esophageal and swallowing disorders brenda beckett, pa-c une pa program
TRANSCRIPT

Esophageal and Swallowing Disorders
Brenda Beckett, PA-C
UNE PA Program

We’ll Cover Dysphagia
– Obstructive disorders• Schatzki Ring• Esophageal Web
– Motility disorders• Achalasia• Diffuse Esophageal Spasm
GERD Diverticula Mallory Weiss Syndrome Esophageal varices Esophageal rupture

Esophagus Muscular tube about 25 cm long
extending from the hypopharynx to the stomach.
Lies posterior to the trachea and heart. Passes through the mediastinum and
the hiatus in its descent from the thoracic to the abdominal cavity.
Terminates at cardia or LES

Symptoms
Dysphagia: Difficulty swallowing Odynophagia: Pain with swallowing Heartburn (pyrosis): Substernal burning,
can radiate to neck

Diagnostic Studies
Upper endoscopy: Study of choice for many esophageal disorders. Visualization and biopsy
Barium Esophagography: Differentiate mechanical from motility
Esophageal Manometry: Pressure. pH recording: Reflux

Dysphagia
Difficulty swallowing. “Food gets stuck” Oropharyngeal dysphagia- abnl function
proximal to esophagus– Neuro or muscular etiology, ie: Parkinsons, MS,
MD, MG
Esophageal dysphagia- difficulty passing food down esophagus due to either– Mechanical obstruction– Motility disorder

Obstructive Disorders
Dysphagia to solids– Bread and meat especially
Lower Esophageal Ring Esophageal Web Neoplasms (covered in separate
lecture)

Lower Esophageal Ring Schatzki’s Ring 2-4 mm mucosal stricture, usually
congenital Causes circumferential narrowing at
squamocolumnar junction at distal esophagus
Severity of sx based on lumen size

Schatzki Ring Assoc with hiatal hernia Dx: endoscopy or barium
esophagography Tx:
– Chew thoroughly– Endoscopic dilation

Esophageal Web Thin mucosal membrane across lumen
of upper esophagus Dysphagia to solids Seen with severe iron deficiency
anemia (as part of Plummer-Vinson) Dx and tx by endoscopy, also will
resolve with tx of Fe-deficiency anemia

Achalasia Neurogenic esophageal motility disorder
characterized by:
-impaired esophageal peristalsis
-lack of lower esophageal sphincter relaxation during swallowing
-elevation of lower esophageal sphincter resting pressure

Achalasia
Onset age 20-40 Progressive dysphagia
– Both liquids and solids Nocturnal regurgitation of undigested
foods in 1/3 of patients

Etiology ? Perhaps viral? Can be secondary to mechanical
obstruction or paraneoplastic process Loss of ganglion cells in mesenteric
plexus of esophagus Leads to denervation of esophageal
musculature

Achalasia Dx Barium studies:
– Absence of progressive peristaltic contractions during swallowing
– Significant esoph dilation– Narrowed “birds beak” distal esoph (at LES)
Manometry: – Lack of peristalsis, lack of relaxation of LES

Achalasia
Complications
Nocturnal regurgitation Cough Aspiration
– pnemonitis

Achalasia Treatment There is no treatment to restore
peristalsis Goal: decrease LES pressure
– Balloon dilation of LES, may repeat– Drugs: Nitrates, CCB, Botox
Surgery: Heller myotomy

Diffuse Esophageal Spasm
Non-productive esophageal contractions
Hyperdynamic contractions Increased LES pressure
Esoph Spasm Sx Substernal squeezing chest pain
– With dysphagia for liquids and solids May occur with exertion May occur with esoph temp extremes Sound familiar?? Can be
indistinguishable from angina pectoris or myocardial infarction
Dysphagia uncommon sx

Esoph Spasm Dx Rule out coronary ischemia Barium swallow:
– Poor progression of bolus– Disordered, simultaneous contractions
Esophageal manometry– Simultaneous, prolonged, high amplitude
contractions– “Nutcracker esophagus” – pressure so high
it can crack a nut

Treatment
CCBs Botox Nitrates Others

Esophageal Diverticula Outpouching of mucosa through the
muscular layer of the esophagus Asymptomatic or dysphagia and
regurgitation

Zenker’s diverticulum Posterior outpouchings of mucosa and
submucosa through the crico-pharyngeal muscle
Likely results from an incoordination between pharyngeal propulsion and cricopharyngeal relaxation
SX: Regurg, choking, protrusion in neck TRT: surgery, stapling

Zenker’s Diverticulum

GERD Gastroesophageal reflux disease
– Reflux of stomach contents causing symptoms Incompetent LES from:
– General loss of intrinsic sphincter tone– Recurrent inappropriate relaxations triggered
by gastric stretch Allows reflux of gastric contents into
esophagus Frequent in infants (also GER)


