esophageal diseases absite lecture series faiz bhora, md attending thoracic surgeon st. luke’s...
TRANSCRIPT

Esophageal Esophageal DiseasesDiseases
ABSITE Lecture SeriesABSITE Lecture SeriesFaiz Bhora, MDFaiz Bhora, MD
Attending Thoracic SurgeonAttending Thoracic Surgeon
St. Luke’s Roosevelt Medical St. Luke’s Roosevelt Medical Center, NY, Center, NY,

Esophagus Lecture Part 1Esophagus Lecture Part 1

Essential Esophageal Essential Esophageal AnatomyAnatomy
The esophagus is 25 cm in length. The lower 5-7 The esophagus is 25 cm in length. The lower 5-7 cm are below the diaphragmcm are below the diaphragm
Average distance from incisors to GE junction is Average distance from incisors to GE junction is 38-40 cm in men. The distance from the incisors 38-40 cm in men. The distance from the incisors to the cricopharyngeus is 15 cmto the cricopharyngeus is 15 cm
Topographically, the esophagus begins at the Topographically, the esophagus begins at the lower border of C6. The diaphragmatic hiatus is lower border of C6. The diaphragmatic hiatus is at T10at T10
The upper 1/3 esophagus is slightly to the left of The upper 1/3 esophagus is slightly to the left of midline, the middle 1/3 slightly to the right, and midline, the middle 1/3 slightly to the right, and the lower 1/3 slightly to the leftthe lower 1/3 slightly to the left

Essential Esophageal Essential Esophageal AnatomyAnatomy The upper 1/3 is composed of striated muscle and is The upper 1/3 is composed of striated muscle and is
innervated by the vagus and its recurrent branch. The lower innervated by the vagus and its recurrent branch. The lower 2/3 is composed of smooth muscle and is supplied by the 2/3 is composed of smooth muscle and is supplied by the vagus and the intrinsic autonomic nerve plexusvagus and the intrinsic autonomic nerve plexus
The arterial blood supply is segmental. These include the The arterial blood supply is segmental. These include the inferior thyroid artery, bronchial arteries and aortic branches, inferior thyroid artery, bronchial arteries and aortic branches, and branches of the left gastric and inferior phrenicand branches of the left gastric and inferior phrenic
The venous drainage likewise is via the azygous, hemiazygous, The venous drainage likewise is via the azygous, hemiazygous, intercostals, and left gastric veinsintercostals, and left gastric veins
The lymphatic drainage of the upper 1/3 is to the internal The lymphatic drainage of the upper 1/3 is to the internal jugular, deep cervical and para tracheal nodes. The middle jugular, deep cervical and para tracheal nodes. The middle 1/3 drains into the subcarinal and inf pulmonary ligament 1/3 drains into the subcarinal and inf pulmonary ligament nodes. The lower 1/3 drains into the paraesophageal and nodes. The lower 1/3 drains into the paraesophageal and celiac nodes. celiac nodes.

Esophageal Spasm Esophageal Spasm SyndromesSyndromes
Inadequate LES relaxationInadequate LES relaxation
Achalasia, epiphrenic diverticulumAchalasia, epiphrenic diverticulum Uncoordinated esophageal contractionUncoordinated esophageal contraction
Diffuse esophageal spasm (DES)Diffuse esophageal spasm (DES) HypercontractionHypercontraction
High-amplitude peristaltic contraction (HAPC, High-amplitude peristaltic contraction (HAPC, “nutcracker esophagus”), Hypertensive lower “nutcracker esophagus”), Hypertensive lower esophageal sphincter (HLES)esophageal sphincter (HLES)
HypocontarctionHypocontarction
Ineffective esophageal motility (IEM)Ineffective esophageal motility (IEM)

Esophageal Spasm Esophageal Spasm SyndromesSyndromes
Pain is the Predominant SymptomPain is the Predominant Symptom
1.1. DESDES Patients present with cardiac like chest painPatients present with cardiac like chest pain Dysphagia to both solids and liquidsDysphagia to both solids and liquids Corkscrew esophagus on contrast esophagogramCorkscrew esophagus on contrast esophagogram Manometry shows > 10% of a series of wet swallows Manometry shows > 10% of a series of wet swallows
associated with simultaneous contractions and with associated with simultaneous contractions and with mean amplitudes of > 30 mmHg. LES is normalmean amplitudes of > 30 mmHg. LES is normal
Treatment includes medications, pneumatic dilatation, Treatment includes medications, pneumatic dilatation, botulinum toxin injections. Operative intervention when botulinum toxin injections. Operative intervention when conservative measures have failedconservative measures have failed

