enhancing children's satisfaction with antibiotic therapy: a taste study of several antibiotic...
TRANSCRIPT

CURRENT THERAPEUTIC RESEARCH~ VOL. 61, No. 8, AUGUST 2000
Enhancing Children’s Satisfaction with Antibiotic Therapy: A Taste Study of Several
Antibiotic Suspensions*
Richard H. Schwartz
Vienna Pediatric Associates, Vienna, Virginia
ABSTRACT
Objective: This randomized, single-blind, paired-comparison crossover study was conducted (1) to compare the taste of cefurox- ime axetil suspension (125 mg/5 mL or 250 mg/5 mL) with that of 3 other antibiotic suspensions (cefpodoxime proxetil 100 mg/5 mL, clarithromycin 250 mg/5 mL, and amoxicillin 250 mg/5 mL); and (2) to determine the effect of a chocolate syrup chaser on the palat- ability of the cefirroxime axetil suspension.
Methods: Two hundred children aged 3 to 8 years received cef- uroxime axetil and 1 of 4 other treatments in counterbalanced or- der. They were asked to indicate which medicine tasted better and rated immediate taste (directly after dosing) and aftertaste (60 seconds after dosing) using a 5-point facial hedonic scale (from 1 = really bad to 5 = really good).
Results: Cefuroxime axetil suspension was chosen as the better- tasting medicine less often than amoxicillin suspension and at least as often as cefpodoxime proxetil and clarithromycin suspensions. Cefuroxime axetil with a chocolate syrup chaser was chosen as the better-tasting medicine over cefuroxime axetil alone by 73% of the children. The mean immediate-taste and aftertaste scores for cefur- oxime axetil were similar to those for cefpodoxime proxetil and clarithromycin, and significantly lower than those for amoxicillin (P c 0.05, Cochran-Mantel-Haenszel test). The mean immediate- taste score for cefuroxime axetil suspension followed by a chocolate syrup chaser was similar to that for cefuroxime axetil alone, but the mean aftertaste score for cefuroxime axetil with a chocolate syrup chaser (3.61) was significantly higher than that for cefuroxime ax- etil alone (2.70; P c 0.05, Cochran-Mantel-Haenszel test) and simi- lar to that for amoxicillin suspension (3.93). Older children (aged 6-8 years) tended to score all medications less favorably than did younger children (aged 3-5 years). The children tended to score the first medicine tried more favorably than they did the second.
* This material was presented in part as a poster at the 36th Annual Meeting of the Infectious Diseases Society of America, November 12-15, 1998, in Denver, Colorado.
Address correspondence to: Richard H. Schwartz, MD, FAAP, Vienna Pediatric Associates, 410 Maple Avenue West #5, Vienna, VA 22180. Accepted for publication June 6, 2000. Printed in the USA. Reproduction in whole or part is not permitted.
570 0011.393)3/00/$19.00

R.H. SCHWARTZ
Conclusions: Children rated the eefuroxime axetil suspension as not tasting as good as amoxicillin suspension but at least as good as suspensions of cefpodoxime proxetil and clarithromycin. With the chocolate syrup chaser, the aftertaste of cefuroxime axetil was rated as palatable as that of amoxicillin and more palatable than that of cefpodoxime proxetil or clarithromycin.
Key words: cefuroxime axetil, pediatrics, antibiotic suspension, taste, palatability. (Curr Ther Res Clin Exp. 2000;61:570-581)
INTRODUCTION
Three of 4 visits to a pediatric or primary care office result in the writing of 2 1 prescription,’ most likely for an antibiotic to treat a respiratory tract infection such as otitis media or pharyngitis.2 In choosing the most appro- priate antibiotic therapy for children, pediatricians and primary care prac- titioners consider a drug’s spectrum of activity, efficacy, and tolerability, and such compliance-influencing features as palatability, appearance, dos- ing frequency, and duration of therapy.3
Cefuroxime axetil fulfills many of the criteria that physicians consider in choosing a pediatric antimicrobial agent. It has a broad spectrum of activity and is stable in the presence of beta-lactamase, characteristics important in the context of recent increases in the incidence of beta- lactamase-producing strains of Haemophilus influenzae and Moraxella ca- tarrhalis and multidrug-resistant Streptococcus pneumoniae.4 Because of its efficacy against multidrug-resistant S pneumoniae in otitis media, ce- furoxime axetil is 1 of 3 medications (and the only oral cephalosporin) recommended by the Centers for Disease Control and Prevention’s Drug- Resistant Streptococcus pneumoniae Therapeutic Working Group in cases of clinical failure after amoxicillin therapy for acute otitis media. It is also recommended as an appropriate choice for initial therapy of acute otitis media when antibiotics have been taken during the previous month.5 Cef- uroxime axetil suspension is as effective as amoxicillin syrup,’ amoxicillin/ clavulanate suspension,7-11 and clarithromycin suspension12 and more ef- fective than cefaclor suspension” in the treatment of acute bacterial otitis media.
