exercise for pain management: brain aerobics? · personality development. 5. the mind-body...
TRANSCRIPT
Exercise for Pain Management: Brain Aerobics?
Dr. Julia AlleyneUniversity of Toronto
Toronto Rehab University Health Network
Copyright © 2017 by Sea Courses Inc.
All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means – graphic, electronic, or mechanical, including photocopying, recording, or information storage and retrieval systems without prior written permission of Sea Courses Inc. except where permitted by law.
Sea Courses is not responsible for any speaker or participant’s statements, materials, acts or omissions.

Disclosures
• No financial investment
• No conflicts of interest
Objectives
• To describe the current understanding of the brain’s role in pain perception and pain modulation
• To identify which exercise methods are effective for pain management control and the prescribing parameters for best outcomes
PAIN: Describe Pain in One Word
PAIN: Describe Pain in One Word
PAIN:
An unpleasant sensory and emotional experience associated
with actual or potential tissue damage
ORdescribed in terms of such
damage
What’s Missing ?
What’s Missing ?
• Function
• Disability
• Impact on role
• Impact on Self Perception
• Fears, Anxieties and Sleep disorders
Approach to the Patient with Chronic Pain
Anatomical Physiological Emotional
Applying Exercise Principles to Pain
How does Pain effect the body?
• Tight Muscles
• Hypersensitivity
• Inactivity
• Cognitive Fog
Does exercise work on Pain?
• Strength
• Flexibility
• Aerobics
• Balance
What are the types of chronic pain conditions ?
• Headache
• Osteoarthritis
• Fibromyalgia
• Low Back Pain
• Neuropathic Pain
• Post Surgical Prolonged Pain
• MSK related Oncology Pain
What is Pain ?
Past Theories of PainSpecificity of Pain
