evaluation of wrist trauma
TRANSCRIPT

Evaluation of Wrist Trauma
Collin May, MS IVDr. Gillian Lieberman
Beth Israel Deaconess Medical CenterHarvard Medical School
November 12, 2007

The wrist is complex…
• Zone of wrist defined as:3cm proximal to radiocarpal joint carpometacarpal joints
http://www.caringmedical.com/conditions/Wrist_Pain.htm
• In this small space, there are 15 bones, 27 articular surfaces and a “sea of ligaments”

Complexity has a price…
http://www.hughston.com/hha/b_14_1_2b.jpg
The wrist is the most commonly injured region of the upper extremity
http://www.stavros.messinis.com/
Fracture of distal radius and ulna account for 75% of wrist injuries
Fracture of carpal bones account for about 15% of wrist injuries

Epidemiology• Three groups affected:
– Children: 5-14– Males < age 50– Females > age 40
The incidence of wrist fractures per 10 000 population per annum related to age and gender.
THE JOURNAL OF BONE AND JOINT SURGERYEpidemiology of fractures in 15 000 adultsTHE INFLUENCE OF AGE AND GENDERB. R. Singer, G. J. McLauchlan, C. M. Robinson, J. Christie
• Fxs in the younger populations typically 2/2 sports and motor vehicle crashes
• Fxs in older females represent osteoporotic fractures usually 2/2 simple fall
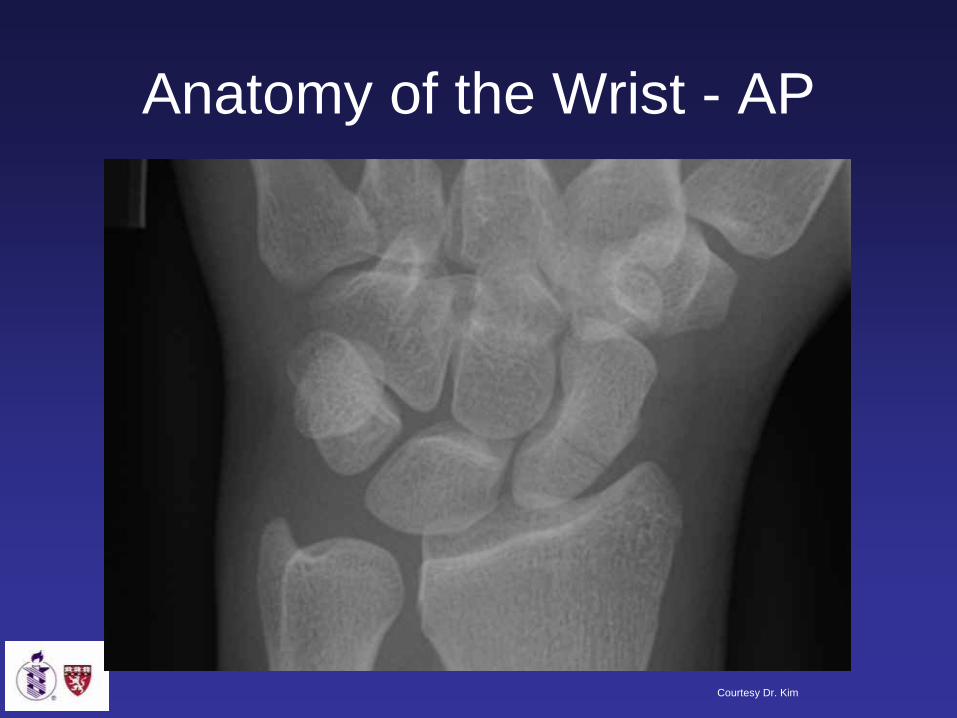
Anatomy of the Wrist - AP
Courtesy Dr. Kim
Courtesy Dr. Kim
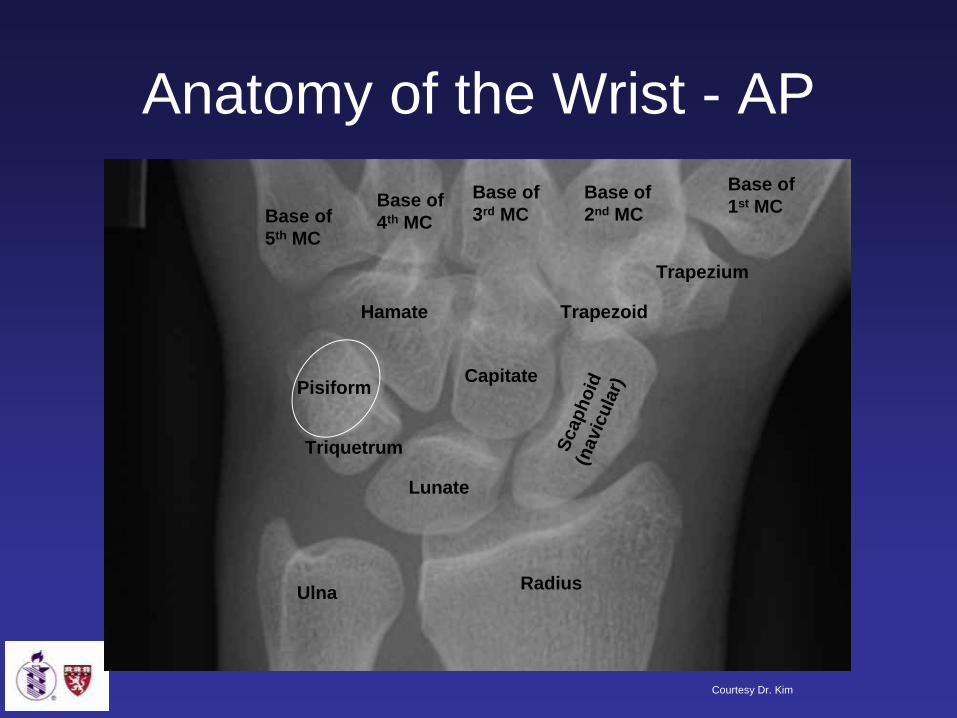
Scap
hoid
(nav
icul
ar)
Lunate
Triquetrum
Pisiform Capitate
Hamate
Trapezium
Trapezoid
Base of 5th MC
Base of 4th MC
Base of 3rd MC
Base of 2nd MC
Base of 1st MC
Ulna Radius
Anatomy of the Wrist - AP

