establishing a culture of safety april 2012
TRANSCRIPT

Maureen Spencer, RN, M.Ed, CIC
Infection Preventionist Consultant
Boston, MA
Establishing a Culture of Safety:
Working Toward Zero
Orthopedic SSIs
Email: [email protected]
www.workingtowardzero.com
www.creativehandhygiene.com
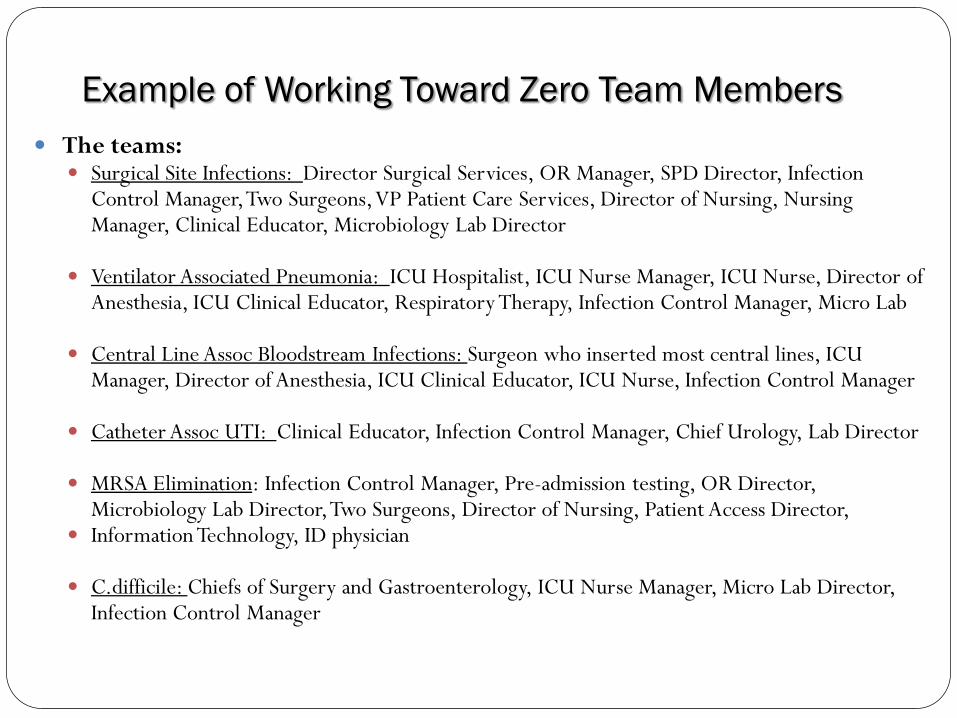
Example of Working Toward Zero Team Members
2
The teams: Surgical Site Infections: Director Surgical Services, OR Manager, SPD Director, Infection
Control Manager, Two Surgeons, VP Patient Care Services, Director of Nursing, Nursing Manager, Clinical Educator, Microbiology Lab Director
Ventilator Associated Pneumonia: ICU Hospitalist, ICU Nurse Manager, ICU Nurse, Director of
Anesthesia, ICU Clinical Educator, Respiratory Therapy, Infection Control Manager, Micro Lab
Central Line Assoc Bloodstream Infections: Surgeon who inserted most central lines, ICU Manager, Director of Anesthesia, ICU Clinical Educator, ICU Nurse, Infection Control Manager
Catheter Assoc UTI: Clinical Educator, Infection Control Manager, Chief Urology, Lab Director MRSA Elimination: Infection Control Manager, Pre-admission testing, OR Director,
Microbiology Lab Director, Two Surgeons, Director of Nursing, Patient Access Director, Information Technology, ID physician C.difficile: Chiefs of Surgery and Gastroenterology, ICU Nurse Manager, Micro Lab Director,
Infection Control Manager

Pre-op:
Screen for MRSA
and Staph aureus
CHG pre-op
shower or cleanse
with impregnated
cloths
Assure OR meets
AORN standards of
practice
Intraoperative: CHG/alcohol skin prep, antibacterial sutures, incisional adhesive
Irrigation?
Consider using saline or new CHG (0.05%) irrigant and eliminate expensive and toxic bacitracin/polymixin or antibiotic irrigant
Post-op:
Incisional adhesive should be the number one consideration for wound closure – prevents dehiscence and exogenous contamination to wound
If not used consider covering incision for length of hospitalization
Patient education is extremely important since many patients are discharged early in the post-op period and have incisions that are in the exudative state of wound healing

