evaluation of intraoperative bleeding during an endoscopic surgery of nasal polyposis after a...
TRANSCRIPT

RHINOLOGY
Evaluation of intraoperative bleeding during an endoscopicsurgery of nasal polyposis after a pre-operative single doseversus a 5-day course of corticosteroid
Saeid Atighechi • Mohammad Reza Azimi • Seyyed Abbas Mirvakili •
Mohammad Hossein Baradaranfar • Mohammad Hossein Dadgarnia
Received: 22 June 2012 / Accepted: 18 December 2012
� Springer-Verlag Berlin Heidelberg 2013
Abstract Nasal polyps are associated with the inflammation
of the nasal cavity and the sinus mucosa. When medical
treatment cannot solve a patient’s problem, a functional
endoscopic sinus surgery may be indicated. Bleeding impairs
the surgery field during operation and increases the operation
risk and time. Pre-operative corticosteroids can reduce
bleeding during surgery. In this study, we have evaluated the
effect of pre-operative single-dose prednisolone (1 mg/Kg/
dose 24 h before surgery) versus 5-day prednisolone (1 mg/
Kg/day before operation) on the bleeding volume and the
surgery field quality during FESS. In this mono blind ran-
domized clinical trial, 80 patients with bilateral nasal polyps
were randomly assigned in two groups. The first group
(A) received a single dose of 1 mg/Kg/dose prednisolone on
the day before the surgery. The second group (B) received
1 mg/Kg/day prednisolone for 5 days before the operation.
The patients were operated on under general anesthesia
through the same protocol. The mean arterial blood pressure
was 70–80 mm Hg in both groups. The surgeons were not
aware of the patients’ group. The bleeding volume and the
surgeons’ opinion about the surgery field quality were recor-
ded at the end of the procedure and analyzed by Chi-square
and t test. The two groups were not significantly different in
their overall demographic and clinical characteristics. The
mean bleeding volume during the operation was
266.5 ± 96.31 ml in group A and 206 ± 52.81 ml in group
B; there was a significant difference between the groups
(P value = 0.038). There was no significant difference
between the groups in the surgeons’ opinion about the surgery
field quality (P value = 0.09). In conclusion, unlike a single
dose (1 mg/kg/dose), treatment with 5-day prednisolone
(1 mg/kg/day) can reduce blood loss during FESS more
efficiently and may improve the surgery field quality slightly.
But this difference is not clinically significant.
Keywords Nasal polyps � Prednisolone � Endoscopic
sinus surgery � Bleeding � Complication � Corticosteroids
Introduction
Rhinosinusitis is an inflammatory process in nose and
paranasal sinuses characterized by at least two of these:
clinical presentation, endoscopic finding, and CT scan
changes [1]. Many patients may be asymptomatic, but large
polyps may lead to a nasal passage block and become
symptomatic. The most common symptoms are hyposmia,
rhinorrhea, posterior nasal discharge, etc [2]. There is a
correlation between nasal polyps and allergy. 68.5 % of
patients with nasal polyps had a positive allergy skin test
although allergy may not be responsible for the rhinosi-
nusitis [3]. Medical therapy for nasal polyps is the main
stage of treatment. It consists of a course of antibiotics with
an effective bacterial coverage and topical steroids [4].
Long-term topical steroids with a reduction in the polyp
size can remove patients’ symptom. Short-term systemic
steroids may be used in more severe cases [5]. When
medical treatment cannot solve the patients’ problem,
surgery may be indicated. The best approach for chronic
rhino sinusitis with nasal polyps is a functional endoscopic
sinus surgery [6]. One of the most common complications
S. Atighechi � M. R. Azimi � S. A. Mirvakili �M. H. Baradaranfar � M. H. Dadgarnia
Department of Otolaryngology, Shahid Sadooghi
University of Medical Sciences, Yazd, Iran
S. Atighechi (&)
Department of Otolaryngology, Shahid Sadooghi Hospital,
Sina Street, Janbaz Square, Yazd, Iran
e-mail: [email protected]
123
Eur Arch Otorhinolaryngol
DOI 10.1007/s00405-012-2340-9

during FESS is bleeding [7]. Bleeding impairs the surgery
field during the operation and increase the risk of compli-
cations like those in the skull base or orbital damages.
Bleeding increases operation time due to multiple stops
during surgery for suctioning and packing [7]. One of the
strategies to reduce bleeding during an operation is the use
of pre-operative corticosteroid, which makes a reduction in
the polyp size and mucosal inflammation [4].
In this study, we tried to answer the question: ‘‘can a pre-
operative regimen of prednisolone be reduced to a single
day before the procedure?’’ A single dose may be better
complied with than a five-course one, and perhaps better
tolerated. So, we evaluated the effect of pre-operative sin-
gle-dose prednisolone (1 mg/Kg/dose 24 h before surgery)
versus a 5-day prednisolone protocol (1 mg/Kg/day before
surgery) on the bleeding volume and the surgery field
quality during FESS.
