evaluation of an intraoral maxillary molar distalization technique
TRANSCRIPT

Evaluation of an intraoral maxillary molar distalization technique
Joydeep Ghosh, BDS, MSfl and Ram S. Nanda, DDS, MS, PhD ~ Oklahoma City, Okla.
The purpose of this study was to determine the effects of the pendulum appliance on distalization of maxillary molars and the reciprocal effects on the anchor premolars and maxillary incisors. Initial and follow-up cephalometric radiographs were obtained on 41 subjects (26 girls and 15 boys) who were treated with the pendulum appliance for bilateral distalization of the maxillary first molar teeth, for correction of the Class II molar relationship or for gaining space in the maxillary arch. Dental casts were available on 31 patients. Dental, skeletal, and soft tissue changes were determined. The mean maxillary first molar distalization was 3.37 mm, with a distal tipping of 8.36 ~ The mean reciprocal mesial movement of the first premolar was 2.55 mm, with a mesial tipping of 1.29 ~ The maxillary first molar position intruded 0.1 mm, whereas the first premolar extruded 1.7 mm. The transverse width between the mesiobuccal cusps of the first molars increased 1.40 mm. The maxillary second molars were also distalized 2.27 mm, tipped distally 11.99 ~ and moved buccally 2.33 mm. The effect of distalization on the maxillary third molars was extremely variable. The eruption of maxillary second molars had minimal effect on distalization of first molars. The lower anterior face height increased by 2.79 mm. This increase was greater in patients with higher Frankfort-mandibular plane angle measurements. The pendulum appliance is an effective and reliabJe method for distalizing maxillary molars, provided the anchor unit is adequately reinforced. Its major advantages are minimal dependence on patient compliance, ease of fabrication, one-time activation, adjustment of the springs if necessary to correct minor transverse and vertical molar positions, and patient-acceptance. (Am J Orthod Dentofac Orthop 1996;110:639-46.)
T r e a t m e n t of Class II malocclusions fre- quently requires distalization of maxillary molars into a Class I relationship. A variety of treatment modalities have been suggested, including those that are heavily dependent on patient compliance such as extraoral trac- tion, l-9 removable appliances with finger springs,'~ Wil- son arches, ]1'12 and sliding jigs with Class II intermaxil- lary elastics) 3 The techniques that rely less on patient cooperation include repelling magnets, j4-'6 transpalatal arches, 17 compressed coil springs, 18 and the Herbst ap- pliance. 19
Extraoral traction with the headgear has been one of the earliest methods used to distalize the maxilla and the maxillary teeth. Since the introductory reports on its use in different malocclusions by Kingsley 2~ and Angle, 2' the headgear has been shown by several authors 1-9 to be very effective in maxillary molar distalization with movements possible in all planes of space. Cetlin and Ten Hoeve 1~ recommended the use of an intraoral re-
From the Department of Orthodontics, University of Oklahoma College of Dentistry. aVisiting Assistant Professor and research associate. bProfessor and Chair. Reprint requests to: Dr. Joydeep Ghosh, Department of Orthodontics, College of Dentistry, 1001 S.L. Young Blvd., Oklahoma City, OK 73190. Copyright �9 1996 by the American Association of Orthodontists. 0889-5406/96/$5.00 + 0 8/1/65231
movable acrylic appliance with finger springs to the mesial of the maxillary first molars to tip the crowns distally. The roots were then distalized by part-time headgear wear, resulting in overall bodily tooth move- ment. Wilson and Wilson, "'~z in a modification of the labiolingual technique, 22 used the mandibular arch as anchorage for Class II elastics on the maxillary arch. The maxillary arch is fitted with coil springs, com- pressed on the first molar headgear tube. To reinforce mandibular anchorage, a removable lingual arch is used. Muse et a l . 23 studied the effects of Wilson molar distal- ization and found the rate of maxillary molar movement to be 0.56 mm per month. This was an overall average, and the amount of distalization during the first and subsequent months were not given. A significant propor- tion of the Class 1I correction occurred with the man- dibular molars moving mesially. Tweed 13 demonstrated the fabrication and application of sliding jigs to distalize maxillary teeth, using Class II elastics from a mandibu- lar arch that had been prepared for anchorage.
Despite their success in tooth movement, all these modalities have the major disadvantage of heavy depen- dence on the patient to comply and to follow directions. Thus appliances were introduced that minimized reli- ance on the patient and were doctor-controlled. Gianelly et al. ~''~ advocated the use of repelling intraoral mag- nets to distalize maxillary first molars, with the anterior
639

640 Ghosh and Nanda American Journal of Orthodontics and Dentofacial Orthopedics December 1996
Fig. 1. A, Pendulum appliance. B, Intraoral view of pendulum appliance.
teeth and the palate as anchorage. The repelling action of the magnets produced molar distalization at an over- all average rate of 1.7 mm per month, without maxillary second molars erupted, and 0.75 to 1.0 mm per month with second molars erupted. Though magnets were shown to be effective, they are very expensive, and the force exerted drops considerably with a small amount of movement. Hence, the patient has to be recalled once
e v e r y 1 to 2 weeks to reactivate the appliance. Com- pressed stainless or nickel titanium coil springs have been used in lieu of the magnets to distalize maxillary molars, is These have a greater range of action than magnets but need reactivation every month. The Herbst appliance has been shown to have maxillary molar dis- talizafion effects, in addition to the already well-docu- mented effects on the mandible. 19 The appliance, how- ever, is prone to breakage and is limited to use in pa- tients who can tolerate proclination of mandibular incisors.