Cefuroxime axetil is generally better tolerated than the macrolides and amoxicillin/clavulanate, which are associated with a higher incidence of gastrointestinal side effects such as nausea and diarrhea than is cefu- roxime axeti1.3s,10,” Wh ereas cefuroxime axetil suspension is adminis- tered twice daily, some other suspensions require dosing 3 times daily, which may hinder compliance with the therapeutic regimen.13’14
Although it meets the criteria of broad-spectrum efficacy, tolerability, and infrequent dosing, cefuroxime axetil suspension is less palatable than some other antibiotic suspensions. For example, in a randomized, investi-
571

CURRENT THERAPEUTIC RESEARCH@
gator-blinded study,‘r more patients rated the taste of cefuroxime axetil as unacceptable (14%) than they did the taste of either cefaclor (0%) or amoxi- cillin/clavulanate (3%).
The present randomized, single-blind, paired-comparison, crossover study was conducted to obtain additional information on how children perceive the taste and appearance of cefuroxime axetil suspension and to explore a strategy for enhancing its taste. Children in the study compared the taste and appearance of cefuroxime axetil suspension with those of amoxicillin, cefpodoxime proxetil, and clarithromycin, and rated the effects of a chocolate syrup chaser on the taste of cefuroxime axetil suspension.
PATIENTS AND METHODS
Patients
Children aged 3 to 8 years who presented to a pediatric clinic with an upper respiratory tract infection such as acute otitis media, streptococcal pharyngitis, or acute sinusitis were eligible for participation in the study. Children aged <3 years were excluded because they could not be expected to understand the study instructions. Enrollment was stratified by age so that approximately equal numbers of 3- to 5-year-olds and 6- to 8-year-olds were enrolled. Children were excluded if they had a body weight ~12 kg; if they had a condition (other than respiratory tract infection) that might interfere with taste; if they had a serious chronic medical condition, in- cluding gastrointestinal, hematologic, renal, or hepatic disease; and if they were allergic to antibiotics or chocolate.
The protocol for this randomized, single-blind, paired-comparison crossover study was approved by an institutional review board for the study site. Written, informed consent was obtained from parents or legal guardians, as was assent from children aged ~5 years, for participation in the study.
Studg Procedures
Children meeting the eligibility criteria were randomly assigned to 1 of 4 groups to receive cefuroxime axetil suspension (125 mg/ 5 mL for the first 100 patients and 250 mg/5 mL for the next 100 patients) and 1 other antibiotic suspension: cefuroxime axetil (125 mg/5 mL or 250 mg/5 mL) with a chocolate syrup chaser; cefpodoxime proxetil (100 mg/ 5 mL); clarithromycin (250 mg/5 mL); or amoxicillin (250 mg/5 mL). On the basis of clinical experience, amoxicillin has been characterized as having good palatability; it was therefore selected as a positive control with which to compare the palatability of cefuroxime axetil and 2 other antibiotic suspensions.3
572

R.H. SCHWARTZ
The children were informed about the test procedure and told that there were no right or wrong answers. They were then administered in counterbalanced order 2.5 mL of 2 suspensions and were asked to rate the immediate taste (directly after dosing) and the aftertaste (60 seconds after dosing) of each medicine using a 5point facial hedonic scale (from 1 = really bad to 5 = really good). The children receiving cefuroxime ax- etil with a chocolate syrup chaser were administered the same concentra- tion of the antibiotic as for the cefuroxime axetil suspension, which was followed immediately by an equal volume (2.5 mL) of chocolate syrup. The rationale for the chaser was based on the ability of thick chocolate syrup to mask aftertaste but not immediate taste. The 2.5 mL of chocolate syrup was not expected to influence the bioavailability of cefuroxime axetil. Ad- ministration of medicines was separated by a 2- to 3-minute washout pe- riod during which the children cleansed their palates with soda crackers and water. After they had rated the second medicine, the children chose which of the 2 medicines tasted better. They also stated which color they preferred, based on inspection of the residual suspension in the medicine cup.
Two trained pediatric nurse-interviewers asked parents standard multiple-choice questions about (1) their children’s reactions to new medi- cines; (2) their children’s antibiotic likes and dislikes before study entry; and (3) methods used to encourage children to take disliked antibiotics.
