enhancing home visiting with mental health...
TRANSCRIPT

Enhancing Home Visiting With Mental HealthConsultation
abstractHome visiting programs have been successful in engaging and enroll-ing families who are at high risk for stress, depression, and substanceabuse. However, many of these mothers may not be receiving mentalhealth services because home visitors lack the knowledge and skills toidentify mental health or determine how to appropriately addressthese problems. In response, a growing number of home visiting pro-grams are expanding their capacity by integrating a mental health pro-vider into their ongoing operations. This approach, referred to as earlychildhood mental health consultation, involves a partnership betweena professional consultant with early childhood mental health expertiseand home visiting or family support programs, staff, and families. Thisintegrated model holds the promise of promoting parent and child be-havioral health by enhancing the capacity of home visitors to identifyand appropriately address the unmet mental health needs of childrenand families. The article highlights efforts under way in several fed-erally funded Linking Actions for Unmet Needs in Children’s HealthProject sites where local programs are testing the effectiveness ofthis model. Pediatrics 2013;132:S180–S190
AUTHORS: Barbara Dillon Goodson, PhD,a Mary Mackrain,MEd,b Deborah F. Perry, PhD,c Kevin O’Brien, LMFT, LCSW,d
and Margaret K. Gwaltney, MBAe
aDillon-Goodson Research Associates, Westfield, Massachusetts,bEducation Development Center, Newton, Massachusetts,cGeorgetown University Center for Child and HumanDevelopment, Washington, District of Columbia, dAurora FamilyService, Milwaukee, Wisconsin, and eAbt Associates Inc, Bethesda,Maryland
KEY WORDSmental health consultation, home visiting, evidence-basedpractice, behavioral health, pediatric medical home
ABBREVIATIONSProject LAUNCH—Linking Actions for Unmet Needs in Children’sHealthSAMHSA—Substance Abuse and Mental Health ServicesAdministration
Dr Goodson was involved in the conceptualization and designof the paper, drafted the initial manuscript, and revised themanuscript in response to reviewers’ comments; Ms Mackrainand Dr Perry were involved in the conceptualization and designof the paper, drafted key sections of the manuscript, and revisedthe manuscript in response to reviewers’ comments; Mr O’Brienwas involved in the conceptualization and design of the paper,and provided data for and drafted portions of the manuscript;Ms Gwaltney was involved in the conceptualization and design ofthe paper, critically reviewed the manuscript, and revised themanuscript in response to reviewers’ comments; and allauthors approved the final manuscript as submitted.
www.pediatrics.org/cgi/doi/10.1542/peds.2013-1021S
doi:10.1542/peds.2013-1021S
Accepted for publication Aug 26, 2013
Address correspondence to Barbara Dillon Goodson, PhD, Dillon-Goodson Research Associates, 409 Montgomery Road, Westfield,MA 01085. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2013 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they haveno financial relationships relevant to this article to disclose.
FUNDING: The US Department of Health and Human Services,Substance Abuse and Mental Health Services Administration isthe funding source for the Linking Actions for Unmet Needs inChildren’s Health program. Funding for the cross-site evaluationof the Linking Actions for Unmet Needs in Children’s Healthprogram is provided to Abt Associates, Inc, through a contractwith the Administration for Children and Families.
POTENTIAL CONFLICT OF INTEREST: The authors have indicatedthey have no potential conflicts of interest to disclose.
S180 Goodson et al by guest on August 10, 2018www.aappublications.org/newsDownloaded from

There is a growing consensus that manychronic health and developmental mor-bidities are the product of a complexinteraction of biological, psychosocial,and environmental influences.1 Recentdiscoveries in neuroscience, for exam-ple, point to the cumulative impact ofadverse childhood experiences on thedevelopment of a broad range of laterconditions.2 Children exposed to ongoingadverse experiences can face prolongedstress, often referred to as “toxic stress,”which puts them at risk for changes inthe architecture and later functioning oftheir brains and immune systems.3
These child risk factors may arise fromdynamics in their own families, includingmaternal depression and clinical andsocial correlates of this depression:trauma and intimate partner violence,poor birth outcomes, and infant mor-tality.4 Maternal depression, oftenunderdiagnosed and untreated in thefirst several years of life, is a particularlyprevalent concern, with estimates rang-ing from 15% in the general populationto double that in low-income mothers.5
As pediatric providers begin to in-corporate the latest findings from neu-roscience into their efforts to establishhigh-quality medical homes for theirpatients, they find themselves servingmany families who may be at risk fortoxic stress and who are experiencingpsychosocial challenges. However, pedi-atricians and primary care providersoften report not having enough knowl-edge to detect and manage mentalhealth problems in young children andto make referrals for mental healthprevention and treatment services.5
Pediatric primary care practices cantake steps to care for young childrenwith mental health problems, as well asnormalizing and destigmatizing mentalhealth, by engaging families in com-munity services like home visitation.6
Home visitation programs are oftendesigned to serve families and youngchildren who are at heightened risk,
including families living in poverty,teenage and single parents, and fami-lies at risk for child maltreatment.
