environmental decontamination
TRANSCRIPT

The presentation is solely meant for Academic purpose
AIFIC '13

Environmental Decontamination:
Paradigms Redefined

Disclosures- nil

800 B.C – Homer described the burning of Sulphur
in the house
4th century A.D. – Susruta used sulphur to clean
rooms for surgery
Mercury, copper, alkalis acids all were used for
‘Purifying’
429 B.C Hippocrates recommended fumigation by
burning odoriferous herbs to control an epidemic
History

Advocated pure air, pure water,
efficient drainage, cleanliness and
light as the cornerstones of good
health and prevention of mortality
1850’s- Crimean war
Hospital
Project
Engineering
Housekeepi
ng
Infection
control
AIFIC '13

It is important to maintain a healthy
environment
What best infection control practices
are available?
How to use it cost effectively to
protect patients and health care
workers from infectious hazards?
The hospital environment

Chain of infection

Reservoirs
AIR
WATER
SURFACE
ENVIRONMENT
HCW

Found in 7-37% environmental samples
More common if patients have diarrhoea
Nurses gowns contaminated
8% of cultures positive even after terminal
cleaning
Boyce 1994, Montecalvo 1995, Boyce 1995
VRE & environment

Burns unit – attack rate 75%
- 33 of 145 environmental swabs positive
Hydrotherapy facilities contaminated
Surgical units without MRSA problem
-1 of 36 samples positive
Crossley 1979
MRSA & environment

25 rooms of MRSA positive patients
53.6% surface samples positive
28% of air samples
Molecular typing PFGE
70% of patient and environmental swabs
indistinguishable
Sexton et al JHI 2006
MRSA & environment

50 ICU rooms occupied with patients
having MDR AB
9.8% (47 of 479) of the environmental
surfaces were contaminated with MDR-AB.
Supply cart handles were the most
frequently contaminated surface (20%),
room floors (16%), infusion pumps (14%),
ventilator touch pads (11.4%) and bed rails
(10.2%).
A. baumanii & environment
Am J Infect Control 2011;39:711-715

Vancomycin-resistant enterococci (VRE),
Clostridium difficile*, and multidrug-
resistant gram-negative bacteria (MDR-
GNB) are increasing
Hence increasing attention being paid to
the role of high-touch environmental
surfaces in transmission
MDRO’s in environment
*Am J Epidemiol. 1988 Jun;127(6):1289-
Am J Infect Control 2010;38:S25-33

Do environmental surfaces play a role in
initiating infection?
OR
Merely reflect the presence of a source
patient contaminating his surroundings?
Environmental surfaces

1
• Source patient (occupant of room or reusable eqpt)
2 • Environmental
surface
3 • Subsequent patient
1 • Source patient
2
• Environmental surface
3 • Hands of HCW
4 • Subsequent patient
Primary role Secondary role
Environmental surfaces
AIFIC '13

Outbreak of Klebsiella pneumoniae in
NICU- 3 cases
Investigations included- handwashing
compliance monitoring, disinfectant usage,
focussed cleaning
Swabs from incubators, ventilator tops,
mobile phone of doctors to look for specific
pathogen
Klebsiella in environment

Klebsiella pneumoniae with similar
antibiogram was isolated from the top of
ventilator.
Increased emphasis of focused cleaning in
and around the patients
Outbreak curtailed
Klebsiella in environment

Dry surface – Gram positive cocci, fungi
Wet surface – Gram negative bacilli
Cleaning with soap and water or detergent
or disinfectant
Cleaning and disinfection of surfaces

Manual cleaning and then application of
disinfectant or detergent/disinfectant
New disinfectants with greater potency and
shorter contact times
Standard environmental cleaning methods

Tertiary care 8 wards
Phenolic disinfection vs detergent
6 months, random selection of wards
Users blind to product used
No difference in HAI rates
Danfoth JHI 1987
Detergent or disinfectant? Study 1

