evolution du système de santé en suisse : questions et ... · by the government through tax...
TRANSCRIPT

Evolution du système de santé en Suisse : questions et problématiques

Outline
• Overview of Healthcare Systems • Swiss and Canadian Comparisons • Challenges to all Healthcare Systems • Evaluation Framework • Current Swiss Challenges • Current Canadian Challeges

Health System Factors and their interactions that influence the health of individuals people and populations:
–Health Status and Outcomes –Determinants of Health –Healthcare System
4

Healthcare System Set of financial, material, human
and informational ‘resources’ used to provide services aimed
to re-establish, maintain or modify the health of individual
people and populations. 5

Four Main Models for Healthcare Systems
• Out of Pocket –health care paid directly by recipient
• Beveridge – Health care is provided and financed by the government through tax payments
• Bismarck – Health care provided via insurers called “sickness funds” funded by employers and employees through payroll deductions
• National Health Insurance – A combination of Beveridge and Bismarck Models – taxation with one “insurer” – the government

Out-of-Pocket
Partly US and some LMIC – get health care according to what you can afford to pay yourself.

Beveridge
UK National Health Services - no health care costs but everyone pays the same taxes even if they do not use
the services.

Bismarck
Started in Germany - insurance has to be offered to everyone and insurance companies are non-profit,
costs individuals more than the Beveridge model but more freedom of choice involved.

National Health Insurance
Canada – single payer so keeps costs low but issues with timely access

Swiss Model: LAMA (1996) & LAMAal (1994)
Modified Bismark from 1911 to today: •Universal coverage through insurance purchased by citizens •No cost past monthly premium and deductible – and may adjust the premium or deductible cost to include less/more coverage and private rooms/private hospitals •Insurance companies cannot make a profit under Swiss law •Most beneficiaries choose their own providers •99.5% of Swiss are insured •Everyone pays the same rates regardless of income •Some subsidies provided by government

Tommy Douglass - the battle with the CMA and Insurance Companies

A Universal Healthcare System in Canada
• Started in 1962 in Saskatchewan with Tommy Douglass • Canadian Medical Association was strongly opposed to
socialized medicine with a strike from July 1-23, 1962: “They’ll have to fill up the profession with the garbage of Europe.
Some of the European doctors who come out here are so bad we wonder if they have ever practiced medicine.”
• Resolved with agreement that medical insurance would remain government-controlled, compulsory, universal and reasonably comprehensive.
• National Medical Care Insurance Act was passed in the House of Commons on December 8, 1966.
• Private health expenditure accounts for 30% of health care financing as the Canada Health Act does not cover prescription drugs, home care or long-term care, prescription glasses or dental care

Canadian Health Act (1994)
1. Public Administration – All administration of provincial health insurance must be carried out by a public authority on a non-profit basis and are subject to audits
2. Comprehensiveness – All necessary health services, including hospitals, physicians and surgical
dentists, must be insured 3. Universality
– All insured residents are entitled to the same level of health care 4. Portability
– A resident that moves to a different province or territory is still entitled to coverage from their home province during a minimum waiting period
– This also applies to residents which leave the country 5. Accessibility
– All insured persons have reasonable access to health care facilities – In addition, all physicians, hospitals, etc., must be provided reasonable
compensation for the services they provide
14

Canada Switzerland
Population: 35.85 million 8.287 million Provinces/Cantons: 13 26 Size: 9.98 million km2 41,284 km2
Density: 3.92/km2 202/km2

Canada vs Switzerland
Canada Switzerland Alcohol Consumption 8.2 l/person 10.1 l/person Tobacco (daily smokers) 16.2 % 20.4 % Overweight & Obese 47.9 % 37.3 % Life Expectancy - Women 83 84.6 Life Expectancy - Men 79 79.8 Population with good health 88 % 87 % Over 65 years 16% 18% GDP per Capita (US$) $30,575 $46,019 Spending on Health (% GDP)* 11.4 % 11.4 % Spending on Promotion and Prevention (%*)
7.1 2.3
Inpatient vs Outpatient Spending 27.3 vs 25.4 45.6 vs 29.3

Challenges of Changing Demographics and Epidemiology
• Decreasing Birth/Fertility Rates (1.7%) • Migration flows – issue of forced migration • Increasing Life Expectancy
– Dependency risk – Retirement decisions – Savings and consumption behaviours
• Multimorbidity increasing • Double burden of chronic and infectious disease
(antibiotic resistance, STD, etc) • Cancer survival - transition to chronic disease

