era eft enrollment form - availity · another advantage of the enrollment tool is the ability to...
TRANSCRIPT
Advanced Electronic Remittance Advice Enrollment
Rev. 09.15.2016.1
THIS TRANSMISSION IS A PROPRIETARY AND CONFIDENTIAL COMMUNICATION The documents accompanying this transmission may contain confidential health information that is legally privileged. This information is intended only for the use of the individuals or entities listed above. If you are not the intended recipient, you are hereby notified that any disclosure, copying, distribution, or action taken in reliance on the contents of these documents is strictly prohibited. If you have received this information in error, please notify the sender immediately and arrange for the return or destruction of these documents.
Overview
Availity® supports the exchange of electronic remittance advice (ERA) files for various payers in the ASC X12 835 format. Complete this enrollment form to receive 835 ERA files from payers through the Availity Web Portal. All information on the form is required unless noted otherwise.
The enrollment process establishes an electronic mailbox where Availity places ERA files received from payers. Availity
requires the provider’s tax ID to establish an ERA receiver mailbox and to parse remittance transactions from the various
payers. Availity will process your enrollment within three to five business days of receipt and will send you a confirmation
e-mail once enrollment is complete.
Instructions
1. Complete the form (type all responses). For information about a field on the form, refer to the field descriptions below. Note: If you are returning the form via e-mail, type the name of the person who would normally sign the form in the
Authorized Signature field.
2. Return the completed, signed form to Availity via:
E-mail Fax Mail
1. Click the Send Form button at the bottom of the form.
2. In the Send Email dialog box, click Default email application, and then click Continue. The form will be attached to an e-mail message that is automatically addressed to: [email protected]
3. Send the e-mail message.
317.580.0027 Availity, LLC P.O. Box 550857 Jacksonville, FL 32255-0857
Who do I contact if I have questions? If you have questions about your enrollment, contact Availity Client Services at 1.800.AVAILITY (282.4548).

Advanced Electronic Remittance Advice Enrollment
Rev. 09.15.2016.1
THIS TRANSMISSION IS A PROPRIETARY AND CONFIDENTIAL COMMUNICATION The documents accompanying this transmission may contain confidential health information that is legally privileged. This information is intended only for the use of the individuals or entities listed above. If you are not the intended recipient, you are hereby notified that any disclosure, copying, distribution, or action taken in reliance on the contents of these documents is strictly prohibited. If you have received this information in error, please notify the sender immediately and arrange for the return or destruction of these documents.
Field Descriptions
Section Field Description
PAYER INFORMATION
Payer Name The name of the payer sending/issuing the X12 835 files.
Payer ID The payer’s unique identifier.
RECEIVER INFORMATION
Who will receive your ERA files? The type of organization that will receive the X12 835 files: Provider, Clearinghouse, or Vendor.
Receiver Name The name of the organization that will receive the X12 835 files.
Availity Customer ID The receiving organization’s customer ID assigned by Availity. To determine your customer ID, click Who controls my access? at the top of any page in the Availity Web Portal.
Contact Name Name of a contact at the receiving organization (if different than the provider contact).
Telephone Number/Ext Telephone number of the receiving organization’s contact.
E-mail Address E-mail address of the receivng organization’s contact.
PROVIDER INFORMATION
Provider Name Complete legal name of institution, corporate entity, practice or individual provider.
Street The number and street name where a person or organization can be found.
City City associated with provider address field.
State/Province ISO 3166-2 Two Character Code associated with the State/Province/Region of the applicable Country.
ZIP Code/Postal Code System of postal-zone codes (zip stands for "zone improvement plan") introduced in the U.S. in 1963 to improve mail delivery and exploit electronic reading and sorting capabilities.
PROVIDER IDENTIFIERS INFORMATION
Provider Federal Tax Identification Number (TIN) or Employer Identification Number (EIN)
A Federal Tax Identification Number, also known as an Employer Identification Number (EIN), is used to identify a business entity.
National Provider Identifier (NPI) A Health Insurance Portability and Accountability Act (HIPAA) Administrative Simplification Standard. The NPI is a unique identification number for covered healthcare providers. Covered healthcare providers and all health plans and healthcare clearinghouses must use the NPIs in the administrative and financial transactions adopted under HIPAA. The NPI is a 10-position, intelligence-free numeric identifier (10-digit number). This means that the numbers do not carry other information about healthcare providers, such as the state in which they live or their medical specialty. The NPI must be used in lieu of legacy provider identifiers in the HIPAA standards transactions.
