exomesequencing and rare diseases - national …/media/files/activity files/research... · and be...
TRANSCRIPT
Exome Sequencing and Rare Diseases
Holly K. Tabor1,2 and Michael Bamshad1,21 Department of Pediatrics, University of Washington2 Seattle Children’s Hospital
IOM Committee on Accelerating Rare Diseases Research and Orphan Product DevelopmentWashington, DCFebruary 4, 2010
Outline
• What is exome sequencing and how does it work?
• Freeman-Sheldon syndrome and proof of principle
• Miller Syndrome
• Family perspectives on whole exome and whole genome sequencing research
• Ethical challenges in genomic research on rare diseases
Rationale
• Rare, monogenic disorders are of intense biomedical interest
• Genetic basis of most Mendelian disorders unknown
• Unlikely to be solved by traditional gene mapping strategies
• Can we use exome sequencing as a genome-wide scan for rare Mendelian disorders?
What is the Exome?• ~30 Mb (~1% of the genome or ~180,000 exons)
• 5% or less sequencing required compared to analysis of whole genome
• Coding variants– Larger effect sizes– Majority of nonsynonymous variants probably deleterious– Easier to interpret results and follow up
Scale Testing• 16 exomes completed
– 64 Gb per individual (mapped 76 bp reads)– 51x mean-fold coverage of each exome– 96.3% called (>8x coverage and quality score >30)– Comparison to Illumina 1M-Duo
• ~99.98% concordance with homozygous calls• ~99.57% concordance with heterozygous calls
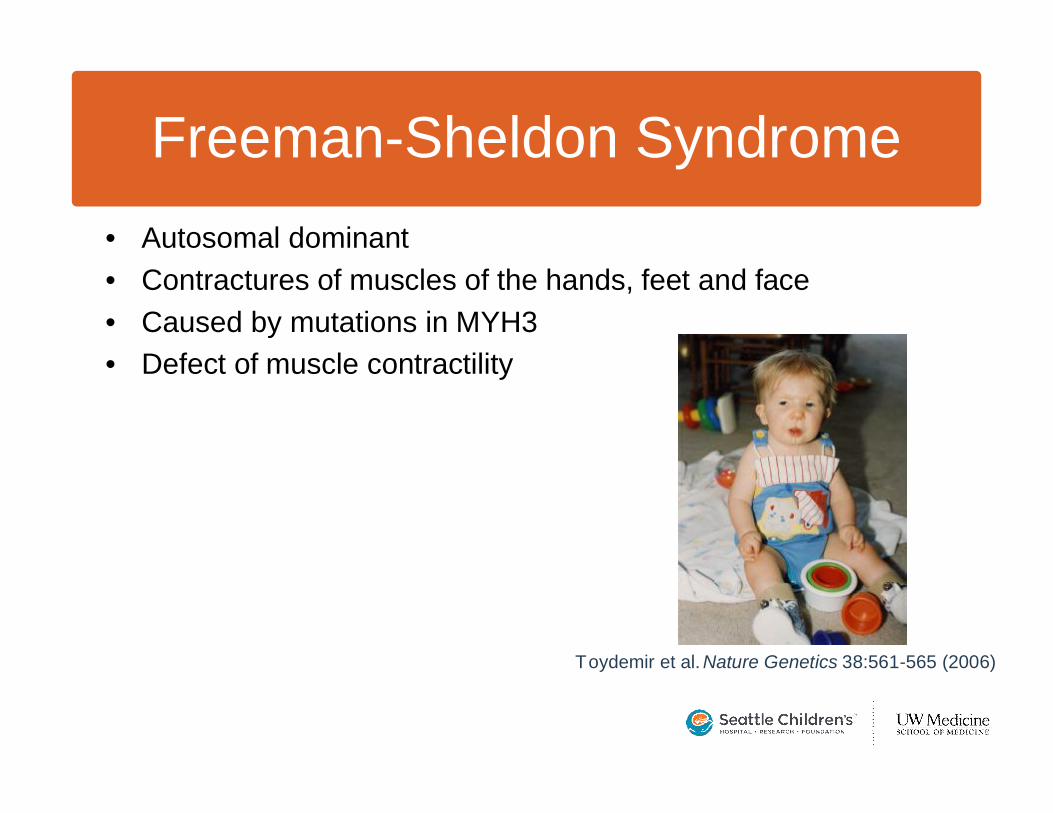
Freeman-Sheldon Syndrome• Autosomal dominant• Contractures of muscles of the hands, feet and face• Caused by mutations in MYH3• Defect of muscle contractility
Toydemir et al. Nature Genetics 38:561-565 (2006)
1 2/2 3/3 4/4 ANY 3/4
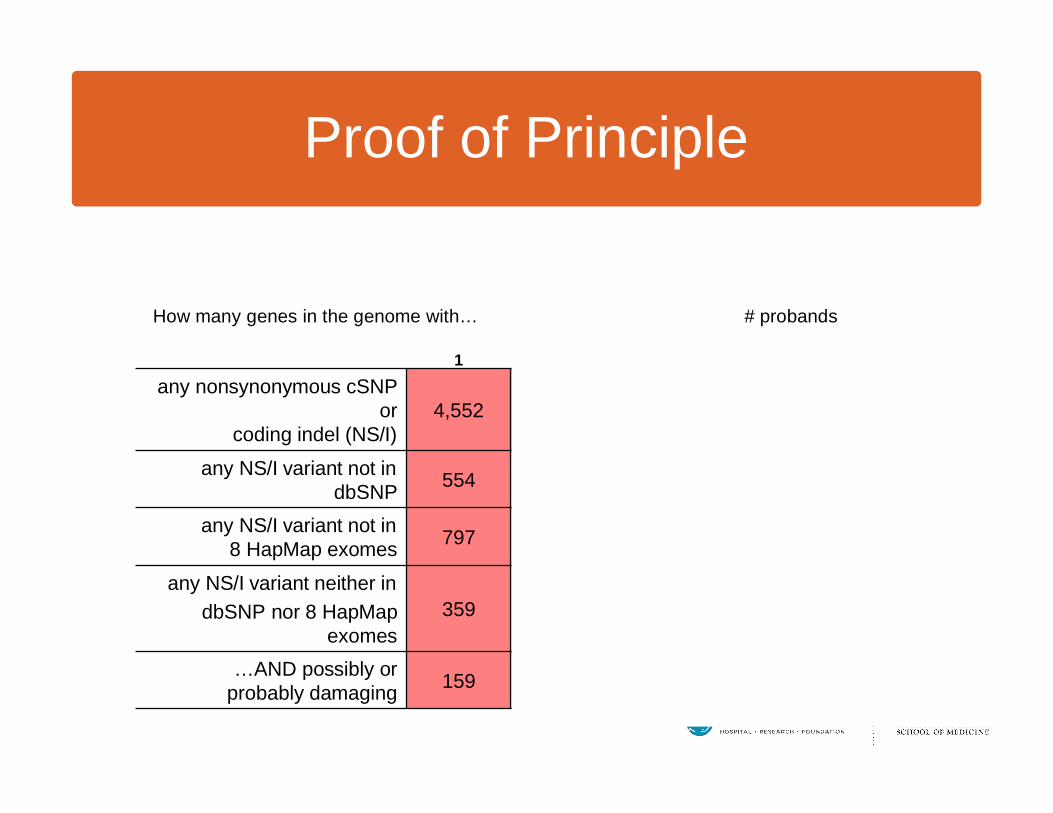
any nonsynonymous cSNPor
coding indel (NS/I)4,552 3,330 2,810 2,522 3,822
any NS/I variant not in dbSNP 554 171 112 87 174
any NS/I variant not in 8 HapMap exomes 797 167 54 22 159
any NS/I variant neither in dbSNP nor 8 HapMap
exomes359 37 8 1 (MYH3) 21
…AND possibly orprobably damaging 159 9 2 1 (MYH3) 2
How many genes in the genome with… # probands
Proof of Principle
1 2 3/3 4/4 ANY 3/4
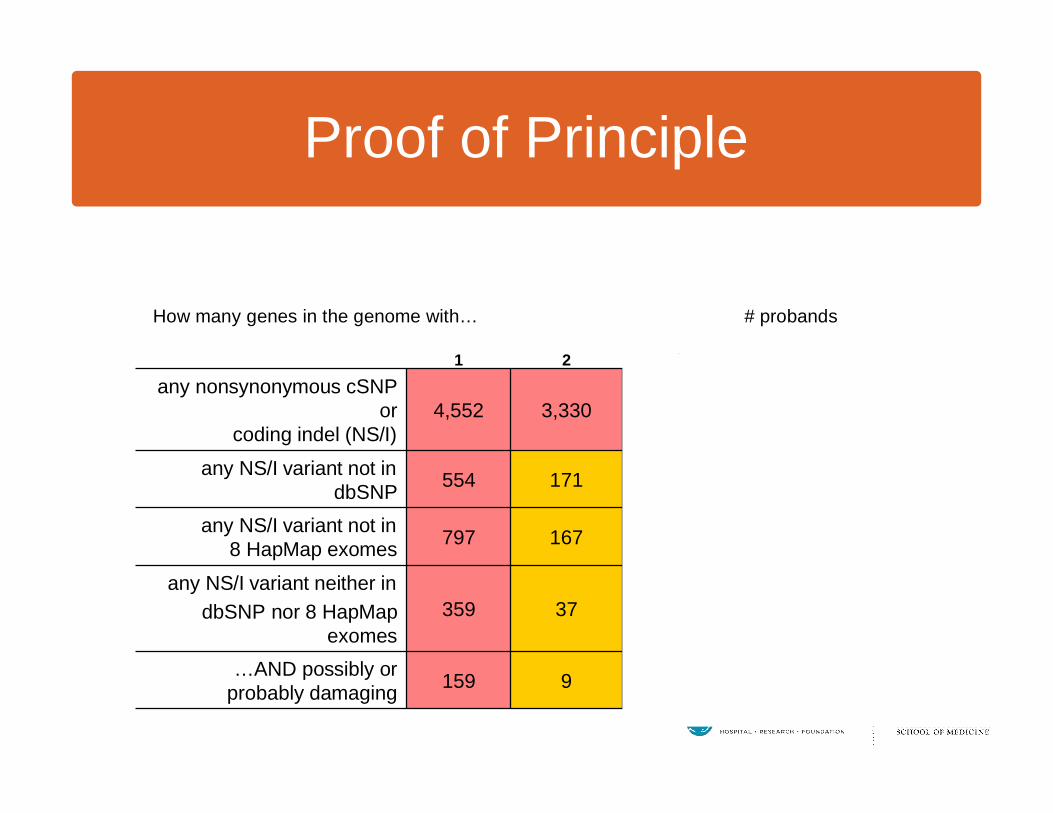
any nonsynonymous cSNP or
coding indel (NS/I)4,552 3,330 2,810 2,522 3,822
any NS/I variant not in dbSNP 554 171 112 87 174
any NS/I variant not in 8 HapMap exomes 797 167 54 22 159
any NS/I variant neither in dbSNP nor 8 HapMap
exomes359 37 8 1 (MYH3) 21
