results Sustain Spread21

Improvement Project-Mapping
What is the current state?
Define Evaluate Design Implement Results Sustain Spread22

Improvement Project-Voiceof the Customer (VOC)
Use SWOTModel to formatyour questions
Strengths
Weaknesses
Opportunities
Threats
Why do VOC?
Collection ofData
Engages nonteam membersin the process
Promotes Buy-Inof the efforts
Define Evaluate Design Implement Results Sustain Spread23

Improvement Project-Voiceof the Customer (VOC)
Analysis of VOC
Themes willemerge
Problems willsurface
VTE Prophylaxis Problems No Scorecard - objective
assessment (a way to know ifwe are doing it right)
No explanation as to noprophylaxis
Uncertain status Risk bleeding Orders continuity , done
(written), implemented Pumps / TED hose Sense of Autonomy Under utilization of CPRS CPRS non-mandatory
training CPRS representative not part
of rounding team No standardization
Define Evaluate Design Implement Results Sustain Spread24

Positive Deviants
Who gets itright?
Follow upquestion andanswer with PDindividuals.
Define Evaluate Design Implement Results Sustain Spread25
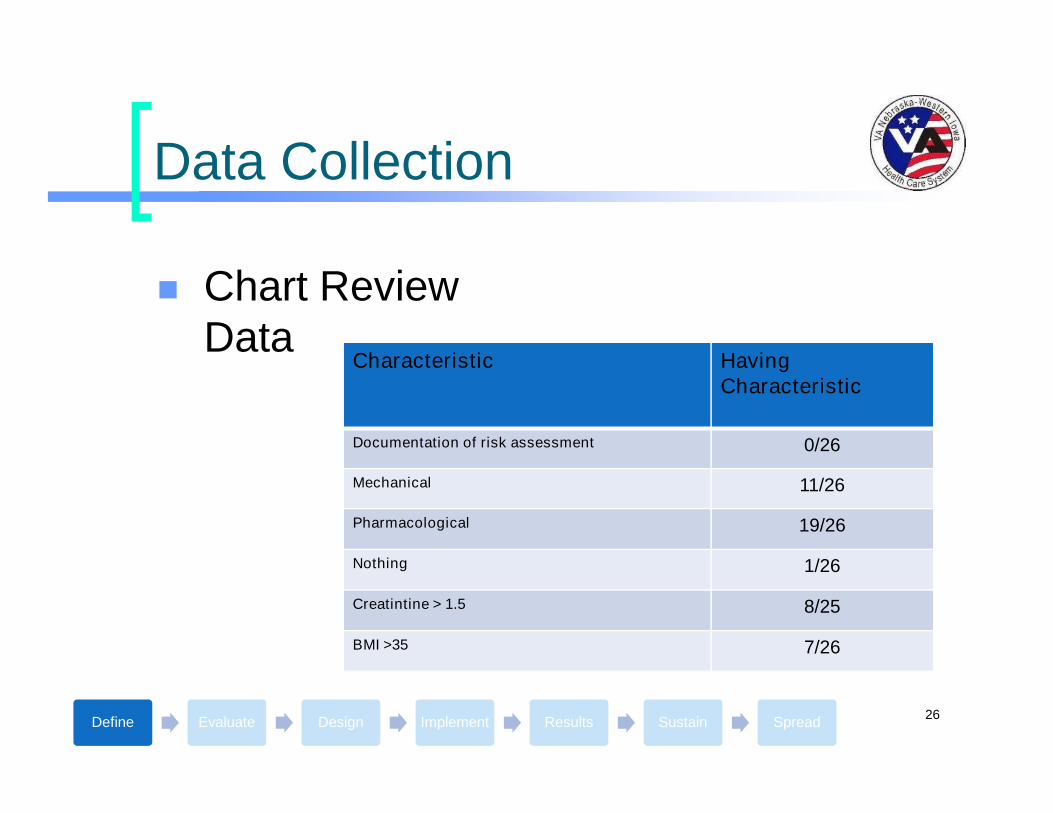
Data Collection
Chart ReviewData
Characteristic HavingCharacteristic
Documentation of risk assessment 0/26
Mechanical 11/26
Pharmacological 19/26
Nothing 1/26
Creatintine > 1.5 8/25
BMI >35 7/26
Define Evaluate Design Implement Results Sustain Spread26