In one study of a Healthy FamiliesAmerica home visiting program, almost30% of mothers enrolled screenedpositive for depression, and about 70%reported experiencing at least 1 violenttrauma in their lives.7 Furthermore,although estimated rates of depres-sion among pregnant, postpartum, andparenting mothers range from 5% to25%,8 a review of studies revealed thatbetween 28% and 61% of mothers en-rolled in home visiting programs wereidentified with depression.7 Experi-ences of depression, substance abuse,or intimate partner violence in preg-nant women have been found to con-tribute to low birth weight, pretermbirths, increased pain and discomfortduring pregnancy and childbirth, andhigher levels of stress.9
At the same time that home visitingprograms appear to be reaching someof the most vulnerable families, evi-dence exists that home visitation pro-grams alone may not be sufficient toaddress all of the mental health needsof the families they serve. A study of aninitiative that implemented 4 homevisiting models (Healthy Start, HealthyFamilies America, and 2 locally de-veloped models) found that fewer than25% of women with depressive symp-toms receivedmental health services inthe6monthsafterenrollment inahomevisiting program.10 Focus groups withhome visitors suggest that trainingmay not equip home visitors to addressthe mental health, substance abuse,and domestic violence in the familiesthey serve.11,12
INTEGRATION OF EARLYCHILDHOOD MENTAL HEALTHCONSULTATION AND HOMEVISITING
Inresponsetothesechallenges,agrowingnumber of home visiting programs are
expanding their capacity to serve high-risk families by integrating a mentalhealth provider into the ongoing oper-ations of their programs. These ap-proaches, referred to as early childhoodmental health consultation, involve apartnership between a professionalconsultant with early childhood mentalhealth expertise and home visitingprograms,staff, and families; themodelsare similar to the integration of mentalhealth consultation in early care andeducation settings, which has yieldedpromising results over the past de-cade.13 In home visiting, the mentalhealth consultation is designed to buildthe capacity of the home visitors torecognize, interpret, and support theindividual socioemotional needs ofchildren and families in their care, es-pecially when there are mental healthconcerns, and to support families increating home environments that arepositive climates for children’s learningand growth.14 Mental health consulta-tion can involve multiple types of sup-port for home visitors, includingconsultation about the individual needsof children and families, professionaldevelopment on mental health–relatedtopics, and group and one-on-one re-flective supervision. Reflective supervi-sion provides home visitors withongoing and regular opportunities forreflection to sort out and cope withstrong feelings brought on by complexwork with families.15–19 Reflective su-pervision also allows the home visitor toexperience the same high-quality, sup-portive relationship that he or she isexpected to provide for infants, tod-dlers, and families.15
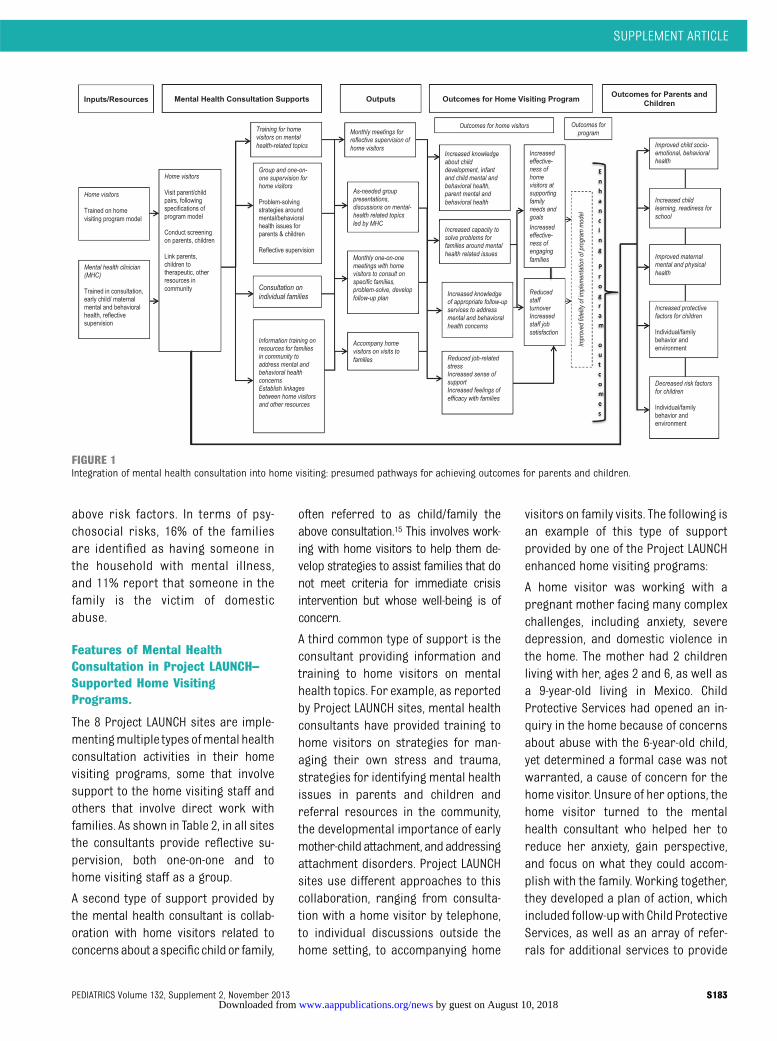
Integrating mental health consultationintohomevisitingprograms isbasedona set of expectations about how pro-grams can enhance their intendedeffects on parents and children served.Figure 1 provides a schema depictingseveral presumed pathways by whichmental health consultation integrated
SUPPLEMENT ARTICLE
PEDIATRICS Volume 132, Supplement 2, November 2013 S181 by guest on August 10, 2018www.aappublications.org/newsDownloaded from

into home visiting programs might en-hance outcomes for parents and chil-dren. The primary pathway is throughthe home visitors: mental health con-sultation provides information andsupport that are intended to equiphome visitors with additional skills andto increase their effectiveness at help-ing families deal with parental or childmental health issues. This could im-prove not only children’s socioemotionaloutcomes but, potentially, other out-comes, if mental or behavioral healthissues have been barriers to otheraspects of child learning and de-velopment. A second potential pathwayto improved parent and child out-comes is through improved identifi-cation of behavioral health problemsand facilitated referral to treatment orbrief intervention, which can lead toincreased capacity for positive par-enting, healthy parent/child inter-actions, and healthy child functioning.A third pathway is through increasedjob satisfaction and reduced job stressfor home visitors, which is hypothe-sized to increase effectiveness inworking with the families they serve. Afourth pathway shown on the logicmodel is through a potential strength-ening of the quality of implementationof the home visiting program (eg,stronger fidelity of implementation). Iffamilies receive help in addressingtheir mental health concerns, theymay engage more fully with the homevisitor who, in turn, may be better ableto implement the planned strategiesfor improving family and child out-comes.
This developing approach in home vis-iting is particularly noteworthy in lightof the rapid expansion in the number offamilies and children with access tohome visitation services. Of the morethan4millionbirths in theUnitedStateseach year, an estimated 400 000 infantsand their families currently receiveintensive home visitation services.20
This number is expected to increaseover the next 5 years, as states expandtheir evidence-based home visiting pro-grams with funding provided by thePatient Protection and Affordable CareAct. This legislation provides $1.5 bil-lion in new federal dollars for the Ma-ternal Infant and Early Childhood HomeVisiting program.
MENTAL HEALTH CONSULTATION INHOME VISITING PROGRAMS IN THELINKING ACTIONS FOR UNMETNEEDS IN CHILDREN’S HEALTHPROJECT
Since 2009, the Substance Abuse andMental Health Services Administration(SAMHSA) has been promoting behav-ioral health and prevention of futuremental health problems in young chil-dren (prenatal to 8 years) and theirfamilies through its Project LAUNCH(Linking Actions for Unmet Needs inChildren’s Health) grant program. Pro-ject LAUNCH provides funding to 35states, tribal nations, and local com-munities to implement evidence-basedprograms that represent 5 broad pre-vention and promotion strategies: en-hanced home visitation, family educationand support, developmental screeningand assessment, early childhood men-tal health consultation, and integrationof behavioral health in primary care.
