evaluating the heart before non-cardiac surgery · 2019-02-23 · different order to risk asses...
TRANSCRIPT

Evaluating the Heart beforeNon-Cardiac Surgery
Dr Rob Stephens
Anaesthetist UCLH + UCL
the centre for
Anaesthesia UCL
www.ucl.ac.uk/anaesthesia/people/stephensGoogle UCL Stephens

www.ucl.ac.uk/anaesthesia/people/stephensGoogle UCL Stephens
Contents
• Introduction
• Basic Principles
• Guidelines: Decisions
• Guidelines: Putting it all together
• Which test?
• ECHO
• CPEx
• B Block?
• Summary
• You’re all experts!
• Seems big, complex
• Conflicting, absent and changing evidence!
• Problem:
Assessing CVS system vs
Lack of effectiveness of interventions
Introduction
Background: Basic Principles
Why assess the CVS system?
Assess risk: consent + patient decisions
Assess risk: specific interventions
Diagnose conditions : caution
Cancer surgery- ‘time limited’
Test: what next?
Ischaemia vs Heart Failure
“Probably”, “reasonable”, “is not well established”

Guidelines 1
• 2014 ACC/AHA guideline revision
• ACC/AHA 2007 (small revision 2009)
• ESC 2009
• Guidelines - Cardiology
• Fraud of Poldermans
• B Blocker story
• Individual Studies
• ?ASA / RCoA / AAGBI ?
2014 Guidelines + others
‘MACE’ Major Adverse Cardiac Event
Different Order to risk asses
Risk Asses using NSQIP
CPEX ’considered for elevated risk procedures in unknown functional capacity’
Coronary Stent Guidelines
POISE 2 study – no benefit in adding aspirin
‘MINS’ myocardial injury after non-cardiac surgery
Troponin –uncertain usefulness in high risk patients


ESC 2009

Mythen, Biccard

Wait for surgery after MI?
Postoperative MI 0 - 30 days 32.8%
31 - 60 days 18.7%
61 - 90 days 8.4%
91 - 180 days 5.9%
30-day mortality 0 - 30 days 14.2%
31 - 60 days 11.5%
61 - 90 days 10.5%
91 - 180 days 9.9%
Livhits 2011

CARP
Vascular Surgery
• 5859 patients screened; 510 selected revascularization vs not
Postoperative 30 day mortality
• 3.1% vs 3.4%, rev vs not; P = .87
Long term mortality 2.8 years
• 22% vs 24%, rev vs not P = .92
McFalls 2004

Guideline 2
ACC AHA
• Surgery Urgency
• Patient Specific risks / Comorbidities
• Surgery Severity
• Patient Exercise Capacity
ESC 2009
• Biomarkers
Guideline 3
ACC AHA
• Surgery Urgency
• Patient Specific risks / Comorbidities
• Surgery Severity
• Patient Exercise Capacity
ESC 2009
• Biomarkers
Guideline 4
Surgery Urgency
– Emergency/ Immediate proceed

Urgency AHA 2014
Emergency• no/little time limited clinical evaluation• life or limb is threatened if no surgery within <6 hours
Urgent • may be time for a limited clinical evaluation• when life or limb is threatened if no surgery within 6 - 24
Time-sensitive• a delay of >1 - 6 week for evaluation / treatment will negatively
affect outcome.
Elective• the procedure could be delayed for up to 1 year.

NCEPOD 2004

Guideline 5
Surgery Urgency
–Truly Elective – time to treat / discuss
– Treat/refer broadly as according to non-preoperative guidelines
–warn about possible delay to surgery
–evidence of benefit for subsequent surgery ?
Guideline 6
Surgery Urgency (US vs NCEPOD)
–Cancer = ‘time limited’
• Consider
– lack of benefit from CVS interventions
–potential delay after CVS intervention
– coronary stent anticoagulation

Guideline 7
ACC AHA
• Surgery Urgency
• Patient Specific risks / Comorbidities
• Surgery Severity
• Patient Exercise Capacity
ESC 2009
• Biomarkers

