evolving a strategy for emergency response to natural disaster
TRANSCRIPT

Emergency Response to Natural Disaster: Floods, Winds, and Earthquakes
Nicholas E. Kman, MD FACEPMedical Team Manager, Ohio Task Force 1The Ohio State University Department of Emergency MedicineTwitter @drnickkman
Disclosures
Ohio Task Force 1: FEMA Urban Search and Rescue
2

September 11th, 2001
http://www.dispatch.com/content/graphics/2015/01/07/meiling-hall.jpg

September 11th, 2001

September 11th, 2001

2005 Hurricane Season
6

March 2011, Japan Earthquake and Tsunami

Hurricane Sandy 10/25/12

Hurricane Sandy

Boston 4/15/13
10

2014-2015 Ebola Outbreak
11

2014-2015 Ebola Outbreak
12

Boko Haram
13

Objectives
Provide a background on Emergency Preparedness and Disaster Response since 9/11/01.
Analyze the Disaster Response Paradigm. Discuss Natural Disasters as they relate to
Preparedness. Define the injury patterns from Collapsed Buildings:
crush injury, compartment syndrome, and crush syndrome
Define the injury patterns from Wind Disasters. Describe flooding dangers.
14

What we will not cover!
Ebola Bomb and Blast Infectious Agents of Bioterrorism Chemical Agents of Terrorism
15

Disaster Defined
The United Nations Disaster Management Training Program defines Disaster as: A serious disruption of the functioning of society,
causing widespread human, material, or environmental losses which exceed the ability of affected society to cope using only its own resources.
Bonnett et al. Surge Capacity: A proposed conceptual framework. Amer J of Emerg Med 2007; 25: 297-306.
Dominique Faget—AFP/Getty Images

A Disaster: more simply…
Any event that threatens or overwhelms the normal operational capacities of the local healthcare system and emergency medical services (EMS).
University of Wisconsin Cooperative Institute for Meteorological Satellite Studies

