enterprise | interest nothing to declare · pancreatoduodenectomy (2012) liver resection for...
TRANSCRIPT

Enterprise | Interest
Nothing to declare

IMMUNOHISTOCHEMICAL EVALUATION OF THE PHOSPHORYLATED AKT-1 EXPRESSION IN WELL-DIFFERENTIATED PANCREATIC NEUROENDOCRINE TUMORS
Vera Delektorskaya, Olesya Solovieva, Galina Chemeris, Yuriy Patyutko
N.N. Blokhin National Medical Research Center of Oncology of the Ministry of Health of the Russian FederationMoscow, Russia

AKT
The PI3K / AKT / mTOR Signaling Pathway
3
SSTR 1-5
PI3K
S6K1
FOXO 1,3
Cell cycle progressioneIF4ES6Protein synthesis
P
FOXO 1,3
AKT
a serine/threonine protein kinase (protein kinase B):
a multifunctional kinase ;
an important regulator of cellproliferation and survival.
GrowthFactors
Thr 308
P
P
Ser 473
Motility
INTRODUCTION
mTORC2 mTORC1
p21cip1
p27kip1
PDK1PIP3 PIP2 PTEN
AKT1
S Falletta et al. mTOR inhibitors response andmTOR pathway in pancreatic neuroendocrinetumors . Endocr Relat Cancer. 2016; 23(11):883-91.
one of the most frequentlyactivated protein kinases;
promotes tumor growth,progression and spreading;
an attractive target for therapy;
a promising predictive markerof response to mTOR inhibitors.
In PNET
HL Robbins, A Hague. The PI3K/Akt Pathway in Tumors of endocrine Tissues. Front. Endocrinol. 2016.6:188
TSC2
RaptorRictor
4EBP

4
The aim of the study was to investigate
phosphorylated from of AKT1 kinase (p-AKT1)
immunoexpression and clinical significance
in well-differentiated pancreatic neuroendocrine tumors (PNETs)
OBJECTIVEOBJECTIVE

5
Invasion/Recurrence :
Adjacent tissue/capsule – 23 (44.2%)Lymphovascular/perineural – 25 (48.1%) Recurrence – 3 (5.8%)
Tumor size:
Mean – 5.2 cm (0.5 - 18 cm)
Metastasis:
Lymph node – 15 (28.8%) Distant during follow-up – 19 (36.5%)
p=0.09
p=0.001
Staging of studied NETsStaging of studied NETs at initial diagnosis
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Grading of studied primary PNETs
G2
G3
I
II
III
IV
G1
Ove
rall
Surv
ivin
gD
ise
ase
fre
e S
urv
ivin
g
Age distribution:
Range – 24– 77 yearsMedian age – 53.4±1.4
Gender distribution:
Male – 23 (44.2%) Female – 29 (55.8%) (M:F – 0.8)
Functional status:
Functional – 7 (13.5%) Nonfunctional – 45 (86.5%)
CLINICAL & PATHOLOGICAL CHARACTERISTICS

6
RESULTS
Pathology & Imunohistochemistry of PNETs. WHO 2017
CgAH&E
SynSSTR-2A
RESULTS
Ki-67 - 1%
NET Grade 1Primary – 14 (26.9%)Liver mts – 3 (21.4%)
NET Grade 2Primary – 30 (57.7%)Liver mts – 15 (50.0%)
NET Grade 3Primary – 8 (15.4%)Liver mts – 4 (50.0%)
Ki-67 - 8%
Ki-67 - 30%
n 4
n 1
n 5
Primary PNETs G1-G3 – 52Liver metastases synchronous – 22Liver metastases metachronous – 5
Ki-67 Index and Grade progression in liver metastases
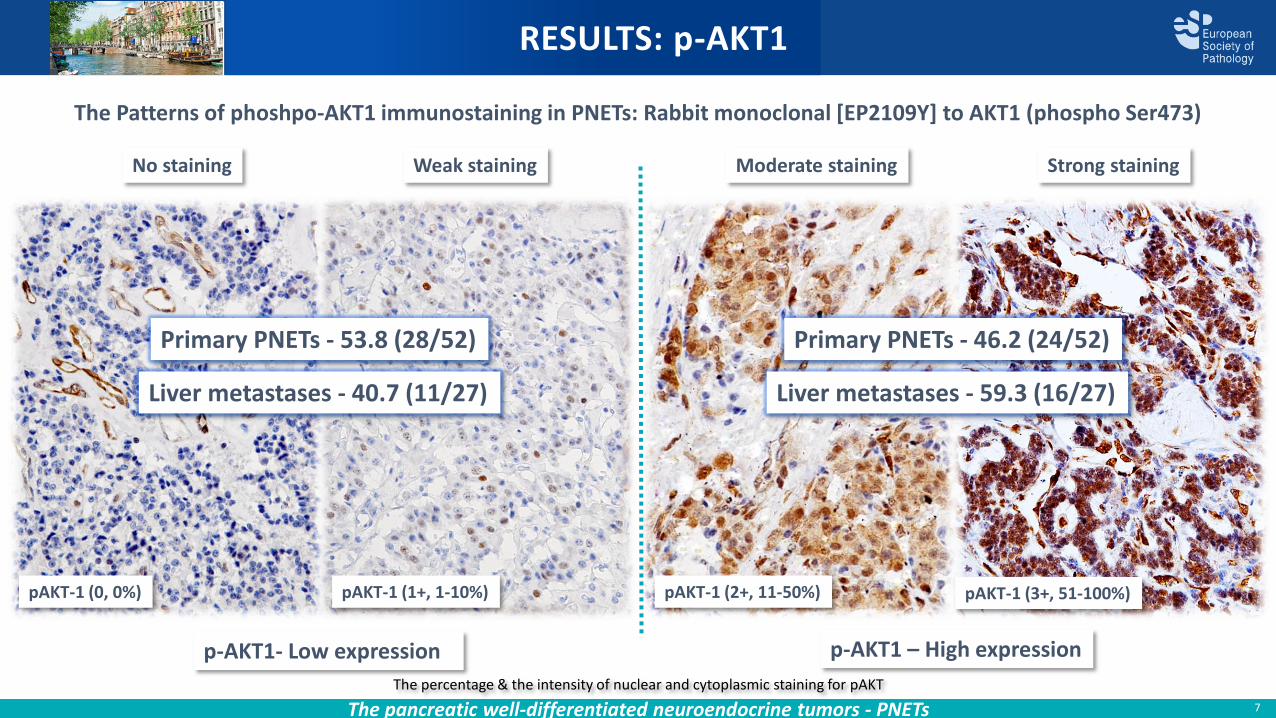
RESULTS: p-AKT1
The Patterns of phoshpo-AKT1 immunostaining in PNETs: Rabbit monoclonal [EP2109Y] to AKT1 (phospho Ser473)
RESULTS: p-AKT1
p-AKT1- Low expression p-AKT1 – High expression
Primary PNETs - 46.2 (24/52)Primary PNETs - 53.8 (28/52)
pAKT-1 (0, 0%) pAKT-1 (1+, 1-10%)
No staining Weak staining Moderate staining Strong staining
pAKT-1 (3+, 51-100%)pAKT-1 (2+, 11-50%)
The pancreatic well-differentiated neuroendocrine tumors - PNETs 7
The percentage & the intensity of nuclear and cytoplasmic staining for pAKT
Liver metastases - 59.3 (16/27)Liver metastases - 40.7 (11/27)

