english: dr. ralph hawkins
TRANSCRIPT
LYME DISEASE FROM THE PERSPECTIVE OF A GENERAL
PHYSICIAN IN ACTIVE CLINICAL PRACTICE.
Ralph G Hawkins MD LLM FRCPC Framework Conference on Lyme Disease
Ottawa, Ontario; May 16, 2016

Faculty/Presenter Disclosure • Faculty: Ralph George Hawkins MD LLM FRCPC
• Relationships with commercial interests:
– Grants/Research Support: I have none to declare. – Speakers Bureau/Honoraria: Merck Canada, Janssen Canada – Consulting Fees: Advisory Boards for: Merck Canada, Eli Lilly Canada,
Boehringer Ingelheim Canada, Janssen Canada, NovoNordisk Canada
– Other: CMA Code of Ethics: “Recognize a responsibility to give generally held opinions of the profession when interpreting scientific knowledge to the public; when presenting an opinion that is contrary to the generally held opinion of the profession, so indicate.”

Disclosure of Commercial Support • This program has received financial support from [organization name] in
the form of [describe support here – e.g. an educational grant]. • This program has received in-kind support from [organization name] in
the form of [describe support here – e.g. logistical support].
• Potential for conflict(s) of interest:
– [Speaker/Faculty name] has received [payment/funding, etc.] from [organization supporting this program AND/OR organization whose product(s) are being discussed in this program].
– [Supporting organization name] [developed/licenses/distributes/benefits from the sale of, etc.] a product that will be discussed in this program: [insert generic and brand name here].

Mitigating Potential Bias
• [Explain how potential sources of bias identified in slides 1 and 2 have been mitigated].
• Refer to “Quick Tips” document

Case History: T.S. • Athletic, healthy mother
of 3 young sons. Married. • Unrecognized arthropod
bite below scapula on April 19, 2015 in residential urban Calgary Alberta
• After a few days developed a rash, larger than a “loonie”, expanding in nature
• Did not seek immediate medical attention

Case History: T.S. • May 27, 2015: Admitted
to hospital with – Persistent headache – Dizziness – Blurred vision – Unexplained collapses
• June 6: Still in hospital, no
diagnosis. New symptoms included: – Generalized arthralgias – Diplopia – Paraesthesias of limbs

Case History: T.S.
• Provincial Laboratory Lyme Screening -- C6 test is negative (drawn 7 weeks post arthropod bite)
• Patient advised by ID consultant that Lyme disease has been “ruled out” by serology.

2-tier testing as recommended by CDC

Here are 100 people who have early Lyme Borreliosis with Erythema Migrans

C6 testing is 64% sensitive in Acute erythema migrans

2-tier testing is acute phase serology, which overall has just 45% sensitivity

Father of Modern Medicine
• Sir William Osler, MD 1849-1919
“Listen to the patient, he is telling you the diagnosis.”