Other Challenges for Healthcare Systems
• Population Age Structure: – Medical care vs elderly care – Costs of last years of life (75+) – Aging population with long life expectancy and low
birth rates: dependency ratio changing • Health care vs Healthcare system:
– Health care contributes little to improved health in high income countries
– Link between infant mortality and GDP attenuates – Health expenditures + for female life expectancy
but negative for males

Technology as a Challenge for the Healthcare System
• Innovation: – Technology - hypothesized greatest driver of
increased health care expenditures – High-tech changes require specialized personnel
and expensive specialized equipment i.e. genetic tumour typing for chemotherapy
– Low-tech changes do not require special or expensive equipment i.e. aspirin after heart attacks
– Change in expertise or evidence

The Shifting Healthcare System
• From institutions to networks of care; from a single site (hospital, nursing home) to many sites
• From a single professional, generally a physician, to teams of health care professionals
• Expectations/knowledge/involvement of patients and family to make decisions about treatment mix
20

The Shifting Healthcare System
• ↑ Complexity • ↑ Interdependency • ↑ Uncertainty • Continuous change • Need work force that is recruited and trained for
these challenges • Increasing preoccupation with costs and
performance leading to increased government intervention/control/reform 21
Evaluation of the Healthcare System
• Interventions in healthcare system should: – Reduce risk of disease – Reduce deaths – Reduce complications – Improve functioning and well-being – Improve quality of life
• Reform strategies must: – Deliver appropriate care in timely manner – Deliver appropriate mix of treatment – Target treatment to those with indications and most likely to
benefit – Improve efficiency – Improve value for money while preserving quality

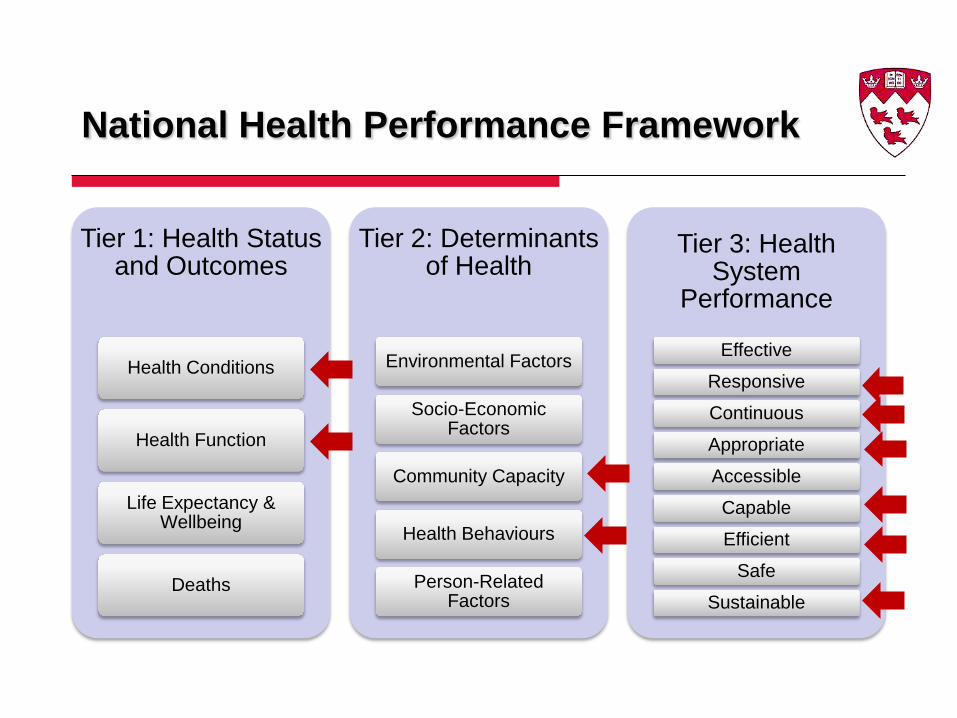
National Health Performance Framework
Tier 1: Health Status and Outcomes
Health Conditions
Health Function
Life Expectancy & Wellbeing
Deaths
Tier 2: Determinants of Health
Environmental Factors
Socio-Economic Factors
Community Capacity
Health Behaviours
Person-Related Factors
Tier 3: Health System
Performance
Effective
Responsive
Continuous
Appropriate
Accessible
Capable
Efficient
Safe
Sustainable