Esophageal Spasm Esophageal Spasm SyndromesSyndromes
Pain is the Predominant SymptomPain is the Predominant Symptom
2.2. HAPC (Nutcracker esophagus)HAPC (Nutcracker esophagus) Patient’s present with sharp, episodic chest painPatient’s present with sharp, episodic chest pain Dysphagia uncommonDysphagia uncommon Contrast esophagogram of low yieldContrast esophagogram of low yield Manometry shows high amplitude, coordinated, Manometry shows high amplitude, coordinated,
peristaltic contractionsperistaltic contractions Treatment with diltiazem has been shown to be helpful. Treatment with diltiazem has been shown to be helpful.
Long esophageal myotomy and partial fundoplication if Long esophageal myotomy and partial fundoplication if medical therapy failsmedical therapy fails

Esophageal Spasm Esophageal Spasm SyndromesSyndromes
Pain is the Not the Predominant SymptomPain is the Not the Predominant Symptom
1.1. AchalasiaAchalasia

AchalasiaAchalasia
Achalasia is best confirmed by:Achalasia is best confirmed by:
1.1. A birds beak appearance on barium A birds beak appearance on barium esophagogramesophagogram
2.2. Aperistalsis of the cervical esophagusAperistalsis of the cervical esophagus
3.3. Failure of the LES to relax on swallowingFailure of the LES to relax on swallowing
4.4. LES pressure < 5 mmHgLES pressure < 5 mmHg
5.5. Biopsy proven esophagitis on flexible Biopsy proven esophagitis on flexible endososcopyendososcopy

AchalasiaAchalasia Achalasia is a primary motor disorder of the Achalasia is a primary motor disorder of the
esophagus characterized by failure of relaxation esophagus characterized by failure of relaxation of the LES and loss of peristaltic waveform in the of the LES and loss of peristaltic waveform in the bodybody
The cause is believed to be neuronal degeneration The cause is believed to be neuronal degeneration in the myenteric plexus (Auerbach’s plexus)in the myenteric plexus (Auerbach’s plexus)
Symptoms include dysphagia, regurgitation, Symptoms include dysphagia, regurgitation, weight loss, chest pain, pneumoniaweight loss, chest pain, pneumonia
Achalasia is a premalignant condition, with Achalasia is a premalignant condition, with carcinoma developing in 1-10% of patients over carcinoma developing in 1-10% of patients over 15-25 years15-25 years

Characteristics of Characteristics of AchalasiaAchalasia
ManometryManometry1.1. Incomplete LES relaxation on swallowingIncomplete LES relaxation on swallowing2.2. Aperistalsis of the bodyAperistalsis of the body3.3. Elevated LES pressure (>35 mmHg)Elevated LES pressure (>35 mmHg)4.4. Increased resting esophageal pressureIncreased resting esophageal pressure
EsophagogramEsophagogram1.1. Esophageal dilationEsophageal dilation2.2. Air/Fluid levelAir/Fluid level3.3. Bird’s beak or Sigmoid esophagusBird’s beak or Sigmoid esophagus
EndoscopyEndoscopy1.1. Esophageal dilationEsophageal dilation2.2. Retained foodRetained food3.3. Frequently normalFrequently normal

Treatment of AchalasiaTreatment of Achalasia Traditionally, the primary therapeutic approach for Traditionally, the primary therapeutic approach for
achalasia involves pharmacological agents, achalasia involves pharmacological agents, endoscopic botulinum toxin into the LES and endoscopic botulinum toxin into the LES and pneumatic dilatation of the LESpneumatic dilatation of the LES
Pharmacologic AgentsPharmacologic Agents
1.1. Calcium channel blockers and long acting Nitrates Calcium channel blockers and long acting Nitrates both decrease LES resting pressure. Usually poor, both decrease LES resting pressure. Usually poor, short-lived response, side effects limit their short-lived response, side effects limit their effectivenesseffectiveness
2.2. Endoscopic botulinum toxin is successful in 80% of Endoscopic botulinum toxin is successful in 80% of patients in relieving dysphagia. However, symptoms patients in relieving dysphagia. However, symptoms return in 50% in 6 months. Retreatment is return in 50% in 6 months. Retreatment is successful in 50% of original responderssuccessful in 50% of original responders

Treatment of AchalasiaTreatment of Achalasia Pneumatic DilatationPneumatic Dilatation
Disrupts LES muscle fibers and produces relief Disrupts LES muscle fibers and produces relief of symptoms in 50-85% of patients. However, of symptoms in 50-85% of patients. However, most patients require multiple dilatations, most patients require multiple dilatations, increasing the risk of perforation (up to 8%). increasing the risk of perforation (up to 8%). Long term relief of symptoms in 40-65%Long term relief of symptoms in 40-65%
Pneumatic Dilation vs Surgical MyotomyPneumatic Dilation vs Surgical Myotomy
Only one randomized controlled trial with long Only one randomized controlled trial with long term follow-up (dysphagia relieved in 91% vs term follow-up (dysphagia relieved in 91% vs 65%)65%)