Statistical Analysis
Because the taste-score data were not normally distributed, nonpara- metric Cochran-Mantel-Haenszel tests were used to compare mean taste scores between each pair of treatments. These analyses were adjusted by covariates for period tie, treatment order), age, and dose (of cefuroxime axetil).
The taste and color-preference data and parents’ responses to the in- terview questions were summarized using descriptive statistics (mean per- centage of respondents in a given category and SEs).
RESULTS
Two hundred patients (112 between 3 and 5 years old and 88 between 6 and 8 years old) were enrolled in the study. Forty-eight percent of pa- tients were female. Demographic characteristics did not differ between groups (Table I).
Taste Scores
Mean immediate-taste scores for cefuroxime axetil suspension (with- out the chocolate syrup chaser) were significantly lower than those for
573
CURRENT THERAPEUTIC RESEARCH~
Table I. Demographic characteristics.
Cefpodoxime Proxetil (II = 50)
Cefuroxime Axetil with Chocolate
Total
Kc?” 27 (48) 29(52) 1:;
AwcgnOy W) 112
6-8 y z [ii{ ;si [El 2: [:;I so’ [@371 88 Body weight (lb),
mean + SD 47.7 5 11.7 46.8 f 11.4 48.5 f 16.3 48.3 + 14.3 NA
NA = not applicable
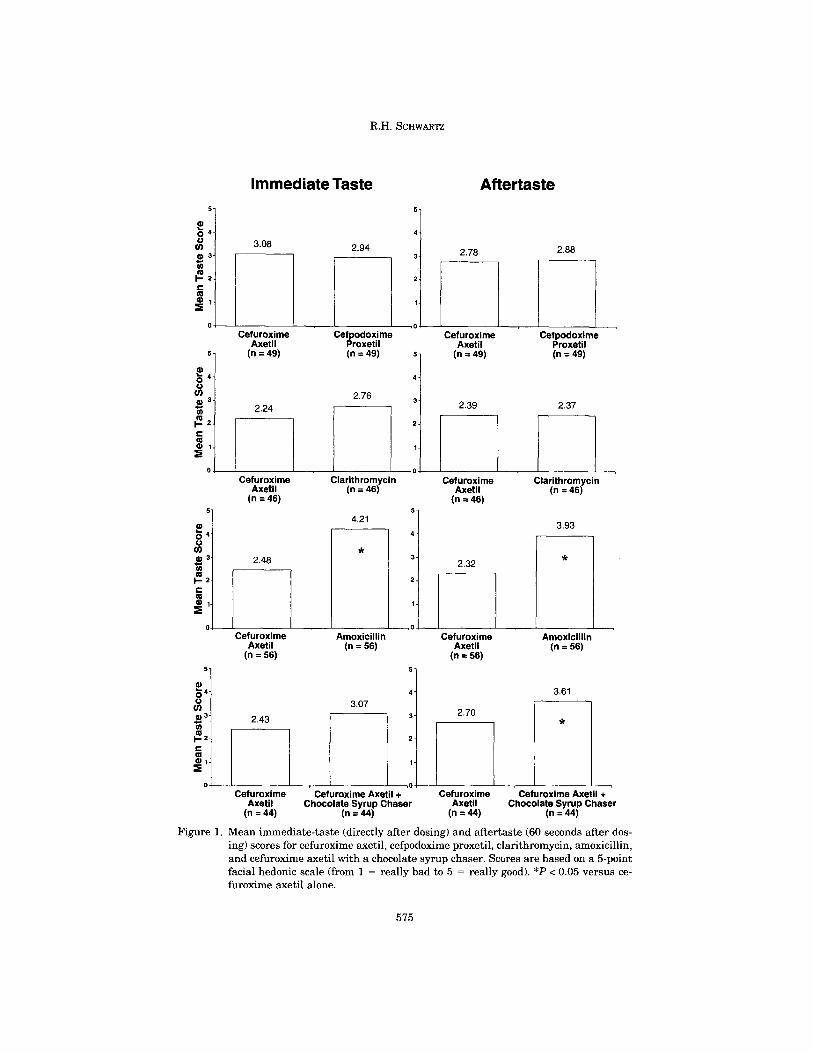
amoxicillin suspension (P < 0.05) and similar to those for the cefpodoxime proxetil and clarithromycin suspensions (Figure 1). The mean immediate- taste score for cefuroxime axetil followed by a chocolate syrup chaser was also similar to that for cefuroxime axetil alone.
Mean aftertaste scores for cefuroxime axetil suspension were sig- nificantly lower than those for amoxicillin (P < 0.05) and similar to those for the cefpodoxime proxetil and clarithromycin suspensions (Figure 1). The mean aftertaste score for cefuroxime axetil followed by a chocolate syrup chaser was significantly higher than that for cefuroxime axetil alone (P < 0.05) and similar to that for amoxicillin.