Factors contributing to LES Competence Angle of cardioesophageal junction Action of diaphragm Gravity
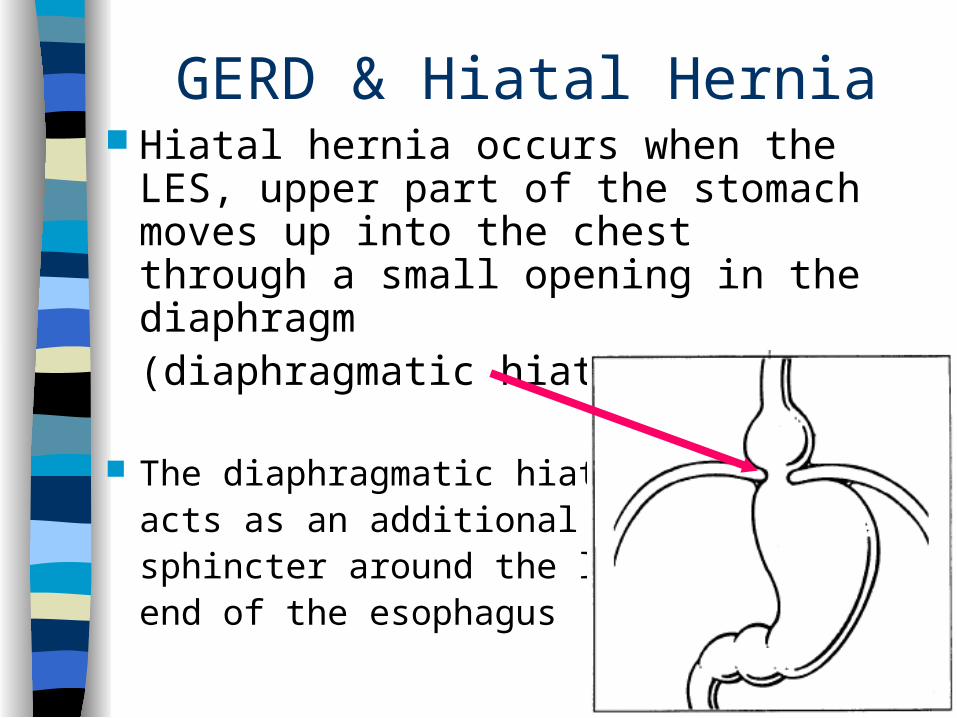
GERD & Hiatal Hernia Hiatal hernia occurs when the LES,
upper part of the stomach moves up into the chest through a small opening in the diaphragm (diaphragmatic hiatus).
The diaphragmatic hiatusacts as an additional sphincter around the lowerend of the esophagus

Factors Contributing to Reflux
Weight gain Fatty foods Caffeine Carbonated beverages EtoH Tobacco Increased intrabdominal pressure Drugs: anticholinergics, antihistamines,
TCAs, CCBs, nitrates, progesterone

Symptoms Heartburn
– Substernal burning– Regurgitation (I think I just threw up in my
mouth…) Hypersalivation (from smoking as well) Belching, nausea Dysphagia, odynophagia *Cough, wheezing, hoarseness, asthma

Complications
Esophagitis Peptic esophageal ulcer Esophageal stricture Barrett’s esophagus

GERD Dx
Detailed history Typical symptoms get trial treatment Work-up reserved for:
– Longstanding sx – Symptoms of complications– Pts who fail empiric tx
Endoscopy with biopsy

GERD Tx HOB 6 inches (not just pillows) NO:
– Eating within 3 hours of bedtime, large meals– Acidic foods(coffee, citrus, tomatoes, etc)– Drugs (see list of contributors to sx)– Smoking (hyposalivation)– Foods that weaken LES (fatty foods, alcohol,
chocolate, peppermint) Meds: PPI x 8-12 weeks (better than H2
blockers, antacids or pro-motility meds) Weight loss Surgical: Fundoplication

Nissen Fundoplication

Esophagitis
GERD (Most common) Pill esophagitis
– Direct erosive effects Radiation esophagitis Infectious esophagitis
– Usually in immunocompromised pts– Candida, CMV, HSV

Esophagitis
Symptoms– Odynophagia. Pain on swallowing– Dysphagia– Chest pain: substernal– Signs of infection

Barrett’s Esophagitis
Normal stratified squamous epithelium of distal esophagus replaced by:– Metaplastic, columnar, glandular intestine-
like mucosa Can give rise to adenocarcinoma Warrants frequent surveillance by
endoscopy


Esophageal varices
Usually caused by portal hypertension secondary to cirrhosis
Can cause painless, sometimes massive upper GI bleed
Bright red hematemesis– NOT coffee-ground emesis
First, stabilize the pt: fluid resuscitation, blood transfusion, etc
Then endoscopic/surgical repair
Mallory-Weiss Syndrome Non-penetrating mucosal laceration of
distal esoph/proximal stomach Caused by vomiting, retching,
hiccupping Often seen in alcoholics, but
any forceful vomiting will do Can cause significant bleeds
– Most stop spontaneously– 10% require transfusion– May need cauterization

Esophageal Rupture
Iatrogenic– ie: during endoscopy
Spontaneous– Boerhaave Syndrome (usu vomiting, so not
truly spontaneous, but differentiates from iatro)
Esoph Rupture
MC site distal esophagus, L side Acid and stomach contents cause
fulminant medistinitis, pneumomediastinum, shock.
Bad.

Esoph rupture S/S
Sx: chest, abd, thoracic pain, hematemesis, shock
Did I say BAD? Subcutaneous emphysema palpable in
30% Hamman’s sign- mediastinal crunch
– Crackling synchronous with heartbeat.– Cool

Rupture Dx & Tx Imaging
– Mediastinal air & widening, pleural effusion Confirm with esophagography with
water soluble contrast dye Broad spectrum abx, fluid resuscitation,
surgical repair.
High mortality