Treatment of AchalasiaTreatment of Achalasia
Surgical MyotomySurgical Myotomy Transabdominal vs TransthoracicTransabdominal vs Transthoracic Dysphagia relief about 90% at 2 yearsDysphagia relief about 90% at 2 years Recurrent dysphagia within 2 months likely due Recurrent dysphagia within 2 months likely due
to incomplete myotomy, torsion of the repair or to incomplete myotomy, torsion of the repair or scarring of the mucosa from cauteryscarring of the mucosa from cautery
Late-onset dysphagia due to mucosal stricture Late-onset dysphagia due to mucosal stricture from reflux, or the latent effects of delayed from reflux, or the latent effects of delayed gastric emptying. These patients ultimately need gastric emptying. These patients ultimately need gastric or esophageal resectiongastric or esophageal resection

Treatment of AchalasiaTreatment of Achalasia
Surgical MyotomySurgical Myotomy A resting LES > 36 mm Hg is associated with a A resting LES > 36 mm Hg is associated with a
good surgical outcomegood surgical outcome Patients with esophageal dilation > 6 cm or with Patients with esophageal dilation > 6 cm or with
loss of the esophageal axis (i.e. sigmoid, tortuous loss of the esophageal axis (i.e. sigmoid, tortuous or convoluted esophagus) will need an or convoluted esophagus) will need an esophagectomyesophagectomy
Addition of an Anti-Reflux Procedure?Addition of an Anti-Reflux Procedure? Reflux symptoms occur in up to 30% of patients. A Reflux symptoms occur in up to 30% of patients. A
partial fundoplication should be added. partial fundoplication should be added. No difference between a 180-degree Dor or a 270-No difference between a 180-degree Dor or a 270-
degree Toupet partial fundoplicationdegree Toupet partial fundoplication

Esophageal Spasm Esophageal Spasm SyndromesSyndromes
Pain is the Not the Predominant SymptomPain is the Not the Predominant Symptom
2.2. Hypertensive Lower Esophageal Sphincter Hypertensive Lower Esophageal Sphincter (HLES)(HLES)
Most patients present with dysphagiaMost patients present with dysphagia Manometry shows elevated basal LES pressure, Manometry shows elevated basal LES pressure,
normal peristalsis and normal LES relaxationnormal peristalsis and normal LES relaxation Treatment options include medication, Treatment options include medication,
pneumatic dilatation or myotomypneumatic dilatation or myotomy

Esophageal Spasm Esophageal Spasm SyndromesSyndromes
Pain is the Not the Predominant SymptomPain is the Not the Predominant Symptom3.3. Ineffective Esophageal Motility (IEM)Ineffective Esophageal Motility (IEM) Most often seen in scleroderma, rheumatoid arthritis, Most often seen in scleroderma, rheumatoid arthritis,
SLE, DM, alcoholismSLE, DM, alcoholism Most patients present with dysphagia and refluxMost patients present with dysphagia and reflux Contrast esophagogram shows a “lead-pipe” esophagusContrast esophagogram shows a “lead-pipe” esophagus Manometry shows low amplitude contractions, Manometry shows low amplitude contractions,
ineffective peristalsis and decreased LES resting ineffective peristalsis and decreased LES resting pressurepressure
Therapy involves medical anti-reflux therapy. Therapy involves medical anti-reflux therapy. Esophageal shortening may occur in these patientsEsophageal shortening may occur in these patients

Esophageal Spasm Esophageal Spasm SyndromesSyndromes
A 55 yr old woman has a 6 month history of A 55 yr old woman has a 6 month history of intermittent heartburn and dysphagia. intermittent heartburn and dysphagia. Endoscopy shows severe esophagitis. The Endoscopy shows severe esophagitis. The barium swallow shows a lead-pipe esophagus. barium swallow shows a lead-pipe esophagus. The LES resting pressure is < 5 mmHg with The LES resting pressure is < 5 mmHg with markedly diminished peristaltic activity. The markedly diminished peristaltic activity. The most likely diagnosis is:most likely diagnosis is:
1.1. AchalasiaAchalasia
2.2. GERDGERD
3.3. Cohn's diseaseCohn's disease
4.4. SclerodermaScleroderma
5.5. Sjogren’s syndromeSjogren’s syndrome

Esophageal DiverticulumEsophageal Diverticulum A 65 yr old man has worsening dysphagia A 65 yr old man has worsening dysphagia
and regurgitation. Barium swallow shows and regurgitation. Barium swallow shows a 5 cm epiphrenic diverticulum. a 5 cm epiphrenic diverticulum. Treatment should be:Treatment should be:
1.1. Distal esophageal resectionDistal esophageal resection2.2. Esophageal dilation and fundoplicationEsophageal dilation and fundoplication3.3. Resection of the diverticulum and long Resection of the diverticulum and long
myotomymyotomy4.4. Resection of the diverticulum onlyResection of the diverticulum only5.5. DiverticulopexyDiverticulopexy

