essential physical health provider communication … · essential physical health provider...
TRANSCRIPT
Essential Physical Health Provider Communication Update 12.13.2017 Page 1 of 9
Essential Physical Health Provider
Communication Meeting Agenda
Logistics Time: 1:00PM – 2:00PM Date: Wednesday, December 13, 2017 Invitees: Physical Health Provider Agencies Teleconference Details:
https://goto.webcasts.com/starthere.jsp?ei=1173429&tp_key=d3f7cba6a6
Meeting Purpose: Cenpatico updates, technical assistance
Location: Webcast Questions: Feel free to email questions and agenda items to [email protected]
Next Meeting: 1/10/2018
Table of Contents Contracts Updates: .................................................................................................................... 2
Teri Krantz (Director of Contracting) ............................................................................ 2
Integrated Care Updates: ........................................................................................................... 3
Linda M. Reiter, Provider Relations Specialist ............................................................. 3
Debbie Yancer (Grant Writer) ...................................................................................... 4
Pharmacy Updates: ................................................................................................................... 5
Kathleen Bryant (Pharmacy Administrator) .................................................................. 5
Training Updates: ....................................................................................................................... 6
Rodney Staggers (Sr. Manager of Workforce & Training Development) ...................... 6
Essential Physical Health Provider Communication Update 12.13.2017 Page 2 of 9
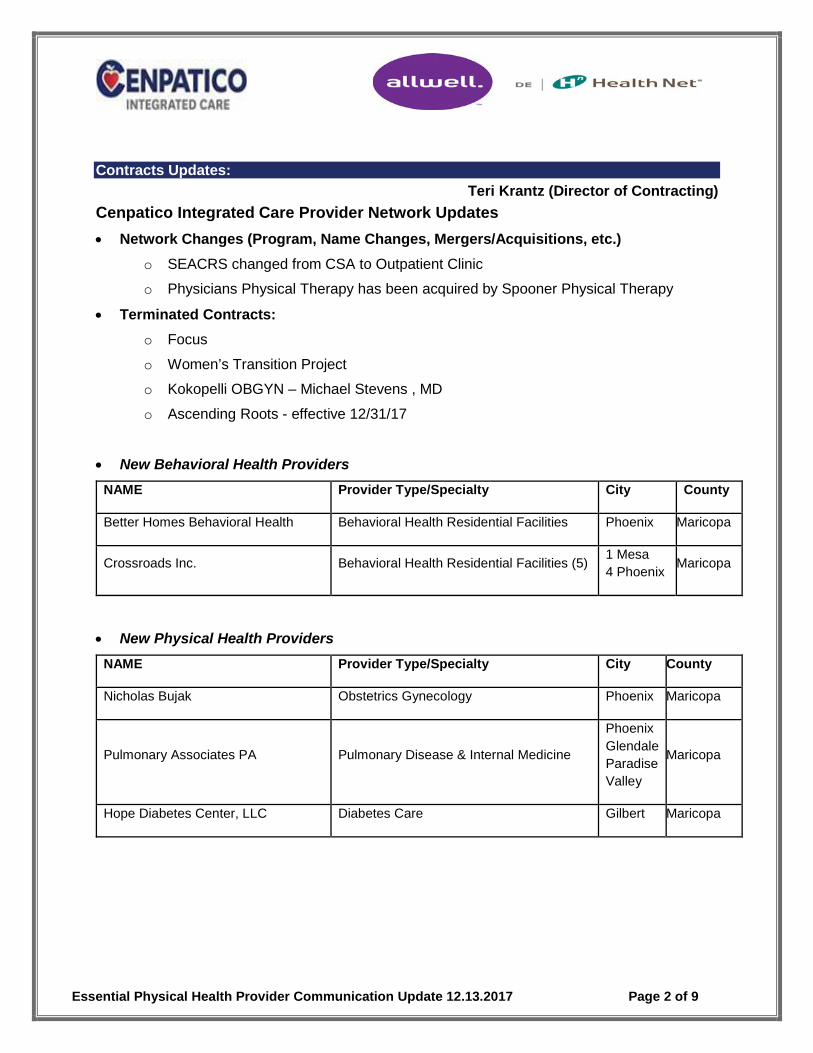
Contracts Updates: Teri Krantz (Director of Contracting)
Cenpatico Integrated Care Provider Network Updates • Network Changes (Program, Name Changes, Mergers/Acquisitions, etc.)
o SEACRS changed from CSA to Outpatient Clinic
o Physicians Physical Therapy has been acquired by Spooner Physical Therapy
• Terminated Contracts: o Focus
o Women’s Transition Project
o Kokopelli OBGYN – Michael Stevens , MD
o Ascending Roots - effective 12/31/17
• New Behavioral Health Providers NAME Provider Type/Specialty City County
Better Homes Behavioral Health Behavioral Health Residential Facilities Phoenix Maricopa
Crossroads Inc. Behavioral Health Residential Facilities (5) 1 Mesa 4 Phoenix Maricopa
• New Physical Health Providers NAME Provider Type/Specialty City County
Nicholas Bujak Obstetrics Gynecology Phoenix Maricopa
Pulmonary Associates PA Pulmonary Disease & Internal Medicine
Phoenix Glendale Paradise Valley
Maricopa
Hope Diabetes Center, LLC Diabetes Care Gilbert Maricopa
Essential Physical Health Provider Communication Update 12.13.2017 Page 3 of 9
Integrated Care Updates: Linda M. Reiter (Provider Relations Specialist)
(Attachments 01-07)
Health Current Updates (1 attachment)
• Health Current Connection to the Prescription Monitoring Program (PMP) Database
o The PMP Database must be checked prior to prescribing opioid or benzodiazepine medications.
o The PMP Database can now be accessed through Health Current.
o To learn more register to attend a webinar demonstration on December 7, 2017, from 12:00pm to 1:00pm, at https://healthcurrent.org/news-events/events/webinar-users-able-comply-pmp-mandate-hie-portal/
• Health Current’s HIE Monthly Webinar Fees and Live Demo
o If you are new to Health Current or your agency has not yet considered connecting to Health Current please register for a live a demonstration on December 27, 2017, from 12:00pm to 1:00pm, at https://www.eventbrite.com/e/health-current-hie-monthly-webinar-fees-live-demo-december-27-at-1200pm-registration-30707154927
ACOM and AMPM Updates (2 attachments)
• Please review the two attachments for the most recent revisions to various ACOM and AMPM Policies. These attachments can be found at the below links:
o https://www.azahcccs.gov/shared/ACOM/
o https://www.azahcccs.gov/shared/MedicalPolicyManual/
• Things to note include reporting requirements for IMD Stays greater than 15 days in ACOM Policy 109.
• AMPM Exhibit 300-1 added new covered services for emergency dental and outpatient occupational therapy as a result of Senate Bill 1527.
• AMPM Policy 320-R was revised to include ALTCS/EPD and Tribal ALTCS into the policy. There is also a new fillable PDF to use.
• AMPM Policy 1060 for Training Requirements was also revised to eliminate mandatory 90 day training requirements.
Appointment Availability Changes (1 attachment)
• Effective 10/1/17 there were changes made to the Appointment Availability Standards per ACOM 417 which is attached.
Essential Physical Health Provider Communication Update 12.13.2017 Page 4 of 9
• Please review the attached policy, train staff regarding the appointment standards and update provider policies and desktops accordingly.
• Cenpatico will continue to conduct quarterly appointment availability telephonic surveys and quarterly onsite reviews of available appointments in accordance to these standards.
• Providers not meeting the standards will receive Corrective Actions.
Important Screenings and HEDIS Measures (2 attachments)
• Breast Cancer Screening measure is defined as the percentage of patients who had a mammogram to screen for breast cancer. The attached communication outlines the patient parameters, the measurement year, what the documentation should contain, the billing codes that can be utilized and the exclusions.
• The Colorector Cancer Screening measure is defined as the percentage of patients who had a screening. Like the above communication this communication outlines the appropriate screenings and time frames for the colorectal cancer screenings, the codes that can be utilized, exclusions and how to document or demonstrate completion of this measure.
• Please be sure to share with staff across the various levels of your organization to facilitate conversations with members about receiving these life-saving screenings.
AHCCCS MCO Survey (1 attachment)
• AHCCCS is conducting a survey to assess the MCO’s performance and responsiveness to its providers and your input and time would be much appreciated.
• A formal communication from Cenpatico Integrated Care was sent out via email on 12/1/17, including the attached memo.
• To participate in the survey please click on the following link: https://www.surveymonkey.com/r/AHCCCSProviderSurvey2017
Debbie Yancer (Grant Writer) (Attachment 08)
Cenpatico Integrated Care Provider Manual Updates
• The Cenpatico Integrated Care Provider Manual has been updated effective 12/1/2017. Attached is the Summary of Changes that have been made to the manual.
• Acronyms will continue to be spelled out to support clarity of understanding.
• The final version, a redline version, and the Summary of Changes have been posted to the Cenpatico Integrated Care website
Essential Physical Health Provider Communication Update 12.13.2017 Page 5 of 9
at: https://www.cenpaticointegratedcareaz.com/providers/provider-resources/provider-manual.html
• Provider Manual forms, attachments, and deliverable templates are also on the Cenpatico Integrated Care website at: https://www.cenpaticointegratedcareaz.com/providers/provider-resources/provider-forms.html
Pharmacy Updates:
Kathleen Bryant (Pharmacy Administrator)
Cenpatico Integrated Care Pharmacy Updates
• Comprehensive Drug list changes effective 12/11/17
o Glucose Test Strips
Changing to True Metrix test strips as the preferred test strip
Impacted members will receive a letter of notification and a coupon for a True Metrix Meter at no cost to them.
True Metrix strips will be allowed as follows:
• Max of 100/90 days for non-insulin users
• Max of 150/30 days for insulin users
All other meters and quantities for strips will require prior authorization
Medicare Members will be allowed to continue using their current brand of test strips and quantities without prior authorization
• Comprehensive Drug list changes effective 1/1/18. Will post on the webpage by 1/1/18.
o Mavyret – Only preferred product for the treatment of Hepatitis C
Revision of the HEP C criteria is pending
o Long-Acting Opioids
Remove Hysingla ER (current utilizers will be grandfathered to continue)
Remove OxyContin ER (current utilizers will NOT be grandfathered)
Adding Xtampza ER with prior authorization
o Short-Acting opioids moving from a 7 day supply to a 5 day supply for opioid naïve members.
o Self-injected Epinephrine - note generic Epi-Pen added
• Prior Authorization Request Forms – Process Change
Essential Physical Health Provider Communication Update 12.13.2017 Page 6 of 9
o In order to meet the 24 hour turn-around time for outpatient medication prior authorization requests effective 1/1/18, we are changing our process to ensure adequate response time.
o Please fax the following requests to Envolve Pharmacy Solutions at 866-399-0929
PMF_10-11-1 Medication Prior Authorization Request
PMF_10-11-2 Specialty Medication Prior Authorization Request
PMF_10-11-4 Makena Prior Authorization Request-Prescription Request
PMF_10-11-5 Long Acting Opioid Prior Authorization Request
o Please continue to fax the following form to Cenpatico IC at 855-766-1554
PMF)10-11-3 Exclusive Pharmacy Prescriber Request
• Specialty Pharmacy Change effective 12/1/17
o AcariaHealth is our preferred vendor for all specialty drugs
o Genoa/QoL Pharmacies will also be preferred for long-acting injectable antipsychotics and Vivitrol
o There will be no changes to the member’s benefits or copayments at this time
• Educational Resource o www.PSYCHU.org
Access thousands of mental health resources Create a login and password No cost to the end user
Provider Education Updates: Rodney Staggers (Sr. Manager of Workforce & Training Development)
Live Conferences
• 15th Annual Nutrition & Health Conference - This conference provides an overview and practical summary of the latest information on nutrition and health presented by leaders in scientific research, clinicians skilled in nutritional medicine, experts on food and agricultural policy, and innovative chefs, May 2, 2018, Location: Boston, MA: Westin Boston Waterfront, CME Credits: 18.25
Online and Enduring Materials
• A Clinician's Guide to Sexual Assault - Describe the changing legal environment surrounding rape and sexual assault.
o Manage patient concerns and law enforcement issues that arise in cases of sexual assault.
o Work with trained sexual assault nurse examiners.
Essential Physical Health Provider Communication Update 12.13.2017 Page 7 of 9
o Perform an appropriate forensic examination.
o Arrange for necessary medical treatment and follow-up of sexual assault victims.
o CME:2 hours, fee $50, register at https://www.vlh.com/shared/courses/course_info.cfm?courseno=146
• Accident or Injury? Managing Abuse in Younger Children – Perform appropriate medical evaluations for suspected abuse, including:
o Obtaining an accurate history.
o Performing a comprehensive physical exam.
o Differentiating between accidental and non-accidental injury.
o Documenting your assessment accurately and comprehensively.
o Ordering the appropriate screening tests based on clinical presentation.
o Apply your role as a mandated reporter to identify and report cases of suspected child maltreatment to the appropriate agencies.
o Effectively communicate with investigative agencies in child maltreatment cases.
o CME: 2 hours, fee $50, register at https://www.vlh.com/shared/courses/course_info.cfm?courseno=166
• Introduction to the Practice of Palliative Medicine – Objectives:
o Manage difficult symptoms commonly seen in palliative care and end-of-life patients.
o Communicate bad news effectively.
o Coordinate palliative care between professionals and across institutional settings.
o Refer a patient for hospice and end-of-life care.
o CME: 1 hour, fee $25, register at https://www.vlh.com/shared/courses/course_info.cfm?courseno=125
• Communicating Through Healthcare Interpreters – Objectives:
o Identify and avoid the potential consequences of using unqualified interpreters (including family members, children, and untrained bilingual staff), including:
Decreased quality of care
Limited access to care, resulting in civil rights violations, accreditation issues, and professional liability
Increased cost of care
o Perform the following when working with an interpreter:
Greet patients appropriately
Perform an appropriate pre-session with the interpreter
Establish the role of the interpreter with the patient
Essential Physical Health Provider Communication Update 12.13.2017 Page 8 of 9
Establish rapport with the patient through the interpreter
Position the interpreter effectively vis-à-vis the patient
Address the patient directly
Modify speech patterns to optimize the accuracy of the interpretation
Ensure that patients know what is being discussed if you need to speak directly with the interpreter
Guide an untrained interpreter
o Propose strategies to address the following issues when working with Limited English Proficient (LEP) patients:
Track language needs
Evaluate your own and your staff's level of language capacity
Choose an appropriate interpreter given different circumstances
Use an interpreter as a culture broker
o Employ the following in mental health settings:
Factor cultural differences into an assessment of abnormal behavior and appropriate development
Identify and manage secondary trauma in interpreters
Adapt the use of standardized testing instruments appropriately across languages
CME: 2 hours, fee: $50, register at https://www.vlh.com/shared/courses/course_info.cfm?courseno=155
o Current Management of Domestic Violence - Responding to IPV, Objectives:
• Screen patients for intimate partner violence (IPV) and appropriately respond to disclosures of abuse.
• Recognize patterns of abuse and properly document IPV.
• Assess the safety of IPV victims.
• Report and refer IPV victims to appropriate community agencies.
• Recognize and support patients' readiness to change their violent situation
• CME: up to 16 hours, fee $25, register at https://www.vlh.com/shared/courses/course_info.cfm?courseno=1762
Live Workshops
• Advanced Disaster Preparedness & Response (ADPR), 4/19/2018, 1:00 PM, Herbert K. Abrams Public Health Building, 3950 S Country Club Rd. Suite 200 Room 3102, Tucson, AZ,
Essential Physical Health Provider Communication Update 12.13.2017 Page 9 of 9
CME: 4, fee $178, contact Jennifer Ronnebaum at 520 626-2305 or [email protected].

