ensuring high quality diabetes care reaches elders · pdf fileensuring high quality diabetes...
TRANSCRIPT

Ensuring High Quality Diabetes Care Reaches Elders
Professor Alan Sinclair
Foundation for Diabetes Research in Older People
www.diabetesfrail.org
Hon Professor of Metabolic Medicine, University of Aston, UK

Foundation for Diabetes Research in Older People at Diabetes Frail - Our mission and vision 2014-17 Director: Professor Alan Sinclair
Our mission
• As a not for profit research organisation, to enhance the quality of diabetes care for older people through new initiatives in clinical practice, audit and research
• To provide a forum for discussion between health professionals and scientists, and involve people with diabetes, their carers and families, in programmes which promote their health and well-being
• To examine the relationship between diabetes and related metabolic disorders to the development of frailty and sarcopaenia
Our vision • Establish sustainable academic partnerships • Ensure policies and strategies are developed to
meet the needs of older people with diabetes and related metabolic disease
At: www.diabetesfrail.org
SPRINTT

Older People’s Diabetes Network (OPDN)
• 3rd National Conference of OPDN took place on November 13
• Hosted by Aston University
• Led by the network’s Clinical Lead Professor Alan Sinclair
• Sharing good practice and latest developments

Type 2 diabetes – A High Impact Disease in Older People
• 7th highest cause of years lost and 8th highest cause of disability adjusted life years in Western countries: in those aged 60–79 years, HR of death is 1.91 (men) and 2.53 (women)
• Older adults with diabetes have the highest rates of major lower-extremity amputation, myocardial infarction (MI), visual loss, and end-stage renal disease of any age group
• Those aged ≥75 years also have double the rate of emergency department visits for hypoglycaemia than the general population with diabetes
• An ADL restriction increases costs of care 3-fold and admission to a care home increases costs 9-fold!
Kirkman MS et al, Diabetes Care 2012; Weiss Co, 2011; Lubitz J et al,2003

• Retrospective cohort study of 71,092 type 2 diabetes patients aged >60 (mean 71 years) in California
• Showed U-shaped relationship between HbA1c and mortality, consistent across all age groups
• Lowest hazard ratio for mortality was at HbA1c of 7.5%
Haz
ard
rat
io
Age groups
HbA1c

Slide 6
• Prospective cohort study to explore hypothesis that dependent older people with diabetes (mean age 80y) able to achieve AGS target HbA1c <8% would have less functional decline than those whose HbA1c >8%
• But results showed the opposite!

2013/4 IDF Recommendations based on Functional Category
Considerations
• Need to provide clear guidance on metabolic targets
• Recognition of the complex spectrum of comorbidity and functional impairment in ageing populations
• Recognition of the ‘Vulnerability’ profile of older people with diabetes
• Acceptance that Frailty is a common pre-disability characteristic
Categories CATEGORY 1: FUNCTIONALLY INDEPENDENT
The usual HbA1c target is 7.0-7.5% / 53-59 mmol/mol.
CATEGORY 2: FUNCTIONALLY DEPENDENT
Subcategory A: Frail
The usual HbA1c target is 7.0-8.0% / 53-64 mmol/mol
Subcategory B: Dementia
An HbA1c target up to 8.5% / 70 mmol/mol may be appropriate
CATEGORY 3: END OF LIFE CARE
The glycaemic target is to avoid symptomatic hyperglycaemia

Figure 1
Diabetes Research and Clinical Practice 2014 105, 102-109DOI: (10.1016/j.diabres.2014.04.012)
Copyright © 2014 The Authors Terms and Conditions
Glycaemic Control in Norwegian Nursing Homes – a case of overtreatment? Andreassen LM et al, 2014.