Lateral
http://www.rad.washington.edu/radanat/WristLat.html
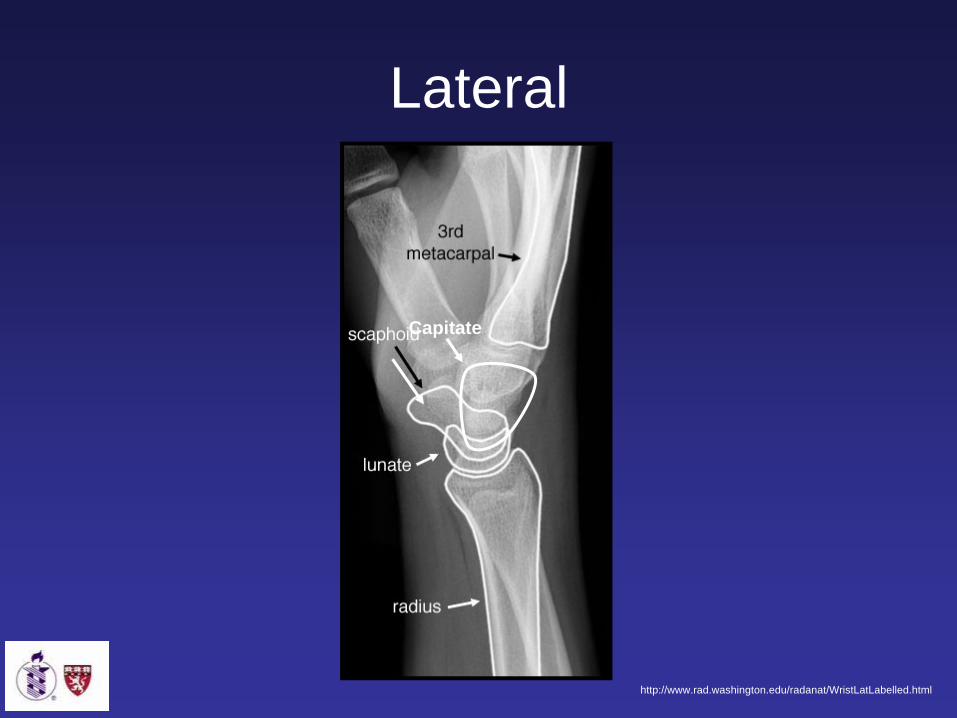
Capitate
http://www.rad.washington.edu/radanat/WristLatLabelled.html
Lateral

The differential for a patient presenting with traumatic wrist pain is broad…
• Distal Radius Fracture – Colles, Smith’s, Barton’s
• Radial Styloid/Ulnar Styloid Fracture
• Scaphoid (navicular) Fracture
• Simple sprain (radiocarpal joint)
• Scapholunate Instability• Perilunate dislocation• Hamate Fracture• TFCC tear
• Lunate dislocation or fracture
• Rupture of Flexor Carpi Radialis tendon
• Trapezium fracture• Extensor Carpi Radialis
Brevis Avulsion• Extensor Carpi Radialis
Longus Avulsion• CMC arthrosis• Cartilage tears• Kienbock’s Disease
Mechanism is typically fall onto outstretched hand
www.nytimes.com

Axial compressive force applied with the wrist in hyperextension
Increasing Force
Rockwood and Green’s Fractures in Adults, 6th edition. 2006. pp 857-908