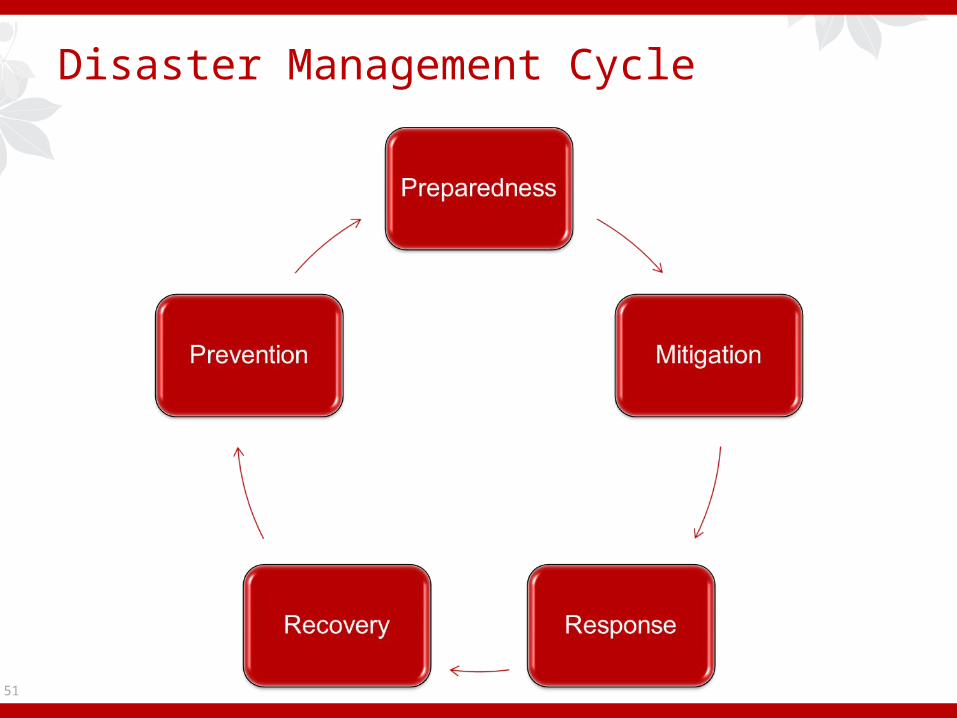
Disaster Management Cycle
18

Disaster Management Cycle
19

Preparation
Getting people and equipment ready to quickly and effectively respond to a disaster.
Conduct a Hazard Assessment Actual and potential hazards
Develop a simple disaster plan (EOP) Failing to plan is planning to fail!
Train all hospital staff in its application Awareness Technicians Patient care
American College of Surgeons, 2008, Advanced Trauma Life Support for Doctors, American College of Surgeons. Eighth Edition.American Medical Association, 2012, Basic Disaster Life Support, Course Manual. V. 3.0.

Preparation
21

Preparation
22

Preparation
23

Preparation-100 Year Flood
24

Preparation and Education
25

Preparation and JCAHO
6 focus areas for hospitals in disaster planning:o Communications –internal and external to
community care partners, state/federal agencieso Supplieso Security – Enabling normal hospital operations
and protection of staff and propertyo Staff – Roles and Responsibilities within a
standard Hospital Incident Command Structureo Utilities – Enabling self-sufficiency for goal of 96
hourso Clinical Activity – Maintaining care, supporting
vulnerable populations, alternate standards of care
26 http://www.jointcommission.org/emergency_management.aspx

Disaster Management Cycle
27

Disaster Management Cycle
28

Mitigation
Sustained actions taken to reduce or eliminate long-term risk to people and property from hazards.Reducing effects before the eventHave an Incident Command System
HICS (Hospital Incident Command System): organizational structure that provides direction for management of disaster response within hospital.
Train all staff in its application and use Plan in advance to ensure a coordinated response
American College of Surgeons, 2008, Advanced Trauma Life Support for Doctors, American College of Surgeons. Eighth Edition.American Medical Association, 2012, Basic Disaster Life Support, Course Manual. V. 3.0.
National Preparedness

National Disaster Medical System

Ohio Task Force-1
1 of 28 Urban Search and Rescue (US&R) teams in National US&R Response System managed by FEMA.
OH-TF1 also State of Ohio rescue response asset. MA-TF1 Urban Search & Rescue Structural Collapse
Training - YouTube

Ropes TrainingCamp Ravenna Joint Military Training Center
Florida State Fire College
Camp Atterbury, Muscatatuck Urban Training Center

National Incident Management System
34

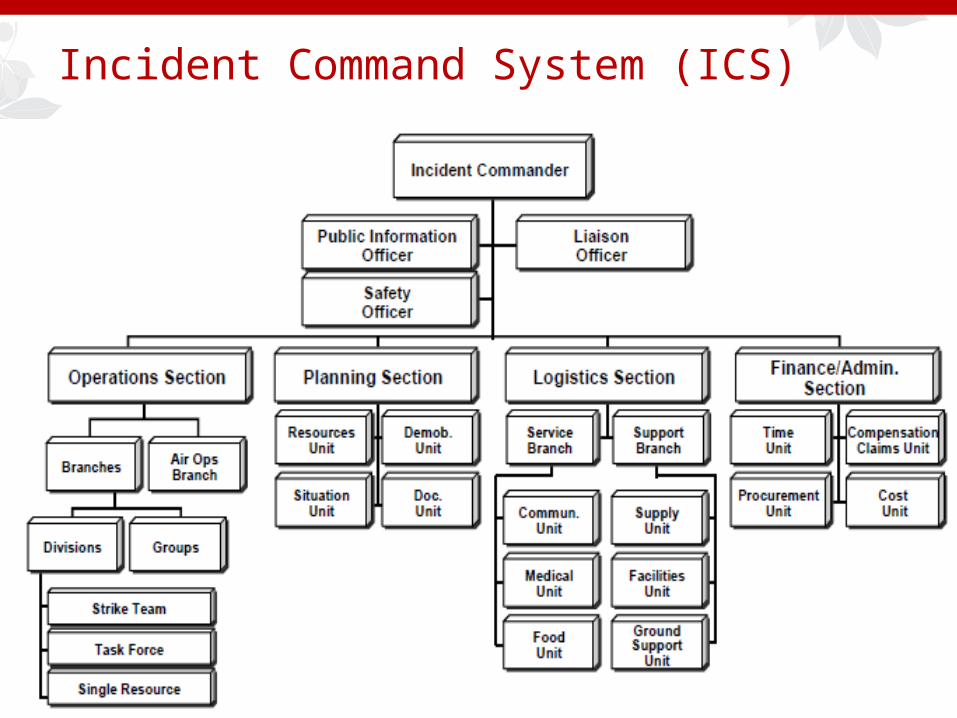
Incident Command System (ICS)
Set of personnel, policies, procedures, facilities, and equipment, integrated into common organizational structure designed to improve emergency response operations of all types.
May be used for planned events, natural disasters, and acts of terrorism.
Is a key feature of the National Incident Management System (NIMS 2004).