ICU floors cleaned 3X daily
6 months detergent
6 months disinfectant
Bedside tables, bed frames etc cleaned with
disinfectant
No difference in HAI rates
Dashner 1980
Detergent or disinfectant? Study 2

1960’s Vesley and Micaelsen – detergents
can achieve microbial reduction equivalent
to disinfectants*
Maki et al- no change in infection rates in
new and old hospital and new environment
was contaminated to old rates in 6-12
months
Detergent or disinfectant?
*Appl Environ Microbiol 1987:53;1042-1045
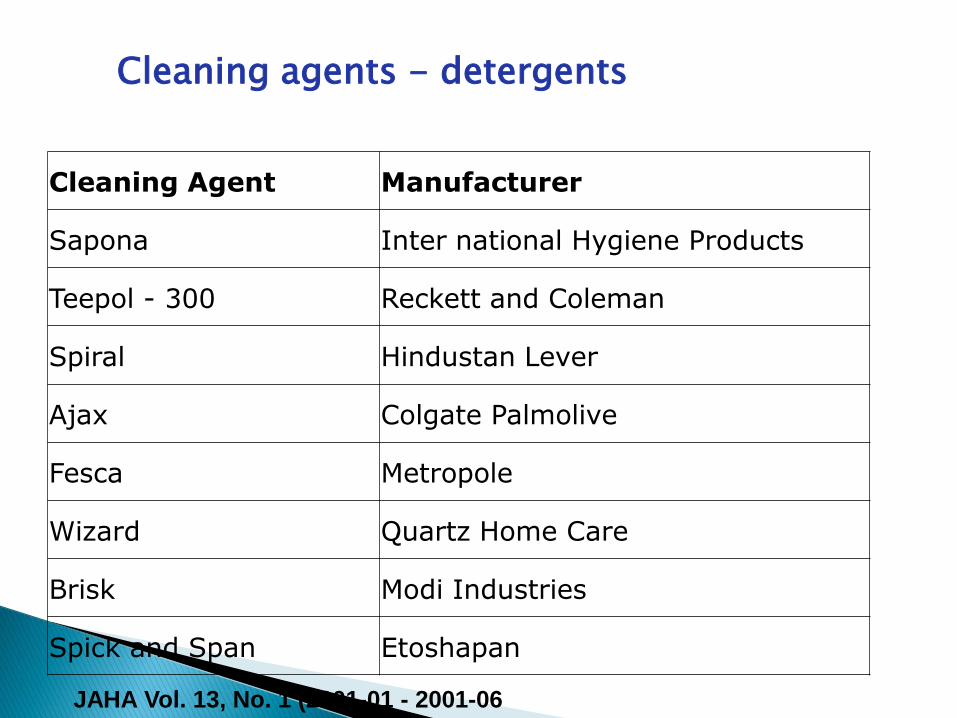
Cleaning Agent Manufacturer
Sapona Inter national Hygiene Products
Teepol - 300 Reckett and Coleman
Spiral Hindustan Lever
Ajax Colgate Palmolive
Fesca Metropole
Wizard Quartz Home Care
Brisk Modi Industries
Spick and Span Etoshapan
Cleaning agents - detergents
JAHA Vol. 13, No. 1 (2001-01 - 2001-06

Detergent Disinfectants
Polysan - (Akyl phenoxy poly active ingredient ethoxy - ethanol, iodine)
Polyphan Pvt. Ltd
Germinol Etosha pan
Lamp phenyl Bengal chemicals
Trishul phenyl Ampey Lean
Phoenix Metro pole
Dettol-H - (Ben 2 alkonim chlorid sol. 1. P40 1v/v disodeim edeati)
Rickett and Colman
Bacilloid Special _ ( D. hydroxy - 2,5, Dioxyhexene glutaaldehydi,
Raman Pvt. Ltd de n 201 konuim chloride, caxosguanidiam ehlondi)
Detergent-disinfectant
JAHA Vol. 13, No. 1 (2001-01 - 2001-06