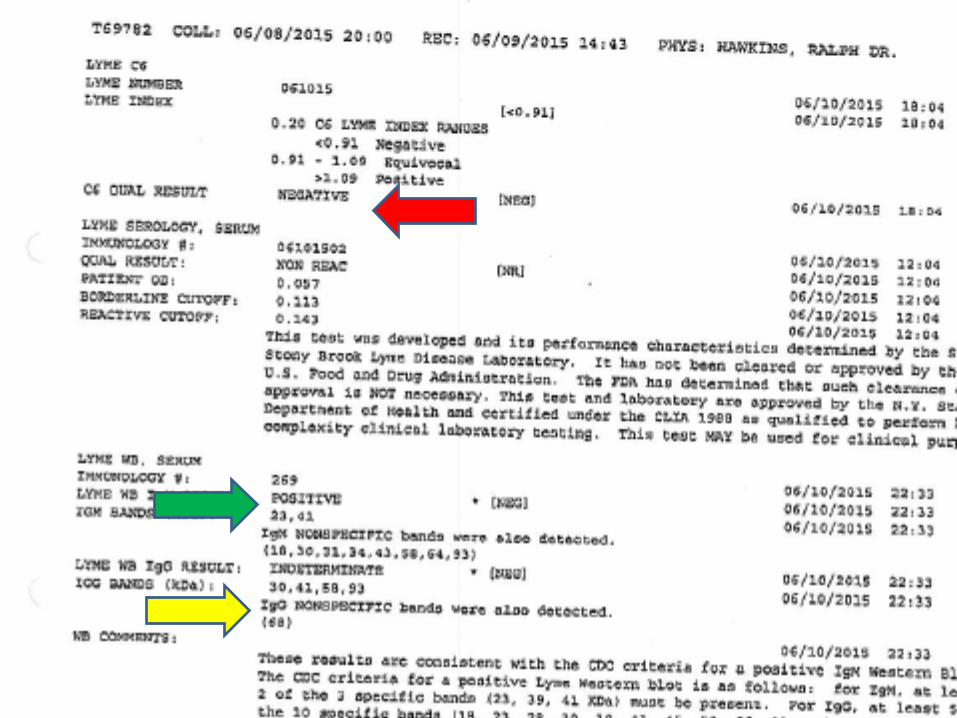
Case History: T.S. • Oral Doxycycline initiated • Serology sent to SUNY Lyme
Laboratory at Stony Brook Medical School, at patient’s expense
• C6 negative, just as it was in Canada
• Western Blot IgM read to be positive (10 bands seen including 2 CDC bands)
• Western Blot IgG read to be indeterminate (5 bands seen including 4 CDC bands)

Stated rationale that Lyme Disease had been “ruled out”:
1. Alberta is a non-endemic region of Canada for Borrelia burgdorferi infected Ixodes ticks
2. The patient did not specifically identify a tick as the source of the bite
3. The rash described was not typical for Erythema migrans, was neither diagnosed by a medical practitioner nor photographed by the patient.
4. The duration of tick attachment described is too short for transmission of Borrelia burgdorferi

Stated rationale that Lyme Disease had been “ruled out”:
5. After the elapsed timeframe (7 weeks), her C6 serology
tested by the Provincial Lab ought to have been positive. It was negative. Because the C6 is negative, Western Blots should not have been obtained.
6. The reported IgM Western Blot is positive by CDC criteria, but since it was analyzed on a specimen obtained more than 4 weeks post bite, it is declared to be a “false-positive”.
7. The reported IgG Western blot is negative according to criteria developed by the CDC in 1995.
8. Symptom persistence following antibiotics goes against diagnosis of early disseminated Lyme disease

1. “Alberta is a non-endemic region of Canada for Borrelia burgdorferi infected Ixodes ticks”
• Response:
• Passive surveillance studies show that infected Ixodes
ticks are consistently identified in distribution much wider than the defined geographic locations of endemic ticks in Canada.
• It is estimated that between 10 to 30 Billion birds migrate to Canada annually. Bird capture studies identify a high proportion of songbirds importing millions of Ixodes ticks

Bird surveillance locations in Canada

• Because songbirds widely disperse infected ticks across Canada, people can contract Lyme disease without exposure to an endemic area
• American Robin, Common Yellowthroat, Golden-Crown Sparrow, Song Sparrow, Swainson’s Thrush are all competent carriers
• Greater genetic diversity of B. burgdorferi is more apparent in Western Canada