Incident Command System (ICS)
Based upon changeable, scalable response organization providing hierarchy within which people can work together effectively.
“First-on-scene" structure: First responder to scene has charge until incident has been declared resolved or more qualified responder arrives and receives command.
Used by all levels of government—Federal, State, local, and tribal—as well as by many private-sector and nongovernmental organizations.
http://emilms.fema.gov/IS200b/ICS0102summary.htm

ICS
Structured to facilitate activities in 5 major functional areas: Command Operations Planning Logistics Finance and administration.
37 http://emilms.fema.gov/IS200b/ICS0102summary.htm
Incident Command System (ICS)

Disaster Management Cycle
39

Disaster Management Cycle
40

Response: Prehospital and Inhospital Care Saving life and property during and immediately
after a disaster. Implement the planned response quickly Decontaminate every patient
Avoid contamination of facility, quarantine
Disaster triage scheme (SALT) Effective surge capability
Expect patient volume increased 20%
Don’t expect outside help for at least 24 hours
American College of Surgeons, 2008, Advanced Trauma Life Support for Doctors, American College of Surgeons. Eighth Edition.American Medical Association, 2012, Basic Disaster Life Support, Course Manual. V. 3.0.
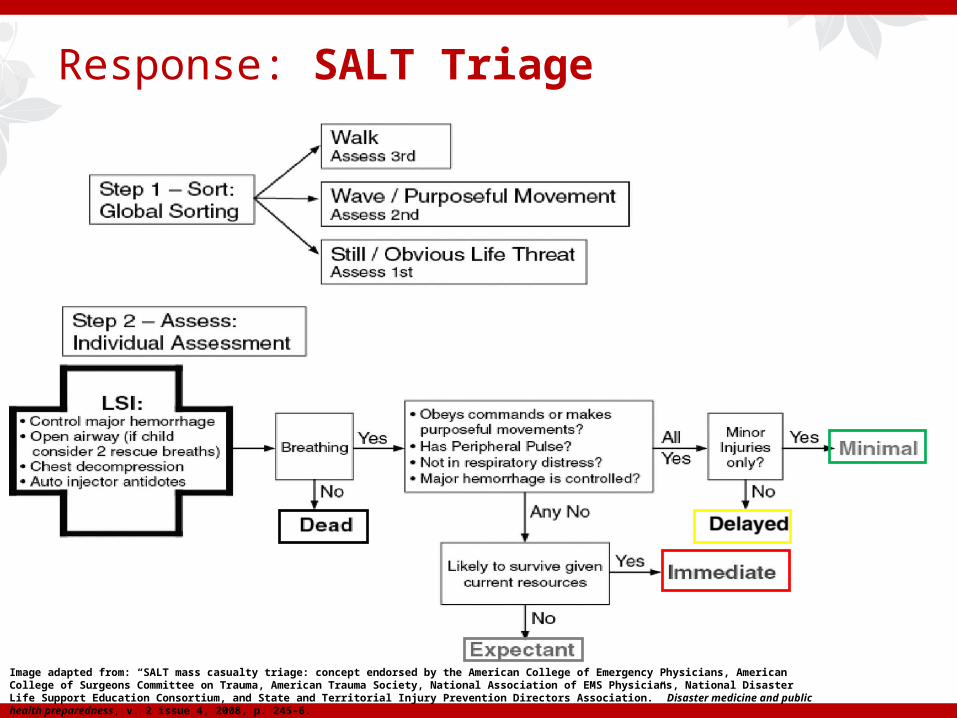
Response: SALT Triage
Image adapted from: “SALT mass casualty triage: concept endorsed by the American College of Emergency Physicians, American College of Surgeons Committee on Trauma, American Trauma Society, National Association of EMS Physicians, National Disaster Life Support Education Consortium, and State and Territorial Injury Prevention Directors Association.” Disaster medicine and public health preparedness, v. 2 issue 4, 2008, p. 245-6.