Why do all of this?
Defining theProblem
Quantifiableinformation
Does not haveto be statisticallysound
Everyone cansee the wholepicture
Ensureimprovementefforts arefocused on thecorrect areas
Define Evaluate Design Implement Results Sustain Spread27

Kapowies and Brainstorming
Stars are barriers
Flowers are opportunities
Brainstorm ideas to overcome the barriers
Define Evaluate Design Implement Results Sustain Spread28

Affinity Diagram
Generation ofideas
Group intoThemes
Define Evaluate Design Implement Results Sustain Spread29
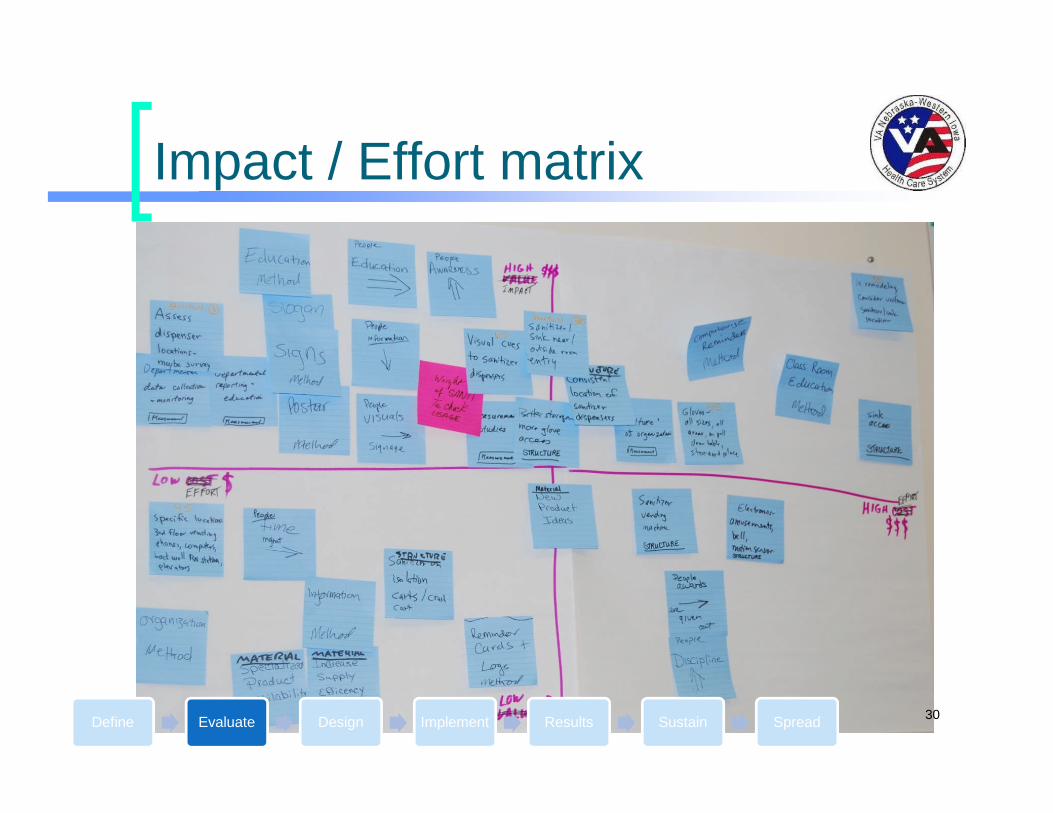
Impact / Effort matrix
Define Evaluate Design Implement Results Sustain Spread30

Design and Try
Rapid cycle changePDSA
Plan
Do
Study
Act
Test hypothesis
Adapt, Adopt,Abandon
Define Evaluate Design Implement Results Sustain Spread31
Examples of PDSA Cycles
FAQ on drugs used for DVT treatment.
Develop tool for QM Nurse to reportback data.
Graph in ward to display VTEperformance.
Education of new residents on usingtools.
Define Evaluate Design Implement Results Sustain Spread32

Aha Moments!
Documentation of assessment mustbe a forced function.
Documentation of assessment mustbe automatically recorded.
The assessment must beuncomplicated.
Define Evaluate Design Implement Results Sustain Spread33

A different approachIntention to treat instead of risk stratification
Why? Universal risk to patients entering the hospital
Literature suggests physician under utilizationof chemo prophylaxis
Literature suggests mechanical devices areminimally effective
Patient population
Risk stratification is complex
You will be treated unless…
Define Evaluate Design Implement Results Sustain Spread34