Douglas A. Ducey, Governor Thomas J. Betlach, Director
801 East Jefferson, Phoenix, AZ 85034 • PO Box 25520, Phoenix, AZ 85002 • 602-417-4000 • www.azahcccs.gov
DATE: November 15, 2017 TO: Holders of the AHCCCS Medical Policy Manual FROM: Contracts and Policy Unit
Division of Health Care Management, AHCCCS
SUBJECT: AHCCCS Medical Policy Manual (AMPM)
This memo describes revisions and/or additions to the AMPM. Please direct questions regarding policy updates to the Contracts and Policy Unit at 602-417-4295 or 602- 417-4055 or email at [email protected].
PLEASE NOTE: We are currently converting the AMPM Headers and Footers to a new format, aligning Policy language for consistency, and changing Exhibits to Attachments. Changes will be done over the next several months
UPDATES AND REVISIONS TO THE AHCCCS MEDICAL POLICY MANUAL (AMPM)
To view the policies and attachments, please access the following link:
AHCCCS MEDICAL POLICY MANUAL (AMPM)
CHAPTER 300, EXHIBIT 300-1, AHCCCS COVERED SERVICES ACUTE CARE AMPM Exhibit 300-1 was revised to align covered services and add new covered services, including an emergency dental benefit and outpatient occupational therapy, as a result of Senate Bill 1527. Post Tribal Consultation Notice/Public Comment period changes to AMPM Exhibit 300-1: • Changed term “Durable Medical Equipment,” to “Medical Equipment and Appliances” to
reflect current terminology. • Clarified outpatient Speech Therapy is covered for ALTCS members age 21 years and older,
stating, “See AMPM Policy 310-X Regarding Limitations.”
The effective date for this policy is 10/01/2017. CHAPTER 300, POLICY 310-N, LABORATORY AMPM Policy 310-N was revised to reflect AHCCCS best practice and to comply with HB 2419. Genetic Testing language was removed from this Policy to new stand-alone AMPM Policy 310-II, Genetic Testing. Clarification also added surrounding Clinical Laboratory Improvement Act (CLIA). The effective date for this policy is 10/01/2017.