Esophageal DiverticulumEsophageal Diverticulum
Epiphrenic DiverticulumEpiphrenic Diverticulum Usually pulsion diverticulum located within the distal 10 Usually pulsion diverticulum located within the distal 10
cm of the thoracic esophaguscm of the thoracic esophagus Usually right sidedUsually right sided Most are found incidentally, however, the most common Most are found incidentally, however, the most common
symptoms are dysphagia, regurgitation symptoms are dysphagia, regurgitation Barium esophagogram remains the best test for diagnosisBarium esophagogram remains the best test for diagnosis Endoscopy, 24 Hr PH and manometry should be performedEndoscopy, 24 Hr PH and manometry should be performed Symptomatic, anatomically dependent and enlarging Symptomatic, anatomically dependent and enlarging
diverticulum should be surgically repaireddiverticulum should be surgically repaired Surgical therapy includes diverticulectomy, myotomy and a Surgical therapy includes diverticulectomy, myotomy and a
partial fundoplication as indicated (Transthoracic or partial fundoplication as indicated (Transthoracic or Transabdominal)Transabdominal)

Esophageal DiverticulumEsophageal Diverticulum
Zenker’s DiverticulumZenker’s Diverticulum Most common esophageal diverticulumMost common esophageal diverticulum Killian’s triangle is usually the site of weaknessKillian’s triangle is usually the site of weakness Symptoms include regurgitation, halitosis, Symptoms include regurgitation, halitosis,
chocking, aspiration, nocturnal coughing, chocking, aspiration, nocturnal coughing, laryngitis. Motility determines symptoms and laryngitis. Motility determines symptoms and not the pouch sizenot the pouch size
Diagnosis made on barium swallowDiagnosis made on barium swallow Endoscopy to rule out malignancyEndoscopy to rule out malignancy Surgical treatment recommended if symptomaticSurgical treatment recommended if symptomatic Treatment consists of cervical esophagomyotomy Treatment consists of cervical esophagomyotomy
and pouch resectionand pouch resection

Esophageal DiverticulumEsophageal Diverticulum
Midesophageal DiverticulumMidesophageal Diverticulum Usually traction diverticulumUsually traction diverticulum These are due to TB and histoplasmosis. Most These are due to TB and histoplasmosis. Most
asymptomatic and need no interventionasymptomatic and need no intervention Midesophageal pulsion diverticulum are due to an Midesophageal pulsion diverticulum are due to an
underlying motility disorder and are due to pulsion. underlying motility disorder and are due to pulsion. Manometry is helpful to define the extent of Manometry is helpful to define the extent of
myotomy myotomy Surgical intervention for large (> 5 cm) and Surgical intervention for large (> 5 cm) and
symptomatic diverticulumsymptomatic diverticulum Buttress repair with pleura, pericardial fat or Buttress repair with pleura, pericardial fat or
omentumomentum

Esophagus Lecture Part 2Esophagus Lecture Part 2

Esophageal PerforationEsophageal Perforation
65 yr old female with achalasia complains of back 65 yr old female with achalasia complains of back pain after pneumatic dilation. The CXR is pain after pneumatic dilation. The CXR is normal post procedure. The next best course of normal post procedure. The next best course of action is:action is:
1.1. Repeat endoscopy to identify any mucosal injuryRepeat endoscopy to identify any mucosal injury
2.2. VATS/or thoracotomy and operative repair as you VATS/or thoracotomy and operative repair as you suspect an esophageal perforationsuspect an esophageal perforation
3.3. Infectious disease consult for the prompt Infectious disease consult for the prompt administration of antibiotic therapyadministration of antibiotic therapy
4.4. Contrast study of the esophagusContrast study of the esophagus
5.5. Admit to ICU, IV hydration. If stable and CXR Admit to ICU, IV hydration. If stable and CXR normal, upper GI endoscopy or gastrografin swallow normal, upper GI endoscopy or gastrografin swallow the next morningthe next morning

Esophageal PerforationEsophageal Perforation
Common Causes of Esophageal PerforationCommon Causes of Esophageal Perforation Endoscopy, esophageal dilation, NG tube Endoscopy, esophageal dilation, NG tube
insertion, traumainsertion, trauma Operative procedures associated with Operative procedures associated with
perforation: anterior spine surgery (cervical), perforation: anterior spine surgery (cervical), gastric fundoplication, thyroidectomy, gastric fundoplication, thyroidectomy, pneumonectomypneumonectomy
Common Sites of Esophageal PerforationCommon Sites of Esophageal Perforation Cricopharyngeus, aortic knob, gastro esophageal Cricopharyngeus, aortic knob, gastro esophageal
junctionjunction

