esophageal cancer treated with surgery and radiation
TRANSCRIPT

Case Study Esophageal Cancer Treated with Surgery and Radiation
Fall 2016 Assignment 8
Due date: Nov 18, 2016
Yeyan Jin CSUID:829840439
FSHN 450
I pledge on my honor that I have not given or received any unauthorized assistance on this assignment
Esophageal Cancer Treated with Surgery and Radiation
FSHN 450
Due Date: November 18, 2016
Nick S. is a 58 year old male seeking medical attention for recurrent heartburn of 1 year duration. He presented with difficulty swallowing for past 4 – 5 months and unexplained weight loss
Education: College degree
Occupation: Contractor
Social Hx: Married, wife age 52, son age 17 in high school, daughter 19 away at college. Smokes 20 cigarettes/day for past 40 years. Drinks 2 beers per day.
Medical Hx: States that “food gets stuck in throat”. Takes TUMS and Pepcid consistently for the past year. Wt loss of 30 pounds past 3 – 4 months. Patient states he has been unable to eat because of heartburn and difficulty swallowing, especially anything with course or crunchy texture.
Physical Exam: thin, pale white male. Temp 98.3, BP 132/90, HR 88 bpm, RR 13 bpm, Ht: 6’3” UBW: 220 # CBW: 190 #
HEENT: eyes sunken, sclera clear, dry mucous membranes
Skin: warm, dry
Chest/lungs: cleat to auscultation and percussion
Abdomen: epigastric tenderness
Nutrition Hx:
Appetite general poor PTA. Regurgitation of some foods, reports pain upon swallowing
Usual Dietary Intake:
AM: eggs, toast, coffee with 2 tsp sugar (but no longer drinks coffee with heartburn)
Lunch: cold sandwich packed for worksite (3 oz meat, two slices white bread). Lately c/o bread sticks in the throat – 24 hour recall notes only tomato soup and 4 crackers
Dinner: Generally eats all meats, vegetables, potato or rice but 24 hour recall notes only baked macaroni and cheese and 1 scoop vanilla ice cream
Evening: Two beers (but has contributed to heartburn so has mostly cut out beer lately)
Food purchased and prepared by wife.
Food allergies: NKA
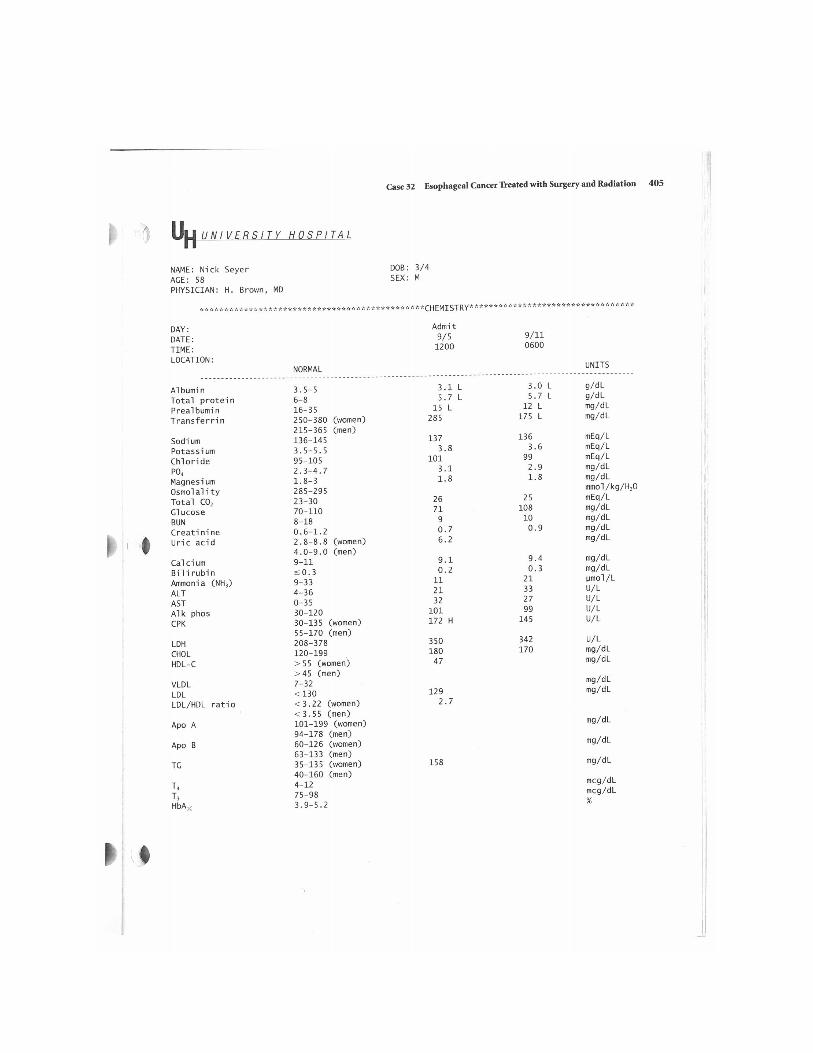
Dx: Diagnosis following X-ray, endoscopy and biopsy – Stage II (T1,N1,M0) adenocarcinoma of the esophagus
See admission laboratory report (attached)
Tx Plan: Esophageal transhiatal esophagectomy with an intrathoracic esophagogastric anastamosis. Jejunal tube surgically placed. Radiation planned post-operatively.