Douglas A. Ducey, Governor Thomas J. Betlach, Director
801 East Jefferson, Phoenix, AZ 85034 • PO Box 25520, Phoenix, AZ 85002 • 602-417-4000 • www.azahcccs.gov
CHAPTER 300, POLICY 310-P, MEDICAL EQUIPMENT, MEDICAL APPLIANCES AND MEDICAL SUPPLIES The title for AMPM Policy 310-P, formerly Medical Supplies, Durable Medical Equipment and Orthotic/Prosthetic Devices was changed to Medical Equipment, Medical Appliances and Medical Supplies and was updated to comply with new Managed Care regulations, which requires a face-to-face evaluation of a FFS member’s need for medical equipment, appliances and supplies prior to the start of service. The regulations further required AHCCCS to ensure no absolute exclusions of medical equipment, appliances and supplies. AHCCCS also removed Orthotics and Prosthetics to a separate, stand-alone policy, and incorporated language from Retired AMPM Policies 1250-F and 310-EE. Finally, the Policy was streamlined for brevity and clarity. Post Tribal Consultation Notice/Public Comment period changes to AMPM Policy 310-P:
• Added Section B.6. to ensure appropriate coverage of customized medical equipment, stating, “The Contractor shall ensure the provider network includes a choice of vendors for customized medical equipment and corrective appliances for members with special healthcare needs. The Contractor shall include, in the contract with the vendor, timeliness standards for creation, repair and delivery of customized equipment and appliances. The Contractor shall monitor the standards and take action when the vendor is found to be out of compliance.”
The effective date for this policy is 10/01/2017. CHAPTER 300, POLICY 320-R, SPECIAL ASSISTANCE FOR MEMBERS DETERMINED TO HAVE A SERIOUS MENTAL ILLNESS AMPM Policy 320-R was revised to simplify, clarify and incorporate ALTCS/EPD and Tribal ALTCS into the Policy as a result of changes implemented with ALTCS/EPD RFP #YH18-0001. Attachment A was updated to include the same, and was replaced with a fillable .pdf version for ease of use. Further, the Policy was updated for consistency to align with AHCCCS Policy formatting and uniform language. The effective date for this policy is 10/01/2017. CHAPTER 1000, POLICY 1060, TRAINING REQUIREMENTS FOR RBHAS AND BEHAVIORAL HEALTH PROVIDERS AMPM Policy 1060 was updated to reflect current practices and personnel training requirements, as well as changes in other policies affecting AMPM Policy 1060. Policy was revised to eliminate the mandatory 90 day training requirement for all newly hired personnel. The Annual Workforce Development and Training Plan was modified to reflect the broader training and development needs of the workforce beyond initial orientation. Post Tribal Consultation Notice/Public Comment period changes to AMPM Policy 1060:

Douglas A. Ducey, Governor Thomas J. Betlach, Director
801 East Jefferson, Phoenix, AZ 85034 • PO Box 25520, Phoenix, AZ 85002 • 602-417-4000 • www.azahcccs.gov
• Corrected erroneous internal references in Section B.1.a, which read, “the in B.2.a Section One, b. Section Two and c. Section Three of this policy” to “the approved training content specified in B.1.d - Section One, B.1.e - Section Two and B.1.f.- Section Three, of this policy.”
• Updated citation in B.1.e, Section Two, from “ASAM PPC 2R” to “ASAM Criteria – Third Edition.”
• Clarified reference in B.1.f, Section Three, to “Confidentiality (Health Insurance Portability and Accountability Act (HIPAA),” adding “at 45 CFR Part 164, and Confidentiality of Substance Use Disorder Patient Records, at 42 CFR Part 2.”
• Removed Section B c. information was no longer needed the training requirements are broke donw in d. Section One, e. Section Two, and f. Section Three.
The effective date for this policy is 11/15/2017.
APPROVED NOT YET EFFECTIVE
To view the policies and attachments, please access the following link:
AMPM Approved Not Yet Effective
None at this time.