Guideline 8
• ACC AHA Patient Risk factors
• 3 levels: Serious / ‘Intermediate ‘ / ’Minor’
• ‘Serious’ ; ‘active cardiac conditions’
– Recent MI/Unstable Angina
– New /Acute Ht Failure
– Serious abnormal rhythm
– Severe valve disease
Pause and discuss with teams

Guideline 8
• ACC AHA Patient Risk factors
• 3 levels: Serious / ‘Intermediate ‘ / ‘minor’
• ‘Intermediate’- same as ‘Lees rCRI’ or
• Calculate NSQIP ‘MACE’ score

Lee’s rCRI revised Cardiac Risk Index
Major Surgery… and
Ischemic heart diseaseCardiac FailureCerebrovascular diseaseDiabetes on InsulinRenal insufficiency (>177 μmol / litre)
No CVS+ 0 0.3- 0.4%1 0.7- 0.9%2 1.7- 6.6%3 3.6- 11%
Boersma 2005Lee 1999
Bowl cuttingPelvicVascular

Guidelines 9
• NSQIP Risk Calculator >1%?
– Think about Preoperative testing IHD
– If it will change your management



Guideline 10
ACC AHA
• Surgery Urgency
• Patient Specific risks / Comorbidities
• Surgery Severity
• Patient Exercise Capacity
ESC 2009
• Biomarkers

Guideline 11
Severity of surgery
• Minor proceed
• Anything else consider further
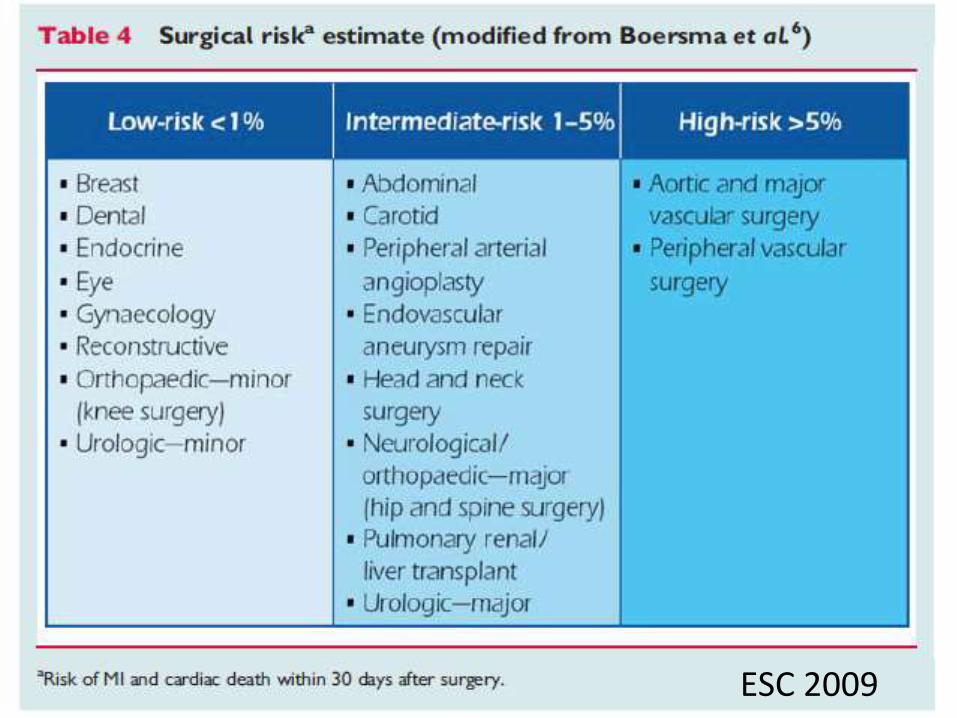
Assessing CVS disease: Guideline 4
ESC 2009
Guideline 12
ACC AHA
• Surgery Urgency
• Patient Specific risks / Comorbidities
• Surgery Severity
• Patient Exercise Capacity
ESC 2009
• Biomarkers