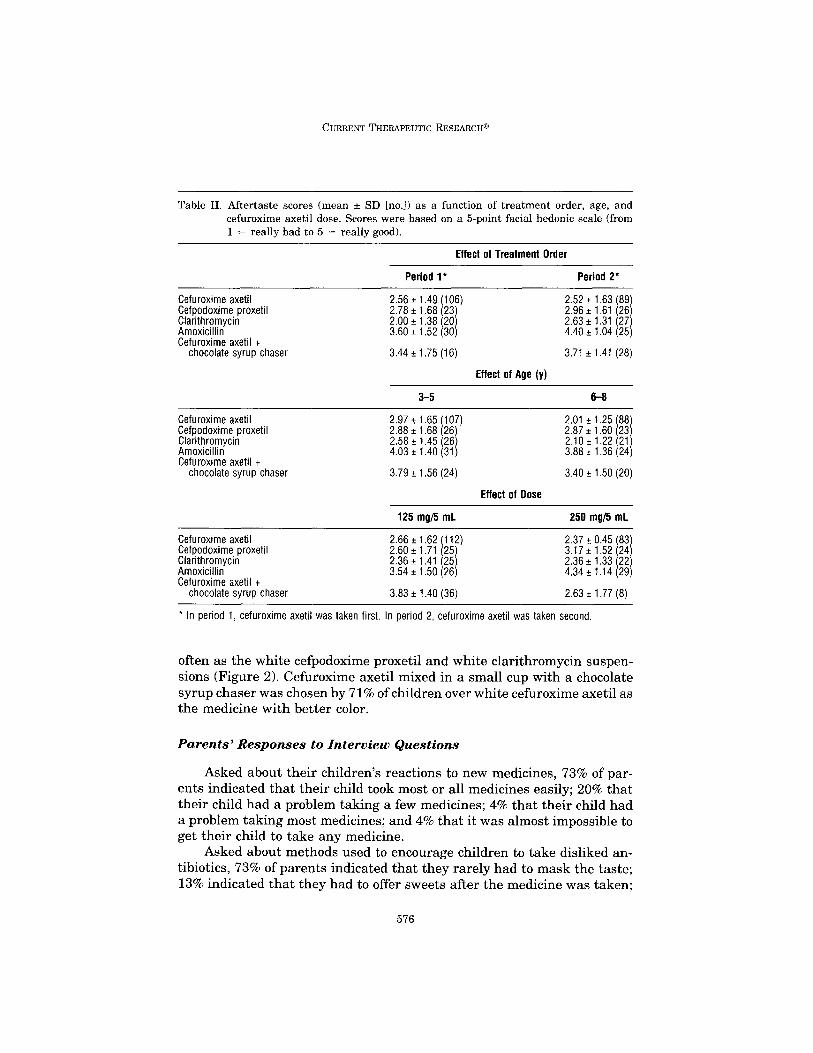
For both the immediate-taste and aftertaste scores, children tended to rate the first medicine tried more favorably than they did the second one (Table II). In addition, older children (aged 6-8 years) tended to rate all medications less favorably than did younger children (aged 3-5 years). Finally, children who received 250 mg/5 mL of cefuroxime axetil rated it less favorably and comparators more favorably than did children who re- ceived 125 mg/5 mL of cefuroxime axetil suspension, an effect applying to both cefuroxime axetil alone and cefuroxime axetil followed by a chocolate syrup chaser.