Response: Surge Capacity
If a mass casualty incident occurs, a healthcare system may be suddenly faced with significant increase of patients (Surge generating event).

Response: Surge Capacity
Surge capacity is the ability of healthcare facility or system to expand operations to safely treat an abnormally large influx of patients.
Surge Generating Event Contained
Geographically Defined (tornado, flood, bombing) Population Based
Infectious Diseases and Bioterrorism
http://buckeyextra.dispatch.com/

Inherent Response Problems
Sudden and unpredictable onset Chaos Loss of services Disruption of gov’t
Loss of infrastructure Transportation Communications Utilities
http://blogs.sacbee.com/photos/2010/08/hurricane-katrina-five-years-l.html

Inherent Response Problems (continued)
Variable mitigation and preparation for response at local level
Loss of basic physiological necessities Shelter Food/water Sanitation
Secondary hazards Further structural
damage Hazardous materials

Medical Response Obstacles
Medical system overwhelmed Non-selective victim process
Unusual medical problems Victims with previous problems Delay in treatment
High risks to rescue personnel
http://video.foxnews.com/v/2674051681001/oklahoma-city-bombing-missing-videos/?#sp=show-clips

Disaster Management Cycle
48

Disaster Management Cycle
49

Recovery
Putting a community back together after a disaster.
50
Disaster Management Cycle
51

Disaster Management Cycle
52

Prevention
Similar to Mitigation.
53

Natural Disaster Crash Course
Photo: NASA GOES Project

Natural Disasters
Natural Disasters Earthquakes Landslides and Mudslides Tsunamis Volcanoes Wildfires
Weather Emergencies Extreme Heat Floods Hurricanes Tornadoes Tsunamis Lightning Winter Weather
An event of nature that overwhelms local resources and threatens the function and safety of the community.

Wind Disasters
56
Marchigiani R, Gordy S, Cipolla J, et al. Wind disasters: A comprehensive review of current management strategies. International Journal of Critical Illness and Injury Science. 2013;3(2):130-142. doi:10.4103/2229-5151.114273.

Hurricanes
Most mortality originates from secondary disasters (storm surges, flash flooding, and tornados) triggered by original event.
In coastal regions, level of hurricane’s storm surge is strong predictor of mortality.
Winds are 2nd deadliest aspect. Most common non‑fatal traumatic injury pattern in a
hurricane consists of superficial lacerations from airborne glass and/or other debris.
57

Tornados
Tornados usually develop during intense “supercell thunderstorms”.
Result from updrafts created by solar warming of earth’s surface. Updrafts then develop into vortex with strong rotary winds and violent pressure changes.
Due to brief or absent warning, community has little time to prepare or seek shelter, and morbidity and mortality is proportionally higher compared to other WDs.
58

Tornado Associated Injuries
Most tornado fatalities die at scene and tend to be either in exposed areas or in mobile homes.
Risk factors for injury and death during a tornado include: Poor building anchorage Occupant location other than a basement Age over 70 years High wind strength
59

Earthquake Injuries
60 Haiti Earthquake 2010 US&R LA County

Crush Injury
Lactic acid produced
Myoglobin, Potassium and other electrolytes released
Other toxins created/released (superoxides, O2 free radicals)
Capillary leak
Thromboxane, prostaglandins, and other immune system substances generated
Muscle cell enzymes released