…AND possibly orprobably damaging 159 9 2 1 (MYH3) 2
How many genes in the genome with… # probands
Proof of Principle
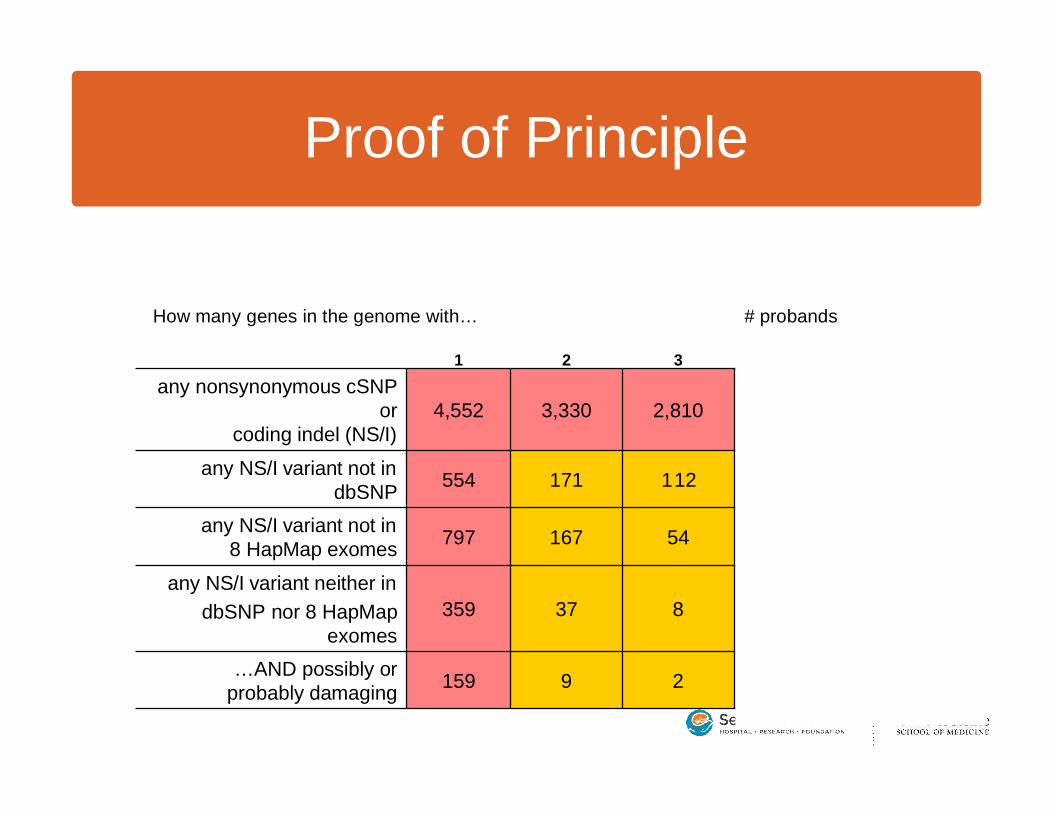
1 2 3 4/4 ANY 3/4
any nonsynonymous cSNP or
coding indel (NS/I)4,552 3,330 2,810 2,522 3,822
any NS/I variant not in dbSNP 554 171 112 87 174
any NS/I variant not in 8 HapMap exomes 797 167 54 22 159
any NS/I variant neither in dbSNP nor 8 HapMap
exomes359 37 8 1 (MYH3) 21
…AND possibly orprobably damaging 159 9 2 1 (MYH3) 2
How many genes in the genome with… # probands
Proof of Principle
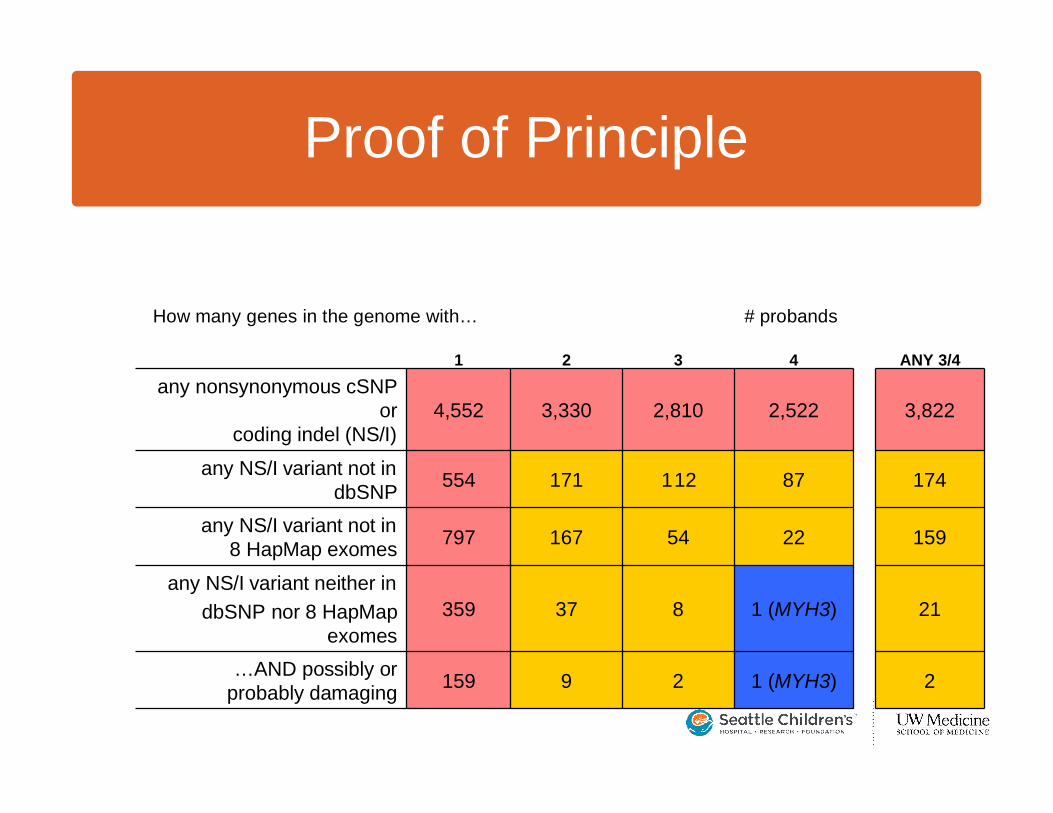
1 2 3 4 ANY 3/4
any nonsynonymous cSNP or
coding indel (NS/I)4,552 3,330 2,810 2,522 3,822
any NS/I variant not in dbSNP 554 171 112 87 174
any NS/I variant not in 8 HapMap exomes 797 167 54 22 159
any NS/I variant neither in dbSNP nor 8 HapMap
exomes359 37 8 1 (MYH3) 21
…AND possibly orprobably damaging 159 9 2 1 (MYH3) 2
How many genes in the genome with… # probands
Proof of Principle
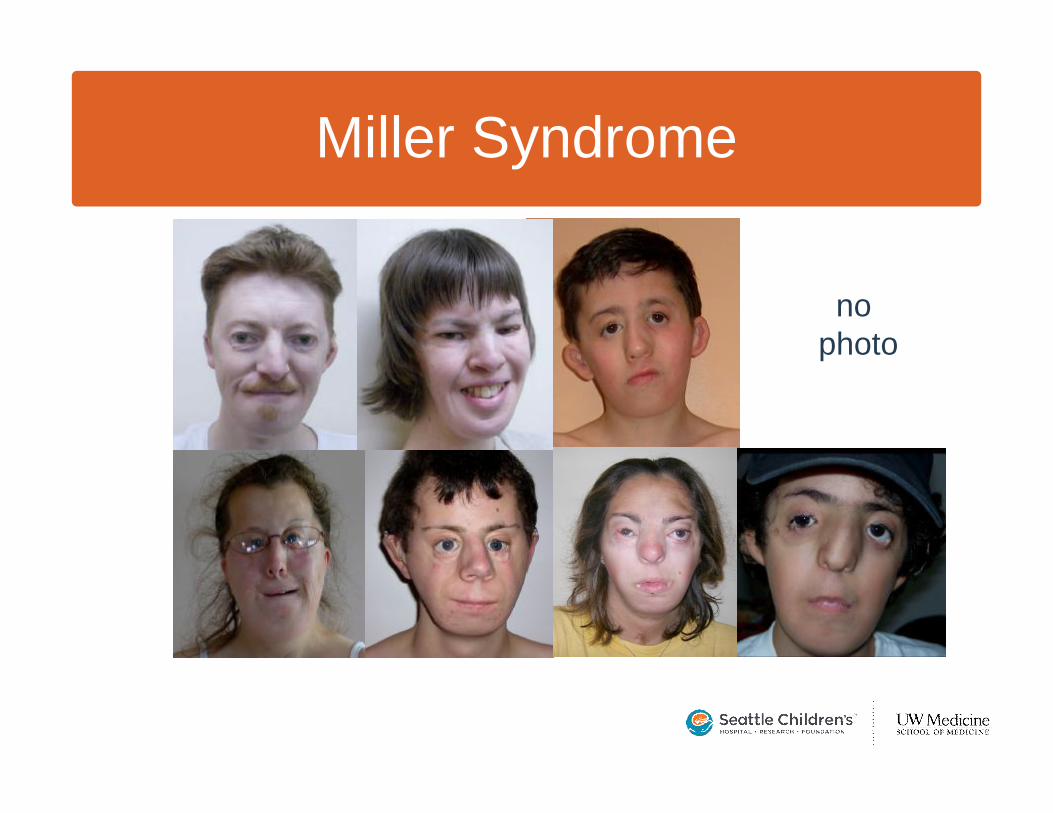
Miller Syndrome
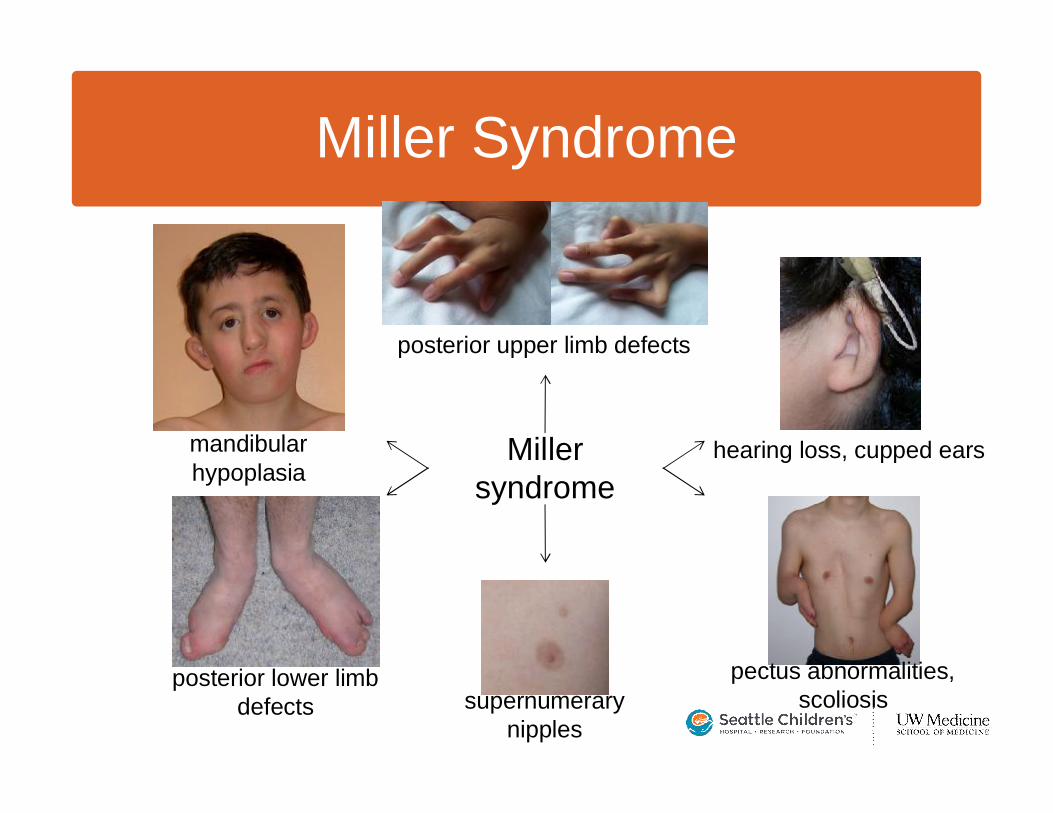
Miller syndrome
posterior upper limb defects
pectus abnormalities, scoliosissupernumerary
nipples
posterior lower limb defects
mandibularhypoplasia
hearing loss, cupped ears