AHCCCS CONTRACTOR OPERATIONS MANUAL
CHAPTER 400 - OPERATIONS
417- Page 1 of 6
417 - APPOINTMENT AVAILABILITY, MONITORING AND REPORTING
EFFECTIVE DATES: 10/01/12, 10/01/13, 04/01/15, 07/01/16, 10/01/16, 10/01/17
REVISION DATES: 01/08/08, 06/26/12, 10/24/12, 07/03/13, 03/05/15, 04/02/15, 05/11/16,
10/20/16, 03/30/17, 06/15/17
I. PURPOSE
This Policy applies to Acute Care, ALTCS/EPD, CRS, DCS/CMDP (CMDP), DES/DDD
(DDD), and RBHA Contractors. The policy establishes appointment accessibility and
availability standards to ensure Contractor compliance with AHCCCS network sufficiency
requirements. The standards delineated in this policy establish a common process for
Contractors to monitor and report appointment accessibility and availability. These policy
requirements do not apply to emergency conditions
II. DEFINITIONS
1800 REPORT
ESTABLISHED
PATIENT
NEW PATIENT
URGENT CARE
APPOINTMENT
An AHCCCS generated document, provided quarterly, that
identifies Primary Care Physicians (PCPs) with a panel of more
than 1800 AHCCCS members.
A member who has received professional services from the
physician or any other physician with that specific subspecialty
that belongs to the same group practice, within the past three
years from the date of appointment.
A member who has not received any professional services from
the physician or another physician with that specific specialty
and subspecialty that belongs to the same group practice, within
the past three years from the date of appointment.
An appointment for medically necessary services to prevent
deterioration of health following the acute onset of an illness,
injury, condition, or exacerbation of symptoms.
III. POLICY
A. MONITORING APPOINTMENT STANDARDS
1. The Contractor is responsible for providing services that are sufficient in amount,
duration and scope to reasonably be expected to achieve the purpose for which the
services are furnished. To ensure this, the Contractor must provide a comprehensive
provider network that provides access to all services covered under the contract for all
members. If the Contractor’s network is unable to provide medically necessary
services required under contract, the Contractor must adequately and timely cover

AHCCCS CONTRACTOR OPERATIONS MANUAL
CHAPTER 400 - OPERATIONS
417- Page 2 of 6
these services through an out of network provider until a network provider is
contracted.
2. The Contractor must ensure adherence to service accessibility standards and the
following contractual appointment standards [42 CFR 438.206].
3. The Contractor must use the results of appointment standards monitoring to assure
adequate appointment availability in order to reduce unnecessary emergency
department utilization.
4. The Contractor shall have written policies and procedures about educating its provider
network regarding appointment time requirements. The Contractor must develop a
corrective action plan when appointment standards are not met. In addition, the
Contractor must develop a corrective action plan in conjunction with the provider
when appropriate [42 CFR 438.206(c)(1)(iv), (v) and (vi)].
B. GENERAL APPOINTMENT STANDARDS FOR ALL CONTRACTORS
1. For Primary Care Provider Appointments:
a. Urgent care appointments as expeditiously as the member’s health condition
requires but no later than two business days of request, and
b. Routine care appointments within 21 calendar days of request.
2. For Specialty Provider Referrals:
a. Urgent care appointments as expeditiously as the member’s health condition
requires but no later than three business days from the request, and
b. Routine care appointments within 45 calendar days of referral.
3. For Dental Provider Appointments:
a. Urgent appointments as expeditiously as the member’s health condition requires
but no later than three business days of request, and
b. Routine care appointments within 45 calendar days of request.
4. For Maternity Care Provider Appointments,
Initial prenatal care appointments for enrolled pregnant members shall be provided as
follows:
a. First trimester - within 14 calendar days of request,
b. Second trimester within seven calendar days of request,
c. Third trimester within three days business of request, and
d. High risk pregnancies as expeditiously as the member’s health condition requires
and no later than three business days of identification of high risk by the
Contractor or maternity care provider, or immediately if an emergency exists.

AHCCCS CONTRACTOR OPERATIONS MANUAL
CHAPTER 400 - OPERATIONS
417- Page 3 of 6
C. GENERAL BEHAVIORAL HEALTH APPOINTMENT STANDARDS FOR ACUTE,
ALTCS/EPD, CRS AND RBHA CONTRACTORS
1. For Behavioral Health Provider Appointments:
a. Urgent need appointments as expeditiously as the member’s health condition
requires but no later than 24 hours from identification of need
b. Routine care appointments:
i. Initial assessment within seven calendar days of referral or request for service,
ii. The first behavioral health service following the initial assessment as
expeditiously as the member’s health condition requires but no later than 23
calendar days after the initial assessment, and
iii. All subsequent behavioral health services, as expeditiously as the member’s
health condition requires but no later than 45 calendar days from identification
of need.
2. For Psychotropic Medications:
a. Assess the urgency of the need immediately, and
b. Provide an appointment, if clinically indicated, with a Behavioral Health Medical
Professional within a timeframe that ensures the member a) does not run out of
needed medications, or b) does not decline in his/her behavioral health condition
prior to starting medication, but no later than 30 calendar days from the
identification of need.
D. ADDITIONAL BEHAVIORAL HEALTH APPOINTMENT STANDARDS FOR
CRS AND RBHA
CONTRACTORS
1. For Behavioral Health Appointments for persons in legal custody of the Department
of Child Safety (DCS) and adopted children in accordance with A.R.S. §8-512.01:
a. Rapid Response when a child enters out-of-home placement within the timeframe
indicated by the behavioral health condition, but no later than 72 hours after
notification by DCS that a child has been or will be removed from their home,
b. Initial Assessment
within seven calendar days after referral or request for
behavioral health services,
c. Initial Appointment within timeframes indicated, by clinical need, but no later than
21 calendar days after the initial evaluation, and
d. Subsequent Behavioral Health Services within the timeframes according to the
needs of the person, but no longer than 21 calendar days from the identification of
need
The appointment standards for members in the legal custody of the Department of Child
Safety and adopted children are intended to monitor appointment accessibility and
availability. For additional information on behavioral health services for persons in the
legal custody of DCS and adopted children in accordance with A.R.S. §8-512.01, see
ACOM Policy 449.