Intention to treat method
Based oncontraindications
Give the physiciana reason not toprovide chemoprophylaxis
Suggestappropriatepharmacologicalagent to treatwith.
Reduce thenumber ofdecisions
Define Evaluate Design Implement Results Sustain Spread35
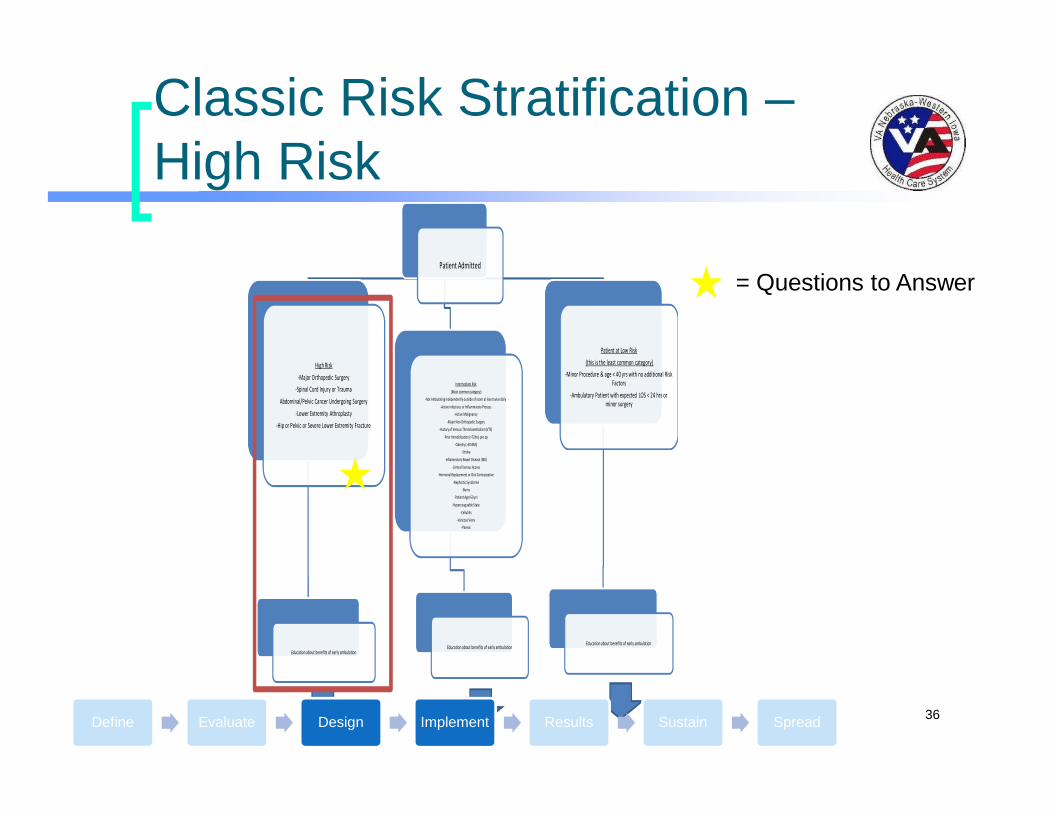
Classic Risk Stratification –High Risk
36
Patient Admitted
High Risk
-Major Orthopedic Surgery
-Spinal Cord Injury or Trauma
Abdominal/Pelvic Cancer Undergoing Surgery
-Lower Extremity Athroplasty
-Hip or Pelvic or Severe Lower Extremity Fracture
Education about benefits of early ambulation
Intermediate Risk
(Most common category)
-Not Ambulating independently outside of room at least twice daily
-Active infectious or Inflammatory Process
-Active Malignancy
-Major Non Orthopedic Surgery
-History of Venous Thromboembolism (VTE)
-Prior Immoblization (>72hrs) pre op
-Obesity (>30 BMI)
-Stroke
-Inflammatory Bowel Disease (IBD)
-Central Venous Access
-Hormonal Replacement or Oral Contraceptive
-Nephrotic Syndrome
-Burns
-Patient Age>50 yrs
-Hypercoaguable State
-Cellulitis
-Varicose Veins
-Paresis
Education about benefits of early ambulation
Patient at Low Risk
(this is the least common category)
-Minor Procedure & age < 40 yrs with no additional RiskFactors
-Ambulatory Patient with expected LOS < 24 hrs orminor surgery
Education about benefits of early ambulation
= Questions to Answer
Define Evaluate Design Implement Results Sustain Spread