Residents at Great Risk of Harm from Glucose-Lowering Agents – a Freedom of Information Study Milligan F, Krentz AJ, Sinclair AJ Dec 2011 – Diabetic Med
• Aim: To analyse adverse drug events in older people with diabetes in the care home setting via incident reports – Jan 2005 – Dec 2009
• A Freedom of Information request was made to the National Reporting and Learning Service via the National Patient Safety Agency.
• RESULTS: There were 684 reports related to insulin and 84 incidents related to oral glucose-lowering agents. The most common error category with both types of drug therapy was wrong or unclear dose: 173 reports for insulin, including one death, and 20 reports for oral therapy.
• CONCLUSIONS: Residents with diabetes in care homes are potentially at risk of harm from adverse drug events pertaining to insulin and oral glucose-lowering agents.
• Because of likely under-reporting, our data most likely represent only a fraction of events.

Setting the Scene
• How common is diabetes in older populations?
• Any diagnostic issues?
• What is this thing we call ‘Frailty’?
• What are we doing in care home diabetes?
• IDF Global Guidance – why are these recommendations different?

Age and Gender of Patients with Types 1 and 2 Diabetes in England and Wales
Type 2 diabetes prevalence Type 1 diabetes prevalence

Varying Presentation of Diabetes in Older People – may be missed or misinterpreted in community-based settings
Patient symptom
Patent sign profile
Lethargy Usually glucose >11 mmol/L
Increased micturition Disturbed sleep patterns, increased fall rate, dehydration, incontinence
Visual impairment Increased fall rate, poor mobility
Erectile impotence Presence of vascular/ischaemic heart disease
Pain Limb pain, decreased threshold
Cognitive impairment Memory disorder, psychomotor slowing
Depressive symptoms Irritability and intolerance
Adapted from: Sinclair AJ. Early Management of type 2 diabetes. In: Sinclair AJ (ed), Diabetes in Old Age, 3rd Edition, 2009, John Wiley & Sons, Chichester

Percentage of Patients Initiating Anti-Hyperglycemic Treatment Within a Specified Time Period – by age group Zhang Q, Davies MJ, Sinclair AJ et al, 2011
47%
37%
33%29%
56%
44%
38%
33%
65%
55%
46%
40%
0%
10%
20%
30%
40%
50%
60%
70%
30-45 45-65 65-75 >75
Age Groups
180 days 1 year 2 years
Less than 50% of those older than 65 years initiate treatment within two year after initial diabetes diagnosis

What is this thing we call ‘Frailty’?