Keeping these shortcomings in mind, Hilgers 24 in- troduced an appliance for Class lI correction in noncom- pliant patients to expand the maxilla and simultaneously
rotate and distalize the maxillary first molars. A modifi- cation of this appliance resulted in the "pendulum" appliance (Fig. 1), a new mechanism for maxillary mo- lar distalization in the treatment of noncompliant pa- tients with Class II malocclusions. 2~ The appliance con- sisted of a palatal acrylic button attached to the first premolar teeth through occlusally bonded rests o r re- taining wires soldered to bands on these teeth, along with 0.032-inch titanium molybdenum alloy (TMA) springs that originated from the palatal acrylic and en- gaged in lingual sheaths on maxillary first molar bands. The springs were activated approximately 60 ~ to pro- duce a force of 230 gm per side. Thus they would produce a swinging arc, or pendulum of force, from the palate to the molars. A loop within each spring could be adjusted to allow for expansion and to prevent any tendency for the maxillary molar to move lingually into crossbite. Once the molars were distalized, they could be stabilized with either a small Nance button attached to the maxillary first molars, a headgear, or fixed appli- ances, along with a maxillary utility arch wire or a stopped continuous arch wire. Hilgers also recom- mended occlusally bonded rests on the second premo- lars to increase stability of the palatal acrylic. These could be removed once first molar distalization was achieved to allow the second premolars to drift distally. Hilgers 25 claimed that it is not unusual to see as much as 5 mm of distal molar movement in 3 to 4 months of treatment with this appliance.
The purpose of this clinical study was (1) to deter- mine the nature of maxillary molar movement in the three planes of space, with the pendulum appliance, (2) to determine the extent of mesial movement of the an- chor premolars and maxillary incisors, (3) to determine the effect of erupted maxillary second molars on distal- ization of the first molar, and (4) to determine the ef- fects, if any, of distalization of maxillary molars on mandibular position.
MATERIALS AND METHODS
Cephalometric radiographs and dental casts were ob- tained on 41 subjects from the practices of three clinicians (25, 13, and 3 patients, respectively). There were 26 girls with a mean age of 12 years, 5 months + 1 year, 10 months (range of 9 years, 6 months to 17 years, 11 months) and 15 boys with a mean age of 12 years, 5 months_+ I year, 2 months (range of l0 years, 9 months to 15 years, 6 months) in the study. Gender differences were not considered because of the short-term of use of the pendulum appliance. All the patients met the following criteria:
1. Use of the pendulum appliance as the first phase of orthodontic treatment for bilateral distalization of the maxillary first molar teeth for correction of the Class II molar relationship or gaining space in the maxillary arch.
2. Nonextraction treatment plan. 3. Good oral hygiene and no damage to the appliance, as

American Journal of Orthodontics and Dentofacial Orthopedics Ghosh and Nanda 641 Volume 110, No. 6
Pm Or
--</ ,
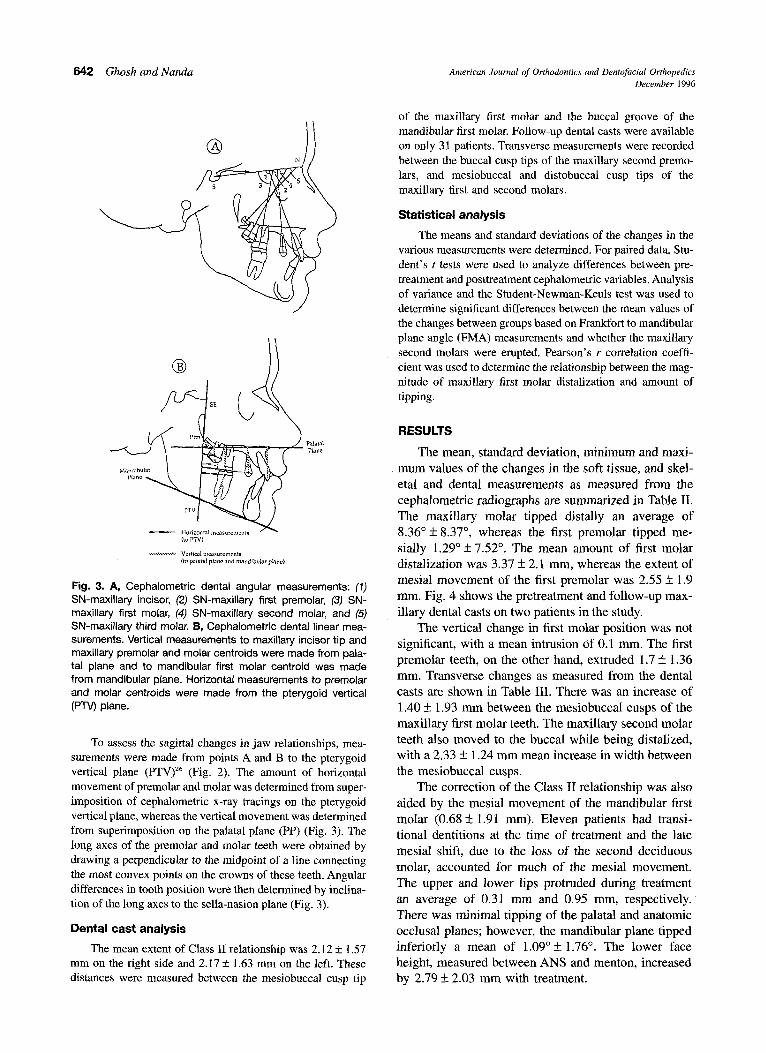
Fig. 2. Cephalometric soft tissue and skeletal measurements used in study: (1) upper lip to E-plane, (2) lower lip to E-plane, (3) SN-palatal plane angle, (4) SN-anatomic occlusal plane angle, (5) Frankfort-mandibular plane angle, (6) PTV to A point, (7') PTV to B point, and (8) ANS to menton.