“The Intensity of Pain is directly related to the amount of tissue Injury” Rene Descartes, 1600
“The meaning associated with the injury was related to the experience of pain Henry Beecher, 1945
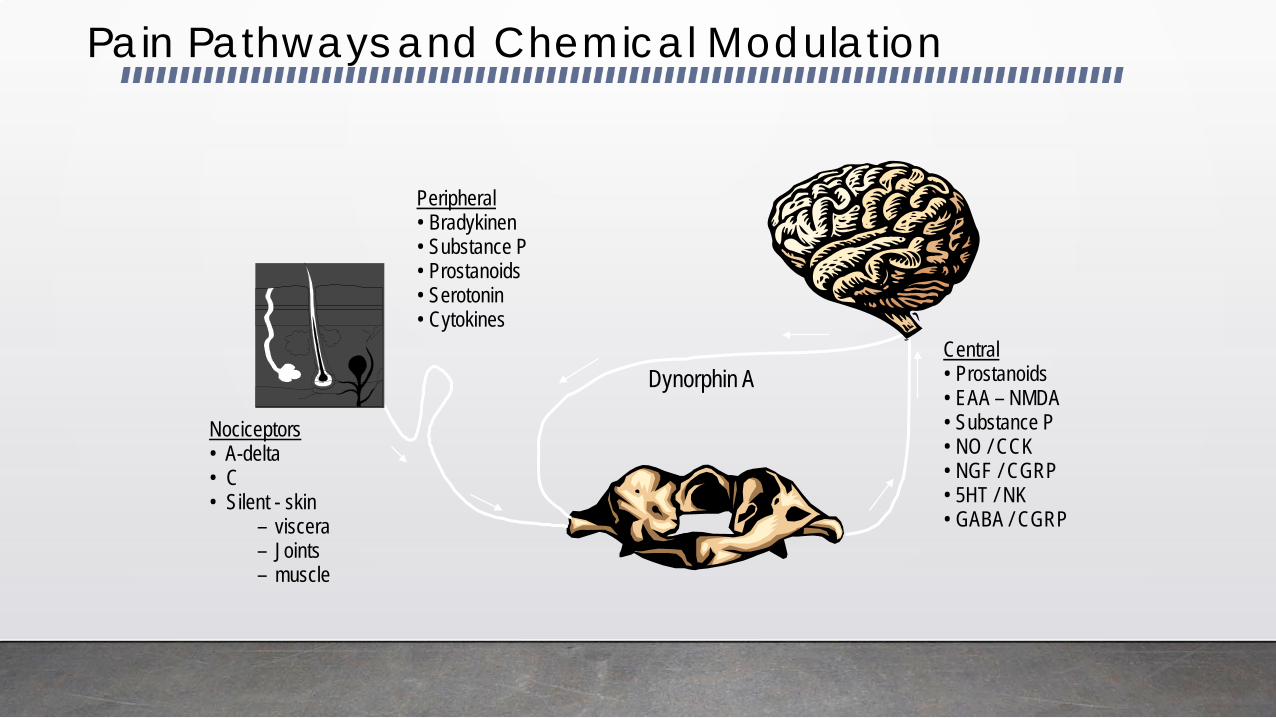
Peripheral• Bradykinen• Substance P• Prostanoids • Serotonin• Cytokines
Central • Prostanoids • EAA – NMDA • Substance P• NO / CCK• NGF / CGRP• 5HT / NK• GABA / CGRP
Nociceptors• A-delta • C • Silent - skin
– viscera – Joints– muscle
Dynorphin A
Pain Pathways and Chemical Modulation
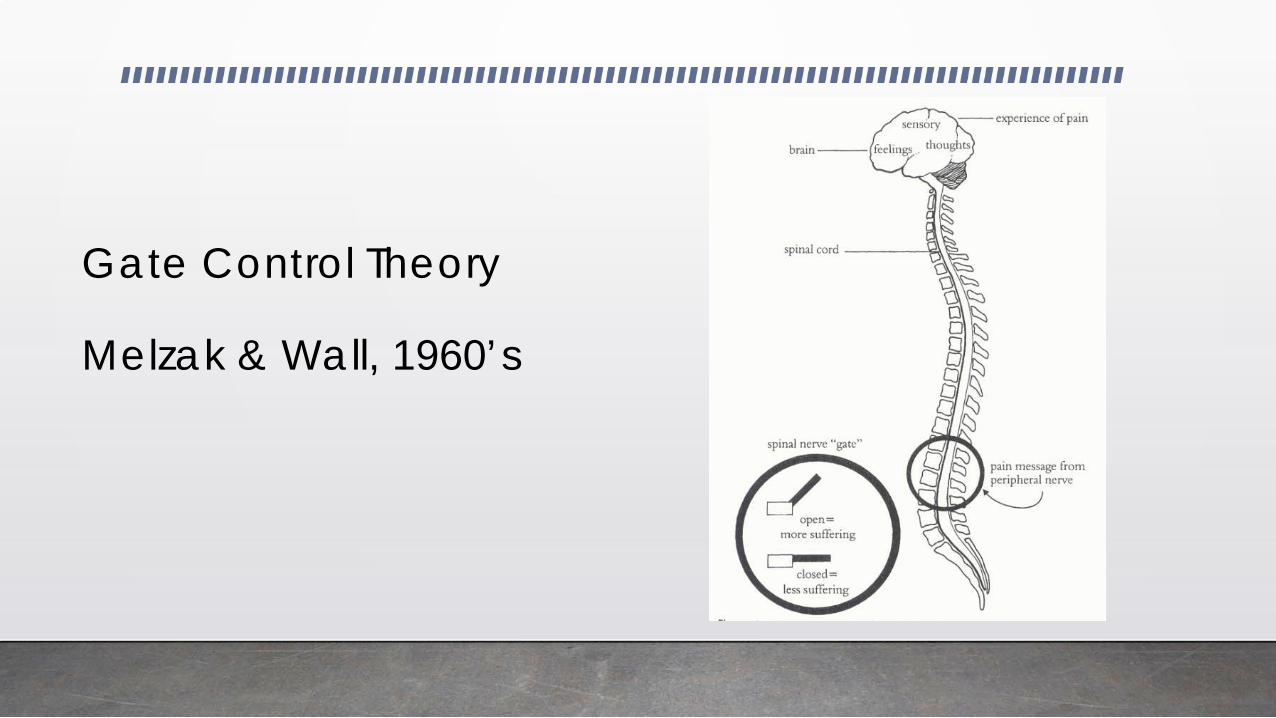
Gate Control Theory
Melzak & Wall, 1960’s
Gate Control Theory
The spinal cord is processing Sensory signals of pressure, temperature and vibration.
• Heat/Cold
• Acupuncture
• Massage
• Neuro reception
Exercise ?
Gate Control
Factors that Open the Gate Factors that Close the Gate
Gate Control
Factors that Open the Gate
Feel – Stress and Tension
Think – Focus and Boredom
Do - Weak and Stiff
Factors that Close the Gate
Feel- Relaxation and Contentment
Think – Distraction and Learning
Do- Activity and Fitness
Heel Raises
The Brain in Pain• Production of Endorphins may inhibit pain
• Exercise, Stress, Excitement
• Cognitive & Emotional Factors a) Increase Pain
Focus, Analysis, Worry and Negative Fearsb) Decrease Pain
Positive Outlook, Purpose, Control, Tasks
The Brain in Pain
New Theories
- Neuro Chemical Receptors
- Neuro Sensitivity and Increased Reaction
- Neuro Processing Blocks
The Brain in Pain
Central Sensitization
Pain itself can change how pain works, resulting in more pain with less provocation
New Theories of Chronic Pain Education
1. Pain does not always reflect Pathology2. Normal Investigations don’t mean “it’s in
your Head”3. Physiology is the key to Function4. Pain Perception is based in genetics and
personality development.5. The Mind-Body Connection is Key.