We will focus on only a few types of wrist injury:
• Distal Radius Fracture – Colles, Smith’s, Barton’s
• Radial Styloid/Ulnar Styloid Fracture
• Scaphoid (navicular) Fracture
• Simple sprain (radiocarpal joint)
• Scapholunate Instability• Hamate Fracture• TFCC tear• Trapezium fracture
• Rupture of Flexor Carpi Radialis tendon
• Carpal Dislocation• Lunate dislocation or
fracture• Extensor Carpi Radialis
Brevis Avulsion• Extensor Carpi Radialis
Longus Avulsion• CMC arthrosis• Cartilage tears• Kienbock’s Disease

Menu of Tests• Xray – Wrist Series
– Standard: AP, Lateral and Oblique– Scaphoid views, usually multiple
• MRI: if clinical suspicion for fracture or ligamentous injury but with negative radiographs
• Special Circumstances:– CT– Bone Scan– Arthrography– Fluoroscopy

Scaphoid Fracture

The Scaphoid is the most frequently fractured carpal bone (71% of all carpal fractures)
• Typically occurs in young-middle aged men due to falls, athletic injuries, or MVA – requires considerable force
http://www.e-radiography.net/radpath/f/scaphoid%20fracture/scaphoid_injuries.gif
• About 345,000 scaphoid fractures/year in US
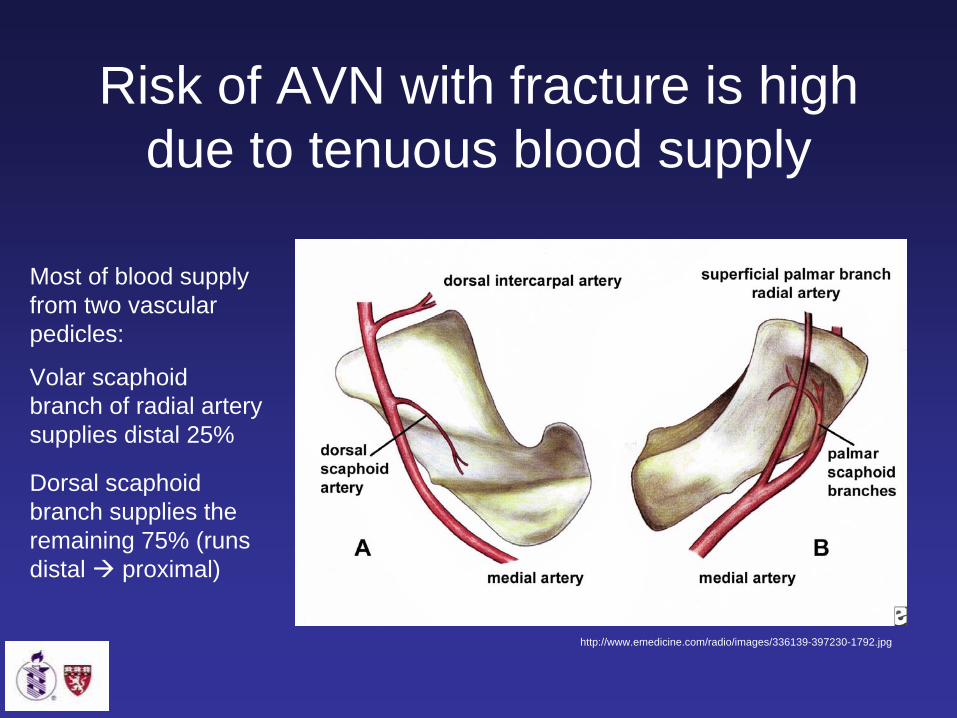
Risk of AVN with fracture is high due to tenuous blood supply
http://www.emedicine.com/radio/images/336139-397230-1792.jpg
Most of blood supply from two vascular pedicles:
Volar scaphoid branch of radial artery supplies distal 25%
Dorsal scaphoid branch supplies the remaining 75% (runs distal proximal)

Clinical• History
– Typically a history of fall on outstretched hand (FOOSH)
• Physical exam– Most consistent sign of carpal injury is well-localized
tenderness– Gross deformity may be present– Provocative tests reproduce or exacerbate pain– Snuffbox tenderness (sens, and spec)– Watson test– Compression Test

Provocative Tests…• Snuffbox Tenderness
– Localized tenderness/swelling present with acute fracture
– Pronation/Ulnar dev increases specificity
– Sens: 90%, Spec: 40%
http://www.fpnotebook.com/ORT145.htm
http://www.aafp.org/afp/20051101/1753.html
• Shift Test (Watson)– Palpate scaphoid tubercle while
wrist moved from ulnar to radial deviation
– Sens: 86%, Spec: 57%
• Compression Test– Axially compress along thumb

Imaging of the ScaphoidAcute presentation
Radiographs: AP, Lat, Oblique, Scaphoid View
Suspect Fx, radiograph Nml Radiograph positive for fx
1. Cast Wrist, repeat xray in 10-14 days
2. MRI w/o contrast
Treat according to severity of fx
D/c with instructions to f/u if sx develop
Xray neg, low clinical suspicion