Esophageal PerforationEsophageal PerforationPresentation and DiagnosisPresentation and Diagnosis
Differential diagnosis includes myocardial infarction, pancreatitis, Differential diagnosis includes myocardial infarction, pancreatitis, perforated peptic ulcer disease, aortic dissection, acute gastric perforated peptic ulcer disease, aortic dissection, acute gastric volvulusvolvulus
Symptoms vary depending on site, mechanism and interval to Symptoms vary depending on site, mechanism and interval to presentation. However, pain is the most common complaintpresentation. However, pain is the most common complaint
Fever, tachycardia, leucocytosis, subcutaneous emphysema and Fever, tachycardia, leucocytosis, subcutaneous emphysema and crepitus, dysphagia, pleural effusion, peritonitis, sepsiscrepitus, dysphagia, pleural effusion, peritonitis, sepsis
Rapid diagnosis is the key: mortality of untreated esophageal Rapid diagnosis is the key: mortality of untreated esophageal perforation increases from 10-20% to 40-60% after the first 24 hoursperforation increases from 10-20% to 40-60% after the first 24 hours
CXR: mediastinal emphysema, pleural effusion, hydropneumothoraxCXR: mediastinal emphysema, pleural effusion, hydropneumothorax Gastrografin swallow (10% missed injuries), followed by thin bariumGastrografin swallow (10% missed injuries), followed by thin barium CT may be helpful in equivocal cases and to help guide non-operative CT may be helpful in equivocal cases and to help guide non-operative
treatmenttreatment

Esophageal PerforationEsophageal Perforation
When to Manage an Esophageal Perforation Non-When to Manage an Esophageal Perforation Non-Operatively?Operatively?
Minimal SymptomsMinimal Symptoms Contrast study shows small, contained leakContrast study shows small, contained leak1.1. About 25% of esophageal perforations meet About 25% of esophageal perforations meet
this criterionthis criterion2.2. Lower tolerance of conservative management Lower tolerance of conservative management
with thoracic and abdominal vs cervical with thoracic and abdominal vs cervical perforationsperforations
3.3. All patients must be admitted to a monitored All patients must be admitted to a monitored setting with initiation of hydration, antibiotics setting with initiation of hydration, antibiotics and monitoring of urine outputand monitoring of urine output

Esophageal PerforationEsophageal Perforation
Operative Management of Cervical PerforationOperative Management of Cervical Perforation Drainage usually is sufficientDrainage usually is sufficient Incision made anterior to the sternocleidomastoid Incision made anterior to the sternocleidomastoid
musclemuscle Mediastinoscopy can be used to drain the middle Mediastinoscopy can be used to drain the middle
mediastinummediastinum Neck drained with closed suction or penrose drainsNeck drained with closed suction or penrose drains Direct operative repair if perforation easily Direct operative repair if perforation easily
localizedlocalized May be combined with thoracic drainage if May be combined with thoracic drainage if
extensive mediastinal and pleural soilage presentextensive mediastinal and pleural soilage present

Esophageal PerforationEsophageal PerforationOperative Management of Thoracic PerforationOperative Management of Thoracic Perforation Most cases can be primarily repaired. Upper 2/3 approached Most cases can be primarily repaired. Upper 2/3 approached
via right 5via right 5thth intercostal space and lower 1/3 via left 7 intercostal space and lower 1/3 via left 7thth intercostal spaceintercostal space
Must debride all necrotic muscle and identify the mucosa. Must debride all necrotic muscle and identify the mucosa. Mucosa closed as a separate layer (4-0 vicryl). Close muscle Mucosa closed as a separate layer (4-0 vicryl). Close muscle over the repair if possible. Reinforce with intercostal, pleural over the repair if possible. Reinforce with intercostal, pleural or pericardial flapor pericardial flap
Widely open the mediastinal pleura and drain the pleural cavityWidely open the mediastinal pleura and drain the pleural cavity NG drainage for 7 days, followed by a contrast studyNG drainage for 7 days, followed by a contrast study
1.1. Esophageal exclusion should rarely be used primarilyEsophageal exclusion should rarely be used primarily
2.2. Esophagectomy reserved if there is an underlying malignancy Esophagectomy reserved if there is an underlying malignancy or with end-stage achalasiaor with end-stage achalasia
3.3. The use of esophageal stent is controversial, but very promisingThe use of esophageal stent is controversial, but very promising

Paraesophageal HerniasParaesophageal Hernias OrganoaxialOrganoaxial stomach rotates about its longitudinal stomach rotates about its longitudinal MesoaxialMesoaxial stomach rotates about a line perpendicular to the stomach rotates about a line perpendicular to the
cardiopyloric linecardiopyloric line
ClassificationClassificationType I: Sliding, fundus only, 1-5 cm, no rotationType I: Sliding, fundus only, 1-5 cm, no rotationType II: True Paraesophageal, fundus/body, 1-5 cm, organoaxial Type II: True Paraesophageal, fundus/body, 1-5 cm, organoaxial
rotationrotationType III: Mixed, fundus and body, ½ or more of stomach, Type III: Mixed, fundus and body, ½ or more of stomach,
organoaxial and mesoaxial rotationorganoaxial and mesoaxial rotationType IV: Mixed with other organs, fundus and body plus other Type IV: Mixed with other organs, fundus and body plus other
organs, ½ or more of stomach and colon, organoaxial and organs, ½ or more of stomach and colon, organoaxial and mesoaxial rotationmesoaxial rotation