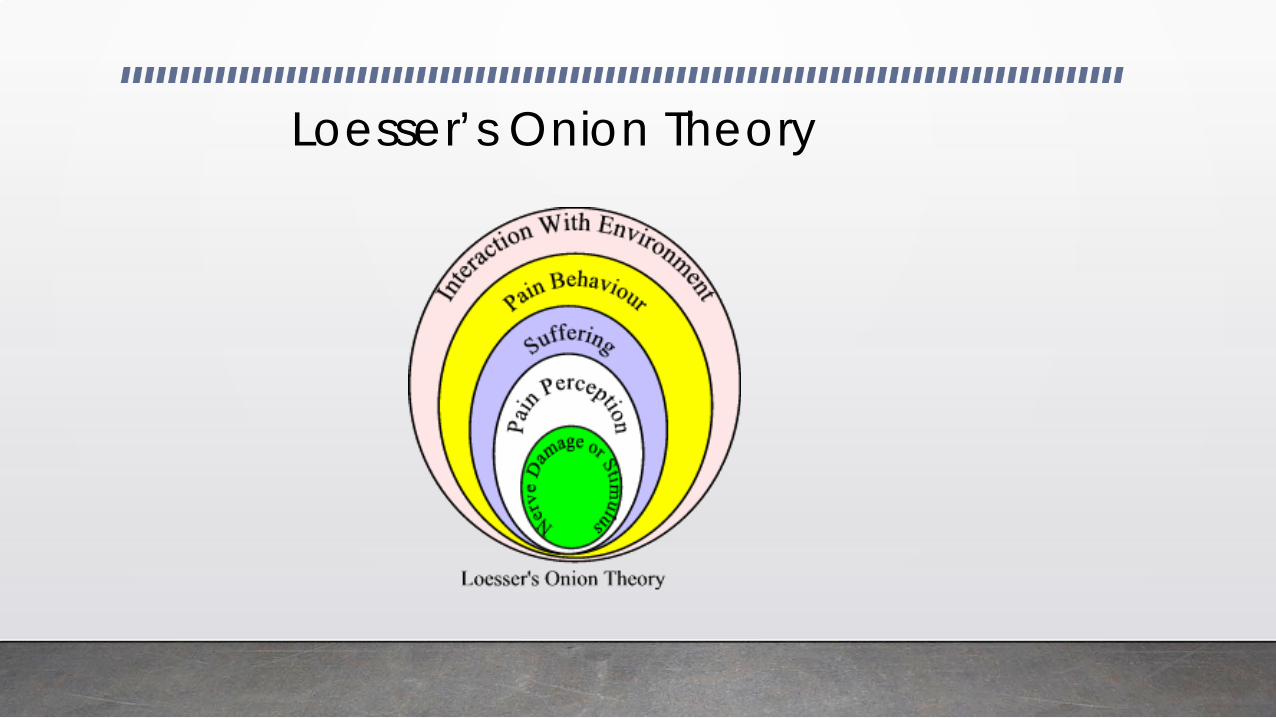
Loesser’s Onion Theory
Assessing the Severity of Pain
• The patient report is valid!
• Verbal: 5 or 10 point scale
• VAS, Brief Pain Inventory
• Pain and activity diaries
Clinical Questions to detect Chronic Pain
• Psychosocial Risk Factors that predict risk or probability of Chronic Pain
• Predictive of Poor Outcome in Rehabilitation
• Indicate the need for early multi-disciplinary treatment including Cognitive BehaviouralCounselling
Assess the Impact on the Patient’s Life
• Activities of daily living
• Sleep
• ‘Downtime’ vs. ‘uptime’
• Relationships
• Coping strategies
• Collateral information
Risk Factors for Poor Prognosis
- Intensity of Initial Pain
- Nature of Collision
- Women more than Men
- Not Prior Personality Features
- Physical Deconditioning