determined from the treatment records. 4. Good quality radiographs, with good landmark visu-
alization and good head posture, with minimal or no rotation of the head, taken before and immediately after removal of the appliance.
5. No other molar distalization procedure, e.g., headgear or elastics, performed in the time period between the two radiographs.
Cephalometric analysis
Cephalometric radiographs were obtained on all patients before treatment. Because the radiographic magnification fac- tor was similar between the three practices, no correction was necessary. The soft tissue and skeletal measurements are shown in Fig. 2 and dental measurements are shown in Fig. 3. When a double image of the molars and first premolars was present, all measurements were made from the distal and smaller image. Centroid points were constructed for the crowns of all three maxillary molars, the mandibular first molar, and the maxillary first premolar as the midpoint be- tween the greatest mesial and distal convexity of the crowns of these teeth, as seen on the cephalometric radiograph. Table I shows the measurements made and summary statistics of the pooled sample before initiation of treatment.
The pendulum appliance
All patients received a pendulum appliance similar to the one described by Hilgers. 25 The palatal acrylic button was about the size of a quarter (25 mm diameter) and was anchored to the first and second premolar teeth (or the first and second deciduous molars) with wires bonded to the occlusal surfaces. The appliances were very similar for all patients, with the exception that two of the three clinicians (for a total of 16 patients) preferred a band on the first
premolar teeth to which the wire from the palatal acrylic was soldered, instead of bonded on the occlusal surface. All appliances used 0.032-inch TMA wire springs, which were inserted into lingual sheaths on the first molar bands. Typi- cally, a one-time initial activation of 60 ~ to 70 ~ was deliv- ered. The adjustment loops on the springs were not modified through treatment, and the appliances were monitored at monthly intervals. After the first molars were distalized to the desired extent, the second premolars were released from the anchor unit and allowed to drift distally. In 29 patients, incisor brackets were bonded toward the end of molar distalization for placement of a sectional wire to align the incisors. After molar distalization was completed and the pendulum appliance removed, a utility arch was placed to
prevent relapse. Twenty-three patients did not show the emergence of
maxillary second molars into the oral cavity. Maxillary second molars were erupted in the rest (18 patients) and were neither banded nor bonded with any attachments. The effects of second molar position were measured and would reflect the indirect effect of first molar distalization. All patients had maxillary third molars visible radiographically in their bony crypts. The positions of the third molars were also evaluated, even though they were unerupted and encrypted in the maxillary tuberosity area.
A second cephalometric radiograph was taken at the time of removal of the pendulum appliance. The mean time period between the initial and follow-up radiograph was 6.21 months (SD 1.44 months, range 4 to 10 months). All the radiographs were traced on acetate paper with a 0.5 mm pencil by one author and digitized. To determine the error of measurement, 20 radiographs were retraced and digitized and 20 casts were remeasured. The combined method error was found to be less than 0.6 ~ and 0.5 mm for any measurement
used.
642 Ghosh and Nanda American Journal of Orthodontics and Dentofacial Orthopedics December 1996
|
Mandibular
- - H o r i z o n t a l n~easurements (~o PTV)
. . . . ~ , - - - ~ - , Vertical measurements (to palatal pbne ,~nd mandibular plaice)
Fig. 3. A, Cephalometric dental angular measurements: (1) SN-maxillary incisor, (2) SN-maxillary first premolar, (3) SN- maxillary first molar, (4) SN-maxillary second molar, and (5) SN-maxillary third molar. B, Cephalometric dental linear mea- surements. Vertical measurements to maxillary incisor tip and maxillary premolar and molar centroids were made from pala- tal plane and to mandibular first molar centroid was made from mandibular plane. Horizontal measurements to premolar and molar centroids were made from the pterygoid vertical (PTV) plane.
To assess the sagittal changes in jaw relationships, mea- surements were made from points A and B to the pterygoid vertical plane (PTV) 26 (Fig. 2). The amount of horizontal movement of premolar and molar was determined from super- imposition of cephalometric x-ray tracings on the pterygoid vertical plane, whereas the vertical movement was determined from superimposition on the palatal plane (PP) (Fig. 3). The long axes of the premolar and molar teeth were obtained by drawing a perpendicular to the midpoint of a line connecting the most convex points on the crowns of these teeth. Angular differences in tooth position were then determined by inclina- tion of the long axes to the sella-nasion plane (Fig. 3).