Method and materials
A total of 80 patients with bilateral nasal polyps were the
candidates for our mono blind randomized clinical trial. All
the patients were in a good health condition (ASA class I) and
aged between 18 and 50 (the inclusion criterion was age
between 18 and 50). They were randomly assigned in two
groups according to the table of random numbers. The first
group (group A) received a single dose of 1 mg/Kg/dose
prednisolone on the day before the surgery. The second
group (group B) received 1 mg/Kg/day prednisolone for
5 days before the operation. The exclusion criteria were
history of previous nasal surgery, antrochoanal polyps,
hemorrhagic disease, hypertension (SBP [ 140 mm Hg or
DBP [ 90 mm Hg), corticosteroid use in 2 months before
screening, and allergy or other contraindications for corti-
costeroid use. Written consents were taken from the patients.
The baseline assessment included the collecting of the
patients’ medical and surgical history and nasal examination.
The size of the nasal polyps was recorded in a diagnostic
endoscopic examination, and the sinus involvement was
determined by CT-scan images according to Lund–Mackay
score. Treatment complications such as high blood glucose
levels, euphoria, stomach irritation, and sleeplessness were
recorded too. The study was approved by the ethics com-
mittee of Shahid Sadoughi Hospital, Yazd, Iran.
The patients were operated on under general anesthesia
by the same protocol (Table 1). The mean arterial blood
pressure was 70–80 mm Hg in both groups during the
surgery. All the surgeons used topical vasoconstriction
(1/10,000 epinephrine solution) and used a 2-ml local
injection of 1/100,000 epinephrine solution in the middle
and inferior turbinate and to the attachment of the middle
turbinate to the lateral nasal wall. The surgeons were not
aware of the patients’ group. The bleeding volume was
precisely assessed according to the volume in the suction
jar (total volume minus irrigation volume) and the excess
weight of the pharyngeal pack. The surgeons’ opinion
about the surgery field quality was recorded according to
0–10 score (Table 2) at the end of the procedure.
A sample t test and Chi-square test were used to com-
pare the baseline and the outcome values. Differences
would prove to be statistically significant if P value was
less than 0.05. All the statistical analyses were performed
with an SPSS software version 11.5 for windows.
Results
80 patients who had the inclusion criteria were randomly
assigned in two equal groups. The overall demographic as
well as the clinical characteristics was not statistically
different in the two groups at the baseline (Table 3). The
prevalence of concomitant asthma in two groups was also
mentioned in Table 3, but the difference was not
significant.
The mean bleeding volume during the operation was
266.5 ± 96.31 ml in group A and 206 ± 52.81 ml in
group B. In this regard, there was a significant difference
between the groups (P value = 0.038).
Table 1 Anesthesia protocol
Premedication Midazolam 1 mg IV ? fentanyl 2.5
micro g/kg IV ? clonidine 1 tablet
Induction Propofol 1.5–2 mg/kg ? atracurium
0.5 mg/kg
Maintenance Propofol 5–10 mg/kg/h ? atracurium
0.5 mg/kg itch 30 min ? N2O 50 %
If
MAP [ 80 mm Hg
TNG drip 0.25-0.5 micro g/kg/min till
MAP \ 80 mm Hg
Table 2 Quality of surgical field during functional endoscopic sinus
surgery
Score Quality of intraoperative surgical field during functional
endoscopic sinus surgery
0–1 No bleeding; excellent to outstanding surgical conditions
2–3 Slight bleeding. Surgery fairly easy. No stop for hemostasis
and/or suctioning is required
4–5 Slight bleeding. Surgery mildly difficult. One stop for
hemostasis and/or suctioning is required
6–7 Moderate bleeding. Surgery Moderately difficult. Occasional
stops for hemostasis and/or suctioning are required
8–9 Moderate to severe bleeding. Surgery very difficult. Multiple
stops for hemostasis and/or suctioning are required.