MRSA and Staph aureus
Elimination Program Before Patients Enter
the Hospital for Surgery
4
Prescreening Process
Topical Decolonization Protocol
Vancomycin for MRSA
1. Kim D, Spencer M, Davidson S, et al. J Bone Joint Surg 2010;92:1820-6 2. Spencer M, Kim D, et al: AAOS, 2010

Provided Evidence: February 2006
Anonymous Nares Cultures To Prove to Administration Patients Are Colonized
With Staph aureus and MRSA
5
N = 133 patients anonymously surveyed and
cultured in OR after anesthetized
Purpose: to determine pre-op MRSA and Staph
aureus colonization rates for administration
Results:
38 – Staph aureus (29%)
*5 - MRSA ( 4%)
*all undiagnosed, no precautions used in OR,
PACU, postop nursing unit
*MRSA cases received Cefazolin for surgical
prophylaxis – THE WRONG ANTIBIOTIC!

Implemented Decolonization Protocol
6
• 5-day application of intranasal 2% mupirocin -
applied twice daily - for MRSA and Staph aureus
positive patients
• Prescription called in by Nurse Practitioner in
prescreening unit
• Daily body wash with chlorhexidine (purchased
by patient)
• MRSA Patients – Unique sticker system to notify
Pre-surgery Unit of Vancomycin surgical
prophylaxis

7

Pre-op MRSA and S. aureus Decolonization
8
Results:
Timeframe: July 17, 2006 through September 2010
Infection rate: 20,065 patient screened
5,988 (23%) positive for Staph aureus
1,027 ( 4%) positive for MRSA
Effectiveness: Repeat nasal screens on MRSA patients
revealed 77% eradication

Pre-op MRSA and S. aureus Decolonization
9
Results: % MRSA and S. aureus SSI
Time Period Inpatient
Surgeries
# of Surgical
Infections %MRSA/MSSA
FY06
10/01/05-07/16/06* 5,293* 24* 0.45%*
FY07
07/17/06-09/30/07 7,019 6 0.08%
FY08
10/01/07-09/30/08 6,323 7 0.11%
FY09
10/01/08-09/30/09 6,364 11 0.17%
FY10
10/01/10-09/30/10 6,437 6 0.09%
*Historical Controls

Pre-op MRSA Decolonization
10
Results: % MRSA SSI in Screened Patients
Time Period
Inpatient
Surgeries
# MRSA
SSIs MRSA%
#Infect/#MRSA
+
FY06
10/01/05-07/16/06 5,293 10 (NA) 0.19% NA
FY07
07/17/06-09/30/07 7,019 3 (3+) 0.04% 3/309 (0.97%)
FY08
10/01/07-09/30/08 6,245 4 (2+) 0.06% 2/242 (0.83%)
FY09
10/01/08-09/30/09 6,336 6* (2+) 0.09% 2/234 (0.85%)
FY10
10/01/10-09/30/10 6,437 1 (1+) 0.01% 1/266 (0.37%)
* isolates have been sent for pulse field gel electrophoresis 5 of the 6 isolates were available for PFGE and were not related genetically

Pre-op Staph aureus Decolonization
11
Results: % S. aureus (MSSA) SSI in Screened Patients
Time Period
Inpatient
Surgeries
# MSSA
SSIs MSSA%
#Infect/#MSSA
+
FY06
10/01/05-07/16/06 5,293 14 (NA) 0.26% NA
FY07
07/17/06-09/30/07 7,019 3 (3+) 0.04% 3/1588 (0.19%)
FY08
10/01/07-09/30/08 6,245 3 (1+) 0.05% 1/ 1422 (0.07%)
FY09
10/01/08-09/30/09 6,336 5 (1+) 0.08% 3/1403 (0.21%)
FY10
10/01/10-09/30/10 6,437 6 (1+) 0.09% 1/1450 (0.06%)

OR Risk Factors:
Contamination from OR Staff
12
• Reviewed orderlies and room turnover procedures
• Improved traffic control – new signage and monitoring system
keep room doors closed and minimize traffic
• Eliminate surgical caps – do not cover hair!
• Cloth cap use – if worn, must be covered in OR room
with disposable cap - hair coverage monitored – Hair harbors organisms – Staff sweat in cloth caps
– How often do they get washed? Hospital laundered
– Where are they stored?
– Would you eat a meal with hair in it? – Why allow hair to potentially fall into
surgical incisions?