A noteworthy migratory songbird
Swainson’s Thrush Catharus ustulatus
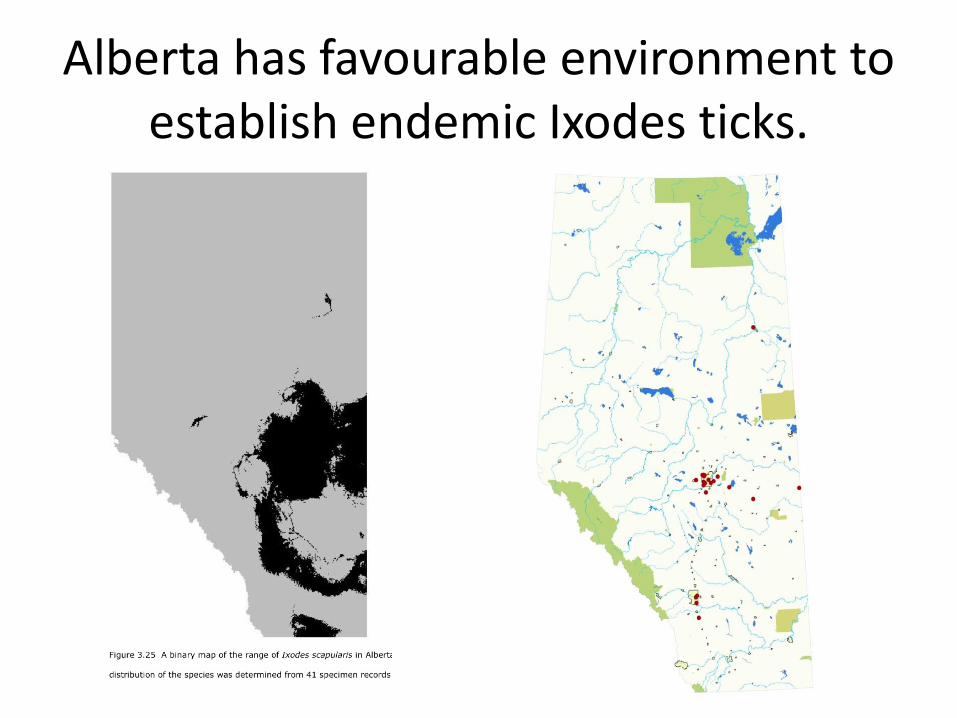
Alberta has favourable environment to establish endemic Ixodes ticks.

Canine surveillance has found B burgdorferi in Alberta

Alberta Health-- Tick surveillance 2013
Surveillance in Alberta in 2013 shows 20% of Ixodes ticks infected with Borrelia burgdorferi
2. “The patient did not specifically identify a tick as the source of the bite” • Response:
• Estimates of tick-bite recollection in those
with laboratory confirmed Lyme borreliosis range between 20 to 50%.

3. “The rash described was not typical of Erythema Migrans rash and was not
corroborated by a physician” • Response: • In a Lyme-endemic area, 106 primary care doctors were
surveyed – 80% correctly identified “classic” erythema migrans rash with
central clearing – 64% correctly identified “atypical” erythema migrans rash which is
described as homogenous without central clearing • In those with laboratory confirmed diagnosis of Lyme disease,
2/3 of EM rashes were atypical and homogenous • Considering the above together, clinical diagnosis will only be
70% sensitive to identify Erythema migrans • In Canada, only 58% of clinically recognized EM will be
managed correctly with prompt antibiotic prescription

Here are 100 people who have early Lyme Borreliosis with Erythema Migrans

Erythema migrans will be recognized in 70 of the 100 people presenting

58% of 70 people, or 41 patients of the original 100, will be treated promptly

Canadian Public Health Laboratory Network Approach for diagnosis

Laboratory Reporting of C6 Results

4. “The duration of tick attachment was too brief for transmission of infection”
• Response: • Studies on infection transmission time are
necessarily done in observed circumstances using unfed ticks to observe attachment time and subsequent disease development
• However, in “the wild”, partially fed ticks may latch upon a new host (human) with unstudied consequences on the time for disease transmission

Study of hard tick feeding and disease transmission

Unfed Previously fed Seroconversion after 12 hrs Seroconversion after 10 min

16 of 18 partially-fed ticks (89%), having reattached to new hosts for only 24 hours, transmitted infection

5. “After 7 weeks, her C6 test ought to indicate infection if present.”
Response: C6 assay is, at best, 75% sensitive in settings such as presented by T.S.

“Negative results (either first or second step) should not be used to exclude Lyme Disease”
Immunetics C6 Product monograph

5. “Since the initial C6 was negative, Western Blot studies should never
have been done”. Response: 2011 Laboratory Criteria for Diagnosis - CDC For the purposes of surveillance, the definition of a
qualified laboratory assay is • Positive Culture for B. Burgdorferi, OR • Two-tier testing interpreted using established criteria,
where: » Positive IgM is sufficient only when < 30 days from symptom
onset » Positive IgG is sufficient at any point during the illness
• Single-tier IgG immunoblot seropositivity using established criteria
• CSF antibody positive for B. burgdorferi by EIA or IFA when the titer is higher than in serum.