Taste and Color Preferences
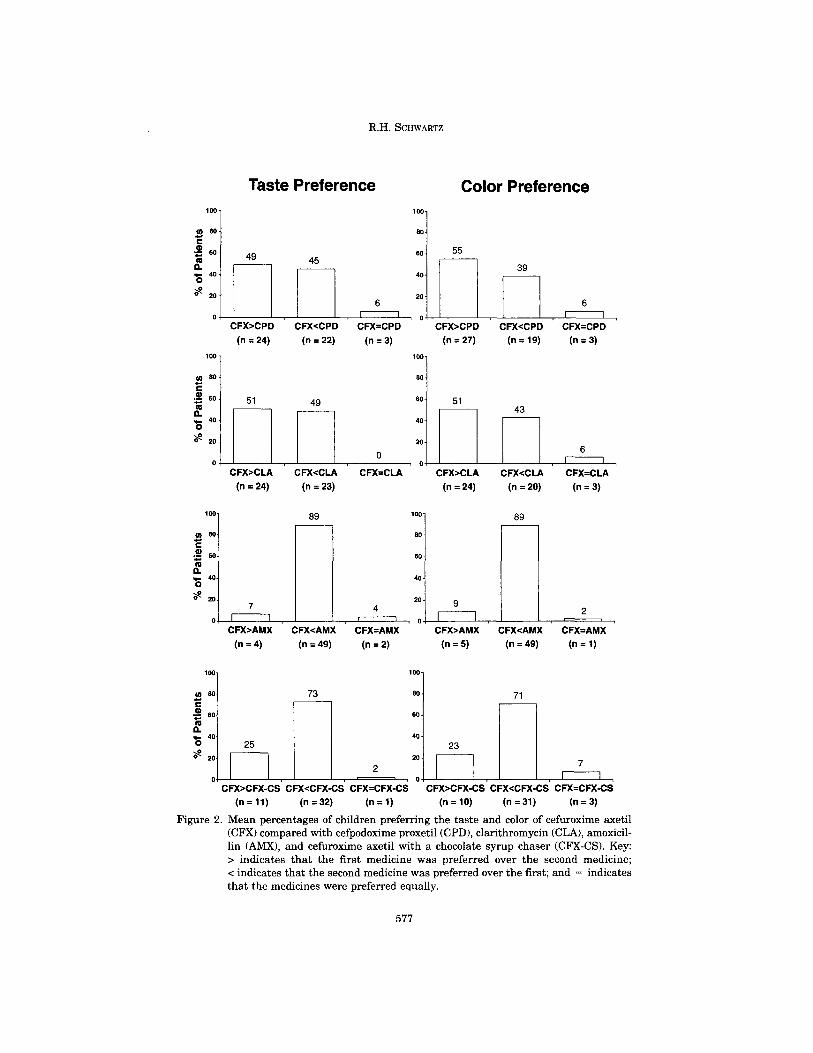
Cefuroxime axetil suspension was chosen as the better-tasting medi- cine less often than the amoxicillin suspension and at least as often as the cefpodoxime proxetil and clarithromycin suspensions (Figure 2). Cefurox- ime axetil with a chocolate syrup chaser was chosen by 73% of children as the better-tasting medicine compared with cefuroxime axetil alone.
White cefuroxime axetil suspension was chosen less often as the medi- cine with better color than the pink amoxicillin suspension and at least as
574
R.H. %XWARTZ
Immediate Taste Aftertaste
3.08 2.94 2.88
K Cefuroxime Cefpodoxime
Axetil Proxetil (n = 49) (n = 49)
2.76
Cefuroxime Cefpodoxime Axetil Proxetil
(n = 49) (n = 49) 5 4 3 2 1 70 1
2.39 2.37
-a 2.24
l-i Cefuroxime
Axetil (n = 46)
I Cef;;w;;me
(n = 46)
Clarithromycin (n ~46)
Clarithromycin (n =46)
4.21 3.93
*
Amoxicillin (n=56)
3.61
Cefuroxime Amoxicillin Cefuroxime Axetil
(n = 56) Axetil
(n = 56) (n = 56)
3.07 * 1 2.70
L 1"
l-.-L-L
2
1
n o- Cefuroxime
Axetil (n =44)
2.43
Cefuroxime Axetil + .- Chocolate Syrup Chaser
(n = 44)
Cefuroxime Cefuroxime Axetil + Axetil
(n=44) Chocolate Syrup Chaser
(n=44)
Figure 1. Mean immediate-taste (directly after dosing) and aftertaste (60 seconds after dos- ing) scores for cefuroxime axetil, cefpodoxime proxetil, clarithromycin, amoxicillin, and cefuroxime axetil with a chocolate syrup chaser. Scores are based on a &point facial hedonic scale (from 1 = really bad to 5 = really good). *P < 0.05 versus ce- furoxime axetil alone.
575
CURRENT THERAPEUTIC RESEARCH@
Table II. Aftertaste scores (mean f SD [no.]) as a function of treatment order, age, and cefuroxime axetil dose. Scores were based on a 5-point facial hedonic scale (from 1 = really bad to 5 = really good).