MRI in acute scaphoid fractureTraditional follow-up for occult fractures: cast and re-image with radiographs in 10-14 daysConcluded MRI cost-effective, and avoided 2 weeks of immobilization if negative
Dorsay TA, et al

Imaging of the Scaphoid Modalities for special situations
• CT Scan:– Scaphoid fx on radiograph, concern for displacement or age of fx CT w/o
contrast– Comminuted Distal radius fx, concern for joint involvement – Suspicion for Hook of hamate fracture
• MRI (other indications):– Chronic wrist pain with nondiagnostic xrays– Chronic wrist pain, suspect ligamentous injury
• Bone scan– Can be used in workup of occult fractures
• Wrist Arthrography– Can be used in suspected TFCC and intercarpal ligament tears
• Fluoroscopy– Helpful in diagnosing dynamic wrist instability

The X-ray is negative but the patient is in pain…what to do?
• Up to 30% of all scaphoid fractures not detected on initial radiographs
• Traditionally, with suspicion for occult fracture, patient is immobilized in a Colles cast for 10 – 14 days, then returns for further radiographs at that time
• Not good consensus about whether MRI is warranted in this setting, or if the traditional approach is still method of choice
• Alternatively, other imaging modalities can also be used…
http://www.medscape.com/content/1999/00/40/84/408495/art-mos4356.fig16.jpg
http://www.hss.edu/conditions_14476.asphttp://www.med.harvard.edu/JPNM/BoneTF/Case1/BoneScan.GIF

Our Patient: S/p Fall Onto Outstretched Hand
AP/Oblique radiographs of wrist
Courtesy of Dr. Kim

Courtesy of Dr. Kim
Scaphoid Fracture

Companion Patient 1: Scaphoid Waist Fracture
Courtesy of Dr. Shetty

Companion Patient 2: Proximal Pole Scaphoid Fracture
Courtesy of Dr. Shetty

Companion Patient 3: Scaphoid Tuberosity Fracture
Courtesy of Dr. Shetty

Scaphoid Views• AP xray with wrist supinated 30 degrees
and in ulnar deviation
Courtesy of Dr. Shetty

Treatment• Undisplaced, Stable Acute
Fractures:– Conservative management is
the norm: immobilization in thumb spica cast for 10-12 weeks, with frequent radiographic followup
• Displaced and Unstable Fractures:– Percutaneous screw fixation or
ORIF
Haisman, et al.
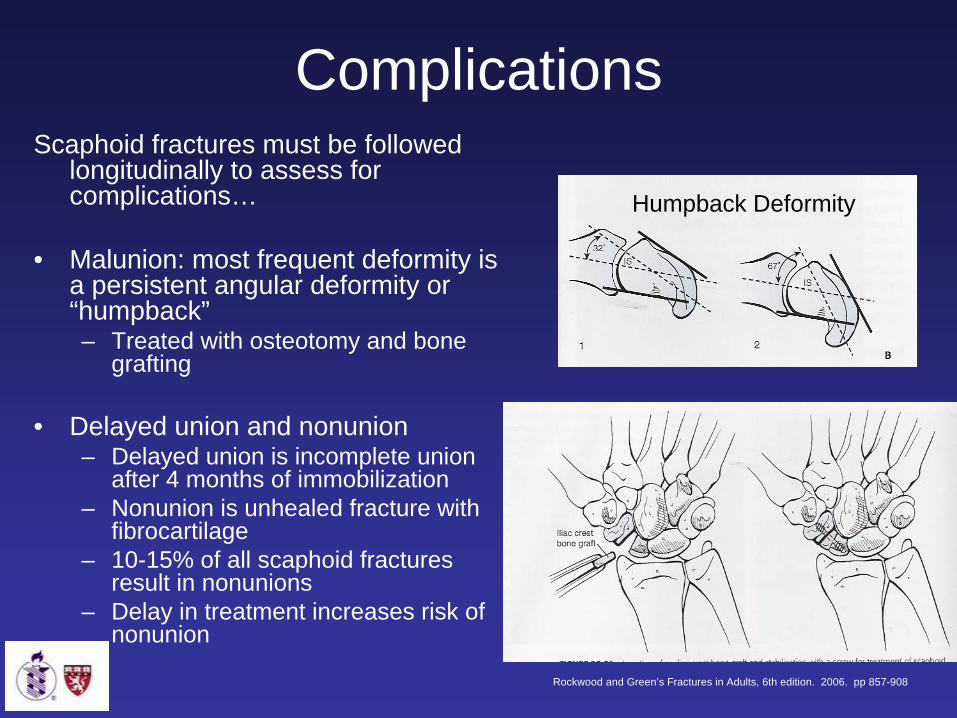
ComplicationsScaphoid fractures must be followed
longitudinally to assess for complications…
• Malunion: most frequent deformity is a persistent angular deformity or “humpback”– Treated with osteotomy and bone
grafting
• Delayed union and nonunion– Delayed union is incomplete union
after 4 months of immobilization– Nonunion is unhealed fracture with
fibrocartilage– 10-15% of all scaphoid fractures
result in nonunions– Delay in treatment increases risk of
nonunion
Humpback Deformity
Rockwood and Green’s Fractures in Adults, 6th edition. 2006. pp 857-908