Paraesophageal HerniasParaesophageal Hernias
Symptoms and SignsSymptoms and Signs 50% are asymptomatic, although minor 50% are asymptomatic, although minor
symptoms are usually overlookedsymptoms are usually overlooked Typical symptoms include epigastric pain, post-Typical symptoms include epigastric pain, post-
prandial discomfort in the chest, heartburn, prandial discomfort in the chest, heartburn, regurgitation, vomiting, weight loss, dyspnearegurgitation, vomiting, weight loss, dyspnea
Important signs include anemia, pneumoniaImportant signs include anemia, pneumonia An incarcerated intrathoracic stomach is a An incarcerated intrathoracic stomach is a
surgical emergency. These patients present with surgical emergency. These patients present with acute chest or epigastric pain and retching, but acute chest or epigastric pain and retching, but the inability to vomitthe inability to vomit

Paraesophageal HerniasParaesophageal Hernias
DiagnosisDiagnosis CXR shows a retro cardiac air bubble, with or CXR shows a retro cardiac air bubble, with or
without an air fluid levelwithout an air fluid level Barium swallow confirms the diagnosis and Barium swallow confirms the diagnosis and
usually shows a large, intrathoracic upside down usually shows a large, intrathoracic upside down stomachstomach
Endoscopy helpful to evaluate for ulcers, Endoscopy helpful to evaluate for ulcers, Barrett’s and neoplasmsBarrett’s and neoplasms
Esophageal motility studies helpful in an elective Esophageal motility studies helpful in an elective setting to help guide decisions regarding a wrapsetting to help guide decisions regarding a wrap

Paraesophageal HerniasParaesophageal Hernias
TreatmentTreatment
All patients with symptoms or signs should undergo All patients with symptoms or signs should undergo elective repair in the absence of prohibitive elective repair in the absence of prohibitive surgical risksurgical risk
Approaches include transthoracic, abdominal or laparoscopicApproaches include transthoracic, abdominal or laparoscopic Transthoracic approach provides the ability to mobilize the Transthoracic approach provides the ability to mobilize the
esophagus, relative ease of dissection of the hernia sac, and esophagus, relative ease of dissection of the hernia sac, and optimal exposure for secure crural closure. A Collis gastroplasty optimal exposure for secure crural closure. A Collis gastroplasty can also easily be performedcan also easily be performed
The main advantage of the abdominal approach is the ability to The main advantage of the abdominal approach is the ability to place the stomach in the appropriate anatomic orientation place the stomach in the appropriate anatomic orientation
Laparoscopy is associated with 5-8% incidence of esophageal Laparoscopy is associated with 5-8% incidence of esophageal perforation, and higher recurrence rate than the open procedureperforation, and higher recurrence rate than the open procedure

Paraesophageal HerniasParaesophageal Hernias
TreatmentTreatment
All patients with symptoms or signs should All patients with symptoms or signs should undergo elective repair in the absence of undergo elective repair in the absence of prohibitive surgical riskprohibitive surgical risk
Need for esophageal mobilization and Need for esophageal mobilization and lengtheninglengthening
The importance of sac excisionThe importance of sac excision The role of gastrostomy and gastropexyThe role of gastrostomy and gastropexy The need for mesh in crural repairThe need for mesh in crural repair

Caustic IngestionCaustic Ingestion
A 7 year old boy swallowed some ammonia (glass A 7 year old boy swallowed some ammonia (glass cleaner). He is crying, complaining of pain and cleaner). He is crying, complaining of pain and is drooling. Which of the following is true:is drooling. Which of the following is true:
1.1. The patient should immediately be intubated to The patient should immediately be intubated to secure his airwaysecure his airway
2.2. Endoscopy is contraindicated, as it could exacerbate Endoscopy is contraindicated, as it could exacerbate the injurythe injury
3.3. Sodium hypochlorite (bleach) ingestion has the Sodium hypochlorite (bleach) ingestion has the highest likelihood of perforationhighest likelihood of perforation
4.4. Gastrografin swallow is performed at 3 weeks and Gastrografin swallow is performed at 3 weeks and helps guide dilation of strictureshelps guide dilation of strictures
5.5. Steroids help decrease the incidence of stricturesSteroids help decrease the incidence of strictures

Gastroesophageal Reflux Gastroesophageal Reflux DiseaseDisease
True statements regarding an abdominal approach True statements regarding an abdominal approach versus a thoracic approach to anti-reflux versus a thoracic approach to anti-reflux surgery include:surgery include:
1.1. A Collis gastroplasty for a shortened esophagus is A Collis gastroplasty for a shortened esophagus is easier performed through the abdomeneasier performed through the abdomen
2.2. Large hernias are easier repaired laparoscopically Large hernias are easier repaired laparoscopically with better resultswith better results
3.3. Redo operations are better performed through the Redo operations are better performed through the abdomenabdomen
4.4. There is a lower incidence of esophageal perforationThere is a lower incidence of esophageal perforation
5.5. The Nissen repair is easier performed The Nissen repair is easier performed transabdominallytransabdominally