10 Surgery terminated due to severe bleeding in surgical field
Eur Arch Otorhinolaryngol
123
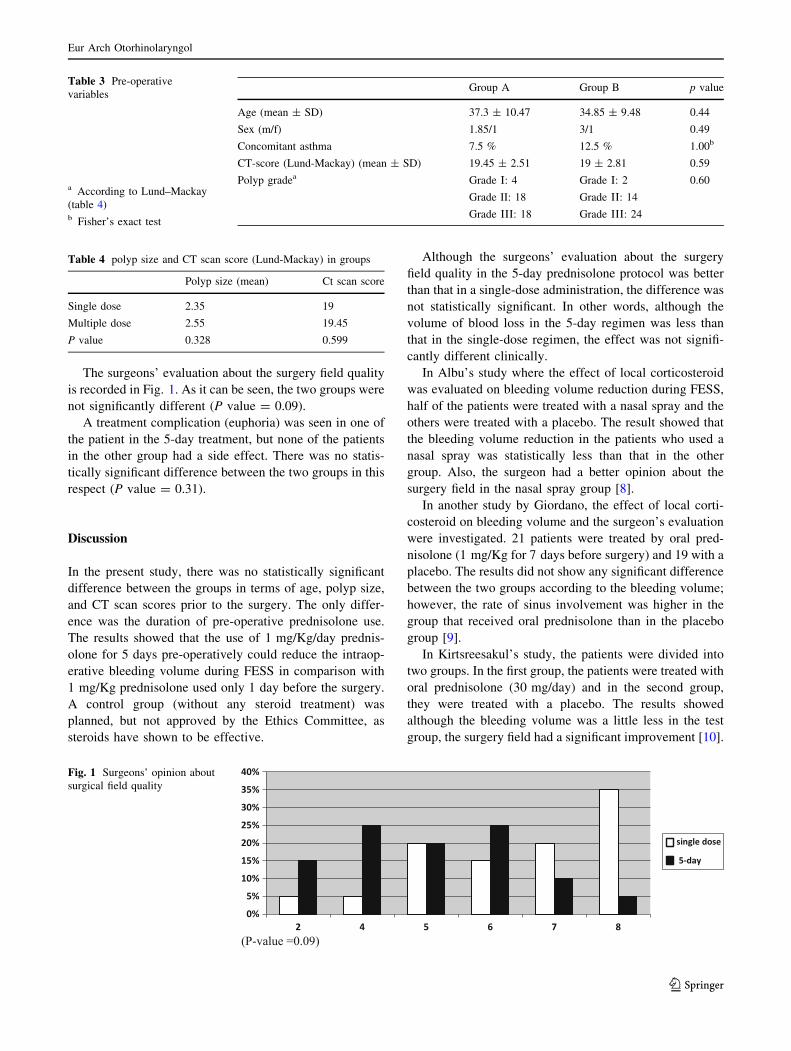
The surgeons’ evaluation about the surgery field quality
is recorded in Fig. 1. As it can be seen, the two groups were
not significantly different (P value = 0.09).
A treatment complication (euphoria) was seen in one of
the patient in the 5-day treatment, but none of the patients
in the other group had a side effect. There was no statis-
tically significant difference between the two groups in this
respect (P value = 0.31).
Discussion
In the present study, there was no statistically significant
difference between the groups in terms of age, polyp size,
and CT scan scores prior to the surgery. The only differ-
ence was the duration of pre-operative prednisolone use.
The results showed that the use of 1 mg/Kg/day prednis-
olone for 5 days pre-operatively could reduce the intraop-
erative bleeding volume during FESS in comparison with
1 mg/Kg prednisolone used only 1 day before the surgery.
A control group (without any steroid treatment) was
planned, but not approved by the Ethics Committee, as
steroids have shown to be effective.
Although the surgeons’ evaluation about the surgery
field quality in the 5-day prednisolone protocol was better
than that in a single-dose administration, the difference was
not statistically significant. In other words, although the
volume of blood loss in the 5-day regimen was less than
that in the single-dose regimen, the effect was not signifi-
cantly different clinically.
In Albu’s study where the effect of local corticosteroid
was evaluated on bleeding volume reduction during FESS,
half of the patients were treated with a nasal spray and the
others were treated with a placebo. The result showed that
the bleeding volume reduction in the patients who used a
nasal spray was statistically less than that in the other
group. Also, the surgeon had a better opinion about the
surgery field in the nasal spray group [8].
In another study by Giordano, the effect of local corti-
costeroid on bleeding volume and the surgeon’s evaluation
were investigated. 21 patients were treated by oral pred-
nisolone (1 mg/Kg for 7 days before surgery) and 19 with a
placebo. The results did not show any significant difference
between the two groups according to the bleeding volume;
however, the rate of sinus involvement was higher in the
group that received oral prednisolone than in the placebo
group [9].
In Kirtsreesakul’s study, the patients were divided into
two groups. In the first group, the patients were treated with
oral prednisolone (30 mg/day) and in the second group,
they were treated with a placebo. The results showed
although the bleeding volume was a little less in the test
group, the surgery field had a significant improvement [10].