The mandate of Project LAUNCH hasbeen an impetus for the LAUNCH com-munities to integrate physical and be-havioral health services and supportsfor children and their families. Oneconsequence has been that a growingnumber of Project LAUNCH granteeshave opted to develop innovative mod-els that integrate early childhoodmental health consultation into existinghome visitation services. This in-tegrated model holds the promise ofpromoting parent and child behavioralhealth by enhancing the capacity ofhome visitors to identify and appro-priately address the unmet mental
health needs of children and families.Additionally, these integration effortsare helping communities align withfederal Project LAUNCH guidelines toenhance existing services, rather thansupplant funds, and, in the case of thenew federal home visiting program,Maternal Infant and Early ChildhoodHome Visiting, grantees are chargedwith supporting efforts to meet thebenchmarks for high-quality imple-mentation.
Project LAUNCH grantees are alsoimplementing mental health consulta-tion in primary care settings. Here, themotivation is the same: to give theprimary care providers who are caringfor young children and families withmental or behavioral health concernsaccess to trained mental health con-sultants. These consultants can providescreening, assessment, and consulta-tion to the primary care providersabout individual children and partici-pate in developing a referral plan forappropriate services.
PROJECT LAUNCH HOME VISITINGMODELS AND THE RISK PROFILEOF FAMILIES IN HOME VISITINGPROGRAMS
Among the Project LAUNCH granteesfunded between 2009 and 2011, 8 areimplementing early childhood mentalhealth consultation within 12 homevisiting programs. Table 1 describesthe program objectives, eligibilitycriteria, and staffing for these 12programs. Data collected by granteeson the families who participated inthe home visiting programs showthat families experience multiplestresses that pose risks to children.On average, most mothers in thehome visiting programs are single(63%) and lack a high school educa-tion (55%); in addition, 41% of themothers are unemployed and 46%are teens. Forty-four percent of themothers experience at least 3 of
S182 Goodson et al by guest on August 10, 2018www.aappublications.org/newsDownloaded from
above risk factors. In terms of psy-chosocial risks, 16% of the familiesare identified as having someone inthe household with mental illness,and 11% report that someone in thefamily is the victim of domesticabuse.
Features of Mental HealthConsultation in Project LAUNCH–Supported Home VisitingPrograms.
The 8 Project LAUNCH sites are imple-mentingmultiple types ofmental healthconsultation activities in their homevisiting programs, some that involvesupport to the home visiting staff andothers that involve direct work withfamilies. As shown in Table 2, in all sitesthe consultants provide reflective su-pervision, both one-on-one and tohome visiting staff as a group.
A second type of support provided bythe mental health consultant is collab-oration with home visitors related toconcernsabout a specific child or family,
often referred to as child/family theabove consultation.15 This involves work-ing with home visitors to help them de-velop strategies to assist families that donot meet criteria for immediate crisisintervention but whose well-being is ofconcern.
A third common type of support is theconsultant providing information andtraining to home visitors on mentalhealth topics. For example, as reportedby Project LAUNCH sites, mental healthconsultants have provided training tohome visitors on strategies for man-aging their own stress and trauma,strategies for identifying mental healthissues in parents and children andreferral resources in the community,the developmental importance of earlymother-child attachment, and addressingattachment disorders. Project LAUNCHsites use different approaches to thiscollaboration, ranging from consulta-tion with a home visitor by telephone,to individual discussions outside thehome setting, to accompanying home
visitors on family visits. The following isan example of this type of supportprovided by one of the Project LAUNCHenhanced home visiting programs:
A home visitor was working with apregnant mother facing many complexchallenges, including anxiety, severedepression, and domestic violence inthe home. The mother had 2 childrenliving with her, ages 2 and 6, as well asa 9-year-old living in Mexico. ChildProtective Services had opened an in-quiry in the home because of concernsabout abuse with the 6-year-old child,yet determined a formal case was notwarranted, a cause of concern for thehome visitor. Unsure of her options, thehome visitor turned to the mentalhealth consultant who helped her toreduce her anxiety, gain perspective,and focus on what they could accom-plish with the family. Working together,they developed a plan of action, whichincluded follow-upwith Child ProtectiveServices, as well as an array of refer-rals for additional services to provide
FIGURE 1Integration of mental health consultation into home visiting: presumed pathways for achieving outcomes for parents and children.
SUPPLEMENT ARTICLE
PEDIATRICS Volume 132, Supplement 2, November 2013 S183 by guest on August 10, 2018www.aappublications.org/newsDownloaded from
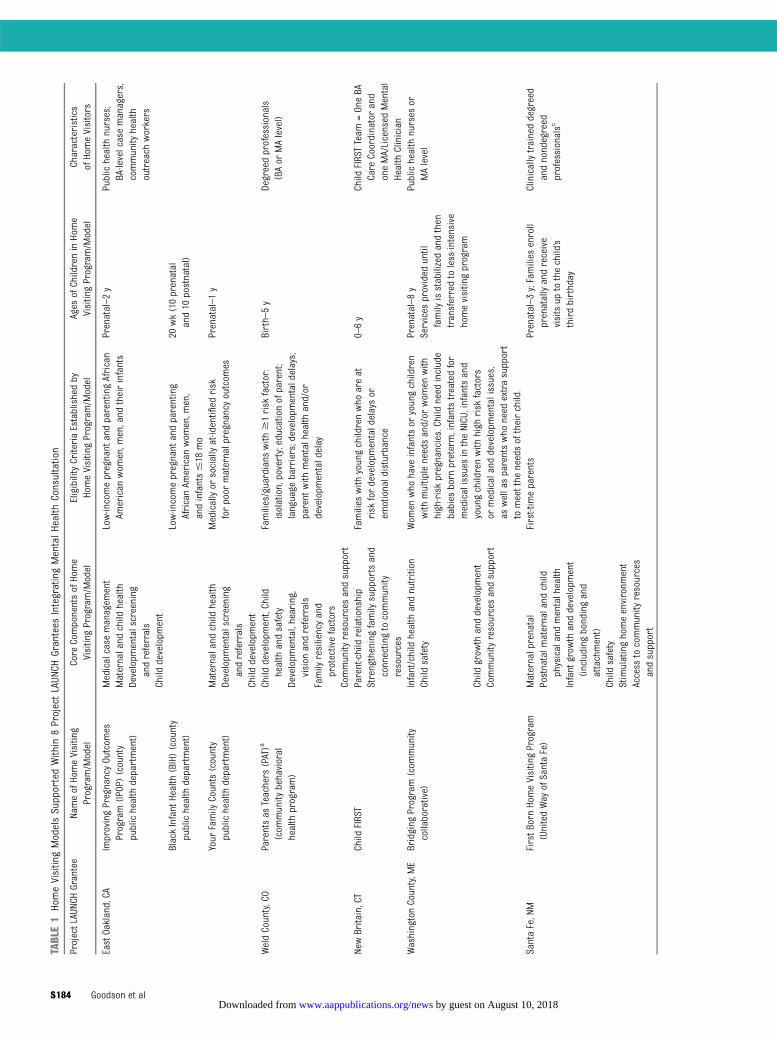
TABLE1
HomeVisitingModelsSupportedWithin