Gastroesophageal Reflux Gastroesophageal Reflux DiseaseDisease
Preoperative Work-upPreoperative Work-up
1) esophagogastroduodenoscopy 1) esophagogastroduodenoscopy
2) esophageal manometric evaluation. 2) esophageal manometric evaluation.
3) 24-hour intraesophageal pH monitoring3) 24-hour intraesophageal pH monitoring
4) barium cineradiography4) barium cineradiography

Gastroesophageal Reflux Gastroesophageal Reflux DiseaseDisease
Indications for SurgeryIndications for Surgery Surgical therapy should be considered in those individuals with Surgical therapy should be considered in those individuals with
documented GERD who:documented GERD who:
1) have failed medical management1) have failed medical management2) opt for surgery despite successful medical management 2) opt for surgery despite successful medical management
(due to life style considerations including age, time or (due to life style considerations including age, time or expense of medications, etc.)expense of medications, etc.)
3) have complications of GERD (e.g. Barrett's esophagus; 3) have complications of GERD (e.g. Barrett's esophagus; grade III or IV esophagitis)grade III or IV esophagitis)
4) have medical complications attributable to a large hiatal 4) have medical complications attributable to a large hiatal hernia. (e.g. bleeding, dysphagia)hernia. (e.g. bleeding, dysphagia)
5) have "atypical" symptoms (asthma, hoarseness, cough, 5) have "atypical" symptoms (asthma, hoarseness, cough, chest pain, aspiration) and reflux documented on 24 hour chest pain, aspiration) and reflux documented on 24 hour pH monitoringpH monitoring

Gastroesophageal Reflux Gastroesophageal Reflux DiseaseDisease
Types of Repairs:Types of Repairs: NissenNissen HillHill ToupetToupet DorDor Belsey Mark IVBelsey Mark IV Collis GastroplastyCollis Gastroplasty

Barrett’s EsophagusBarrett’s Esophagus False statements regarding Barrett’s False statements regarding Barrett’s
esophagus include:esophagus include:1.1. 20-40% of patients with severe dysplasia will have 20-40% of patients with severe dysplasia will have
invasive carcinoma in the resected specimeninvasive carcinoma in the resected specimen2.2. The likelihood of developing cancer in the first 3-5 The likelihood of developing cancer in the first 3-5
years after severe dysplasia has been identified is years after severe dysplasia has been identified is 25-50%25-50%
3.3. The ideal therapy for Barrett's with severe dysplasia The ideal therapy for Barrett's with severe dysplasia is endoscopic laser ablation of the mucosa and an is endoscopic laser ablation of the mucosa and an anti-reflux procedureanti-reflux procedure
4.4. The ideal therapy for uncomplicated Barrett's The ideal therapy for uncomplicated Barrett's esophagus is controversialesophagus is controversial
5.5. It is a premalignant condition and occurs in 10% of It is a premalignant condition and occurs in 10% of all patients with refluxall patients with reflux

Esophageal CancerEsophageal Cancer 14,000 new cases each year, more common in 14,000 new cases each year, more common in
menmen Adenocarcinoma now represents about 60-70% Adenocarcinoma now represents about 60-70%
of these tumorsof these tumors
PresentationPresentation
1.1. 90% present with dysphagia90% present with dysphagia
2.2. 70% present with weight loss70% present with weight loss
3.3. 50% present with substernal or epigastric pain50% present with substernal or epigastric pain
4.4. Hoarseness is rareHoarseness is rare

Esophageal CancerEsophageal Cancer
Role of EUS in T Stage AssessmentRole of EUS in T Stage Assessment Esophageal carcinoma presents as a hypo echoic mass Esophageal carcinoma presents as a hypo echoic mass
that disrupts the normal anatomy of the esophagusthat disrupts the normal anatomy of the esophagus Accuracy for assessing depth of tumor penetration is Accuracy for assessing depth of tumor penetration is
85-90%85-90%
Role of EUS in N Stage AssessmentRole of EUS in N Stage Assessment Hypo echoic nodes, sharply demarcated and larger Hypo echoic nodes, sharply demarcated and larger
than 5 mm are likely to be malignantthan 5 mm are likely to be malignant Accuracy for overall N stage accuracy is 77%. FNA Accuracy for overall N stage accuracy is 77%. FNA
added to EUS increases the accuracy to 91%added to EUS increases the accuracy to 91%

Esophageal CancerEsophageal Cancer
PET/CT now widely used for pre operative PET/CT now widely used for pre operative assessmentassessment
Bronchoscopy is done if tracheal or Bronchoscopy is done if tracheal or bronchial involvement is suggestedbronchial involvement is suggested