OR Risk Factors:
Cleaning/Sterilization of Instruments
13
• Inspection of Orthopedic Instruments – Lumens, grooves, sorting, hand cleaning,
disassembly required – massive kits – Many instruments cannot be disassembled
• Instituted better pre-soaking and rinsing of tissue and blood from the instruments in the operating room before decontamination
• There was a recent outbreak investigated by CDC of shoulder infections - found shavers and cannulas with biofilm and tissue observed inside instruments with small camera

Pathogens survive on surfaces
Organism Survival period
Clostridium difficile 35- >200 days.2,7,8
Methicillin resistant Staphylococcus aureus (MRSA) 14- >300 days.1,5,10
Vancomycin-resistant enterococcus (VRE) 58- >200 days.2,3,4
Escherichia coli >150- 480 days.7,9
Acinetobacter 150- >300 days.7,11
Klebsiella >10- 900 days.6,7
Salmonella typhimurium 10 days- 4.2 years.7
Mycobacterium tuberculosis 120 days.7
Candida albicans 120 days.7
Most viruses from the respiratory tract (eg: corona,
coxsackie, influenza, SARS, rhino virus)
Few days.7
Viruses from the gastrointestinal tract (eg: astrovirus, HAV,
polio- or rota virus)
60- 90 days.7
Blood-borne viruses (eg: HBV or HIV) >7 days.5
1. Beard-Pegler et al. 1988.. J Med Microbiol. 26:251-5.
2. BIOQUELL trials, unpublished data.
3. Bonilla et al. 1996. Infect Cont Hosp Epidemiol. 17:770-2
4. Boyce. 2007. J Hosp Infect. 65:50-4.
5. Duckworth and Jordens. 1990. J Med Microbiol. 32:195-200.
6. French et al. 2004. ICAAC.
7. Kramer et al. 2006. BMC Infect Dis. 6:130.
8. Otter and French. 2009. J Clin Microbiol. 47:205-7.
9. Smith et al. 1996. J Med. 27: 293-302.
10. Wagenvoort et al. 2000. J Hosp Infect. 45:231-4.
11. Wagenvoort and Joosten. 2002. J Hosp Infect. 52:226-7.

Why Better Environmental Cleaning?
Prior room occupancy increases risk
Study Healthcare associated pathogen Likelihood of patient acquiring HAI
based on prior room occupancy
(comparing a previously ‘positive’
room with a previously ‘negative’
room)
Martinez 20031 VRE – cultured within room 2.6x
Huang 20062 VRE – prior room occupant 1.6x
MRSA – prior room occupant 1.3x
Drees 20083
VRE – cultured within room 1.9x
VRE – prior room occupant 2.2x
VRE – prior room occupant in previous two
weeks 2.0x
Shaughnessy 20084 C. difficile – prior room occupant 2.4x
Nseir 20105 A. baumannii – prior room occupant 3.8x
P. aeruginosa – prior room occupant 2.1x
1. Martinez et al. Arch Intern Med 2003; 163: 1905-12.
2. Huang et al. Arch Intern Med 2006; 166: 1945-51.
3. Drees et al. Clin Infect Dis 2008; 46: 678-85.
4. Shaughnessy. ICAAC/IDSA 2008. Abstract K-4194.
5. Nseir et al. Clin Microbiol Infect 2010 (in press).