AHCCCS CONTRACTOR OPERATIONS MANUAL
CHAPTER 400 - OPERATIONS
417- Page 4 of 6
E. PROVIDER APPOINTMENT AVAILABILITY REVIEW
The Contractor is required on a quarterly basis to conduct provider appointment availability
reviews to assess the availability of Routine and Urgent appointments for Primary Care,
Specialist, Dental, CRS providers, Behavioral Health providers and Behavioral Health
appointments for persons in the legal custody of DCS. The Contractor must also review
these standards for Maternity Care providers relating to the first, second, and third
trimesters, as well as high risk pregnancies.
The Contractor must conduct provider appointment availability reviews in sufficient
quantity to ensure results are meaningful and representative of the services provided by the
Contractor’s network. Appropriate methods include:
1. Appointment schedule review where the Contractor independently validates appointment
availability,
2. Secret shopper phone calls, where the Contractor anonymously validates appointment
availability, and
3. Other methods approved by AHCCCS.
The Contractor may supplement these efforts by targeting specific providers identified
through performance monitoring systems such as the 1800 report, quality of care concerns,
complaints, grievances and the credentialing process.
To obtain approval for any additional methods, the Contractor should submit a request for
approval outlining details (including scope, selection criteria, and any tools used to collect
the information) prior to implementing the proposed method, as specified in Contract,
Section F, Attachment F3, Contractor Chart of Deliverables and RBHA Contract, Exhibit-9,
Deliverables.
F. TRACKING AND REPORTING
The Contractor must track provider compliance with appointment availability on a quarterly
basis for both New and Established Patients by Provider Type and appointment type
utilizing the reporting template, Attachment A. The Contractor must submit this
information quarterly as identified in Contract, Section F, Attachment F3, Contractor Chart
of Deliverables and RBHA Contract, Exhibit-9, Deliverables. A cover letter must be
included which summarizes the data, describes how the survey methodology is
representative of appointment standards across the Contractor’s network, explains
significant trending in either direction (positive or negative), and describes any interventions
applied to areas of concern including, any corrective actions.
In addition, annually the Contractor must summarize the results, trends, and interventions as
a component of the Network Development and Management Plan. See ACOM Policy 415

AHCCCS CONTRACTOR OPERATIONS MANUAL
CHAPTER 400 - OPERATIONS
417- Page 5 of 6
for additional guidelines for the submission of the Network Development and Management
Plan.
The Contractor’s submission of the Network Development and Management Plan must also
include an attestation affirming the validity of the methodologies utilized and significance
of the results, along with any planned changes to the methodologies for the coming year.
AHCCCS may review Contractor monitoring and any corrective actions implemented as a
result of provider non-compliance with appointment standards.
G. ATTACHMENT A, APPOINTMENT AVAILABILITY PROVIDER REPORT
Instructions for Completing Attachment A, Appointment Availability Provider Report:
PCP, SPECIALIST, AND DENTAL APPOINTMENTS
SURVEYS Enter the number of provider surveys conducted both New and
Established patients for each provider type.
PASS Enter the total number of providers that were in compliance with
the AHCCCS appointment standards (Urgent and Routine).
FAIL Enter the total number of providers that were not in compliance
with the AHCCCS appointment standards.
COMPLIANCE
PERCENTAGE
The percentage of providers that are compliant with the AHCCCS
appointment standards. This field is automatically populated.
MATERNITY CARE PROVIDER APPOINTMENTS
SURVEYS Enter the number of provider surveys conducted with Maternity
care providers related to compliance with the AHCCCS standards
for initial prenatal care appointments by trimester and risk.
PASS Enter the total number of providers that were in compliance with
the AHCCCS appointment standards for maternity care.
FAIL Enter the total number of providers that were not in compliance
with the AHCCCS appointment standards for maternity care.
COMPLIANCE
PERCENTAGE
The percentage of providers that are compliant with the AHCCCS
appointment standards for maternity care. This field is
automatically populated.

AHCCCS CONTRACTOR OPERATIONS MANUAL
CHAPTER 400 - OPERATIONS
417- Page 6 of 6
BEHAVIORAL HEALTH, AND REPORT FOR PERSONS IN DCS CUSTODY
APPOINTMENTS
SURVEYS Enter the number of provider surveys conducted for each
behavioral health appointment category.
PASS Enter the total number of providers that were in compliance with
the AHCCCS appointment standards.
FAIL Enter the total number of providers that were not in compliance
with the AHCCCS appointment standards.
COMPLIANCE
PERCENTAGE
The percentage of providers that are compliant with the AHCCCS
appointment standards. This field is automatically populated.

Healthcare Effectiveness Data and Information Set (HEDIS) Colorectal Cancer Screening
What: The Colorectal Cancer Screening (COL) HEDIS measure is defined as the percentage of patients who had a colorectal cancer
screening.1
Why: Colorectal cancer is the second leading cause of cancer deaths in the United States. Colorectal cancer screenings can save
lives.2
Who: Patients ages 50–75.1
When: The table below specifies the appropriate screenings and time frames for colorectal cancer screening.
Test Time frame
Fecal occult blood test (gFOBT/FIT) (guaiac and immunochemical)
During the measurement year
Fecal immunological test (FIT)-DNA
During the measurement year or the two years prior
Computed tomography (CT) colonography
During the measurement year or the four years prior
Flexible sigmoidoscopy
During the measurement year or the four years prior
Colonoscopy
During the measurement year or the nine years prior
How: To report evidence of screening for this measure administratively, submission of any of the following CPT or HCPCS codes is
required. Please utilize current procedure codes as appropriate for flexible sigmoidoscopy, colonoscopy and CT colonography. For services performed elsewhere, document these services in the patient’s history section with test performed, date conducted and the result.
Test/Description CPT codes HCPCS codes
FIT-DNA 81528 G0464
FOBT 82270, 82274
G0328
Exclusions: Be sure to document and code appropriately for patients with a history of colorectal cancer or colectomy, which should be
excluded from this measure. Exclude Medicare patients ages 65 or older as of January 1 of the measurement year who are enrolled in an Institutional Special Needs Plan (I-SNP) or living long-term in an institution any time during the measurement year. Also exclude patients that are in hospice. Note this in the patient’s chart. Where: To demonstrate evidence of screening for this measure, documentation in the medical record must include patient name, date
of birth, date of service, and a note indicating the date (at least the year) of when the colorectal cancer screening was performed. A result is not required if the documentation is clearly part of the “medical history” section of the record.1
References 1NCQA’s HEDIS 2018 Technical Specifications for Health Plans, Volume 2, Washington, D.C., 2017. 2Centers for Disease Control and Prevention. Colorectal Cancer Screening. Retrieved from www.cdc.gov/cancer/colorectal/basic_info.index.html, August 28, 2017.