Guideline 13
Patient Exercise Capacity
4 METS without significant symptoms
Operations proceed
Less than 4 METS consider testing
No Chest PainNo SOB

Guideline 14
Patient Exercise Capacity
• Metabolic Equivalent of Task - MET
• 1 MET is 02 uptake at rest =
= 3.5 ml/min/kg 02 uptake
2 METS ~ 2x 02 uptake of 1 METS
Easily Quantified by CPEx
Mostly quantified by history
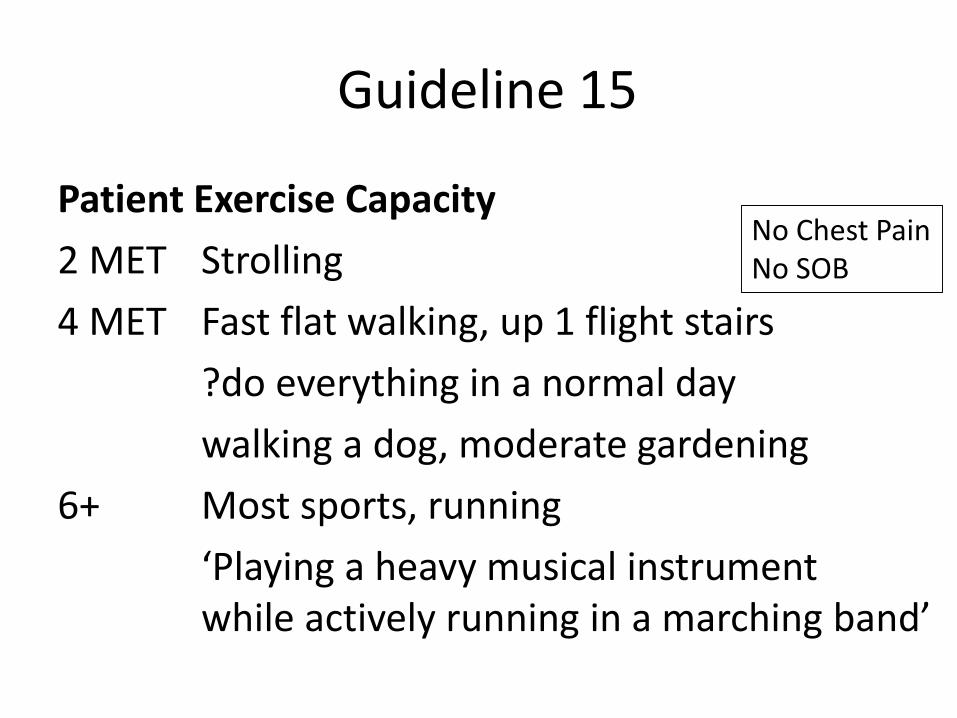
Guideline 15
Patient Exercise Capacity
2 MET Strolling
4 MET Fast flat walking, up 1 flight stairs
?do everything in a normal day
walking a dog, moderate gardening
6+ Most sports, running
‘Playing a heavy musical instrumentwhile actively running in a marching band’
No Chest PainNo SOB
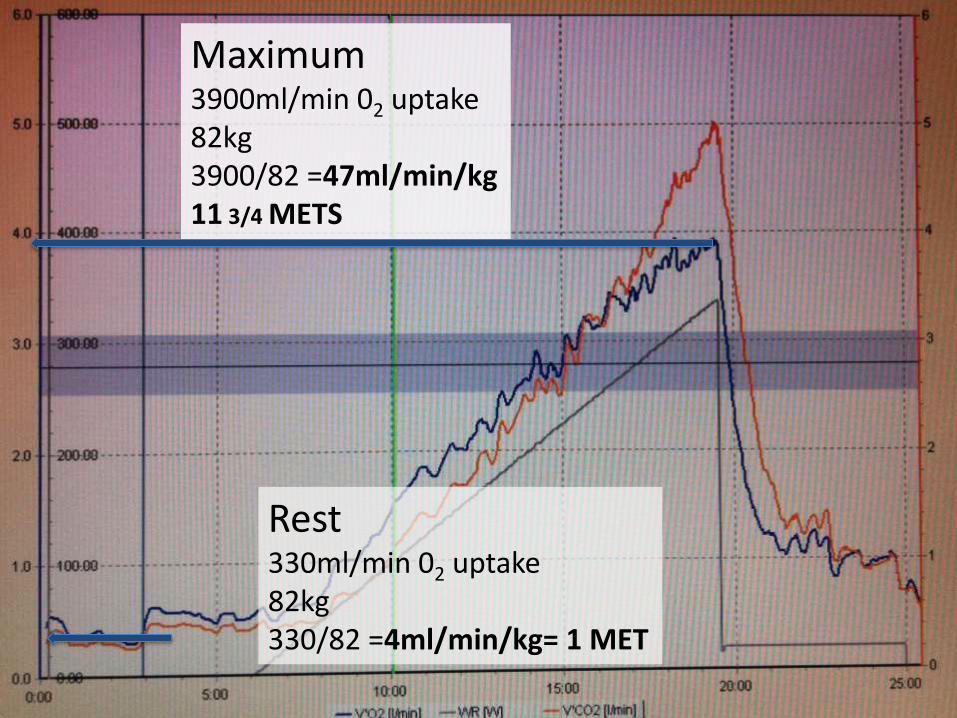
Rest330ml/min 02 uptake82kg330/82 =4ml/min/kg= 1 MET
Maximum3900ml/min 02 uptake82kg3900/82 =47ml/min/kg11 3/4 METS