Properties Phenolic Quaternary Iodophor peroxides
Effectiveness
against S. aureus Fair to good Good Good good
M tuberculosis Fair to good Good Good good
Effect on organic
matter Good Good Fair good
Skin irritation
properites Harsh Mild Mild mild
Odour
Strong to
mild Mild Mild mild
pH of use
soulution
Alkaline(pH9.
10)
Neutral or
alkaline(pH7.10)
Acidic(pH3.
6)
Soil removal
property Poor to good Good Fair fair
Corrosion to floor
Surface
Safe at
correct
dilutions Safe Safe safe
Properties of disinfectants
JAHA Vol. 13, No. 1 (2001-01 - 2001-06

Cost
Area to be disinfected- steel OT –
lysoformin
Vinyl floors- QAC (benzalkonium chloride)
Room occupied with patient with
Clostridium difficile – Hypochlorite
solutions
Choice of disinfectant

Operation theatres , BMT units , ICU –
disinfectant after cleaning
Wards – disinfectant/ detergent
General areas- detergent
Choice of disinfectant / detergent

First clean with detergent and surfactant to
remove organic matter, salt and visible
soils.
The physical action of scrubbing and
rinsing removes large numbers of
microorganisms
Factors affecting Disinfection of surfaces

Potential for direct patient contact
Degree and frequency of hand contact
Potential contamination of surfaces with
body fluids and environmental
contamination
Choice of disinfectant – QAC, hypochlorites,
hydrogen peroxides, lysoformin etc
Strategies for Cleaning and disinfection of surfaces

Surfaces with minimal hand-contact –
ceiling, floor
Areas with frequent hand-contact – high
touch surfaces (door knobs, bed rails, wall
around toilet, light switches, edges of
curtains) require more cleaning/
disinfection
Housekeeping surfaces

Solutions to be replaced frequently
Two bucket system to be used
Mop heads to be changed at each shift
Mops to be dried before use
Detergent / disinfectant solutions can
support Gram negative bacteria
(pseudomonas) if stored for a long time
Cleaning solutions and tools – a source of pathogens

“Nontouch disinfection” (NTD) methods
Microcondensation hydrogen peroxide
vapor
hydrogen peroxide dry mist system
gaseous ozone
alcohol/quaternary ammonium power
sanitizing system
ultraviolet light room decontamination
Newer Strategies for Terminal Room Decontamination

Both methods appear highly efficacious in
inactivating the microbial bioburden
present on surfaces
Both remove much of the variance inherent
in human cleaning activity via a high degree
of automation and feedback loops for
verification that contact or irradiation times
are adequate
HP Vapour & UVGI

Patients admitted to rooms using HPV were
64% less likely to acquire any MDRO (esp
VRE).
The proportion of rooms environmentally
contaminated with MDROs was reduced
significantly on the HPV units (relative risk,
0.65, P = .03), but not on non-HPV units.
HPV efficacy v/s standard disinfectant
Passaretti et al .Clin Infect Dis. 2013:56:27-35.

An automated mobile UV light unit that
emits UV-C light was placed in 25 patient
rooms after patient discharge and operated
The mobile UV-C light unit significantly
reduced aerobic colony counts and C.
difficile spores on contaminated surfaces in
patient rooms
UV light disinfection
Infect Control Hosp Epidemiol2011 Aug;32(8):737-42.