PROVIDER CONTACT INFORMATION
Provider Contact Name Name of a contact in provider office for handling ERA issues.
Telephone Number Associated with contact person.
E-mail Address An electronic mail address at which the health plan might contact the provider.
ELECTRONIC REMITTANCE ADVICE INFORMATION
Preference for Aggregation of Remittance Data (e.g., Account Number Linkage to Provider Identifier)
Provider preference for grouping (bulking) claim payment remittance advice – must match preference for EFT payment. Provider Tax Identification Number (TIN) – Enter a TIN in the field
provided if you select this option. National Provider Identifier (NPI) – Enter an NPI in the field provided
if you select this option.

Advanced Electronic Remittance Advice Enrollment
Rev. 09.15.2016.1
THIS TRANSMISSION IS A PROPRIETARY AND CONFIDENTIAL COMMUNICATION The documents accompanying this transmission may contain confidential health information that is legally privileged. This information is intended only for the use of the individuals or entities listed above. If you are not the intended recipient, you are hereby notified that any disclosure, copying, distribution, or action taken in reliance on the contents of these documents is strictly prohibited. If you have received this information in error, please notify the sender immediately and arrange for the return or destruction of these documents.
Field Descriptions (cont.)
Section Field Description
SUBMISSION INFORMATION
Reason for Submission Select one of the following options: New Enrollment, Change Enrollment, or Cancel Enrollment.
Authorized Signature The signature of an individual authorized by the provider or its agent to initiate, modify or terminate an enrollment. May be used with electronic and paper-based manual enrollment
Printed Name of Person Submitting Enrollment
The printed name of the person signing the form; may be used with electronic and paper-based manual enrollment.
Submission Date The date on which the enrollment is submitted.
Advanced Electronic Remittance Advice Enrollment
Rev. 09.15.2016.1
THIS TRANSMISSION IS A PROPRIETARY AND CONFIDENTIAL COMMUNICATION The documents accompanying this transmission may contain confidential health information that is legally privileged. This information is intended only for the use of the individuals or entities listed above. If you are not the intended recipient, you are hereby notified that any disclosure, copying, distribution, or action taken in reliance on the contents of these documents is strictly prohibited. If you have received this information in error, please notify the sender immediately and arrange for the return or destruction of these documents.
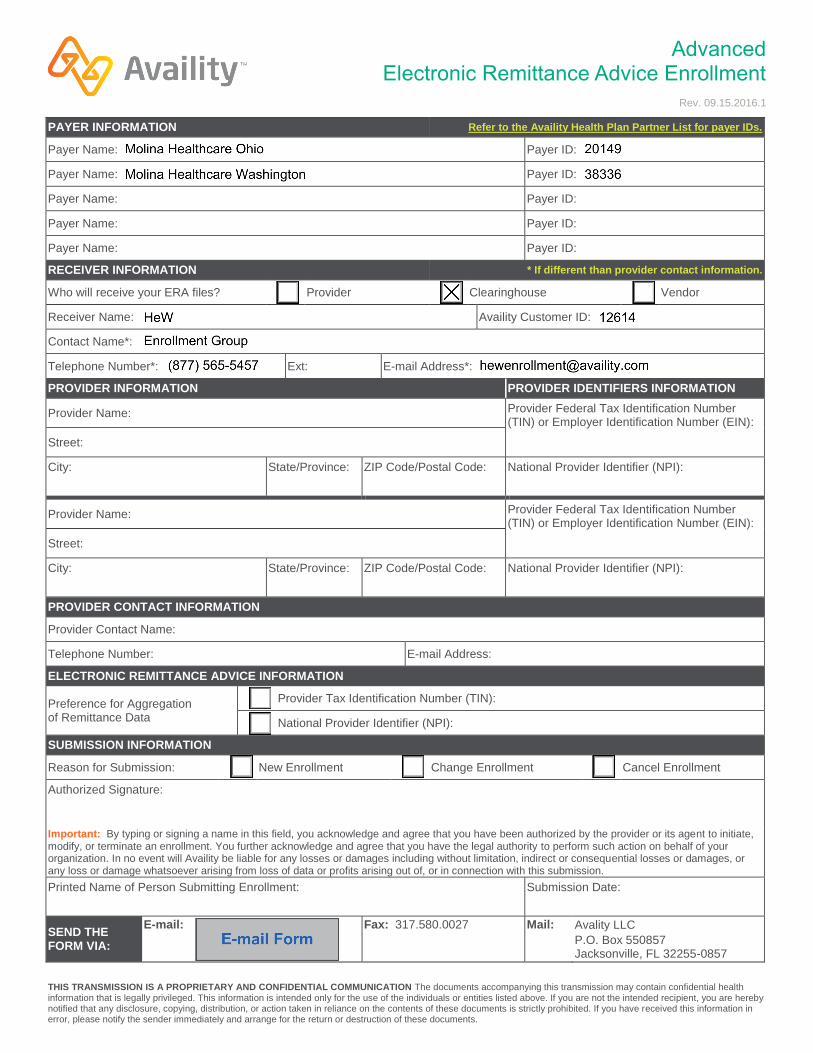
PAYER INFORMATION Refer to the Availity Health Plan Partner List for payer IDs.