Floors:
MRSA 55%
C. Difficile 48%
Patient Gowns:
MRSA 51%
Bedsheets:
MRSA 53%
VRE 40%
Windowsill:
C. Difficile 33%
Overbed Table:
MRSA 40%
VRE 20%
Bedrail:
MRSA 29%
VRE 28%
C. Difficile 19%
Blood Pressure Cuff:
VRE 14%
Commode:
C. Difficile 41%
Rates of Surface Contamination (in hospitals) with MSRA, VRE, and C. Difficile
Did you know that every time you get a new roommate, there is an
increase of 3-10% that you will acquire an HAI.
Boyce J.M. et al.: Environmental contamination due to methicillin-resistant Staphylococcus aureus: Possible infection control implications. Infect Control Hosp Epidemiol 18:622-627, Sep. 1997.
Slaughter S., et al.: A comparison of the effect of universal use of gloves and gowns with that of glove use alone on acquisition of vancomycin-resistant enterococci in a medical intensive care
unit. Ann Intern Med 125: 448-456, Sep 15, 1996.
Samore M.H., et al.: Clinical and molecular epidemiology of sporadic and clustered cases of nosocomial Clostridium difficile diarrhea. Am J Med 100:32-40, Jan. 1996.
Huang SS, Datta R, Platt R. Risk of acquiring antibiotic-resistant bacteria from prior room occupants. Arch Intern Med.
2006 Oct 9;166(18):1945-51

Environmental Disinfection – Joint
Commission and CMS Focus on Surveys
17
Developed cleaning schedules for Patient Care
Services – what equipment, how
cleaned/disinfected, how often, by who, contact
times for disinfectants?
Eliminate dirty buckets of water and string mops
institute micro fiber cloths and mops
Assure staff know proper cleaning technique: left to right, high to low, clean to dirty with
competencies
Daily check sheet for terminal cleaning of OR at
night and for all precaution cases

Decontamination of Portable Equipment
with Contracted Services
18
Ultrasonic scrub
Movable carts
Tables
Poles
Small equipment
1500 pieces cleaned
OR, radiology, nursing
Cost: ~$20,000 / year
M Spencer, at al: The E=MC2 Project: Environment = Maintaining Cleanliness: A Multidisciplinary Approach To
Establish a Routine Cleaning Schedule for Medical Equipment.
APIC 2005 Poster

SSI risk can be addressed by
controlling risk factors
19
Precautions are already in place to control the risk of bacterial
contamination throughout the peri-operative period
However, additional controllable risk factors remain – wound
closure provides an opportunity to address these risks
Controlled Risks Potentially Uncontrolled Risks
Scrubbing in Gowning Skin antisepsis Controlling OR environment Sterilizing instruments Using minimally invasive techniques
☐ Bacterial colonization of the suture ☐ Contamination of the incisional site
after the wound is closed ☐ Entry of bacteria from the skin during
wound closure ☐ Bacterial infiltration due to dehiscence

Uncontrolled Risk Factor:
Bacterial colonization of the suture
20
Like all foreign bodies, sutures can be colonized by bacteria: Implants provide nidus for attachment of bacteria1
Bacterial colonization can lead to biofilm formation1
Biofilm formation increases the difficulty of treating an infection2
On an implant, such as a suture, it takes only 100 staphylococci per gram of tissue for an SSI to develop3
1. Ward KH et al. J Med Microbiol. 1992;36: 406-413. 2. Kathju S et al Surg infect. 2009;10:457-461 3. Mangram AJ et al. Infect Control Hosp Epidemiol.1999;27:97-134..
Contamination Colonization Biofilm
Formation

Why Plus Suture?
OR Air Current Contamination
In teaching hospitals:
Surgeon leaves room
Resident, Physician Assistant or Nurse
Practitioner work on incision
Circulating Nurse counts sponges and
starts room breakdown
Scrub Technician starts breaking down
tables and preparing instruments for
Central Processing
Anesthesia move in and out of room
Instrument representative might leave
room and Visitors may leave room

Suture with Staphylococcus colonies
Air settling plates in the operating room at the last hour of a total joint case
Potential for Contamination of Sutures at
End of Case

Plus Antibacterial Sutures:
Impact in a Real-World Setting
23
Plus sutures not only kill bacteria on the suture, but also create an
inhospitable environment around the suture
NEBH studied the “zone of inhibition” around the suture
A pure culture—0.5 MacFarland Broth—of S. aureus was
prepared on a culture plate
An antibacterial suture was aseptically cut, planted on the
culture plate, and incubated for 24 hrs
5 day zone of inhibition 10 day zone of inhibition
Traditional suture
Antimicrobial suture