Fig. 1 Surgeons’ opinion about
surgical field quality
Table 3 Pre-operative
variables
a According to Lund–Mackay
(table 4)b Fisher’s exact test
Group A Group B p value
Age (mean ± SD) 37.3 ± 10.47 34.85 ± 9.48 0.44
Sex (m/f) 1.85/1 3/1 0.49
Concomitant asthma 7.5 % 12.5 % 1.00b
CT-score (Lund-Mackay) (mean ± SD) 19.45 ± 2.51 19 ± 2.81 0.59
Polyp gradea Grade I: 4 Grade I: 2 0.60
Grade II: 18 Grade II: 14
Grade III: 18 Grade III: 24
Table 4 polyp size and CT scan score (Lund-Mackay) in groups
Polyp size (mean) Ct scan score
Single dose 2.35 19
Multiple dose 2.55 19.45
P value 0.328 0.599
Eur Arch Otorhinolaryngol
123

An aim of the present study was to evaluate the side
effects of short-term use of corticosteroid. The results
showed that the side effects were less in the single-dose
group, but the difference was not statistically significant
(P value = 0.31).
In a study, Bolanos showed that short-term corticoste-
roid use was safe and side effects such as sleep disorders,
weight gain, euphoria, and gastrointestinal disorders were
seen rarely according to a meta-analysis done in 2005.
Severe side effects were seen in 6 % of the patients while
mild–moderate side effects were seen in 28 % of the
patients. The most common side effects in short-term
corticosteroid use were hypomania and euphoria. It was
due to hypocamp neurons disequilibrium [11].
In the Sieskiewicz study, bleeding and surgeon evalua-
tion was compared in 18 patients on 30 mg of oral pred-
nisone daily for 5 consecutive days before the operation
with control group. Although total blood loss was reduced
slightly in steroid group, but surgical field improved sig-
nificantly as a result of the anti-edematous and anti-
inflammatory activity of steroid, which provided a better
vision for the surgeon [12].
Conclusion
Treatment with 5-day prednisolone (1 mg/kg/day) as
compared to single-dose prednisolone (1 mg/kg/dose) can
reduce blood loss during FESS more efficiently, but may
not improve surgery field quality significantly. So, in case
of time restriction, a single dose of prednisolone before
operation may be useful for the reduction of bleeding
volume and the improvement of surgeon’s opinion. Also, it
has no side effect or complication.
References
1. Fokkens WJ, Lund VJ, Mullol J et al (2012) European position
paper on rhinosinusitis and nasal polyps 2012. Rhinol Suppl 23:3
(preceding table of contents, 1-298)
2. Damm M, Quante G, Jungehuelsing M et al (2002) Impact of
functional endoscopic sinus surgery on symptoms and quality of
life in chronic rhinosinusitis. Laryngoscope 112(2):310–315
3. Kirtsreesakul V (2004) Nasal polyps: the relationship to allergy,
sinonasal infection and histopathological type. J Med Assoc Thai
87(3):277–282
4. Aukema AA, Mulder PG, Fokkens WJ (2005) Treatment of nasal
polyposis and chronic rhinosinusitis with fluticasone propionate
nasal drops reduces need for sinus surgery. J Allergy Clin
Immunol 115(5):1017–1023
5. Mullol J, Obando A, Pujols L et al (2009) Corticosteroid treat-
ment in chronic rhinosinusitis: the possibilities and the limits.
Immunol Allergy Clin North Am 29(4):657–668
6. Dykewicz MS, Hamilos DL (2010) Rhinitis and sinusitis.
J Allergy Clin Immunol 125(2 Supplement 2):s103–s115
7. Lal D, Stankiewicz JA (2012) Primary sinus surgery. In: Flint
PW, Haughey BH, Lund VJ et al (eds) Cummings otolaryngol-
ogy, head and neck surgery. Mosby Elsevier, Philadelphia, p 743
8. Albu S, Gocea A, Mitre I (2010) Preoperative treatment with
topical corticoids and bleeding during primary endoscopic sinus
surgery. Otolaryngol Head Neck Surg 143(4):573–8
9. Giordano J, Darras J, Chevalier D et al (2009) Preoperative
corticosteroid treatment and nasal polyposis. Ann Otolaryngol
Chir Cervicofac 126(3):120–124
10. Kirtsreesakul V, Wongsritrang K, Ruttanaphol S (2011) Clinical
efficacy of a short course of systemic steroids in nasal polyposis.
Rhinology 49(5):525–532
11. Bolanos SH, Khan DA, Hanczyc M (2004) Assessment of mood
states in patients receiving long-term corticosteroid therapy and
in controls with patient-rated and clinician-rated scales. Ann
Allergy Asthma Immunol 92:500–505
12. Sieskiewicz A, Olszewska E, Rogowski M et al (2006) Preop-
erative corticosteroid oral therapy and intraoperative bleeding
during functional endoscopic sinus surgery in patients with severe
nasal polyposis: a preliminary investigation. Ann Otol Rhinol
Laryngol 115(7):490–494
Eur Arch Otorhinolaryngol
123