8ProjectLAUN
CHGrantees
IntegratingMentalHealth
Consultation
ProjectLAUNCHGrantee
NameofHomeVisiting
Program/M
odel
Core
ComponentsofHome
VisitingProgram/M
odel
EligibilityCriteriaEstablishedby
HomeVisitingProgram/M
odel
Ages
ofChildreninHome
VisitingProgram/M
odel
Characteristics
ofHomeVisitors
EastOakland,CA
ImprovingPregnancyOutcom
esProgram(IP
OP)(county
publichealth
department)
Medicalcase
managem
ent
Low-incomepregnant
andparentingAfrican
American
wom
en,m
en,and
theirinfants
Prenatal–2y
Publichealth
nurses;
BA-levelcasemanagers,
community
health
outreach
workers
Maternaland
child
health
Developm
entalscreening
andreferrals
Child
developm
ent
BlackInfant
Health
(BIH)(county
publichealth
department)
Low-incomepregnant
andparenting
AfricanAm
erican
wom
en,m
en,
andinfants#18
mo
20wk(10prenatal
and10
postnatal)
Your
Family
Counts(county
publichealth
department)
Maternaland
child
health
Medicallyor
sociallyat-identified
risk
forpoor
maternalpregnancy
outcom
esPrenatal–1y
Developm
entalscreening
andreferrals
Child
developm
ent
WeldCounty,CO
Parentsas
Teachers
(PAT)a
(com
munity
behavioral
health
program)
Child
developm
ent,Child
health
andsafety
Families/guardians
with
$1risk
factor:
isolation,poverty;educationofparent;
language
barriers;developmentaldelays;
parent
with
mentalhealth
and/or
developm
entaldelay
Birth–5y
Degreedprofessionals
(BAor
MAlevel)
Developm
ental,hearing,
vision
andreferrals
Family
resiliencyand
protectivefactors
Community
resourcesandsupport
NewBritain,CT
Child
FIRST
Parent-childrelationship
Families
with
youngchildrenwho
areat
risk
fordevelopm
entaldelaysor
emotionaldisturbance
0–6y
Child
FIRSTTeam
=OneBA
Care
Coordinatorand
oneMA/Licensed
Mental
Health
Clinician
Strengtheningfamily
supportsand
connectingtocommunity
resources
WashingtonCounty,M
EBridging
Program(com
munity
collaborative)
Infant/childhealth
andnutrition
Wom
enwho
have
infantsor
youngchildren
with
multipleneedsand/or
wom
enwith
high-riskpregnancies.Child
need
include
babies
born
preterm,infantstreatedfor
medicalissues
intheNICU,infantsand
youngchildrenwith
high
risk
factors
ormedicalanddevelopm
entalissues,
aswellasparentswho
need
extrasupport
tomeetthe
needsoftheirchild.
Prenatal–8y
Publichealth
nurses
orMAlevel
Child
safety
Services
provided
until
family
isstabilizedandthen
transferredtoless-intensive
homevisitingprogram
Child
grow
thanddevelopm
ent
Community
resourcesandsupport
SantaFe,NM
FirstB
ornHomeVisitingProgram
(UnitedWay
ofSantaFe)
Maternalprenatal
First-timeparents
Prenatal–3y;Families
enroll
prenatallyandreceive
visitsup
tothechild’s
thirdbirthday
Clinicallytraineddegreed
andnondegreed
professionalsc
Postnatalm
aternaland
child
physicalandmentalhealth
Infant
grow
thanddevelopm
ent
(including
bondingand
attachment)
Child
safety
Stimulatinghomeenvironm
ent
Access
tocommunity
resources
andsupport
S184 Goodson et al by guest on August 10, 2018www.aappublications.org/newsDownloaded from

TABLE1
Continued
ProjectLAUNCHGrantee
NameofHomeVisiting
Program/M
odel
Core
ComponentsofHome
VisitingProgram/M
odel
EligibilityCriteriaEstablishedby
HomeVisitingProgram/M
odel
Ages
ofChildreninHome
VisitingProgram/M
odel
Characteristics
ofHomeVisitors
NewYork
City,NY
Nurse-Family
Partnership
Program(NFP)a
Healthypregnanciesandinfants
First-timemother,28
wkpregnant
orless,low
income
Prenatal–2y
Publichealth
nurses
Child
health,development,
andscreening
Families
have
the
opportunity
toparticipate
for2+
y(until
child’ssecond
birthday)
Family
socialsupportand
econom
icself-sufficiency
Parent-infant
attachmentCommunity
resourcesandsupport
Multnom
ahCounty,OR
HealthyStart∼HealthyFamilies
Oregon–HealthyFamilies
Americaa
Preventionofchild
abusethrough
improved
parent-childrelationship
First-timemothers
0–3y
BA-levelprofessionals
Family
stability
Atleast2risk
factors,or
depression
orsubstanceabuse
Families
typically
participate
for6–12
mo
Schoolreadiness
Healthychild
developm
ent
Milw
aukee,WI
EmpoweringFamilies
ofMilw
aukee—
includes
HealthyFamilies
America,
PATa(city
publichealth
department)
Improved
birthoutcom
esMothers
atrisk
forpoor
birthoutcom
esPrenatal–age3
Socialworker(BSW
/MSW
)or
community
health
workerandpublic
health
nurseteam
Infant
andchild
health
Families
enrollprenatallyand
receivevisitsuntilchild’s
thirdbirthday
Child
Safety
Child
grow
thanddevelopm
ent
Family
functioning
NFPa
(city
publichealth
department)
Improved
pregnancyandbirth
outcom
esFirst-timepregnant
teensand
wom
en,28
wkpregnant
Prenatal–2y
Publichealth
nurses
Child
health
anddevelopm
ent
Families
enrollprenatallyand
receivevisitsuntilchild’s
second
birthday
Family
econom
icself-sufficiency
HomeInstructionforParentsof
PreschoolYoungsters(HIPPY)a
(COA
bYouthandFamily
Centersa)
Parent
involvem
ent
Resident
ofMilw
aukee
3–5y
Parents
Schoolreadiness
Programoperates
foraschool
year
(30wk),and
families
can
participatemultipletim
eswhen
child
isbetweenages
3and5
BA,bachelor’s
degree;BSW
,bachelor’s
degree
insocialwork;MA,master’s
degree;M
SW,m
aster’s
degree
insocialwork.
aEvidence-based
programmodel.
bCOA(the
Community
OutingAssociation)
isanonprofitagencysupportingsocialserviceandeducationalprojectsinMilw
aukee.
cProgrammodelspecifies
thathomevisitors
arepublichealthnurses;because
thereisashortsupplyofclinicallytrainedstaffinthecounty,inSantaFe,the
homevisitors
areamixofbachelor’sdegree
andnon-BA
staffw
ithexperience
insocial
services.