Esophageal CancerEsophageal Cancer
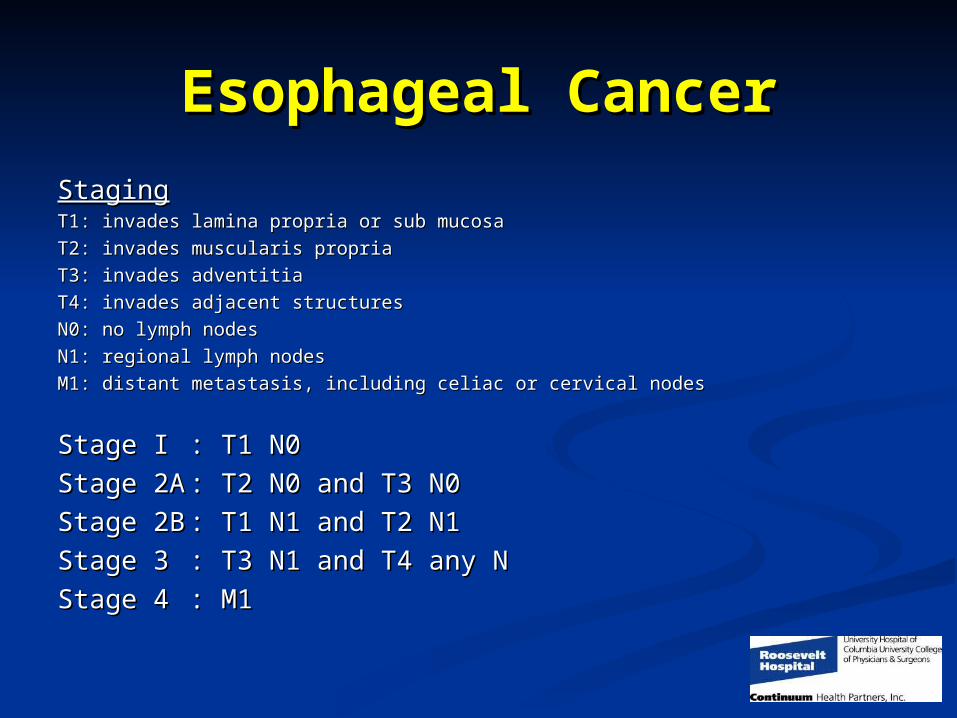
StagingStaging
T1: invades lamina propria or sub mucosaT1: invades lamina propria or sub mucosa
T2: invades muscularis propriaT2: invades muscularis propria
T3: invades adventitiaT3: invades adventitia
T4: invades adjacent structuresT4: invades adjacent structures
N0: no lymph nodesN0: no lymph nodes
N1: regional lymph nodesN1: regional lymph nodes
M1: distant metastasis, including celiac or cervical nodesM1: distant metastasis, including celiac or cervical nodes
Esophageal CancerEsophageal Cancer
StagingStagingT1: invades lamina propria or sub mucosaT1: invades lamina propria or sub mucosa
T2: invades muscularis propriaT2: invades muscularis propria
T3: invades adventitiaT3: invades adventitia
T4: invades adjacent structuresT4: invades adjacent structures
N0: no lymph nodesN0: no lymph nodes
N1: regional lymph nodesN1: regional lymph nodes
M1: distant metastasis, including celiac or cervical nodesM1: distant metastasis, including celiac or cervical nodes
Stage IStage I : T1 N0: T1 N0
Stage 2AStage 2A : T2 N0 and T3 N0: T2 N0 and T3 N0
Stage 2BStage 2B : T1 N1 and T2 N1: T1 N1 and T2 N1
Stage 3Stage 3 : T3 N1 and T4 any N: T3 N1 and T4 any N
Stage 4Stage 4 : M1: M1

Esophageal CancerEsophageal Cancer
Neoadjuvant TherapyNeoadjuvant Therapy 5 yr survival with surgery alone is 25%5 yr survival with surgery alone is 25% Although 7 randomized trials have been done, Although 7 randomized trials have been done,
only one 1996 study (Walsh) shows a survival only one 1996 study (Walsh) shows a survival benefit at 3 yearsbenefit at 3 years
We employ neoadjuvant therapy for Stage 2B or We employ neoadjuvant therapy for Stage 2B or higherhigher
Chemotherapy is 5FU and CisplatinChemotherapy is 5FU and Cisplatin Radiation is about 40GRadiation is about 40G

Esophageal CancerEsophageal Cancer
Surgical ApproachesSurgical Approaches Transhiatal esophagectomyTranshiatal esophagectomy Ivor-Lewis esophagectomyIvor-Lewis esophagectomy Esophagectomy with cervical Esophagectomy with cervical
anastomosisanastomosis Thoracoabdominal with left chest Thoracoabdominal with left chest
anastomosisanastomosis

Esophageal CancerEsophageal Cancer Regarding esophageal cancer and its Regarding esophageal cancer and its
management, which statement is false:management, which statement is false:
1.1. Its incidence is rising in the USIts incidence is rising in the US
2.2. Preoperative workup should include EUS, Preoperative workup should include EUS, PET/CT and PFT’sPET/CT and PFT’s
3.3. Neoadjuvant treatment is the standard of care for Neoadjuvant treatment is the standard of care for T2, N0 esophageal cancerT2, N0 esophageal cancer
4.4. There is no significant difference in survival There is no significant difference in survival between the transhiatal or transthoracic between the transhiatal or transthoracic approachapproach
5.5. The leak rate is higher with the transhiatal The leak rate is higher with the transhiatal approachapproach