Single room
Use of gloves and gown when in contact
with patient / patient environment
Donning PPE at room entry and discarding
before exiting room
Duration of precautions is not known
Contact precautions for MDRO, C. difficile
http://www.cdc.gov/ncidod/dhqp/pdf/isolation2007.pdf

Previous room occupancy by patients with
VRE or MRSA increases risk for acquiring
these multidrug-resistant organisms in
patients subsequently admitted to the same
rooms.
The need for terminal cleaning and disinfection
Clin Infect Dis. 2008;46:678-685.
Arch Intern Med. 2003;163:1905-1912
Arch Intern Med. 2006;166:1945-1951
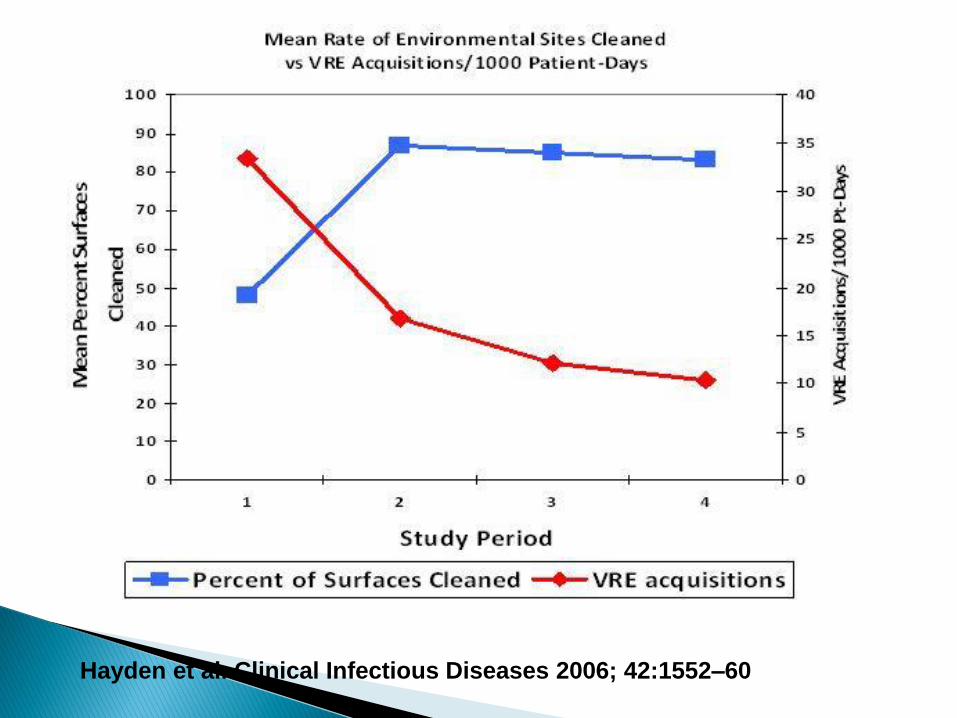
Hayden et al. Clinical Infectious Diseases 2006; 42:1552–60

Carpets to be avoided (especially in ICU, OR,
BMT units)
If flowers are present, the water should be
changed frequently and these should be
handled by staff not having patient contact
Flowers (fresh and dried ) can harbour
Aspergillus spores
Other factors

Have housekeeping managers conduct visual
inspection (not reliable)
Mark high touch surfaces with a fluorescent solution
and check later to determine whether the mark has
been removed by housekeepers during room
cleaning
Count aerobic colonies of specimens obtained from
high touch surfaces
Use adenosine triphosphate (ATP) bioluminescence
assay to assess the cleanliness of surfaces
Monitoring Cleaning and Disinfecting Practices

Terminal cleaning is often suboptimal.
Only about 50% of the surfaces in patient
rooms that should be cleaned are wiped by
housekeepers.
This phenomenon has been documented in
different types of hospitals and intensive
care units as well as on general medical or
surgical wards.
Monitoring cleaning practices
Clin Infect Dis. 2006;42:385-388, Infect Control Hosp Epidemiol. 2008;29:1-7
Infect Control Hosp Epidemiol. 2008;29:593-599

Providing housekeepers with feedback
about the results of such monitoring and
educating them about the importance of
their activities has led to significant
improvements in the proportion of surfaces
that are cleaned by housekeepers
Feedback & Education
Infect Control Hosp Epidemiol. 2009;30:678