SUPPLEMENT ARTICLE
PEDIATRICS Volume 132, Supplement 2, November 2013 S185 by guest on August 10, 2018www.aappublications.org/newsDownloaded from
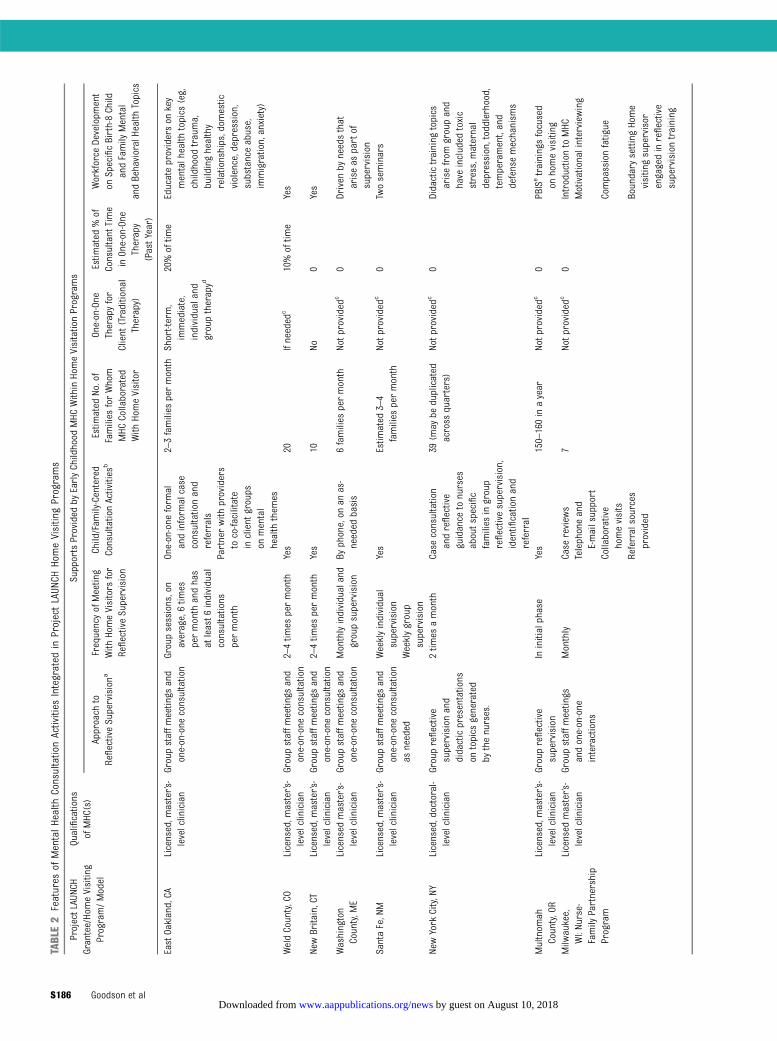
TABLE2
Features
ofMentalHealth
ConsultationActivities
Integrated
inProjectLAUN
CHHomeVisitingPrograms
ProjectLAUN
CHGrantee/HomeVisiting
Program/Model
Qualifications
ofMHC(s)
SupportsProvided
byEarlyChildhood
MHC
WithinHomeVisitationPrograms
Approach
toReflectiveSupervisiona
FrequencyofMeeting
With
HomeVisitors
for
ReflectiveSupervision
Child/Fam
ily-Centered
ConsultationActivities
bEstim
ated
No.of
Families
forWhom
MHC
Collaborated
With
HomeVisitor
One-on-One
Therapyfor
Client
(Traditional
Therapy)
Estim
ated
%of
Consultant
Time
inOne-on-One
Therapy
(PastYear)
Workforce
Developm
ent
onSpecificBirth-8Child
andFamily
Mental
andBehavioralHealth
Topics
EastOakland,CA
Licensed,m
aster’s-
levelclinician
Groupstaffm
eetings
and
one-on-one
consultation
Groupsessions,on
average,6tim
espermonth
andhas
atleast6
individual
consultations
permonth
One-on-one
form
alandinform
alcase
consultationand
referrals
2–3families
permonth
Short-term,
immediate,
individualand
grouptherapyd
20%oftim
eEducateproviderson
key
mentalhealth
topics
(eg,
childhood
trauma,
buildinghealthy
relationships,dom
estic
violence,depression,
substanceabuse,
immigration,anxiety)
Partnerwith
providers
toco-facilitate
inclient
groups
onmental
health
them
esWeldCounty,CO
Licensed,m
aster’s-
levelclinician
Groupstaffm
eetings
and
one-on-one
consultation
2–4tim
espermonth
Yes
20Ifneeded
c10%oftim
eYes
NewBritain,CT
Licensed,m
aster’s-
levelclinician
Groupstaffm
eetings
and
one-on-one
consultation
2–4tim
espermonth
Yes
10No
0Yes
Washington
County,M
ELicensed
master’s-
levelclinician
Groupstaffm
eetings
and
one-on-one
consultation
Monthlyindividualand
groupsupervision
Byphone,on
anas-
needed
basis
6families
permonth
Notp
rovidedc
0Driven
byneedsthat
ariseas
partof
supervision
SantaFe,NM
Licensed,m
aster’s-
levelclinician
Groupstaffm
eetings
and
one-on-one
consultation
asneeded
Weeklyindividual
supervision
Yes
Estim
ated
3–4
families
permonth
Notp
rovidedc
0Twoseminars
Weeklygroup
supervision
NewYork
City,NY
Licensed,doctoral-
levelclinician
Groupreflective
supervisionand
didacticpresentations
ontopics
generated
bythenurses.