6. “Because the IgM Western Blot was analyzed more than 4 weeks after the
bite, it is “falsely-positive”.” Response:
• “IgM values were highest a median of six weeks after disease onset.”

IgM in Lyme Borreliosis persists and can emerge as a late feature
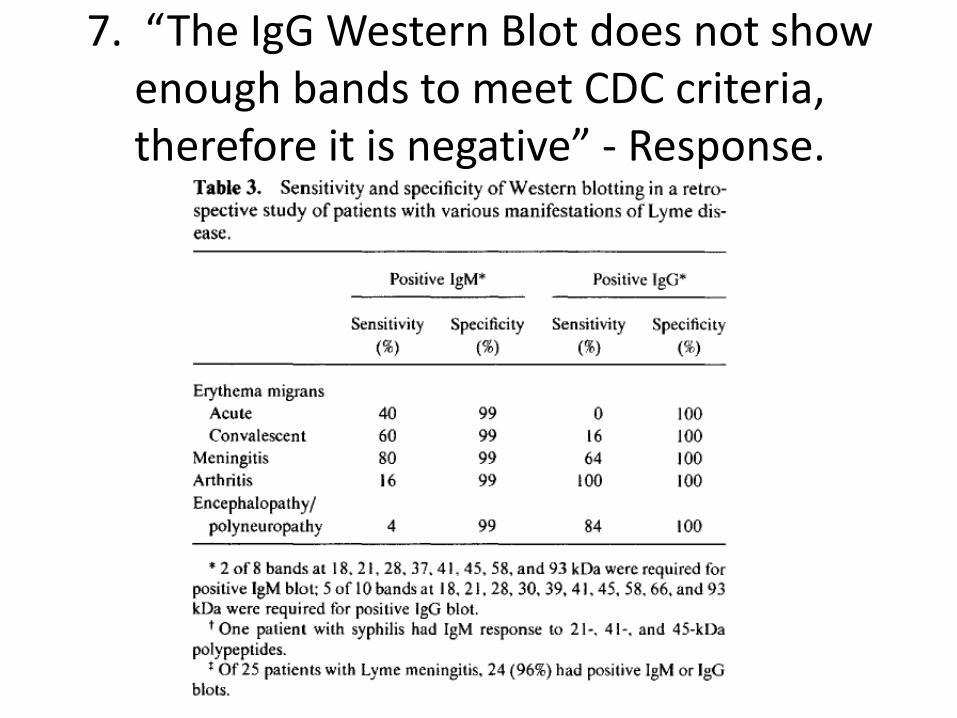
7. “The IgG Western Blot does not show enough bands to meet CDC criteria, therefore it is negative” - Response.