Effect of Treatment Order
Cefuroxime axetil Cefpodoxime proxetil Clarithromycin Amoxicillin Cefuroxime axetil -t
chocolate syrup chaser
Period l*
2.56 f 1.49 2.78 + 1.68 2.00 t 1.38
1 106) 23 i 20
3.60 f 1.52 (30)
3.44_+1.75(16)
Period 2*
2.52 t 1.63 1.61
(89) 2.96 k (26) 2.63 t 1.31 (27) 4.40 f 1.04 (25)
3.71 f 1.41 (28)
Effect of Age (y)
3-5 6-8
Cefuroxime axetil Cefpodoxime proxetil Clarithromycin Amoxicillin Cefuroxime axetil +
chocolate chaser syrup
2.97 i 1.65 (107) 2.01 t 1.25 (88 2.88 t 1.68 2.87 f 1.60 (26) (23 2.58 e 1.45 2.10 f 1.22 (26) 4.03 * 1.40 3.88 + 1.36
(21) (31) (24)
3.79 f 1.56 (24) 3.40 f 1.50 (20)
Effect of Dose
125 mg/5 mL 250 mgi5 mL
Cefuroxime axetil Cefpodoxime proxetil Clarithromycin Amoxicillin Cefuroxime axetil +
chocolate syrup chaser
2.66~1.62 112) 2.60 2 1.71 2.36 1.41
I 25) 2.37 + 0.45 (83) 3.17 f 1.52
t (25) (24)
2.36 i 1.33 3.54 f 1.50 (26)
(22) 4.34 f 1.14 (29)
3.83 f 1.40 (36) 2.63 f 1.77 (8)
l In period 1, cefuroxime axetil was taken first. In period 2, cefuroxime axetil was taken second
often as the white cefpodoxime proxetil and white clarithromycin suspen- sions (Figure 2). Cefuroxime axetil mixed in a small cup with a chocolate syrup chaser was chosen by 71% of children over white cefuroxime axetil as the medicine with better color.
Parents’ Responses to Interview Questions
Asked about their children’s reactions to new medicines, 73% of par- ents indicated that their child took most or all medicines easily; 20% that their child had a problem taking a few medicines; 4% that their child had a problem taking most medicines; and 4% that it was almost impossible to get their child to take any medicine.
Asked about methods used to encourage children to take disliked an- tibiotics, 73% of parents indicated that they rarely had to mask the taste; 13% indicated that they had to offer sweets after the medicine was taken;
576
R.H. SCHWARTZ
Taste Preference 100 1
45
80 80 1 55
n,,L i,n,,8,< 1 CFXxzPD CFX-ZPD CFX=CPD CFX>CPD CFXcCPD CFX=CPD
(n = 24) (n = 22) (n = 3) (n = 27) (n = 19) (n = 3)
Color Preference
CFX>CLA CFX<CLA CFX=CLA CFX>CLA CFX<CLA CFX=CLA
(n = 24) (n = 23) (n = 24) (n = 20) (n = 3)
89 loo- 89
80.
60.
40.
20- 9
2 0, 1 II I’ ‘I
CFX>AMX CFXeAMX CFX=AMX CFX>AMX CFX<AMX CFX=AMX
(n = 4) (n = 49) (n = 2) (n = 5) (n = 49) (n=l)
20
0 CFXaCFX-CS CFXeCFXCS
(n=ll) (n = 32)
2
CFX=CFX-CS
(n = 1)
mw--lI I7 oti CFX>CFX-CS CFX<CFX-CS CFX=CFX-CS
(n = 10) (n = 31) (n = 3)
Figure 2. Mean percentages of children preferring the taste and color of cefuroxime axetil (CFX) compared with cefpodoxime proxetil (CPD), clarithromycin (CLA), amoxicil- lin (AMX), and cefuroxime axetil with a chocolate syrup chaser (CFX-CS). Key:
> indicates that the first medicine was preferred over the second medicine; < indicates that the second medicine was preferred over the first; and = indicates that the medicines were preferred equally.

CURRENT THERAPEUTIC RESEARCH@
4% indicated that they had to mix sweets intermittently with medicine; 9% indicated that they had to cajole, scold, bribe, and/or threaten in addi- tion to offering sweets; and 1% indicated that they could not persuade their child to take antibiotics at all.
The top 5 medicines that parents indicated their children liked (before study entry) were amoxicillin (69% of parents), azithromycin (5%), amoxi- cillin/clavulanate (4%), cefuroxime axetil (3%), and cefixime (3%). The top 5 medicines that parents indicated their children mildly liked (before study entry) were amoxicillin (8% of parents), amoxicillin/clavulanate (5%), azithromycin (3%), cefuroxime axetil (3%), and penicillin (3%). The top 5 medicines that parents indicated their children did not like (before study entry) were amoxicillin/clavulanate (5% of parents), amoxicillin (4%), cef- uroxime axetil (3%), all chewable antibiotics (2%), and azithromycin (2%).