Crush Injury
Effects are LOCAL ONLY until pressure released and tissue reperfused
Reason that patients survive entrapment despite severe crush injury
Adverse processes begin immediately upon pressure release

Effects of Releasing Compressed Tissue
Immediate: Capillary leak
Hypovolemia/Hypotension Shock
Severe metabolic acidosis: dysrhythmias, V-fib High serum potassium: cardiac dysrhythmia or arrest
Delayed: Myoglobin/uric acid/renal toxins: kidney failure Other toxins: lung/liver/renal injuries

Cause of Death
Major Hypovolemia Dysrhythmia Renal failure
Other Adult Respiratory Distress Syndrome (ARDS) Sepsis Other electrolyte disturbances Ischemic tissue infection (gangrene)

EKG Abnormalities
Related to Potassium levels and rate of rise Acidosis Other electrolyte abnormalities Other injuries Peaked T-waves, AV blocks, widened QRS, sine wave
Responds rapidly to effective intervention

Strategies to Prevent Renal Injury
Maximize renal perfusion IV normal saline
Diuresis (brisk urine flow)
Careful alkalinization of urine (pH > 6.5) Sodium bicarbonate
Monitor urine flow and pH (Bladder catheterization if possible)

Initial Management “in the Rubble”
Maintain ABCs Protect airway Assess for crush injury potential Provide psychological support
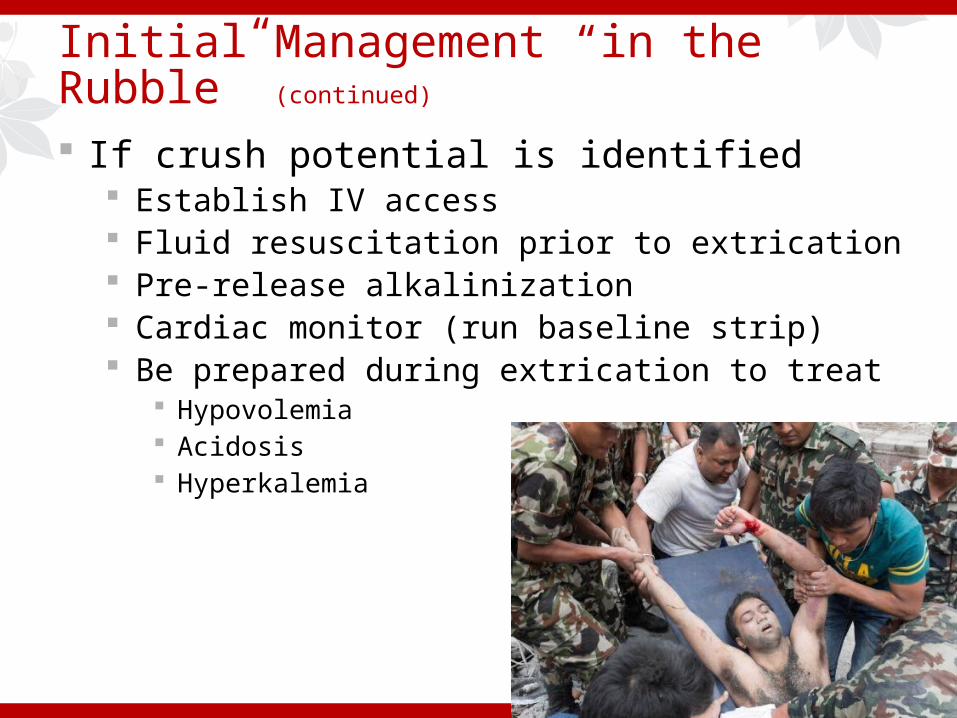
Initial Management “in the Rubble” (continued)
If crush potential is identified Establish IV access Fluid resuscitation prior to extrication Pre-release alkalinization Cardiac monitor (run baseline strip) Be prepared during extrication to treat
Hypovolemia Acidosis Hyperkalemia

Floods-Preparedness
Recognize Flood Risk Identify flood-prone or landslide-prone areas near
you. Know your community’s warning signals, evacuation
routes, and emergency shelter locations. Know flood evacuation routes near you.
69 www.dispatch.com