Dental cast analysis
The mean extent of Class II relationship was 2.12 5- 1.57 mm on the right side and 2.175- 1.63 mm on the left. These distances were measured between the mesiobuccal cusp tip
of the maxillary first molar and the buccal groove of the mandibular first molar. Follow-up dental casts were available on only 31 patients. Transverse measurements were recorded between the buccal cusp tips of the maxillary second premo- lars, and mesiobuccal and distobuccal cusp tips of the maxillary first and second molars.
Statistical analysis
The means and standard deviations of the changes in the various measurements were determined. For paired data, Stu- dent's t tests were used to analyze differences between pre- treatment and posttreatment cephalometric variables. Analysis of variance and the Student-Newman-Keuls test was used to determine significant differences between the mean values of the changes between groups based on Frankfort to mandibular plane angle (FMA) measurements and whether the maxillary second molars were erupted. Pearson's r correlation coeffi- cient was used to determine the relationship between the mag- nitude of maxillary first molar distalization and amount of tipping.
RESULTS
The mean, standard deviation, minimum and maxi- mum values of the changes in the soft tissue, and skel- etal and dental measurements as measured from the cephalometric radiographs are summarized in Table II. The maxil lary molar t ipped distally an average of 8.36~ 8.37 ~ whereas the first premolar t ipped me- sially 1.29~ 7.52 ~ The mean amount of first molar distalization was 3.37 _+ 2.1 mm, whereas the extent of mesial movement of the first premolar was 2.55 +_ 1.9 ram. Fig. 4 shows the pretreatment and follow-up max- i l lary dental casts on two patients in the study.
The vertical change in first molar posit ion was not significant, with a mean intrusion of 0.1 mm. The first premolar teeth, on the other hand, extruded 1.7 -+ 1.36 ram. Transverse changes as measured from the dental casts are shown in Table III. There was an increase of 1.40 -+ 1.93 m m between the mesiobuccal cusps of the maxil lary first molar teeth. The maxil lary second molar teeth also moved to the buccal while being distalized, with a 2.33 _+ 1.24 m m mean increase in width between the mesiobuccal cusps.
The correction of the Class II relationship was also aided by the mesial movement of the mandibular first molar (0.68 • 1.91 mm). Eleven patients had transi- tional dentitions at the time of treatment and the late mesial shift, due to the loss of the second deciduous molar, accounted for much of the mesial movement. The upper and lower lips protruded during treatment an average of 0.31 mm and 0.95 rnm, respectively. There was minimal t ipping of the palatal and anatomic occlusal planes; however, the mandibular plane t ipped inferiorly a mean of 1.09~ 1.76 ~ The lower face height, measured between ANS and menton, increased by 2.79 _+ 2.03 m m with treatment.
American Journal of Orthodontics and Dentofacial Orthopedics Volume l l0, No. 6
Ghosh and Nanda 643
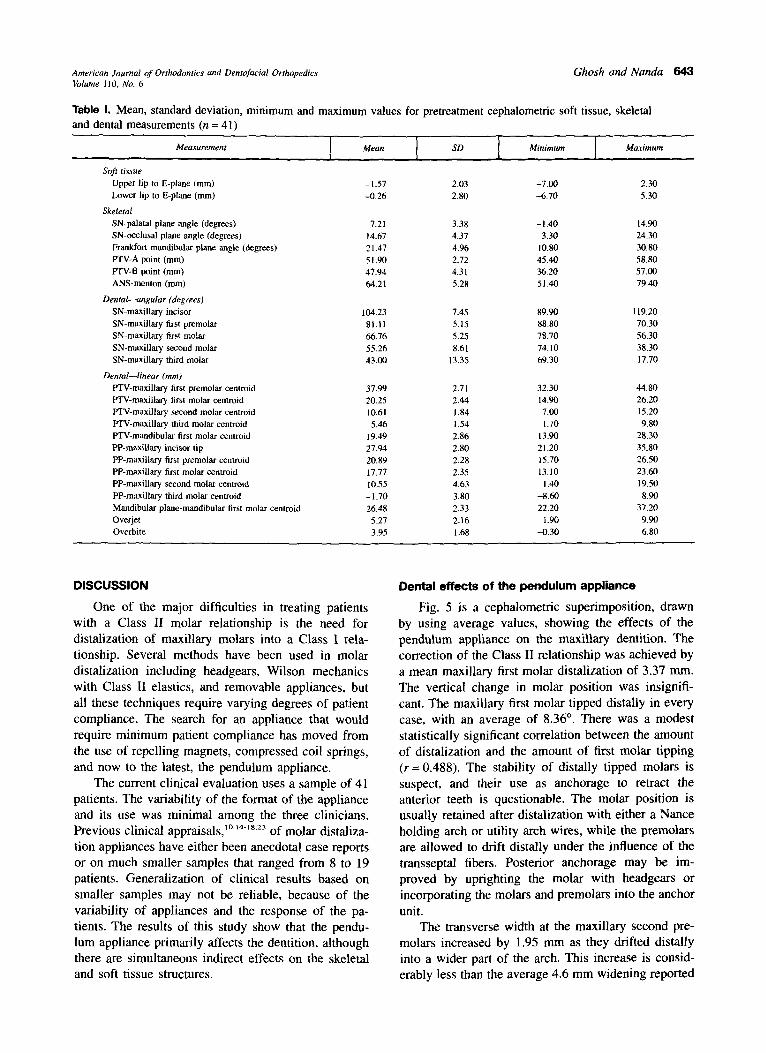
Table I. Mean, standard deviation, minimum and maximum values for pretreatment cephalometric soft tissue, skeletal and dental measurements (n = 41)
Measurement ] Mean I SD ~ _ , M i n i m u m - I Maximum
Soft tissue Upper lip to E-plane (mm) -1.57 2.03 -7.00 2,30 Lower lip to E-plane (ram) -0.26 2.80 -6.70 530