Increasing Effect of Diabetes on Disability Levels Study of Osteoporotic Fractures Gregg E et al, 2002
• Data from 8,344 women aged ≥ 65y – 6.3% with diabetes
• Questionnaire/physical examination
• 12y follow-up
0
2
4
6
8
10
12
Walking 1/4
mile
Heavy
housework
Climbing 10
steps
Prepare
meals
Shopping Any Task
Yearly incid
ence (
%)
No Diabetes
Diabetes
(Gregg et al., Diabetes Care, 2002)
Figure 3: Yearly incidence of inability to do physical and household tasks among women
> 65 years with and without diabetes: Study of Osteoporotic Fractures
Results Diabetes was associated with 42% increased risk of any incident disability and a 53-98% increased risk for specific tasks
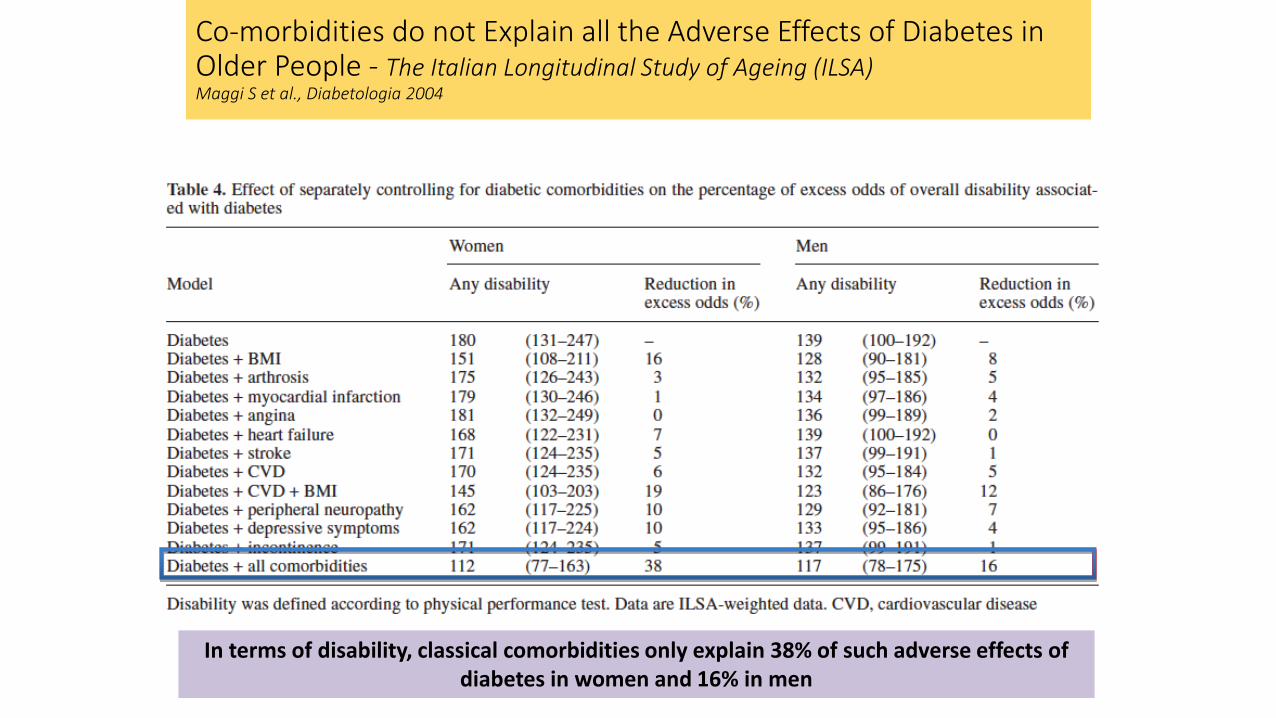
In terms of disability, classical comorbidities only explain 38% of such adverse effects of diabetes in women and 16% in men
Co-morbidities do not Explain all the Adverse Effects of Diabetes in Older People - The Italian Longitudinal Study of Ageing (ILSA) Maggi S et al., Diabetologia 2004
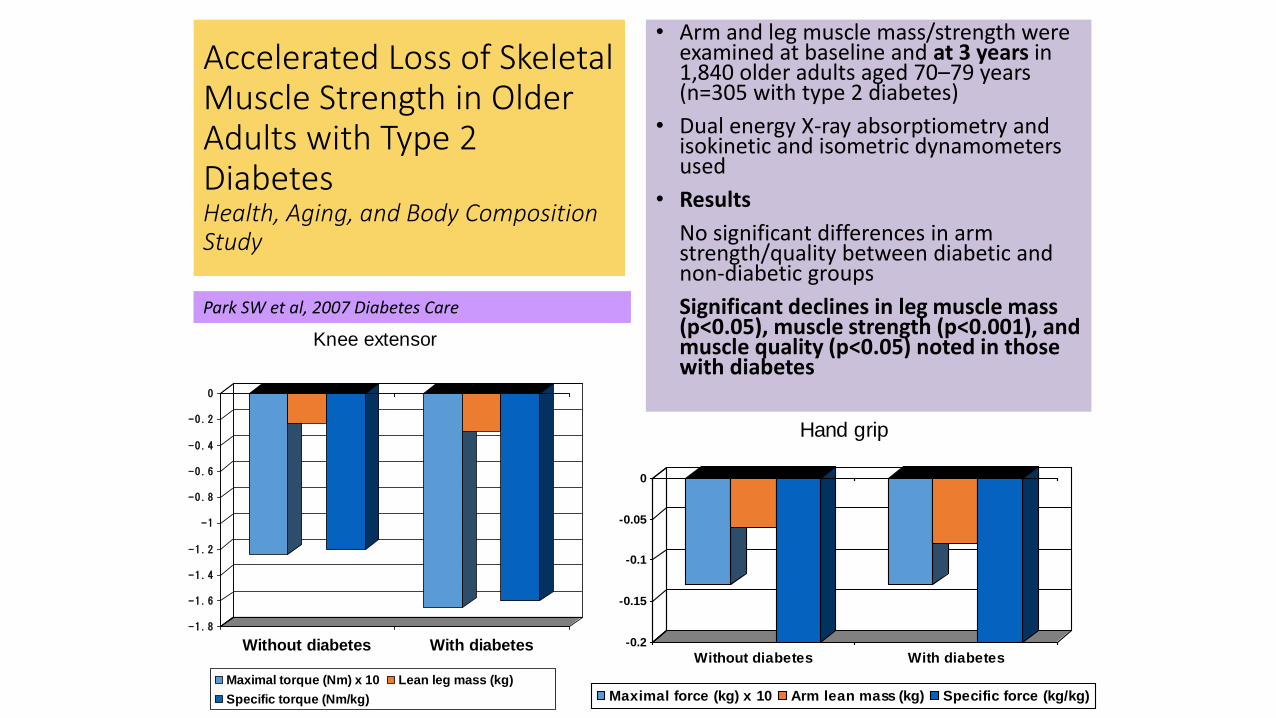