Healthcare Effectiveness Data and Information Set (HEDIS) Breast Cancer Screening
What: The Breast Cancer Screening (BCS) measure is defined as the percentage of patients who had a mammogram to screen for breast cancer.1
Why: Approximately 230,000 cases of breast cancer are diagnosed in women, and approximately 40,000 women die each year of breast cancer in the United States. Regular mammograms can reduce the risk of dying of breast cancer.2 Who: Female patients ages 50–74.1 When: October 1, two years prior to the measurement year, through December 31 of the measurement year.1
Where: Documentation in the medical record must include patient name, date of birth, date of service, and documentation of mammography with date of service completed (MM/YYYY), along with proof of completion versus merely ordered, to code for this measure.1 Note: All types and methods of mammograms (screening, diagnostic, film, digital, or digital breast tomosynthesis) meet the numerator compliance.1
How: The evidence of screening for this measure is captured administratively; therefore, correct coding with any of the following CPT, HCPCS and UBREV codes is required.
Exclusions: Document and code appropriately for patients with bilateral mastectomy any time during the patient’s history through December 31 of the measurement year.1 Any of the following meet criteria for bilateral mastectomy:
Bilateral mastectomy
Unilateral mastectomy with a bilateral modifier
Two unilateral mastectomies with service dates 14 days or more apart
Absence of the left breast and absence of the right breast on the same or different date of service
Both of the following (on the same or different date of service): o Unilateral mastectomy with a left-side modifier o Unilateral mastectomy with a right-side modifier
References 1NCQA’s HEDIS 2018 Technical Specifications for Health Plans, Volume 2, Washington, D.C., 2017. 2Centers for Disease Control and Prevention. Breast Cancer Statistics retrieved from www.cdc.gov/cancer/breast/statistics/index.htm, August 15, 2017.
Mammography
CPT HCPCS UBREV
77055 77061 77065 77056 77062 77066 77057 77063 77067
G0202 G0204 G0206
0401 0403
Exclusion Codes
CPT ICD-10-PCS ICD-10-PCM
Bilateral modifier: 50, 00950
Left modifier: LT
Right modifier: RT
Unilateral mastectomy: 19180, 19200, 19220, 19240, 19303, 19304, 19305, 19306, 19307
Bilateral mastectomy: 0HTV0ZZ
Unilateral mastectomy left: 0HTU0ZZ
Unilateral mastectomy right: 0HTT0ZZ
History of bilateral mastectomy: Z90.13
Absence of left breast: Z90.12
Absence of right breast: Z90.11

NEWS & ANNOUNCEMENTS | NOVEMBER, 15, 2017 | 1 PAGE |
THIS UPDATE APPLIES TO CENPATICO INTER-GRATED CARE PROVID-ERS:
Physicians
Medical Groups
Hospitals
Ancillary Providers
PROVIDER SERVICES 1-866-495-6738 www.cenpaticointegratedcareaz.com
PROVIDERUpdate
Health Current has become one of the primary tools for Arizona providers under a new
statewide Prescription Monitoring Program mandate (PMP mandate). The PMP mandate
requires prescribers to check patient prescription histories before prescribing opioid or benzo-
diazepine drugs.
The Arizona Legislature passed the PMP mandate in March of 2017, but the effective date of
this mandate was delayed for several months to allow electronic health record (EHR) compa-
nies and Arizona's HIE, Health Current, to integrate with the state PMP database. This allows
users of EHRs and Health Current to more efficiently access the PMP database as part of
their daily workflow.
There are the three ways that prescribers can access the PMP database:
via the Arizona State Board of Pharmacy Website
via a Provider EHR
via Health Current, Arizona's HIE
Health Current will be offering lunch and learn webinars on the PMP Mandate with a demon-
stration of how HIE Portal users are able to comply with the mandate. All webinars are from
12:00 noon to 1:00 p.m.
Webinar dates:
To register for any of the webinar demonstrations above please visit:
https://healthcurrent.org/news-events/events/webinar-users-able-comply-pmp-mandate-hie-
portal/
ADDITIONAL INFORMATION
For more information regarding the controlled substance prescription monitoring program
please visit the Arizona State board of Pharmacy website: https://arizona.pmpaware.net/login
here you can create an account to access the PMP database.
.
November 2, 2017 November 16, 2017 December 7, 2017
Health Current Connection to State Prescription Database is Now Available

Douglas A. Ducey, Governor Thomas J. Betlach, Director
801 East Jefferson, Phoenix, AZ 85034 • PO Box 25520, Phoenix, AZ 85002 • 602-417-4000 • www.azahcccs.gov 1
DATE: November 15, 2017
TO: Holders of the AHCCCS Contractor Operations Manual and AHCCCS Operational Guidelines
FROM: DHCM Contracts and Policy
SUBJECT: AHCCCS Contractor Operations Manual (ACOM) and AHCCCS Operations Reporting Guidelines
This memo describes revisions and/or additions to the ACOM and AHCCCS operations reporting guidelines including the Claims Dashboard Reporting Guide, Grievance System Reporting Guide, and Provider Affiliation Transmission (PAT) User Manual. Please direct questions regarding policy updates to the Contracts and Policy Unit at 602-417-4295 or 602-417-4055 or email at [email protected].
UPDATES AND REVISIONS TO THE AHCCCS CONTRACTOR OPERATIONS MANUAL (ACOM)
To view the policies and attachments, please access the following link:
AHCCCS CONTRACTOR OPERATIONS MANUAL (ACOM) POLICY 109, INSTITUTION FOR MENTAL DISEASE (IMD) ACOM Policy 109, is a new Policy created to address 42 CFR 438.6(e): Payments to Managed Care Organizations and PIHPs for enrollees that are a patient in an institution for mental disease.
o ATTACHMENT A, IMD PLACEMENT EXCEEDING 15 DAYS Contractors shall complete and submit Attachment A within one business day of identification of an IMD Stay greater than 15 days.
POLICY 323, REGIONAL BEHAVIORAL HEALTH ATHORITIES CYE 16 & CYE 17 TITLE XIX/XXI RECONCILIATION AND SFY 17 AND FORWARD NON-TITLE XIX/XXI PROFIT LIMIT ACOM Policy 323 is a new Policy. Reconciliation language from the RBHA Financial Reporting Guide was moved from the Guide into this Policy. Additional changes were made to be consistent with other reconciliation policies.
o ATTACHMENT A, CYE 16 ONLY MARICOPA COUNTY CONTRACTOR TITLE XIX/XXI RECONCILIATION – EXAMPLE Attachment A to this Policy provides an example of the calculation of the Title XIX/XXI reconciliation for the Maricopa County Contractor and the Greater Arizona Contractors for CYE 16.
o ATTACHMENT B, MARICOPA COUNTY CONTRACTOR TITLE XIX/XXI RECONCILIATION Attachment B to this Policy provides an example of the Title XIX/XXI reconciliation calculation for the Maricopa County Contractor for CYE 17.