- Hypervigilance of Body Awareness

Green Flags
• Involved in Fitness and sport
• Good Family Life
• Satisfied in Career
• Insight and Intelligence
• Low Anxiety Factor
• Response versus Resistance
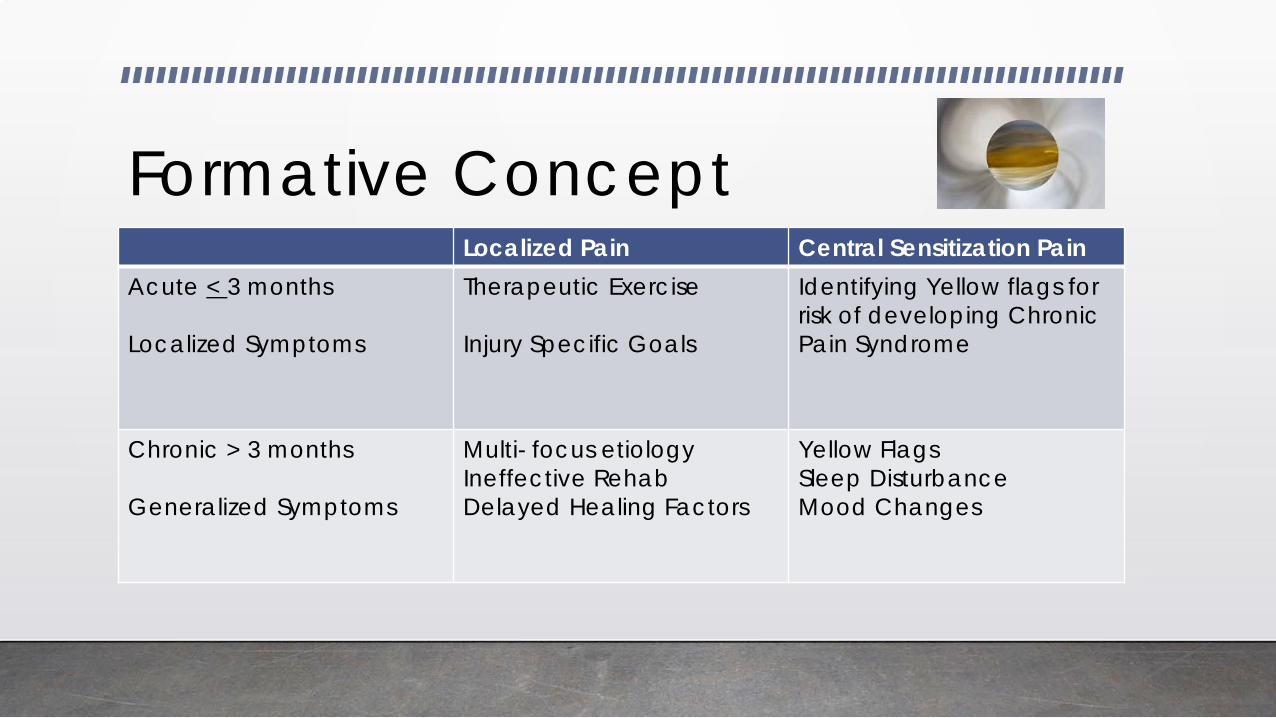
Formative ConceptLocalized Pain Central Sensitization Pain
Acute < 3 months
Localized Symptoms
Therapeutic Exercise
Injury Specific Goals
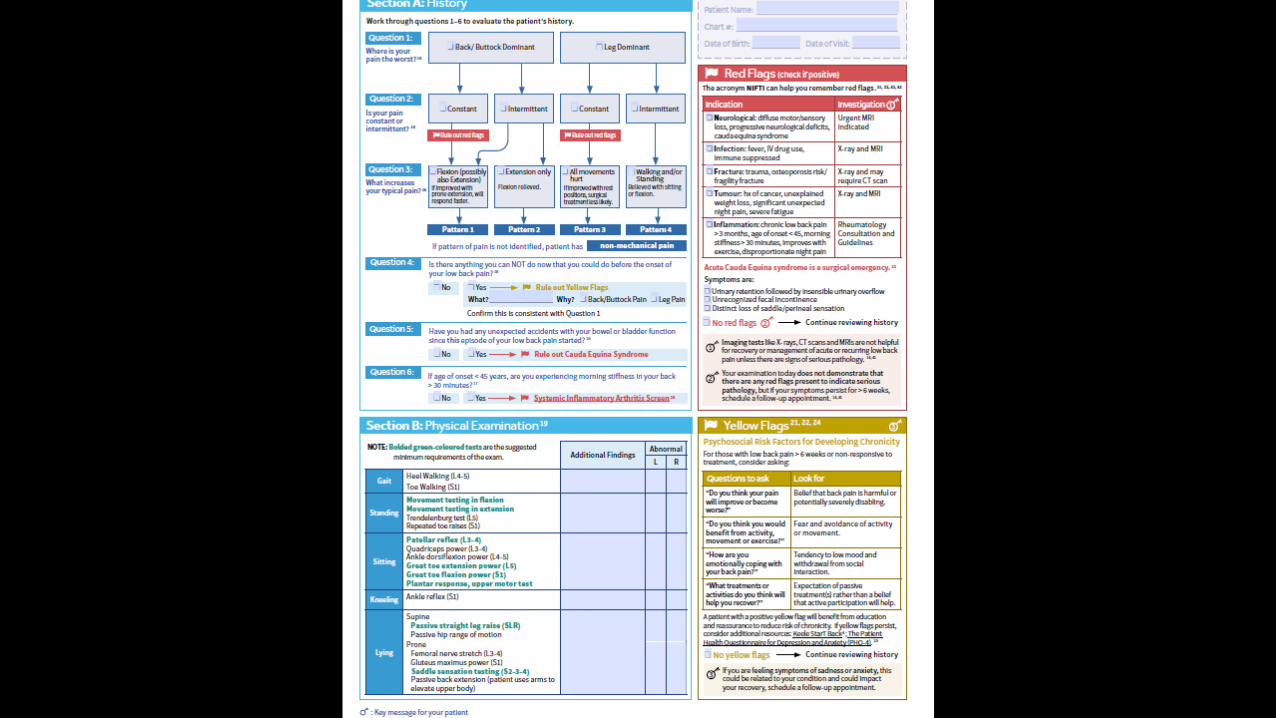
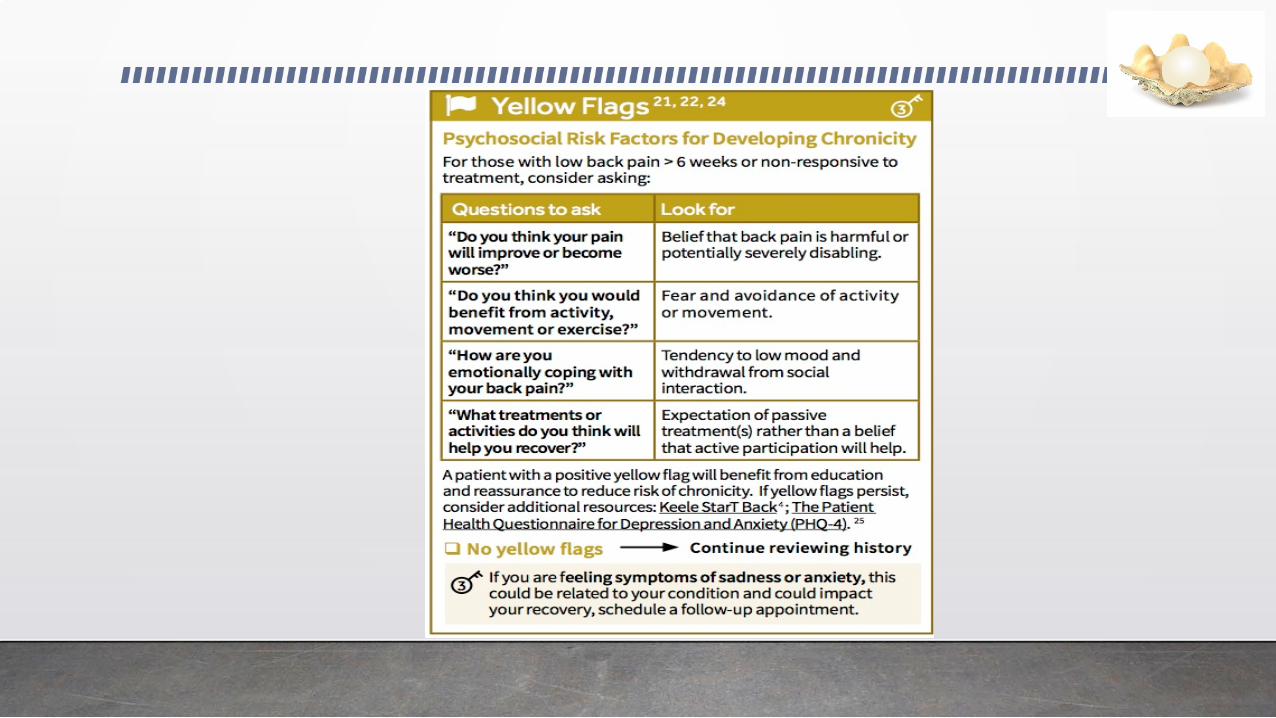
Identifying Yellow flags for risk of developing Chronic Pain Syndrome
Chronic > 3 months
Generalized Symptoms
Multi- focus etiologyIneffective RehabDelayed Healing Factors
Yellow FlagsSleep DisturbanceMood Changes

Pain Spiral
Pain Centred Life
Withdrawal from social activities
StigmaSurgery
Injury
Tissue Damage Depression
Rest/Passive Surgery
Harm vs. Hurt Limits Activities