DISCUSSION AND CONCLUSIONS
Administration of cefuroxime axetil suspension with a chocolate syrup chaser significantly reduced the unpleasant aftertaste of the suspension. With the chocolate syrup chaser, the aftertaste of cefuroxime axetil was rated as being as palatable as amoxicillin. Another possible way of admin- istering the chocolate syrup would be to mix equal parts of chocolate syrup with cefuroxime axetil and to administer the premixed brown suspension, an option not evaluated in this study.
Amoxicillin is characterized as having excellent palatability in sus- pension.3 Thus, amoxicillin served as a positive control in this study. With an aftertaste score as favorable as that of amoxicillin, cefuroxime axetil suspension with a chocolate syrup chaser combines palatability with broad-spectrum efficacy and tolerability. Cefuroxime axetil suspension with a chocolate syrup chaser may possess advantages over amoxicillin, particularly when broad-spectrum coverage is desired or infection with amoxicillin-resistant bacteria is likely.
“Taste” consists not only of flavor, aftertaste, and color, but also of consistency (degree of grittiness and thickness) and odor. In addition to flavor and color, consistency and odor may have influenced children’s ratings and preferences in this study. The similarity in the children’s responses to cefuroxime axetil, cefpodoxime proxetil, and clarithromycin may be attributed in part to the thickness and grittiness of these suspensions.
This study extends previous taste research in pediatric suspensions, much of which involved adult subjects. 15-18 The relevance of the previous adult work to children is questionable, given the recent demonstration that adult subjects’ judgment of the palatability of oral suspensions differs from that of children.lg In addition, adults’ subjective experience of other medi-
578

R.H. SCHWARTZ
cation attributes that may affect compliance, such as color, is likely to differ from children’s experience.
Subjective experience of medication attributes may vary with age, even among children. Older children (aged 6-8 years) rated medicines less favorably than did younger children (aged 3-5 years) in this study. These data are consistent with previous research suggesting that older children are more discriminating than younger children in their evaluation of medi- cine tastes.20 Whereas children aged 26 years preferred and showed greater acceptance of a sweetened test suspension of phenoxymethylpeni- cillin than of the standard suspension in one 319-patient study,20 children aged <6 years did not distinguish between the 2 on the basis of taste, accepting both formulations equally. Applied to the present study, these findings suggest that use of a chocolate syrup chaser with cefuroxime axetil suspension may be particularly important in enhancing older chil- dren’s gustatory experience of the medication.
Children generally rated the medicines tried first more favorably than they did those tried second. This primacy effect has also been observed in paired-comparison taste tests conducted in adults. In 2 consumer research studies21 including 11 taste tests, 13- to 49-year-old subjects (n = 1196) tended to prefer and to assign the highest rating scores to the taste sampled first. It was suggested that this primacy effect could be attributed to desensitization of the palate or to reduction of attention over the testing session, either of which may apply to the data from the present pediatric study.
In the present study, taste scores systematically varied not only with patient age and treatment order but also with cefuroxime axetil dose. Patients receiving the high dose of cefuroxime axetil suspension (250 mgl 5 mL) rated cefuroxime axetil less favorably and comparators more favor- ably than did patients receiving the low dose (125 mg/5 mL). This result is not surprising, since children given the high dose received twice the con- centration of medicine as did children given the low dose.
Children’s preferences for antibiotic color matched their taste prefer- ences. Both cefuroxime axetil followed by a chocolate syrup chaser and amoxicillin were preferred more often than cefuroxime axetil alone, whereas cefpodoxime proxetil and clarithromycin suspensions were pre- ferred about as often as cefuroxime axetil alone. Amoxicillin suspension is pink; the other 3 suspensions are white. The color pink is often particularly pleasing to young children, and it is not surprising that they rated amoxi- cillin’s color favorably. The finding that white cefuroxime axetil was pre- ferred for color much more often when it was followed by a chocolate syrup chaser (71%) than when it was not (23%) suggests that children’s color preferences were dictated by their taste experience, which was more pleas- ant with the chocolate syrup chaser. This finding is not surprising in view of the fact that for all children in the study, the taste test occurred imme-
579

CURRENT THERAPEUTIC RESEARCH@
diately before the indication of color preference. Future research might counterbalance the order of taste and color-preference ratings to more precisely define the role of color in children’s preferences for antibiotic suspensions.
The finding from this study conducted in a suburban Virginia pediat- ric practice that >70% of parents indicated their child takes most or all medications easily suggests that for the majority of pediatric patients in this sample, taste was not a major concern. However, for the children in whom taste is an issue, the results of this study show that administration of cefuroxime axetil suspension with a chocolate syrup chaser significantly enhances its palatability. Parents can be advised that administering cefur- oxime axetil suspension mixed with or followed by chocolate syrup is a simple, effective strategy for enhancing children’s satisfaction with anti- biotic therapy.