Plus Antibacterial Sutures:
Impact in a Real-World Setting
24
NEBH One Year Prospective Study of 3800 Total Joints
and Antimicrobial Sutures
In July 2005, implemented a full-year evaluation of
antibacterial sutures usage in an orthopedic setting
Changed product over July 4th holiday and did not tell
all surgeons (only those involved with study)
At the end of the year-long trial period:
45% reduction in SSIs caused by Staph aureus and
MRSA
Infection rate dropped from
0.44% to 0.33% with three less infections
Spencer M, et al: Reducing the Risk of Orthopedic Infections: The Role of Innovative Suture Technology
NAON Poster Presentation - 2010
0
0.1
0.2
0.3
0.4
0.5
FY05 FY06
Series1

Articles Related To Antibacterial Sutures
*Justinger, C, et al. Antibiotic coating of abdominal closure sutures and wound infection. Surgery 2009;145:330-4. (*RCT)
Rothenburger S, et al. In vitro antimicrobial evaluation of Coated VICRYL* Plus Antibacterial Suture (coated polyglactin 910 with triclosan) using zone of inhibition assays. Surg Infect 2002;3 Suppl 1:S79-87
Ford HR, et al. Intraoperative handling and wound healing: controlled clinical trial comparing coated VICRYL plus antibacterial suture (coated polyglactin 910 suture with triclosan) with coated VICRYL suture (coated polyglactin 910 suture). Surgical Infections. 6(3):313-21, 2005.
Edmiston CE, et al. Bacterial adherence to surgical sutures: can antibacterial-coated sutures reduce the risk of microbial contamination? Journal of the American College of Surgeons. 203(4):481-9, 2006 Oct

Innovative wound closure technologies
can address risk factors for SSIs
26
Topical Skin Adhesive provides a microbial barrier during the
critical wound healing period
SSI Risk Factor Innovative Technology
Bacterial colonization of the suture
Contamination of the incisional site after the
wound is closed
Entry of bacteria from the skin during
wound closure
Bacterial infiltration due to dehiscence
Antibacterial Sutures
Chlorhexidine/alcohol skin prep
Prevention of Dehiscence and
Exogenous Contamination with
Topical Skin Adhesive or
Antimicrobial Dressings

27
Antisepsis with Chlorhexidine
2% CHG/70% alcohol skin preparation (tinted orange) Has a lasting effect on the skin ~ 2 days postop
Iodophors are fast kill but no long term effect
CHG dry time is 3 minutes (to prevent fires)
• Evidence that chlorhexidine/alcohol achieves
better skin antisepsis than iodophor Darouiche et al NEJM 2010 Ostrander et al JBJS Am 2005 Saltzman et al JBJS Am 2009

Post-op Skin Issues in Orthopedics
Anterior fusion with tape burns
Posterior fusion with contaminated steri-strips
Contaminated steri-strips
Staples increase infection rate

Associated Wound Infection or Separation After
Cesarean Delivery: Sutures vs Staples
Prospective, randomized study of 435 c-section patients1
197 patients: staples
219 patients: 4-0 MONOCRYL™ (poliglecaprone 25) Suture on PS2 needle
– Wound separation rate: 17% (staples) vs. 5 % (sutures)
– Wound complication rate: 22% (staples) vs. 9% (sutures)
– Staple closure was a significant independent risk factor for wound
separation after adjustment for all other factors (GDM, BMI >30, incision
type, etc)
Meta-analysis of 6 studies with a total of 1487 c-section patients2
803 patients: staples
684 patients: subcuticular suture closure
– Staple closure was associated with a two-fold increase in risk of wound
infection or separation
1. Basha et al. Am J Obstet Gynecol. 2010;203:285.e1. 2. Tuuli et al. Obset Gynecol. 2011;117:682.