2tim
esamonth
Case
consultation
andreflective
guidance
tonurses
aboutspecific
families
ingroup
reflectivesupervision,
identificationand
referral
39(m
aybe
duplicated
across
quarters)
Notp
rovidedc
0Didactictraining
topics
arisefrom
groupand
have
included
toxic
stress,m
aternal
depression,toddlerhood,
temperament,and
defensemechanism
s
Multnom
ahCounty,OR
Licensed,m
aster’s-
levelclinician
Groupreflective
supervision
Ininitialphase
Yes
150–160inayear
Notp
rovidedc
0PBISetrainingsfocused
onhomevisiting
Milw
aukee,
WI:Nurse-
Family
Partnership
Program
Licensed
master’s-
levelclinician
Groupstaffm
eetings
andone-on-one
interactions
Monthly
Case
review
s7
Notp
rovidedc
0Introductionto
MHC
Telephoneand
E-mailsupport
Motivationalinterview
ing
Collaborative
homevisits
Compassionfatigue
Referralsources
provided
Boundary
settingHome
visitingsupervisor
engagedinreflective
supervisiontraining
S186 Goodson et al by guest on August 10, 2018www.aappublications.org/newsDownloaded from

TABLE2
Continued
ProjectLAUN
CHGrantee/HomeVisiting
Program/Model
Qualifications
ofMHC(s)
SupportsProvided
byEarlyChildhood
MHC
WithinHomeVisitationPrograms
Approach
toReflectiveSupervisiona
FrequencyofMeeting
With
HomeVisitors
for
ReflectiveSupervision
Child/Fam
ily-Centered
ConsultationActivities
bEstim
ated
No.of
Families
forWhom
MHC
Collaborated
With
HomeVisitor
One-on-One
Therapyfor
Client
(Traditional
Therapy)
Estim
ated
%of
Consultant
Time
inOne-on-One
Therapy
(PastYear)
Workforce
Developm
ent
onSpecificBirth-8Child
andFamily
Mental
andBehavioralHealth
Topics
Providesupportin
addressing
screeningresults
Milw
aukee,WI:
Empowering
Families
ofMilw
aukee:
HealthyFamilies
America,Parents
asTeachers
(PAT)
Licensed
master’s-
levelclinician
Groupstaffm
eetings
andone-on-one
interactions
Monthly
Case
review
s43
Notp
rovidedc
0Introductionto
MHC
Telephoneand
E-mailsupport
Motivationalinterview
ing
Collaborative
homevisits
Compassionfatigue
Referralsources
provided
Boundary
setting
Providesupportin
addressing
screeningresults
Homevisitingsupervisor
engagedinreflective
supervisiontraining
HIPPY
Licensed
master’s-
levelclinician
Groupstaffm
eetings
andone-on-one
interactions
Monthly
Case
review
s19
Notp
rovidedc
0Introductionto
MHC
Telephoneand
E-mailsupport
Mandatory
reporting
Collaborative
homevisits
Referralsources
provided
HIPPY,HomeInstructionforParentsofPreschoolYoungershomevisitingprogrammodel;M
HC,m
entalhealth
consultant.
aReflectivesupervisionreferstotheMHC
working
with
homevisitorstobuild
capacityandproblem-solving
skillsaround
family/childmentalhealth
concerns;although
reflectivesupervisionmay
involvediscussion
ofspecificfamilies,the
focusisless
onproblemsolvingabouta
particular
family
andmoreon
thedevelopm
entofthe
homevisitors’ownskillsandstrategies
forworking
with
families
tosolveproblems.Itisintended
tocreatean
environm
entcharacterized
bysafety,calmness,and
support,in
which
supervisor
andsupervisee
exploretherangeofem
otions
(positive
andnegative)relatedtothefamilies
andissues
thesupervisee
ismanaging.Theroleofthesupervisor
istohelpthesupervisee
toansw
erhisor
herow
nquestions,and
toprovide
thesupportand
know
ledgenecessarytoguidedecision
making.Inaddition,thesupervisor
provides
anem
pathetic,nonjudgmentalear
tothesupervisee.W
orking
throughcomplex
emotions
ina“safeplace”allowsthesupervisee
tomanagethestress
heor
sheexperienceson
thejob.21
bCollaborationwith
homevisitorsinworking
with
individualfamilies
with
family/childconcerns.M
ayaccompany
homevisitorson
visitstofamilies
(1–3tim
es/fam
ily),may
jointly
developreferralplan,based
oninform
ationinconsultationinterviewwith
family,child/parentscreening.TheMHC
andhomevisitors
sharesomelevelofresponsibilityforoutcom
esforfamily,but
theMHC
isnottheprimaryclinicianor
therapisttofamily;the
MHC
hasamoreindirectrole.
cInmostofthe
ProjectLAUNCHsites,thehomevisitingprogramspurposelydo
notrefer
families
totheMHC
fortherapy,outofconcern
thatthiscouldaltertheobjectiveofmaintaining
theprimaryrelationshipbetweenthefamily
andthehomevisitor.
Exceptions
have
been
made,however,w
hentheMHC
hasbeen
abletoforgeabridge
totreatm
entthroughbuildingtrustduring
abriefinterventionwith
afamily
that
was
reluctanttoaccess
traditionalmentalhealth
services.
dInthisproject,theMHC
takeson
theroleofprovidingbrieffam
ilytherapy,motivated
largelyby
theprogram’srecognition
ofthenearlycompletelack
ofmentalhealth
services
inthecommunity.Treatmentincludesdyadicworkwith
newmothers
with
bondingdifficulty
with
theirinfantrelatedtoprevious
traumaor
depression;treatmentofsituationaldepressionoftenrooted
inprevious
trauma,issues
ofchild
abuse,or
substanceabuse;treatm
entofgeneralized
anxietyoftenbroughtonby
birthofthe
child
andrelatedtoprevious
traumaor
depression,and
perceivedlack
ofsupport;grouptherapyfocusedon
psycho-educationalcorefactorsofresiliency,attachment,healing,healthyrelationships,buildingacommunity
ofsupport,andhowtoprotect
them
selves
andtheirchildren.
ePBIS=PositiveBehavior
Interventions
andSupports,anapproach
thatuses
atieredpreventionfram
eworkforyoungchildren;basedon
a“teachingpyramid”representsacontinuumofsupportsandservices
designed
toprom
otesocioemotional
competenceandaddresschallengingbehaviorsinyoungchildren.
SUPPLEMENT ARTICLE
PEDIATRICS Volume 132, Supplement 2, November 2013 S187 by guest on August 10, 2018www.aappublications.org/newsDownloaded from

mental health, health, social, and medi-cal supports to the family. Unfortunately,cases such as these are common andthe mental health consultant playsakey role insupportinghomevisitors inaddressing complex family situations(ShinkleJ, EastOaklandProject LAUNCH,unpublished observations, 2012).
EVALUATING INTEGRATION OFMENTAL HEALTH CONSULTATION INHOME VISITING
Project LAUNCH has been a platform forinnovative models of early childhoodmental health consultation in homevisiting. If this integrated model con-tinues to develop as an approach inhome visiting, the field will need addi-tional research first on the imple-mentation of themodel, and, second, onits effects, to provide the evidence thefield needs to build quality standardsfor this approach. Comprehensive im-plementation studies are needed toilluminate how mental health consul-tation can be integrated with differentevidence-based home visiting models.Then, rigorous impact evaluationsshould be conducted on the value-added of integrating mental healthconsultation into home visiting forhome visitors and the families andchildren they serve. One of the unan-swered questions concerns the impactofmental health consultation on fidelityof implementation for evidence-basedhome visiting models: on the one hand,model developers have expressed con-cern that adding mental health con-sultants coulddetract from local effortsto adhere to the model specifications.On the other hand, as depicted in thelogicmodel, mental health consultationcouldresult inbetteradherence, throughincreased engagement of hard-to-reachclients, greater likelihood of deliveringthe intended content, and reductions instaff turnover.