Guideline 16
ACC AHA
• Surgery Urgency
• Patient Specific risks / Comorbidities
• Patient Exercise Capacity
• Surgery Severity
ESC 2009
• Biomarkers
Guideline 17• Biomarkers in Guidelines 2009 and 2014
“a characteristic that can be objectively measured that is an indicator of pathology or an abnormal response to treatments”
Troponin - myocardial cell injury
BNP - myocardial wall stress increases
+ pro NT BNP
CRP - liver and smooth muscle
ESC, Biccard, Devereaux 2012

Guideline 18• Biomarkers in ESC Guidelines 2009
Troponin
Postop – small associated mortality ‘VISION’
Preop – predictive, no ideal cut off
BNP + pro NT BNP
Ht Failure /IHD / ACS - rises relate to outcome
Preop – adds predictive ability >48 pg/ml
CRP – ‘inflammatory marker’
ESC, Biccard, Devereaux 2012

Guideline 19
• AHA/ACC 2014‘no data to suggest that targeting biomarkers for treatment or
intervention will lower postoperative risk.
• Biomarkers in ESC Guidelines 2009Higher in patients that have postoperative cardiac events or die
Troponin
BNP
CRP

Assessing CVS disease: Together

ACC/AHA2014
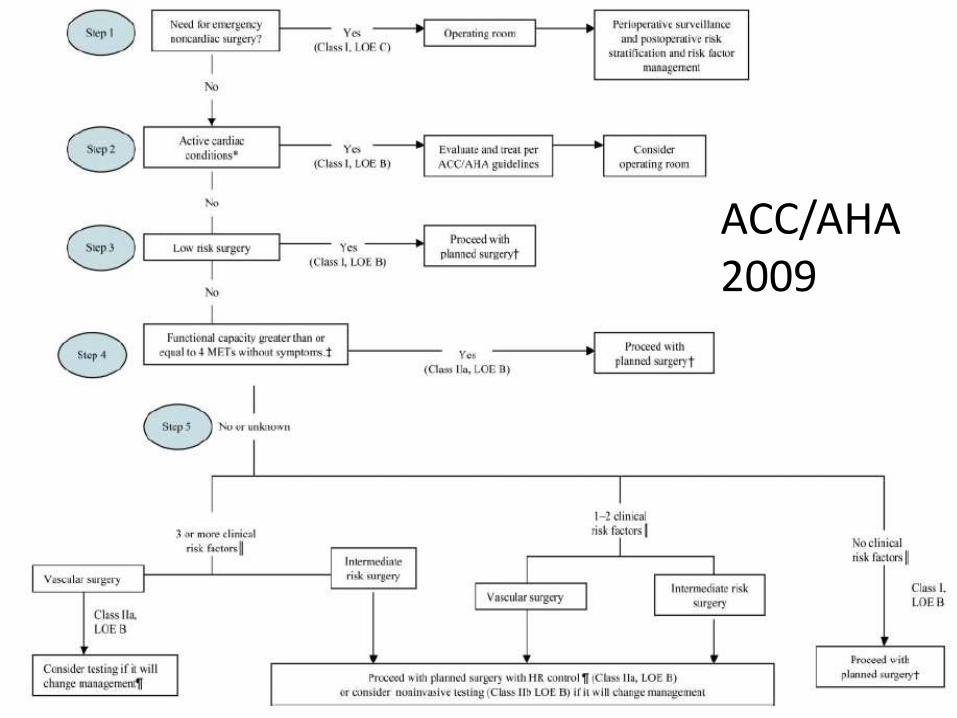
ACC/AHA2009

ESC 2009

Putting it together 1: Urgency
• Emergency or Urgent operation
• Time- limited or Elective consider further

Putting it together 2:Active Cardiac Condition
Putting it together 2:Active Cardiac Condition
• Serious’ = ‘active cardiac condition’
–Recent MI/Unstable Angina
–Acute LVF
– Serious abnormal rhythm
– Severe valve disease
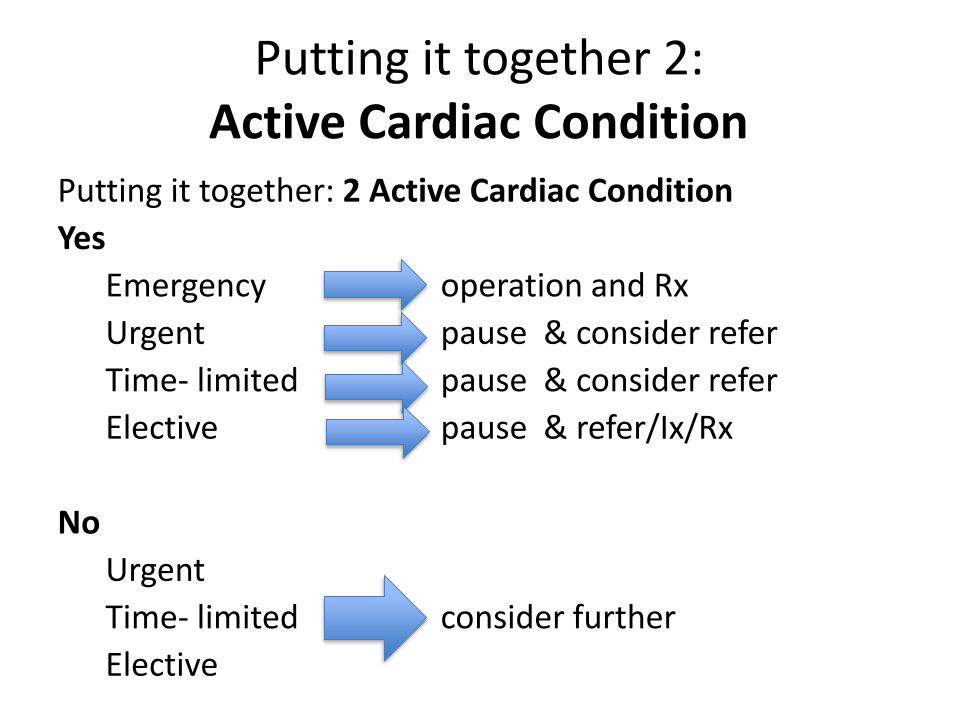
Putting it together 2:Active Cardiac Condition
Putting it together: 2 Active Cardiac Condition
Yes
Emergency operation and Rx
Urgent pause & consider refer
Time- limited pause & consider refer
Elective pause & refer/Ix/Rx
No
Urgent
Time- limited consider further
Elective
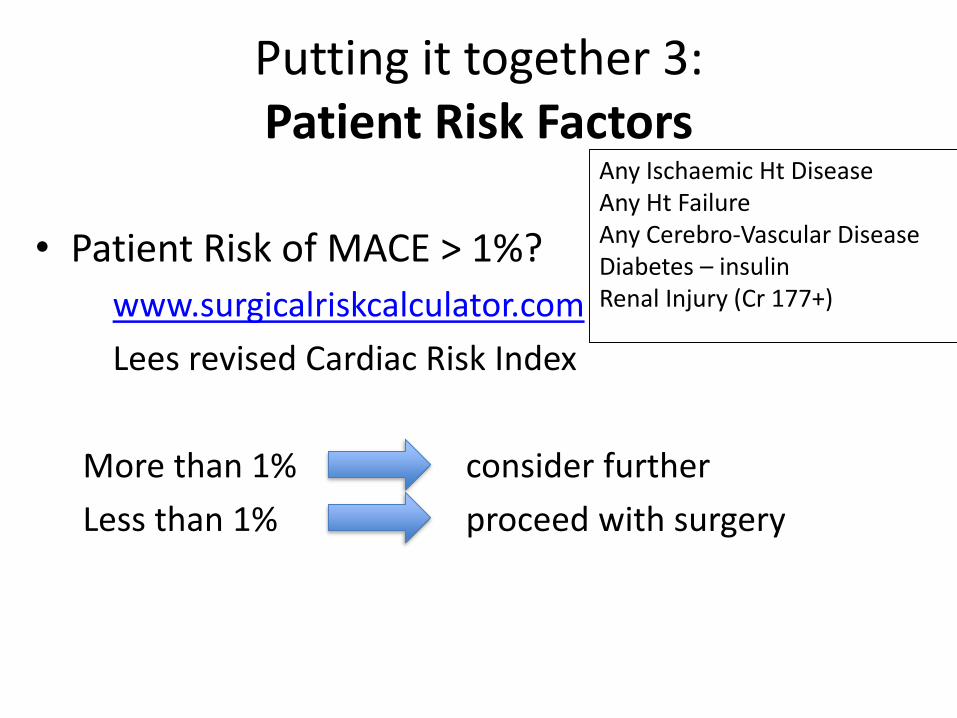
Putting it together 3:Patient Risk Factors
• Patient Risk of MACE > 1%?
www.surgicalriskcalculator.com
Lees revised Cardiac Risk Index
More than 1% consider further
Less than 1% proceed with surgery
Any Ischaemic Ht DiseaseAny Ht FailureAny Cerebro-Vascular DiseaseDiabetes – insulinRenal Injury (Cr 177+)

