evaluation of undescended testes
TRANSCRIPT
UNDESCENDED TESTES
7th Year Surgery Tutorial28th June 2016Dr. PASHI V.
CONTENTS
Introduction EmbryologyRelevant anatomyClinical presentationManagement Complications
Introduction UDT also known as cryptorchismFailure of the testis to descend normally from the abdominal cavity into the scrotumUDT is associated with a variety of potential consequences:Malignancy, infertility, torsion of testis, and inguinal hernia.Treatment of UDT is aimed at minimising these risks.
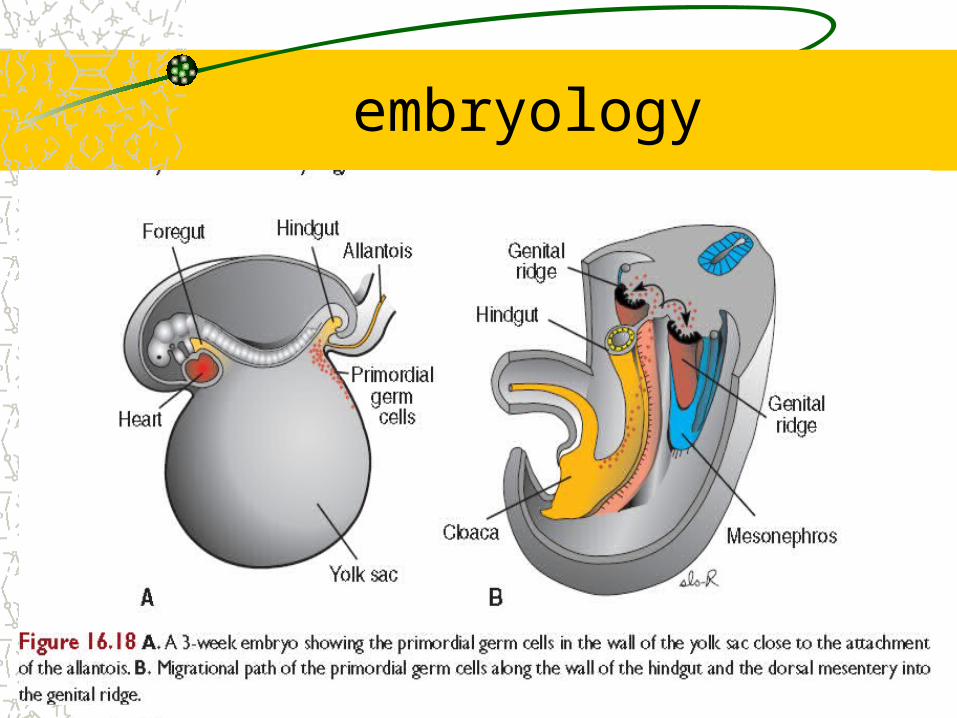
EMBRYOLOGYNORMAL DESCENT OF TESTES
Germ cells migrate from yolk sac to genital ridges at 6 weeks
The gonads acquire male or female morphological in the 7th week of development
By the 8th week of gestation, Leydig cells begin production of testosterone and sexual differentiation begins
embryology
embryology
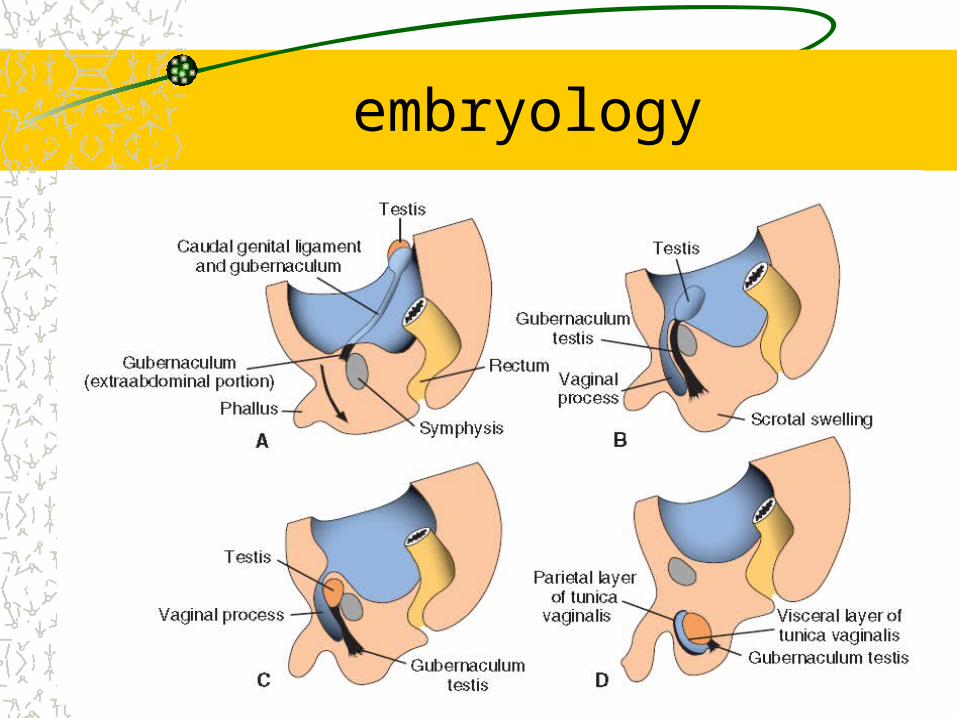
DESCENT OF TESTES By the end of 8th week the testes have acquired two
attachments The caudal genital ligament and the gubernaculum Descent is believe to be achieved by:
Abdominal descent by the out growth of the extra abdominal gubernaculum
Inguinal descent by the raising intra abdominal pressure Regression of the extra abdominal gubernaculum facilitates