Weak, tight muscles
Deconditioning
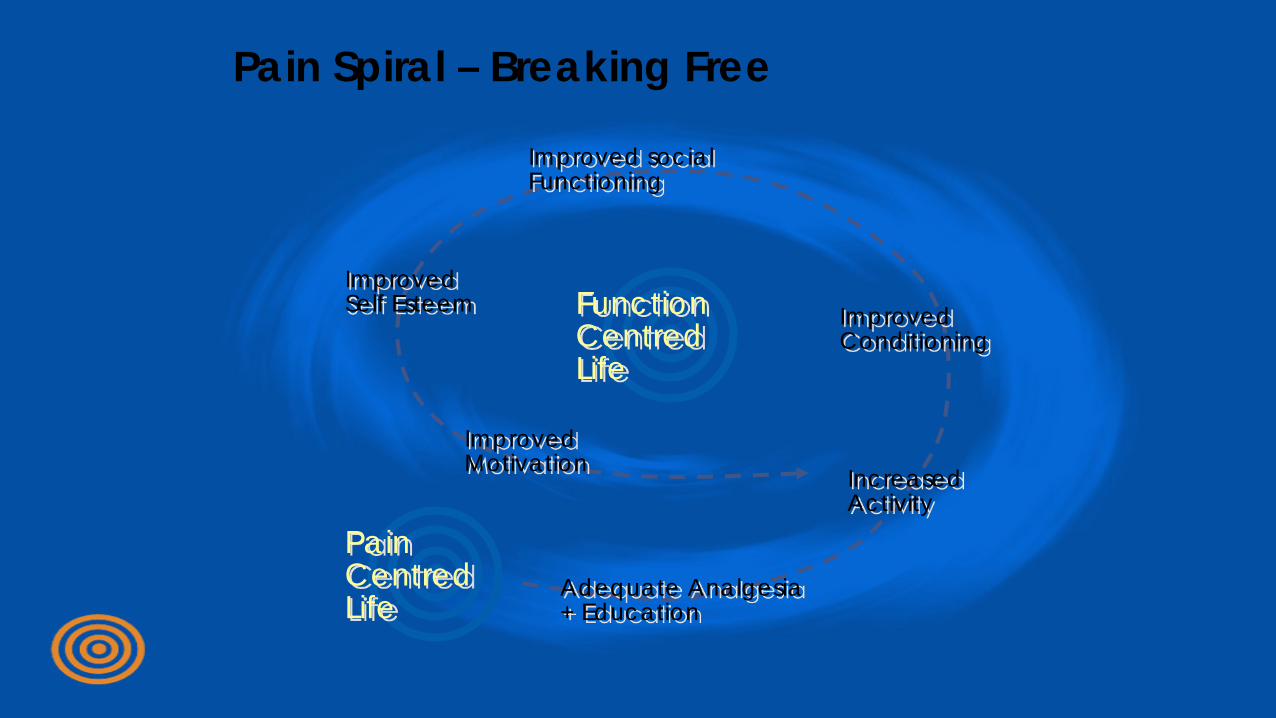
Pain Spiral – Breaking Free
Function Centred Life
Pain Centred Life
Improved social Functioning
Improved Self Esteem
Improved Motivation
Improved Conditioning
Increased Activity
Adequate Analgesia + Education
Pain Centered Exercise Prescription
• Target Large Muscles with Functional Activities
Increase Strength
• Target Tight Postural with Frequent Micro-stretches
Increase Flexibility
• Sub-optimal threshold with goal of 12-15 minutes
Increase Aerobic Endurance
Case Study
Frau Jaeger is a 41 year old office worker who began to experience generalized aching and stiffness in her back, legs and shoulders over the last year. She does not recall a trigger event. She is irritable and frustrated and wants to be investigated and diagnosed.