Putting it together 4: Operation risk
?Low risk surgery Proceed operation
Intermediate high consider further
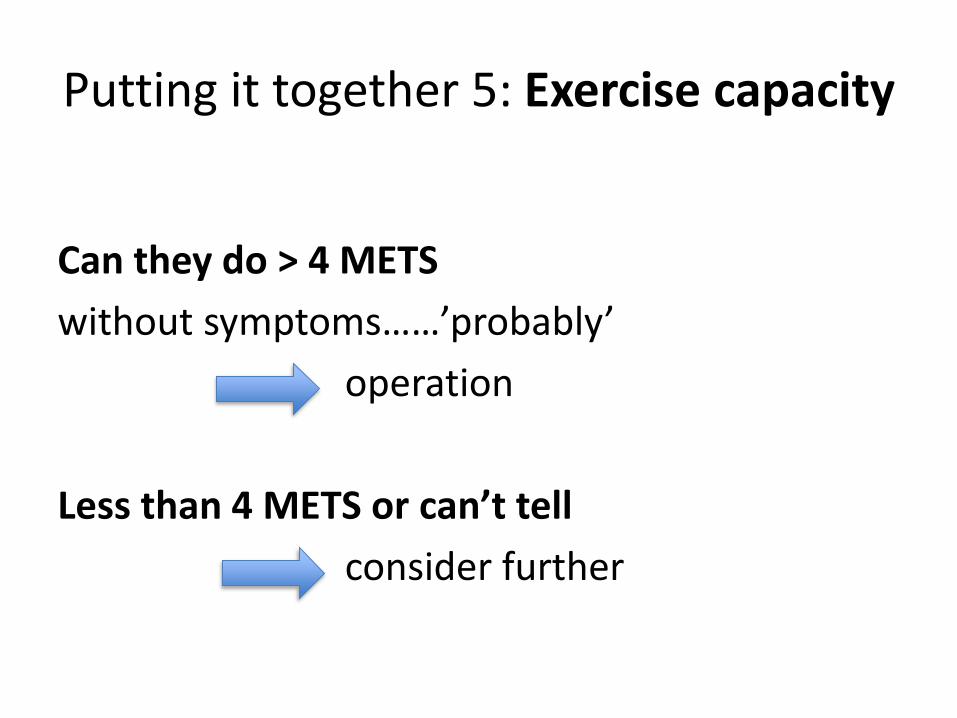
Putting it together 5: Exercise capacity
Can they do > 4 METS
without symptoms……’probably’
operation
Less than 4 METS or can’t tell
consider further