Floods-Response
Unplug appliances to prevent electrical shock when power comes back on.
Gather emergency supplies and follow local radio or TV updates.
Do NOT drive or walk across flooded roads. Cars and people can be swept away
70 www.cdc.gov

Floods-Response and Recovery
Practice safe hygiene Wash hands with soap and water to prevent germs. Listen for information from local officials on how to
safely use water to drink, cook, or clean. Use fans, air conditioning units, and dehumidifiers for
drying. For cleanup, wear rubber boots and plastic gloves.
Clean walls, hard floors, and other surfaces with soap and water. Use mixture of 1 cup bleach and 5 gallons water to disinfect.
71 http://emergency.cdc.gov/disasters/floods/readiness.asp

Disaster Management Cycle Review
72

Disaster Management Cycle Review
73
Emergency Preparedness
Disaster Management

Final Pearls
Have a straightforward disaster plan and educate everyone in its use.
Have an incident command structure and drill often.
Have a disaster triage scheme, and mobilize surge resources as needed.
Have a traffic control system and communication system.
74

Final Pearls
Communications-Cell Phones Go Down! Redundant modes / systems / equipment
Supplies-Bring your own Ample supply stores / reliable supply chains
Security Control traffic flow / patient, staff safety
Volunteers Physician role is hospital-based patient care
75

What can you do?
Be Informed: Learn your Emergency Operations Plan (EOP) and exercise it.
Find out where you would report in a disaster. Make a Plan: Prepare yourself and your family (
www.ready.gov). Build a kit.
76
http://www.costco.com/American-Preparedness-Emergency-Backpack-Kit.product.11100551.html

What can you do?
Get Involved: Join your Emergency Preparedness Committee.
Go Regional, then National!
77

References
FEMA Medical Team Training Student Reference CD (2/2009)
FEMA WMD for Medical Specialist Training CD
Franco et al. The National Disaster Medical System: Past, Present, and Suggestions for the Future. Biosecurity and Bioterrorism: Biodefense Strategy, Practice, Science 2007; 5: 319-325.
Bonnett et al. Surge Capacity: A proposed conceptual framework. Amer J of Emerg Med 2007; 25: 297-306.
ATLS 8th Edition.
Kman NE, Bachmann D. “Biosurveillance: A review and Update.” In Special issue: Advances in Development of Countermeasures for Potential Biothreat Agents. Advances in preventive medicine, v. 2012, 2012, p. 301408.
Kman N, Rund D. “Disaster Preparedness 10 years after 9/11: The Experts Weigh In”. Emergency Medicine. Emerg Med 2011; 43(9): 12-13. (September) www.emedmag.com.
Marchigiani R, Gordy S, Cipolla J, et al. Wind disasters: A comprehensive review of current management strategies. International Journal of Critical Illness and Injury Science. 2013;3(2):130-142. doi:10.4103/2229-5151.114273

References
www.fema.gov
www.cdc.gov
http://phil.cdc.gov/phil/home.asp
Marchigiani R, Gordy S, Cipolla J, Kman NE, Stawicki S, et al. "Wind disasters: A comprehensive review of current management strategies." International journal of critical illness and injury science. Vol. 3, no. 2. (Apr 2013): 130-142.
Kman N, Bachmann D, Folley A, Adams J, Greer M. Emergency Preparedness Simulation Cases for Medical Students: Crush and Organophosphate Exposure. MedEdPORTAL; 2013. Available from: http://www.mededportal.org/publication/9330.
Yuri Rojavin, Mark J Seamon, Ravi S Tripathi, Thomas J Papadimos, Sagar Galwankar, Nicholas Kman, James Cipolla, Michael D Grossman, Raffaele Marchigiani, Stanislaw P A Stawicki. “Civilian nuclear incidents: An overview of historical, medical, and scientific aspects.” Journal of emergencies, trauma and shock, v. 4 issue 2, 2011, p. 260-72.
Kman NE, Nelson R. Infectious Agents of Bioterrorism: A Review for Emergency Physicians. Emerg Med Clin N Am 2008; 26: 517-547.

Questions
80