31, 34, 37 and 74 kDa bands

Alternative interpretation criteria have been published historically

Zoller’s 1990 Western blot criteria

How the National Laboratory Presents An Obstacle to Making A Diagnosis

Non-reporting of band patterns is intentional
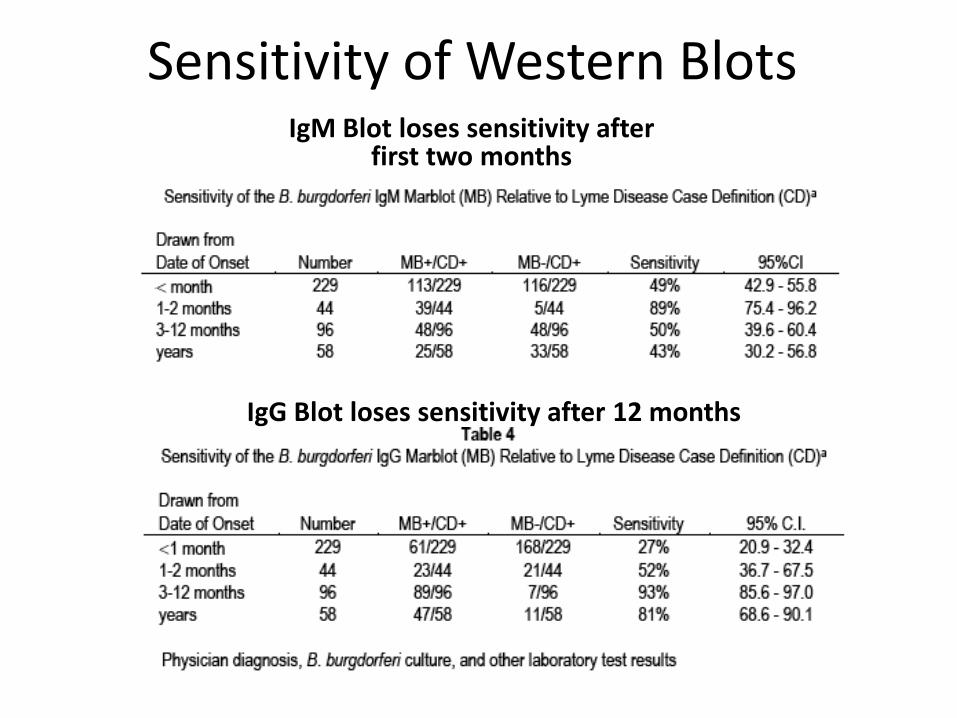
Sensitivity of Western Blots IgM Blot loses sensitivity after
first two months
IgG Blot loses sensitivity after 12 months

Here are 100 people who have early Lyme Borreliosis with Erythema Migrans

C6 testing is 64% sensitive in Acute erythema migrans

Only 33 people with early erythema migrans will have positive IgG 2-tier

CAN CURRENT DIAGNOSTIC TESTS BE UTILIZED MORE SENSITIVELY?

C6 testing is 64% sensitive in Acute erythema migrans

If IgG WB is run on the C6 negative people, 19 more patients are correctly found
Tests run parallel rather than in series: Calculated Sensitivity 83%; Specificity 97.5%
100 people with late Lyme Borreliosis of > 1 year duration

C6 testing is 98% sensitive in late Lyme Borreliosis >1 year duration

2-tier testing is limited to <80% sensitivity in late Lyme Borreliosis

8. Does symptom persistence following antibiotics goes against the diagnosis of
early disseminated Lyme Borreliosis? One in seven treated patients will have prolonged disability

Clinical Diagnoses of Lyme Borreliosis Expanding the acceptable criteria
Definite
Probable
Plausible