descent to the scrotum
embryologyFEATURES OF TESTICULAR DESCENCE
The testes will reach the internal ring by 12 weeks, pass through the inguinal canal by 28 weeks and finally in the scrotum by 33 weeks
Endocrine factors probably play a major role in descent– Testosterone induces testis descent in humans– Androgens affect the nuclei of the genitofemoral
nerve to release modulating factors for gubernacular development
embryology
FEATURES OF TESTICULAR DESCENCE Blood supply from the aorta is maintained with testicular
arteries arising from the lumber region The testes emerge from the abdominal cavity carrying
with it the abdominal coverings and peritoneum Peritoneum makes the processus vaginalis Canal portion of processus obliterates, testicular portion
persists as tunica vaginalis Gubernaculum atrophies
embryology
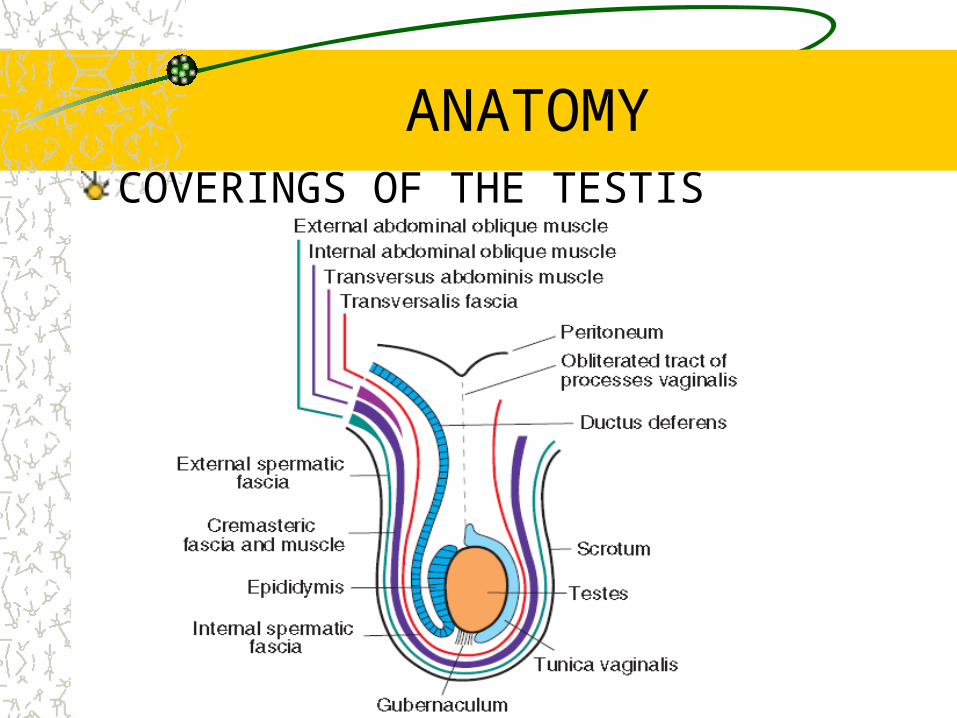
ANATOMYCOVERINGS OF THE TESTIS
CLINICAL PRESENTATION
UDT occurs in 3% of term male infants and in up to 33% of premature male infants.A true UDT has had its descent halted somewhere along the path of normal descent. The ectopic UDT has deviated from the path of normal descent and can be found in the inguinal region, perineum, femoral canal, penopubic area, or even the contralateral hemiscrotum.