Douglas A. Ducey, Governor Thomas J. Betlach, Director
801 East Jefferson, Phoenix, AZ 85034 • PO Box 25520, Phoenix, AZ 85002 • 602-417-4000 • www.azahcccs.gov 2
o ATTACHMENT C, GREATER ARIZONA CONTRACTORS TITLE XIX/XXI RECONCILIATION New Attachment addressing Greater Arizona Contractors Title XIX/XXI Reconciliation.
o ATTACHMENT D, NON-TITLE XIX/XXI PROFIT LIMIT EXAMPLE Attachment C to this Policy provides an example of the Title XIX/XXI reconciliation calculation for the Greater Arizona Contractors for CYE 17.
APPROVED NOT YET EFFECTIVE
To view the policies and attachments, please access the following link:
ACOM APPROVED NOT YET EFFECTIVE
None at this time.
UPDATES AND REVISIONS TO THE AHCCCS OPERATIONAL REPORTING GUIDELINES
INCLUDING: CLAIMS DASHBOARD REPORTING GUIDE, GRIEVANCE SYSTEM REPORTING GUIDE, PROVIDER AFFILIATION TRANSMISSION (PAT) USER MANUAL
To view the current Reporting Guides, please access the following link: AHCCCS OPERATIONS REPORTING GUIDELINES
CLAIMS DASHBOARD REPORTING GUIDE No revisions at this time. GRIEVANCE AND APPEAL SYSTEM REPORTING GUIDE No revisions at this time. PROVIDER AFFILIATION TRANSMISSION (PAT) USER MANUAL No revisions at this time.

Revised 7.2015 Page 1 of 5 SEE PAGE 5 FOR FAX AND PHONE INFORMATION
Credentialing Alliance PRACTITIONER DATA FORM
PLEASE COMPLETE THIS FORM IN ITS ENTIRETY INCLUDING ATTACHMENTS SO THAT WE MAY PROCESS YOUR REQUEST. New providers receive written confirmation of their effective date with the health plan. Members may not be seen until the provider receives written confirmation that a request or change is approved and completed (this includes approval by the Credentialing Committee if applicable). Please Type or Print Clearly.
To: Return To:
Fax #: Phone #: Fax #: Phone #:
DIRECTIONS: Please type or print this form clearly and return the completed form with attachments Certification in your requested specialty or documentation of your examination date is required in order to successfully complete the
contracting process
Post the following items (as applicable) to CAQH - Check box to indicate items posted:
IRS 941 coupon or accurate W9 Documentation of board certification or scheduled exam date Medicaid required
insurance certificates as applicable (see page 3 for requirements) Fluoride Varnish Application Training Certificate (PCPs only) Developmental Screening Tool Training Certificate-PEDS/ASQ/M-CHAT (PCPs only)
General Anesthesia Permit, Conscious Sedation Permit and/or Oral Conscious Sedation Permit (Dental providers only)
CAQH Registration is required (http://www.caqh.org - for assistance please contact CAQH HELP DESK 1-888-599-1771)
CAQH # ________ Please ensure your application and attestation is up to date and that each health plan you are requesting
participation in is authorized to access your data.
Practitioner’s Name & Degree: (Last) (First) (M.I.) (Degree)
Female Male Practitioner’s Effective Date w/Practice:
DOB:
1099 Registered Name (Required):
Tax ID #:
Group Practice Name (DBA) if applicable:
Are you associated with any of the following: IPA PHO N/A
If IPA or PHO marked please provide Name:
Group Type (check all that apply):
PCP OBGYN Dentist Specialist
Lines of Business: Medicaid
Medicare Commercial
Individual NPI#: Organizational NPI#: Malpractice Policy #
SSN: DEA #: State: Exp. Date: License #: State: Exp. Date:
Is provider a Medicare participating provider? Yes No AHCCCS I.D.#:
Primary Specialty: Board Certification: Yes No Date of Exam:
New Graduate 1 : Yes No
Graduation/Completion Date:
Secondary Specialty: Board Certification: Yes No
Date of Exam:
Want Contract as PCP? Yes No Accepting New Patients? Yes No Patient Age Range:
Do you provide services to individuals with special needs/chronic conditions (check all that apply)? Physical Developmental Behavioral Emotional None
Physician Assistant Supervising Physician Name:
Do you provide services to individuals who have difficulty communicating or cooperating (i.e. those with autism or intellectual disabilities)? Yes No
Do you provide services to individuals with mobility limitations (i.e. wheelchair bound)? Yes No
Do you treat any of the following diagnoses (check all that apply)? Anxiety ADHD Depression HIV None
PCPs & OBs ONLY: Do you provide any of the following services (check all that apply)? EPSDT OB None
Do you participate in VFC (Vaccines for Children)? Yes No (PCPs seeing AHCCCS members 18 & < must participate) VFC PIN Code:
Is Practice/Practitioner FQHC or RHC? FQHC RHC N/A
Hospitals & Ambulatory Surgery Center(s) where practitioner has privileges:
Names of Practitioners in Call Group (Must be contracted with plan): 1 licensed to practice medicine or dentistry for the first time in your career and/ or completed post-graduate training for the first time within the last 6 months

Revised 7.2015 Page 2 of 5 SEE PAGE 5 FOR FAX AND PHONE INFORMATION
PLEASE COMPLETE THIS FORM IN ITS ENTIRETY INCLUDING ATTACHMENTS SO THAT WE MAY PROCESS YOUR REQUEST. New providers will receive written confirmation of their effective date with the health plan. Members may not be seen until the provider receives written confirmation that a request or change is approved and completed (this includes approval by the Credentialing Committee if applicable). Please Type or Print Clearly.
BILLING SERVICE (If applicable)
Name:
Address: Phone:
City: State: Zip Code: Fax:
PAY TO ADDRESS
(All payments sent to this address)
Address: City: State:
Billing Phone #: Billing Fax #: Zip Code:
PRIMARY ADDRESS (Physical location where services are performed)
Address: City: Zip Code:
Phone #: Fax #: County:
Office Hours: Office Contact (All Other):
ADDITIONAL OFFICE: (Indicate other additional offices on an separate sheet)
Address: City: Zip Code:
Phone #: Fax #: County:
Office Hours:
MAILING ADDRESS: (All correspondence will be sent to this address)
Address: City: Zip Code:
E-mail Address: County:
CREDENTIALING CONTACT:
Name: E-mail Address:
Address: Phone:
City: State: Zip Code: Fax:
Languages other than English spoken by PRACTITIONER: N/A
Languages other than English spoken by OFFICE STAFF: N/A
Any other Name(s) Possible in Records? N/A
Describe Your Medical Record Keeping System(s) (i.e. EMR, Paper, etc.):
Describe Your Cost Record Keeping System(s) (i.e. Billing or A/R system):
Electronic Claims Submission? Yes No Internet Access? Yes No Is this a minority or female owned business? Yes No
Electronic Funds Transfer? Yes No