The risk for infection after joint surgery is higher with staples vs traditional
stitches, according to the results of a meta-analysis reported in the March
16 2010 issue of the BMJ.
In 6 publications reporting on a total of 683 wounds, 332 patients underwent
wound closure with sutures, and 351 underwent closure with staples.
Compared with suture closure, staple closure was associated with more
than triple the risk for the development of a superficial wound
infection after orthopaedic surgery (RR, 3.83; 95% CI, 1.38 – 10.68; P =
.01).
When hip surgery was analyzed as a separate subgroup, the risk for the
development of a wound infection was 4 times greater with use of
staples vs use of sutures (RR, 4.79, 95% CI, 1.24 – 18.47; P = .02). Suture
closure and staple closure did not differ significantly in development of
inflammation, discharge, dehiscence, necrosis, or allergic reaction.
“The Medical Journal of Australia” has recently updated its guidelines for skin
closure in the treatment of hip fractures, and they state that superficial wound
complication rates are higher for wounds closed with metallic staples than for
wounds closed with subcuticular vicryl.

Obesity and Surgical Incision
31
Incision collects fluid – serum, blood - growth medium for organisms
Spine fusions -incisions close to the buttocks or neck
Heavy perspiration common
Body fluid contamination from bedpans/commodes
Friction and sliding - skin tears and blisters
Itchy skin - due to pain medications - skin breakdown

Topical Skin Adhesive: A Proven Microbial
Barrier
32
Provides a flexible, protective microbial barrier that moves with the patient,
preventing breakage and acting like a temporary “skin”1,2
Adhesive demonstrates inhibition of gram-positive bacteria (MRSA and MRSE) and
gram-negative bacteria (E coli) in vitro2-4
Provides greater than 99% protection for 72 hours against organisms commonly
responsible for SSIs2,3:
S. epidermidis
E. coli
S. aureus
Pseudomonas aeruginosa
Enterococcus faecium
No fractures,
wound failure
or dehiscence
1. Quinn et al. JAMA. 1997;277:1527-1530 2. Bhende et al. Surg Infect (Larchmt). 2002;3:251-257. 3. Narang et al. J Cutan Med Surg. 2003;7:13. 4. World Health Organization. WHO Guidelines for Safe Surgery 2009. 2009.

Topical Skin Adhesive: Benefits Beyond Risk
Reduction
33
For Hospital Staff No time spent removing staples or sutures Reduced hospitalization costs Reduces number of suture set ups Simplifies post-op wound checks Reduces number of wound dressings
For Patients
7 days of wound healing strength in less than 95 seconds of application Shower immediately Outstanding cosmesis Reduced follow-up Less pain and anxiety

Incisional Adhesive on Total Knee Incision

Clinical Use of Incisionial Adhesive
Knee: Sealed with incisional
adhesive, covered with Telfa
and a transparent dressing
for incision protection Healed incision
Hip: Sealed with adhesive
covered with gauze and
transparent dressing for
incision protection