Surgical site exposes sterile tissue to microorganisms from :
respiratory droplets and nuclei,
skin scales carried on air currents,
direct contact with the surgical team's skin,
and contaminated fomites.
The route with the most significant potential for
iatrogenic bacterial transfer is direct physical
contact.
Air
Dermatol Surg. 2011 Dec;37(12):1709-20
Talking – 3000 droplet nuclei
Sneezing – 40,000 droplet nuclei
Sweeping
Dry plants
Staphylococci, Streptococci, Fungal spores
Microbial contamination of air


Filtration
Air changes
Pressure differentials
Ultraviolet installations
Laminar air flow
Strategies to reduce air contamination

Isolation room BMT unit Operating room
Air pressure Negative Positive Positive
Room air changes
≥12 ≥ 12 ≥ 20
Sealed Yes Yes yes
Room leakage (0.1 cfm/ft2 ) (0.1 cfm/ft2 )
(0.1 cfm/ft2 )
Directed airflow Clean- to- dirty (HCW clean)
Clean- to- dirty (patient clean)
Displacement flow in surgical site critical
Filtration supply 90% 99.97% HEPA @0.3um
90%
Special ventilation areas

Pressurisation
Air changes
Filtration – non microbiologic method –
particle count
Verification of ventilation parameters

Non viable airborne particles detected by
particle counter, optical or laser.
Particle size >0.5 um used for assessing
clean room
Air – particle count

Classification based on HEPA filtered (99.7%
efficient at 0.3 um diameter particles)
operating room or BMT room with no
people should be capable of class 1000
clean room status
(there are <1000 particles per cubic foot
>0.5 um in diameter)
Clean room classification - ISO

Clean room classification - ISO
A comparison of air counts and
environmental contamination rates was
made with the Inov8 units on and off. The
Inov8 unit produced an overall reduction in
both air sample and settle plate counts in
each setting (P < 0.001)
? Effect on specific pathogens
? Safety issues for patients and HCW
Hydroxyl radical air disinfection system
J Hosp Infect. 2011:78;194-99

Ozone fumigation successfully controlled and
eradicated multidrug-resistant Acinetobacter
baumanii from an intensive care unit
Environmental samples positivity decreased
from 31% to 7 % following ozone fumigation
Ozone
R Stümpfle et al Critical Care 2010, 14(Suppl 1):P67

Respiratory therapy equipment
Fiberoptic endoscopes
Faucet shower heads with Pseudomonas
Shower heads and Legionellosis
Faucet aerators & Stenotrophomonas
maltophilia
Water and HAI

Hot water supplies
Hydrotherapy pools and tanks
Potable water
Sinks
Water baths
Dialysis water
Toilets
Dental unit water systems
Water reservoirs

Contamination by Gram negative bacteria
Monthly testing for bacterial counts and
endotoxin levels
Dialysis fluid

Hemodialysis fluid
Method Maximum heterotrophs (cfu/ml)
Max. endotoxin level (EU/ml)
Product water Plate count 500ul on TSA
200 2
Dialysate LAL gel clot assay
200 2
AAMI standards for dialysis fluid
ANSI/AAMI RD52:2004 Dialysate for hemodialysis

Environmental decontamination
Earlier thoughts
• Fumigation with formalin- the final solution to a clean environment
Current concepts
• Focused cleaning of high contact areas
• Isolation of patients with MDR
• Terminal cleaning
• Vapour methods
AIFIC '13
Before 1970’s in US, regular scheduled
culturing of air and environmental surfaces
was done
By 1970, CDC advised discontinuation of
routine environmental surveillance as not
association of HAI with levels of
environmental contamination was noted
Microbiologic sampling of environment

Used currently for:
Research (potential reservoirs on surface,
survival of pathogens, sources of
contamination)
As part of epidemiologic investigation
Specific QA purposes
Microbiologic sampling of environment – current concepts