Putting it together: Investigations
Always in the context of ‘what next?’ ie
‘will/should it change management?’
“Consider testing” ACC/AHA
Stress ECHO
Myocardial Perfusion Scan
CPEx – includes Exercise ECG
Exercise ECG
MRI or CT

ECHO Evidence• Valves, Function, estimates pulmonary pressures
• Degree of dysfunction, regional wall motion abn
• LVEF <40% - 2x higher risk
– sensitivity 43%
– positive predictive 13%
• “resting LV function was not found to be a consistent predictor of perioperative ischemic events or death”
• But ECHO enthusiasts in preassessment..
– 30% new CVS disease, Mx 20% Mx34%
Halm, Rofdhe, Canty

ECHO indication
Routine Evaluation – NO
Dyspnea of unknown origin – reasonable
New murmur - reasonable
Ht Failure with symptoms - reasonable
Ht Failure clinically stable - ‘may be considered’
Valves clinically stable - ‘recommended’ > 1 year
ACC/AHA
CPEx / CPET BackgroundFunctional assessment
Population data – survival
VO2 peak, AT, VE/VCO2, ECG ischaemia etc
But
Associations with outcome and complications
Most studies unblinded, small
Await results of only RCT
‘Prehabilitation’ studies- some positives
Older, Hennis, Snowden, O’Doherty