Radiographic Findings of Nonunion
• Sclerosis at the fracture site• Persistent lucent line (usually >
2mm)• Cystic cavitation• Displacement of > 1mm• Local tenderness• +/- AVN of proximal pole
http://www.wheelessonline.com/image5/i1/scphn1.jpg

Treatment of Nonunions
Treatment of delayed and nonunion vary:• If fracture is stable and less than 6 months
old, some advocate prolonged cast immobilization
• For symptomatic nonunion, internal fixation with bone graft or intercarpal fusion are typical treatments
• Occasionally proximal row carpectomy is performed
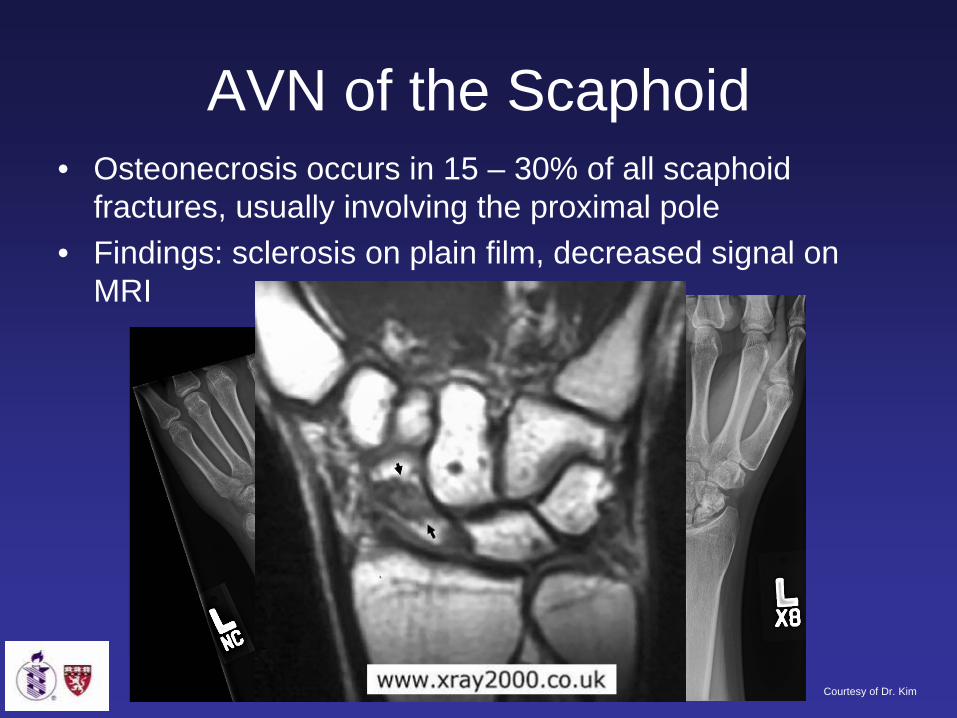
AVN of the Scaphoid• Osteonecrosis occurs in 15 – 30% of all scaphoid
fractures, usually involving the proximal pole• Findings: sclerosis on plain film, decreased signal on
MRI
Courtesy of Dr. Kim

Ligamentous injury: Sprains and carpal Instability

Background
• Perilunate instability injuries are one of the most common forms of carpal ligamentous injury
• Ligament injuries of wrist:simple sprains severe ligamentous disruption
• Low-grade injury very common• If serious injury goes untreated,
leads to chronic disability
http://akimages.crossmediaservices.com/dyn_li/80.80.75.0/a1061_g_akamai_net/7/1061/5412/home/www.walgreens.com/dbimagecache/307352.jpg

Ligamentous Anatomy
Lots of ligaments…important ones are:1. Radioscaphocapitate2. Radioscapholunate3. Radiolunate4. Radiolunotriquetral5. Scapholunate
Rockwood and Green’s Fractures in Adults, 6th edition. 2006. pp 857-908
•Extrinisic ligaments connect radius to carpus and carpus to metacarpals
•Intrinsic ligaments connect carpus to carpus

Mechanism and Pattern of Injury
• Like Scaphoid fractures, typically results from dorsiflextion injury (can be assoc with fractures as well)
• Injuries about the lunate occur in a predictable pattern:
I: Disruption of the Scapholunate ligament (often with scaphoid fracture)
II: Disruption of midcarpal joint (capitolunate)
III: Disruption of lunotriquetral joint
IV: Disruption of radiolunate joint, ultimately causing volar dislocation of lunate
Mayfield’s Stages:Vulnerable Zones of the Carpus
Lesser Arc
Greater Arc
Rockwood and Green’s Fractures in Adults, 6th edition. 2006. pp 857-908