Skeletal SN-palatal plane angle (degrees) 7.21 3.38 -1.40 14.90 SN-occlusal plane angle (degrees) 14.67 4.37 3.30 24.30 Frankfort-mandibular plane angle (degrees) 21.47 4.96 10.80 30.80 PTV-A point (mm) 51,90 2.72 45.40 58.80 PTV-B point (mm) 47.94 4.31 36.20 57.00 ANS-menton (ram) 6421 5.28 51.40 79.40
Dental---angular (degrees) SN-maxillary incisor 104.23 7.45 89.90 119.20 SN-maxillary first premolar 8 I. 11 5.15 88.80 70.30 SN-maxillary first molar 66.76 5.25 78.70 56.30 SN-maxillary second molar 55.26 8.61 74, l0 38.30 SN-maxillary third molar 43.00 13.35 69.30 17.70
Dental--linear (ram) PTV-maxillary first premolar centroid 37,99 2.71 32.30 44,80 PTV-maxillary first molar centroid 20.25 2.44 14.90 26.20 PTV-maxillary second molar centroid 10.61 1.84 7.00 15,20 PTV-maxillary third molar centroid 5.46 1.54 1.70 9.80 PTV-mandibular first molar centroid 19.49 2.86 13.90 28,30 PP-maxillary incisor tip 27.94 2.80 21.20 35.80 PP-maxillary first premolar centroid 20.89 2.28 15.70 26.50 PP-maxillary first molar centroid 17.77 2.35 13.10 23.60 PP-maxillary second molar centroid 10.55 4.63 1.40 19.50 PP-maxillary third molar centroid -1.70 3.80 -8.60 8.90 Mandibular plane-mandibular first molar centroid 26.48 2.33 22.20 37.20 Overjet 5.27 2.16 1.90 9.90 Overbite 3.95 1.68 -0.30 6.80
DISCUSSION
One of the major difficulties in treating patients with a Class II molar relationship is the need for distalization of maxillary molars into a Class I rela- tionship. Several methods have been used in molar distalization including headgears, Wilson mechanics with Class II elastics, and removable appliances, but all these techniques require varying degrees of patient compliance. The search for an appliance that would require minimum patient compliance has moved from the use of repelling magnets, compressed coil springs, and now to the latest, the pendulum appliance.
The current clinical evaluation uses a sample of 41 patients. The variability of the format of the appliance and its use was minimal among the three clinicians. Previous clinical appraisals, ~~ of molar distaliza- tion appliances have either been anecdotal case reports or on much smaller samples that ranged from 8 to 19 patients. Generalization of clinical results based on smaller samples may not be reliable, because of the variability of appliances and the response of the pa- tients. The results of this study show that the pendu- lum appliance primarily affects the dentition, although there are simultaneous indirect effects on the skeletal and soft tissue structures.
Dental effects of the pendulum appliance
Fig. 5 is a cephalometric superimposition, drawn by using average values, showing the effects of the pendulum appliance on the maxillary dentition. The correction of the Class II relationship was achieved by a mean maxillary first molar distalization of 3.37 ram. The vertical change in molar position was insignifi- cant. The maxillary first molar tipped distally in every case, with an average of 8.36 ~ There was a modest statistically significant correlation between the amount of distalization and the amount of first molar tipping ( r= 0.488). The stability of distally tipped molars is suspect, and their use as anchorage to retract the anterior teeth is questionable. The molar position is usually retained after distalization with either a Nance holding arch or utility arch wires, while the premolars are allowed to drift distally under the influence of the transseptal fibers. Posterior anchorage may be im- proved by uprighting the molar with headgears or incorporating the molars and premolars into the anchor unit.