Payer Name: Payer ID:
Payer Name: Payer ID:
Payer Name: Payer ID:
Payer Name: Payer ID:
Payer Name: Payer ID:
RECEIVER INFORMATION * If different than provider contact information.
Who will receive your ERA files? Provider Clearinghouse Vendor
Receiver Name: Availity Customer ID:
Contact Name*:
Telephone Number*: Ext: E-mail Address*:
PROVIDER INFORMATION PROVIDER IDENTIFIERS INFORMATION
Provider Name: Provider Federal Tax Identification Number (TIN) or Employer Identification Number (EIN):
Street:
City: State/Province: ZIP Code/Postal Code: National Provider Identifier (NPI):
Provider Name: Provider Federal Tax Identification Number (TIN) or Employer Identification Number (EIN):
Street:
City: State/Province: ZIP Code/Postal Code: National Provider Identifier (NPI):
PROVIDER CONTACT INFORMATION
Provider Contact Name:
Telephone Number: E-mail Address:
ELECTRONIC REMITTANCE ADVICE INFORMATION
Preference for Aggregation of Remittance Data
Provider Tax Identification Number (TIN):
National Provider Identifier (NPI):
SUBMISSION INFORMATION
Reason for Submission: New Enrollment Change Enrollment Cancel Enrollment
Authorized Signature:
Important: By typing or signing a name in this field, you acknowledge and agree that you have been authorized by the provider or its agent to initiate, modify, or terminate an enrollment. You further acknowledge and agree that you have the legal authority to perform such action on behalf of your organization. In no event will Availity be liable for any losses or damages including without limitation, indirect or consequential losses or damages, or any loss or damage whatsoever arising from loss of data or profits arising out of, or in connection with this submission.
Printed Name of Person Submitting Enrollment: Submission Date:
SEND THE FORM VIA:
E-mail: Fax: 317.580.0027 Mail: Avality LLC P.O. Box 550857 Jacksonville, FL 32255-0857

PAYER ENROLLMENT INSTRUCTIONS FOR
Before enrolling please be sure your Capario contract includes the transactions you will be using.
Complete the payer enrollment process BEFORE submitting claims to Capario for this payer. If you
are unsure about your contract status please contact Capario Support team at: [email protected] or
800‐792‐5256.
We recommend enrolling using our Portal enrollment tool. This free Portal tool allows you to enter
Providers and select the payers and transactions for your enrollment as it prefills the agreement
forms for you. Another advantage of the enrollment tool is the ability to follow the progress of
enrollments from initial generation through to payer approval. Our team will set you up and provide
a quick tutorial. Contact us at [email protected]
If you are not enrolling with the free portal Enrollment tool, please following these instructions:
If this payer does not require an agreement, go to Step 2. STEP 1: COMPLETE AGREEMENT
Complete all required fields on agreement and verify that information entered is correct.
If an agreement requires signatures, we recommend signing in blue ink. Do not use signature stamps.