Accelerated Loss of Skeletal Muscle Strength in Older Adults with Type 2 Diabetes Health, Aging, and Body Composition Study
• Arm and leg muscle mass/strength were examined at baseline and at 3 years in 1,840 older adults aged 70–79 years (n=305 with type 2 diabetes)
• Dual energy X-ray absorptiometry and isokinetic and isometric dynamometers used
• Results
No significant differences in arm strength/quality between diabetic and non-diabetic groups
Significant declines in leg muscle mass (p<0.05), muscle strength (p<0.001), and muscle quality (p<0.05) noted in those with diabetes
-1.8
-1.6
-1.4
-1.2
-1
-0.8
-0.6
-0.4
-0.2
0
Without diabetes With diabetes
Knee extensor
Maximal torque (Nm) x 10 Lean leg mass (kg)
Specific torque (Nm/kg)
-0.2
-0.15
-0.1
-0.05
0
Without diabetes With diabetes
Hand grip
Maximal force (kg) x 10 Arm lean mass (kg) Specific force (kg/kg)
Park SW et al, 2007 Diabetes Care
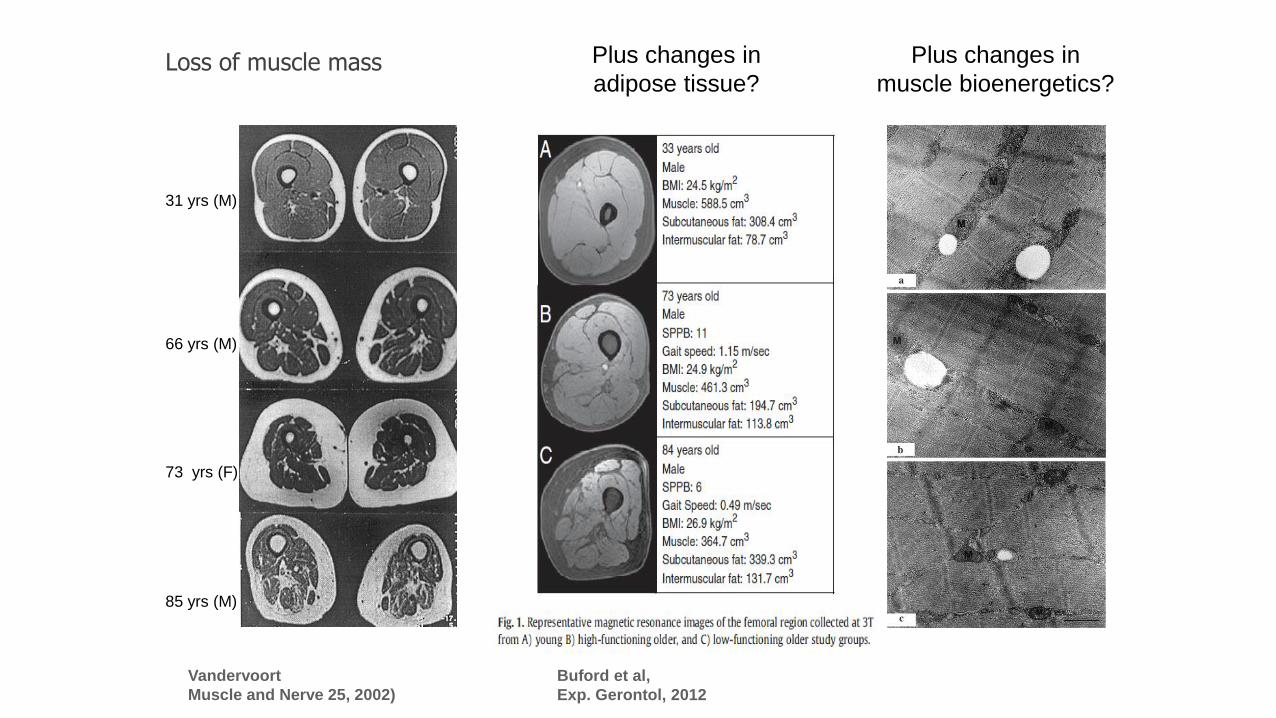
Loss of muscle mass
Vandervoort
Muscle and Nerve 25, 2002)
31 yrs (M)
66 yrs (M)
73 yrs (F)
85 yrs (M)
Buford et al,
Exp. Gerontol, 2012
Plus changes in
adipose tissue?
Plus changes in
muscle bioenergetics?