Miller Syndrome
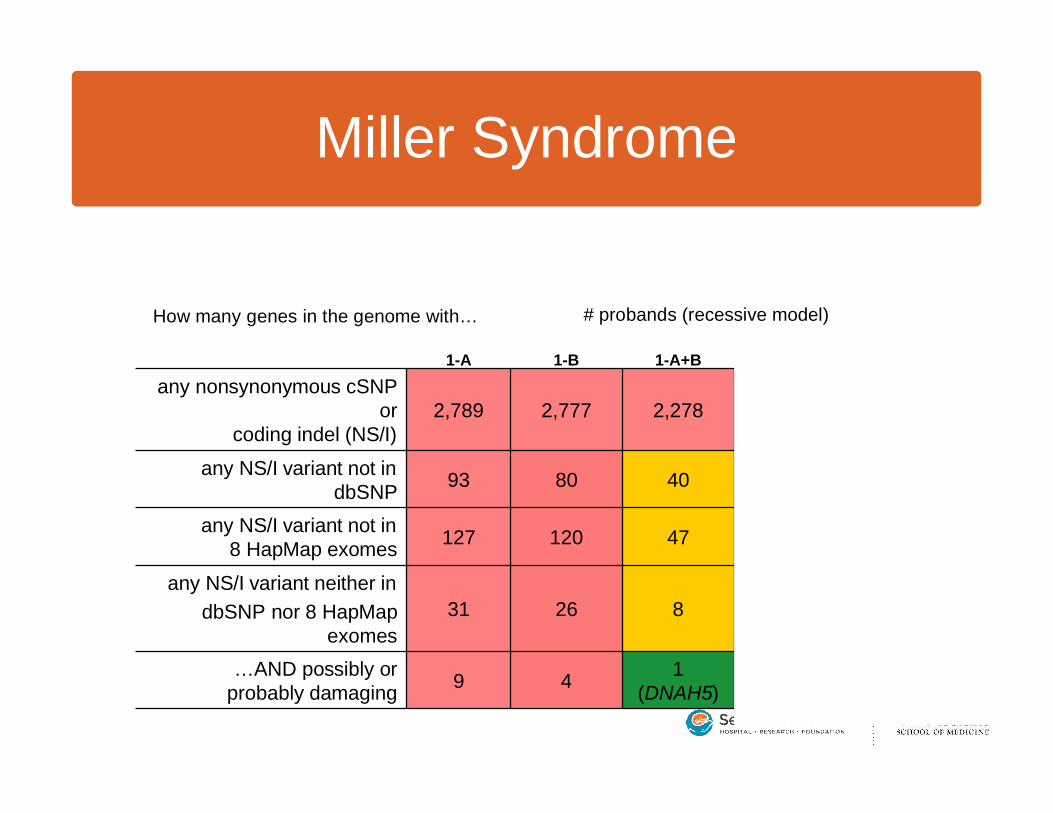
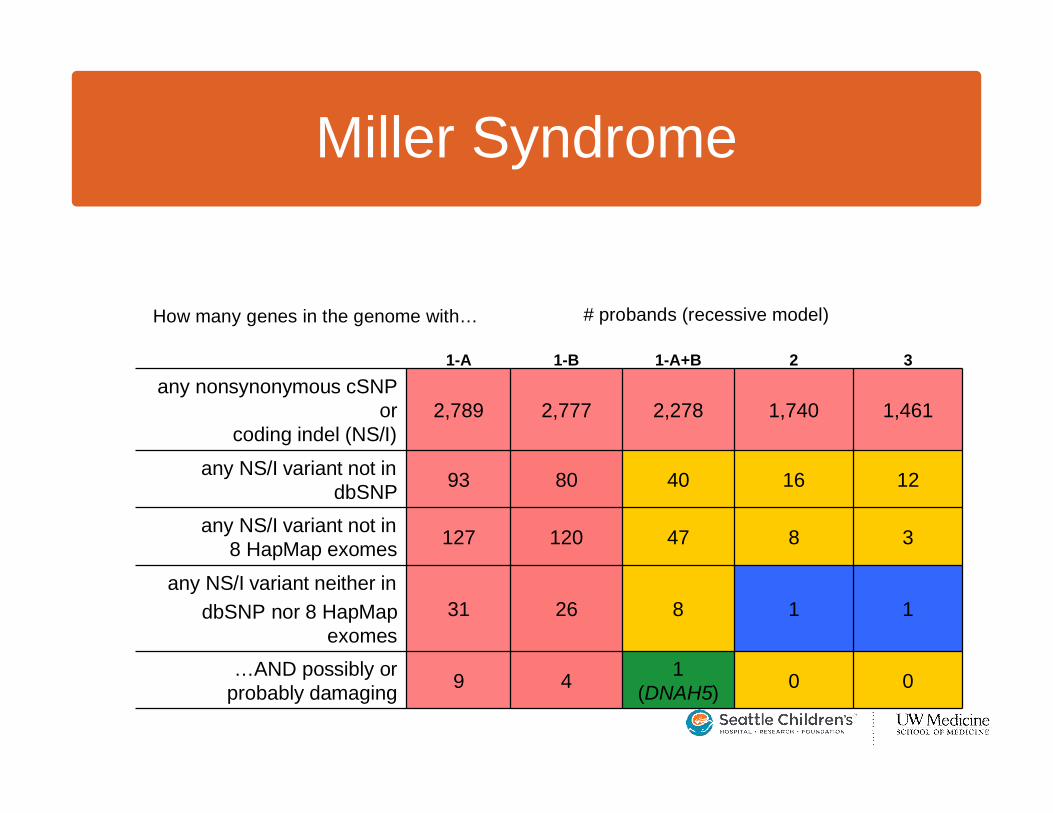
1-A 1-B 1-A+B 2 3
any nonsynonymous cSNP or
coding indel (NS/I)2,789 2,777 2,278 1,740 1,461
any NS/I variant not in dbSNP 93 80 40 16 12
any NS/I variant not in 8 HapMap exomes 127 120 47 8 3
any NS/I variant neither in dbSNP nor 8 HapMap
exomes31 26 8 1 1
…AND possibly orprobably damaging 9 4 1
(DNAH5) 0 0
How many genes in the genome with… # probands (recessive model)
Miller Syndrome
1-A 1-B 1-A+B 2 3
any nonsynonymous cSNP or
coding indel (NS/I)2,789 2,777 2,278 1,740 1,461
any NS/I variant not in dbSNP 93 80 40 16 12
any NS/I variant not in 8 HapMap exomes 127 120 47 8 3
any NS/I variant neither in dbSNP nor 8 HapMap
exomes31 26 8 1 1
…AND possibly orprobably damaging 9 4 1
(DNAH5) 0 0
How many genes in the genome with… # probands (recessive model)
Miller Syndrome

Nature Genetics, Nov. 13, 2009
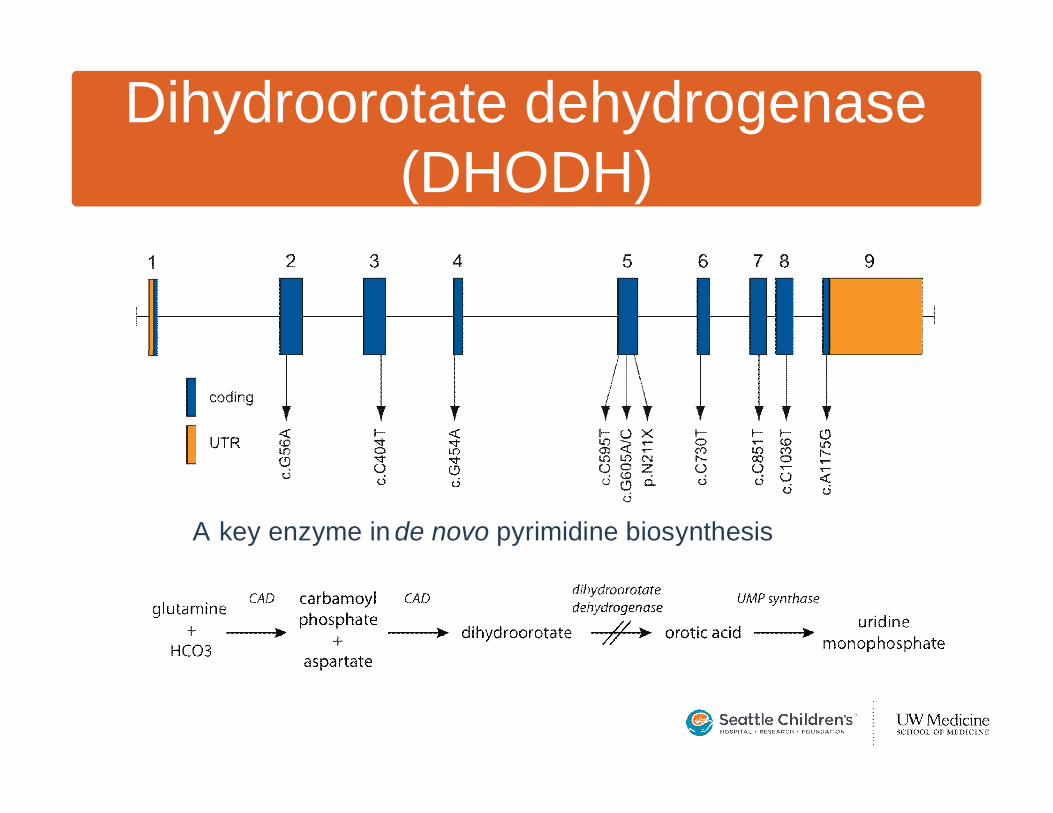
Dihydroorotate dehydrogenase(DHODH)
A key enzyme in de novo pyrimidine biosynthesis
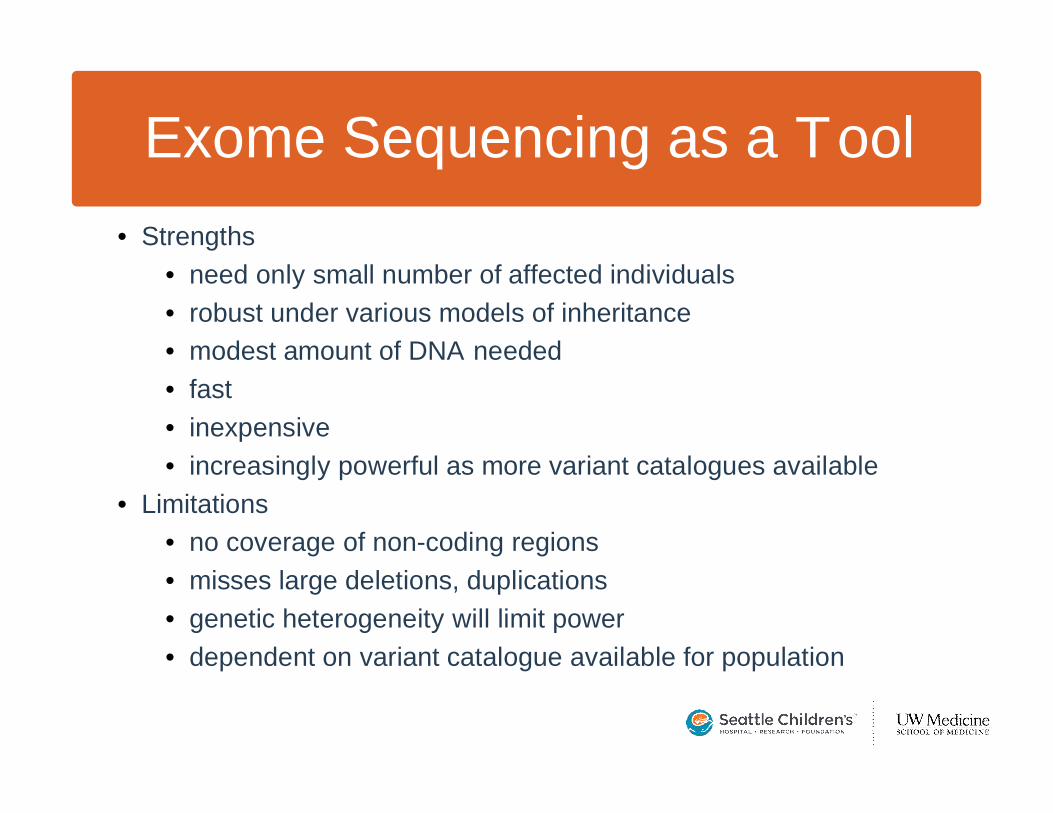
Exome Sequencing as a Tool• Strengths
• need only small number of affected individuals• robust under various models of inheritance• modest amount of DNA needed• fast• inexpensive• increasingly powerful as more variant catalogues available