History Probe
- Sleep patterns are disrupted- Difficulty falling asleep- Frequent waking during the night
- Pain is described as frequent aching which intensifies with prolonged positioning or fatigue
- Tingling experiences intermittently circumferentially in hands and legs
Patient Symptom Inventory
- Fatigue
- Generalized weakness, hard to climb a hill
- Lumbar pain with occasional associated neck pain
- Morning stiffness in her hips, shoulders and back x 10 min
- Mood Swings described as irritability with some sadness
F. I.T.T.
Is exercise or activity a usual part of your week ?
“I like to walk when I’m not sore but that isn’t very often”
When was the last time that you were able to walk ?
“ About 2 weeks ago, I walked with a friend for an hour and really hurt for the next week”
When you walked, did you have to stop and start ? Did you recall if you were sweating?
“ I usually stop every 5 minutes and sit down, I don’t think I sweat when I walk”
F. I.T.T.
“I like to walk when I’m not sore but that isn’t very often”
About 2 weeks ago, I walked with a friend for an hour and really hurt for the next week”
“ I usually stop every 5 minutes and sit down, I don’t think I sweat when I walk”
F – Sedentary to Occasional
I – Low
T – Walking
T – 5 minutes
Disruptive Sleep & ExercisePartial Truth : Exercise will help your Sleep
Full Truth:
Sleep disturbance is reduced by 27% in Active Healthy Adults• 12 Population based studies that report better sleep patterns with physically active
adults• 2 Studies indicate a lower risk of Sleep Apnea with regular physical activity
Sleep Disturbance and Depression• Strength Training Exercise reduces sleep disturbance symptoms by 30%• Strength training > General Exercise• High Intensity > Low Intensity
P.J. O’Connor et al, American Journal of Lifestyle Medicine4(5)Mental Health Benefits of Strength Training in Adults ,September 2010Volume, 4(Issue5)Page, p.377To-396
http://reso
Sleep Disturbance
R- Routine
E- Exercise
S- Stimulants
T- Turmoil
Medications
Shifting Time Zones
Frau Jaeger
Risk Factors for Chronic Pain
- History of Motor Vehicle Collision , 9 months ago- Treated with medication, no rehab.
- Sedentary Lifestyle
- Underweight
- Family History of Rheumatoid Arthritis
- Susceptible to Anxiety and Stress
Psychological Screen
- Anxiety related headaches and increased muscle soreness
- Feels stressed and overwhelmed- Cries more easily - No vegetative depression signs- Complains of poor memory and
concentration- Mental Status is normal
Muscle Tension Reduction
Physical– Posture– ADL– Tight Muscle Groups– Stretching Techniques– Injury Prevention– Rest– Ice
Psychological– Stressors– Anxiety– Pain Cycle– Sleep Quality– Deep Breathing
Stress Management
Personality Preferences
Priorities & Planning
Decision Making
Circle of Support
Assertiveness
Attitudes
Motivation
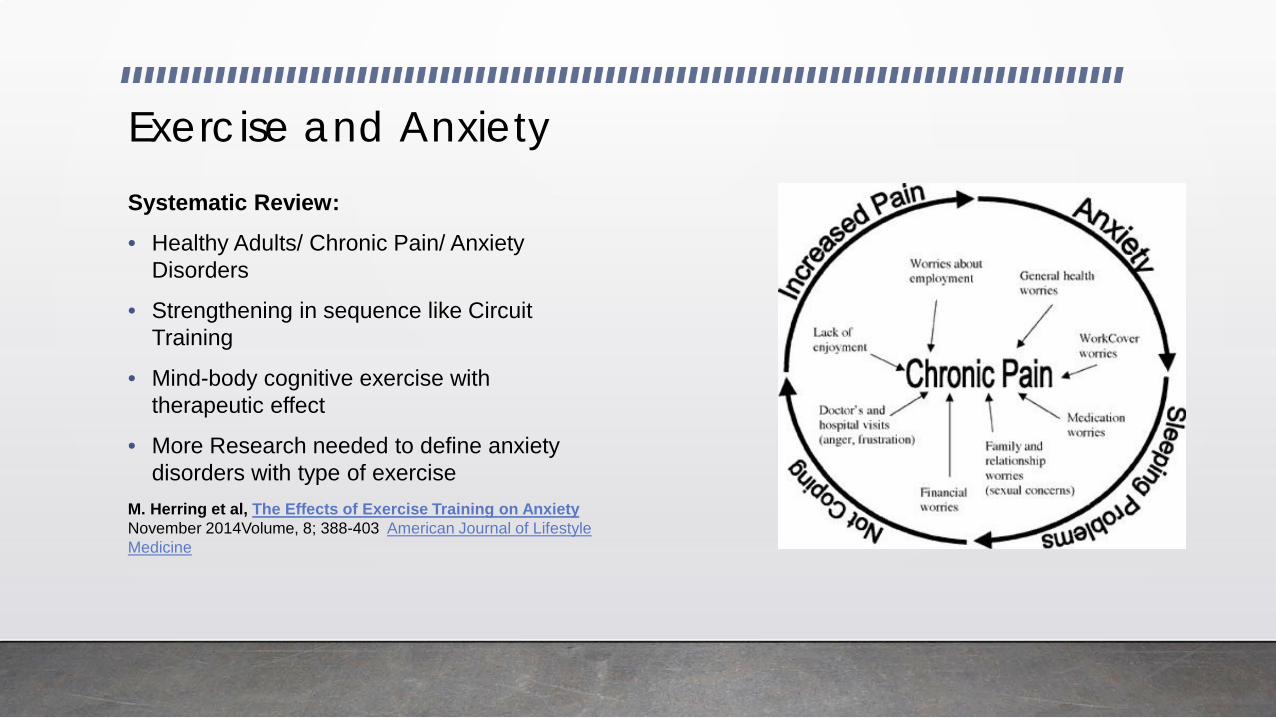
Exercise and AnxietySystematic Review:• Healthy Adults/ Chronic Pain/ Anxiety
Disorders
• Strengthening in sequence like Circuit Training
• Mind-body cognitive exercise with therapeutic effect