Imaging• Standard Wrist Views: AP, Lat, Oblique, and
Scaphoid• On AP view, Assess:
– Gilula’s Lines– Scapholunate gap
• On Lateral view:– Scapholunate Angle– Radiolunate Angle
• Scaphoid:– Rule out concomitant scaphoid fracture

AP View: Gilula’s Lines
1: Proximal margin of scaphoid, lunate, triquetral
2: Distal margin of S, L, Tq3: Proximal margin of capitate
and hamate
Courtesy of Dr. Shetty
Carpal bones organized in 2 rows, borders of these rows are smooth lines
Disruption of these arcs indicates ligamentous instability

Filippo et al.
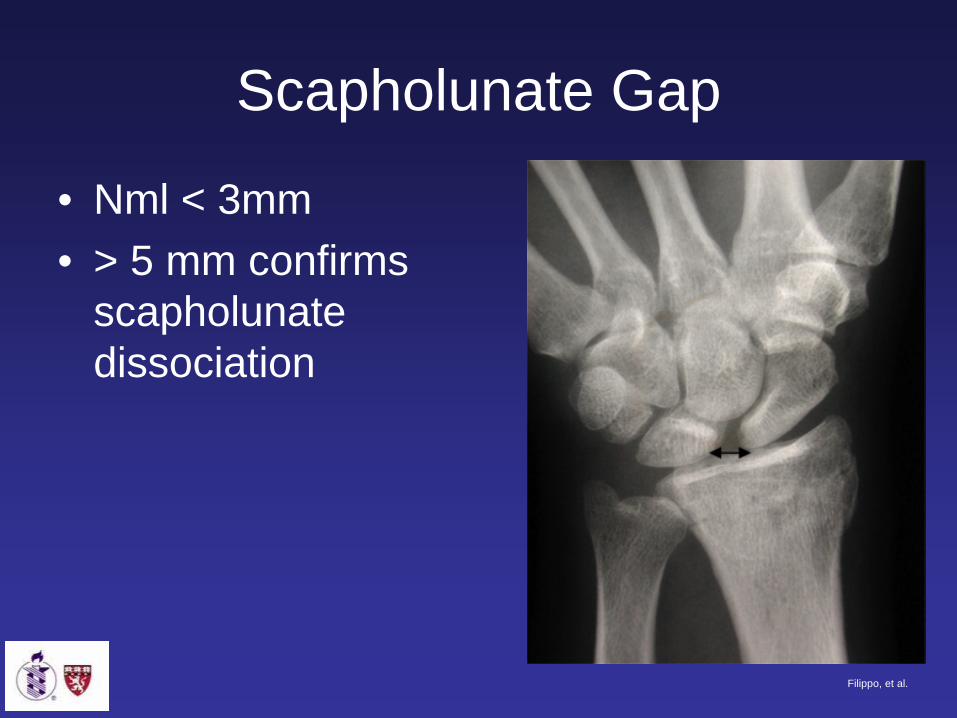
Scapholunate Gap
• Nml < 3mm• > 5 mm confirms
scapholunate dissociation
Filippo, et al.

Terry Thomas Sign…
http://en.wikipedia.org/wiki/Terry-Thomas


Signet Ring Sign
Filippo, et al.

On Lateral View:• Scapholunate angle
normally ranges 30 - 60 degrees– Angle > 60 degrees
suggests scapholunate instability
– Angle > 80 confirms scapholunate instability
• Radiolunate angle >20 degrees confirms scapholunate instability
Rockwood and Green’s Fractures in Adults, 6th edition. 2006. pp 857-908

Our Second Patient: also s/p fall onto outstretched hand
Scapholunate dissociation, perilunate dislocation, and Scaphoid fracture
AP Wrist Radiograph
Courtesy of Dr. Kim

* Courtesy of Dr. Kim
Our Second Patient: Scapholunate dissociation, perilunate dislocation, and Scaphoid fracture
Oblique Wrist Radiograph

Courtesy of Dr. Kim
Our Second Patient: Scapholunate dissociation, perilunate dislocation, and Scaphoid fracture
Lateral Wrist Radiograph

Courtesy of Dr. Kim
Our Second Patient: Scapholunate dissociation, perilunate dislocation, and Scaphoid fracture
Magnified View

Our Second Patient, s/p Closed Reduction
Courtesy of Dr. Kim
AP radiographs the wrist