The transverse width at the maxillary second pre- molars increased by 1.95 mm as they drifted distally into a wider part of the arch. This increase is consid- erably less than the average 4.6 mm widening reported
644 Ghosh and Nanda American Journal of Orthodontics and Dentofacial Orthopedics December 1996
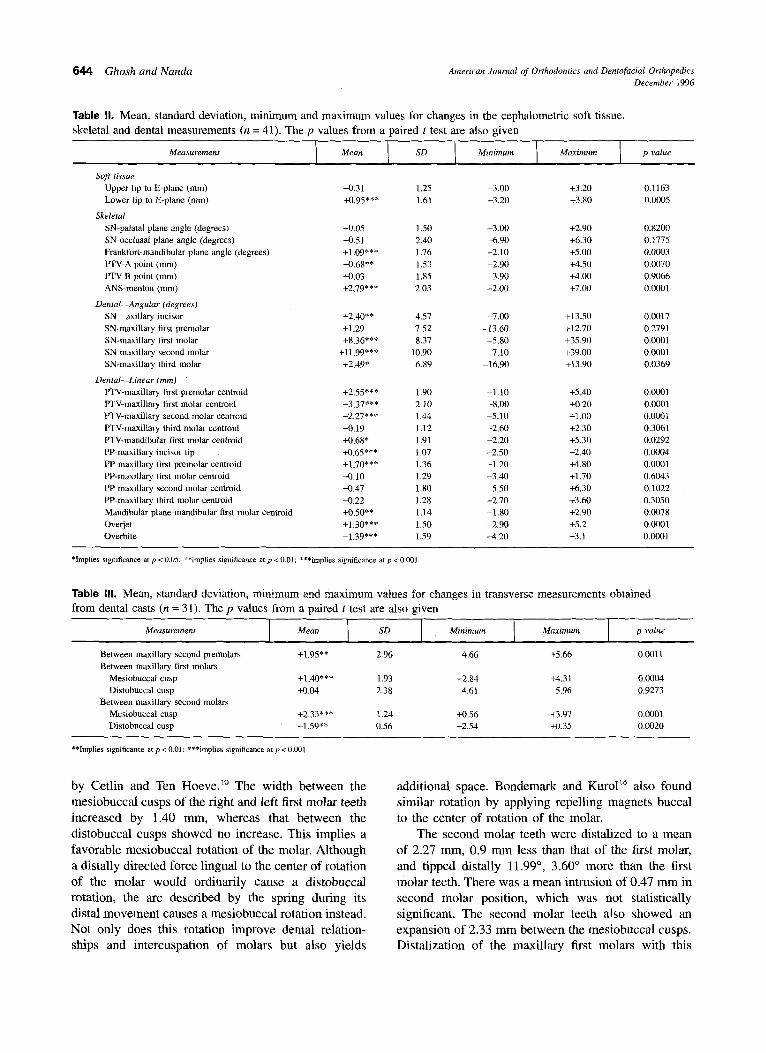
Table II. Mean, standard deviation, minimum and maximum values for changes in the cephaiometric soft tissue, skeletal and dental measurements (n = 41). The p values from a paired t test are also given
Soft tissue Upper lip to E-plane (ram) +0.31 1.25 -3.00 +3.20 0.1163 Lower lip to E-plane (ram) +0.95*** 1.61 -3.20 +3.80 0.0005
Skeletal SN-palatal plane angle (degrees) -0.05 1.50 -3.00 +2.90 0.8200 SN-occlusal plane angle (degrees) -0.51 2.40 -6.90 +6.30 0.1775 Frankfort-mandibular plane angle (degrees) +1,09"** 1.76 -2,10 +5.00 0,0003 PTV-A point (mm) +0,68** 1.53 -2.90 +4.50 0.0070 PTV-B point (mm) +0,03 1.85 -3.90 +4.00 0.9066 ANS-menton (ram) +2,79*** 2.03 -2.00 +7.00 0.0001
Dental--Angular (degrees) SN axillary incisor +2.40** 4.57 -7,00 +13.50 0.0017 SN-maxillary first premolar +1.29 7.52 -13,60 +12.70 0.2791 SN-maxillary first molar +8.36*** 8.37 -5,80 +35.90 0.0001 SN-maxillary second molar +11.99"** 10.90 -7.10 +39,00 0,0001 SN-maxillary third molar +2.49* 6.89 -16.90 +13,90 0.0369
Dental- -Linear (ram) PTV-maxillary first premolar eentroid +2.55*** 1.90 -1,10 +5.40 0.0001 PTV-rnaxillary first molar centroid -3.37*** 2.10 -8.00 +0.20 0.0001 PTV-maxiltary second molar centroid -2.27*** 1.44 -5 . I0 +1.00 0.000t PTV-maxillary third molar centroid -0.19 1.12 -2.60 +2.30 0.3061 PTV-mandibular first molar centroid +0.68* 1.91 -2,20 +5.30 0.0292 PP-maxillary incisor tip +0.65*** 1.07 -2.50 +2.40 0.0004 PP-maxillary first premolar centroid +1.70"** 1.36 -1.20 +4.80 0.0001 PP-maxillary first molar centroid -0.10 1.29 -3.40 +1.70 0.6043 PP-maxillary second molar centroid -0.47 1.80 -5.50 +6.30 0.1022 PP-maxillary third molar centroid -0.22 1.28 -2.70 +3.60 0.3050 Mandibular plane-mandibular first molar centroid +0.50** 1.14 -1.80 +2.90 0.0078 Overjet +1.30"** 1.50 -2,90 +5.2 0.0001 Overbite -1.39"** 1.59 -4.20 +3.1 0.13001
*Implies significance at p < 0.05; *~implies significance at p < 0,01; * **implies significance at p < 0.001.
Table from dental casts (n = 31). The p values from a paired t test are also given
IlL Mean, standard deviation, minimum and maximum values for changes in transverse measurements obtained
Between maxillary second premolars +1.95"* 2.96 -4.66 +5.66 0.0011 Between maxillary first molars
Mesiobuccal cusp +1.40"** 1.93 -2.84 +4.3l 0.0004 Distobuccal cusp +0.04 2.38 -4.61 5.96 0.9273
Between maxillary second molars Mesiobuccal cusp +2.33*** 1.24 +0.56 +3.97 0.0001 Distobuccal cusp +1.59"* 0.56 -2.54 +0.35 0.0020
**Implies significance at p < 0.01; ***implies significance at p < 0,001.
by Cetlin and Ten Hoeve? ~ The width between the mesiobuccal cusps of the right and left first molar teeth increased by 1.40 ram, whereas that between the distobuccal cusps showed no increase. This implies a favorable mesiobuccal rotation of the molar. Although a distally directed force lingual to the center of rotation of the molar would ordinarily cause a distobuccal rotation, the arc described by the spring during its distal movement causes a mesiobuccal rotation instead. Not only does this rotation improve dental relation- ships and intercuspation of molars but also yields
additional space. Bondemark and Kuro116 also found similar rotation by applying repelling magnets buccal to the center of rotation of the molar.