Parameters G1-NETs G2-NETs
n 14 30
Ki-67 index
< 3% 3-20%
Angioinvasion
4 15
Liver mts 3 12
SSTR-2A positive
8 25
p-AKT1High levels
3; 21.4% 14; 46.7%
p-AKT1Low levels
11; 78.6% 15; 53.3%
8
RESULTS: p-AKT1
Expression of p-AKT1 in WHO Grade 1/Grade 2 PNETs (primary & metastatic)
21.4% (3/14)
RESULTS: p-AKT1
p-AKT1 (2+) in NET G1, Ki-67 – 2%
PNETs Grade 1
46.7% (14/30)
p-AKT1 (3+) in NET G2, Ki-67 - 5%
PNETs Grade 2
Liver metastases Grade 1/2
46.7% (7/15)
p-AKT1 (3+) in NET G2, Ki-67 – 8% p-AKT1 (3+) in NET G2, Ki-67 – 15%

Parameters G3-NETs Pancreas
G3-NETs Liver
n 8 12
Ki-67 index
23% -35%
25% - 45%
SSTR-2A positive
7 10
p-AKT1High levels
7; 87.5% 9; 75.0%
p-AKT1Low levels
1; 12.5% 3; 25.0%
9
RESULTS: p-AKT1
Expression of p-AKT1 in WHO Grade 3 PNETs (primary & metastatic)
RESULTS: p-AKT1
pAKT-1 (3+) in NET G3, Ki-67 - 26%
87.5% (7/8)
pAKT-1 (3+) in NET G3, Ki-67 – 35%
Primary PNETs Liver Metastases
75.0% (9/12)
pAKT-1 (3+) in NET G3, Ki-67 - 40%

RESULTS: p-AKT1
Matched pair analysis: Expression of p-AKT1 in primary PNET and corresponding liver metastases
RESULTS: p-AKT1
10
pAKT-1 (2+) pAKT-1 (2+) pAKT-1 (3+)
Primary PNET G2 Ki-67 - 30%Liver metastasis (metachronous)
Grade 3in 3 years
Grade 2
Liver metastasis (synchronous)Ki-67 - 4%
Pancreatoduodenectomy (2012) Liver resection for metastases (2012) Liver resection for metastases (2015)
Ki-67 - 9%
p-AKT1 in metastases as compared to primary
≈ 15 (55.6%) | ↑ 9 (33.3%) |↓ 3 (11.1%)

11
RESULTS: pAKT-1
Correlation of pAKT-1 expression in PNETs to clinicopathological parameters and survival
p=0.05p=0.11
Time, months
RESULTS: p-AKT1
Overall survival Disease free survival
Correlation to
• Grade (0.004), Ki-67 Index (p=0.029), perineural invasion (0.031), and pTNM stage (p=0.0008)
• Disease free survival, % (Kaplan-Meier) according to p-AKT1 expression in 52 cases of PNETs
No Correlation to
• Age, gender, angioinvasion, tumor size, lymph node & distant metastasis (p=0.09), and SSTR 2A status
• Overall survival, % (Kaplan-Meier) according to p-AKT1 expression in 52 cases of PNETs
LowHigh
LowHigh
p-AKT1 expression
p-AKT1 expression

12
CONCLUSION
PHOSPHORYLATED AKT1 EXPRESSION IN PNETs
P-AKT1 is observed in different groups of PNET patients with the highestnuclear expression levels in well-differentiated primary and metastaticG3-NETs;
The association of p-AKT1 to enhanced aggressiveness and histologicalgrade suggests its potential value as prognostic and predictive biomarkerand target for therapy in PNETs.
CONCLUSION

13
29th European Congress of pathology
N.N. Blokhin National Medical Research Center of Oncology of the Ministry of Health of the Russian [email protected]