Incisional Adhesive and Total
Shoulder Replacements
0
0.5
1
1.5
2
2.5
Total Shoulder Rates
2003 2004 2005 2006 2007 2008 2009 2010
• Propionibacterium acnes related total shoulder infections (TSR)
• Eliminated the use of staples for TSR
• Instituted the use of incisional adhesive
• Covered dressing until day of discharge for protection
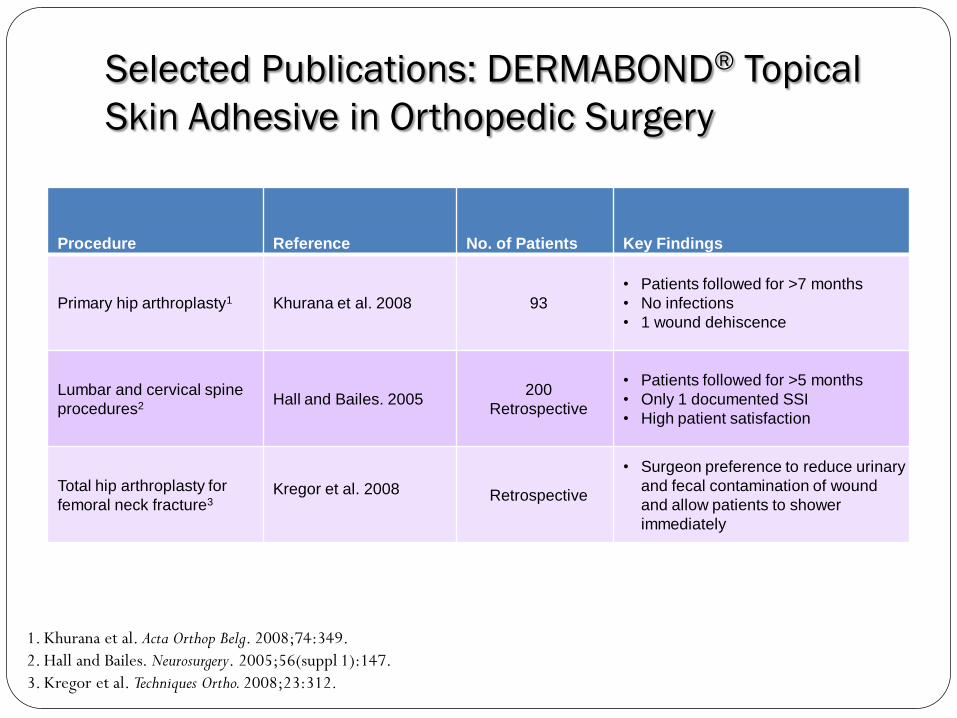
Selected Publications: DERMABOND® Topical
Skin Adhesive in Orthopedic Surgery
Procedure Reference No. of Patients Key Findings
Primary hip arthroplasty1 Khurana et al. 2008 93
• Patients followed for >7 months
• No infections
• 1 wound dehiscence
Lumbar and cervical spine
procedures2 Hall and Bailes. 2005 200
Retrospective
• Patients followed for >5 months
• Only 1 documented SSI
• High patient satisfaction
Total hip arthroplasty for
femoral neck fracture3 Kregor et al. 2008 Retrospective
• Surgeon preference to reduce urinary
and fecal contamination of wound
and allow patients to shower
immediately
1. Khurana et al. Acta Orthop Belg. 2008;74:349.
2. Hall and Bailes. Neurosurgery. 2005;56(suppl 1):147.
3. Kregor et al. Techniques Ortho. 2008;23:312.

A protective barrier that adds strength and reduces bacteria
• Has been shown in ex vivo studies to have superior tensile strength versus other octyl
and butyl based products
• Creates a microbial barrier against organisms commonly responsible for SSIs*
DERMABOND ADVANCED™ Topical Skin Adhesive
Data on File. Ethicon, Inc.
*Staphylococcus epidermidis, Staphylococcus aureus, Escherichia coli, Enterococcus faecium and Pseudomonas aeruginosa
Innovative

Comparison of TSA Components Among Currently
Available Agents
Components
DERMABOND
ADVANCED™
Topical Skin
Adhesive SurgiSeal™
derma+flex® QS™
(octylseal™) INDERMIL®
Histoacryl®
(Repara) LiquiBand® Skinstitch®
Octyl
adhesive
Plasticizers ?
Inert storage
vial,
stabilizer, and
no
refrigeration
Initiator and
heat-
dissipating
agent
High-
viscosity
formulation
The third-party trademarks used herein are trademarks of their respective owners. Data on file: Ethicon Inc.

Evidence-Based Performance
The largest randomized clinical trial database of any TSA
8x the number of patients vs the leading competitor
Product
Total Number
of RCTs
Total Number of
Patients Treated
DERMABOND®
Topical Skin Adhesive 40 4075
Histoacryl® 6 534
INDERMIL® 2 150
LiquiBand® 1 78
SurgiSeal® 0 0
derma+flex® QS™
(octylseal™) 0 0
RCTs only; reasons for exclusion were language of publication other than German or English, nonhuman studies, case series or
case reports, and inappropriate indication.
No RCTs identified for any other competitors.
The third-party trademarks used herein are trademarks of their respective owners.
RCT = randomized controlled trials.
Data on file: Ethicon Inc, Literature Search 2/2011 PubMed

41
A unique combination of
2 components
• A 2-octyl cyanoacrylate topical skin
adhesive for proven strength and
microbial protection1,2
– Sets in approximately 60 seconds
when applied to mesh
– 2-hour working time3
• A flexible, self-adhesive polyester mesh
for superior approximation and healing1,3
– Contains initiator that accelerates
polymerization of liquid adhesive
– Each dispenser contains 60 cm of tape
New, innovative, minimally invasive DERMABOND™ PRINEO™ Skin Closure System
1. DERMABOND™ PRINEO™ IFU. PM72449C. STATUS 6/2010.
2. Shapiro AJ et al. Am Surg. 2001;67(11): 1113‐1115. 3. Data on file. Ethicon, Inc.