Initial findings are promising. Somestudies have reported evidence that
home visitors with access to a men-tal health consultant have decreasedstress levels, lessened rates of “com-passion fatigue,” and reported an in-crease in professional growth, comparedwith home visitors who do not haveconsultation.22–24 Furthermore, Borisand colleagues25 showed excellent fea-sibility of augmenting nurse home vis-itors with a mental health consultantwho assisted with issues related topostpartum depression, domestic vio-lence, and the impact of these riskfactors on maternal-child interaction.Ammerman and colleagues26 have de-veloped and implemented a model ofhome visitation for depressed mothersthat includes home-based mentalhealth clinicians working in collabora-tion with home visitors. This augmen-tation of home visitation has helpedhome visitors facilitate successful re-ferrals, along with mothers’ active en-gagement with services.
Within Project LAUNCH, preliminaryfindings based on self-reports of homevisitors are encouraging. As part ofthe local evaluations in each of theProject LAUNCH sites, home visitors areasked about changes in their knowledgeand practice associated with ProjectLAUNCH–funded activities. Responsesfrom home visitors in 6 programs inwhich mental health consultation hadbeen in place for at least a year showedthat nearly 90% of the home visitorsreported change in their knowledge ofchildren’s socioemotional and behav-ioral health and development, and ofavailable options for follow-up servicesfor children with behavioral healthissues (Goodson, BD, Gwaltney, MK,Walker, DK. Cross-Site Evaluation ofProject LAUNCH: Interim Findings.Washington, DC: Office of Planning, Re-search and Evaluation, Administrationfor Children and Families, U.S. De-partment of Health and Human Ser-vices; in review). Additional qualitativedata from these Project LAUNCH sites
support the notion that these changesin knowledge resulted from collabora-tion with the mental health consultants.In the words of 3 home visitors:
My mental health consultant has spe-cialized knowledge and skills that I don’thave. She has helped me to see thingsthat I didn’t pick up on. She really fo-cuses on engagement of the family inthe process. And those are specializedskills that, again, most teachers, nurses,even social workers aren’t taught toaddress—such as readiness for changeand motivation and things that might beblocking a family’s engagement. I’m notdiagnosing, but now I pick up on possibleundiagnosed problems. [Home visitor,Project LAUNCH]
I am able to focus more on secure at-tachment, discipline, and toddler be-havior than I was before I had help froma mental health consultant. My obser-vational skills of parent/child interactionhave improved. [Home visitor, ProjectLAUNCH]
With support from my mental healthconsultant, I now pay more attention toa family’s mental health issues. It makesworking with families easier becausethe mental health consultant helps to de-stigmatize mental health needs. We areworking more with families on mentalhealth issues, and providing referrals (tomental health consultation, as well asother services). As a result of mentalhealth consultation, I am more skilled atassessing needs and have new ways tosee and understand the complexities ofmental health and well-being in families.[Home visitor, Project LAUNCH]
RECOMMENDATIONS AND NEXTSTEPS
Home visiting and pediatric practicesshare common goals and are serving thesame clients at a critical time in the livesof young children and their families.27
Families who are experiencing risk fac-tors, especially maternal depression,can benefit from enhanced collaborationbetween their pediatricians and homevisiting programs.5 In primary carepractices that are conducting routinescreening for maternal depression,home visiting programs, especiallythose with enhanced mental healthconsultation, can be an excellent placefor ongoing support to families who
S188 Goodson et al by guest on August 10, 2018www.aappublications.org/newsDownloaded from

exhibit depressive symptoms. Moth-ers with depression and familiesdealing with toxic stressors may beunlikely on their own to follow throughon health promotion and preventionsuggestions provided by the pediatri-cian. However, by linking with homevisiting programs, pediatric practiceshave access to home visitors who canreinforce guidance from pediatricians,prepare parents for an anticipated de-velopment, and facilitate a family’s useof appropriate ancillary services.28
Thus, home visiting programs that pro-videmental health consultation to homevisitors represent a potential resourcefor pediatricians who themselves maynot be able to meet the needs of thegrowing population of children andfamilies with mental health issues. Theexistence of these enhanced home vis-iting programs may increase the pedi-atric community’s ability to connectfamilies with other public and privatecommunity services that are importantfor the overall health of the child andfamily and encourage partnerships withreferral networks to access these re-sources for their patients. Home visitationinformed by mental health consultation
can be an important piece of the medi-cal home model for delivering primarycare that is continuous, comprehensive,family-centered, coordinated, compas-sionate, and culturally effective to allchildren and youth, regardless of theirhealth needs.
Project LAUNCH, which has been aspringboard for innovation in the in-tegration of mental health consultationin home visiting programs as well asin primary care settings, may be apromising platform for future research.Studies are needed on partnership ap-proaches between pediatric practicesandhomevisitingprograms that includemental health consultation and theeffects of these partnerships on theprevalence of maternal depression andthe healthy development of young chil-dren. The epidemic of mental healthconcerns in the nation makes it imper-ative that we determine service modelsthat can be effective with the most vul-nerable families in our communities.
ACKNOWLEDGMENTSWe acknowledge SAMHSA, which pro-vides funding for the Project LAUNCHprogram and the Training and Techni-
cal Assistance Contract led by the Ed-ucation Development Center, and theOffice of Planning, Research and Eval-uation within the Administration forChildrenand Families, which overseesthe cross-site evaluation of ProjectLAUNCH, led by Abt Associates. Wethank Jennifer Oppenheim, ProjectLAUNCHCoordinatorat SAMHSA, LauraHoard, Social Science Research Ana-lyst at the Administration for Chil-dren and Families, and Deborah KleinWalker, VicePresidentatAbtAssociates,for reviewing an early draft of this arti-cle. We also thank the 8 Project LAUNCHgrantees highlighted in the article andtheir local evaluators for providing in-formation about their home visitingprograms that integrate mental healthconsultation. Specific acknowledgmentgoes to the evaluators, local projectstaff, and technical assistance special-ist for the East Oakland, CA, ProjectLAUNCH site: Lisa Erickson, Jill Shinkle,and Gabriel Fain; and the project di-rector and local evaluator for theMilwaukee, WI, Project LAUNCH site:Leah Jepson and Courtenay Kessler. Fi-nally, we acknowledge Missy Robinsonfor her production assistance.