• Limitations• no coverage of non-coding regions• misses large deletions, duplications• genetic heterogeneity will limit power• dependent on variant catalogue available for population
Ethical Challenges
• Greater absolute risk to privacy and confidentiality, particularly in light of data sharing requirements
• How should sequence data of individuals with rare diseases be identified in dbGAP?
• Are the goals and risks/benefits of data sharing the same for rare diseases as for GWAS of common complex traits?
• How can increases in absolute risk be balanced with increased perceived/potential benefit?
Confidentiality and Privacy• Not concerned about risks to confidentiality and privacy• A “published life” and a ranking of priorities
– “We’ve never kept our kids hidden…our kids have been published. Our life has been published, if you like, their medical history has already been published. It’s there for people to see, and it’s there for other medical professions to be involved with….there’s more things to be worried about in our life right now, than whether we might be known or not, in a study.” (parent)
Confidentiality and Privacy• Different concerns, perceptions for families with disease• Challenges to living with a disease with visible disability
– “They [researchers] don’t understand what little privacy we have, every day we step out the door. When I’m with…[my children], I have no privacy as far as people staring?…[My children] can’t go anywhere and be incognito, or invisible. So again, our perception of privacy is a lot different than, than somebody who has a normal body.” (parent)

Confidentiality and Privacy• In a pool with information from others
– “It doesn’t sort of really worry me, because there are lots of other things that are in medical journals…And so mine would just be in a pool with all the other information really..” (affected offspring)
• Worth the risk– “I understand the amount [of privacy protection].... And
beyond that, nobody can control anything. So it’s worth the risk.” (parent)
Ethical Challenges
• Challenges around return of results• How and whether to return carrier status? • How many clinically relevant mutations reside in the exome of
every individual?• Should information about these mutations be given to research
participants? • How should decisions about the clinical relevance of mutations
be made? • Who should make these decisions?