42
Gently and evenly disperses tension across the entire area
of the incision, without penetrating the skin
Minimally invasive closure that distributes tension away from the wound
Traditional closure DERMABOND™ PRINEO™ Skin Closure
System

DERMABOND™ PRINEO™ removal
Patient is shown 2 weeks after circumferential body lift and immediately
after removal of
DERMABOND™ PRINEO™ Skin Closure System.

Areas for Cost Savings

45
Surgical Incise Drapes
Iodophor- impregnated incise
barrier drape
No data to support these
drapes reduce SSI – although
do reduce bacteria on skin
Surgeon preference based on
adhesion to skin and drapes
Consider using non-
impregnated drapes and using
cost savings for other innovative
technologies

Use of plastic adhesive drapes during surgery for preventing surgical site infection
Objective:
Compared the effect of adhesive drapes used during surgery on surgical site infection, cost, mortality and morbidity
Five studies involving 3,082 participants comparing adhesive drapes with no drape
Two studies involving 1,113 participants comparing iodine-impregnated adhesive drapes with no drape
Conclusion:
A significantly higher proportion of patients in adhesive drape group developed a surgical site infection when compared with no drape
Iodine-impregnated adhesive drapes had no effect on the surgical site infection rate
Cochrane Database Syst Rev. 2007 Oct 17;(4):CD006353

47
Bacitracin/Polymixin Irrigation
Feb 2007 - stopped routine use of Bacitracin/Polymixin Irrigation
Cost: > $110,000/year reduced to $10,000
Limited use for revisions, allografts and infected cases (irrigation and
debridements)
New irrigant available – FDA approved for mucous membranes with
0.05% CHG - Irrisept
Fletcher N, et al: Prevention of perioperative infections. J Bone
Joint Surg Am. 2007;89:1605-1618

48
Finally, an alternative to saline and antimicrobial irrigation The first and only FDA-cleared cleansing and debridement system, containing
0.05% Chlorhexidine Gluconate (CHG) in Water for Irrigation
IrriSept O.R. (sterile packaging)
Irrigation Applicators: Custom designed
applicators facilitate
cleansing for a variety of
applications
SplatterGuard® LT SplatterGuard® IrriProbe®
IRRISEPT

Review: Bundled Approach to Eliminating SSIs
1. Pre-screen inpatient surgeries for MRSA and Staph aureus (MSSA) using PCR rapid molecular technology
2. Decolonization protocol for MRSA/MSSA positive patients (eg mupirocin 2% ointment 2 x day, daily CHG wash x 5 days)
3. Preoperative shower with CHG (eg Hibiclens) or CHG washcloths (eg Sage) night before/morning of surgery
4. Assure OR standards are being met (traffic control, surgical attire, surgical hand scrub, sterilized instruments, room turnover and terminal cleaning, precautions in OR)
5. Assure surgical prophylaxis is delivered for maximum tissue concentrations
6. Surgical skin prep with CHG/alcohol prep
7. Irrigation with CHG if necessary (eg Irrisept)
8. Antibacterial sutures (eg Ethicon)
9. Incisional Adhesive (octyl cyanoacrylate) (eg Dermabond and Prineo)
10. Post-op incision care instructions
11. Data driven, analysis and calculation of rates, communication/feedback

Reducing Risk Factors for SSIs:
Tools for success
50
Institutional support
Senior leadership and “C Suite” involvement
“lead the effort” from top down
Clear goals
Structured program with clearly defined goal of
zero tolerance for HAIs
Theoretical foundation to IP Program: Social
Learning Theory (Role Modeling, Self Efficacy,
Positive Deviance)
Communication – effective and consistent
Ongoing and creative education
Financial support to Infection Prevention program

Thank You