Classic Risk Stratification –High Risk
=
37
VTE Prophylaxis:HIGH RISK Cont.
Contraindications to VTE Prophylaxis for Patients at HighRisk
Absolute
-Acute Hemorrhage from wounds ordrains or lesions
-Intracranial hemorrhage within the prior24 hrs
-Heparin induced Thrombocytopenia(HIT)
-Severe trauma to head or spinal cord orextremities
-Neuraxial anesthesia/spinal blockwithin12 hours of initiation or
discontinuation of anticoagulation
-Patient on Warfarin or Heparin orEnoxaparin for other indications
Relative
-GI or GU hemorrhage within the past 6months
-Coagulopathy (INR>1.5)
-Intracranial Lesion/Neoplasm
-Severe Thrombocytopenia (Plt < 50k)
-Neuraxial Anesthesia/Spinal Block
-Intracranial Hemorrhage within the past 6months
No Contraindications to Prophylaxis
= Questions to Answer
Define Evaluate Design Implement Results Sustain Spread

Classic Risk Stratification –High Risk
38
VTE Prophylaxis:HIGH RISK Cont.
ABSOLUTE CONTRAINDICATION
NonpharmacologicalTreatment
-Sequential CompressionDevices (SCDs)
-Antiembolic Stockings(TEDs)
RELATIVE CONTRAINDICATION
Pharmacologic Benefit Outweighs Risk
-Enoxaparin 40 mg SQ daily
-Enoxaparin 30 mg SQ daily
(CrCl < 30 mL/min but not onhemodialysis)
-Enoxaparin 30 mg SQ Q 12 hrs
(Total Knee Arthroplasty)
-Fondaparinux 2.5 mg SQ daily
(CrCl < 30 mL/min)
-Warfarin
-Heparin 5000 units SQ Q 8 hrs
AND
Nonpharmacologic Treatment
-Sequential Compression Devices (SCDs)
-Antiembolic Stockings (TEDS)
Pharmacologic Risk Outweighs Benefit
-Sequential Compression Devices (SCDs)
-Antiembolic Stockings (TEDS)
NO CONTRAINDICATIONS
Pharmacologic Treatment (MUST USE)
-Enoxaparin 40 mg SQ daily
-Enoxaparin 30 mg SQ daily
(CrCl < 30 mL/min but not onhemodialysis)
-Enoxaparin 30 mg SQ Q 12 hrs
(Total Knee Arthoplasty)
-Fondaparinux 2.5 mg SQ daily
(CrCl < 30 mL/min)
-Warfarin
-Heparin 5000 units SQ Q 8 hrs
AND
Nonpharmacological Treatment
-Sequential Compression Devices (SCDs)
-Antiembolic Stockings (TEDS)
= Questions to Answer
Define Evaluate Design Implement Results Sustain Spread

Classic Risk Stratification –Intermediate Risk
39
Patient Admitted
High Risk
-Major Orthopedic Surgery
-Spinal Cord Injury or Trauma
Abdominal/Pelvic Cancer Undergoing Surgery
-Lower Extremity Athroplasty
-Hip or Pelvic or Severe Lower Extremity Fracture
Education about benefits of early ambulation
Intermediate Risk
(Most common category)
-Not Ambulating independently outside of room at least twice daily
-Active infectious or Inflammatory Process
-Active Malignancy
-Major Non Orthopedic Surgery
-History of Venous Thromboembolism (VTE)
-Prior Immoblization (>72hrs) pre op
-Obesity (>30 BMI)
-Stroke
-Inflammatory Bowel Disease (IBD)
-Central Venous Access
-Hormonal Replacement or Oral Contraceptive
-Nephrotic Syndrome
-Burns
-Patient Age>50 yrs
-Hypercoaguable State
-Cellulitis
-Varicose Veins
-Paresis
Education about benefits of early ambulation
Patient at Low Risk
(this is the least common category)
-Minor Procedure & age < 40 yrs with no additional RiskFactors
-Ambulatory Patient with expected LOS < 24 hrs orminor surgery
Education about benefits of early ambulation
Define Evaluate Design Implement Results Sustain Spread