Survival of agent (Clostridium spores persist
for years, Staphylococcus for months)
Interference from particulates- dust, heavy
metals
Adherence of microorganism
Methods of detection
Variables affecting sampling

Sampling devices:
Wipe
Swab
Agar Contact plate
Microvacuum sampling
HEPA vacuum collection sock
Microbiologic sampling of Environmental surfaces

Use of neutralisers for residual
disinfectants
Media
Microbiologic sampling of Environmental surfaces

Results:
Have we found what we were looking for –
the target organism?
No standard guidelines for validation of
surveillance cultures
Microbiologic sampling of Environmental surfaces

ATP technology for real time analysis of
surfaces suspected of being contaminated
Bioluminescent material attached to protein
or ATP from living cells.
Done as a quality audit
Environmental surfaces

2. For research purposes – for e.g to
compare HAI rates in old and new facility
before and after occupation
Can provide new information regarding
spread of HAI
Environmental sampling - indications

3. To monitor a potentially hazardous
environmental condition, confirm the
presence of hazardous chemical or
biological agent, to validate the
successful abatement of the hazard
e.g. to monitor bioaerosols released from
health care equipment
Environmental sampling - indications

4. For quality assurance purposes to evaluate
the effects of a change in infection control
practices
Or to ensure that equipment or systems
perform according to specifications and
expected outcomes
Environmental sampling - indications
Air sampling for qualitative measurement of
microbial contamination during prolonged
construction to look for breach in
environmental control measures
Sampling before commissioning special
care areas (OR’s, BMT units)
Air sampling

Impingement in liquids
Impaction on solid surfaces (slit samplers)
Sedimentation (settle plates)
Filtration
Centrifugation
Electrostatic precipitation
Air Sampling Methods

Active air samplers are used, which collect a
known volume of air, blown on to a nutrient
medium by different techniques.
Active Air sampling
Slit samplers Petri samplers (sieve impaction)

Lack of uniform air quality standards
The microbial air contamination can be
measured by counting the number of cfu
per cubic metre (cfu/m3) of air.
Active Air sampling
C. Pasquarella*, O. Pitzurra† and A. Savino . The index of microbial air
contamination. Journal of Hospital Infection (2000) 46: 241–256
The schedule 1/1/1 was devised as a
standard
The Petri dish must be left open to the air
for 1 h, 1m above the floor, 1m from the
wall.
After 48 h incubation at 36°C the cfu are
counted. The number of cfu is the Index of
microbial air contaminatopn (IMA).
Passive air sampling -Settle plates
Fisher G, Fodré S, Nehéz M. Z Ges Hyg 1971; 17: 576–579

British bacteriological standard for
ultraclean operating room air of 10 cfu/m3
Surface contamination rate of 350
cfu/m2/h measured by means of settle
plates
Standards for colony counts
Friberg B, Friberg S, Burman LG. J Hosp Infect 1999; 42:
287–293.

IMA value Cfu/m3/h Performance locations
0-5 0-9 Very good OR- ultra clean, BMT
6-25 10-39 Good Conventional OR, dialysis unit, ICU
26-50 40-84 Fair Wards, day care
51-75 85-124 Poor
>76 >125 Very poor
Maximum acceptable risks of IMA
C. Pasquarella*, O. Pitzurra† and A. Savino . The index of microbial air
contamination. Journal of Hospital Infection (2000) 46: 241–256

Routine water testing is not indicated
Done to detect water borne pathogens
To determine quality of finished water in
the distribution systems
To be done in outbreak situations to initiate
appropriate infection control measures
Dialysis water to be tested monthly
Water sampling
Plate count
Membrane filtration
Potable water – coliform count
Water sampling

Environment can serve as reservoirs for
pathogens
Hand hygiene is paramount
Cleaning and disinfecting environmental
surfaces is mandatory
Surveillance cultures neither cost-effective
nor warranted.
Summary

Thank you
AIFIC '13