Revised 7.2015 Page 3 of 5 SEE PAGE 5 FOR FAX AND PHONE INFORMATION
AHCCCS INSURANCE REQUIREMENTS – Required ONLY if requesting to participate in the Plan’s Medicaid Line of Business
AHCCCS updated its Minimum Subcontract Provisions to include additional insurance requirements for Acute Care, ADHS/DBHS, CMDP and CRS Subcontractors. The AHCCCS insurance requirements include Commercial General Liability, Business Automobile Liability, Worker’s Compensation and Employers’ Liability and Professional Liability.
For the purpose of this Attachment, the following definition applies: “Subcontractor” means any party with a contract with the Contractor (AHCCCS Plan) for the provision of any or all services or requirements specified under the Contractor’s contract with AHCCCS.
Your commercial general liability policy and your business automobile policy (if applicable), need to include an endorsement (see letter a. below under Commercial General Liability and letter a. below under Business Automobile Liability) and a waiver of subrogation (see letter b. below under Commercial General Liability and letter b. below under Business Automobile Liability) in the Description field of your policy. Your worker’s compensation and employers’ liability policy require only the waiver of subrogation language (see letter a. below under Worker’s Compensation and Employers’ Liability).
A. MINIMUM SCOPE AND LIMITS OF INSURANCE: Subcontractor shall provide coverage with limits of liability not less than those stated below as applicable in accordance with the services provided by the Subcontractor.
1. Commercial General Liability (CGL) – Occurrence Form Policy shall include bodily injury, property damage, and broad form contractual liability coverage.
General Aggregate $2,000,000
Products – Completed Operations Aggregate $1,000,000
Personal and Advertising Injury $1,000,000
Damage to Rented Premises $ 50,000
Each Occurrence $1,000,000
a. As required by AHCCCS, the policy shall include an endorsement that includes the State of Arizona, and its departments, agencies, boards, commissions, universities, officers, officials, agents, and employees as additional insureds with respect to liability arising out of the activities performed by or on behalf of the Contractor.
b. Policy also shall contain a waiver of subrogation endorsement, as required by AHCCCS, for the State of Arizona, and its departments, agencies, boards, commissions, universities, officers, officials, agents, and employees for losses arising from work performed by or on behalf of the Subcontractor.
2. Business Automobile Liability Bodily Injury and Property Damage for any owned, hired, and/or non-owned vehicles used in the performance of the services under
contract.
Combined Single Limit (CSL) $1,000,000
a. As required by AHCCCS, the policy shall include an endorsement that includes the State of Arizona, and its departments, agencies, boards, commissions, universities, officers, officials, agents, and employees as additional insureds with respect to liability arising out of the activities performed by or on behalf of the Contractor involving automobiles owned, leased, hired and/or non-owned by the Contractor.
b. Policy shall contain a waiver of subrogation endorsement, as required by AHCCCS, in favor of the State of Arizona, and its departments, agencies, boards, commissions, universities, officers, officials, agents, and employees for losses arising from work performed by or on behalf of the Subcontractor.
3. Worker's Compensation and Employers' Liability Workers' Compensation Statutory Employers' Liability
Each Accident $ 500,000 Disease – Each Employee $ 500,000 Disease – Policy Limit $1,000,000
a. Policy shall contain a waiver of subrogation endorsement, as required by AHCCCS, in favor of the State of Arizona, and its departments, agencies, boards, commissions, universities, officers, officials, agents, and employees for losses arising from work performed by or on behalf of the Subcontractor.

Revised 7.2015 Page 4 of 5 SEE PAGE 5 FOR FAX AND PHONE INFORMATION
4. Professional Liability (Errors and Omissions Liability) Each Claim $1,000,000 Annual Aggregate $3,000,000
a. In the event that the professional liability insurance required by contract is written on a claims-made basis, Provider warrants that any retroactive date under the policy shall precede the effective date of the contract; and that either continuous coverage will be maintained or an extended discovery period will be exercised for a period of two (2) years beginning at the time work under the contract is completed.
b. The policy shall cover professional misconduct or negligent acts for those positions defined in the Scope of Work of the contract.
B. NOTICE OF CANCELLATION: For each insurance policy required by the insurance provisions of this Contract, the subcontractor must
provide to the Contractor, within two (2) business days of receipt, a notice if a policy is suspended, voided, or cancelled for any reason. C. ACCEPTABILITY OF INSURERS: Subcontractor’s insurance shall be placed with companies licensed in the State of Arizona or hold
approved non-admitted status on the Arizona Department of Insurance List of Qualified Unauthorized Insurers. Insurer shall have an “A.M. Best” rating of not less than A- VII.

The fax number and phone number for each participating plan is listed in the table below.
If your intent is to apply for participation in a Health Plan network, please send only to the Plan(s) you are interested in joining. NOT ALL Plans provide services in every county. Please contact the Plan directly to verify that they provide services in your county and that they are accepting new providers.
If you are adding a practitioner under an existing Health Plan contract, please only send to the Plan(s) you are contracted with.
Revised 7.2015 Page 5 of 5 SEE PAGE 5 FOR FAX AND PHONE INFORMATION
HEALTH PLAN PHONE FAX WEBSITE Bridgeway Health Solutions
(866) 475-3129
(866) 687-0514
www.bridgewayhs.com
Care1st Health Plan Arizona
(602) 778-1800 (options in order 5, 7)
(602) 778-1875 www.care1st.com/az
Comprehensive Medical and Dental Program (CMDP)
(602) 351-2245 or
(800) 201-1795 (options in order 1, 2, 3)
(602) 264-3801 www.azdes.gov/cmdp
Health Choice Arizona (800) 322-8670 (options in order 4, 7)
Maricopa/Pima/Pinal/Gila: (480) 760-4975
Apache/Navajo/Mohave/Coconino: (480) 760-4709
www.healthchoiceaz.com
Health Net Access (800) 289-2818 Apache/Coconino/Gila/LaPaz/ Maricopa/Mohave/Navajo/ Yavapai:
(602) 794-1803 Cochise/Graham/Greenlee/Pima/PinalSanta Cruz/Yuma:
(520) 258-5172
www.healthnet.com
Mercy Care Plan
(602) 263-3000 (Express Code 631)
(860) 975-3201 www.mercycareplan.com
Mercy Maricopa (800) 564-5465
(860) 975-0841 www.mercymaricopa.org
Phoenix Health Plan (602) 824-3720 (602) 674-6670 www.phoenixhealthplan.com
UnitedHealthcare Community Plan
(877) 842-3210 (612) 234-0211 www.uhccommunityplan.com
The University of Arizona Health Plans
(520) 874-5290 or
(800) 582-8686
(520) 874-7142 www.ufcaz.com www.mhpaz.com
www.universitycareadvantage.com www.universityhealthcaregroup.com
Each plan retains the right to make their own contracting decisions (whether or not to add practitioners to their network) and also will make their own credentialing committee decisions (review of the primary source verification information obtained by OptumInsight™ resulting in approval/denial by the plan’s committee). You will receive separate communication from each plan regarding the effective date of your credentialing and the effective date of your contract.
As a reminder, this form includes Personally Identifiable Information (PII) such as practitioner name, date of birth and SSN and should be sent in a secure manner.