Acknowledgment
This study was funded by Glaxo Wellcome, Inc, Research Triangle Park, North Carolina.
References:
1. Nelson CR, Knapp DE. Medication Therapy in Ambulatory Medical Care: National Am- bulatory Medical Care Survey and National Hospital Ambulatory Medical Care Survey, 1992. Vol. 290. Rockville, Md: US Department of Health and Human Services; 1997.
2. Woodwell DA. National Ambulatory Medical Care Survey: 1997 Summary. Vol. 205. Rockville, Md: US Department of Health and Human Services; 1999.
3. Pichichero ME. Empiric antibiotic selection criteria for respiratory infections in pediatric practice. Pediatr Infect Dis J. 1997;16(Suppl 3):S60-S64.
4. Klein JO. Management of acute otitis media in an era of increasing antibiotic resistance. Znt J Pediatr Otorhinolaryngol. 1999;49(Suppl l):S15-S17.
5. Dowel1 SF, Butler JC, Giebink S, et al. Acute otitis media: Management and surveillance
in an era of pneumococcal resistance-a report from the Drug-Resistant Streptococcus pneumoniae Therapeutic Working Group. Pediatr Infect Dis J. 1999;18:1-9.
6. Brodie DP, Griggs JV, Cunningham K. Comparative study of cefuroxime axetil suspen- sion and amoxicillin syrup in the treatment of acute otitis media in general practice. JZnt Med Res. 1990;18:235-239.
7. McLinn SE, Moskal M, Goldfarb J, et al. Comparisons of cefuroxime axetil and amoxi- cillin-clavulanate suspensions in treatment of acute otitis media with effusion in chil-
dren. Antimicrob Agents Chemother. 1994;38:315-318.
8. Gooch WM III, Blair E, Puopolo A, et al. Effectiveness of five days of therapy with
cefuroxime axetil suspension for treatment of acute otitis media. Pediatr Znfect Dis J. 1996;15:157-164.
9. Gooch WM III, Blair E, Puopolo A, et al. Clinical comparison of cefuroxime axetil sus- pension and amoxicillin/clavulanate suspension in the treatment of pediatric patients with acute otitis media with effusion. Clin Ther. 1995:17:838-851,
580

R.H. SCHWARTZ
10. Pessey JJ, Gehanno P, Thoroddsen E, et al. Short course therapy with cefuroxime axetil for acute otitis media: Results of a randomized multicenter comparison with amoxicillim clavulanate. Pediatr Infect Dis J. 1999;18:854-859.
11. Pichichero M, Aronovitz GH, Gooch WM, et al. Comparison of cefuroxime axetil, cefaclor, and amoxicillin-clavulanate potassium suspensions in acute otitis media in infants and
children. South Med J. 1990;83:1174-1177.
12. Kafetzis DA, Malaka-Zafiriou C, Bairamis T, et al. Comparison of the efficacy and tol-
erability of clarithromycin suspension and cefuroxime axetil suspension in the treatment of acute otitis media in paediatric patients. Clin Drug Invest. 1997;14:192-199.
13. Werk LN, Bauchner H. Practical considerations when treating children with antimicro-
bials in the outpatient setting. Drugs. 1998;55:779-790.
14. Eisen SA, Miller DK, Woodward RS, et al. The effect of prescribed daily dose frequency on patients’ medication compliance. Arch Intern Med. 1990;150:1881-1884.
15. Steele RW, Estrada B, Begue RE, et al. A double-blind taste comparison of pediatric antibiotic suspensions. Clin Pediatr. 1997;36:193-199.
16. Dagan R, Shvartzman P, Liss Z. Variation in acceptance of common oral antibiotic sus- pensions. Pediatr Infect Dis J. 1994;13:686-690.
17. Uhari M, Eskelinen L, Jokisalo J. Acceptance of antibiotic mixtures by infants and children. Eur J Clin Pharmacol. 1986;30:503-504.
18. Samulak KM, El-Chaar GM, Rubin LG. Randomized, double-blind comparison of brand and generic antibiotic suspensions: A study of taste in adults. Pediatr Infect Dis J. 1996;15:14-17.
19. Matsui D, Lim R, Tschen T, et al. Assessment of the palatability of beta-lactamase- resistant antibiotics in children. Arch Pediatr Adolesc Med. 1997;151:599-602.
20. Bagger-Sjoback D, Bondesson G. Taste evaluation and compliance of two paediatric for- mulations of phenoxymethylpenicillin in children. Stand J Prim Health Care. 1989;7: 87-92.
21. Dean ML. Presentation order effects in product taste tests. JPsychol. 1980;105:107-110.
581