Classic Risk Stratification –Intermediate Risk
40
VTE Prophylaxis:INTERMEDIATE RISK Cont.
Contraindications to VTE Prophylaxis for Patients atIntermediate Risk
Absolute
-Acute Hemorrhage from wounds ordrains or lesions
-Intracranial hemorrhage within the prior24 hrs
-Heparin induced Thrombocytopenia(HIT)
-Severe trauma to head or spinal cord orextremities
-Neuraxial anesthesia/spinal blockwithin12 hours of initiation or
discontinuation of anticoagulation
-Patient on Warfarin or Heparin orEnoxaparin for other indications
Relative
-GI or GU hemorrhage within the past 6months
-Coagulopathy (INR>1.5)
-Intracranial Lesion/Neoplasm
-Severe Thrombocytopenia (Plt < 50k)
-Neuraxial Anesthesia/Spinal Block
-Intracranial Hemorrhage within the past 6months
No Contraindications to Prophylaxis
Define Evaluate Design Implement Results Sustain Spread

Classic Risk Stratification –Intermediate Risk
41
VTE Prophylaxis:INTERMEDIATE RISK Cont.
ABSOLUTE CONTRAINDICATION
NonpharmacologicalTreatment
-Sequential CompressionDevices (SCDs)
-Antiembolic Stockings(TEDs)
RELATIVE CONTRAINDICATION
Pharmacologic Benefits Outweigh Risk
-Enoxaparin 40 mg SQ daily
-Enoxaparin 30 mg SQ daily
(CrCl < 30 mL/min but not onhemodialysis)
-Enoxaparin 30 mg SQ Q 12 hrs
(Total Knee Arthroplasty)
-Fondaparinux 2.5 mg SQ daily
(CrCl < 30 mL/min)
-Warfarin
-Heparin 5000 units SQ Q 8 hrs
OPTIONAL
Nonpharmacologic Treatment
-Sequential Compression Devices (SCDs)
-Antiembolic Stockings (TEDS)
Pharmacologic Risk Outweighs Benefit
-Sequential Compression Devices (SCDs)
-Antiembolic Stockings (TEDS)
NO CONTRAINDICATIONS
Pharmacologic Treatment (MUST USE)
-Enoxaparin 40 mg SQ daily
-Enoxaparin 30 mg SQ daily
(CrCl < 30 mL/min but not onhemodialysis)
-Fondaparinux 2.5 mg SQ daily
(CrCl < 30 mL/min but not onhemodialysis)
-Heparin 5000 units SQ Q 8 hrs
-Heparin 5000 units SQ Q 12 hrs
(if underweight or age > 75)
OPTIONAL
Nonpharmacological Treatment
-Sequential Compression Devices (SCDs)
-Antiembolic Stockings (TEDS)
Define Evaluate Design Implement Results Sustain Spread

Classic Risk Stratification –Low Risk
42
Patient Admitted
High Risk
-Major Orthopedic Surgery
-Spinal Cord Injury or Trauma
Abdominal/Pelvic Cancer Undergoing Surgery
-Lower Extremity Athroplasty
-Hip or Pelvic or Severe Lower Extremity Fracture
Education about benefits of early ambulation
Intermediate Risk
(Most common category)
-Not Ambulating independently outside of room at least twice daily
-Active infectious or Inflammatory Process
-Active Malignancy
-Major Non Orthopedic Surgery
-History of Venous Thromboembolism (VTE)
-Prior Immoblization (>72hrs) pre op
-Obesity (>30 BMI)
-Stroke
-Inflammatory Bowel Disease (IBD)
-Central Venous Access
-Hormonal Replacement or Oral Contraceptive
-Nephrotic Syndrome
-Burns
-Patient Age>50 yrs
-Hypercoaguable State
-Cellulitis
-Varicose Veins
-Paresis
Education about benefits of early ambulation
Patient at Low Risk
(this is the least common category)
-Minor Procedure & age < 40 yrs with no additional RiskFactors
-Ambulatory Patient with expected LOS < 24 hrs orminor surgery
Education about benefits of early ambulation
Define Evaluate Design Implement Results Sustain Spread

Classic Risk Stratification –Low Risk
43
VTE Prophylaxis:LOW RISK Cont.
OOB AD LIB
Define Evaluate Design Implement Results Sustain Spread