With permission from H. Bergmann
Comorbidity decreases its predictive accuracy as the age of the population increases
Co-morbidities, frailty and mortality

Frailty – a definition
• Frailty is a multidimensional geriatric syndrome characterized by increased vulnerability to stressors as a result of reduced capacity of different physiological systems.
• Implications
Associated with an increased risk of adverse health-related outcomes in older persons, including falls, disability, hospitalizations and mortality; also associated with biological abnormalities (e.g. biomarkers of inflammation) regardless of the definition used to assess frailty.

Weight loss
Low grip strength
Exhaustion Low
physical activity
Low gait speed
Score 0–1 = Not frail 2 = Pre-frailty 3–5 = Frailty
Frailty is multisystem impairment associated with increased vulnerability to stressors
Fried L et al J Gerontol A Biol Sci 2001
The Frailty Syndrome Approach to Case Finding in Older People

Baseline Frailty Status Predicting Adverse Outcomes Clinically Associated with Frailty
Hazard ratios* Estimated over 3 Years
Frail
Incident fall 1.29
Worsening mobility 1.50
Worsening ADL disability
1.98
First hospitalisations 1.29
Death 2.24
* Covariate adjusted, p≤0.05
Fried et al, 2001

3-Years Mortality in Older Type 2 DM Patients According to Frailty Status and Disease Data from the Toledo Study of Healthy Aging
P<0.01
P=0.09
P<0.01
P=0.09
FOLLOW-UP (WEEKS) FOLLOW-UP (WEEKS)
Adjusted by age, sex, and comorbidity
≤ 5 yrs since the diagnosis of DM > 5 yrs since the diagnosis of DM SU
RV
IVA
L
SUR
VIV
AL
Personal communication from Professor Leo Rodriguez Manas (Toledo study).