Not Yet Thought It Through“Whatever answers or information that they do GIVE, that’s what I
will start asking about, ‘cause obviously, now, I don’t, I don’t even know what to be asking for...” (affected offspring)
“I think I’d just be happy in general to get results back…I’ve never really thought about what I WOULDN’T want to know…”(unaffected offspring)
“I honestly don’t know how I’m going to feel…if I’m told I have a gene for Alzheimer’s…I have no idea how I’ll feel about it until it happens. So, I may not want to just like say, “okay, everybody. Bye, I’m gonna go back to work now…I just think I didn’t realize how I would want it until right now.” (parent)
Impact of Results“I was kind of surprised, since we’ve lived with the rarity of the condition
and everything for so long that the next day, I was really kind of accosted with... emotions in how unlucky we’ve been…I actually felt just the sadness of the whole reality.” (parent)
“what I thought about genetics and hereditary (sic) has changed considerably, from before the test and after the test…hereditary traits don’t mean the same thing that they meant to me when, like, say, six months ago….” (parent)
“I get to create a normal human being, even though I’m... I’m different. And that’s sort of like a... I guess that my brain is thinking about it like a... a... like an “up yours” kind of thing, I guess?” (affected offspring)
Ethical Challenges
• Challenges in making translational genomics a reality
• How to make genetic tests rapidly clinically available?• How to facilitate translational research that may lead to the
development of treatments and interventions that mitigate the effects of these diseases and improve quality of life?
• How to make interventions accessible and affordable for all?
Ethical Challenges
• Challenges in recruitment and enrollment for rare disease research
• Oct 2008 OHRP guidance makes the traditional model of referral and recruitment for rare diseases impossible
• IRBs are struggling with the implementation of this guidance• Revision/exemptions to the guidance for rare diseases are