STEP 2: PROCESS
STEP 3: COMPLETE CAPARIO ENROLLMENT SPREADSHEETS
Capario Provider Spreadsheet – This is completed for each new provider.
http://www.capario.com/downloads/xls/provider_bulk_spreadsheet.xlsx
Capario Payer Enrollment Spreadsheet – This is completed when requesting enrollment with a payer for providers previously added to the Capario system. Please refer to the instruction tab on each spreadsheet form for details about the information to enter in each column.
**PLEASE NOTE** The fields for tracking information are key for both your record keeping of enrollments and for Capario following up with payers for approvals. Be sure to enter all tracking for each enrollment.
http://www.capario.com/downloads/xls/enrollment_bulk_spreadsheet.xlsx
Email the completed spreadsheet(s) to: [email protected]
Questions? Contact us:
Phone: (800) 792‐5256 Option 1 Fax: (404) 877‐ 3324 Email: [email protected]

Change Healthcare ProviderNet – Registration
Instructions
Page 1 of 12
If you have any questions or concerns the ProviderNet Customer Support Team is available 8 a.m. – 6 p.m. CT at 877-389-1160 or email us at
Change Healthcare ProviderNet Registration Instructions
1. Go to https://providernet.adminisource.com
2. Click the “Register” button…
3. Accept the Terms and Conditions…
Change Healthcare ProviderNet – Registration
Instructions
Page 2 of 12
If you have any questions or concerns the ProviderNet Customer Support Team is available 8 a.m. – 6 p.m. CT at 877-389-1160 or email us at
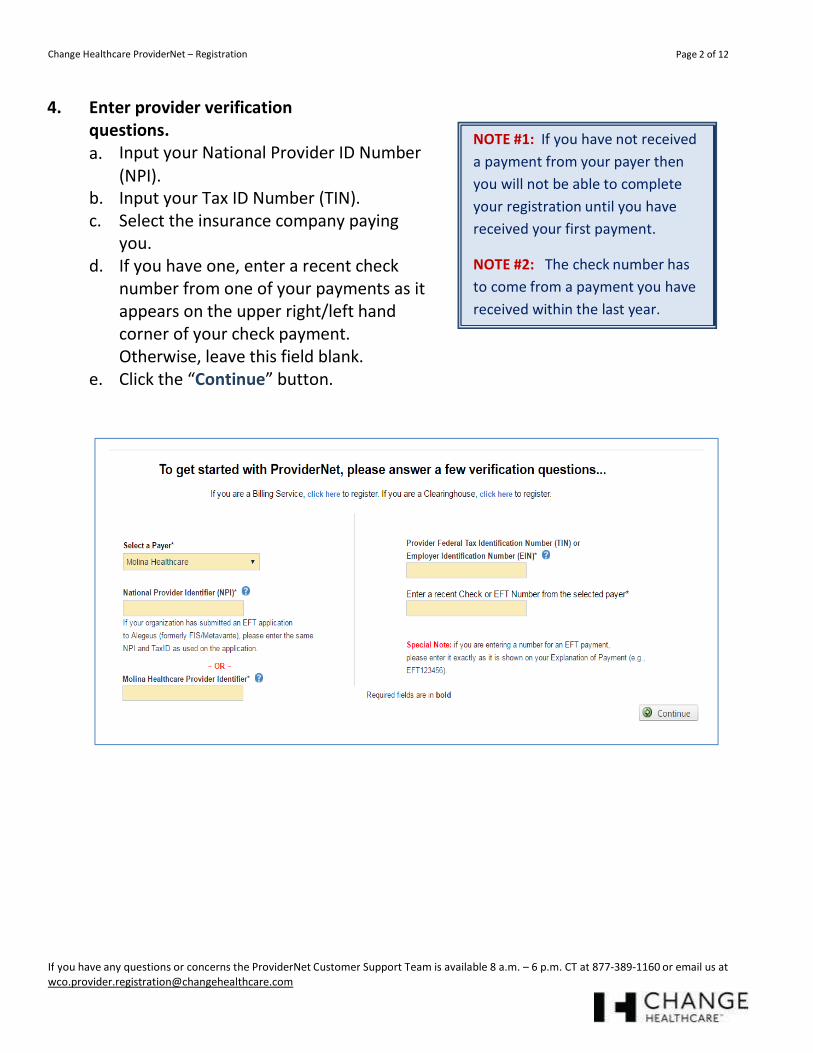
4. Enter provider verification
questions.
a. Input your National Provider ID Number
(NPI).
b. Input your Tax ID Number (TIN).
c. Select the insurance company paying
you.
d. If you have one, enter a recent check
number from one of your payments as it
appears on the upper right/left hand
corner of your check payment.