Core Standards for Evidence in Canadian Law
• Proof beyond a reasonable doubt • Proof on a preponderance of the evidence; or
balance of probabilities (>50%) “More likely than not.”
• Evidence raising a reasonable doubt. (In science or statistics, we typically set the limit for chance findings at 5%; or set confidence limits at 95%, meaning “19 times out of 20”).
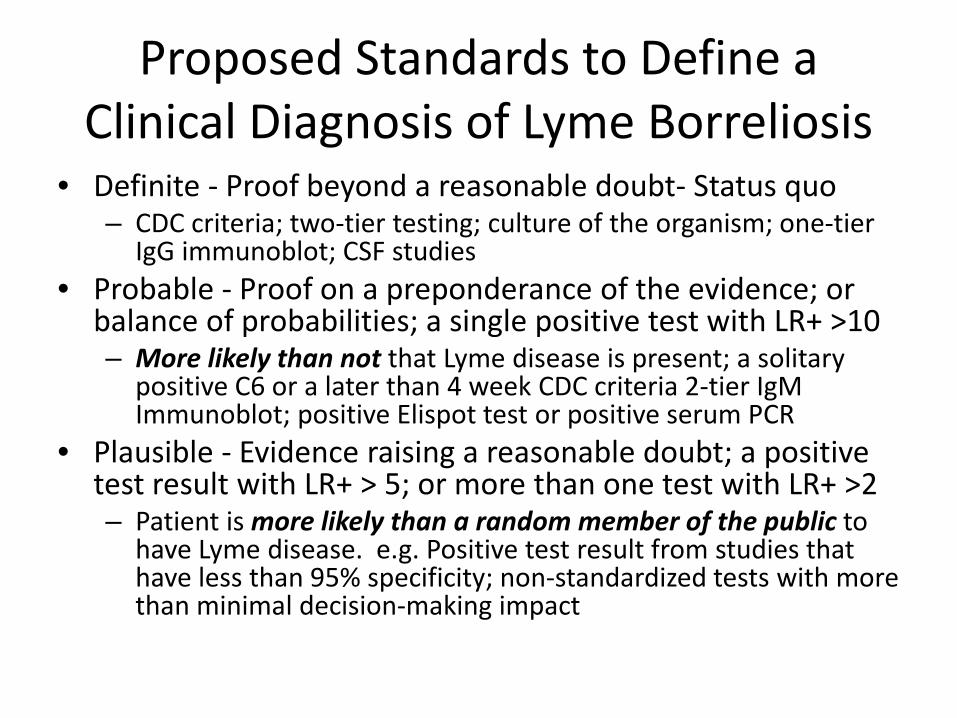
Proposed Standards to Define a Clinical Diagnosis of Lyme Borreliosis
• Definite - Proof beyond a reasonable doubt- Status quo – CDC criteria; two-tier testing; culture of the organism; one-tier
IgG immunoblot; CSF studies • Probable - Proof on a preponderance of the evidence; or
balance of probabilities; a single positive test with LR+ >10 – More likely than not that Lyme disease is present; a solitary
positive C6 or a later than 4 week CDC criteria 2-tier IgM Immunoblot; positive Elispot test or positive serum PCR
• Plausible - Evidence raising a reasonable doubt; a positive test result with LR+ > 5; or more than one test with LR+ >2 – Patient is more likely than a random member of the public to
have Lyme disease. e.g. Positive test result from studies that have less than 95% specificity; non-standardized tests with more than minimal decision-making impact

Points to Consider: • If songbirds visit your yard in spring, you could conceivably have a
Lyme disease “micro-environment” until next freeze • All Canadians live in the migratory pathway of common songbirds
creating risk for adventitious tick exposure everywhere • 2-tier testing run in series is demonstrably insensitive early or late • Western blot band results are intentionally not reported in Canada,
precluding the opportunity to utilize published alternative interpretation criteria with high specificities