The second molar teeth were distalized to a mean of 2.27 ram, 0.9 m m less than that of the first molar, and tipped distally 11.99 ~ , 3.60 ~ more than the first molar teeth. There was a mean intrusion of 0.47 m m in second molar position, which was not statistically significant. The second molar teeth also showed an expansion of 2.33 m m between the mesiobuccal cusps. Distalization of the maxillary first molars with this

American Journal of Orthodontics and Dentofacial Orthopedics Ghosh and Nanda Volume 110, No, 6
u C.,' %/', "%J ,~l
Fig. 5. Cephalometric superimposition, drawn using mean values, showing effects of pendulum appliance on maxillary dentition.
Fig. 4. Pretreatment and follow-up maxillary dental casts on two patients in study. Note increase in width between maxil- lary second molars with first molar distalization.
appliance therefore causes both distal as well as buccal tipping of the second molars. Bondemark and Kurol, ~6 on the other hand, found no change in the transverse dimension between the maxillary second molars with distalization of the first molars with the use of repelling magnets. In this study, there was less expansion be- tween the distobuccal cusps (1.59 mm) than the me- siobuccal cusps (2.33 mm) of the second molars, which implies a mesiobuccal rotation. Bondemark and Kurol ~6 found a similar rotation for the maxillary second molars with first molar distalization.
The effect of distalization on the maxillary third molars was extremely variable. No patient showed more than half of root formation on the third molar teeth, and only the crowns were visible in most radio- graphs. The third molars showed a net distal tipping of 2.49 ~ , but an insignificant amount of horizontal or vertical change in position (0.19 mm distalization and 0.22 mm intrusion). It would be interesting to follow- up these patients longitudinally to determine whether maxillary first molar distalization has any effect on either the timing, path of eruption or imminent impac- tion of maxillary third molars.
Loss of anchorage was measured at the first pre- molar teeth. The anchor unit, which consisted of the first and second premolars connected through a wire frame and acrylic coverage in the palatal depth, was unable to completely resist the reciprocal mesial force of the pendulum appliance. The first premolars were mesialized 2.55 mm, tipped mesially 1.29 ~ and ex- truded 1.7 ram. Thus, for every millimeter of distal
molar movement, the premolar moved mesially 0.75 mm. To reinforce the anchor unit, it is recommended that the anterior framework include all the incisors and canines and complete coverage of the palate. By using such a modified Nance button with repelling magnets to distalize maxillary molars, for every millimeter of distal molar movement, the premolar-incisor segment was found to move mesially 0.25 mm by Gianelly et al. j5 in eight patients and 0.35 mm by Bondemark and Kurol ]6 in 10 patients. J-hook headgears or Class II elastics attached to the anterior teeth would also help control the anchor unit; however, this would require patient compliance.
The overjet increased by 1.30 mm and the overbite decreased by 1.39 mm as a result of treatment. The maxillary central incisor was proclined an average of 2.40 ~ relative to the SN line. The upper lip protruded 0.31 mm and the lower lip protruded 0.95 mm relative to the E plane. However, this data must be interpreted with caution, because some of the protrusion of the incisor and lips may have resulted from slippage of anchorage and some may have resulted from the placement of brackets and the sectional wires on the incisors in 29 patients.
Effect of eruption of the maxillary second molar
There were no statistically significant differences in maxillary first molar movement, as well as anchorage loss between the group of l 8 patients who had erupted maxillary second molars and the 23 who did not, indicating that the eruption of maxillary second molars had minimal effect on first molar distalization. This is contrary to the beliefs of other clinicians '4'~7'~8 who state that distalization of the first molar is dependent on the stage of eruption of the second molar and that maxillary first molar distalization be accomplished before the second molars erupt and/or when the second

646 Ghosh and Nanda American Jounzal of Orthodontics and Dentofacial Orthopedics December 1996
molars have erupted, the distalization of molars should be done in stages, first the second molars and then the first molars. The findings of Muse et a l . 23 support our conclusions.
Skeletal effects with the pendulum appliance
The pendulum appliance caused insignificant changes in the cant of the palatal and occlusal planes. The mandibular plane, on the other hand, showed a small backward rotation of 1.09 ~ with treatment, which caused a decrease in the overbite by 1.39 mm. Because there was no vertical change in the maxillary molar position and only an extrusion of 0.5 mm in mandibu- lar first molar position, most of the backward mandibu- lar rotation would have been caused by distalizing the maxillary molar "into the wedge." The lower anterior face height, as a result, increased by 2.79 mm.