Key objectives: • Effectiveness of multimodal intervention in
subjects aged ≥70 years with T2D
• Effectiveness of an intervention on healthcare expenditure, hypoglycaemic events, incidence of hospital admission or carer burden
• Mechanisms underlying the effect of the intervention (e.g., changes in body composition)
• Efficacy of new therapeutic devices and new ways to measure changes in QoL (substudies)
A randomized clinical trial to evaluate the effectiveness of a multi-modal intervention in older people with Type 2 diabetes on Frailty and Qualify of Life: Phase IIb
Results will be reported in Month 48
The MID-Frail Study

Explaining why Diabetes Care for Residents is Challenging
• Albert Einstein said that if you can't explain something in a simple way then you don't know the subject well enough
• Well let's see:
• Residents of nursing homes are often frail, have multiple medical problems, poly-pharmacy, complex illness, often immobile, cognitively impaired and incontinent, lowered quality of life - so how do I explain this simply? The answer is that when a resident enters a nursing home they are entering a high risk environment where: - there is little medical supervision, no access to specialists, cared for by unqualified and uneducated staff, in essence an end of life care scenario and are likely to die within 24 months usually - is that simple enough?

The 99% rule!
• 99% of all the species ever lived are extinct
• 99% of PowerPoint presentations you never remember (including this one probably! )
• 99% of nursing home residents are dead within 3 years
• (sady) 99% of UK diabetologists never take an active interest in care home diabetes……..

Not certain why this is? • Diabetes is a
highly prevalent in care homes
• Diabetes is often a complicated management problem
• Diabetes increases the risk of hospital admission 6-fold

England-wide Care Home Diabetes Audit
Developing The Audit
• This work stemmed from the recommendations of “Good Clinical Practice Guidelines For Care Home Residents With Diabetes” 2010
• The Audit piloted in Beds & Herts
• Collaboration between 9 key partner organisations
• Over 2000 responses were received from around 9000 homes
Available at: www.diabetesfrail.org

Raising Standards of Diabetes Care -CQC diabetes guidance
• Guidelines to improve the quality of care for people with diabetes living in care homes.
• Series of indicators to help inspectors assess whether a service is meeting needs.
• An assessment and support framework to protect dignity and rights.

CQC Elements of Good Practice – Diabetes 2015
7. What are the elements of good diabetes care?
Good diabetes care begins with a diabetes policy. A good diabetes policy describes and requires the four elements set out below.
1. Diabetes screening on admission that
is recorded and audited.
This can reduce the number of GP call-outs and hospital admissions linked to undiagnosed diabetes and associated complications.
1. Availability of a fully-stocked and
maintained hypoglycaemia kit.
This can reduce ambulance call-outs and hospital admissions due to hypoglycaemia.
1. A risk-calculation and assessment tool
for diabetes foot disease.
Use of such a tool by suitably trained staff can reduce unnecessary amputations.
1. Access to good quality diabetes
education and training for care home
staff.
Good training can lead to fewer GP call-outs and hospital admissions for hypoglycaemia, infections, and other common medical problems associated with diabetes.
Good leadership and management in relation to the care of diabetes includes regular audit and assessment of these elements in practice.
Appendix 1 below sets out a flow chart for assessing diabetes care in care homes.

2015 CQC Guidance for Inspectors
Summary and Optimism for the Future
• Growing recognition of the unique characteristics of the diabetes state in ageing populations
• The emergence of frailty as a complication of diabetes
• Making progress with diabetes care in care homes – at last!
• New IDF Guidelines that support categorisation based on co-morbidity and functional/dependency level
• Re-emphasis of the need for comprehensive assessment and the delivery of ‘compassionate’ approach by health and social care professionals

Influencing Stakeholders to Enhance Diabetes Care – 3 Key Themes • Hospital Avoidance Measures
• Changing Clinical Behaviour
• Raising Standards of Diabetes Care

Octabaix study