Current Issues for Switzerland
• Healthcare system is high-performing but costly • Demands on the system will continue to increase • The strengths of the system (high availability of services) may
become its greatest weakness – High number of hospitals for population and geographic size – Range of services being covered by insurance is increasing – Inter-cantonal variations in financing and access may mask
inequities and work against federal initiatives • Managed competition amongst health insurers needs to address
quality and costs not only coverage and choice • Limited national policies for prevention and health promotion • Lack of information on health inequities, quality of care and
health technology assessment • Issue with data collection, management (EMRs/health
information systems) and, therefore, coordination of care

Incentives in the Swiss Healthcare System
• Limit of different economic and regulatory incentives (level in Switzerland): – Cost to patient (intermediate) – Payments to Physicians (low) – Payments to hospitals (low) – Review of micro-technology use (little or none) – Review of macro-technology (little or none) – Choice and competition among insurance plans
(limited to supplemental coverage)
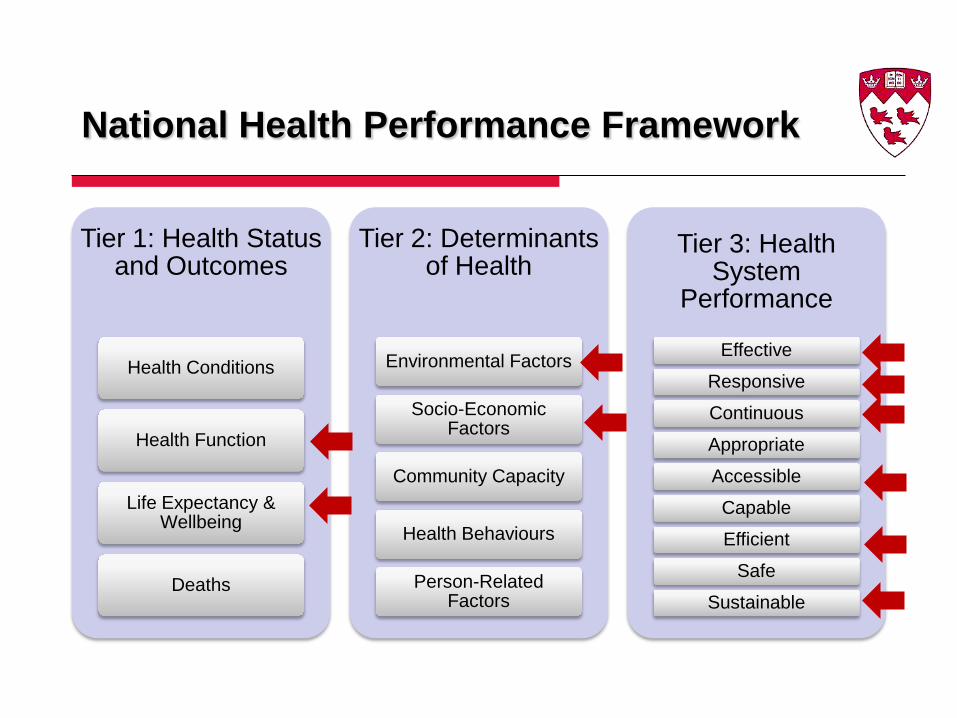
National Health Performance Framework
Tier 1: Health Status and Outcomes
Health Conditions
Health Function
Life Expectancy & Wellbeing
Deaths
Tier 2: Determinants of Health
Environmental Factors
Socio-Economic Factors
Community Capacity
Health Behaviours
Person-Related Factors
Tier 3: Health System
Performance
Effective
Responsive
Continuous
Appropriate
Accessible
Capable
Efficient
Safe
Sustainable

Calls for Policy Changes in Switzerland
• Improve governance and develop better information – Standards for information and reporting for quality of
care – Use of EMRs & PHR – Unique patient identifier
• Enhance quality, effectiveness, efficiency and coordination of care (health technology assessment)
• Change in workforce planning • Improving health promotion and disease prevention • Address over-diagnosis & over-treatment

Issues in Canada….
National Health Performance Framework
Tier 1: Health Status and Outcomes
Health Conditions
Health Function
Life Expectancy & Wellbeing
Deaths
Tier 2: Determinants of Health
Environmental Factors
Socio-Economic Factors
Community Capacity
Health Behaviours
Person-Related Factors
Tier 3: Health System
Performance
Effective
Responsive
Continuous
Appropriate
Accessible
Capable
Efficient
Safe
Sustainable


Gillian Bartlett, PhD Associate Chair, Professor Research and Graduate Program Director
Department of Family Medicine McGill University 5858 Cotes des Neiges, Suite 300 Montreal, Quebec Canada H2S 1Z1