REFERENCES
1. Garner AS, Shonkoff JP; Committee on Psy-chosocial Aspects of Child and FamilyHealth; Committee on Early Childhood,Adoption, and Dependent Care; Section onDevelopmental and Behavioral Pediatrics.Early childhood adversity, toxic stress, andthe role of the pediatrician: translating de-velopmental science into lifelong health.Pediatrics. 2012;129(1). Available at: www.pediatrics.org/cgi/content/full/129/1/e224
2. Dube SR, Felitti VJ, Dong M, Giles WH, AndaRF. The impact of adverse childhoodexperiences on health problems: evidencefrom four birth cohorts dating back to1900. Prev Med. 2003;37(3):268–277
3. National Scientific Council on the DevelopingChild. Excessive stress disrupts the architec-ture of the developing brain: working paper#3. Cambridge, MA: Harvard University; 2005.Available at: www.developingchild.net
4. Ammerman RT, Putnam FW, Bosse NR, TeetersAR, Van Ginkel JB. Maternal depression inhome visitation: a systematic review. AggressViolent Behav. 2010;15(3):191–200
5. Earls MF; Committee on PsychosocialAspects of Child and Family HealthAmerican Academy of Pediatrics. Incor-porating recognition and management ofperinatal and postpartum depressioninto pediatric practice. Pediatrics. 2010;126(5):1032–1039
6. Foy JM, Kelleher KJ, Laraque D; AmericanAcademy of Pediatrics Task Force on Men-tal Health. Enhancing pediatric mentalhealth care: strategies for preparing a pri-mary care practice. Pediatrics. 2010;125(suppl 3):S87–S108
7. Stevens J, Ammerman RT, Putnam FG, VanGinkel JB. Depression and trauma history
in first time mothers receiving home visi-tation. J Community Psychol. 2002;30:551–564
8. Gaynes BN, Gavin N, Meltzer-Brody S, et al.Perinatal Depression: Prevalence, ScreeningAccuracy, and Screening Outcomes. Evi-dence Report/Technology Assessment,Number 119. Rockville, MD: Agency forHealthcare Research and Quality; 2005
9. Holden KB, McKenzie R, Pruitt V, Aaron K,Hall S. Depressive symptoms, substanceabuse, and intimate partner violenceamong pregnant women of diverse eth-nicities. J Health Care Poor Underserved.2012;23(1):226–241
10. Tandon SD, Parillo KM, Jenkins C, Duggan AK.Formative evaluation of home visitors’ rolein addressing poor mental health, domesticviolence, and substance abuse among low-
SUPPLEMENT ARTICLE
PEDIATRICS Volume 132, Supplement 2, November 2013 S189 by guest on August 10, 2018www.aappublications.org/newsDownloaded from

income pregnant and parenting women.Matern Child Health J. 2005;9(3):273–283
11. Harden BJ, Denmark N, Saul D. Un-derstanding the needs of staff in HeadStart programs: the characteristics, per-ceptions, and experiences of home visitors.Child Youth Serv Rev. 2009;32:371–379
12. Tandon SD, Parillo K, Mercer C, Keefer M,Duggan AK. Engagement in paraprofessionalhome visitation: families’ reasons for en-rollment and program response to identi-fied reasons. Womens Health Issues. 2008;18(2):118–129
13. Perry DF, Allen MD, Brennan E, Bradley J.The evidence base for mental health con-sultation in early childhood settings: a re-search synthesis addressing children’sbehavioral outcomes. Early Educ Dev. 2010;21(6):795–824
14. Cohen E, Kaufmann R. Early ChildhoodMental Health Consultation. Washington,DC: Substance Abuse and Mental HealthServices Administration and the GeorgetownUniversity Child Development Center; 2005
15. Fenichel E, ed. Learning through Supervi-sion and Mentorship to Support the De-velopment of Infants, Toddlers, and Their
Families. Arlington, VA: ZERO TO THREE/National Center for Clinical Infant Pro-grams; 1992
16. Bertacchi J. Relationship-based organ-izations. Zero to Three. 1996;17(2):1–7
17. Norman-Murch T. Reflective supervision asa vehicle for individual and organizationaldevelopment. Zero to Three. 1996;7(2):16–20
18. Norman-Murch T and Ward G. First steps inestablishing reflective practice and super-vision: Organizational issues and strate-gies. Zero to Three. 1999;20(1):10–14
19. Parlakian R. Look, Listen, and Learn: Re-flective Supervision and Relationship-based Work. Washington, DC: ZERO TOTHREE; 2001
20. Gomby D. Home Visitation in 2005: Out-comes for Children and Parents. Sunnyvale,CA: Invest in Kids Working Paper No. 7.Committee for Economic Development: In-vest in Kids Working Group; 2005.
21. Zero to Three National Center for Infants.Toddlers and Families. Three Building Blocksto Reflective Supervision. Washington, DC:ZERO TO THREE; 2011
22. Boris NW, Larrieu JA, McNeill P, Nagle GA,Steier A, Zeanah PD. The process and
promise of mental health augmentation ofnurse home visiting programs: Data fromthe Louisiana nurse-family partnership. In-fant Ment Health J. 2006;27(1):26–40
23. Fox RA, Mattek RJ, Gresl BL. Evaluation ofa university-community partnership toprovide home-based, mental health ser-vices for children from families living inpoverty. Community Ment Health J. 2013;49(5):599–610
24. Wasik BH. Staffing issues for home visitingprograms. The Future of Children 1993;3(3):140-157
25. Boris NW, Larrieu JA, Nagle GA, Zeanah PD.Nurse home visiting: perspectives fromnurses. Infant Ment Health J. 2006;27(1):41–54
26. Ammerman RT, Putnam FW, Kopke JE, et al.Development and implementation of a qualityassurance infrastructure in a multisite homevisitation program in Ohio and Kentucky. JPrev Interv Community. 2007;34(1-2):89–107
27. Nelson CS, Tandon SD, Duggan AK, SerwintJR. Communication between key stake-holders within a medical home: a qualita-tive study. Clin Pediatr (Phila). 2009;48(3):252–262
S190 Goodson et al by guest on August 10, 2018www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2013-1021S2013;132;S180Pediatrics
Margaret K. GwaltneyBarbara Dillon Goodson, Mary Mackrain, Deborah F. Perry, Kevin O'Brien and
Enhancing Home Visiting With Mental Health Consultation
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/132/Supplement_2/S180including high resolution figures, can be found at:
References
#BIBLhttp://pediatrics.aappublications.org/content/132/Supplement_2/S180This article cites 16 articles, 2 of which you can access for free at:
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on August 10, 2018www.aappublications.org/newsDownloaded from
DOI: 10.1542/peds.2013-1021S2013;132;S180Pediatrics
Margaret K. GwaltneyBarbara Dillon Goodson, Mary Mackrain, Deborah F. Perry, Kevin O'Brien and
Enhancing Home Visiting With Mental Health Consultation
http://pediatrics.aappublications.org/content/132/Supplement_2/S180located on the World Wide Web at:
The online version of this article, along with updated information and services, is
ISSN: 1073-0397. 60007. Copyright © 2013 by the American Academy of Pediatrics. All rights reserved. Print the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on August 10, 2018www.aappublications.org/newsDownloaded from