• Single-tier Western Blot, one of the CDC case surveillance criteria, is unattainable in Canada due to intentionally restrictive practices
• Borrelia heterogeneity is well described, which may affect disease phenotype and test sensitivity
• Borrelia burgdorferi spirochetes likely persist post-treatment in cystic or granular phenotypes, even if few, which may in turn lengthen immunologic disease duration due to persistent antigen expression.
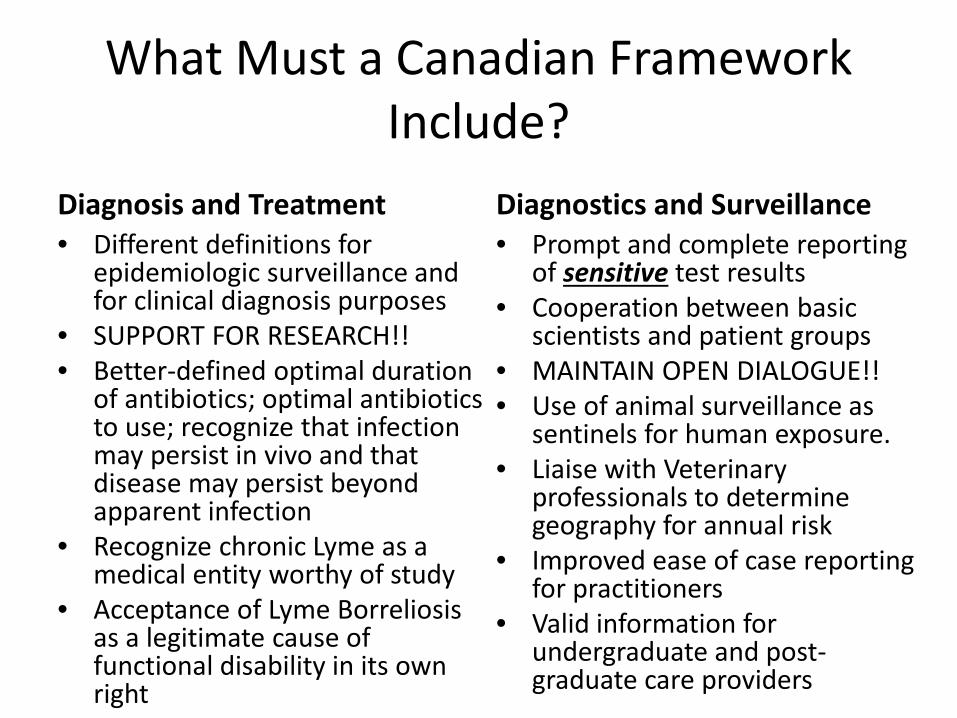
What Must a Canadian Framework Include?
Diagnosis and Treatment • Different definitions for
epidemiologic surveillance and for clinical diagnosis purposes
• SUPPORT FOR RESEARCH!! • Better-defined optimal duration
of antibiotics; optimal antibiotics to use; recognize that infection may persist in vivo and that disease may persist beyond apparent infection
• Recognize chronic Lyme as a medical entity worthy of study
• Acceptance of Lyme Borreliosis as a legitimate cause of functional disability in its own right
Diagnostics and Surveillance • Prompt and complete reporting
of sensitive test results • Cooperation between basic
scientists and patient groups • MAINTAIN OPEN DIALOGUE!! • Use of animal surveillance as
sentinels for human exposure. • Liaise with Veterinary
professionals to determine geography for annual risk
• Improved ease of case reporting for practitioners
• Valid information for undergraduate and post-graduate care providers
Let’s listen to the patient(s), They are telling us the diagnosis.
• T.S. now is in clinical
remission after treatment for disseminated Lyme Borreliosis
• T.S. meets the clinical diagnosis of Lyme Borreliosis by “probable” criteria, as discussed herein.

