evidence based practice early childhood webcast training september 29, 2005 presented by california...
TRANSCRIPT
Evidence Based PracticeEarly Childhood
Webcast Training
September 29, 2005
Presented by
California Institute for Mental Health
Early Childhood Evidence Based Practices 2
Main Points
Defining evidence-based practices Early childhood social-emotional
development Early childhood specific practices Disorders in early childhood (DC:0-3)
Early Childhood Evidence Based Practices 3
Typical Emotional Development
Established sleeping and eating patterns Demonstrates arousal and focused attention Sustained attention, concentration and
persistence Inhibition of outburst to developmentally
appropriate expectations Expression of autonomy in a socially
acceptable manner
Early Childhood Evidence Based Practices 4
Typical Emotional Development
Enduring and supportive relationship with primary caregivers
Initiates play, discovery & learning Persists when discouraged or distracted Recovers from disruption, transition or
disappointment Emotional responses match social-cultural
context
Early Childhood Evidence Based Practices 5
Factors that Promote Optimal Development
Physically healthy Temperamentally easy Developmentally competent Caregivers have social support and strong
parenting skills Caregivers provide emotional support, guidance
and loving supervision Safe, stable and calm home/community
environment
Early Childhood Evidence Based Practices 6
Factors that Contribute to Emotional Disorders
Child is not “emotionally” available Inborn capacity to initiate and respond to
relationships, sustain attention, inhibit outbursts, and so forth
Parent is not “emotionally” available Learned capacity to read and respond to
infant/toddler’s cues, parenting model, and life circumstances
Early Childhood Evidence Based Practices 7
Signs of a Problem
Problematic behaviors are intensive, extensive, or pervasive; and/or
Primary caregivers are overwhelmed
Early Childhood Evidence Based Practices 8
Child’s Emotional Availability
Neurobehavioral functioning is compromised including sensory threshold, intensity of reaction, and self-regulation Low birth weight Development delays Physical disabilities Inadequate nutrition Drug or lead poisoning Maltreatment Exposure to violence
Early Childhood Evidence Based Practices 9
Caregiver Emotional Availability
Care-giving is compromised by inadequate parenting models, lack of social support, health/mental health or substance use disorders, or interpersonal/external stress Mental illness Substance abuse Limited parenting skills Teen parenthood Limited social support Poverty Domestic violence
Early Childhood Evidence Based Practices 10
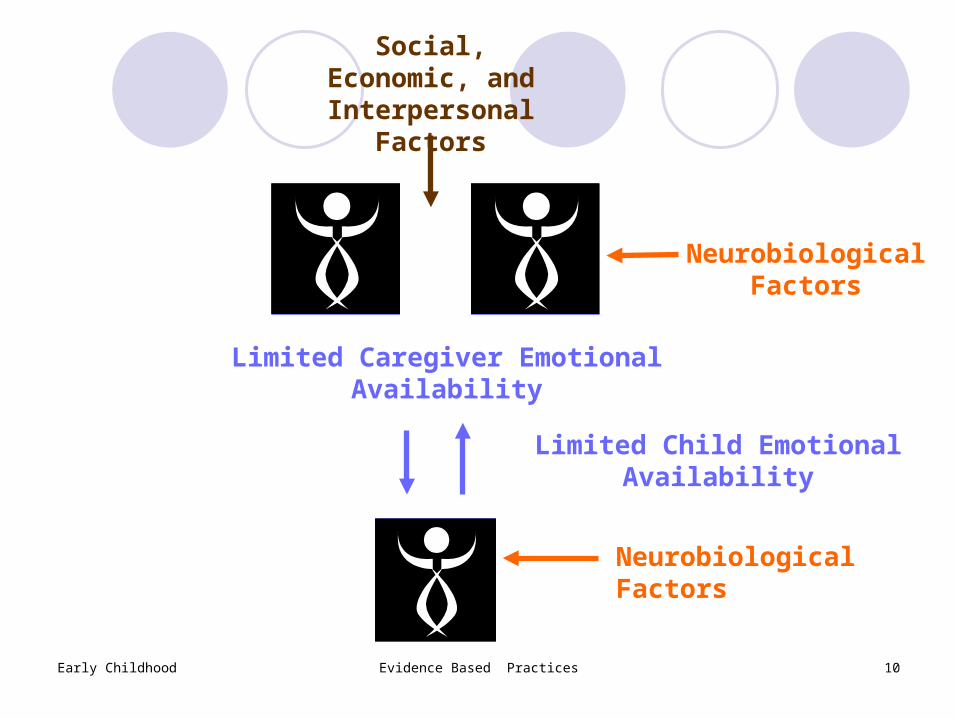
Neurobiological Factors
Limited Caregiver Emotional Availability
Social, Economic, and Interpersonal
Factors
Neurobiological Factors
Limited Child Emotional Availability
Early Childhood Evidence Based Practices 11
Evidence-Based Practices
“…the integration of the best research evidence with clinical expertise and patient values”
Based on the definition used in “Crossing the Quality Chasm: A New Health System for the 21st Century” (2001), by the Institute of Medicine
Early Childhood Evidence Based Practices 12
Levels of Science
Effective--achieves outcomes, controlled research (random assignment), with independent replication in usual care settings.