The patients in the sample were arbitrarily divided into three groups, based on their initial Frankfort horizontal to mandibular plane angle (FMA) measure- ments. Group I consisted of patients with FMA mea- surements less than 20 ~ (n = 17), group II consisted of those with FMA measurements between 20 ~ and 25 ~ (n = 14), and group III consisted of those with mea- surements greater than 24 ~ (n = 10). Analyses of vari- ance were conducted to determine treatment differ- ences between these three groups. Although there was a trend for greater increase in FMA in group IlI (1.86 ~ versus 1.28 ~ in group II and 0.48 ~ in group I), this difference was not statistically significant at p < 0.05. The increase in the lower face height as a result of molar distalization, however, was more than double in group III (4.13 ram) than in group I (1.97 mm). This difference was statistically significant at p < 0.05. The increase in lower anterior face height in group II was 2.84 ram, which was not significantly different from either of the other two groups. The facial patterns of most patients were either short or in the range of normal, as indicated by the range of their Frankfort- mandibular plane angle between 10.8 ~ and 30.8 ~ and range of percentage of lower face height (ANS-men- ton/N-menton percent) between 49.1% and 60.8%. It is possible that the posterior mandibular rotation and the increase in lower face height could have been signifi- cant, had a larger sample of patients with high man- dibular plane angles been present.
CONCLUSIONS
The results of this study have shown that the pendulum appliance is an effective and reliable method for distalizing
maxillary molars. However, molar distalization is at the expense of moderate anchorage loss, which could possibly be reduced if the anchor unit is adequately reinforced by full palatal coverage and incorporation of all the teeth in the appliance. The major advantages of the appliance lie in its minimal dependence on patient compliance, ease of fabrica- tion, one-time activation, adjustment of the springs if neces- sary to correct minor transverse and vertical molar positions, and patient-acceptance.
We gratefully acknowledge the help received from Drs. J. Michael Steffen and Robert C. Penny, as well as the University of Oklahoma College of Dentistry for a seed grant that made the project possible.
REFERENCES
1, Graber TM. Extraoral force---facts and fallacies. Am J Orthod 1955;41:490-505. 2. Bernardi E A cephalometric analysis of the stability and type of movement obtained in
Class II, division 1 maloeclusions treated with extra-oral forces. [Masters thesis.] St Louis: Saint Louis University Department of Orthodontics, 1956.
3. Graber TM. Appliances at the crossroads. Am J Orthod 1956;42:683-701. 4. Klein PL. An evaluation of cervical traction on the maxilla and the upper first
permanent molar. Angle Or~hed 1957;27:61-8. 5. Newcomb MR. Some observations on extraoral treatment. Angle Orthod 1958;28:131-
48. 6. Kloehn SJ. Evaluation of cervical anchorage force in treatment. Angle Orthod
1961;31:91-104. 7. Funk AC. Mandibular response to headgear therapy and its clinical significance. Am J
Orthod 1967;53:182-216. 8. Melsen B, Enemark H. Effect of cervical anchorage studied by the implant method.
Trans Eur Orthod Soc 1969:435-47. 9. Wieslander L. Early or late cervical traction therapy of Class II malocclusion in the
mixed dentition. Am J Orthod 1975;67:432-9. 10. Cetlin NM, Ten Hoeve A. Nonextracton treatment. J Clin Ortbod 1983;17:396-413. 11. Wilson Re, Wilson WL. Enhanced orthodontics: book 1, concept, treatment and case
histories. Denver, Colorado: Rocky Mountain Orthodontics, 1988. 12. Wilson Re, Wilson WL. Enhanced orthodontics: book 2, force systems mechano-
therapy manual. Denver, Colorado: Rocky Mountain Orthodontics, 1988. 13. Tweed CH. Clinical orthodontics. Vol. 1. St Louis: CV Mosby, 1966. 14. Gianelly AA, Vaitas AS, Thomas WM, Berger OG. Distalization of molars with
repelling magnets. J C/in Orthod 1988;22:40-4. 15. Gianelly AA, Vaitas AS, Thomas WM. The use of magnets to move molars distally. Am
J Orthod Dentofac Orthop 1989;96:161-7. 16. Bondemark L, Kurol J. Distalization of maxillary first and second molars simultaneously
with repelling magnets. Eur J Orthod 1992;14:264-72. 17. Ten Hoeve A. Palatal bar and lip bumper in nonextraction treatment. J Clin Orthod
1985;19:272-91. 18. Jeckel N, Rakosi 32 Molar distalization by intra-oral force application. Eur J Orthod
t991;13:43-6. 19. Pancherz H, Anehus-Pancherz M. The headgear effect of the Herbst appliance: a
cephalometric long-term study. Am J Orthod Dentofac Orthop 1993;103:510-20. 20. Kingsley NW. A treatise on oral deformities as a branch of mechanical surgery. New
York: D Appleton, 1880:131-4. 21. Angle El-/. Treatment of malocclusion of the teeth and fractures of the maxillae. 6th ed.
Philadelphia: SS White Dental Manufacturing, 1900:115. 22. Oliver OA, Irish RE, Wood CR. Labio-lingual technic. St Louis: CV Mosby, 1940. 23. Muse DS, Fillman MJ, Emmerson WJ, Mitchell RD. Molar and incisor changes with
Wilson rapid molar distalization. Am J Orthod Dentofac Orthop 1993;104:556-65. 24. Hilgers JJ. A palatal expansion appliance for non-compliance therapy. J Clin Orthod
1991;25:491-7. 25, Hilgers JJ. The pendulum appliance for Class 1I non-compliance therapy, J Clin Orthod
1992;26:706-14. 26. Enlow DH, Kuroda T, Lewis AB. The morphological and morphogenetic basis for
craniofacial form and panern. Angle Orthod 1971;41:1fil-88.