Clinical presentationA retractile testis is a normally descended testis that retracts into the inguinal canal as a result of cremaster muscle contraction.
It can be manipulated down into the scrotum on examination without tension and will remain in placeAcquired UDT refers to a testis that was previously descended on examination and can no longer be brought down into the scrotum.
Clinical presentation
Palpable–Normal–Retractile–Ectopic–Undescended
Impalpable–Canalicular– Intra-abdominal–Emergent–Absent
• Agenesis• atrophy
Whitaker/Kaplan Classification for UDT
Clinical presentationMost common dilemma is distinguishing retractile testis from one that may or may not descend spontaneouslyManeuvers used: 1. examine boy in crosslegged position,
2. soaping the examiner’s fingers 3. examining in a warm bath
Physical exam is very important to evaluate retractile testes –Non-palpable testis is intraabdominal, intracanalicular,
absent
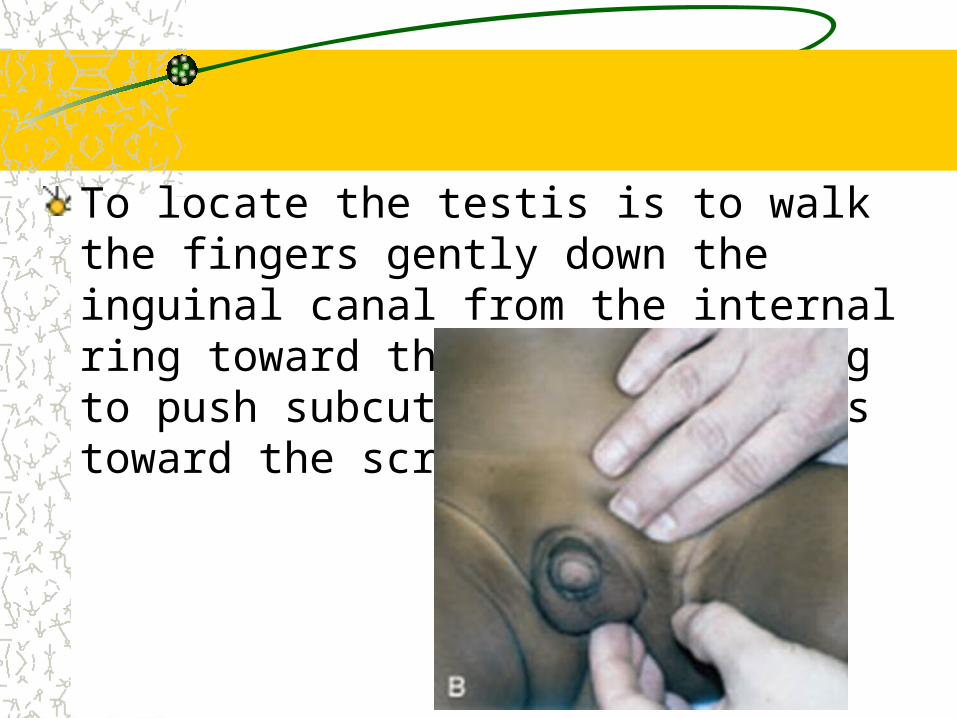
To locate the testis is to walk the fingers gently down the inguinal canal from the internal ring toward the scrotum, trying to push subcutaneous structures toward the scrotum.