END OF FRAMEWORK PLENARY PRESENTATION

SUPPLEMENTARY SLIDES

Dr. Ralph Hawkins – Disclosure



Global distribution of Lyme carrying Ixodes ticks

Northern Wheatears traverse European Lyme territory en route here

B garinii in North America


Provincial Health surveillance has found B burgdorferi in Alberta

B. burgdorferi positive ticks collected within the city of Calgary

Response: But, at 1-2 mos only 78% sensitivity
The C6 assay will be falsely negative in 22% of cases of true Lyme disease in the 1-2 month period post-infection.
5. “After 7 weeks, her C6 test ought to indicate infection if present”.

4-lab comparison sensitivity

4-lab comparison specificity

Likelihood ratio
• The formula for calculating the likelihood ratio is: LR = probability of an individual with the
condition having the test result probability of an individual without the condition having the test result
• Thus, the positive likelihood ratio is: LR + = probability of an individual with the
condition having a positive test probability of an individual without the condition having a positive test

Likelihood Ratio Impact on Decision-Making LR Interpretation
> 10 Large and often conclusive increase in the likelihood of disease
5 - 10 Moderate increase in the likelihood of disease
2 - 5 Small increase in the likelihood of disease
1 - 2 Minimal increase in the likelihood of disease
1 No change in the likelihood of disease
0.5 - 1.0 Minimal decrease in the likelihood of disease
0.2 - 0.5 Small decrease in the likelihood of disease
0.1 - 0.2 Moderate decrease in the likelihood of disease
< 0.1 Large and often conclusive decrease in the likelihood of disease
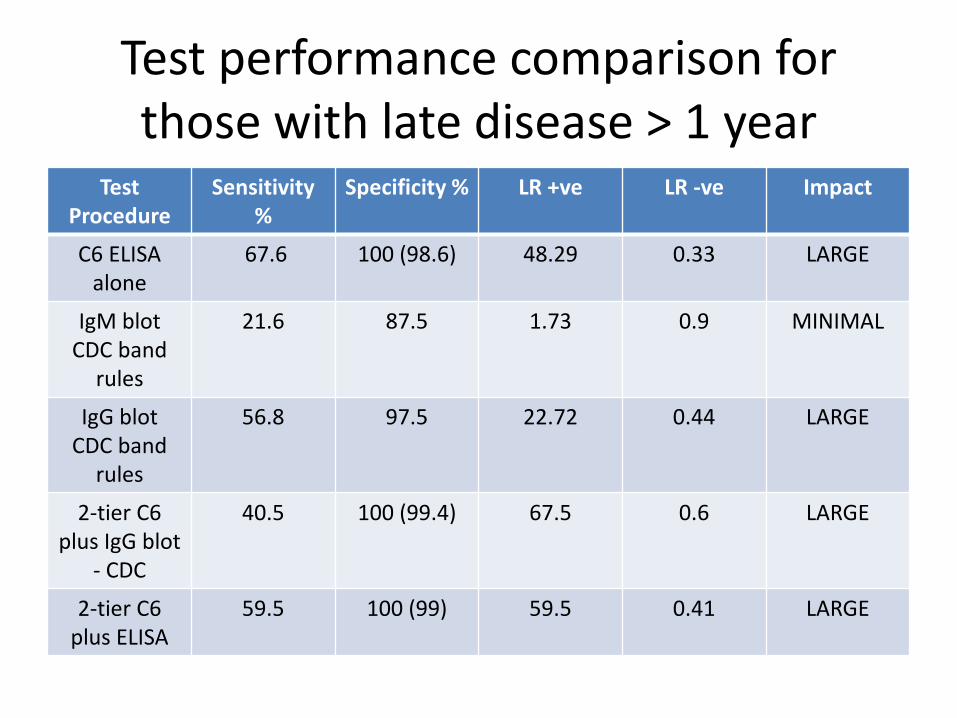
Test performance comparison for those with late disease > 1 year
Test Procedure
Sensitivity %
Specificity % LR +ve LR -ve Impact
C6 ELISA alone
67.6 100 (98.6) 48.29 0.33 LARGE
IgM blot CDC band
rules
21.6 87.5 1.73 0.9 MINIMAL
IgG blot CDC band
rules
56.8 97.5 22.72 0.44 LARGE
2-tier C6 plus IgG blot
- CDC
40.5 100 (99.4) 67.5 0.6 LARGE
2-tier C6 plus ELISA
59.5 100 (99) 59.5 0.41 LARGE

Other alternative tests that patients voluntarily will access
Test Procedure
Sensitivity %
Specificity % LR +ve LR -ve Impact
Lab B IgG Blot CDC
rules
48.6 92.5 6.48 0.56 MODERATE
IgG blot Lab B rules
70.3 72.5 2.56 0.41 SMALL
Lab B IgM Blot CDC
rules
43.2 80 2.16 0.71 SMALL
IgM blot Lab B rules
62.2 62.5 1.66 0.6 MINIMAL
Urinary nanotrap
41 87.5 3.28 0.67 SMALL
Elispot 84 92 10.5 0.17 LARGE
Serum PCR 6 99.9 60 0.94 LARGE

A neuro-immune model for CFS/ME
“(H)istologic derangements suggest immunologic damage in response to persistence of the spirochete, however few in number. “– Dulay P and Steere A, 1988

Should this disease have a better name?
• “Lyme disease” originates from an illness that was predominantly arthritic in nature, and does not identify the borrelia spirochete as the etiologic agent
• “Post-Treatment Lyme Disease Syndrome” implies that adequate treatment has been applied and that the disorder is not related to the incident illness; and implies a non-infectious pathophysiology
Consider renaming Lyme Borreliosis with prolonged symptoms: BEND
Borrelia-Exposure Neurocognitive Disorder
• This nomenclature identifies Borrelia as the causative agent, and is neutral with respect to persistence or chronicity of infection.
• The name describes the predominant feature leading to persistent disability, namely a Neurocognitive disorder
• The World Health Organization has categorized Chronic Fatigue Syndrome as a neurologic disorder since 1969; accordingly the identification of persistent Borreliosis with chronic fatigue or cognitive impairment as a parallel neurologic disorder is sensible by extension
• Chronic Borreliosis is not Chronic Fatigue Syndrome, but both conditions share symptoms with overlapping phenotypes.