Otherwise, leave this field blank.
e. Click the “Continue” button.
NOTE #1: If you have not received
a payment from your payer then
you will not be able to complete
your registration until you have
received your first payment.
NOTE #2: The check number has
to come from a payment you have
received within the last year.

Change Healthcare ProviderNet – Registration
Instructions
Page 3 of 12
If you have any questions or concerns the ProviderNet Customer Support Team is available 8 a.m. – 6 p.m. CT at 877-389-1160 or email us at
5. Create your User Account.
a. Input and confirm your Email Address. This will be your login id.
b. Input your User Name (First and Last).
c. Input and confirm a Password.
d. Select a Password Reset Question.
e. Input a Password Reset Response.
f. Click the “Continue” button.
Password requirements
*No less than 8 characters
*No more than 10 characters
*At least 1 number

Change Healthcare ProviderNet – Registration
Instructions
Page 4 of 12
If you have any questions or concerns the ProviderNet Customer Support Team is available 8 a.m. – 6 p.m. CT at 877-389-1160 or email us at
6. Primary Administrative Contact Information
a. Input the Business Name.
b. Input the Provider Contact Name (First and Last) for this account.
c. Input the Provider Contact Title.
d. Input the Primary Contact Phone Number. Enter an extension if applicable.
e. Input the Fax Number.
f. Input the Primary Contact Email Address.
g. Click the “Continue” button.

Change Healthcare ProviderNet – Registration
Instructions
Page 5 of 12
If you have any questions or concerns the ProviderNet Customer Support Team is available 8 a.m. – 6 p.m. CT at 877-389-1160 or email us at
7. Select whether you would like to continue registering without EFT enrollment or
continue registering for EFT.
a. If you selected to “Continue Without EFT Enrollment” confirm your selection.
You will be able to set it up later. Click “OK” to continue registration without EFT
election Click “Cancel” to continue with EFT setup.
NOTE: If you elect to continue
registration without EFT payment
you will be directed to your Start
page. Skip to page 11 for further
instruction.
b. If you selected “Continue to EFT Enrollment” you are electing to receive your payer
(insurance company) payments direct deposited to an account you will designate.

Change Healthcare ProviderNet – Registration
Instructions
Page 6 of 12
If you have any questions or concerns the ProviderNet Customer Support Team is available 8 a.m. – 6 p.m. CT at 877-389-1160 or email us at
8. If you have one, enter the mailing address exactly as it appears on your Remittance
Advice in the upper left hand corner. Otherwise, please put the address Molina has on
file for you.
Note: You will have the
opportunity to enter additional
addresses after your registration
is completed.
9. This page displays your Federal Tax ID Number and NPI.
a. Your NPI and Federal TaxID are populated on your ACH Authorization form. The
fields have been disabled since these are the only values that are eligible for EFT
enrollment at this time.
b. Click the “Continue” button.

Change Healthcare ProviderNet – Registration
Instructions
Page 7 of 12
If you have any questions or concerns the ProviderNet Customer Support Team is available 8 a.m. – 6 p.m. CT at 877-389-1160 or email us at
10. Enter the bank account information where you would like to receive your deposits for
this NPI/TIN.
a. Enter your bank name.
b. Enter your routing number.
c. Select the type of account you have.
d. Enter your account number.
e. Select whether you would like your bank account linked to your TaxID or your NPI
f. Click the “Continue” button.
Identifying your routing number
Your routing number is located
between two special symbols
Note #1: It will take 7-10 business days for your bank to set up processes to ensure delivery of ACH payment
related Information.
Note #2: You will have the opportunity to enter additional accounts after registration is completed.