Treatment Options
• Acutely: Closed reduction
• Early surgical reconstruction if swelling allows (immediate surgery if median nerve compromised)
• Closed vs. Open reduction with pinning
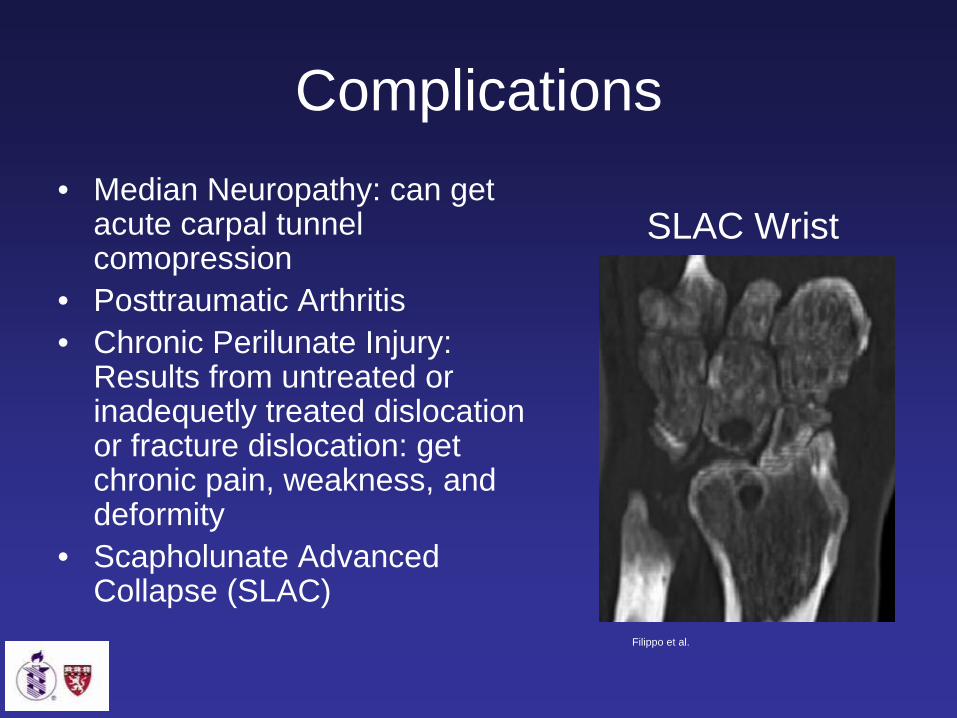
Complications• Median Neuropathy: can get
acute carpal tunnel comopression
• Posttraumatic Arthritis• Chronic Perilunate Injury:
Results from untreated or inadequetly treated dislocation or fracture dislocation: get chronic pain, weakness, and deformity
• Scapholunate Advanced Collapse (SLAC)
SLAC Wrist
Filippo et al.

Courtesy of Dr. Kim
Companion Patient:
Complications of Wrist Trauma: SLAC Wrist
AP Radiograph of Hand

Courtesy of Dr. Kim
Companion Patient:
Complications of Wrist Trauma: SLAC Wrist
Lateral Radiograph of Hand

Courtesy of Dr. Kim
Companion Patient:
Complications of Wrist Trauma: SLAC Wrist
AP Radiograph of Wrist

Examples of Other Wrist Fractures… Colles
Goldfarb, et al. Wrist Fractures: What the Clinician Wants to Know. Radiology 2001; 219:11-28

Smith
Goldfarb, et al. Wrist Fractures: What the Clinician Wants to Know. Radiology 2001; 219:11-28
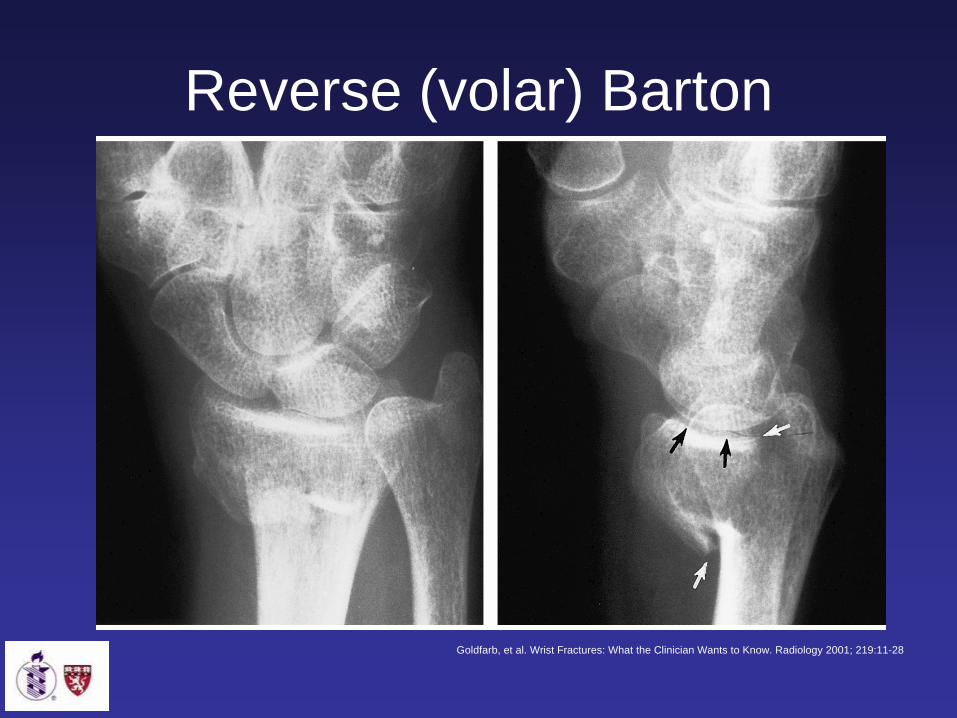
Reverse (volar) Barton
Goldfarb, et al. Wrist Fractures: What the Clinician Wants to Know. Radiology 2001; 219:11-28