Efficacious--achieves outcomes, controlled research (random assignment), independent replication in controlled settings.
Not effective--significant evidence of a null, negative, or harmful effect.
Promising--some positive research evidence, quasi-experimental, of success and/or expert consensus.
Emerging practice--recognizable as a distinct practice with “face” validity or common sense test.
Early Childhood Evidence Based Practices 13
Which Level of Science to Select
Higher levels mean more confidence that if implemented in your community (with high model adherence) similar good outcomes will be achieved
Consider lower levels of science when there is no alternative at a higher level, or interested in a practice-to-science initiative
Early Childhood Evidence Based Practices 14
Treatment Approaches
Play therapy (therapist--child) Behavioral skills (practitioner--child) Parent training (practitioner--parent) Dyadic interaction (guided parent--child) Teacher trained (teacher--child) Childcare consultation (practitioner--teacher) Home visitation(practitioner--parent--child) Wraparound (interagency child and family
team)
Early Childhood Evidence Based Practices 15
The Incredible Years Effective Children 2-12 Decreases child behavior problems Increases parenting competencies Decreases maternal stress Strengthens parent-teacher and parent-caregiver
relationships Carolyn Webster-Stratton, University of Washington www.incredibleyears.org
Early Childhood Evidence Based Practices 16
Incredible Years Facilitated group intervention, practitioners with diverse
educational backgrounds Three sets of comprehensive developmentally based
curriculums for parents, teachers and children to promote emotional and social competence Basic parenting (early and school age) Advanced parenting Supporting your child’s education Child social skills Classroom based Teacher training
Weekly groups (12-14 sessions), 2 hours in length Uses work books, and video-vignettes to illustrate skills
Early Childhood Evidence Based Practices 17
Triple P Parenting Effective Children 0-16 Improves parenting skills Decrease in parental stress and depression Improves coping skills Decrease in child behavior problems Improves partner support Improves parent anger management skills Decreases social isolation Matt Sanders, University of Queensland www1.triplep.net
Early Childhood Evidence Based Practices 18
Triple P Parenting Practitioners with diverse educational backgrounds Parenting program Titrated levels of intervention Detailed support material for parents Five levels of intervention from primary prevention to
treatment Universal Triple P (primary prevention) Selected Triple P Primary Care Triple P Standard Triple P (individual or group) Enhanced Triple P
Early Childhood Evidence Based Practices 19
Parent-Child Interaction Therapy
Effective Children ages 2-8 years Parent-child guided intervention Decrease child behavior problems Increases parenting competencies Sheila Eyberg and colleagues, University of Florida www.pcit.org http://www.ucdmc.ucdavis.edu/caare/mental/pcit_traince
nter.html
Early Childhood Evidence Based Practices 20
Parent-Child Interaction Therapy
TherapistsClinic with two-way mirror, and “bug in the
ear” technologyIndividual sessions (about 12)Home models being developedParent-child guided intervention
Relationship Discipline
Early Childhood Evidence Based Practices 21
Nurse Family Partnership Effective Low-income, high risk first time parents
(pregnancy-age 2) Intensive home visitation to promote health and
welfare of parents and children Improved pregnancy outcomes Improved child health and well being Increases economic self-sufficiency David Olds and his colleagues, University of
Colorado www.nursefamilypartnership.org
Early Childhood Evidence Based Practices 22
Nurse Family Partnership
Registered nurseIntensive home visitation
Mother’s personal health Quality of care Life course outcomes
Visitations begin no later than 28 weeks of gestation until age 2
Visits involve mother’s support system
Early Childhood Evidence Based Practices 23
Early Intervention Foster Care Promising--efficacious Preschool age foster children Increases foster parent competencies Strong support for foster parents Decrease in child behavior problems Develops age appropriate child competencies Improves parenting competencies Decreases parental stress and depression Increase in social support Promotes reunification Phil Fisher and colleagues from Oregon Social