Change Healthcare ProviderNet – Registration
Instructions
Page 8 of 12
If you have any questions or concerns the ProviderNet Customer Support Team is available 8 a.m. – 6 p.m. CT at 877-389-1160 or email us at
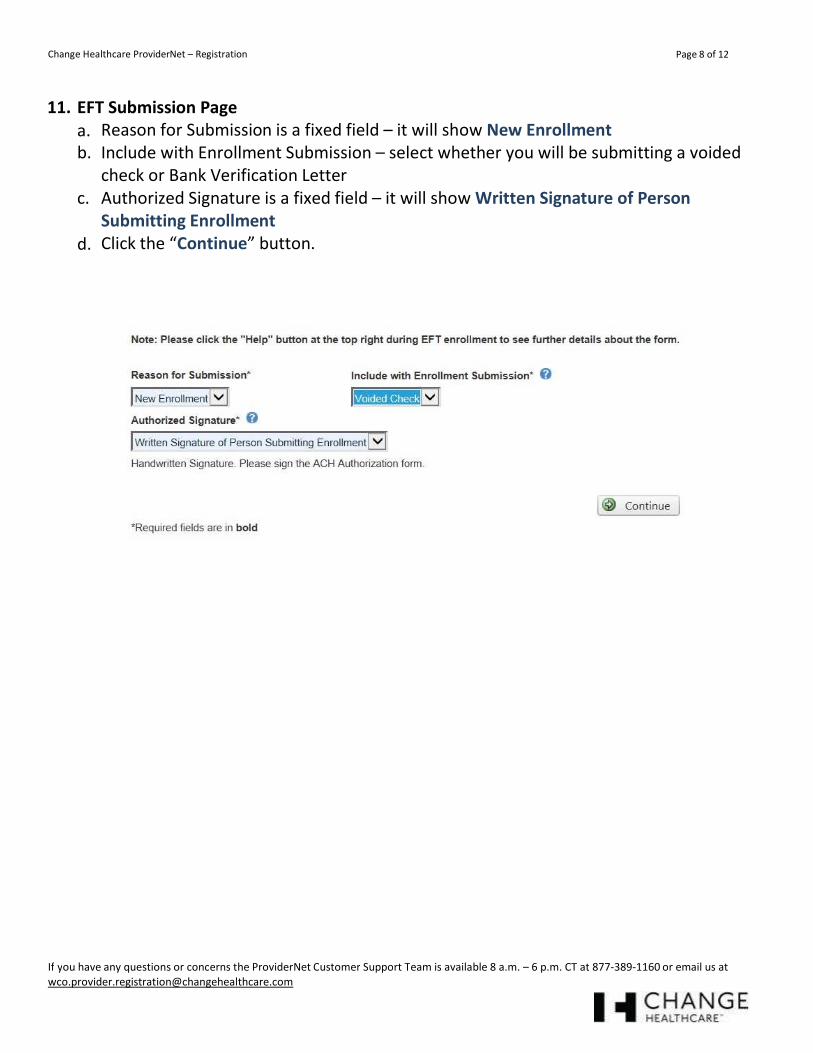
11. EFT Submission Page
a. Reason for Submission is a fixed field – it will show New Enrollment
b. Include with Enrollment Submission – select whether you will be submitting a voided
check or Bank Verification Letter
c. Authorized Signature is a fixed field – it will show Written Signature of Person
Submitting Enrollment
d. Click the “Continue” button.