n=548
Lower anaerobic threshold worse: higher mortalityRaised Respiratory Equivalent: higher mortality
Mortality
AT more 14 ml/min /kg 0%AT more 11 ml/min /kg but other badness 1.7%AT less 11 ml/min /kg 4.6%
CPEx / CPET Background
Older 1999
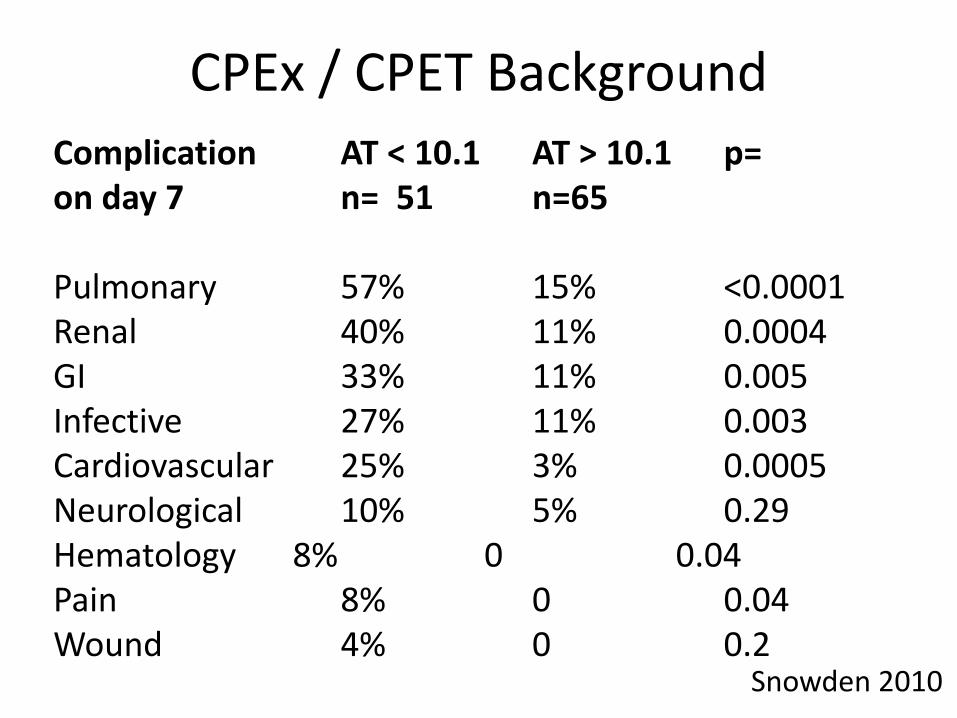
Complication AT < 10.1 AT > 10.1 p=on day 7 n= 51 n=65
Pulmonary 57% 15% <0.0001Renal 40% 11% 0.0004GI 33% 11% 0.005Infective 27% 11% 0.003Cardiovascular 25% 3% 0.0005Neurological 10% 5% 0.29Hematology 8% 0 0.04Pain 8% 0 0.04Wound 4% 0 0.2
Snowden 2010
CPEx / CPET Background
CPEx / CPET use• ACC/AHA 2014
“…considered for patients undergoing elevated risk procedures with unknown functional capacity”
• Awaiting RCT on CPEx vs Dr
• Use very variable, increasing
• Best not to emphasise one single value
– VO2 peak, AT, VE/VCO2, ECG ischaemia
• Enthusiasts vs sceptics

B Block? background
• B blockers – in community– reduce adrenergic activity + myocardial 02 use
– associated with survival
• RCT Perioperative studiesMangano
POISE
‘DECREASE’, Others
• Observational perioperative data
• US and European Perioperative Guidelines
Mangano, London, Sear, Devereaux, Bouri

B Block?
ESC 2009

B Block?: Endpoints important!POISE Lancet 2008• 8351 patients• with/at risk of, atherosclerotic disease • non-cardiac surgery • B Block 24 hrs preoperatively – 30 days postop
Metoprolol vs Placebo
MI 4·2% vs 5·7% 0·84 p=0·002
Stroke 1·0% vs 0·5% 2·17 p=0·005BP 15.0% vs. 9.7% p < 0.0001Bradycardia 6.6% vs. 2.4% p < 0.0001
Deaths 3·1% vs 2·3% 1·33 p=0·03
Devereaux


B Block• Maintain current B Blockade
• Treat concomitant anaemia
• Meta-analysis / prospective studies don’t support
• May use in ‘high risk’ people only– Those that may be on B Blockers anyway
– rCRI >1
• ?Atenolol or Bisoprolol
• Start /titrate 60-80 bpm
• ?7+ days before

‘VISION’: MINS15,065 patients > 45+ yrs; in-patient non-cardiac surgery
‘MINS’ myocardial injury after non-cardiac surgery=
Troponin T level of > 0.03 ng/ml
MINS 30-day mortality 3.87x
(adjusted hazard ratio; 95% CI, 2.96-5.08)
8.0% had MINS
58.2% of these did not fulfill a conventional MI definition
15.8% of patients with MINS had ischemic symptoms
Botto 2014

Summary
• Introduction
• Basic Principles
• Guidelines: Decisions
• Guidelines: Putting it all together
• Which test?
• ECHO
• CPEx
• B Block?
• Summary

Thank you
For listening
Please Google ‘stephens UCL’ for website
This full talk
Some References
AHA/ACC and European Guidelines