Learning Center [email protected]
Early Childhood Evidence Based Practices 24
Early Intervention Foster Care
Interdisciplinary team Intensive foster parent training Foster parent support groups Daily support calls 24 support to foster parent and biological family Child focused therapy Behavioral specialist for child in preschool, childcare or
home settings Parent training
Early Childhood Evidence Based Practices 25
Diagnostic Classification 0-3 Provisional system Multiaxial
Axis I: Primary classification Axis II: Relationship classification Axis III: Physical, neurological, developmental or
mental health disorders Axis IV: Psychosocial stress Axis V: Functional emotional developmental level
Designed to supplement Problems not addressed Earlier manifestations
Early Childhood Evidence Based Practices 26
Primary Diagnoses
Traumatic stress Disorders of affect Adjustment disorder Regulatory disorders Sleeping behavior disorder Eating behavior disorder Disorders of relating and communicating
Early Childhood Evidence Based Practices 27
Traumatic Stress
Existence of a traumatic eventRe-experiencing of the traumatic eventNumbing of responsiveness in a child or
interference with developmental momentum
Symptoms of increased arousalFears or aggression
Early Childhood Evidence Based Practices 28
Disorders of Affect
General feature of the child’s functioningNo severe developmental delays or
significant constitutional variationsNot specific to only a single relationship or
context
Early Childhood Evidence Based Practices 29
Disorders of Affect
Anxiety Prolonged bereavement/grief reaction Depression Mixed disorder of emotional expressiveness Gender identity disorder Reactive attachment deprivation/maltreatment
disorder
Early Childhood Evidence Based Practices 30
Adjustment Disorder
Mild, transient situational disturbancesNot explained by other conditionsOnset tied to a clear event or changeLasting days, up to 4 months
Early Childhood Evidence Based Practices 31
Regulatory Disorders
Sensory, sensory-motor, or processing difficulty and one or more behavioral symptoms
Hypersensitive Fearful and cautious Negative and defiant
Under-reactive Withdrawn and difficult to engage Self-absorbed
Motorically disorganized, impulsive
Early Childhood Evidence Based Practices 32
Sleep Behavior Disorder
Sleep disturbance is the only presenting problem for a child <3 years
Initiating or maintaining or excessive sleep Not attributable to affect or relationship
disturbances, trauma or adjustment problems
Early Childhood Evidence Based Practices 33
Eating Behavior Disorder
Difficulties in establishing regular feeding patterns with adequate food intake; does not regulate eating in accordance with physiologic feelings of hunger
Not attributable to sensory reactivity or processing or motor difficulties
Not explained by relationships, trauma, or adjustments
Early Childhood Evidence Based Practices 34
Disorders of Relating and Communicating (Multisystem Developmental Disorder) Significant impairment in, but not complete lack
of, the ability to engage in an emotional and social relationship with a primary caregiver
Significant impairment in forming, maintaining and developing communication
Significant dysfunction in auditory processing Significant dysfunction in the processing of other
sensations
Early Childhood Evidence Based Practices 35
Differential Diagnosis
Traumatic stress disorder considered first Regulatory disorders if clear constitutionally
or maturational-based sensory, motor, processing difficulty
Adjustment disorder considered if mild and of relatively short duration
Disorders of affect considered when there is no constitutionally or maturational-based difficulty or trauma/stress, and the difficulty is not mild or of short duration
Early Childhood Evidence Based Practices 36
Differential Diagnosis
Multisystem developmental disorder and reactive attachment, deprivation/maltreatment take precedence over all other categories
Relationship disorders considered when difficulty occurs only in relationship to a particular person
Early Childhood Evidence Based Practices 37
Relationship Disorders
OverinvolvedUnderinvolvedAnxious/TenseAngry/HostileMixedAbusive
Early Childhood Evidence Based Practices 38
Functional Emotional Developmental Level
Mutual attentionMutual engagementInteractive intentionality and reciprocityRepresentational/affective communicationRepresentational elaborationRepresentational differentiation I & II