Rx: NPO with TPN post-operatively progressing to tube feeding as tolerated.
Case report:
Answer the following questions.
1. What does the term adenocarcinoma mean? What are an esophageal transhiatal esophagectomy and an esophagogastric anastomosis? Hint go to this website for a thorough and accurate explanation by University of Michigan who developed the prodcedure:
http://surgery.med.umich.edu/thoracic/patient/what_we_do/esophagectomy_faq.shtml
Adenocarcinoma is a type of cancer tumor that found in in the glands. It usually occurs in breasts, esophagus, lungs, pancreas, or prostate. Esophageal transhiatal esophagectomy is an operation to remove esophagus through the diaphragmatic hiatus without opening the chest. It goes through an abdominal incision and a neck incision without open the chest. Then connects the remaining esophagus to the stomach in the chest. Esophagogastric anastomosis is to connect the remaining esophagus to the stomach in the chest.
2. What are the two most common risk factors for esophageal cancer? Does the patient have these risk factors?
The two most common risk factors for esophageal cancer are alcohol and Tabaco. He has alcohol consumption which will increase risk of esophageal cancer. His BMI is 27.5 which is overweight. Obesity is also a risk factor for esophageal cancer.
3. The patient’s stage was TII. What is the meaning of the terms T1, N1, M0?
T is used to describe the tumor, whether the cancer has grown into the wall of the esophagus or nearby tissue, and how deep. T1 means cancer cells have spread into the lining of the esophagus.

N is used to describe lymph nodes. N1 means The cancer has spread to 1 or 2 lymph nodes in the chest, near the tumor. M is used to describe whether the cancer has spread to other parts of the body. M0 means The cancer has not spread to other parts of the body.
4. Why is cancer therapy multi-modality?
There are several types of cancer treatment, such as radiation, surgery, chemotherapy and biotherapy/immunotherapy. Using multiple treatments together is good to preventing recurrence. It’s not sure which single cancer treatment will work to the patient. Using single cancer treatment will cost more time to figure out witch treatment is most effective for patient. In most case, time is most important thing for cancer therapy. The more time is used during treatment will give more time for cancer development.
5. Evaluate the patient’s usual body weight and current body weight and risk factors for malnutrition.
%UBW= 190/220=86.4% 13.6%UBW weight loss. He is losing weight. His risk factors for malnutrition are eating disorder (swallowing difficulty), unable to eat because of heartburn and hospitalization.
6. Assess the patients Kcal and protein needs for TPN. You do not need to calculate a TPN but suggest a protein sources and % Kcal from protein, fat and glucose.
Kcal: 30Kcal/Kg * (190/2.2) lb.= 2590 Kcal/Day Protein:1.2g/Kg * (190/2.2) lb.= 103.7g/Day He is suggested to eat lean animal protein and limit red meats intake. 55% Kcal from glucose, 15% Kcal from protein, 30% Kcal from fat.
7. Describe how you will transition the patient from TPN to tube feeding. Suggest a product that you will use for tube feeding that will meet the need of this patient a) in the post-operative period and 2) long term.
Start with 40 cc per hour. If feeding is tolerated, can proceed at 20 to 25 cc per hour increments over a 12-or 24-hour period until achieve the final volume. In the post-operative period: I suggest him to use Vital 1.5 Cal Nutritional Supplement by Abbott tube feeding. Since he need more protein to get recover from surgery. It will provide 101.25 g protein from 1.5 serving of this product. 2250 Cal per day. Long term: I suggest him to use Perative Nutritional Supplement by Abbott tube feeding. Since he is out of the hospital, his calories require is increased. That product will provide him 2600 Cal per day from 2 serving of this product.
8. Describe the volume and method of administration of the TF you selected for a) post-operative recovery in the hospital and b) TF you selected for home (long term).
a) Vital 1.5 Cal Nutritional Supplement by Abbott:It has 1000 ml, 1500 Cal per serving. I would like him to use 1 and a half of this product per day for in hospital use. Use continuous drip method via gravity or a pump. It is usually tolerated better than bolus feedings. b) Perative Nutritional Supplement by Abbott: It has 1000ml, 1300 Cal per serving. I would like him to use 2 of this product per day for long term use. Use Bolus feeding. That allows him has more mobility than continuous drop method.
9. Compare fluid requirements to the amount of fluid provided in each tube feeding. How will you make up the difference?
His fluid requirement is 3500ml (35ml/Kg * (220/2.2)Kg). In the post-operative period: Tube feeding contains 1500 ml. Add additional water flushes per day. 250 ml per time, 8 times per day. Long term: Tube feeding contains 2000 ml. Add additional water flushes per day. 500 ml 3 times before or after meal.
10. Write a PES statement for the patients discharge plan including goals and follow –up (list at least four factors you should monitor)
Low food intake r/t swallowing difficulty AEB 13.6% UBW weight lose
Use Perative Nutritional Supplement by Abbott tube feeding. 2 serving per day.
After few weeks I want to know his prealbumin level, transferrin level and body weight.
11. The patient will receive outpatient radiation therapy following D/C. List additional nutritional complications that may occur.
Anorexia and Weight Loss. Fatigue, food aversions. Increase BMR Increase Lipolysis and FFA release Increase Serum FFA and fat oxidation Decrease Lipogenesis