• More Research needed to define anxiety disorders with type of exercise
M. Herring et al, The Effects of Exercise Training on Anxiety November 2014Volume, 8; 388-403 American Journal of Lifestyle Medicine
Physical Exam
- Strength - Static- normal- Endurance- sit to stand or ¼ squat- Stability- single stand or heel raise
- Neurological- Normal dermatomes, myotomes, reflexes
- Special Tests- Pain Behaviours- Joint Specific
Physical Exam
- Observation:- Facial pain expression, slowness in movement
- Active R.O.M. - Full with painful stretch at the end of range
- Passive R.O.M. normal
- Positive Trigger points 11/14
Planning Priorities
Education
Correct the Sleep Disturbance
Reduce the Muscle Tension
Stress Management and Relaxation
Increase Daily Physical Activity/ Exercise
Targeted Strengthening
Increase Endurance
Education
Fears and Myths and Language
Physiology
Good Pain/ Bad Pain
Triggers and Reactions
Guidelines and Acronyms
Daily Physical Activity
Energy Conservation
Energy Spenditure
Choosing when to use automation
Good Day Activity
Bad Day Activity
Using rest wisely
Treatment Plan – Exercise and Chronic Pain
• Osteoarthritis – Moderate Strengthening of lower extremity is very effective and can be done as aerobic walking or resisted movements (8 RCT’s)
• Low Back Pain – Moderate strengthening yielded functional change and 40% reduced pain levels equal to aerobic training. (5 RCT’s)
• Fibromyalgia- Strength training demonstrated more benefit than flexibility. Aerobic benefit was equal to strength but patient compliance was low. (4RCT’s )
Targeted Strengthening
Address Large muscles first
Flexors tend to tighten
Extensors tend to weaken
Postural muscles are a priority
Trunk Stabilization
Assessment must be detailed to customize program
Consider Right, Left, Upper, Lower
Aerobic Exercise
• Retrain the Brain
• Increase chemical changes
• Overall coordination
• Neuromuscular Benefits
• Mindfulness Movement
• Mind-Body Movement

Urbanpoling.com
Endurance Guidelines
The One Minute Manager
Increase 10% every 3 sessions
Increase one parameter at a time– Repetitions, Length of Hold, Weight, Time
Reduce 25% for every week off
Off one month, restart at Baseline
Warm-up, cardio, strengthen, stretch, cool down
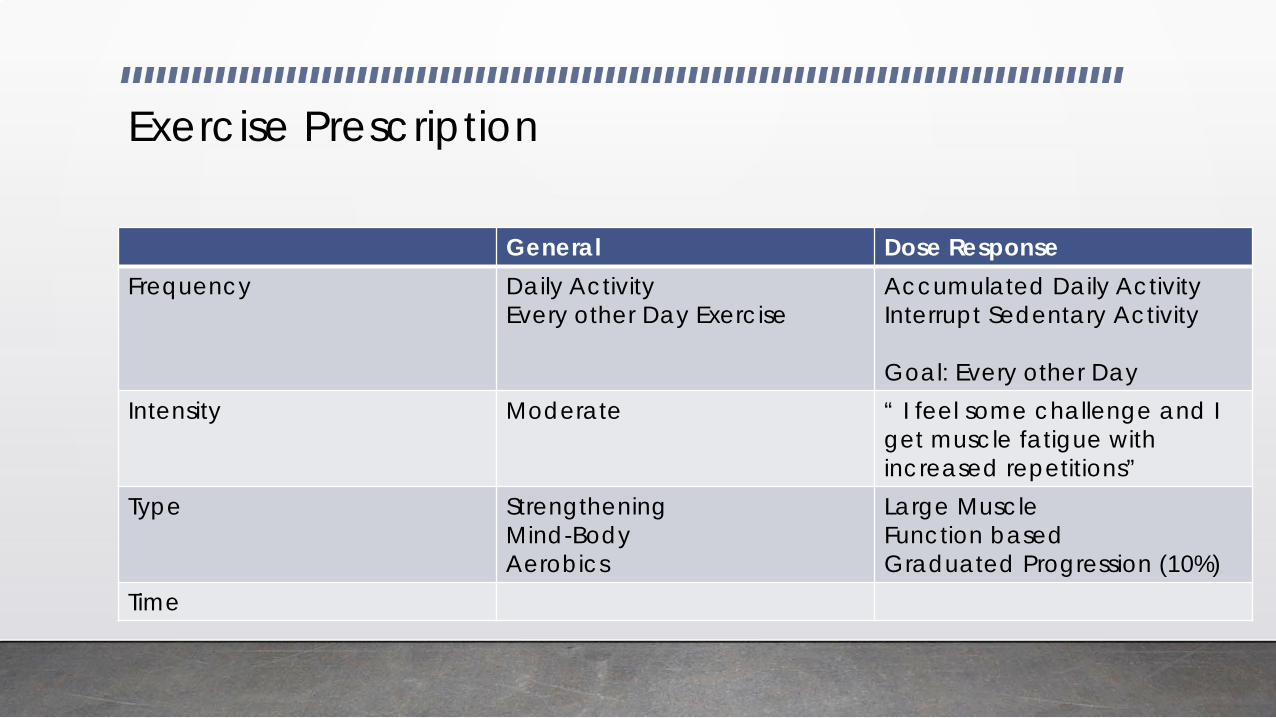
Exercise Prescription
General Dose ResponseFrequency Daily Activity
Every other Day ExerciseAccumulated Daily ActivityInterrupt Sedentary Activity
Goal: Every other DayIntensity Moderate “ I feel some challenge and I
get muscle fatigue with increased repetitions”
Type StrengtheningMind-BodyAerobics
Large MuscleFunction basedGraduated Progression (10%)
Time
Summary
1. Exercise is evidence-informed treatment for Acute and Chronic Pain conditions – targeting pain pathways, mood changes & sleep disorder
2. Combine with Education, Activities of Daily Living and Pain Medication
3. Start with Strengthening – Large muscles, Low Repetition, Long Holds
4. Add mind-body awareness movement – Function based, Posture based
5. Add Endurance/ Aerobics
Case 2: My Aching Bones
58 year old male with complaints of bilateral knee pain and left hip pain.