Change Healthcare ProviderNet – Registration
Instructions
Page 9 of 12
If you have any questions or concerns the ProviderNet Customer Support Team is available 8 a.m. – 6 p.m. CT at 877-389-1160 or email us at
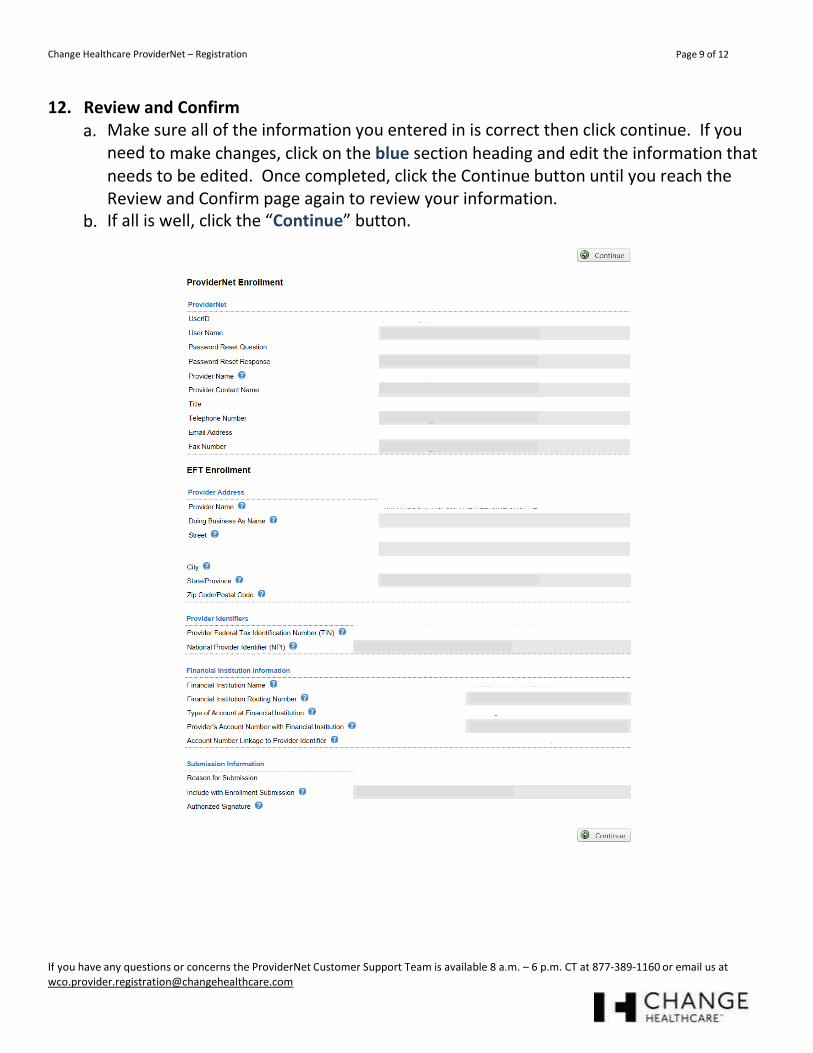
12. Review and Confirm
a. Make sure all of the information you entered in is correct then click continue. If you
need to make changes, click on the blue section heading and edit the information that
needs to be edited. Once completed, click the Continue button until you reach the
Review and Confirm page again to review your information.
b. If all is well, click the “Continue” button.

Change Healthcare ProviderNet – Registration
Instructions
Page 10 of 12
If you have any questions or concerns the ProviderNet Customer Support Team is available 8 a.m. – 6 p.m. CT at 877-389-1160 or email us at
13. ACH Authorization Form
a. Using the Print Icon at the bottom of the form Print, sign and email your ACH
Authorization Form along with a copy of a voided check or bank verification letter to
b. Click the “Continue” button. You will be directed to the start page to begin using
ProviderNet.

Change Healthcare ProviderNet – Registration
Instructions
Page 11 of 12
If you have any questions or concerns the ProviderNet Customer Support Team is available 8 a.m. – 6 p.m. CT at 877-389-1160 or email us at
14. ProviderNet Start Page
It takes up to 10 business days for your account to be verified and your EFTs to begin. You can
check the status of this process by logging in and clicking on the “Accounts” tab on your Control
Panel. If your account status says “verified” you should begin to receive your EFTs.
If your account status says “verified” and you still are receiving check payments please give
ProviderNet Customer Support a call, (877) 389-1160.
The red type at the top of this page indicates we have not received your ACH Authorization Form
or Voided Check/Bank Verification Letter. Once we receive and process both, that red type will
disappear.

Change Healthcare ProviderNet – Registration
Instructions
Page 12 of 12
If you have any questions or concerns the ProviderNet Customer Support Team is available 8 a.m. – 6 p.m. CT at 877-389-1160 or email us at
15. Control Panel
a. Use your control panel to navigate around ProviderNet
Payment Search – This page contains search options you can use to
search for particular payments. At the bottom of the page you will see
all of your payments, listed from newest to oldest dating back a year.
User Activity – This page allows Administrators to view each of the
user’s activity while using ProviderNet.
Provider Info - This page allows the Administrator to view or modify
your provider Information. You can also add additional payers and
NPI/TINs.
Accounts – You can view, add, change, or delete your Bank Account
Information.
Tax IDs – You can view, add, change, or delete your Tax IDs.