Bilateral UDT requires hormonal evaluation and challenge–Elevated gonadotropins (FSH) suggest
bilateral anorchia–Normal serum gonadotropins=>hCG
challenge (2000 IU x 3days)–No testosterone response indicates bilateral
anorchia
Imaging Herniography-poor sensitivity and specificityU/S-good for inguinal testes, not reliable if higherCT-may be helpful for bilateral impalpable testes– Difficult to perform in young children
MRI-least invasive, most expensive– Difficult to perform in young children
Imaging Venography-invasive, pampiniform plexus present=>testis present– Non-visualized plexus or blindending does not
eliminate testisAngiography-difficult to perform, high complicationsOverall accuracy of radiologic imaging for UDT = 44%– PE is 53% - 84%
Hormonal Treatment
hCG is given to stimulate Leydig cells to produce testosterone=>descent of testesGnRH is given if basal LH is low and abnormality in GnRH secretion is suspected
Surgical TreatmentBasic principles of orchidopexy are: localization, mobilization, cord dissection, isolation of processus, tension-free relocation to scrotumPexation does not reduce risk of cancerOrchidopexy should be performed before 2 y.o.Orchidectomy is an option for post-pubertal males and dysgenetic testes
Standard OrchidopexyTransverse inguinal incision, watch for testisIdentify testis and divide gubernaculumOpen tunics and evaluate testisOpen external oblique fascia, avoid nerveMobilize spermatic cordFinger dissection to enlarge scrotal cavity mediallyIncise scrotal skin, create dartos pouch
Standard Orchidopexy contn