Triquetral Fracture
Goldfarb, et al. Wrist Fractures: What the Clinician Wants to Know. Radiology 2001; 219:11-28

Trapezial Fx
Goldfarb, et al. Wrist Fractures: What the Clinician Wants to Know. Radiology 2001; 219:11-28
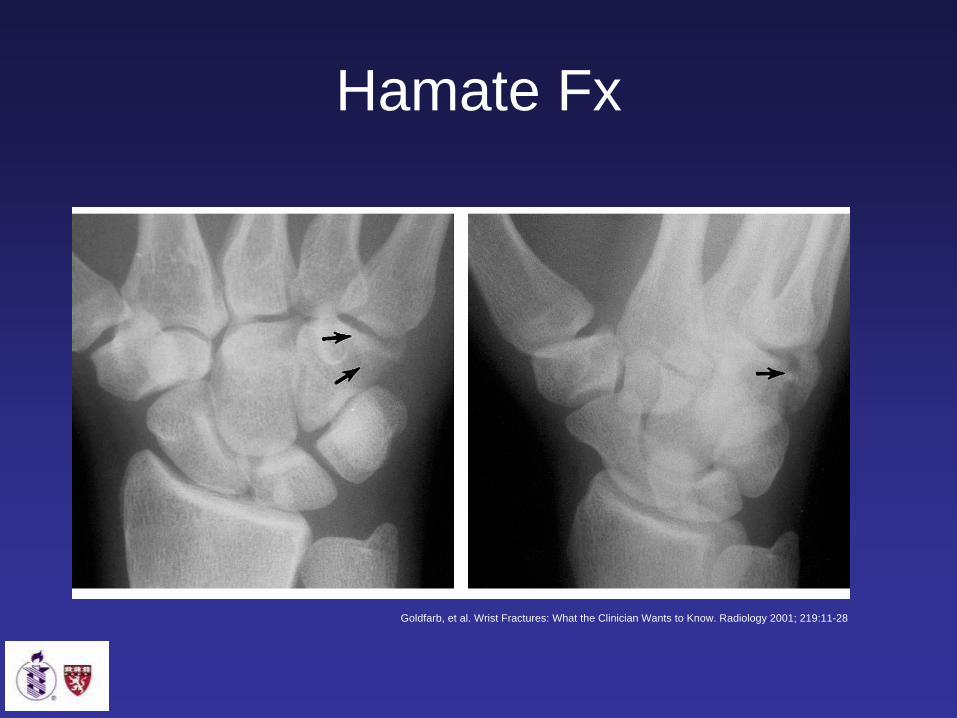
Hamate Fx
Goldfarb, et al. Wrist Fractures: What the Clinician Wants to Know. Radiology 2001; 219:11-28

Capitate Fx
Goldfarb, et al. Wrist Fractures: What the Clinician Wants to Know. Radiology 2001; 219:11-28

Trapezoidal Fx
Goldfarb, et al. Wrist Fractures: What the Clinician Wants to Know. Radiology 2001; 219:11-28

Acknowledgements
• Big thanks to: – Dr. Gillian Leiberman– Dr. Sanjay Shetty– Dr. AC Kim– Maria Levantakis– My HMS colleagues

References• American College of Radiology. Appropriateness Criteria: Acute Hand and Wrist Trauma. Last
review date, 2005• American College of Radiology. Appropriateness Criteria: Chronic Wrist Pain. Last review date,
2005• Boles, Carol A. Wrist, Scaphoid Fracture. eMedicine. Accessed 11/11/07.
http://www.emedicine.com/radio/topic747.htm#ref3• Cerezal L, Abascal F, Canga A. Usefulness of gadolinium-enhanced MR imaging in the evaluation
of the vascularity of scaphoid nonunions. AJR Am J Roentgenol. Jan 2000;174(1):141-9. • Dorsay TA, et al. Cost-Effectiveness of Immediate MR Imaging Versus Traditional Follow-Up for
Revealing Radiographically Occult Scaphoid Fractures. American Journal of Roentgenology 2001; 177:1257-1263
• Filippo, et al. Pathogenesis and evolution of carpal instability: imaging and topography. Acta Biomedica 2006; 77:68-180
• Goldfarb, et al. Wrist Fractures: What the Clinician Wants to Know. Radiology 2001; 219:11-28 • Haisman et al. Acute trauma to the Scaphoid. JBJS 2006; 12:2750 -2758• Rockwood and Green’s Fractures in Adults, 6th edition. 2006. pp 857-908