Contacts – This page allows you to view, add, change, or delete your
contacts.
Addresses – This page allows you to view, add, change, or delete your
Office Information (address).
EFT Enrollment – If during your initial registration you elected not to
receive your payments direct deposited you may click here to enroll in
EFT.
Connectivity – You can set up connectivity to receive your ERA (EDI
835s/ERA (PDF) files via FTP or have them automatically sent over to
your Clearinghouse.
User Administration – You can view, add, change, or delete user access
for your ProviderNet account.
My Profile – This page allows you to view, add, change, or delete your
User Profile Information.
Frequently Asked Questions – ProviderNet Q and A.
Icons – At the bottom of each page is an Icon Legend showing what the
Icons on that page represents.
SOFTWARE AND ANALYTICS l NETWORK SOLUTIONS l TECHNOLOGY‐ENABLED SERVICES
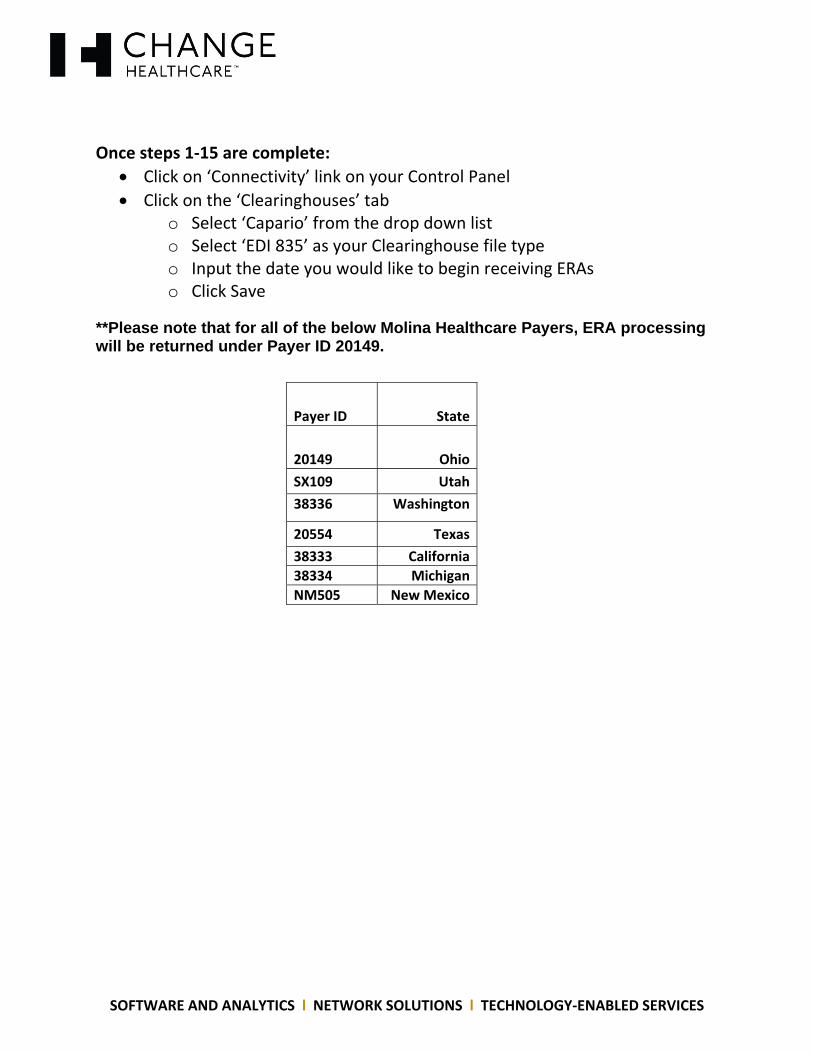
Once steps 1‐15 are complete:
Click on ‘Connectivity’ link on your Control Panel
Click on the ‘Clearinghouses’ tab o Select ‘Capario’ from the drop down list o Select ‘EDI 835’ as your Clearinghouse file type o Input the date you would like to begin receiving ERAs o Click Save
**Please note that for all of the below Molina Healthcare Payers, ERA processing will be returned under Payer ID 20149.
Payer ID State
20149 Ohio
SX109 Utah
38336 Washington
20554 Texas
38333 California
38334 Michigan
NM505 New Mexico