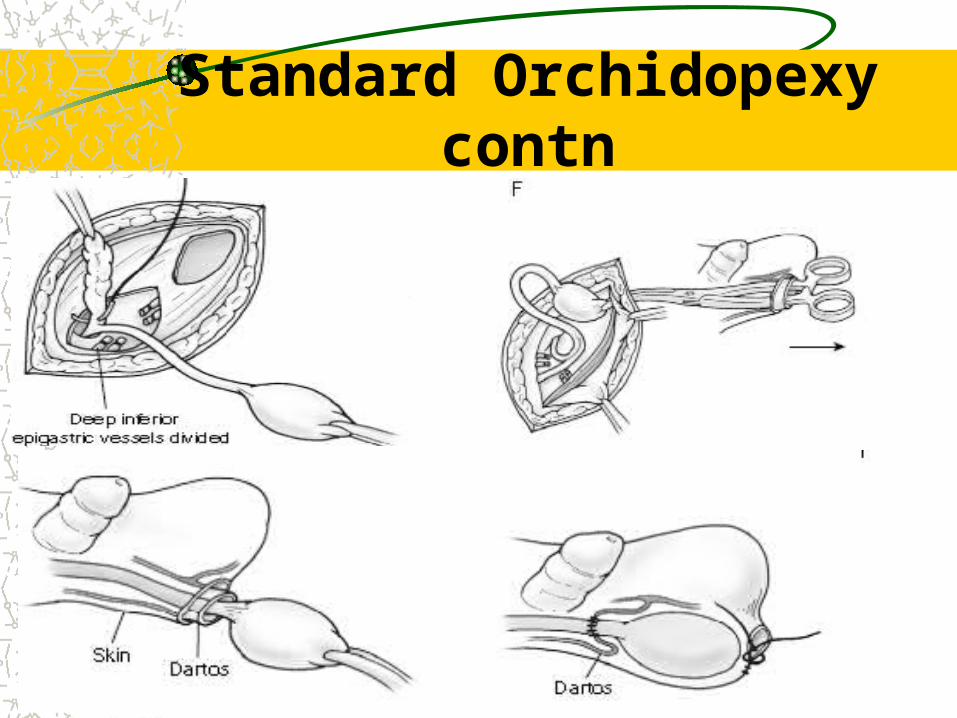
Pass clamp through pouch into inguinal area and bring testis into pouch by gubernaculum or tunicaPex testis with 4-0 vicryl suturesComplications: atrophy, retraction, torsion, hematoma, nerve or vas injury
Standard Orchidopexy contn
Complications Neoplasm and UDT– 10% of testis CA are in UDT– UDT is 35-48x more likely to have malignancy– Abdominal UDT is 4x more likely than inguinal testis to develop
CA– UDT tumors typically occur around puberty– CIS occurs in 1.7% of UTD– Orchiopexy should be performed between 1-1.5 years old– 1/5 of testis CA in patients w/ hx of UDT occurs in contralateral
testis– Seminoma is most common CA in UDT
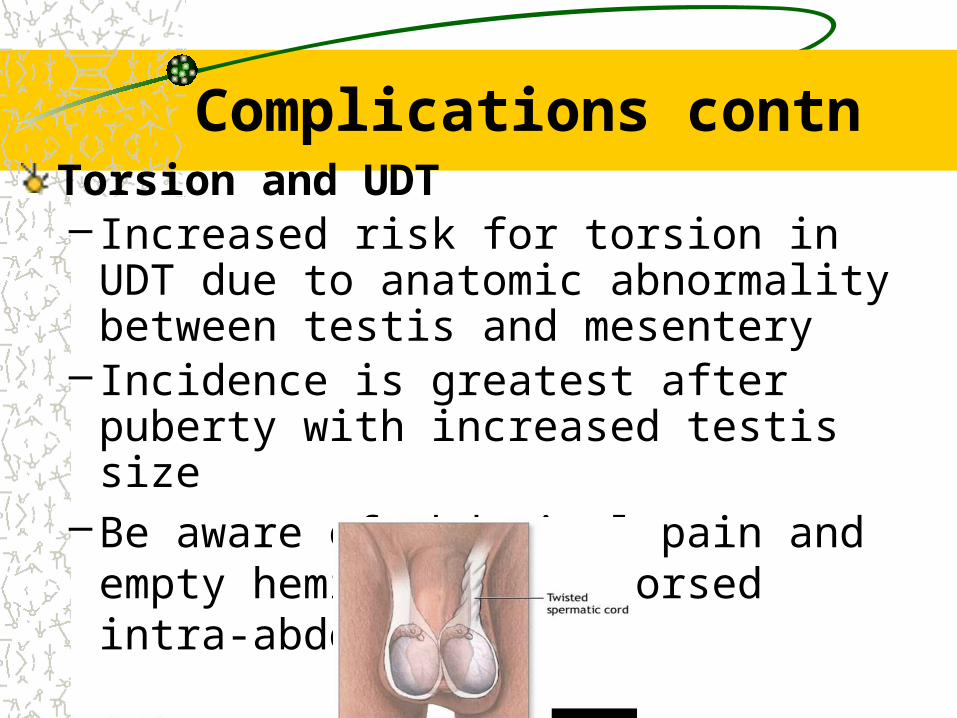
Complications contnTorsion and UDT– Increased risk for torsion in UDT due to anatomic
abnormality between testis and mesentery– Incidence is greatest after puberty with increased
testis size–Be aware of abdominal pain and empty
hemiscrotum=> torsed intra-abdominal UDT
Complications contnHernia and UDTProcessus vaginalis should obliterate between the 8th month of gestation and 1st month of lifeUDT results in patent processus vaginalisHernias are found in 90% of patients w/ UDT
Complications contnInfertility and UDTSpermatogenesis is retarded by maldescentBilateral UDT => poor fertilityHigher UDT => more damage to seminiferous tubulesEarlier orchidopexy may improve chances for recovery of spermatogenesisSperm counts in unilateral UDT are much lower than normal – Contralateral testis may also be defective
Futher reading
Fowler-stephens orchidopexyLaparoscopic orchidopexy