- morning stiffness lasting an hour
- reduced walking tolerance to 15 minutes painfree
- using acetominophen on a regular basis
- Wants to continue with jogging and tennis
Physical Exam
- Medial Joint line tenderness
- Mild effusions
- 5 degree flexion contractures
- Valgus mal-alignment
- Decreased proprioception
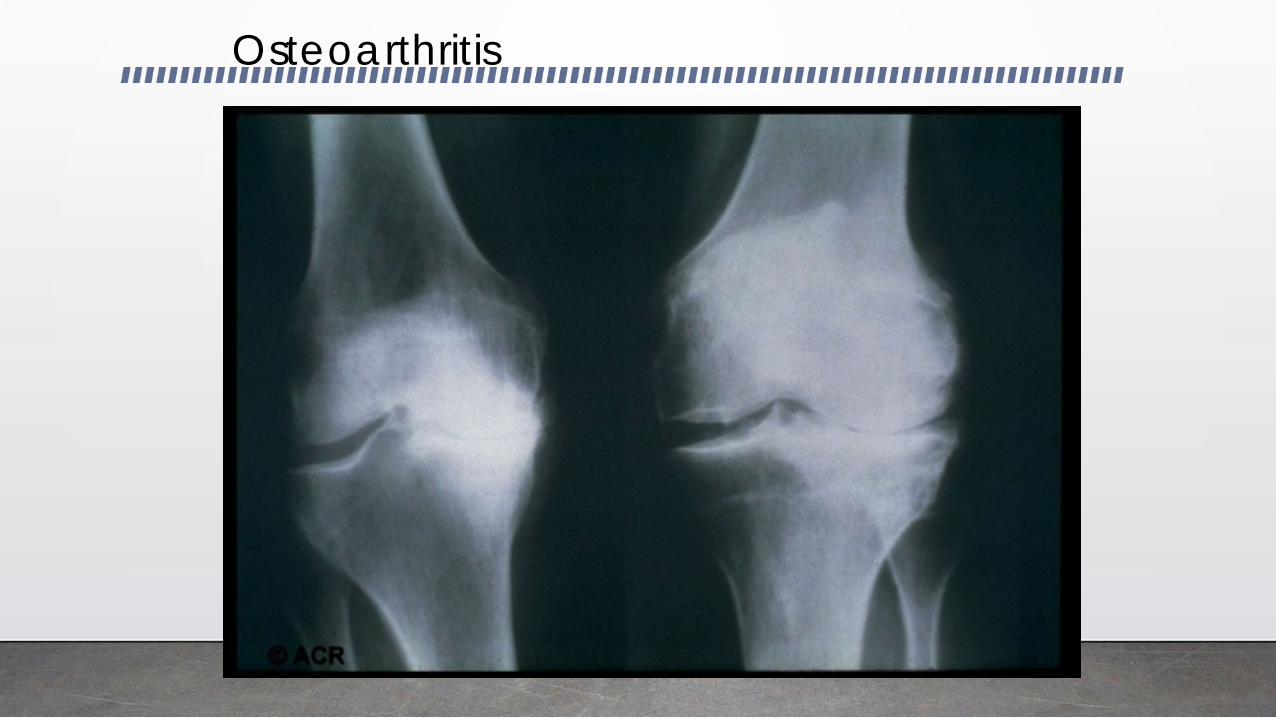
Osteoarthritis
American College of Rheumatology
Guidelines for Care:
1) Control Pain
2) Improve of Quality of Life
3) Avoidance of Drug Toxicity
Arthritis & Rheumatism, Vol 43, No. 9, Sept. 2000, pp 1905-1915
Non-Pharmacological Treatment of Knee Osteoarthritis
Patient Education
Self management Programs
Weight Loss
Exercise: ROM, Strength, Aerobics
Gait Assistance
Joint Protection
Assistive Devices
Hot water exercise therapy
Pharmacological TreatmentDecrease Pain = Increase Function
Oral:
- Acetominophen
- NSAID’s
- Topicals
- Tramacet
- Injectables