needed• New models of recruitment, consent, ongoing engagement with
research participants and communities is required
Conclusions• Exome resequencing is a powerful strategy to for
dramatically reducing the pool of candidate genes for monogenic disorders, if not identifying the responsible gene(s).
• Miller syndrome is an inborn error of metabolism caused by mutations in DHODH and reveals a novel role/pathway in craniofacial and limb development
• Approach will likely become a standard tool for the discovery of genes for rare monogenic disorders, modifiers of monogenic disease, and rare variants contributing to common disease
Conclusions• Exome resequencing presents familiar and novel
challenges in research ethics and translation• Empirical data is needed about how to communicate with
research participants about the risks and benefits of this kind of research and about research findings
• Researchers, institutions, funding agencies and regulatory bodies need to develop novel approaches to managing these challenges and engaging with participants and disease communities
Next• distal arthrogryposis type 5• Kabuki syndrome• Nager syndrome• Hallermann-Streiff• pontine tegmental cap dysplasia• idiopathic thrombocytopenic purpura• Joubert syndrome• scalp-ear-nipple syndrome• Toriello-Carey
AcknowledgementsThe Study Participants
University of Washington• Michael Bamshad• Jay Shendure• Maggie McMillin
Seattle Children’s Hospital/Treuman Katz Center for Pediatric Bioethics
• Jacquie Stock• Tracy Brazg• Kaiti Carpenter• Ben Wilfond
University of Utah• Karin Dent
Institute for Systems Biology• David Galas
Funding from NHGRI and NHLBI
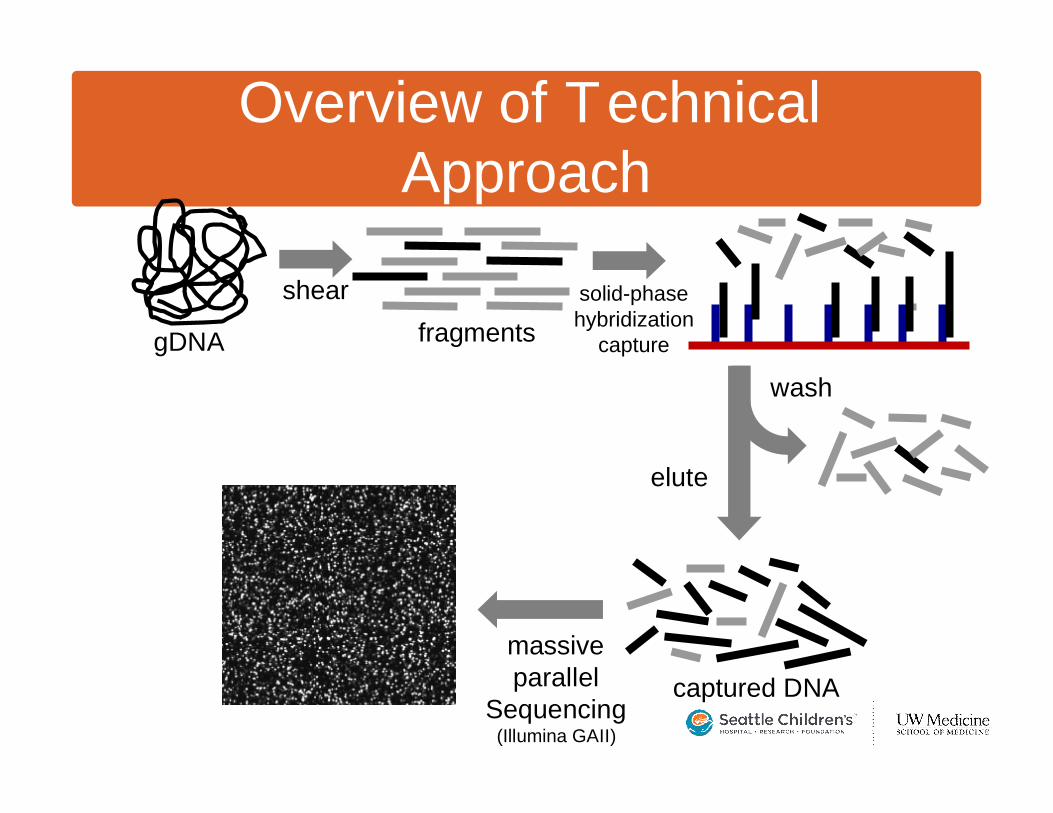
shear
gDNA fragments
wash
captured DNAmassiveparallel
Sequencing(Illumina GAII)
elute
solid-phasehybridization
capture
Overview of Technical Approach
no photo
Miller Syndrome
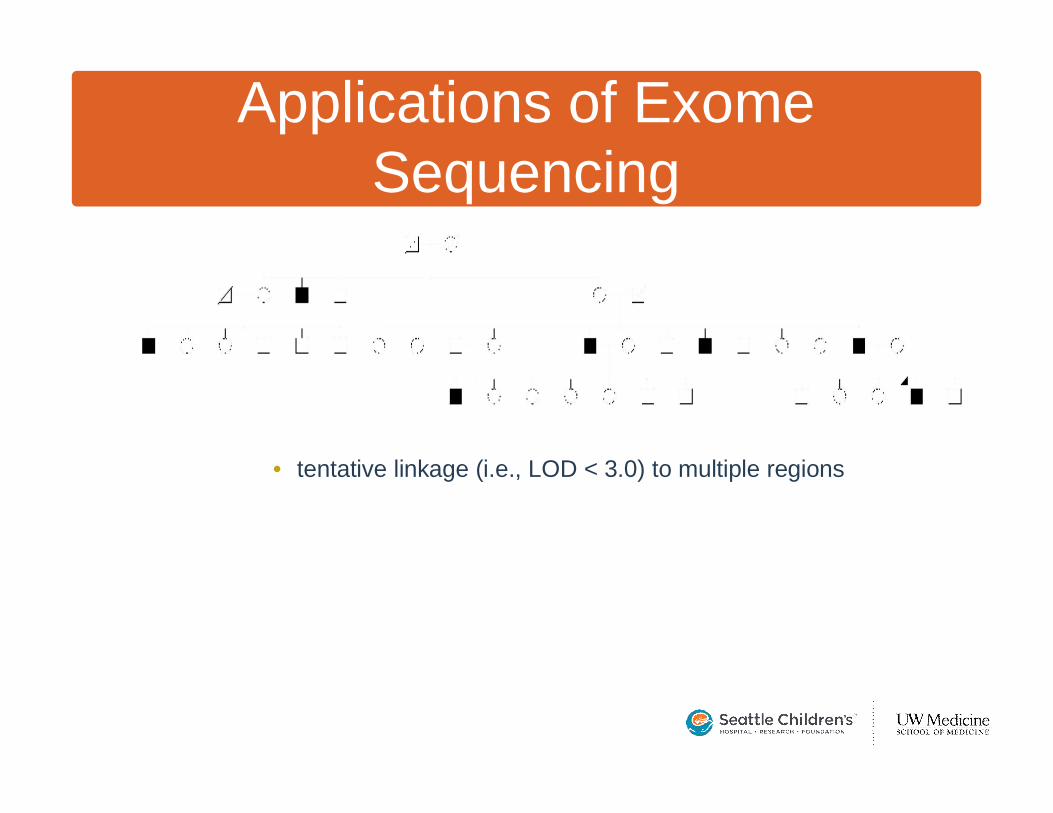
• tentative linkage (i.e., LOD < 3.0) to multiple regions
Applications of ExomeSequencing
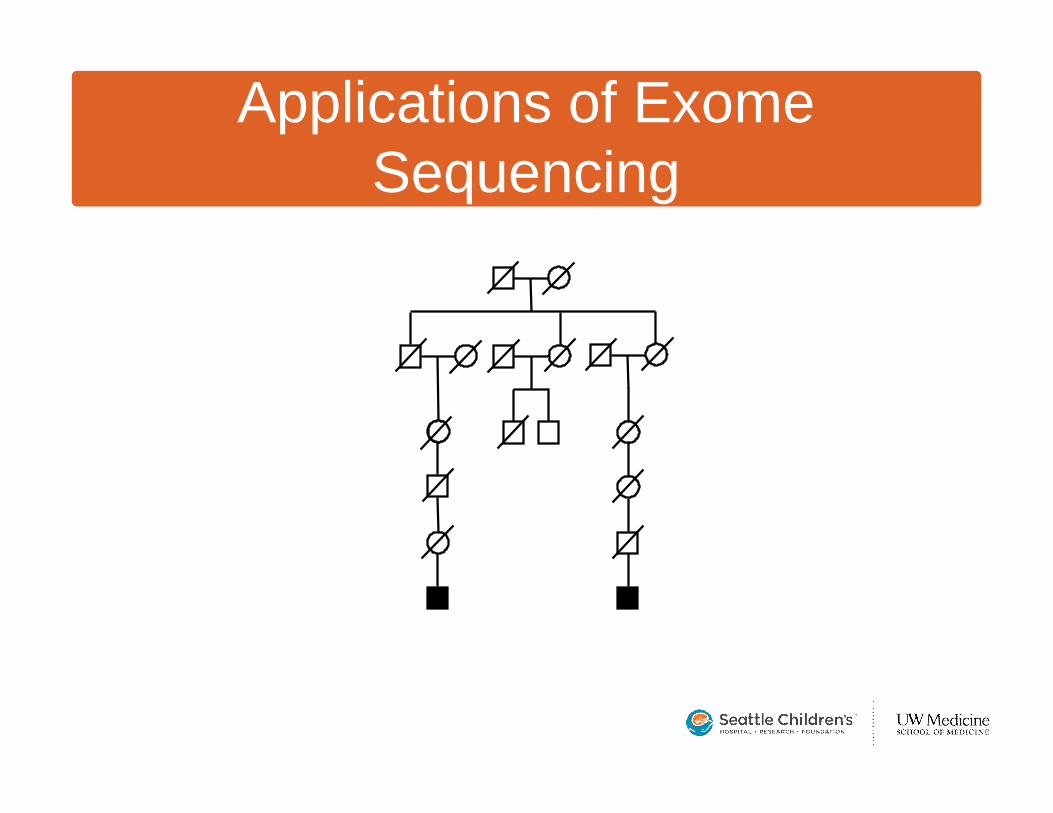
Applications of ExomeSequencing