Intention to treat
44
Patient Admitted
Assess the Patient for the following conditions that would be CI forpharmacologic VTE therapy
-Uncontrolled hypertension (i.e. hypertensive crisis)
-Active, uncontrollable bleeding
-Spinal Tap within 12 hours or epidural catheter placement
-Comfort care patient
-Severe head trauma
-Previous history of HIT or hypersensitivity to UFH or LMWH
-Patient is < 40 yrs of age and hospital length of stay is predicted to beless than 48 hours
-Other (blank box to fill in)
Conditions Present
Select the non-pharmacologicalmeasures that you would like the
patient to receive while hospitalized
(multiple selections available)
- SCDS
-TED Hose
-Ambulation
None of theconditions present
Does the patient:
-Weigh less than 50 kg
OR
-Have a CrCl < 30mL/min
NO
Select a pharmacological agent that you would like the patientto receive for DVT prophylaxis :
(Ambulation is not sufficient by itself)
-Fondaparinux (Arixtra) 2.5 mg SQ daily
(Half-life: 17 - 21 hrs)
-Enoxaparin (Lovenox) 40 mg SQ dailiy
(Half-life: 6 – 8 hrs)
-Unfractionated Heparin (UFH) 5,000 units SQ Q 8 hrs
(Not preferred with malignancy)
AND/OR
Select the non-pharmacological measures that you would likethe patient to receive while hospitalized in addition to the
pharmacological agent already prescribed :
(Multiple sections available)
-SCDS
-TED Hose
-Ambulation
YES
Select a pharmacologicalagent that you would like thepatient to receive for DVT prophylaxis:
(Ambulation is not sufficient by itself)
-Enoxaparin (Lovenox) 30 mg SQ daily
-Unfractionated Heparin (UFH) 5,000 units SQ Q 12 hrs
AND/OR
Select the non-pharmacological measures that you wouldlike the patient to receive while hospitalized in addition to
the pharmacological agent already prescribed :
(Multiple sections available)
-SCDS
-TED Hose
-Ambulation
= Questions to Answer
Define Evaluate Design Implement Results Sustain Spread
Human factors - Usability
Improve performance
Safer system
More efficient system
Test system with various scenarios
Test the system in a sandbox to preventunintended harm to patients
Evaluate design for desired outcomes
Can we make it even better?
Define Evaluate Design Implement Results Sustain Spread45
Usability Study
Test “Intention to Treat” methodagainst “Risk stratification”
Do we get the right answers?
Is one faster than the other?
Are some physicians better than others?
Define Evaluate Design Implement Results Sustain Spread46

Test knowledge - “Intent to treat”method, “Risk stratification” method
Use 6 differentscenarios
10 randomizedruns
Use online toolto collect data
Evaluatedecision of 1,2,3year residentswhile in clinic
Define Evaluate Design Implement Results Sustain Spread47

Online Tool - LimeSurvey
Open source
Ability to branchlogic – the nextquestion isdetermined bypreviousanswers
Modified tocollect timestamp of eachselection
Ability to importexportmethod/logic
Define Evaluate Design Implement Results Sustain Spread48

Do we get the right answer?
Scenario
Correct Outcome
Intention to TreatMethod
RiskStratificationMethod
A 95% 68%
B 93% 78%
C 90% 66%
D 85% 66%
E 83% 71%
F 56% 29%
Define Evaluate Design Implement Results Sustain Spread49

Is it faster?
64%
100%
Intention to Treat Risk Stratification
Perc
en
t
Method
Average Time to Complete
Define Evaluate Design Implement Results Sustain Spread50

Correct Answers byResident Year
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Year 1 Year 2 Year 3
Intention to Treat
Risk Stratification
Define Evaluate Design Implement Results Sustain Spread51
Going forward
Integration into EMR
Forcing functions
Lead you to the right answer
Automated data collection
Reporting
Define Evaluate Design Implement Results Sustain Spread52
References
Heit JA, O’Fallon WM, Petterson TM, et al. Relative impact of risk factors for deep vein thrombosis and pulmonaryembolism, Arch Intern Med, 2002;162:1245-1248.
Tapson VF, Hyers TM, Waldo AL, et al. Antithrombotic therapy practices in US hospitals in an era of practice guidelines,Arch Intern Med, 2005;165:1458-1464.
Clagett GP, Anderson FA, Heit JA, et al. Prevention of venous thromboembolism, Chest, 1995;108:312-334.
53